Pmg. Nemo-Psychophannocol & Biol. Psychiat 1985, Vol. 9, pp. 349-359 0278-5846185 $0.00 + .50 Printed in Great Britain. Pergamon Press Ltd. CORTICOTROPIN RELEASING FACTOR: BASIC STUDIES AND CLINICAL APPLICATIONS GEORGE P. CHROUSOS' JOSEPH R. CALABRESE3, PETER AVGERI MITCHEL A. KLING3: DAVID RUBINOW3, EDWARD H. OS', OLDFIELD !! THOMAS SCHUERMEYERl, CHARLES H. KELLNER3, GORDON B. CUTLER'JR.1, D. LYNN LORIAUXl and PHILIP W. GOLD3 2Nati 'National Institute of Child Health and Human Development, nal Institute of Neurological and Communicative Disorders and Stroke, and s National Institute of Mental Health, National Institutes of Health, Bethesda, Maryland, U.S.A. (Final form, March 1985) Contents Abstract Introduction Subhuman primate studies Pharmacoloqical prooerties of CRF Pharmacokinetic properties of CRF Studies with CRF in man Pharmacological properties Pharmacokinetic properties Patient studies Conclusions Acknowledgments References 350 350 353 353 353 354 357 357 357 358 Abstract Chrousos, George P., Joseph R. Calabrese, Peter Avgerinos, Mitchel A. Kling, David Rubinow, Edward H. Oldfield, Thomas Schuermeyer, Charles H. Kellner, Gordon B. Cutler Jr., D. Lynn Loriaux and Philip W. Gold: Corticotropin releasing factor: Basic studies and clinical applications. Prog. Neuro-Psychopharmacol. & Biol. Psychiat. 1985, 2 (4): 349-359. 1. 2. 3. 4. Corticotropin releasing factor (CRFI is a newly sequenced peptide first isolated from sheep hypothalami and thought to be an important modulator of both the pituitary- adrenal axis and the sympathetic nervous system. We administered intravenous, intramuscular, and intracerebroventricular CRH to non- human primates and measured plasma ACTH, beta endorphin, cortisol, GH and PRL responses to CRF. In addition, we determined the pharmacokinetic properties of II25 in these primates. We administered CRF as an intravenous bolus or as a continuous infusion to normal vol- unteers and as an intravenous bolus to patients with disorders of the hypothalamic- pituitary-adrenal axis, such as Cushing's syndrome and adrenal insufficiency, and patients with endogenous depression and mild hypercortisolism, and assessed their plasma ACTH, cortisol, GH and PRL responses. In addition, we determined the pharmaco- kinetic properties of CRF in man by measuring CRF immunoreactivity in plasma. CRF given intravenously to primates or man is a slowly metabolized, long-acting, secre- tagogue of ACTH, beta-endorphin and cortisol. When given intracerebroventricularly to primates it stimulates the hypothalamic-pituitary-adrenal axis without escaping into the plasma and it is actively cleared in the CNS. It does not cross the blood brain barrier appreciably when given intravenously. CRF given to primates and men as an intravenous continuous infusion has only mild ACTH stimulating effects and this may be 349

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pmg. Nemo-Psychophannocol & Biol. Psychiat 1985, Vol. 9, pp. 349-359 0278-5846185 $0.00 + .50 Printed in Great Britain. Pergamon Press Ltd.
CORTICOTROPIN RELEASING FACTOR: BASIC STUDIES AND CLINICAL APPLICATIONS
GEORGE P. CHROUSOS' JOSEPH R. CALABRESE3, PETER AVGERI MITCHEL A. KLING3: DAVID RUBINOW3, EDWARD H.
OS', OLDFIELD !!
THOMAS SCHUERMEYERl, CHARLES H. KELLNER3, GORDON B. CUTLER'JR.1, D. LYNN LORIAUXl and PHILIP W. GOLD3
2Nati 'National Institute of Child Health and Human Development,
nal Institute of Neurological and Communicative Disorders and Stroke, and s National Institute of Mental Health, National Institutes of Health,
Bethesda, Maryland, U.S.A.
(Final form, March 1985)
Contents
Abstract Introduction Subhuman primate studies Pharmacoloqical prooerties of CRF Pharmacokinetic properties of CRF Studies with CRF in man Pharmacological properties Pharmacokinetic properties Patient studies Conclusions Acknowledgments References
350 350 353 353 353 354 357 357 357 358
Abstract
Chrousos, George P., Joseph R. Calabrese, Peter Avgerinos, Mitchel A. Kling, David Rubinow, Edward H. Oldfield, Thomas Schuermeyer, Charles H. Kellner, Gordon B. Cutler Jr., D. Lynn Loriaux and Philip W. Gold: Corticotropin releasing factor: Basic studies and clinical applications. Prog. Neuro-Psychopharmacol. & Biol. Psychiat. 1985, 2 (4): 349-359.
1.
2.
3.
4.
Corticotropin releasing factor (CRFI is a newly sequenced peptide first isolated from sheep hypothalami and thought to be an important modulator of both the pituitary- adrenal axis and the sympathetic nervous system. We administered intravenous, intramuscular, and intracerebroventricular CRH to non- human primates and measured plasma ACTH, beta endorphin, cortisol, GH and PRL responses to CRF. In addition, we determined the pharmacokinetic properties of II25 in these primates. We administered CRF as an intravenous bolus or as a continuous infusion to normal vol- unteers and as an intravenous bolus to patients with disorders of the hypothalamic- pituitary-adrenal axis, such as Cushing's syndrome and adrenal insufficiency, and patients with endogenous depression and mild hypercortisolism, and assessed their plasma ACTH, cortisol, GH and PRL responses. In addition, we determined the pharmaco- kinetic properties of CRF in man by measuring CRF immunoreactivity in plasma. CRF given intravenously to primates or man is a slowly metabolized, long-acting, secre- tagogue of ACTH, beta-endorphin and cortisol. When given intracerebroventricularly to primates it stimulates the hypothalamic-pituitary-adrenal axis without escaping into the plasma and it is actively cleared in the CNS. It does not cross the blood brain barrier appreciably when given intravenously. CRF given to primates and men as an intravenous continuous infusion has only mild ACTH stimulating effects and this may be
349
350 G. P. Chrousos et al.
due to an intact cortisol negative feedback system. Finally, CRF causes characteristic plasma hormone responses in patients with Gushing's disease, adrenal insufficiency and depression.
v adrenal insufficiency, cortocotropin releasing factor (CRF), Cushing's syndrome,
epression, hypothalamic-pituitary-adrenal axis (HPA-axis), primates.
Abbreviations: corticotropin (ACTH), corticotropin releasing factor (CRF), growth hormone (GHl growth hormone releasing hormone (GHRH), hypothalamic-pituitary-adrenal axis (HPA- axisi, intracerebroventricularly (i.c.v.1, intramuscularly (i.m.1, intravenously (i.v.1, prolactin (PRL).
1. Introduction
Corticotropin releasing factor (CRF) is a 41 amino acid peptide first isolated frun ovine hypothalami (Vale et al. 19811. Its existence has been postulated for years and it is in fact the first hypothalamic releasing factor for which there was convincing experimental evidence (Saffran and Schally, 1955). CRF is a trophic factor that stimulates the corti- cotroph cells of the anterior pituitary to synthesize and secrete ACTH, which, in turn, activates cortisol secretion from the adrenal zona fasciculata. Several recent discover- ies have expanded interest in the hypothalamic-pituitary adrenal axis and its regulation. First, it was shown that ACTH is secreted synchronously with beta-endorphin, an opioid pep- tide, and that both hormones are contained within a canmon precursor molecule, proopiomela- nocortin (POMC) (Mains et al. 1977). Second, a large subgroup of patients with depression, and some alcoholics, have a hyperactive pituitary adrenal axis (Carroll et al. 1976, Stokes 1973). The hypercortisolism seen in these conditions can be difficult to distinguish from Cushing's syndrome, and have been described as "pseudo-Cushing's" syndrome. Third, excit- ing new information suggests a broader role for CRF in coordinating many extrahypothalamic sites, including parts of the limbic system and the hindbrain (Bloan et al. 19R2, Olschowka et al. 19821. CRF neuron bodies and terminal fields have been found in close association with the central autonomic system and the locus coeruleus (Olschowka et al. 1982). Intra- ventricular (i.c.v.1 administration of CRF leads not only to activation of the HPA-axis but also to activation of the sympathetic nervous systm (Brown et al. 1982). Various behav- ioral changes are noted in rats that have received i.c.v. CRF (Sutton et al. 1982, Rritton et al. 19821. These behaviors, which include increased locomotor activity, changes in the feeding behavior, and assumption of the "freeze“ posture when placed in a foreign environment, are all similar to those occurring in stressed rats. This new information suggests a coordinating role of CRF during stress. Thus, CRF may mediate metabolic, circulatory and behavioral adaptations that are activated in "demanding" situations. In this paper, we will review data from our laboratory obtained from primates and man, on the pharmacokinetic properties of CRF when administered i.v., i.m., and i.c.v., and on its effects on anterior pituitary function.
2. Subhuman Primate Studies
2.1. Pharmacological Properties of CRF:
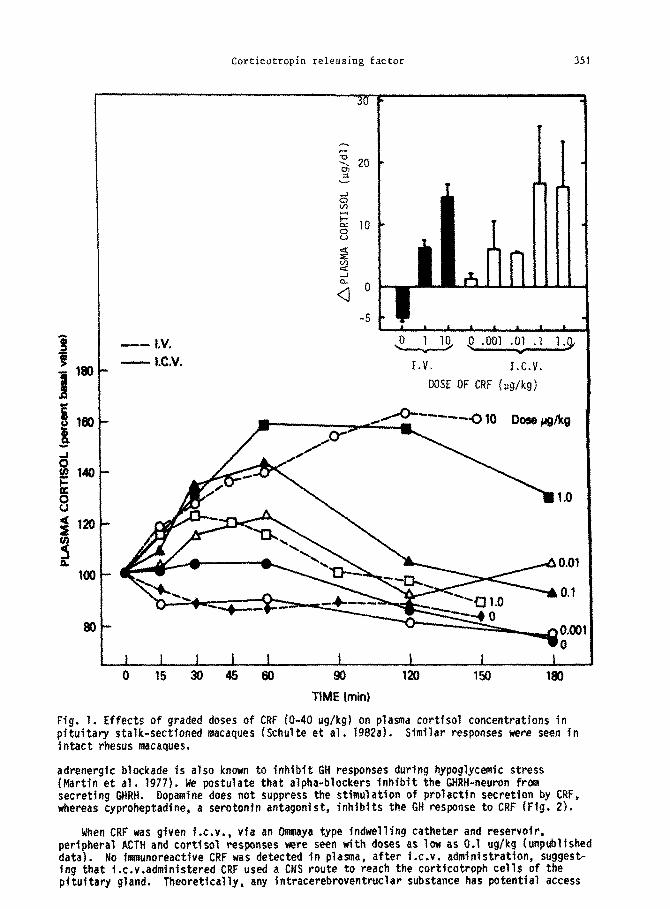
CRF given i.v. or i.m. to cynomolgus or rhesus macaques causes activation of the HPA- axis (Schulte et al. 1982a). The active doses are similar in magnitude to those of other hypothalamic releasing factors such as GnRH, TRH, or GHRH. Intramuscular injections to CRF also stimulate the HPA axis. As shown in Fig. 1, doses above 1 ug/kg are maximal.
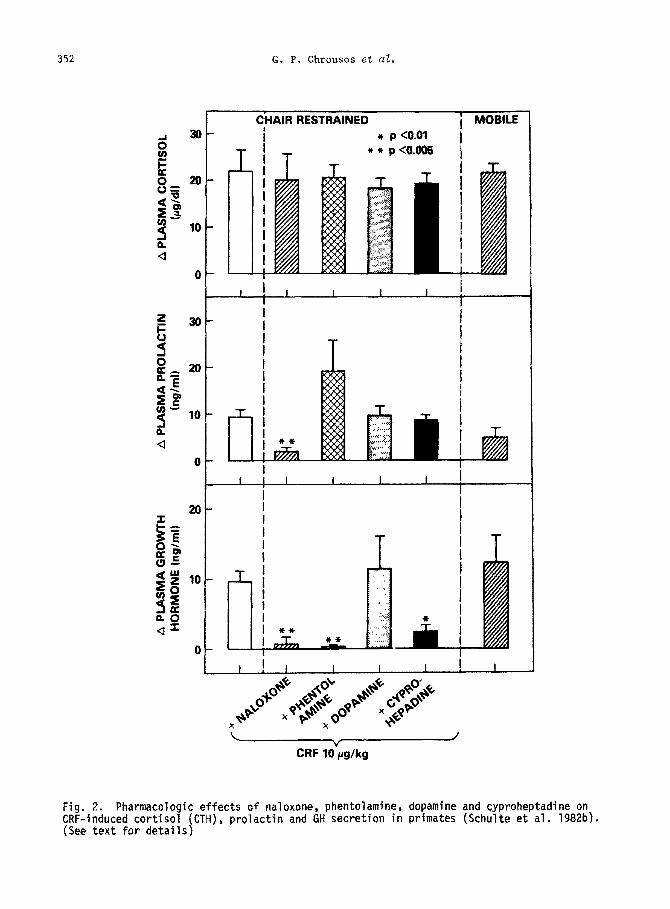
In addition to causing ACTH secretion, CRF also causes dose-dependent GH and PRL secre- tory responses. This is interesting because these two pituitary.hotmones are known to be secreted physiologically during stress along with ACTH (Noel et al. 1972). Opioids are known to stimulate GH and PRL secretion (Panerai et al. 1980). Pretreatment and simul- taneous treatment of the animals with naloxone inhibited both GH and PRL responses with- out affectinq the activitv of the HPA axis (Schulte et al. 1982bI (Fio. 2). This suqqests that beta-endorphin, which is secreted in response to CRF, may mediate the stimulation of these hormones. An alpha-adrenergic-blocker inhibits only the GH response (Fig. 21. Alpha-
Corticotropin releasing factor
‘ ‘ 1 * ’
p ,001 .Ol .7 l.cJ -w
I.V. I.C.V.
DOSE OF CRF lug/kg)
1 I 1 I I I I 1 I
0 I5 3045 60 90 120 150 180
TIME Iminj
Fig. 1. Effects of graded doses of CRF (O-40 ug/kg) on plasma cortfsol concentrations in pituitary stalk-sectioned macaques (Schulte et al. 1982a). Similar responses were seen in fntact rhesus macaques.
adrenergfc blockade is also known to inhibit GH responses during hypoglycemfc stress (Martin et al. 1977). Me postulate that alpha-blockers inhibit the GHRH-neuron from secreting GHRH. Dopamine does not suppress the stimulation of prolactfn secretion by CRF, whereas cyproheptadfne, a serotonfn antagonist, fnhibits the GH response to CRF (Fig. 2).
When CRF was given Ix.!!., via an Ommaya type fndwellfng catheter and reservoir, peripheral ACTH and cortisol responses were seen with doses as low as 0.1 ug/kg (unpublfshed data). No immunoreactfve CRF was detected in plasma, after f.c.v. administration, Suggest- ing that i.c.v.admfnfstered CRF used a CNS route to reach the cortfcatroph cells of the pituitary gland. Theoretically, any intracerebroventruclar substance has potential access
352 G. P. Chrousos s-t al.
CHAIR RESTRAINED
i
i MOBILE * p <O.Ol
T ! T *+ p<o.o06
CRF lO‘pg/kg
Fig. 2. Pharmacologic effects of naloxone, phentolamine, dopamine CRF-induced cortisol (CTH), prglactin and GH secretion in primates (See text for details)
and cyproheptadine on (Schulte et al. 1982b).
Corticotropin releasing factor 353
to any site within the brain, 1974).
including the hypothalamic pituitary portal system (Oldendorf, Centrally administered CRF also increased CSF ACTH concentrations. In contrast,
peripherally administered CRF had no effect on CSF ACTH. These preliminary findings sug- gest that CRF cannot cross the blood brain barrier, which was also suggested by pharmaco- kinetic data (vide infra), and that there may be a group of ACTH-secreting neurons which respond to cenmCRFnd secrete within the CNS.
At high intravenous doses (10 ug/kgl, CRF caused tachycardia in primates (Schulte et al. 1982cl. Although no drop in arterial blood pressure was seen, we postulate that the tachycardia was a compensatory mechanism for mesenteric vessel dilatation and sequestration of blood. In the dog, it has been shown that CRF and two homologous molecules, urotensin I and sauvagine, which were isolated from the fish and the frog, respectively, cause specific dilatation of the superior mesenteric vasculature (MacCannell et al. 1982).
Chronic treatment of primates with i.m. CRF (1 ug/kg/day) over a period of 3 months did not result in hypercortisolemia or hypercortisoluria. Basal and 2hr stimulated plasma cor- tisol concentrations were unaltered throughout this period. In addition, continuous i.v. infusion of CRF (10 ug/kd), for up to 2 weeks caused only small elevations of the morning plasma cortisol concentrations and 24hr urinary cortisol excretion (unpublished data). Thus, cortisol negative feedback may limit the pituitary response to chronic CRF administration, leading to only mild hypercortisolism.
2.2. Pharmacokinetic Properties of CRF:
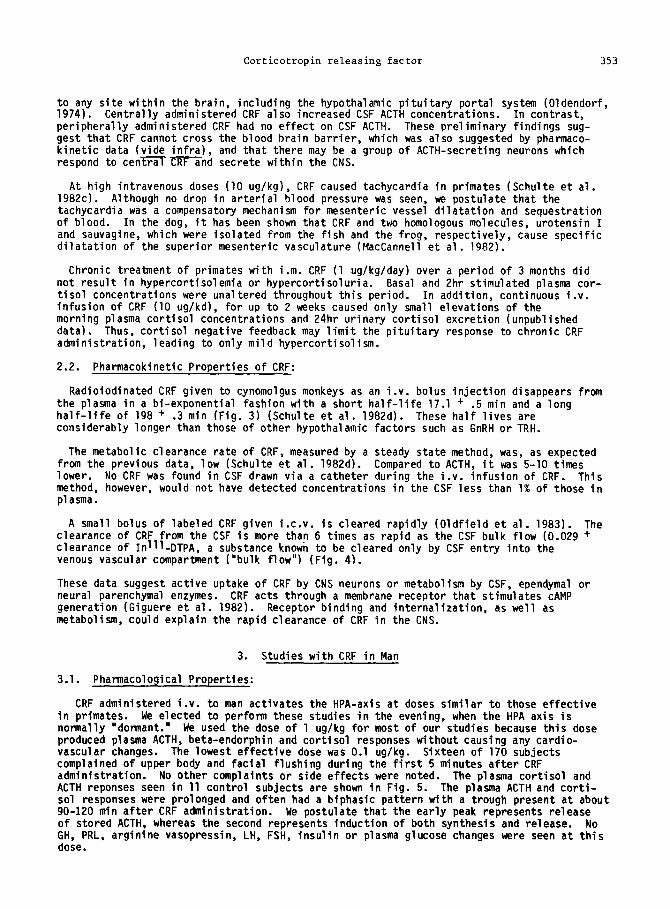
Radioiodinated CRF given to cynomolgus monkeys as an i.v. bolus injection disappears from the plasma in a bi-exponential fashion with a short half-life 17.1 + .5 min and a long half-life of 198 + .3 min (Fig. 31 (Schulte et al. 1982d). These half lives are considerably longer than those of other hypothalamic factors such as GnRH or TRH.
The metabolic clearance rate of CRF, measured by a steady state method, was, as expected from the previous data, low (Schulte et al. 1982d). Compared to ACTH, it was 5-10 times lower. No CRF was found in CSF drawn via a catheter during the i.v. infusion of CRF. This method, however, would not have detected concentrations in the CSF less than 1% of those in plasma.
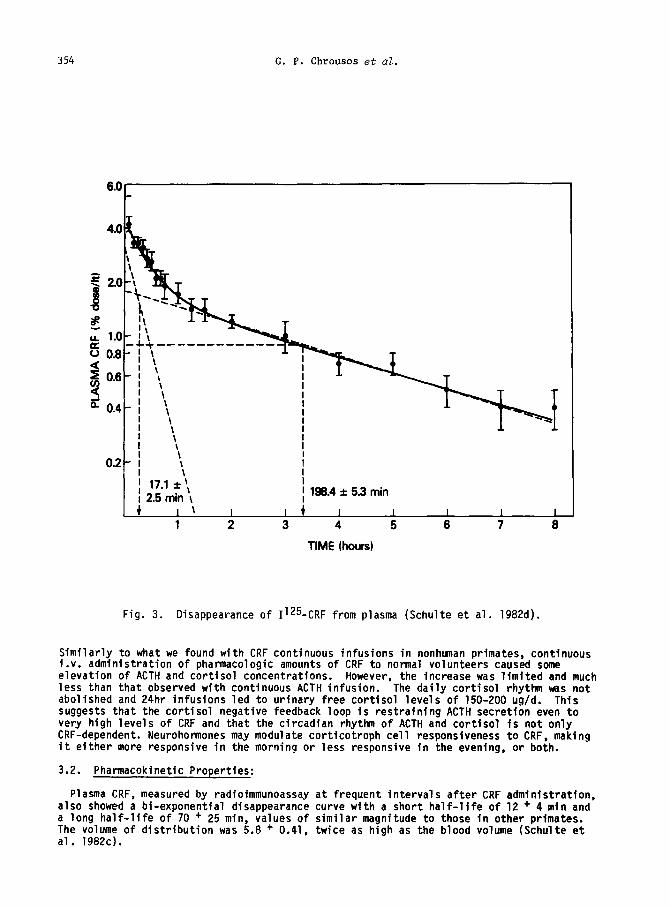
A small bolus of labeled CRF given i.c.v. is cleared rapidly (Oldfield et al. 19831. The clearance of CRF from the CSF is more than 6 times as rapid as the CSF bulk flow (0.029 + clearance of Inlll-DTPA, a substance known to be cleared only by CSF entry into the venous vascular compartment ("bulk flow") (Fig. 4).
These data suggest active uptake of CRF by CNS neurons or metabolism by CSF, ependymal or neural parenchymal enzymes. CRF acts through a membrane receptor that stimulates CAMP generation (Giguere et al. 19821. Receptor binding and internalization, as well as metabolism, could explain the rapid clearance of CRF in the CNS.
3. Studies with CRF in Man
3.1. Pharmacological Properties:
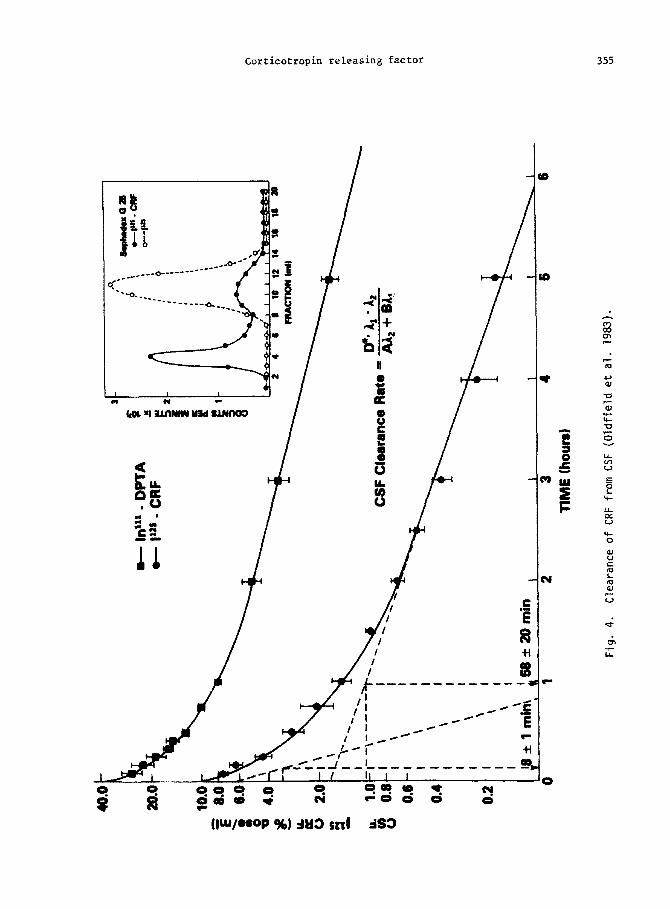
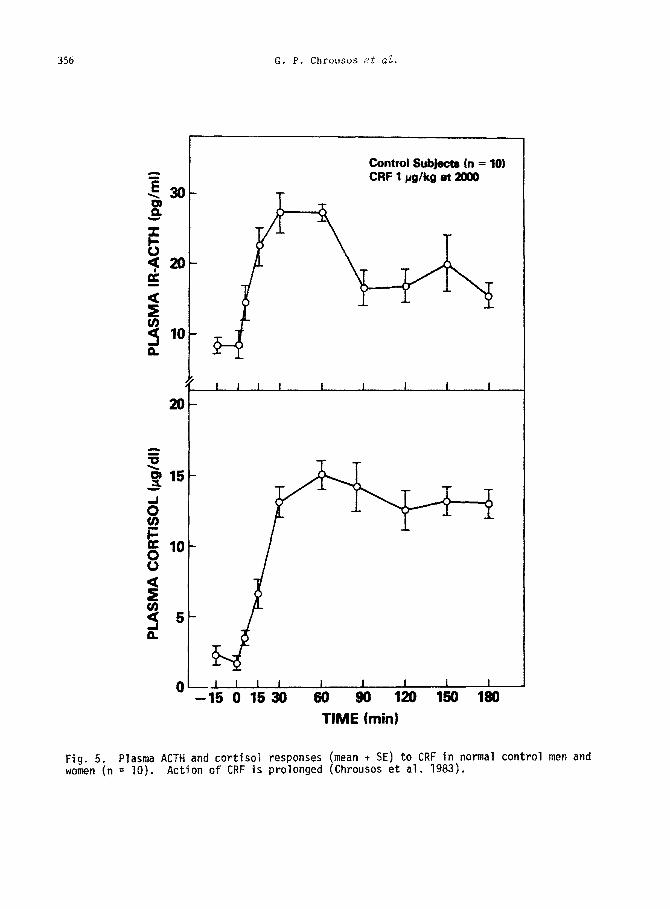
CRF administered i.v. to man activates the HPA-axis at doses similar to those effective in primates. We elected to perform these studies in the evening, when the HPA axis is normally "dormant." We used the dose of 1 ug/kg for most of our studies because this dose produced plasma ACTH, beta-endorphin and cortisol responses without causing any cardio- vascular changes. The lowest effective dose was 0.1 ug/kg. Sixteen of 170 subjects complained of upper body and facial flushing during the first 5 minutes after CRF administration. No other complaints or side effects were noted. The plasma cortisol and ACTH reponses seen in 11 control subjects are shown in Fig. 5. The plasma ACTH and corti- sol responses were prolonged and often had a biphasic pattern with a trough present at about 90-120 min after CRF administration. We postulate that the early peak represents release of stored ACTH, whereas the second represents induction of both synthesis and release. No GH, PRL, arginine vasopressin, LH, FSH, insulin or plasma glucose changes were seen at this dose.
354 G. P. Chrousos et al.
1 2 3 4 5 6 7 8
TIME hours)
Fig. 3. Disappearance of 1125 -CRF from plasma (Schulte et al. 1982d).
Similarly to what we found with CRF continuous infusions in nonhunan primates, continuous i.v. administration of pharmacologic amounts of CRF to normal volunteers caused some elevation of ACTH and cortisol concentrations. However, the increase was limited and much less than that observed with continuous ACTH infusion. The daily cortisol rhythm was not abolished and 24hr infusions led to urinary free cortisol levels of 150-200 ug/d. This suggests that the cortisol negative feedback loop is restraining ACTH secretion even to very high levels of CRF and that the circadian rhythm of ACTH and cortisol is not only CRF-dependent. Neurohonaones may modulate corticotroph cell responsiveness to CRF, making it either more responsive in the morning or less responsive in the evening, or both.
3.2. Pharmacokinetic Properties:
Plasma CRF, measured by radioimmunoassay also showed a bf-exponential disappearance a long half-life of 70 + 25 mfn, values of The volume of distribution was 5.8 + 0.41, al. 1982cl.
at frequent intervals after CRF administration, curve with a short half-life of 12 + 4 min and similar magnitude to those in other primates. twice as high as the blood volume (Schulte et
Corticotropin releasing factor 355
356 G. P. Chrousos et al.
Control Subjects (n = 10) CRF 1 pg/lcg at #)oo
I I I I I I I 1 1
25 0 15 30 60 90 120 150 180 TIME (min)
Fig. 5. Plasma ACTH and cortisol responses (mean t SE) to CRF in normal control men and women (n = 10). Action of CRF is prolonged (Chrousos et al. 1983).
Corticotropin releasing factor 357
Extrapolating these data to the lowest peripheral effective dose in man, which is 0.1 ug/kg, we believe that the minimum effective CRF concentration in plasma would be about 0.5 - 1 ug/ml. Since the cross-reactivity of our antisera for human or primate CRF is unknown, we have not been able to draw conclusions about endogenous circulating CRF in primates or man. However, we have attempted to measure CRF in sheep plasma and CSF. All plasma samples have had values below the detection limit of our assay (< 5 pg/mll. We have concluded that CRF concentrations in peripheral blood are very low and are probably too low to stimulate ACTH secretion. However, we found CRF immuoreactivity in the CSF of adrenalecromized sheep at concentrations similar to those of opioid peptides and ACTH (50 - 150 pg/ml).
3.3. Patient Studies:
CRF, given to subjects with abnormalities of the pituitary-adrenal axis such as Cushing's syndrome and adrenal insufficiency produces elevations of plasma ACTH and cortisol (Chrousos et al. 19831. In Cushing's disease a hyperresponse of both ACTH and cortisol usually occurred. Basal concentrations of both hormones were elevated due to loss of diurnal rhythm in this disorder. Transsphenoidal removal of an ACTH-secreting pituitary adenoma has led to normalization of the response in three patients. In adrenal insufficiency, the CRF test can readily differentiate between primary and secondary causes. Plasma/cortisol responses are diminished in both settings, whereas ACTH responses are increased in primary but decreased in secondary insufficiency. We have preliminary results that showed differences in the shape of the curves between secondary adrenal insufficiency due to pituitary gland damage and that observed in patients with hypothalamic lesions. In the latter a delayed and pro- longed ACTH response was seen reminiscent of TSH responses to TRH in hypothalamic hypothyroidism.
We also have administered CRF to several drug-free patients with depression. The ACTH responses appeared to be suppressed whereas cortisol responses were in the normal range. These patients did not have overt hypercortisoluria at the time of the study but their uri- nary free cortisol was at the upper or slightly above the upper limit of normal. These findings suggest that a normal cortisol negative feedback on the pituitary is operational in these patients and that their adrenal glands are slightly hypertrophied or hypersensitive to ACTH. CRF neuron hyperactivity in depression and a normal negative feedback could also explain why these patients rarely have urinary free cortisol levels < 200 ug/day. This is strengthened by the observation that continuous infusions of pharmacologic amounts of CRF in normal men never cause elevations of 24h urinary free cortisol above 200 ug/day. A notable difference between the responses of depressed subjects and normals was the presence of GH responses to CRF in the depressed but not in the control subjects. GH responses to CRF were also seen in the chair-restrained orimates. The common link between deoressed oatients and chaired primates may be priming of the GHRH neuron by increased alpha-adrenergic' stimulation common to both the depressed subjects and stressed, restrained primates. This concept was supported by the observation that alpha-adrenergic blockade abolished the GH response to CRF in primates.
4. Conclusions
Corticotropin releasing factor is a neuropeptide which is an important modulator of the pituitary-adrenal axis. Our data suggests that this peptide can be clinically useful in determining differential diagnosis of illnesses such as depression and Cushing's disease and in furthering our understanding of the pathophysiology of hypercortisolism seen in these disorders. Moreover, CRF, like many neuropeptides, is widely distributed in brain. This distribution provides the context for the observation that CRF influences the complex, interrelated behavioral and physiological events characteristic of stress. Hence, further study of CRF may help extend our understanding of the biological basis of certain psychiatric disturbances, particularly ones like depression which are characterized by sustained hypercortisolism.
Acknowledgments
The authors gratefully acknowledge the technical assistance provided by William Gallucci.
358 G. P. Chrousos et aZ.
References
BLOOM, R.E., BATTENBERG, E.L.F., RIVIER, J., and VALE, W. (1982) Corticotropin releasing factor (CRF): 43-48.
Immunoreactive neuronesand fiber in rat hypothalamus. Regl. Pept. Q:
BRITTON, D.R., KOOB, G.F., RIVIER, J., and VALE, W. (19821 Intraventricular corticotropin releasing factor enhances behavioral effects of novelty. Life Sci. 31: 363-367.
BROWN, M.R., FISHER, L.A., SPIESS, J., RIVIER, C., RIVIER, J., and VALC W. (1982) Corti- cotropin releasing factor: Actions on the sympathetic nervous system and metabolism. Endocrinology III: 928-931.
CARROLL, B.J., CURfIS, G.C., and MENDELS, J. (1976) Neuroendocrine regulation in depres- sion I. Limbic system - adrenocortical dysfunction. Arch. Gen. Psychiatry 33: 1039- 1058.
-
CHROUSOS, G.P., SCHULTE, H.M., OLDFIELD, E.H., CUTLER, G.B., Jr., GOLD, P.W., and LORIAUX, D.L. (1983) The effects of corticotropin releasing factor in man. American Federation of Clinical Research, Abstract.
GIGUERE, V., LARRE, F., COTE, J., COY, D.H., SUEIRAS-DIAZ, J., and SCHALLY, A.V. (1982) Stimulation of cyclic AMP accumulation and corticotropin release by synthetic ovine corticotropin-releasing factor in rat anterior pituitary cells: site of glucocorticoid action. Proc. Natl. Acad. Sci., USA 79: 3466-3469.
MACCANNELL, K.L., LEDERIS, K., HAMILTON;P.L., and RIVIER, J. (1982) Amunine (oCRF), urotensin I and sauvagine, three structurally related peptides, produce selective dila- tion of the mesenteric circulation. Pharmacology 25: 116-120.
MAINS, R., EIPPER, E., and LING, N. (1977) Common precursor to corticotropin and endor- phins. Proc. Natl. Acad. Sci., USA 74: 3014-3018.
MARTIN, J.B., REICHLIN, S., and BROWN,T.M. (1977) Clinical Neuroendocrinology, F.A. Davis Company, Philadelphia, p. 147-178.
NOEL, G.L., SUG, H.K., STONE, J.G., and FRANTZ, A.G. (19721 Human prolactin and growth hormone release during surgery and after conditions of stress. J. Clin. Endocrinol.
Metab. 35: 840-851. OLDENDORF,T.H. (1974) Blood-brain barrier permeability to drugs. Annu. Rev. Pharmacol.
Toxicol. 14: 239-248. OLDFIELD, Ex., CHROUSOS, G.P. SCHULTE, H.M., ROCK, J.P., POPLACK, D.G., O'NEILL, D.L.,
GOLD, P.W., CUTLER, G.B., Jr., KORNBLITH, P.L., and LORIAUX, D.L. (1983) Active clear- ance of corticotropin releasing factors from the cerebrospinal fluid. American Associa- tion of Neurological Surgeons, Abstract.
OLSCHOWKA, J.A., O'DONOHUE, T.L., MUELLER, G.P., and JACOBOWITZ, D.M. (19821 The distribution of corticotropin releasing factor-like immunoreactive neurons in rat brain. Neuroendocrinology 35: 305-308.
PANERAI, A.E., CASANmA, F., MARTINI, A., MANTEJARRA, P., and DI JUILIO, A.M. (1980) Opiates act centrally on GH and PRL release. Endocrinology 108: 2400-2402.
SAFFRAN, M., and SCHALLY, A.V. (1955) Release of corticotropifiy anterior pituitary tis- sue in vitro. Can. J. Biochem. Physiol. 31: 408-415. --
SCHULTE H.M. CHROUSOS, G.P., OLDFIELD, ET., GOLD P.W CUTLER, G.B., Jr., and LDRIAUX, D.L. 11982aj The effects of corticotropin releasfng f&Or on the anterior pituitary function of stalk-sectioned cynomolgus macaques: Dose response of cortical secretion. J. Clin. Endocrinol. Metab. 55: 810-812.
SCHULTE, H.M., CHROUSOS, G.P.,TOLD, P.W., OLDFIELD, E.H., HOBAN, M.C., CUTLER, G.B., Jr., and LORIAUX, D.L. (1982b) Corticotropin releasing factor (CRF): a common link between anterior pituitary and sympathetic responses to stress. Acta Endocrinol. !Suppl! (Copenhagen) 253: 32-33.
SCHULTE, H.M., mOUSOS, G.P., GOLD, P.W., OLDFIELD, E.H., CUTLER, G.B., Jr., and LORIAUX, D.L. (1982c) Corticotropin releasing factor elicits responses characteristic of stress reaction in primates. Society for Neuroscience, Abstract.
SCHULTE, H.M., CHROUSOS, G.P., GOLD, P.W., OLDFIELD, E.H., PHILLIPS, J.M., MUNSON, P.J., CUTLER, G.B., Jr., and LORIAUX, D.L. (1982dl Metabolic clearance rate and plasma half- life of radioiodinated corticotropin releasing factor in a primate. J. Clin. Endocrinol. Metab. 55: 1023-1025.
STOKES, P.r (1973) Adrenocortical activation in alcoholics during chronic drinking. Ann. NY Acad. Sci 215: 77-83. -
Corticotropin releasing factor 359
SUTTON, R.E., KOOB, G.F., LE MOAL, M., RIVIER, J., and VALE, W. (1982) Corticotropin releasing factor produces behavioral activation in rats. Nature 297: 331-333.
VALE, W., SPIESS, J., RIVIER, C., and RIVIER, J. (19811 Characterization of a 41-residue ovine hypothalamic peptide that stimulates secretion of corticotropin and beta-endorphin. Science 213: 1394-97. -
Inquiries and reprint requests should be addressed to: Dr. George P. Chrousos, NIH Bldg. 10, Room lOBO9 Developmental Endocrinology Branch National Institute of Child Health and Human Development Bethesda, MD 2205, USA
Related Documents











