1 Correlation Between Signal-Averaged Electrocardiogram and the Histologic Evaluation of the Myocardial Substrate in Right Ventricular Outflow Tract Arrhythmias Running title: Santangeli et al.; SAECG and the diagnosis of RVOT arrhythmias substrate Pasquale Santangeli, MD 1 ; Maurizio Pieroni, MD, PhD 4,6 ; Antonio Dello Russo, MD, PhD 5 ; Michela Casella, MD, PhD 5 ; Gemma Pelargonio, MD; PhD 4 ; Luigi Di Biase, MD, PhD, FHRS 1,2,3 ; Andrea Macchione, MD 1 ; J. David Burkhardt, MD, FACC, FHRS 1 ; Fulvio Bellocci, MD 4 ;Pietro Santarelli, MD 4 ; Claudio Tondo, MD, PhD 5 ; Andrea Natale, MD, FACC, FHRS, FESC 1,2 1 Texas Cardiac Arrhythmia Institute, St. David’s Medical Center, Austin, TX; 2 Dept of Biomedical Engineering, University of Texas, Austin, TX; 3 Dept of Cardiology, University of Foggia, Foggia; 4 Catholic University of the Sacred Heart, Rome; 5 Cardiac Arrhythmia Research Centre, Centro Cardiologico Monzino, Milan; 6 Department of Cardiovascular Diseases, San Donato Hospital, Arezzo, Italy Corresponding author: Andrea Natale, MD, FACC, FHRS, FESC Executive Med Director, TX Cardiac Arrhythmia Inst at St. David’s Medical Ctr, Austin, TX, Consulting Prof, Division of Cardio, Stanford Univ, Palo Alto, CA, Clinical Assoc Prof of Med, Case Western Reserve Univ, Cleveland, OH, Director, Interventional Electrophysiology, Scripps Clinic, San Diego, Sr Clinical Director, EP Services, CA Pacific Med Ctr, San Francisco, CA 3000 N. I-35, Suite 720; Austin, TX 78705 Tel: +15215448186 Fax: +15125448184 E-mail: [email protected] Journal Subject Codes: [5] Arrhythmias, clinical electrophysiology, drugs; [171] Electrocardiology. M M M M M M MD D D D D D D 4 ;P ;P ;P ;P ;P ;P ;Pie ie ie ie ie ie etr tr tr tr tr tr tro o o o o o o Sa Sa Sa Sa Sa Sa Sant nt nt nt nt nt nt ACC, C, F F F F F F FHR HR HR HR HR HR HRS, S, S, S, S, S, S, F F F F F F FE E E E ES E E Arrhythmia Institute, St. David’s Medical Center, Austin, T e y a y a r Donato Hospital Arezzo Italy Arrhythmia Institute, St. David’s Medical Center, Austin, T eering, Univer sity of Texas, Austin, TX; 3 Dept of Cardiology atholic University of the Sacred Heart, Rome; 5 Cardiac Arrhy ardiologico Monzino, Milan; 6 Department of Cardiova scular Donato Hospital Arezzo Italy by guest on May 7, 2018 http://circep.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Correlation Between Signal-Averaged Electrocardiogram and the
Histologic Evaluation of the Myocardial Substrate in Right
Ventricular Outflow Tract Arrhythmias
Running title: Santangeli et al.; SAECG and the diagnosis of RVOT arrhythmias substrate
Pasquale Santangeli, MD1; Maurizio Pieroni, MD, PhD4,6; Antonio Dello Russo, MD, PhD5;
Michela Casella, MD, PhD5; Gemma Pelargonio, MD; PhD4;
Luigi Di Biase, MD, PhD, FHRS1,2,3; Andrea Macchione, MD1;
J. David Burkhardt, MD, FACC, FHRS1; Fulvio Bellocci, MD4;Pietro Santarelli, MD4;
Claudio Tondo, MD, PhD5; Andrea Natale, MD, FACC, FHRS, FESC1,2
1Texas Cardiac Arrhythmia Institute, St. David’s Medical Center, Austin, TX; 2Dept of Biomedical Engineering, University of Texas, Austin, TX; 3Dept of Cardiology, University of
Foggia, Foggia; 4Catholic University of the Sacred Heart, Rome; 5Cardiac Arrhythmia Research Centre, Centro Cardiologico Monzino, Milan; 6Department of Cardiovascular Diseases, San
Donato Hospital, Arezzo, Italy
Corresponding author:
Andrea Natale, MD, FACC, FHRS, FESC
Executive Med Director, TX Cardiac Arrhythmia Inst at St. David’s Medical Ctr, Austin, TX,
Consulting Prof, Division of Cardio, Stanford Univ, Palo Alto, CA, Clinical Assoc Prof of Med,
Case Western Reserve Univ, Cleveland, OH, Director, Interventional Electrophysiology, Scripps
Clinic, San Diego, Sr Clinical Director, EP Services, CA Pacific Med Ctr, San Francisco, CA
3000 N. I-35, Suite 720; Austin, TX 78705
Tel: +15215448186
Fax: +15125448184
E-mail: [email protected]
Journal Subject Codes: [5] Arrhythmias, clinical electrophysiology, drugs; [171] Electrocardiology.
MMMMMMMDDDDDDD4;P;P;P;P;P;P;Pieieieieieieetrtrtrtrtrtrtro o o o o o o SaSaSaSaSaSaSantntntntntntnt
ACC,C,,,,,, F F F F F F FHRHRHRHRHRHRHRS,S,S,S,S,S,S, F F F F F FFEEEEESEE
Arrhythmia Institute, St. David’s Medical Center, Austin, Te ya ya r
Donato Hospital Arezzo Italy
Arrhythmia Institute, St. David’s Medical Center, Austin, Teering, University of Texas, Austin, TX; 3Dept of Cardiologyatholic University of the Sacred Heart, Rome; 5Cardiac Arrhyardiologico Monzino, Milan; 6Department of Cardiovascular
Donato Hospital Arezzo Italy by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

2
Abstract:
Background - The differential diagnosis between idiopathic and cardiomyopathy-related right
ventricular outflow tract (RVOT) ventricular arrhythmias (VAs) is crucial. Signal-averaged
electrocardiogram (SAECG) abnormalities are frequent in cardiomyopathy-related RVOT-VAs,
although their pathophysiologic basis and diagnostic value in this setting are undefined. We
tested the association between SAECG and the myocardial substrate underlying RVOT-VAs.
Methods and Results - 24 consecutive patients (median age 50 [42-59] years, 12 men) with
RVOT-VAs (10 with frequent [>1,000/24h] PVCs, 14 with VTs) underwent SAECG with 40 Hz
filtering and electroanatomic mapping (EAM) with EAM-guided biopsy for characterization of
the RVOT-VAs substrate. A filtered averaged QRS (fQRS) was obtained and analyzed for fQRS
duration, low amplitude signal duration below 40 mV (LAS40) and root mean square voltage in
last 40 ms of the QRS (RMS40). Standard definition of EAM scar was used. EAM-guided
biopsy diagnosed ARVC in 11 (46%), myocarditis in 8 (33%), and idiopathic RVOT-VAs in 5
(21%) patients. Patients with cardiomyopathy-related RVOT-VAs had 1 EAM scar (median 2
[1-2], all with RVOT scar). EAM of patients with idiopathic RVOT-VAs was normal. Patients
with cardiomyopathy-related RVOT-VAs had significantly longer fQRS (106 [92-132] ms vs. 83
[82-84] ms, P = 0.01) and LAS40 (39 [36-51] ms vs. 19 [18-21] ms, P = 0.02), and lower
RMS40 (18 [9-26] V vs. 33 [32-33] V, P = 0.04). A significant linear correlation was found
between the extension (cm2) of the RVOT scar and all three SAECG parameters (rs = 0.76, P <
0.001 for the fQRSd; rs = 0.73, P < 0.001 for the LAS40; and rs = -0.72, P < 0.001 for the
RMS40). Using the established 2 of 3 criteria (i.e., late potentials) SAECG diagnosed
cardiomyopathy-related RVOT-VAs with high positive (100%) but low negative (38%)
predictive values, and missed 7/9 (78%) patients with RVOT scar <8 cm2.
Conclusions - In patients with RVOT-VAs, abnormal SAECG parameters reflect the presence of
extensive cardiomyopathic involvement of the RVOT. However, a negative SAECG does not
reliably rule out cardiomyopathy-related RVOT-VAs in the presence of a small RVOT scar.
Key words: right ventricular outflow tract tachycardia, signal-averaged electrocardiogram, three dimensional electroanatomic mapping.
arararararrar w w w w w w wasasasasasasas u u uuuuusesesesesesesed.d.ddddd EEEEEEEAAAAAAA
nd iididididididid opopopopopopopatatatatatatathihihihihihihic c cc c cc RRRRRVRVR
e
T o
y
1 a
ents with cardiomyopathy-related RVOT-VAs had 1 EAM
T scar). EAM of patients with idiopathic RVOT-VAs was no
y-related RVOT-VAs had significantly longer fQRS (106 [9
1) and LAS40 (39 [36-51] ms vs. 19 [18-21] ms, P = 0.02), a
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from
3
Introduction
Right ventricular outflow tract ventricular arrhythmias (RVOT-VAs) are the most common
variant of nonischemic VAs.1, 2 The majority of RVOT-VAs has an idiopathic origin with a
benign clinical course;2 however, they may also represent an early manifestation of potentially
life-threatening structural heart diseases, such as myocarditis or arrhythmogenic right ventricular
cardiomyopathy (ARVC).3 Accordingly, syncope and sudden cardiac death have been reported
in patients presenting with RVOT-VAs and an apparently normal heart.4-6 An accurate
distinction between idiopathic and cardiomyopathy-related RVOT-VAs carries important clinical
and prognostic implication. Unfortunately, such distinction is often challenging especially in
early and segmental forms of ARVC, or in focal myocarditis, which may selectively affect the
RVOT without other evidence of RV involvement. The signal-averaged electrocardiogram
(SAECG) is a quick and inexpensive test to disclose areas of slow and fragmented conduction in
the RV associated with underlying cardiomyopathic substrates.7
Accordingly, SAECG abnormalities (i.e., late potentials) are frequently encountered in
patients with cardiomyopathy-related RVOT-VAs.7-9 However, the pathophysiologic
significance and diagnostic reliability of SAECG abnormalities in the setting of cardiomyopathy-
related RVOT-VAs are still undefined.
Recent studies have shown that three-dimensional electroanatomic voltage mapping
(EAM) with EAM-guided endomyocardial biopsy allow to reliably localize and quantify affected
RV segments in patients with different variants of cardiomyopathy-related VAs.10
The aim of this study was to establish the value of the SAECG in the differential
diagnosis between idiopathic and cardiomyopathy-related RVOT-VAs, by testing the association
Between SAECG abnormalities and the RVOT histologic substrate identified through EAM with
en challengingngngngngngng e
hichh mmmmmmmayayayayayayay s s s s ss selelelelelelelecececececececttitit v
r
e
w
r evidence of RV involvement. The signal-averaged electroc
and inexpensive test to disclose areas of slow and fragmente
with underlying cardiomyopathic substrates.7
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

4
EAM-guided biopsy in a series of patients with RVOT-VAs.
Methods
We studied 24 patients (median age 50 [42-59] years, 12 males) with RVOT-VAs according to
standard 12-lead ECG criteria.11 All patients underwent a complete cardiovascular examination
including history, physical examination, 24-h Holter monitoring, SAECG, two-dimensional
echocardiography, and gadolinium contrast-enhanced cardiac magnetic resonance (CMR) (not
performed in 2 patients due to claustrophobia).
Diagnosis of ARVC was established according to current diagnostic criteria defined by
the European Society of Cardiology and International Society and Federation of Cardiology Task
Force.12 Diagnosis of myocarditis was established according to standardized histologic and
immunohistochemistry criteria (see below).
A structurally normal heart (i.e., idiopathic RVOT-VAs) was defined on the basis of
normal resting ECG, normal dimension and function (global and regional) of the left ventricular
(LV) and RV chambers as determined by echocardiography and CMR, absence of late
gadolinium enhancement on CMR, and normal EAM and EAM-guided biopsy.
Patients were excluded from this study if: they had atrial fibrillation or pacemaker rhythm
at the time of SAECG; they needed antiarrhythmic therapy at the time of SAECG and EAM; the
noise level of the SAECG was 0.5 mV.
Signal-averaged electrocardiogram
The SAECG was obtained with an Arrhythmia Research Technology-101 or 1200 System, with
bidirectional Butterworth filtering (40 to 250 Hz), as previously described.13 The following
quantitative SAECG variables of the filtered QRS were evaluated: 1) total duration (fQRSd), 2)
diagnostic crritititititititee
d FFededededededederererererereratatatatattatioioioioioioion n n n n nn ooooofofo
o t
t
y
of myocarditis was established according to standardized hist
try criteria (see below).
y normal heart (i.e., idiopathic RVOT-VAs) was defined on
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

5
duration of the low-amplitude signals (<40 mV) in the terminal portion (LAS40), and 3) root-
mean-square voltage of the last 40 ms (RMS40). Between 300 and 500 QRS complexes were
averaged for each recording to reach a noise level <0.5 mV. Ventricular late potentials were
considered positive when 2 of the following criteria were fulfilled:7, 14, 15 1) fQRSd >114 ms, 2)
LAS40 >38 ms, and 3) RMS40 <20 V.
Cardiac magnetic resonance
Cardiac magnetic resonance was performed with a 1.5-T Signa Excite 2 scanner (General
Electric Medical Systems, Milwaukee, Wisconsin) using a cardiac 8-channel phased-array coil,
with vector ECG gating at end-expiration. Morphological evaluation of the cardiac chambers and
presence of intra-myocardial fatty infiltration were obtained by black-blood double- and triple-
inversion recovery fast spin-echo sequences (repetition time 2 RR intervals, echo time 34 ms,
slice thickness 8 mm, image matrix 256 to 256, and field of view 30 to 36 cm) along axial, short-
axis, and horizontal long-axis planes. Functional assessment was carried out using bright-blood
high-resolution steady-state free precession sequence (repetition time 3.4 ms, echo time 1.5 ms,
flip angle 50°, image matrix 224 to 288, field of view 30 to 36 cm) in axial, vertical long-axis,
horizontal long-axis, and short-axis stack. Finally, late gadolinium enhancement images were
acquired using an inversion recovery prepared breath-hold gradient-echo sequence obtained 20
min after intravenous administration of 0.2 mmol/kg gadodiamide (Omniscan, Amersham
Health, Princeton, New Jersey). Late gadolinium enhancement was reported when it was
detected in more than one imaging plane, using cross-plane localizers to confirm the position.
Post-processing was performed on an Advantage Windows Workstation using MASS
software (Medis, Leiden, the Netherlands). This software was used to view images using
standardized window width and level settings. The same software was also used for
tion of the cararrrrrrddiddddd
blackkkkkkk-b-b-b-b-b-b-blololololololoododododododod d ddddddouououououoo b
fa o
m l
long-axis planes. Functional assessment was carried out usin
fast spin-echo sequences (repetition time 2 RR intervals, echo
m, image matrix 256 to 256, and field of view 30 to 36 cm) al
long-axis planes. Functional assessment was carried out usin
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from
6
measurement of RV end-diastolic and end-systolic diameter. Cardiac magnetic resonance
analysis was performed by an expert radiologist with Society of Cardiovascular Magnetic
Resonance level-3 experience, who was blinded to the clinical, SAECG, and endomyocardial
biopsy data.
Invasive study
All patients were submitted to coronary and left and right ventricular angiography (right and left
anterior oblique views), three-dimensional EAM, and EAM-guided endomyocardial biopsy. In
particular RV angiography was performed before EAM to provide RV silhouette in two views,
thus improving the anatomical accuracy of EAM. On the basis of EAM, endomyocardial
biopsies were withdrawn from areas presenting electrical abnormalities, as previously shown.10
Three-dimensional electroanatomic mapping
All patients underwent high-density RV three-dimensional electroanatomic voltage mapping
with the CARTOTM system (Biosense-Webster, Diamond Bar, CA). Mapping points were
sampled with a 7-Fr 3.5-mm irrigated tip Navi-Star ThermocoolTM catheter (Biosense-Webster,
Diamond Bar, CA) to generate an accurate three-dimensional electroanatomic map of the RV,
reflecting the shape evidenced by angiography. High-density mapping was obtained in sinus
rhythm, and the voltage maps were edited setting the point density (fill threshold) at 15 mm and
manually eliminating intracavitary points.10 Adequate catheter contact was confirmed by
concordant catheter tip motion with the cardiac silhouettes on fluoroscopy and by adherence of
voltage map to frozen angiographic right ventricular shape. In addition, to avoid low voltage
recordings due to poor contact, the following tools were used: 1) the signal had to satisfy the
three stability criteria automatically detected by the CARTOTM system in terms of cycle length,
local activation time and beat-to-beat difference of the location of the catheter (<2%, <3 ms, and
f EAM, endomymymymmymm
malititiiiiiiesesesesesess, , , , , ,, asasasasasasas p p p p p pprererererererevvvvviviv
e
e a
system (Biosense-Webster, Diamond Bar, CA). Mapping po
electroanatomic mapping
ent high-density RV three-dimensional electroanatomic volta
system (Biosense-Webster, Diamond Bar, CA). Mapping po
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

7
<4 mm, respectively); 2) both bipolar and unipolar signals were simultaneously acquired to
confirm true catheter contact through the analysis of local electrograms (in particular the shape
of the unipolar electrograms); 3) in the presence of a low voltage area, at least 3 additional points
were further acquired at the same site to confirm the reproducibility of the voltage measurement.
The color display to identify normal and abnormal voltage myocardium ranged from red,
indicating electroanatomic scar tissue (amplitude <0.5 mV), to purple, indicating electroanatomic
normal tissue (amplitude 1.5 mV). Intermediate colors represented the electroanatomic border
zone (signal amplitudes between 0.5 and 1.5 mV). The CARTOTM-incorporated surface area
calculation tool was used to measure the extension of RV electroanatomical scars. The
anatomical distribution of the pathological areas was evaluated dividing the RV voltage map into
five areas: 1) the outflow tract; 2) the free (anterolateral) wall; 3) the apex; 4) the
inferior/posterior wall (including the inferior and posterior basal segments); and 5) the septal
wall. According to previous studies, “electroanatomic scar” was defined as an area including at
least 3 adjacent points with bipolar signal amplitude <0.5 mV; the reference value for normal
endocardium was set at 1.5 mV as previously described for the identification of normal and
scarred areas.10
Endomyocardial biopsy, histology and immunohistochemistry
Right ventricular endomyocardial biopsies (4-5 samples from each patient) were obtained via the
femoral vein with the use of a preformed long sheath and a disposable bioptome (Cordis,
Johnson and Johnson, FL, USA). Once EAM was completed, the mapping catheter’s tip was
directed against abnormal voltage areas and the distal end of the sheath was placed close to it.
Sheath position was checked in right and left anterior oblique view and then biopsies were
withdrawn from wall segments with abnormal voltage, as previously shown.10 In case of normal
anatomical scccccararaaaaa
ivididididiididingngngngngngng t t t t tthehehehehehehe R RRRRRRV V VVVVV v
tflow tract 2) the free (anterolateral) wall 3) the a 4) the
a
p r
tflow tract; 2) the free (anterolateral) wall; 3) the apex; 4) the
all (including the inferior and posterior basal segments); and
previous studies, “electroanatomic scar” was defined as an ar
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

8
EAM, endomyocardial biopsies were withdrawn from conventional sites including apex and
interventricular septum.
Two to three samples were processed for histology and immunohistochemistry. For
histology, multiple 5- m-thick sections were cut and stained with hematoxylin-eosin, Miller’s
elastic Van Gieson, Masson’s trichrome, and examined by light microscopy.
Immunohistochemistry for the characterization of inflammatory infiltrates was performed using
the following antibodies: CD3, CD8, CD45RO, CD68, (Dako Corporation, Glostrup, Denmark),
as previously described.10, 16-18 To quantify the inflammatory infiltrates, CD8+ and CD45RO+
positive lymphocytes were counted per high-power field (400-fold magnification) in all available
fields, and the mean number was calculated, as previously described.16-18 In patients presenting
histologic evidence of fibro-fatty replacement, a histomorphometric analysis was performed on
Masson’s trichrome-stained sections to calculate the extent of myocardial atrophy and fibro-fatty
replacement. Images obtained at 5× magnification with a digital camera (Leica DFC 420C, Leica
microsystems, Switzerland) were stored as TIFF files and analyzed with a dedicated imaging
software (Leica Application Suite v3.0, Leica microsystems, Switzerland) to calculate the
percent area occupied by adipose tissue, replacement fibrosis and residual myocardium. The
diagnosis of myocarditis was based on Dallas criteria and immunohistochemistry:19 in particular
a T-lymphocyte infiltration (>7/mm2) in the presence of cytotoxic (CD8+) and activated
(CD45RO+) lymphocytes, was considered diagnostic.20 The diagnosis of ARVC was made on
the basis of extensive fibro-fatty myocardial atrophy with a percentage of fat >3% and fibrous
tissue >40% associated with amounts of residual myocytes <45% of the specimen at
morphometric analysis.21
Statistical analysis
ld magng ificattiiiiiiiononooooo
bed.......16-16-1818 I I I I I I In n nnnnn papapapapapapattittt e
o s
- h
s D
of fibro-fatty replacement, a histomorphometric analysis was
-stained sections to calculate the extent of myocardial atrophmm
s obtained at 5× magnification with a digital camera (Leica D
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from
9
Between-group comparisons were assessed by the unpaired t-test or Mann-Whitney U test, as
appropriate, and proportions were compared by Fisher’s exact test. Bivariate linear correlations
analyses were assessed with the Spearman’s rank correlation coefficient. The diagnostic
performance of late potentials and, separately, of different SAECG parameters in diagnosing
cardiomyopathy-related RVOT-VAs was evaluated computing the sensitivity, specificity,
positive and negative predictive values with their 95% confidence interval (CI). The best cut-off
value of each SAECG parameter for the diagnosis of cardiomyopathy-related RVOT-VAs was
assessed by means of a receiver operating characteristic (ROC) analysis. Data are reported as
median (interquartile range), unless differently indicated. A level of P < 0.05 was considered for
statistical significance. Statistical analyses were done by STATA 11.2 software package (Stata
Corporation, College Station, Texas, USA).
Results
Clinical features and non-invasive findings
Clinical characteristics and noninvasive findings of the patient population are summarized in
Table 1. Spontaneous RVOT-VAs (i.e., left bundle branch block pattern and inferior axis) were
documented in all patients, and included sustained monomorphic ventricular tachycardia (VT) in
6 (25%), multiple runs of nonsustained VT in 8 (33%), and frequent (i.e., >1,000/24h) premature
ventricular contractions (PVCs) in 10 (42%) patients. Overall, 17 (71%) patients presented either
one clinical, ECG or imaging abnormality suggestive of ARVC. Among these, 10 (42%) patients
presented ECG depolarization (i.e., epsilon wave or localized prolongation of the QRS complex
in right precordial leads) or repolarization (i.e., inverted T waves beyond lead V1) abnormalities,
5 (21%) major abnormalities at non-invasive imaging evaluation (two-dimensional
l of P < 0.05 wwwwwwwaaaaa
A 111.2.2.2.2222 s s s s s ssofofofofofofoftwtwtwtwtwtwtwararararararare eeeee p
ee Station, Texas, USA).
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

10
echocardiography or CMR), and 2 (8%) had family history of ARVC. No association between
different types of presenting RVOT arrhythmia (sustained vs. nonsustained VT vs. frequent
VPBs) and presence of baseline major abnormalities at non-invasive evaluation was found (P =
0.14 for multiple comparison). Seven patients (29%) had history of unexplained syncope and
arrhythmia-related symptoms (mainly palpitations) were present in 20 patients (83%).
Electroanatomic voltage mapping results
Table 2 reports the results of the invasive study (EAM and EAM-guided endomyocardial
biopsy). Nineteen patients (79%) had an abnormal voltage map, presenting at least one area
(median 2 [1-2]) with contiguous bipolar electrograms with voltage values < 0.5 mV (scar tissue)
surrounded by a larger zone with signal amplitudes comprised between 0.5 and 1.5 mV
indicating abnormal myocardium. The RVOT was involved in all 19 patients with abnormal
EAM, and the RV free wall represented the second most frequently affected segment (10/19
cases, 53%). Focal involvement of the RVOT was present in 5/19 (26%) patients, with a median
scar extension of 10 (9-17) cm2. The remaining 14 patients presented a more diffuse RV
involvement (2 RV segments in 11 cases, and 3 RV segments in 3 cases), corresponding to a
median scar extension of 28 (12-46) cm2.
Endomyocardial biopsy findings and final diagnosis of the RVOT-VAs substrate
In 11/19 (58%) patients with abnormal EAM, the presence of myocardial atrophy and fibro-fatty
replacement at EAM-guided endomyocardial biopsy definitely established the diagnosis of
ARVC according to current diagnostic criteria (Tables 2 to 4). In the remaining 8/19 (42%)
cases with abnormal EAM, histology showed the presence of inflammatory infiltrates associated
with necrosis of adjacent myocytes, consistent with the diagnosis of active myocarditis according
to Dallas criteria (Tables 2 and 4). In all these patients immunohistochemistry showed
age values < 00.5.5.5.5.5.5.5
etweeenenenenenenen 0 0 0 0 0 0 .5.5.5.5.5.5.5 a a a a a aandndndndndndnd 1
t
r m
n s
myocardium. The RVOT was involved in all 19 patients wit
ree wall represented the second most frequently affected segm
nvolvement of the RVOT was present in 5/19 (26%) patients
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

11
inflammatory infiltrates to be mainly represented by activated and cytotoxic T lymphocytes. No
patient showed histological features of sarcoidosis, granulomatous and/or giant cell myocarditis.
With the exception of being slightly older, patients with ARVC did not differ from those with
myocarditis in terms of other clinical and instrumental findings.
Finally, all 5 patients with normal EAM displayed also normal histology at
endomyocardial biopsies, which were withdrawn from conventional sites including the RV apex
and the interventricular septum. In all these patients, non-invasive evaluation showed also no
abnormality, and a final diagnosis of idiopathic RVOT-VAs was definitely established. Of note,
all patients with idiopathic RVOT-VAs presented with nonsustained VAs (i.e., frequent PVCs or
nonsustained VT), whereas 6/19 (32%) patients with cardiomyopathy-related RVOT-VAs
presented with sustained VT (P = 0.28 for comparison).
Signal-averaged ECG and the histologic substrate of RVOT-VAs
Overall, ventricular late potentials at SAECG were present in 11 patients (46%), all with
cardiomyopathy-related RVOT-VAs (7 ARVC and 4 myocarditis, P = 0.041 for comparison with
idiopathic RVOT-VAs). Of note, patients with late potentials were more likely to have history of
syncope (P = 0.023), and RV morpho-functional abnormalities at CMR (Table 1).
Patients with idiopathic RVOT-VAs had significantly shorter duration of the fQRS
complex (83 [82-84] ms vs. 106 [92-132] ms, P = 0.01) and LAS40 (19 [18-21] ms vs. 39 [36-
51] ms, P = 0.02), and significantly higher values of RMS40 (33 [32-33] V vs. 18 [9-26] V, P
= 0.04) (Figure 1). No significant differences in SAECG parameters were found between
patients with ARVC-related RVOT-VAs and those with myocarditis (fQRSd 106 [91-132] ms
vs. 106 [96-127] ms, P = 0.83; LAS40 39 [36-51] ms vs. 42 [36-68] ms, P = 0.33; RMS40 18
[15-28] V vs. 18 [8-25] V, P = 0.48, respectively).
ned VAs (i.e.,.,,,,,, f f r
pathyhyyyyyy-r-rrrrrrelelelelelele atatatatatatatededededededed R R R R RRRVV
C
l
ined VT (P = 0.28 for comparison).
CG and the histologic substrate of RVOT-VAs
late potentials at SAECG were present in 11 patients (46%),
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

12
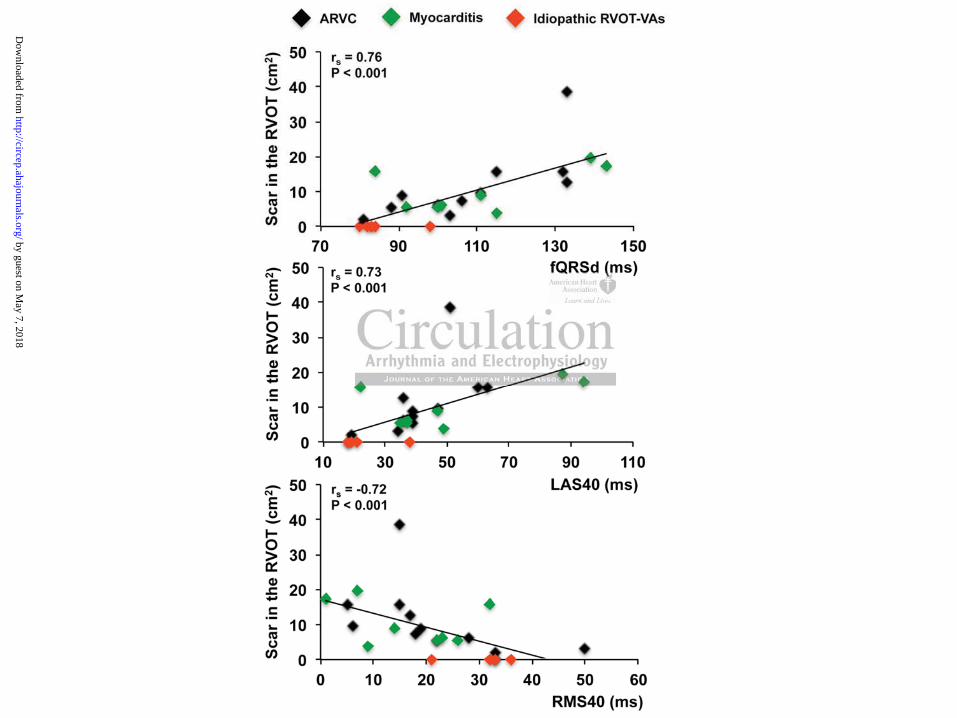
A significant linear correlation was found between all SAECG parameters and the
extension of RVOT cardiomyopathic involvement (i.e., cm2 of RVOT scar), with the most
significant association being observed for the fQRSd (rs = 0.76, P < 0.001) and for the LAS40 (rs
= 0.73, P < 0.001) (Figure 2). Of note, SAECG parameters were not associated with presence of
scar in other RV segments (Table 2).
Overall, presence of late potentials at SAECG diagnosed cardiomyopathy-related RVOT-
VAs with a sensitivity of 58% (95% CI 38% to 78%), a specificity of 100%, a very high positive
predictive value (100%), but relatively low negative predictive value (38% [95% CI 19% to
58%]), since late potentials were absent in 8/19 (42%) patients with cardiomyopathy-related
RVOT-VAs (4 ARVC and 4 myocarditis). The presence of late potentials was associated with
higher extension of electroanatomic scar in the RVOT (13 [9-17] cm2 vs. 5 [4-6] cm2, P = 0.01),
and late potentials were absent in 7/9 (78%) patients with RVOT scar <8 cm2. Accordingly, at
ROC analysis, an extension of electroanatomic scar 8 cm2 was found the best predictor of
positive late potentials (sensitivity 91%, specificity 92%).
When analyzed according to established cut-off values (i.e., fQRSd >114 ms; LAS40 >38
ms, and RMS40 <20 V), all three individual SAECG parameters showed high specificity
(100%) for the diagnosis of cardiomyopathy-related RVOT-VAs. However, the sensitivity
ranged from 37% (95% CI 18% to 56%) for the fQRSd, to 58% (95% CI 38% to 78%) for the
LAS40 and RMS40. The sensitivity of the fQRSd reached 74% (95% CI 56% to 91%) without
affecting the 100% specificity adopting a cut-of value of 100 ms, while the established cut-off
values for LAS40 and RMS40 were confirmed the best cut-off values also at ROC analysis.
Adopting a cut-off value to define abnormal fQRSd of 100 ms, the recalculated
sensitivity and negative predictive value of late potentials (i.e., at least 2 abnormal SAECG
with cardiomyyopopopopopopopa
potennnnnnntitititititiialalalalalala s s sssss wawawawawawawas s s s s s s asa
e
w
x p
electroanatomic scar in the RVOT (13 [9-17] cm2 vs. 5 [4-6]
were absent in 7/9 (78%) patients with RVOT scar <8 cm2. A
xtension of electroanatomic scar 8 cm2 was found the best p
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

13
parameters) to diagnose cardiomyopathy-related RVOT-VAs reached 84% (95% CI 70% to
99%) and 63% (95% CI 43% to 82%), respectively, while the specificity and positive predictive
value remained high (100%) (Figure 3).
Discussion
The differential diagnosis between idiopathic and cardiomyopathy-related RVOT-VAs is a major
clinical challenge for cardiologists; RVOT-VAs may represent the early manifestation of
concealed cardiomyopathies that can unpredictably lead to sudden cardiac death in the absence
of overt structural RV abnormalities.4-6 The SAECG is a quick and inexpensive diagnostic tool to
disclose the presence of pathologically slow conduction areas in the RV (i.e., late potentials) due
to underlying cardiomyopathic substrates.7, 12, 15 Although SAECG abnormalities have been
described in patients with cardiomyopathy-related RVOT-VAs,7, 10, 15 their pathophysiologic
basis and diagnostic relevance are still undefined.
The present study elucidates the pathophysiologic basis of SAECG abnormalities in
patients with RVOT-VAs, showing that they correlate with the extent of the pathologic
involvement of the RVOT by cardiomyopathic substrates. Of note, epsilon waves at surface
ECG, which represent the macroscopic manifestation of late potentials at SAECG, were found in
3 patients in the ARVC group who had significantly larger RVOT scars compared to those
without epsilon waves. This finding is in line with seminal experiences on endocardial mapping
of epsilon waves in ARVC.22
Presence of late potentials was strikingly associated with cardiomyopathy-related RVOT-
VAs, and such association was observed independently from the underlying histologic substrate
identified through EAM-guided endomyocardial biopsy (i.e., ARVC or myocarditis). The
nd inexpensiveveeeeee d
the RRRRRRRV V V V V VV (i(i(i(i(i(i(i.e.e.e.e.e.e.e.,.,.,.,.,.,., l l l l l l laaaatataa e
m s
s o
myopathic substrates.7, 12, 15 Although SAECG abnormalities
s with cardiomyopathy-related RVOT-VAs,7, 10, 15 their patho
relevance are still undefined.
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

14
clinical overlap between these two clinical entities has been well-reported in recent years;10, 23, 24
the present study shows that such overlap may extend also to SAECG abnormalities, which
could be caused by either slow conduction due to fibro-fatty tissue, as it is the case for ARVC, or
to underlying myocardial inflammation, as it is the case for myocarditis. Importantly, a
significantly higher prevalence of late potentials was found among patients with history of
previous syncope, further supporting the concept that SAECG abnormalities in these patients
underlie potentially life-threatening cardiomyopathic substrates. Indeed, syncope has been
consistently demonstrated an ominous predictor of sudden cardiac death in patients with RV
cardiomyopathy.25 Moreover, late potentials were associated with a higher prevalence of RV
dilatation and dysfunction, which is consistent with previous studies.9 While the presence of late
potentials was strikingly associated with underlying RVOT cardiomyopathic substrates, absence
of SAECG abnormalities did not reliably rule out RVOT pathologic involvement, since 7/9
patients with a small RVOT scar (i.e., <8 cm2) actually displayed normal SAECG. These
findings account for a high specificity and positive predictive value, but relatively low sensitivity
and negative predictive value of SAECG in diagnosing cardiomyopathy-related RVOT-VAs,
which is in line with recent data on SAECG in ARVC.15
At ROC analysis, the diagnostic performance of individual SAECG parameters adopting
established cut-off values appeared optimal for the LAS40 and RMS40, but suboptimal for the
fQRSd. However, the diagnostic sensitivity of the fQRSd increased from 37% (95% CI 18% to
56%) to 74% (95% CI 56% to 91%) after decreasing the cut-off value to define abnormal fQRSd
from 114 ms to 100 ms. Although the results of our ROC analysis should be interpreted with
caution due to the small sample size of our patient population, they may also suggest that
different cut-off values for the fQRSd may be necessary to improve the diagnostic performance
h a higher preevavavvvvv
dies..9999999 W W W W W WWhihihihihihihilelelelelelele t t t t t tthehehhhhh
n b
l n
l G
ngly associated with underlying RVOT cardiomyopathic sub
lities did not reliably rule out RVOT pathologic involvemen
l RVOT scar (i.e., <8 cm2) actually displayed normal SAECG
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

15
of SAECG in the setting of RVOT-VAs. To this regard, it is important to emphasize that the
current cut-off values for late potentials have been derived from studies in patients with ischemic
cardiomyopathy after acute myocardial infarction.14
Clinical implications
The significant correlation between SAECG abnormalities and cardiomyopathic involvement of
the RVOT, whatever the underlying pathological substrate, may have important clinical
implication, particularly in segmental and early forms of ARVC and in younger patients with
ventricular arrhythmias due to focal myocarditis and mild or absent RV abnormalities. On the
basis of the observed high positive predictive value, the detection of abnormal SAECG
parameters during the noninvasive workup of patients with RVOT-VAs should raise the
suspicion of underlying cardiomyopathic substrates and point to further investigation. On the
other hand, absence of late potentials does not reliably rule out the presence of small RVOT
scars reflecting underlying pathologic substrates, at least when adopting current cut-off values
for defining abnormal SAECG parameters.
In these cases, EAM with EAM-guided endomyocardial biopsy appears important to
reach a definite diagnosis of substrate, especially in the presence of peculiar clinical features
such as family history of ARVC, sustained VAs, or typical ECG depolarization/repolarization
abnormalities. Indeed, in our study no other non-invasive diagnostic tool, including contrast-
enhanced cardiac magnetic resonance, was able to distinguish between patients with ARVC-
related VAs and those with myocarditis. The definite diagnosis of the substrate underlying
RVOT-VAs might have important clinical consequences on the therapeutic approach (e.g.,
ablation, ICD, drugs), prognosis, and familial screening (indicated in the presence of a diagnosis
of ARVC).
n of abnormall S SS S SSSA
T-VAVAVAVAVAVAVAs s sss s shshshshshhshouououououououldldldldldldld r
y a
m
e
ying cardiomyopathic substrates and point to further investiga
of late potentials does not reliably rule out the presence of sm
erlying pathologic substrates, at least when adopting current
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

16
On the other hand, our study suggests also that the sensitivity and negative predictive
value of the SAECG may significantly increase when adopting a cut-off value for defining
abnormal fQRSd of 100 ms, and this finding warrants a prospective validation in properly
designed studies.
Study limitations
This study included a relatively small sample of patients who underwent an extensive diagnostic
study protocol, including EAM and EAM-guided endomyocardial biopsy. As such, caution
should be exercised in generalizing our findings to a larger and unselected cohort of patients with
RVOT-VAs, especially the computations on the diagnostic performance of the SAECG in
diagnosing cardiomyopathy-related RVOT-VAs.
It is also important to emphasize that our Institution is a tertiary center for the study of
arrhythmic manifestations of cardiomyopathies, and many patients with clinical suspicion of
underlying cardiomyopathic substrates (e.g., family history of sudden death,
depolarization/repolarization abnormalities at the 12-lead ECG) are usually sent from other other
Institutions or referring physicians. Therefore, a possible referral bias may also have influenced
the features of study population.
Finally, our cohort of patients with cardiomyopathy-related RVOT-VAs consisted only of
patients with ARVC and myocarditis. Whether our results may be generalized also to patients
with RVOT-VAs and underlying myocardial substrates other than that reported in our series
(e.g., sarcoidosis, Chagas cardiomyopathy, or myocardial infarction) warrants further
investigation.
Conclusions
In patients with RVOT-Vas, abnormal SAECG parameters reflect the presence of
rmance of the e e e ee SSSSS
o
a
y
ortant to emphasize that our Institution is a tertiary center fo
ations of cardiomyopathies, and many patients with clinical
yopathic substrates (e.g., family history of sudden death,
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

17
cardiomyopathic involvement of the RVOT, and should prompt to perform further diagnostic
investigations, including EAM with EAM-guided biopsy, to identify the underlying myocardial
substrate. Our findings clarify the pathophysiologic basis of SAECG abnormalities in such
patients, and provide an explanation to the observed high specificity but low sensitivity of late
potentials in diagnosing cardiomyopathy-related RVOT-VAs. With the current cut-off values to
define abnormal SAECG parameters, most patients with small RVOT areas of cardiomyopathic
involvement (i.e., <8 cm2) are missed. The diagnostic sensitivity of SAECG in detecting
cardiomyopathy-related RVOT-VAs may significantly increase (16/19 [84%] patients correctly
diagnosed) considering a value of the fQRSd 100 ms as abnormal. Such findings, if confirmed
in larger series, could lead to redefine the relevance of SAECG in the differential diagnosis
between idiopathic and cardiomyopathy-related RVOT-VAs.
Funding Sources: This study was partially supported by a Telethon Foundation Grant (GGP10186 to M.P.).
Conflict of Interest Disclosures: Dr. Andrea Natale has received consultant fees or honoraria from Biosense Webster, Boston Scientific, Medtronic, Biotronic, and LifeWatch. Dr. Claudio Tondo has served as a member of the advisory board of Biosense Webster and has been a consultant for and received lecture fees from St. Jude Medical. Dr. Luigi Di Biase has received consultant fees from Biosense Webster and Hansen Medical.
References:
1. Buxton AE, Waxman HL, Marchlinski FE, Simson MB, Cassidy D, Josephson ME. Right ventricular tachycardia: clinical and electrophysiologic characteristics. Circulation. 1983;68:917-927. 2. Lerman BB, Stein K, Engelstein ED, Battleman DS, Lippman N, Bei D, Catanzaro D. Mechanism of repetitive monomorphic ventricular tachycardia. Circulation. 1995;92:421-429. 3. Marcus FI, Fontaine GH, Guiraudon G, Frank R, Laurenceau JL, Malergue C, Grosgogeat Y. Right ventricular dysplasia: a report of 24 adult cases. Circulation. 1982;65:384-398.
mal. Such findiiiiiingnnnnnn
n thhe e e e ee e dididididididiffffffffffffferererererererenenenenenenentititititititia
a
T)
and cardiomyopathy-related RVOT-VAs.
This study was partially supported by a Telethon Foundation ).
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

18
4. Pedersen DH, Zipes DP, Foster PR, Troup PJ. Ventricular tachycardia and ventricular fibrillation in a young population. Circulation. 1979;60:988-997. 5. Lesch M, Lewis E, Humphries JO, Ross RS. Paroxysmal ventricular tachycardia in the absence of organic heart disease. Report of a case and review of the literature. Ann Intern Med. 1967;66:950-960.
6. Maddox K. Intermittent ventricular tachycardia in youth: report of case with fatal termination. Am Heart J. 1947;33:739-740. 7. Santangeli P, Infusino F, Sgueglia GA, Sestito A, Lanza GA. Ventricular late potentials: a critical overview and current applications. J Electrocardiol. 2008;41:318-324. 8. Nasir K, Rutberg J, Tandri H, Berger R, Tomaselli G, Calkins H. Utility of SAECG in arrhythmogenic right ventricle dysplasia. Ann Noninvasive Electrocardiol. 2003;8:112-120. 9. Nava A, Folino AF, Bauce B, Turrini P, Buja GF, Daliento L, Thiene G. Signal-averaged electrocardiogram in patients with arrhythmogenic right ventricular cardiomyopathy and ventricular arrhythmias. Eur Heart J. 2000;21:58-65. 10. Pieroni M, Dello Russo A, Marzo F, Pelargonio G, Casella M, Bellocci F, Crea F. High prevalence of myocarditis mimicking arrhythmogenic right ventricular cardiomyopathy differential diagnosis by electroanatomic mapping-guided endomyocardial biopsy. J Am Coll Cardiol. 2009;53:681-689. 11. Jadonath RL, Schwartzman DS, Preminger MW, Gottlieb CD, Marchlinski FE. Utility of the 12-lead electrocardiogram in localizing the origin of right ventricular outflow tract tachycardia. Am Heart J. 1995;130:1107-1113. 12. Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, Calkins H, Corrado D, Cox MG, Daubert JP, Fontaine G, Gear K, Hauer R, Nava A, Picard MH, Protonotarios N, Saffitz JE, Sanborn DM, Steinberg JS, Tandri H, Thiene G, Towbin JA, Tsatsopoulou A, Wichter T, Zareba W. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the task force criteria. Circulation. 2010;121:1533-1541. 13. Santarelli P, Lanza GA, Biscione F, Natale A, Corsini G, Riccio C, Occhetta E, Rossi P, Gronda M, Makmur J. Effects of thrombolysis and atenolol or metoprolol on the signal-averaged electrocardiogram after acute myocardial infarction. Late Potentials Italian Study (LAPIS). Am J Cardiol. 1993;72:525-531.
14. Breithardt G, Cain ME, el-Sherif N, Flowers NC, Hombach V, Janse M, Simson MB, Steinbeck G. Standards for analysis of ventricular late potentials using high-resolution or signal-averaged electrocardiography. A statement by a Task Force Committee of the European Society of Cardiology, the American Heart Association, and the American College of Cardiology. Circulation. 1991;83:1481-1488.
Thiene G. Sigiggggggnnannnnnulululllullaaaaaaarrr rrrr cacacacacacacardrdrdrdrdrdrdioioioioioioiomymymymymymymyopopopopopopopaaaaaaa
o ra ys s
hwartzman DS Preminger MW Gottlieb CD Marchlinski F
o Russo A, Marzo F, Pelargonio G, Casella M, Bellocci F, Crarditis mimicking arrhythmogenic right ventricular cardiomyrrs by electroanatomic mapping-guided endomyocardial biops1-689.
hwartzman DS Preminger MW Gottlieb CD Marchlinski F by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

19
15. Kamath GS, Zareba W, Delaney J, Koneru JN, McKenna W, Gear K, Polonsky S, Sherrill D, Bluemke D, Marcus F, Steinberg JS. Value of the signal-averaged electrocardiogram in arrhythmogenic right ventricular cardiomyopathy/dysplasia. Heart Rhythm. 2011;8:256-262. 16. Chimenti C, Calabrese F, Thiene G, Pieroni M, Maseri A, Frustaci A. Inflammatory left ventricular microaneurysms as a cause of apparently idiopathic ventricular tachyarrhythmias. Circulation. 2001;104:168-173. 17. Chimenti C, Pieroni M, Maseri A, Frustaci A. Histologic findings in patients with clinical and instrumental diagnosis of sporadic arrhythmogenic right ventricular dysplasia. J Am Coll Cardiol. 2004;43:2305-2313. 18. Frustaci A, Priori SG, Pieroni M, Chimenti C, Napolitano C, Rivolta I, Sanna T, Bellocci F, Russo MA. Cardiac histological substrate in patients with clinical phenotype of Brugada syndrome. Circulation. 2005;112:3680-3687. 19. Baughman KL. Diagnosis of myocarditis: death of Dallas criteria. Circulation.2006;113:593-595. 20. Noutsias M, Fechner H, de Jonge H, Wang X, Dekkers D, Houtsmuller AB, Pauschinger M, Bergelson J, Warraich R, Yacoub M, Hetzer R, Lamers J, Schultheiss HP, Poller W. Human coxsackie-adenovirus receptor is colocalized with integrins alpha(v)beta(3) and alpha(v)beta(5) on the cardiomyocyte sarcolemma and upregulated in dilated cardiomyopathy: implications for cardiotropic viral infections. Circulation. 2001;104:275-280. 21. Angelini A, Basso C, Nava A, Thiene G. Endomyocardial biopsy in arrhythmogenic right ventricular cardiomyopathy. Am Heart J. 1996;132:203-206.
22. Belhassen B, Caspi A, Miller H, Shapira I, Laniado S. Extensive endocardial mapping during sinus rhythm and ventricular tachycardia in a patient with arrhythmogenic right ventricular dysplasia. J Am Coll Cardiol. 1984;4:1302-1306.
23. Corrado D, Basso C, Leoni L, Tokajuk B, Bauce B, Frigo G, Tarantini G, Napodano M, Turrini P, Ramondo A, Daliento L, Nava A, Buja G, Iliceto S, Thiene G. Three-dimensional electroanatomic voltage mapping increases accuracy of diagnosing arrhythmogenic right ventricular cardiomyopathy/dysplasia. Circulation. 2005;111:3042-3050. 24. Ladyjanskaia GA, Basso C, Hobbelink MG, Kirkels JH, Lahpor JR, Cramer MJ, Thiene G, Hauer RN, MF VO. Sarcoid myocarditis with ventricular tachycardia mimicking ARVD/C. JCardiovasc Electrophysiol. 2010;21:94-98. 25. Corrado D, Calkins H, Link MS, Leoni L, Favale S, Bevilacqua M, Basso C, Ward D, Boriani G, Ricci R, Piccini JP, Dalal D, Santini M, Buja G, Iliceto S, Estes NA, 3rd, Wichter T, McKenna WJ, Thiene G, Marcus FI. Prophylactic implantable defibrillator in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia and no prior ventricular fibrillation or sustained ventricular tachycardia. Circulation. 2010;122:1144-1152.
teria. Circulatttttttioioioiioii
hner H de Jonge H Wang X Dekkers D, Houtsmuller AB, c ru at mf
so C Nava A Thiene G Endomyocardial biopsy in arrhythm
hner H, de Jonge H, Wang X, Dekkers D, Houtsmuller AB, ch R, Yacoub M, Hetzer R, Lamers J, Schultheiss HP, Pollerus receptor is colocalized with integrins alpha(v)beta(3) and ate sarcolemma and upregulated in dilated cardiomyopathy: imdfections. Circulation. 2001;104:275-280.
so C Nava A Thiene G Endomyocardial biopsy in arrhythm by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

20
Table 1. Clinical characteristics and noninvasive findings of the overall sample and according to
results of the SAECG. Overall Sample
(n = 24) Positive LPs
(n = 11) Negative LPs
(n = 13) P*
Age, years 50 (42-59) 51 (47-64) 45 (39-54) 0.10 Sex, male 12 (50) 5 (45) 7 (54) >0.99 Presenting RVOT-VA
Sustained VT 6 (25) 5 (45) 1 (8) 0.06 Nonsustained VT 8 (33) 3 (27) 5 (38) 0.68 Frequent PVCs (>1,000/24h) 10 (42) 3 (27) 7 (54) 0.24
Family history of ARVC 2 (8) 0 (0) 2 (15) 0.48 Clinical symptoms
Cardiac arrest 0 (0) 0 (0) 0 (0) - Syncope 7 (29) 6 (55) 1 (8) 0.023 Palpitations 17 (71) 8 (73) 9 (69) >0.99 No symptoms 4 (17) 0 (0) 4 (31) 0.09
ECG abnormalities Right precordial QRS duration 110 ms 9 (38) 7 (64) 2 (15) 0.033 Epsilon wave 3 (13) 3 (27) 0 (0) 0.08 Inverted T waves beyond lead V1 4 (17) 3 (27) 1 (8) 0.30
CMR abnormalities RV dilatation 6/22 (27) 5/9 (55) 1/13 (8) 0.023 RV global dysfunction 5/22 (23) 5/9 (56) 0/13 (0) 0.005 RV delayed enhancement, % 7/22 (32) 5/9 (56) 2/13 (15) 0.07 RV ejection fraction, % 58 (50-59) 49 (49-50) 59 (58-60) <0.001 LV ejection fraction, % 60 (56-65) 60 (55-66) 60 (59-64) 0.56
Values expressed as median (interquartile range) or n (%). LPs = ventricular late potentials; RVOT-VA = right ventricular outflow tract ventricular arrhythmia; VT = ventricular tachycardia; PVC = premature ventricular contraction; CMR = cardiac magnetic resonance; RV = right ventricular; LV = left ventricular. *Comparison between “Positive LPs” and “Negative LPs”
Table 2. Invasive findings of the overall sample and according to results of the SAECG. Overall Sample
(n = 24) Positive LPs
(n = 11) Negative LPs
(n = 13) P*
Electroanatomic scar 19 (79) 11 (100) 8 (62) 0.041 N. of EAM scars 2 (1-2) 2 (1-2) 2 (0-2) 0.69 Localization of EAM
Outflow tract 19 (79) 11 (100) 8 (62) 0.041 Free wall 10 (42) 6 (55) 4 (31) 0.41 Inferior/Posterior wall 6 (25) 1 (9) 5 (38) 0.17 Septal wall 1 (4) 0 (0) 1 (8) >0.99 Apex 0 (0) 0 (0) 0 (0) -
Endomyocardial biopsy ARVC 11 (46) 7 (64) 4 (31) 0.22 Myocarditis 8 (33) 4 (36) 4 (31) >0.99 Normal myocardium 5 (21) 0 (0) 5 (38) 0.041
Values expressed as median (interquartile range), or n (%).LPs = ventricular late potentials; N. = number; EAM = electroanatomic mapping. *Comparison between “Positive LPs” and “Negative LPs”
3 3 (2(2(( 7)7))) 3333333 ( ( ( ( (( (27272727272727) ) ) )) ) )
6/22 (27) 5/9 (55)
on 5/22 (23) 5/9 (56)ement, % 7/22 (32) 5/9 (56)n, % 58 50-5 49 9-50, % 60 (56-65) 60 (55-66) nrhythmia; VT = ventricular tachycardia; PVC = premature ventricular contract o
sitive LPs” and “Negative LPs”
6/22 (27) 5/9 (55) on 5/22 (23) 5/9 (56)
ement, % 7/22 (32) 5/9 (56) n, % 58 (50-59) 49 (49-50) , % 60 (56-65) 60 (55-66) n (interquartile range) or n (%). LPs = ventricular late potentials; RVOT-VA = rrhythmia; VT = ventricular tachycardia; PVC = premature ventricular contractioright ventricular; LV = left ventricular. sitive LPs” and “Negative LPs” by guest on M
ay 7, 2018http://circep.ahajournals.org/
Dow
nloaded from
21
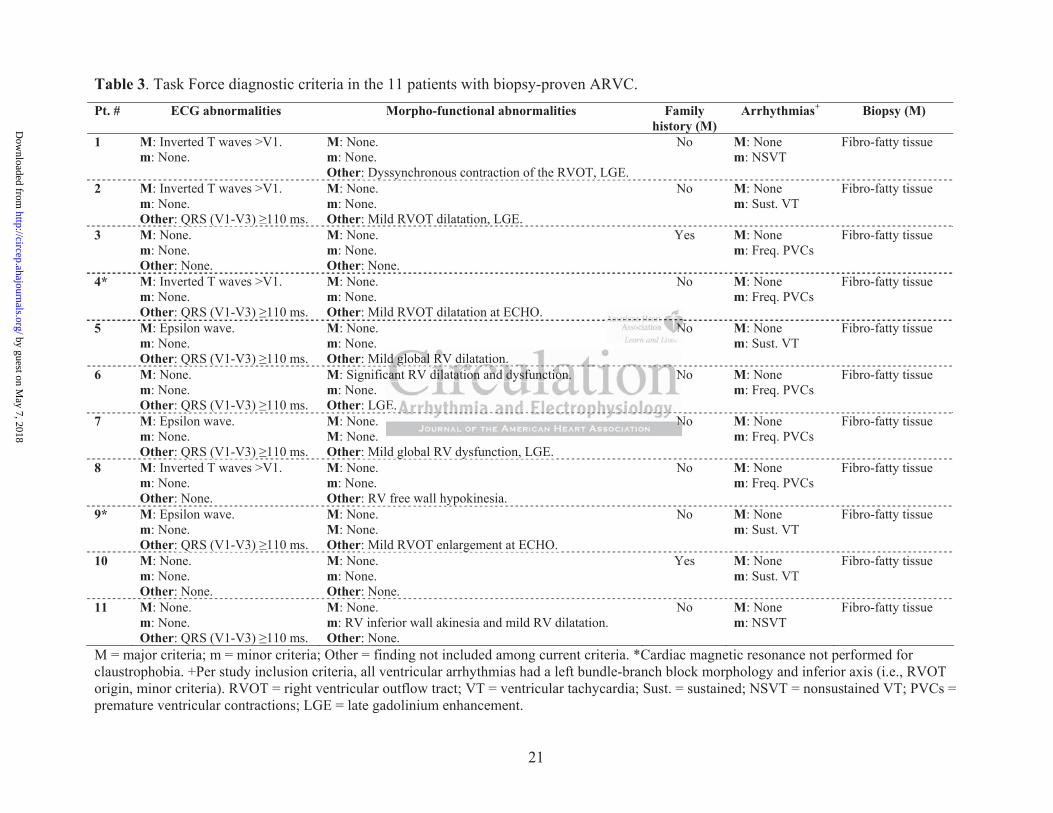
Table 3. Task Force diagnostic criteria in the 11 patients with biopsy-proven ARVC. Pt. # ECG abnormalities Morpho-functional abnormalities Family
history (M) Arrhythmias+ Biopsy (M)
1 M: Inverted T waves >V1. m: None.
M: None. m: None. Other: Dyssynchronous contraction of the RVOT, LGE.
No M: None m: NSVT
Fibro-fatty tissue
2 M: Inverted T waves >V1. m: None. Other: QRS (V1-V3) 110 ms.
M: None. m: None. Other: Mild RVOT dilatation, LGE.
No M: None m: Sust. VT
Fibro-fatty tissue yyyyyy yyyyy ,
3 M: None. m: None. Other: None.
M: None. m: None. Other: None.
Yes M: None m: Freq. PVCs
Fibro-fatty tissue Q ((((( )))) ,
4* M: Inverted T waves >V1. m: None. Other: QRS (V1-V3) 110 ms.
M: None. m: None. Other: Mild RVOT dilatation at ECHO.
No M: None m: Freq. PVCs
Fibro-fatty tissue
5 M: Epsilon wave. m: None. Other: QRS (V1-V3) 110 ms.
M: None. m: None. Other: Mild global RV dilatation.
No M: None m: Sust. VT
Fibro-fatty tissue Q ((((((( ))))))
6 M: None. m: None. Other: QRS (V1-V3) 110 ms.
M: Significant RV dilatation and dysfunction. m: None. Other: LGE.
No M: None m: Freq. PVCs
Fibro-fatty tissue Q ((((( ))))
7 M: Epsilon wave. m: None. Other: QRS (V1-V3) 110 ms.
M: None. M: None. Other: Mild global RV dysfunction, LGE.
No M: None m: Freq. PVCs
Fibro-fatty tissue Q ((((((( ))))))
8 M: Inverted T waves >V1. m: None. Other: None.
M: None. m: None. Other: RV free wall hypokinesia.
No M: None m: Freq. PVCs
Fibro-fatty tissue Q ((((( )))) ggggg yyyyy ,
9* M: Epsilon wave. m: None. Other: QRS (V1-V3) 110 ms.
M: None. M: None. Other: Mild RVOT enlargement at ECHO.
No M: None m: Sust. VT
Fibro-fatty tissue ypypypypypy
10 M: None. m: None. Other: None.
M: None. m: None. Other: None.
Yes M: None m: Sust. VT
Fibro-fatty tissue Q ((((((( )))))) ggggg
11 M: None. m: None. Other: QRS (V1-V3) 110 ms.
M: None. m: RV inferior wall akinesia and mild RV dilatation. Other: None.
No M: None m: NSVT
Fibro-fatty tissue
M = major criteria; m = minor criteria; Other = finding not included among current criteria. *Cardiac magnetic resonance not performed for claustrophobia. +Per study inclusion criteria, all ventricular arrhythmias had a left bundle-branch block morphology and inferior axis (i.e., RVOT origin, minor criteria). RVOT = right ventricular outflow tract; VT = ventricular tachycardia; Sust. = sustained; NSVT = nonsustained VT; PVCs = premature ventricular contractions; LGE = late gadolinium enhancement.
NNNNNNN
lc
E
N
N
ld global RV dilatation. cant RV dilatation and dysfunction.
E.
Nggggggg
N
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from
22
Table 4. Clinical features of the 19 patients with cardiomyopathy-related RVOT-VAs. ARVC(n = 11)
Myocarditis (n = 8)
P
Age, years 59 (48-68) 44 (38-53) 0.04 Sex, male 4 (36) 5 (63) 0.37 Presenting RVOT-VA
Sustained VT 4 (36) 2 (25) >0.99 Nonsustained VT 2 (18) 3 (38) 0.60 Frequent PVCs (>1,000/24h) 5 (45) 3 (38) >0.99
Family history of ARVC 2 (18) 0 (0) 0.49 Clinical symptoms
Cardiac arrest 0 (0) 0 (0) - Syncope 5 (45) 2 (25) 0.63 Palpitations 8 (73) 4 (50) 0.38 No symptoms 1 (9) 3 (38) 0.26
ECG abnormalities Right precordial QRS duration 110 ms 7 (64) 2 (25) 0.17 Epsilon wave 3 (27) 0 (0) 0.23 Inverted T waves beyond lead V1 4 (36) 0 (0) 0.10
CMR abnormalities RV dilatation 3/9 (33) 3/8 (38) >0.99 RV global dysfunction 3/9 (33) 2/8 (25) >0.99 RV delayed enhancement, % 4/9 (44) 3/8 (38) >0.99 RV ejection fraction, % 53 (50-58) 56 (49-58) 0.68 LV ejection fraction, % 60 (56-64) 60 (56-65) 0.91
Values expressed as median (interquartile range) or n (%). LPs = ventricular late potentials; RVOT-VA = right ventricular outflow tract ventricular arrhythmia; VT = ventricular tachycardia; PVC = premature ventricular contraction; CMR = cardiac magnetic resonance; RV = right ventricular; LV = left ventricular Figure Legends:
Figure 1. SAECG parameters in patients with cardiomyopathy-related and idiopathic RVOT-VAs.
Vertical bars represent milliseconds (ms) for the fQRSd and LAS40, and microvolts ( V) for the
RMS40.
Figure 2. Linear correlation between mean bipolar voltages in the right ventricular outflow tract and
signal averaged electrocardiogram variables (fQRSd and LAS-40). rs = Spearman’s correlation
coefficient.
Figure 3. Panel A: performance of late potentials ( 2 abnormal SAECG parameters) in diagnosing
cardiomyopathy-related RVOT-VAs according to established cut-off values of SAECG parameters
(fQRSd >114 ms; LAS40 >38 ms, and RMS40 <20 V). Panel B: performance of late potentials in
diagnosing cardiomyopathy-related RVOT-VAs according to cut-off values of SAECG parameters
derived from ROC analysis (fQRSd 100 ms; LAS40 >38 ms, and RMS40 <20 V).
3/9 (33) 22/8/8//4/4/4/4/4/4/4/9 9 9 9 9 9 9 (4(4(4(4(4(4(44)4)4)4)4)4)4) 3 3333 3 3/8/8/8/8/8/8/83 (50000000-5-5-5-5-5-5-58)8)8)8)8)8)8) 5 55 5 5 5 56 6 6 6 6 6 6 (4(4(4(4(4(4(40 (566-6-6-6-6-6-6-64)4)4)4)4)4)4) 66 6 6 6 660 0 0 0 000 (5
(interquartile range) or n (%). LPs = ventricular late potentials; RVOT-Vh n(interquartile range) or n (%). LPs = ventricular late potentials; RVOT-V
hythmia; VT = ventricular tachycardia; PVC = premature ventricular contt RV = right ventricular; LV = left ventricular
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from

Tondo and Andrea NataleLuigi Di Biase, Andrea Macchione, J. David Burkhardt, Fulvio Bellocci, Pietro Santarelli, Claudio Pasquale Santangeli, Maurizio Pieroni, Antonio Dello Russo, Michela Casella, Gemma Pelargonio,
Myocardial Substrate in Right Ventricular Outflow Tract ArrhythmiasCorrelation Between Signal-Averaged Electrocardiogram and the Histologic Evaluation of the
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2012 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Arrhythmia and Electrophysiology
published online March 15, 2012;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/early/2012/03/15/CIRCEP.111.967893World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answerinformation about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Arrhythmia and Electrophysiology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 7, 2018
http://circep.ahajournals.org/D
ownloaded from
Related Documents











