
CPAP primer for the otolaryngologist - AOCOOHNS primer for the otolaryngologist Tod C. Huntley, MD FACS [email protected]
Mar 27, 2018
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


OSA panelOSA treatment: medical and surgical
Tod C. Huntley, MD FACSIndianapolis, IN

CPAP for Dummies The preferred initial treatment option
Roles in OSA treatment1. Definitive long-term therapy2. Temporary bridge until definitive therapy3. As combo therapy with surgery or oral appliance4. Testing modality for mild OSA:
If symptoms persist, rethink the diagnosis
Preferred by insurance, usually covered
3

APAP: auto-titrating PAPPressure needs can vary with body position and stage of sleep
APAP avoids a fixed pressure
Measures airflow breath-by-breath by measuring resistance to breathing
Adjusts to flow limitationAdjusts pressure slowly
Does not adapt to each event
4

BPAP: Bi-level PAP 2 levels of pressure
IPAP: higher inspiratory pressureEPAP: lower expiratory pressure Allows for easier exhalation
When to consider:“I can’t breathe out against the machine”
Allows for easier exhalation
IPAP and EPAP settings independently adjusted
Starting point: 4 cwp insp/exp gradient (e.g.: 20/16 cwp)
Generally for patients with higher pressure needs (~ > 14 cwp)
Expiratory Pressure Relief (EPR): “Poor man’s BiPAP” 5

Optional PAP features Heated humidifier Heated tubing
Ramp Exhalation pressure relief (C-flex, A-flex, EPR) Altitude adjustment
Compliance meters, downloadability
Chin straps Mask liners
6

CPAP goals Reduction or elimination of respiratory events
Reduction of morbidities associated with OSAObjective: cardiovascular events, hypertensionSubjective:Daytime somnolenceBedpartner satisfaction
Your job:Educate patientOptimize patient acceptanceMaximize long term adherence
Make patient healthier if planning surgery7

Adherence: 4 hr/night for 70% of nights
Non-adherence rate: 46-83% (!)Weaver TE, Grunstein RR. Proc Am Thorac Soci 2008;5:173–8.
Self-reported CPAP usage over-estimates nightly use cf download data by 1 hour
CPAP side effects:• insomnia• nocturnal awakenings• upper airway irritation• sneezing• nasal dryness• rhinorrhea• epistaxis
8
CPAP effectiveness & adherence

Data is continuously recorded Downloads by card or wirelessly
Usage dataNightly Cumulative
Mask leak: > 0.1-0.4 L/sec = poor mask fit
Residual event detection (AHI) Pressure data:
Mean pressureMean peak pressure90th percentile pressure
9
CPAP downloads

Pressure determination: options1. In-lab titration followed by fixed pressure CPAP
• Gold standard used by most sleep docs• Most expensive
2. Empiric APAP with lab titration when needed• Increasingly utilized; my preferred method
3. Fixed pressure CPAP after 1 week of APAP• Alternative to #2 preferred by some insurance
4. Fixed pressure CPAP determined by algorithm• Least precise, less efficacious with BP
normalization than other modalities
10

The sleep lab titration Objective pressure determination in the sleep lab Sleep parameters studied at different pressures Optimal pressure reported
Most labs: Done automatically as soon as OSA dx’dWorst night on CPAP is the first night--
why spend it in the expensive lab?
Pro: Most robust dataTime-proven
Con:CostAPAP proven as an effective alternative
11

The sleep lab titrationOptimal role : my opinion
Determination of optimal pressures in a patient already compliant with PAP therapy
Treatment of the more difficult patientSuspected complex OSAPersistent symptoms despite PAPHigh AHI with APAPSevere OSA Confirmation of APAP pressures
12

Empiric APAP vs. lab titrations APAP saves $$ by eliminating lab titration Reduces sleep lab’s revenue
APAP more expensive than CPAP
Many studies show similar outcomesPatient adherence and satisfaction may
be better with APAPBoth improve AHI to similar levels
Caveats:APAP might miss the rare complex OSA ptCaution: AHI from APAP download not a true
surrogate for PSG AHI (but is validated)
13

My usual CPAP algorithm Sleep study: Know what you are treating
Introduce. Educate. Show masks.
Set up with APAPSufficiently wide pressure range (6-20 cwp)Mask of choiceHeated humidifier
Troubleshooting:VendorOffice staff
14

My usual CPAP algorithm
15
Follow up at 6 weeksPatient brings the CPAP machine & mask to visit Data download and subjective report from patient Trouble shoot
If patient adherent and willing to continue: Continue with APAP if sufficiently improved Follow up 3-6 months later with downloads Follow up every 6-12 months and prn
Consider lab titration for Patient who is past over the honeymoon period Persistent symptoms, severe cases, etc.

My usual CPAP algorithm
If nasal obstruction interfering: treat the nose
If patient won’t use and can’t be convinced:Thorough discussion of risks, benefits, alternativesConsider oral appliance if applicableConsider appropriate surgical procedures
Communication and education: the keys to success
16

CPAP adherence problems Lack of education / communication / follow up
Overly eager patient or surgeon
Improper set-upMask fit (like buying shoes)Too little pressure (still snoring or tired)Too much pressure (aerophagia, arousals)Difficulty in exhalation: consider EPR, BiPAPImproper humidificationToo short of ramp
Claustrophobia, discomfort Lifestyle: travel, camping, etc. Nasal obstruction, sinus issues
17

CPAP masks: nasal
18
Profile LiteWisp

CPAP masks: pillows
19
Nasalaire
Adam Circuit
Comfort Lite

CPAP masks: full face
20

CPAP masks: other
21
CPAP Pro
Oracle
Hybrid

“Just like buying shoes”
22

CPAP ordering It’s not rocket science
Involve the patient
Know your vendorsHands on examination of masksAvailability, communication
Manufacturers will provide demos:Samples of masksDummy machinesEducational materials
23

HOW TO IMPROVE CPAP ADHERENCE
24

Motivate your patient

Nasal obstruction prevalence in CPAP users: 25-45%Hoffstein V et al. Am Rev Respir Dis 1992;145:841–5, Brander PE et al. Respir Int Rev Thorac Dis 1999;66:128–35, Pep JL et al. Chest1995;107:375–81
Compliance affected by • Nasal airway volume & cross-sectional volume Li et al. Sleep 2005;28:1554–9
• Increased nasal resistance Sleep 2005;28:1554–9
• Poiseuille’s Law: resistance to airflow is directly proportional to the length & inversely proportional to the fourth-power of the radius.
• 10% increase in cross-sectional area of the nasal airway can result in an increase of 21% of nasal airflow
Multiple studies: Nasal surgery reduces CPAP pressures and/or improves CPAP acceptance, compliance, tolerance, adherence, or use.
Don’t forget the nose!

Nasal obstruction? Consider C-flex or BiPAP
PAPFlex will improve adherence in patients with high nasal resista

Meta-analysis of isolated nasal surgery on CPAP
18 articles, 279 patients
Isolated nasal surgery results in:• CPAP mean pressure reduction of 2.66 cwp (0.8-4.8)
• Best results: septoplasty with turbs, though results observed independent of surgery subset addressed
• CPAP use increase (11 studies)• Regular use increased from 38.7% to 90.2%• Mean hrs of use incr from 3.0 + 3.1 to 5.5 + 2.0 hr
Nasal surgery can help CPAP use
ORAL APPLIANCES

SomnoMed
TAP EMA
Oasis
Klearway
PM Positioner
OPAP

SomnoGuard AP
Titratable thermoplastic appliances

ORAL APPLIANCE
Success (AHI < 10): varies with severity Mild OSA: 81%
Moderate OSA: 60%Severe OSA: 25%

EFFICACY
AHI reductionAll studies:
• Success rate (AHI < 10): 54%
• Response rate (50+% ↓ AHI, AHI > 10): 21%
Randomized, cross-over, placebo-controlled trials:
• Success rate: 50%; response rate: 14%
Snoring
Review of 89 studiesn = 3,027

Compliance at 1 year 24% discontinuation (148/619)
Best predictors of successNo nasal obstruction
Positional OSA (defined as lateral AHI < 10) Women
Mild OSA or non-apneic snoring

POOR PREDICTORS FOR OAInadequate dentition:
8-10 teeth/arch, > 2 posterior teethSignificant periodontal disease
< 25 mm opening, unable to protrude > 7 mm
Active TMJ
Progressive neuromuscular disease
Steep mandibular plane
Neck circumference > 20” men, 17” womenChronic nasal obstruction

SIDE EFFECTS OF OA THERAPY
Most common
• Excessive salivation
• Pain -- tooth, TMJ, headache, tongue
• Dental / occlusion changes in up to 85% of patients• Variable and progressive• Not always clinically relevant• Usually reversible over 1st 6 months
• Long term follow up necessary
• OSA control supercedes maintenance of baseline occlusion
AM Aligner

Other surgical options

Hyoid and tongue base suspension

Siesta MedicalAirlift system

Inspire Upper airway stimulation

The Inspire® system

No stimulation Stimulation on

Reference: 2 slices
Palate
Tongue base
Off
Off
On
On
Drug-induced sleep endoscopy

Resultsn = 126 (124 completed f/u at 12 mo)• AHI 32 + 11.8, BMI 28.4 + 2.6 (18.4-32.5)• 22 prior UPPP• Mean age 54.5 yr (31-80)• All non-adherent to CPAP therapy• Self-reported daily use: 86%; average objective use: > 5 hr / noc
Median AHI reduction: 68% (29.3 to 9.0)Median ODI reduction: 70% (25.4 to 7.4)Reduction or AHI >50% and AHI <20: 66% (83 of 126)ODI reduction of >25%: 75% subjectsFOSQ & ESS changes: clinical significantMedian % sleep time <90%: 5.4% to 0.9%
RESULTS DURABLE TO 3 YEARS
Strollo et al. NEJM 370; 2 1/9/2014

Woodson et al, Oto HNS epub before print 9/9/2014
Therapy effect on AHI and ODI at baseline, 12 months, randomized controlled therapy (RCT), and 18 months
(mean and standard error)aP < 0.05 vs baseline; bP < 0.05 vs 12 mo; cP < 0.05 vs RCT

Adverse adventsSerious device-related adverse events requiring repositioning:
• n = 2 (discomfort)
Serious non-related adverse events: n = 33• Most (88%) within 30 days of procedure• Sore throat from ETT, incisional pain, muscle soreness
Temporary tongue weakness: 18% of subjects• Resolved after 2 weeks in 100%
Other— most resolved with acclimation: • 40% with some discomfort with stimulation• 21% with tongue soreness
Strollo et al. NEJM 370; 2 1/9/2014
n = 126 total subjects

Tod C. Huntley, MD 5/9/2015

da Vinci® TORS BOT reduction

What the surgery entailsTransoral endoscopic resection of lingual tonsillar tissue w/ or w/o underlying muscle
Resection of 25-30 cc, up to 50 cc
May safely resect < 10 mm thickness within entire BOT limits w/o neurovascular risk
May resect additional 5 mm deep strip within 5 mm of midline if needed
Optional partial epiglottidectomy with mucosal resection in vallecula
Secondary intention healing pulls epiglottis forward, in attempt to tighten supraglottis
Based on tongue base TORS work done at UPenn

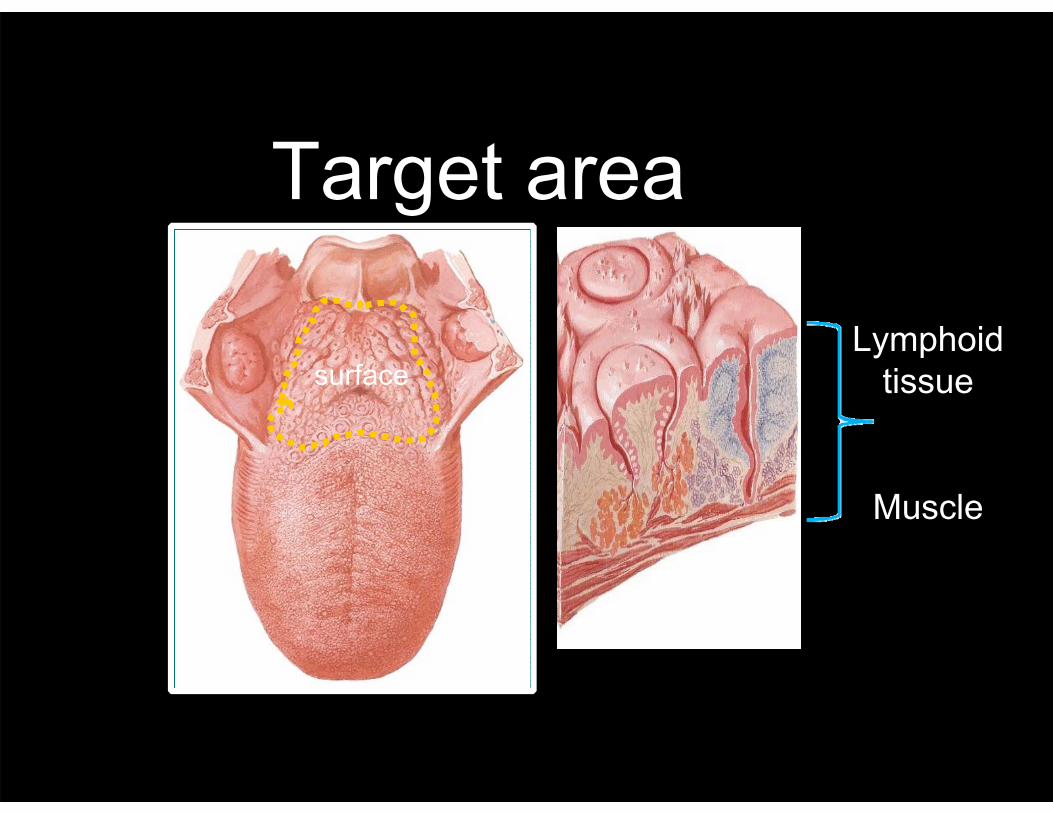
Target area
surfaceLymphoid
tissue
Muscle

Selection criteria“triple L”: low, localized, lymphatic
56

26
da Vinci® TORS BOT reduction

27
da Vinci® TORS BOT reduction
Related Documents











