COVID-19 and LTC July 15, 2021 Guidance and responses were provided based on information known on 7/15/2021 and may become out of date. Guidance is being updated rapidly, so users should look to CDC and NE DHHS guidance for updates.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
COVID-19 and LTCJuly 15, 2021
Guidance and responses were provided based on information known on 7/15/2021 and may become out of date. Guidance is being updated rapidly, so users should look
to CDC and NE DHHS guidance for updates.
Panelists today are:
Slides and a recording of this presentation will be available on the ICAP website:https://icap.nebraskamed.com/covid-19-webinars/
Use the Q&A box in the webinar platform to type a question. Questions will be read aloud by the moderator.If your question is not answered during the webinar, please either e-mail it to NE ICAP or call during our office hours to speak with one of our IPs.
Presentation Information:
Dr. Salman Ashraf [email protected]
Margaret Drake, MT(ASCP),CIC [email protected]
Lacey Pavlovsky, RN, MSN, CIC [email protected]
Rebecca Martinez, BSN, BA, RN, CIC [email protected]
Dan German [email protected]
Melody Malone, PT, CPHQ, MHA, CDP, CADDCT [email protected]
Debi Majo, BSN, RN [email protected]
Moderated by Marissa Chaney [email protected]
Additional Q&A Support:In attempt to answer even more questions, ICAP Infection Preventionists and guest panelists are standing by!
Some questions may be answered before the live discussion Q&A session!
Please review the "Answered" tab for already-answered questions.
We appreciate your understanding that all written answers provided during this webinar are based on information known on 7/01/2021 and may become out of date.
Please continue to review questions for upvoting.
Continuing Education Disclosures
▪1.0 Nursing Contact Hour and 1 NAB Contact Hour is awarded for the LIVE viewing of this webinar
▪In order to obtain nursing contact hours, you must be present for the entire live webinar and complete the post webinar survey
▪No conflicts of interest were identified for any member of the planning committee, presenters or panelists of the program content
▪This CE is hosted Nebraska Medicine along with Nebraska ICAP and Nebraska DHHS
▪ Nebraska Medicine is approved as a provider of nursing continuing professional development by the Midwest Multistate Division, an accredited approver by the American Nurses Credentialing Center’s (ANCC) Commission on Accreditation
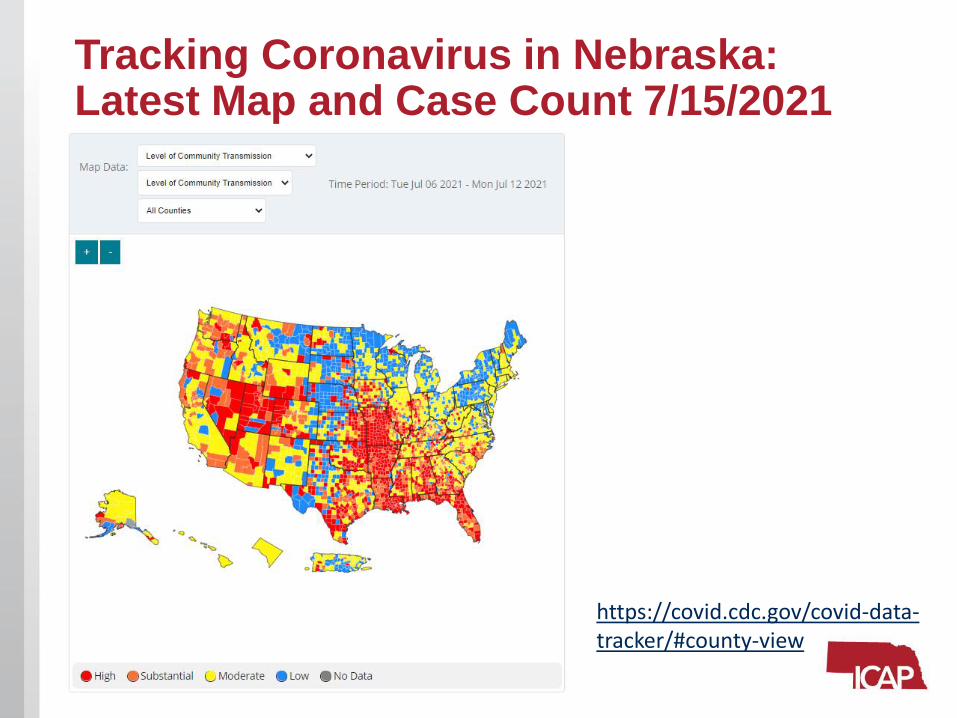
Tracking Coronavirus in Nebraska: Latest Map and Case Count 7/15/2021
https://covid.cdc.gov/covid-data-tracker/#county-view

Tracking Coronavirus in Nebraska: COVID-19 Integrated County View
https://covid.cdc.gov/covid-data-tracker/#county-view
7/1/2021 6/23/2021
7/8/20217/15/2021
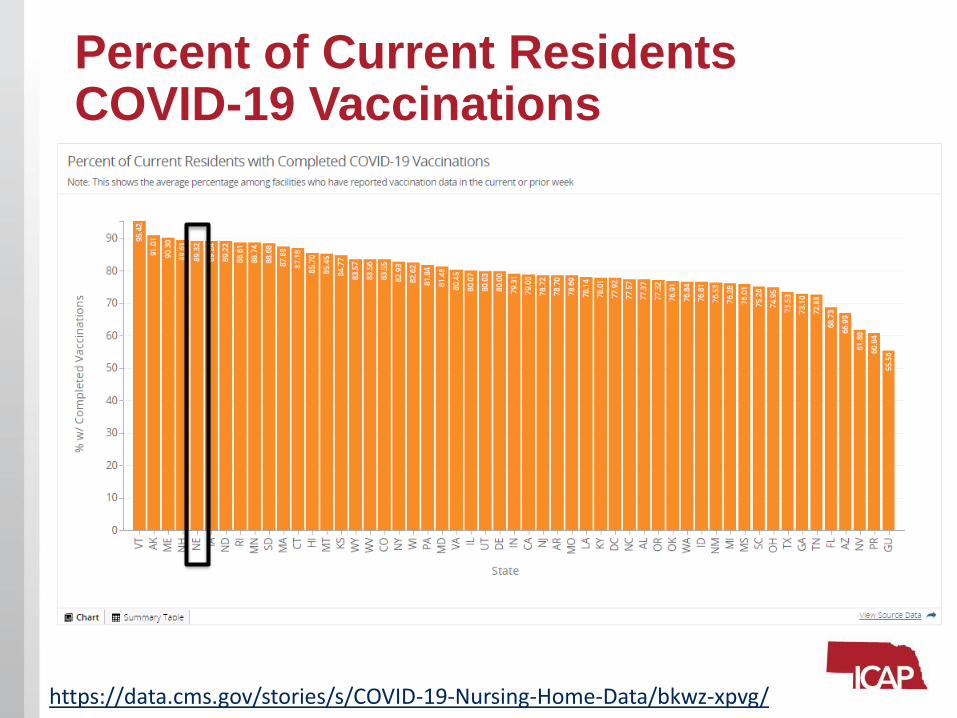
Percent of Current Residents COVID-19 Vaccinations
https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg/
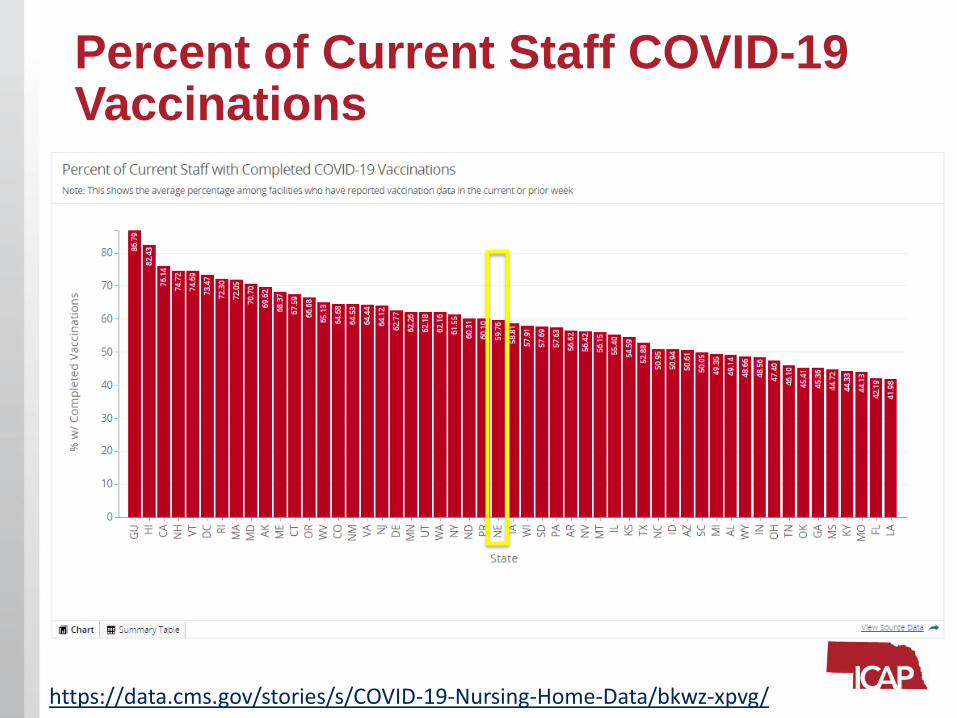
Percent of Current Staff COVID-19 Vaccinations
https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg/
Assisted-Living Facility Masking
Guidance Updated 7/14/2021
Update and Refresher on Monoclonal
Antibody TherapyAndrew B. Watkins, PharmD
Pharmacy Coordinator, Nebraska ASAP
Background/History• Monoclonal antibody (mAb) pilot project began 11/2020 with
bamlanivimab
• Doses specifically for use in LTCF patients (both SNF and ALF)
• Hybrid model with drug administered in the facilities or coordination with local hospitals
• Dedicated website created with informational materials and custom-built order form templates (https://asap.nebraskamed.com/monoclonal-antibody-project/)
• Request process established through a REDCap survey (https://redcap.nebraskamed.com/surveys/?s=74H88YD3RE)
• >500 doses administered statewide
• COVID-related hospitalization rate = 4.3%
• COVID-related mortality rate = 4.7%
mAb Updates• Due to increase in variants with decreased susceptibility to
bamlanivimab, we have switched to casirivimab-imdevimab (REGEN-COV)
• Expected to maintain activity against currently prevalent variants, including the Delta variant
• Clinical trials have shown ~70% relative reduction in COVID-related hospitalization and mortality
• Casirivimab-imdevimab is an IV infusion given peripherally over 30 minutes, with 1 hour of monitoring after the dose.
• It has been authorized for subcutaneous use, but this is not preferred at this time
• Our website remains updated with new casirivimab-imdevimab drug information, fact sheets, and order form templates (https://asap.nebraskamed.com/monoclonal-antibody-project/)
Eligibility Criteria• Positive COVID test (antigen or PCR)
• Mild to moderate symptoms (e.g., fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste/smell)
• No increased oxygen requirements
• Must be given within 10 days of symptom onset
• At least 1 high-risk condition:• Age ≥65 years
• BMI ≥25 kg/m2
• Diabetes
• Heart disease or high blood pressure
• Immunocompromising condition or medication
• Chronic respiratory disease
• Any other condition that a provider deems as high-risk
Request Process
• When patient becomes symptomatic, request mAb therapy using the below survey link
• https://redcap.nebraskamed.com/surveys/?s=74H88YD3RE
• Link can also be found at the top of the Nebraska ASAP mAbwebpage
• I will promptly reach out to confirm eligibility, coordinate logistics (drug delivery, administration, etc.), provide informational documents, and answer any questions.
• Do not hesitate to email [email protected] for any questions about mAbs or patient eligibility
Eye Protection Risk Assessment
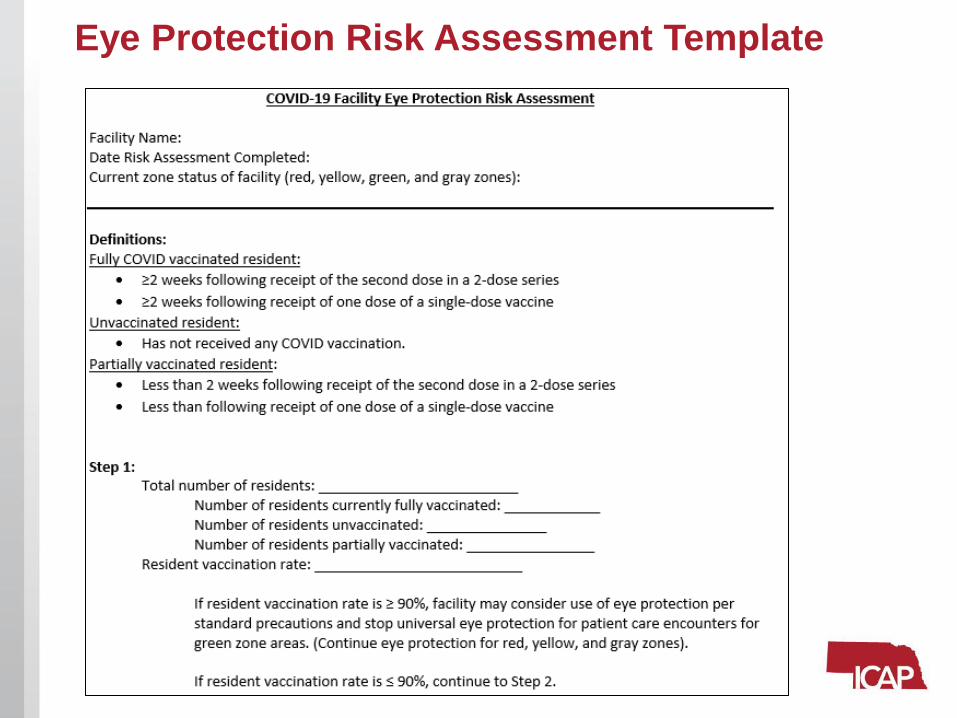
Eye Protection Risk Assessment Template
Eye Protection Risk Assessment Template
Eye Protection Risk Assessment Template available at https://icap.nebraskamed.com/wp-content/uploads/sites/2/2021/05/COVID-19-Eye-Protection-Risk-Assessment-Template.pdf
Community transmission rates can change regularly.ICAP Recommends checking the CDC COVID Data Tracker at least weekly.
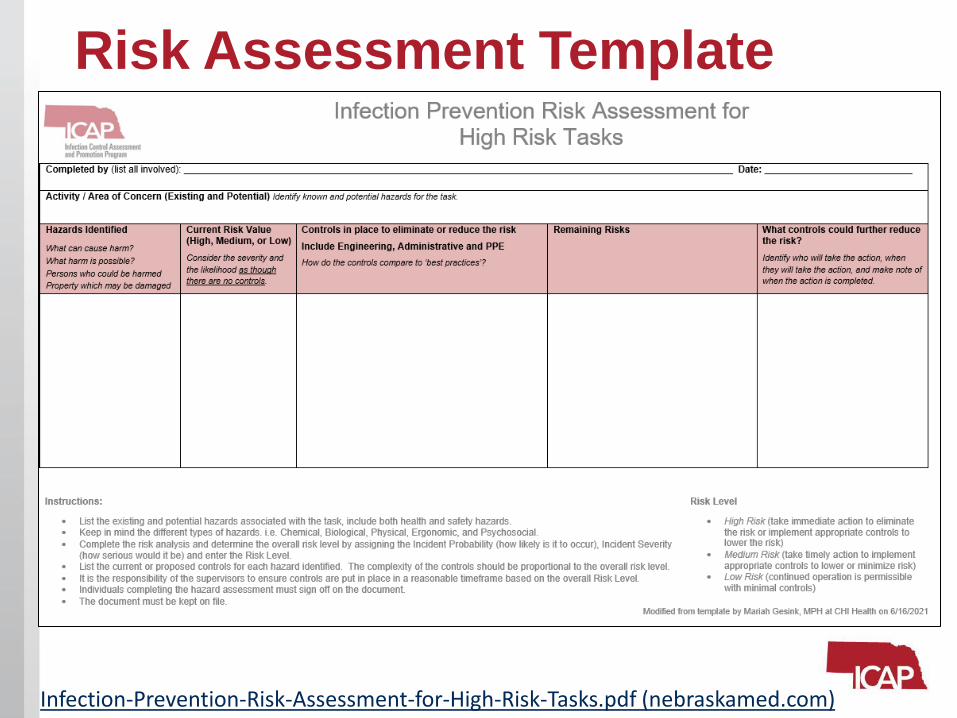
Risk Assessment Template
Infection-Prevention-Risk-Assessment-for-High-Risk-Tasks.pdf (nebraskamed.com)
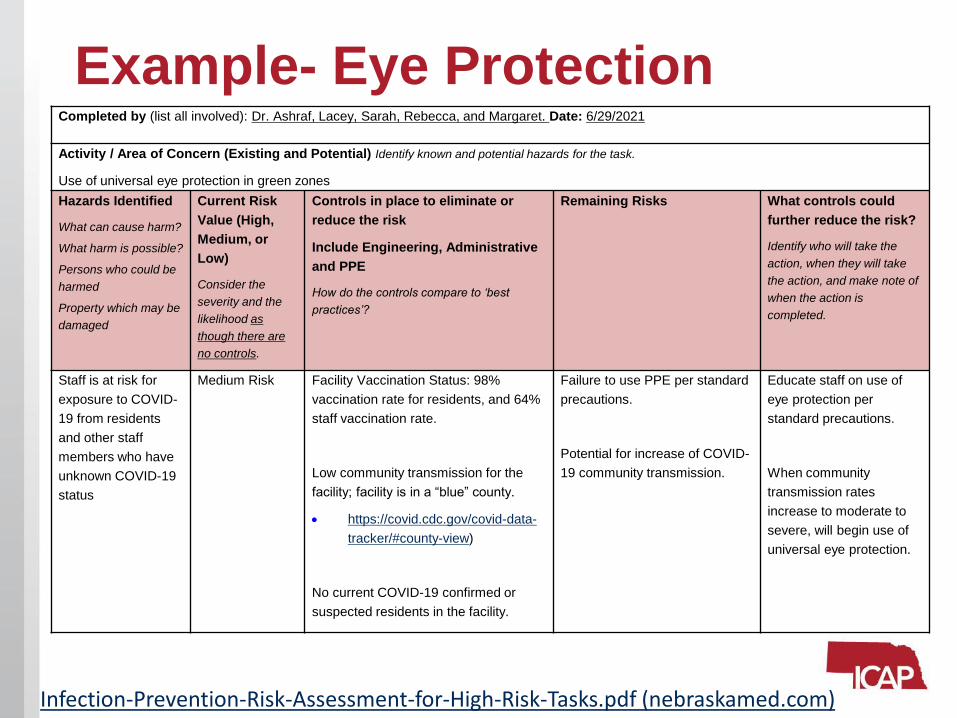
Example- Eye Protection
Infection-Prevention-Risk-Assessment-for-High-Risk-Tasks.pdf (nebraskamed.com)
Completed by (list all involved): Dr. Ashraf, Lacey, Sarah, Rebecca, and Margaret. Date: 6/29/2021
Activity / Area of Concern (Existing and Potential) Identify known and potential hazards for the task.
Use of universal eye protection in green zones
Hazards Identified
What can cause harm?
What harm is possible?
Persons who could be
harmed
Property which may be
damaged
Current Risk
Value (High,
Medium, or
Low)
Consider the
severity and the
likelihood as
though there are
no controls.
Controls in place to eliminate or
reduce the risk
Include Engineering, Administrative
and PPE
How do the controls compare to ‘best
practices’?
Remaining Risks What controls could
further reduce the risk?
Identify who will take the
action, when they will take
the action, and make note of
when the action is
completed.
Staff is at risk for
exposure to COVID-
19 from residents
and other staff
members who have
unknown COVID-19
status
Medium Risk Facility Vaccination Status: 98%
vaccination rate for residents, and 64%
staff vaccination rate.
Low community transmission for the
facility; facility is in a “blue” county.
• https://covid.cdc.gov/covid-data-
tracker/#county-view)
No current COVID-19 confirmed or
suspected residents in the facility.
Failure to use PPE per standard
precautions.
Potential for increase of COVID-
19 community transmission.
Educate staff on use of
eye protection per
standard precautions.
When community
transmission rates
increase to moderate to
severe, will begin use of
universal eye protection.
Actions needed to be taken upon identification
of a COVID-19 case at a facility
https://icap.nebraskamed.com/wp-content/uploads/sites/2/2021/07/Actions-needed-to-be-taken-
upon-identification-of-a-COVID-19-Case-7.14.2021.pdf
21
Notification
• Inform Local Health Department (LHD) of positive COVID-19 case
• Inform Licensure (LTC-CMS Survey team)
• Notify facility leadership and activate Incident Command System if it has not already been activated.
• Notify HCP, residents, and families per CMS QSO-20-29-NH (cms.gov) and OSHA requirements.
• Identify a point person (IP, DON, ADON etc.) who will subsequently get in touch with Nebraska ICAP.
– ICAP will assist long-term care (including skilled nursing and assisted living facilities) with implementation of infection prevention strategies and may advise on testing, isolation, staff cohorting, PPE use and other infection control related issues
Testing• Initiate outbreak testing per QSO-20-38-NH REVISED (cms.gov) for
any staff or resident positive.
• In general, outbreak testing involves testing all staff and residents (regardless of their vaccination status) in the building every 3 to 7 days until no cases are identified in the building for 14 days.
• Note: Once notified, ICAP team will be working with facilities to make sure that all their questions are being answered throughout the duration of the outbreak
• If facility is using antigen tests, then they will need to follow the testing algorithm from the CDC which describes in which situations a confirmatory PCR tests is needed.
• In general, symptomatic individuals who test negative on antigen test need a confirmatory PCR. Similarly, asymptomatic individuals who test positive on antigen test also need a confirmatory test
• The detailed guidance can be found here: Considerations for Interpretation of Antigen Tests in Long-Term Care Facilities (cdc.gov)
• Note: When there is a discrepancy between the antigen and PCR test results, ICAP can provide further assistance on interpretation of those test results, as needed)
If a Resident is identified to have COVID-19: Isolate the resident (either in a designated isolation area if already established or in the resident own room if no isolation area is yet established).
Information to collect on positive resident:
– Symptoms, vaccination status, previous history of COVID-19 infection, and If PCR has been done where was it sent for testing.
• If only POC testing was performed, another specimen for PCR testing may need to be collected.
• If mildly symptomatic, the positive resident may meet criteria for monoclonal antibody therapy.
• State or local health department may also need additional information such as full name, date of birth, dates of recent travels outside the facility (e.g., within last 14 days), dates and names of recent visitors (e.g., within last 14 days)
• Facility should also start looking into staff schedule to develop a list of staff who may have recently worked with the positive resident (e.g., within the last 14 days)
If a Resident is identified to have COVID-19: Perform contact tracing for the positive resident starting from 48 hours prior to positive test date/symptom-onset (whichever was first):
– Review the movements of the resident diagnosed with COVID-19 and determine potential exposures to staff and other residents.
• Also consider the type of care the positive resident have been receiving (e.g., nebulizers, multiple person assist, etc.) to determine further exposure to residents and staff members.
• High-risk areas to include in the review include communal dining, group activities, resident’s roommate, community outings, etc. The goal is to identify all the residents and staff who may be exposed in different areas of the building.
If a Staff Member is identified to have COVID-19: Make sure the positive staff member is not working and has been sent home.
– Review the Return-to-Work Criteria for Healthcare Workers | CDC
– Information to collect on positive staff member:
• Symptoms, vaccination status, previous history of COVID-19 infection, and if PCR has been done where was it sent for testing.
– If only POC testing was performed, another specimen for PCR testing may need to be collected.
– State or local health department may also need additional information such as full name, date of birth etc. so that they can pursue further public health investigations
Perform contact tracing for the positive staff member for 48 hours prior to positive date/symptom onset:
– Review assigned duties and interview staff member (who was identified with COVID-19) to determine exposure risk for other staff and residents.
• High-risk areas to include in review include the unit/work assignment, PPE use in the resident rooms/care areas such as universal masking/eye protection and use of PPE in nursing station/break rooms. The goal is to identify all the residents and staff who may be exposed in different areas of the building.

Exposure guidance for staff and residents:
Vaccination Status Exposure GuidanceUnvaccinated residents
and partially vaccinated
residents
Any exposure to a COVID+ individual should result in
placement into yellow zone precautions
Fully Vaccinated
residentsAny significant exposure (prolonged close contact) to an
individual with COVID-19 should result in placement into
yellow zone precautions.Unvaccinated and
partially vaccinated staff
members
Will need to quarantine following exposure unless there is a
staffing crisis in which case further risk assessments may be
needed before making final decision (Note: ICAP may be able
to help facilities with those assessments). Facilities can
determine healthcare worker exposure risk using the CDC
risk classification Table available at Interim U.S. Guidance for
Risk Assessment and Work Restrictions for Healthcare
Personnel with Potential Exposure to SARS-CoV-2 | CDC.Fully Vaccinated staff
members
Fully vaccinated staff members with higher-risk exposures
who are asymptomatic do not need to be restricted from
work for 14 days following their exposure.
Setting up Zones after Identification of a COVID-19 case in the facility:
When a resident case is identified then proceed with setting up a red zone.
– If a facility has a completely separate unit or a walled off area in the building with empty rooms, a COVID-unit/red zone can be established in that area. Always evaluate airflow in the area where a red zone is being set up.
– If the empty rooms are located in another unit which is not physically separated from the rest of the unit and sharing the same air space, DO NOT transfer the resident with COVID-19 in that unit without first checking with ICAP team. (Note: Transferring a positive or exposed resident from one unit to another unit may lead to further transmission of COVID-19 in the building.
– If a completely separate or walled off unit with all empty beds is not available, initiate isolation in a private room within the same unit where the case is identified (sometimes it can be the resident own room if it is a private room). Consider that private room as a red zone/red room. If the resident with COVID-19 has a roommate, quarantine the roommate by themselves and do not cohort them with anyone else.
Setting up Zones after Identification of a COVID-19 case in the facility:
Yellow zone set up depends on the nature of the exposures
– All unvaccinated residents who have some exposure to the individual with COVID-19 or those fully vaccinated residents who had significant exposures (prolonged close contact) will need to be quarantined in the yellow zone.
– In most cases, exposed residents own rooms will be considered a yellow zone/yellow rooms.
– In general, it is best to avoid moving residents from one unit to another unit during an outbreak, as much as possible. ICAP is available to assist facilities with safe movement, if a transfer from one unit to another unit is considered necessary.

TMF Health Quality Institute CMS Quality Improvement
OrganizationDebi Majo, BSN, RN
Quality Improvement Specialist
NHSN Release Coming Soon• Webinar Session held Monday, July 12, 2021 from
1:00 – 2:00 PM EST should be posted, soon.
• For NHSN change details, go to: https://tmfnetworks.org/Resources/Online-Forums/aft/372
31
Weekly NHSN COVID-19 Vaccination Data Module Alert• ‘COVID-19 Vaccination Summary Data Alerts’ will
appear on the NHSN homepage.
• Implemented to flag if vaccination rates are less than or equal to 10 percent for reporting weeks starting March 1, 2021 through the present.
32
CMS Targeted COVID-19 Training for Frontline Nursing Home Staff & Management Learning
• Available through the CMS Quality, Safety & Education Portal (QSEP).
• Can be completed on a cell phone
• Frontline nursing home staff modules:
Module 1: Hand Hygiene and PPE
Module 2: Screening and Surveillance
Module 3: Cleaning the Nursing Home
Module 4: Cohorting
Module 5: Caring for Residents with Dementia in a Pandemic
• 3 hours total training time
• Management staff modules:
Module 1: Hand Hygiene and PPE
Module 2: Screening and Surveillance
Module 3: Cleaning the Nursing Home
Module 4: Cohorting
Module 5: Caring for Residents with Dementia in a Pandemic
Module 6: Basic Infection Control
Module 7: Emergency Preparedness and Surge Capacity
Module 8: Addressing Emotional Health of Residents and Staff
Module 9: Telehealth for Nursing Homes
Module 10: Getting Your Vaccine Delivery System Ready
• 4 hours total training time
CMS Targeted COVID-19 Training for Frontline Nursing Home Staff & Management Learning• CMS says it’s not permitted to put their trainings in
Relias or any other training program.
• There is no way, that we are aware of, to get any of the CMS training that was completed in another platform recognized in the QSEP platform.
• Therefore, the staff will have to re-take the sessions for your facility to get a 100% complete in the CMS system.
• Remember to build in time for new staff to do the training. 34
NHSN RESOURCES• TMF NHSN resources: NHSN Resources
• CDC NHSN COVID19 Module: https://www.cdc.gov/nhsn/ltc/covid19/index.html
LTC ConnectJuly 22 - 1:30-2 p.m. CT
• Topic: Vaccine Hesitancy: Concerns with Fertility and Pregnancy
• Register: LTC Connect
• Speaker: Gloria Richard-Davis, MD, MBA, NCMP, FACOG, with the University of Arkansas Medical Sciences (UAMS).
36

Reach out to us at: [email protected]
to submit requests for assistance with
NHSN reporting problems or quality improvement
assistance.
ICAP Updates

COVID-19 Tele-ICAR Reviews
• ICAP is offering COVID-19 focused virtual ICAR reviews to LTC, outpatient and acute care facilities
• The review will assess the status of COVID-19 policies and procedures and offer a summary of recommendations from ICAP
• Home Health Agencies fall under the outpatient umbrella and ICAP has developed a HH focused review to support our HH partners
• Contact NE ICAP at 402.552.2881 to be connected with the IP responsible for the facility
NAB:
➢ Completion of survey is required.
➢ The survey must be specific to the individual obtaining credit. (i.e.: 2 people cannot be listed on the same survey)
➢ You must have a NAB membership
➢ Credit is retrieved by you
➢ Any issues or questions regarding your credit must be directed to NAB customer service.
➢ ICAP can verify survey completion and check the roster list
Nursing Contact Hours:
➢ Completion of survey is required.
➢ The survey must be specific to the individual obtaining credit. (i.e.: 2 people cannot be listed on the same survey)
➢ One certificate is issued monthly for all webinars attended
➢ Certificate comes directly from ICAP via email
➢ Certificate is mailed by/on the 15th of the next month
Contact Marissa with questions:[email protected]
Webinar CE Process
1 Nursing Contact Hour and 1 NAB Contact Hour is offered for attending this LIVE webinar
A separate survey must be completed for each attendee.
Infection Prevention and ControlHotline Number:
Call 402-552-2881Office Hours are Monday – Friday
8:00 AM - 4:00 PM Central Time
On-call hours are available for emergencies onlyWeekends and Holidays from 8:00 AM- 4:00 PM
**Please call the main hotline number only during on-call hours**

Questions and Answer Session
Use the QA box in the webinar platform to type a question. Questions will be read aloud by the moderator.
Panelists:
• Dr. Salman Ashraf
• Margaret Drake, MT(ASCP),CIC
• Lacey Pavlovsky, RN, MSN, CIC
• Rebecca Martinez, BSN, BA, RN, CIC
• Dan German• Melody Malone, PT, CPHQ, MHA• Debi Majo, BSN, RN
• Moderated by Marissa Chaney
• Supported by Margaret Deacy
• Slide support from Lacey Pavlovsky,
RN, MSN, CIC
https://icap.nebraskamed.com/resources/
Don’t forget to Like us on Facebook for important updates!
Related Documents











