Corrosive injury of esophagus Philip WY Chiu Associate Professor Department of Surgery Department of Surgery Prince of Wales Hospital Chinese University of Hong Kong

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Corrosive injury of esophagus
Philip WY ChiuAssociate Professor
Department of SurgeryDepartment of SurgeryPrince of Wales Hospital
Chinese University of Hong Kong
BackgroundBackground
• Relatively rareRelatively rare• Dire emergency for UGI• Corrosive:• Corrosive:
– Substance that causes destruction of or damage to living tissue on contactto living tissue on contact
• Prevalence– Varies geographicallyVaries geographically– Local domestic and industrial customs– Availability of substancey

Type of caustic related to injuryType of caustic related to injury
• Acid– Generally less severe injury– Coagulative necrosis– Coagulum lessen tissue penetration– Coagulum lessen tissue penetration
• Alkaline– Liquefactive necrosis– Sodium hydroxide (哥士的)
Very hazardous– Very hazardous– 30% causes full thickness necrosis
in animal model for a second exposureexposure

Early managementResuscitation
U i• Upper airway– Assessment of severity of damage
Secure the airway– Secure the airway• Fiberoptic intubation
• Tracheostomy
• ? Dilutioni d i i i i j– May induce vomiting – more extensive injury
– Rapid action of caustics – probably useless

Early managementhPathogenesis
• Animal studiesAnimal studies– Corrosive enter to stomach ‐> reflex pyloric spasm
Limit passage of corrosive to duodenum– Limit passage of corrosive to duodenum
– Regurgitation of corrosive against a closed cricopharyngeus ‐> damage to esophagus andcricopharyngeus ‐> damage to esophagus and stomach
– 3‐5 mins ‐> gastric atonia ‐> opening of pylorus3 5 mins > gastric atonia > opening of pylorus
Goldman et al Am J Gastro 1984
Early managementf fAssessment of extent of injury
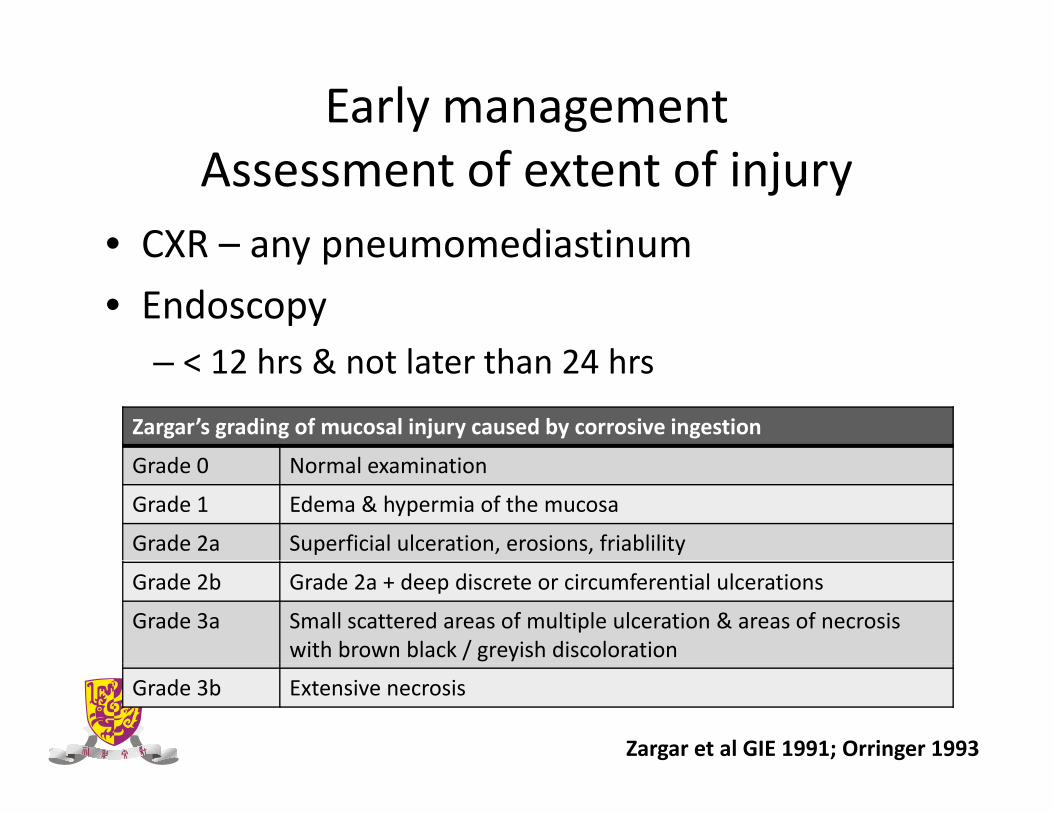
• CXR – any pneumomediastinumCXR any pneumomediastinum
• Endoscopy< 12 h & t l t th 24 h– < 12 hrs & not later than 24 hrs
Zargar’s grading of mucosal injury caused by corrosive ingestion
G d 0 N l i iGrade 0 Normal examination
Grade 1 Edema & hypermia of the mucosa
Grade 2a Superficial ulceration, erosions, friablility
Grade 2b Grade 2a + deep discrete or circumferential ulcerations
Grade 3a Small scattered areas of multiple ulceration & areas of necrosis with brown black / greyish discoloration
Grade 3b Extensive necrosis
Zargar et al GIE 1991; Orringer 1993

Endoscopic assessmentEndoscopic assessment

Endoscopic classificationlImplications
• Grade 1 – 2Grade 1 2– Conservative management– Insertion of feeding tubeg
• Grade 3bGrade 3b– Immediate Surgical Resection
• Problems– Difficult to differentiate between 2b and 3Difficult to differentiate between 2b and 3

Conservative managementf dUse of Steroid?
• AIM• AIM– Reduction of stricture formation
– 80% of grade 3 injuries developed stricture80% of grade 3 injuries developed stricture
– 67% of grade 2 injuries developed pyloric sternosis
• RCT• RCT– 18 yr prospective study in 60 children
– 10 / 31 steroid group developed stricture vs 11 / 29– 10 / 31 steroid group developed stricture vs 11 / 29 non‐steroid group
– No use in preventing stricturep g
Anderson et al. NEJM 1990

Conservative managementConservative management
• ICU care
• IV antibiotics
• IV PPI
• Nutritional support
• Close monitoring

Operative treatmentOperative treatment
• Indications– Full thickness injury of esophagus, stomach or duodenum
↑– Clinical deterioration with ↑sepsis
• Early Radical Surgery– 10 / 22 patients underwent esophagogastrectomy– 4 of 10 patients died (40%)– 7 of 12 conservative had stricture– Authors advocate early surgery
Olah et al Orv Hetil 1992
Approach to emergency resectionApproach to emergency resection
• Laparotomy + Transhiatal + Cervicalp y– Laparotomy first to assess the extent of disease in abdomen
– Transhiatal• Avoid opening the thorax• Risk of bleedingRisk of bleeding
• Laparotomy + Transthoracic + CervicalLaparotomy Transthoracic Cervical– Transthoracic
• Need to open thorax• Extent of injury within thorax can be assessed

Emergency EsophagectomyEmergency Esophagectomy
Author Journal / yr Number Method Survival
Gossot J Thorac Cardiovasc Surg1987
29 Transhiatal Stripping 62%
Brun BJS 1984 17 Transhiatal Stripping 76.5%
Hendrickx Acta Chir Belg 1990 1 Transhiatal Stripping 100%
Sarfati E BJS 1987 44 Transhiatal 45.5%
Pruvot Ann Chir 2003 28 Transhiatal Stripping / exclusion
82%exclusion
Dapril Surg Endosc 2007 1 Lap Transhiatal 100%

Next Step… ReconstructionNext Step… Reconstruction
• Colonic interpositionp– Left colon basing on left colic arteryRight colon– Right colon
• Blood supply• Distal ileum can be used to connect to esophagusconnect to esophagus
– Isoperistaltic
• Route– Presternal
l– Retrosternal
Related Documents