Correlates of cognitive impairment in first episode schizophrenia: The EUFEST study Silvana Galderisi a, ⁎, Michael Davidson b , René S. Kahn c , Armida Mucci a , Han Boter c , Mihai D. Gheorghe d , Janusz K. Rybakowski e , Jan Libiger f , Sonia Dollfus g , Juan J. López-Ibor h , Joseph Peuskens i , Luchezar G. Hranov j , Wolfgang W. Fleischhacker k and EUFEST group 1 a Department of Psychiatry, University of Naples SUN, Naples, Italy b Sheba Medical Center, Tel Hashomer, Israel c Department of Psychiatry, Rudolf Magnus Institute of Neuroscience University Medical Centre Utrecht, Utrecht, The Netherlands d Department of Psychiatry, Central Military Hospital, Bucharest, Romania e Department of Adult Psychiatry, University of Medical Sciences, Poznan, Poland f Department and Clinic of Psychiatry, Charles University Medical School and Faculty Hospital, Hradec Králové, Czech Republic g Centre Esquirol, Centre Hospitalier Universitaire, Caen, France h Institute of Psychiatry and Mental Health, Hospital Clínico San Carlos, Madrid, Spain i University Psychiatric Centre, Campus St. Jozef Kortenberg, Katholieke Universiteit Leuven, Leuven, Belgium j Department and Clinic of Psychiatry, University Hospital of Neurology and Psychiatry St Naum, Sofia, Bulgaria k Department of Biological Psychiatry, Medical University Innsbruck, Innsbruck, Austria article info abstract Article history: Received 8 March 2009 Received in revised form 17 September 2009 Accepted 21 September 2009 Available online 12 October 2009 Background: Profile and correlates of cognitive deficits in first episode (FE) schizophrenia patients are still debated. The present study is aimed to clarify in a large sample of FE patients the extent of impairment in key cognitive domains and its relationships with demographic and clinical variables. Schizophrenia Research 115 (2009) 104–114 ⁎ Corresponding author. Department of Psychiatry, University of Naples SUN, Largo Madonna delle Grazie, 80138 Naples, Italy. Tel.: +39 081 5666504; fax: +39 081 5666523. E-mail addresses: [email protected], [email protected] (S. Galderisi), [email protected], [email protected] (M. Davidson), [email protected] (R.S. Kahn), [email protected], [email protected] (A. Mucci), [email protected] (H. Boter), [email protected] (J.K. Rybakowski), [email protected] (J. Libiger), [email protected] (S. Dollfus), [email protected] (J.J. López-Ibor), [email protected] (J. Peuskens), [email protected] (L.G. Hranov), [email protected] (W.W. Fleischhacker). 1 Management group: R S Kahn, W W Fleischhacker, H Boter, C Brugman, H Burger, D E Grobbee, M C Hafkamp, I P M Keet, K Nijssen. Steering Committee: R S Kahn, W W Fleischhacker, H Boter, I P M Keet, C Brugman, M Davidson, S Dollfus, W Gaebel, S Galderisi, M Gheorghe, I Gonen, D E Grobbee, L G Hranov, M Hummer, J Libiger, N Lindefors, J J López-Ibor, K Nijssen, J Peuskens, A Riecher-Rössler, J K Rybakowski, G Sedvall, M v Wilmsdorff. Office manager: P C Ywema. Julius Centre Study Team: data management—N Boekema, H den Breeijen, M van den Haak, P Huizinga, R Veen; project managers—C Brugman, M C Hafkamp, K M Nijssen; site monitoring—P Berackova, A Blizanowska, C Brugman, M C Hafkamp, T Huizinga, H van Gelderen, M Gordat, S Lorteau, G Makhanlal, H Moqadar. Tangent Data Study Team (co-monitoring Romania): I Gonen, A Mihailescu, R Radici, C Zus. Participating investigators (CC = Country coordinator; SC = site coordinator), centres, and countries: Austria—M Hummer (CC and SC Innsbruck), M Muhlbacher (SC Salzburg), H Widmoser (SC Hall in Tirol); Belgium—J Peuskens (CC), J Hulselmans (SC Antwerpen), C Mertens (SC Gent),E Thijs (SC Kortenberg); Bulgaria—L G Hranov (CC and SC Sofi a),S Georgiev (SC Plovdiv), L Sayan (SC Bourgas); Czech Republic—J Libiger (CC and SC Hradec Kràlové, E Češkovà (SC Brno), D Seifertovà (SC Praha-Bohnice); France: S Dollfus (CC and SC Caen I), G Allio (SC Rouen), B Chabot (SC Caen II), A Navarre Coulaud (SC Dieppe), P Thomas (SC Lille); Germany—W Gaebel (CC), M Krebs (SC Berlin), R Lencer (SC L eck), K Leopold (SC Berlin), T Wobrock (SC Homburg); Israel—M Davidson (CC), Y Abramovitch (SC Beer- Yaakov), D Amital (SC Ness Ziona), A Caspi (SC Ramat Gan), A Kaplan (SC Beer Sheva), I Treves (SC Shalvata), P Zipris (SC Pardessiya); Italy—S Galderisi (CC), M Casacchia (SC L'Aquila), M Mauri (SC Milano II), A Mucci (SC Naples); Netherlands—H Boter (CC and SC Utrecht), I P M Keet (CC and SC Utrecht); Poland—J K Rybakowski (CC and SC Poznan), M Jarema (SC Warsaw), M Masiak (SC Lublin), J Rabe-Jablonska (SC Lodz); Romania—M Gheorghe (CC), V Burtea (SC Brasov), P Boisteanu (SC Iasi), C Friedman (SC Constanta), M Ienciu (SC Timisoara), A Ionescu (SC Buzau), I Miclutia (SC Cluj), T Mihai (SC Tulcea), D Prelipceanu (SC Bucuresti II), T Udistroiu (SC Craiova), D Vasile (SC Bucuresti I); Spain—J J López-Ibor (CC), J L Carrasco (SC Madrid); Sweden—N Lindefors (CC and SC Stockholm), G Sedvall (CC), F A Wiesel (SC Uppsala); Switzerland—A Riecher-Rössler (CC), U Gschwandtner (SC Basel). 0920-9964/$ – see front matter © 2009 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2009.09.022 Contents lists available at ScienceDirect Schizophrenia Research journal homepage: www.elsevier.com/locate/schres

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Schizophrenia Research 115 (2009) 104–114
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r.com/ locate /schres
Correlates of cognitive impairment in first episode schizophrenia:The EUFEST study
Silvana Galderisi a,⁎, Michael Davidson b, René S. Kahn c, Armida Mucci a, Han Boter c,Mihai D. Gheorghe d, Janusz K. Rybakowski e, Jan Libiger f, Sonia Dollfus g, Juan J. López-Ibor h,Joseph Peuskens i, Luchezar G. Hranov j, Wolfgang W. Fleischhacker k
and EUFEST group 1
a Department of Psychiatry, University of Naples SUN, Naples, Italyb Sheba Medical Center, Tel Hashomer, Israelc Department of Psychiatry, Rudolf Magnus Institute of Neuroscience University Medical Centre Utrecht, Utrecht, The Netherlandsd Department of Psychiatry, Central Military Hospital, Bucharest, Romaniae Department of Adult Psychiatry, University of Medical Sciences, Poznan, Polandf Department and Clinic of Psychiatry, Charles University Medical School and Faculty Hospital, Hradec Králové, Czech Republicg Centre Esquirol, Centre Hospitalier Universitaire, Caen, Franceh Institute of Psychiatry and Mental Health, Hospital Clínico San Carlos, Madrid, Spaini University Psychiatric Centre, Campus St. Jozef Kortenberg, Katholieke Universiteit Leuven, Leuven, Belgiumj Department and Clinic of Psychiatry, University Hospital of Neurology and Psychiatry St Naum, Sofia, Bulgariak Department of Biological Psychiatry, Medical University Innsbruck, Innsbruck, Austria
a r t i c l e i n f o
⁎ Corresponding author. Department of Psychiatry, U081 5666523.
E-mail addresses: [email protected], [email protected]@umcutrecht.nl (R.S. Kahn), [email protected], [email protected] (J. Libiger), [email protected]@mail.orbitel.bg (L.G. Hranov), Wolfgang.Fleis
1 Management group: R S Kahn,WWFleischhacker, HFleischhacker, H Boter, I P M Keet, C Brugman, M DavidLindefors, J J López-Ibor, K Nijssen, J Peuskens, A Riechermanagement—NBoekema,H denBreeijen,MvandenHaABlizanowska, C Brugman,MCHafkamp, THuizinga, H vGonen, A Mihailescu, R Radici, C Zus. Participating investInnsbruck), M Muhlbacher (SC Salzburg), H WidmoserKortenberg); Bulgaria—L G Hranov (CC and SC Sofi a),S GBrno),D Seifertovà (SCPraha-Bohnice); France: SDollfusGermany—WGaebel (CC), M Krebs (SC Berlin), R LencerYaakov), D Amital (SC Ness Ziona), A Caspi (SCRamat Ga(SC L'Aquila),MMauri (SCMilano II), AMucci (SCNaplesPoznan),M Jarema (SCWarsaw), MMasiak (SC Lublin),(SC Constanta), M Ienciu (SC Timisoara), A Ionescu (SC B(SCBucuresti I); Spain—J J López-Ibor (CC), J L Carrasco (SRiecher-Rössler (CC), U Gschwandtner (SC Basel).
0920-9964/$ – see front matter © 2009 Elsevier B.V.doi:10.1016/j.schres.2009.09.022
a b s t r a c t
Article history:Received 8 March 2009Received in revised form 17 September 2009Accepted 21 September 2009Available online 12 October 2009
Background: Profile and correlates of cognitive deficits in first episode (FE) schizophreniapatients are still debated. The present study is aimed to clarify in a large sample of FE patientsthe extent of impairment in key cognitive domains and its relationships with demographic andclinical variables.
niversity of Naples SUN, LargoMadonna delle Grazie, 80138 Naples, Italy. Tel.: +39 081 5666504; fax: +39
gmail.com (S. Galderisi), [email protected], [email protected] (M. Davidson),[email protected] (A. Mucci), [email protected] (H. Boter), [email protected] (J.K. Rybakowski),(S. Dollfus), [email protected] (J.J. López-Ibor), [email protected] (J. Peuskens),[email protected] (W.W. Fleischhacker).Boter, C Brugman, H Burger, D EGrobbee,MCHafkamp, I PMKeet, KNijssen.Steering Committee:R S Kahn,WWson, S Dollfus, W Gaebel, S Galderisi, M Gheorghe, I Gonen, D E Grobbee, L G Hranov, M Hummer, J Libiger, N-Rössler, J K Rybakowski, G Sedvall, M vWilmsdorff. Office manager: P C Ywema. Julius Centre Study Team: dataak, PHuizinga, RVeen;projectmanagers—CBrugman,MCHafkamp, K MNijssen; sitemonitoring—PBerackova,anGelderen,MGordat, S Lorteau, GMakhanlal, HMoqadar. Tangent Data Study Team (co-monitoring Romania): Iigators (CC=Country coordinator; SC=site coordinator), centres, and countries: Austria—MHummer (CC and SC(SC Hall in Tirol); Belgium—J Peuskens (CC), J Hulselmans (SC Antwerpen), C Mertens (SC Gent),E Thijs (SCeorgiev (SC Plovdiv), L Sayan (SC Bourgas); Czech Republic—J Libiger (CC and SC Hradec Kràlové, E Češkovà (SC(CCandSCCaen I),GAllio (SCRouen), B Chabot (SCCaen II), ANavarre Coulaud(SCDieppe), P Thomas (SC Lille);(SC L eck), K Leopold (SC Berlin), TWobrock (SC Homburg); Israel—MDavidson (CC), Y Abramovitch (SC Beer-n), A Kaplan (SC Beer Sheva), I Treves (SC Shalvata), P Zipris (SC Pardessiya); Italy—SGalderisi (CC),MCasacchia);Netherlands—HBoter (CC and SCUtrecht), I PMKeet (CC and SCUtrecht);Poland—J K Rybakowski (CC and SCJ Rabe-Jablonska (SC Lodz); Romania—MGheorghe (CC), V Burtea (SC Brasov), P Boisteanu (SC Iasi), C Friedmanuzau), I Miclutia (SC Cluj), TMihai (SC Tulcea), D Prelipceanu (SC Bucuresti II), T Udistroiu (SC Craiova), D VasileCMadrid); Sweden—NLindefors (CC andSC Stockholm), G Sedvall (CC), F AWiesel (SCUppsala); Switzerland—A
All rights reserved.

105S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
Method: The European First Episode Schizophrenia Trial collected demographic, clinical andneurocognitive baseline data in 498 FE patients with minimal or no prior exposure toantipsychotics. Two-hundred-twenty healthy subjects (HS) were also evaluated. Neurocognitiveassessment included theReyAuditoryVerbal Learning Test; TrailMakingAandB, Purdue Pegboardand Digit-Symbol Coding.Results: Patients performed worse than HS on all tests (effect sizes from −0.88 to −1.73).Correlations with psychopathological dimensions were weak and involved reality distortion anddisorganization. The duration of untreated psychosis (DUP) was not associated with cognitiveimpairment. Subjects living alone had a better neurocognitive performance, while the occupationstatus did not reveal any association with cognition.Conclusions:Amoderate/severe impairment of processing speed, motor dexterity, verbal memoryand cognitive flexibility was found in the largest sample of FE patients analyzed so far. Theimpairment was largely independent from psychopathology and not associated with DUP.
© 2009 Elsevier B.V. All rights reserved.
Keywords:CognitionNeuropsychologyPsychopathological dimensionsAntipsychoticsDuration of untreated psychosisPsychosis
1. Introduction
Cognitive deficits are considered key features of schizo-phrenia, important determinants of poor psychosocial outcomeand targets for both pharmacological and nonpharmacologicaltreatment strategies (Green et al., 2004; Keefe, 2008; Kremenet al., 2004;Marder and Fenton, 2004). However, in spite of thehuge number of publications on cognitive impairment inschizophrenia, studies involving large cohorts of first episode(FE) patients are still scarce. Consistency between the cognitiveprofile observed in FE patients and the one reported inmultiepisode ones is debated (Braw et al., 2008). It is generallyagreed that cognitive deficits in FE patients involve severaldomains (attention, memory, executive functions and psycho-motor speed) and show a degree of severity ranging from0.5 to1.5 standard deviation below normative values (Addingtonet al., 2003; Bilder et al., 2000;Heydebrand et al., 2004;Hoet al.,2003). Discrepant findings, however, were also published,suggesting that someaspects of cognition (e.g., speed on simplereaction time tasks), generally impaired in adult/chronicpatients, may be within the normal range in the young/firstepisode ones (Braw et al., 2008; Kravariti et al., 2007; Oie et al.,1998; Pedersen et al., 2008; Rund et al., 1998).
A significant association between cognitive impairmentand negative symptoms has been more commonly reported(Ayres et al., 2007; Bilder et al., 2000; Heydebrand et al.,2004), but associations with positive symptoms or disorgani-zation were also found (Lucas et al., 2004; Rund et al., 2004).
A relationship with the duration of untreated psychosis(DUP)was found by some (Amminger et al., 2002; Lappin et al.,2007), but not all investigators (Heydebrand et al., 2004; Hoet al., 2003;Norman et al., 2001; Perkins et al., 2005; Rund et al.,2004). In these studies duration of the illness before cognitiveassessment is often not well defined (ranging up to five years);previous exposure to antipsychotic drugs is common and haslasted for more than six months in some instances (Ayres et al.,2007; Rund et al., 2004). Selection criteria excluding subjectswith substance abuse were important to differentiate theimpact of illness and of psychotropic substances on cognitiveimpairment. However, they also limit the generalisability ofstudy findings.
The European First Episode Schizophrenia Trial or EUFEST(Fleischhacker et al., 2005; Kahn et al., 2008), an openrandomized trial, involving registered antipsychotics and notexcluding subjectswith comorbidities, such as substance abuse,
collected demographic, clinical, psychosocial and cognitivebaseline data in a large cohort of first episode patients withschizophrenia, schizophreniform or schizoaffective disorder.For its characteristics, the study enabled the recruitment of afirst-episode sample more representative than those involvedin other studies.Data fromEUFESTmayclarify, in a large sampleof FE patients, hardly ever exposed to antipsychotics andrelatively unselected, the extent of impairment in key cognitivedomains and its relationships with demographic, psychosocialand clinical variables.
2. Materials and methods
2.1. Subjects recruitment and clinical evaluation
EUFESTwasdesigned to compareone-year retention rates ofpatients with first-episode schizophrenia, schizoaffective orschizophreniform disorder, treated with second-generationantipsychotics or low-dose haloperidol. Details of the entrycriteria have been presented elsewhere (Fleischhacker et al.,2005; Kahn et al., 2008). Patients included in EUFEST wererecruited at 50 sites in 13 European countries and Israel. Theywere 18–40 years of age and met the following inclusioncriteria: DSM-IV criteria for schizophrenia, schizoaffective orschizophreniform disorder, confirmed with the Mini Interna-tional Neuropsychiatric Interview Plus (MINI-Plus, Sheehanet al., 1998); first-episode psychosis with no more than twoyears elapsed between the onset of positive symptoms andrecruitment into the trial; previous use of antipsychotic drugsless than twoweeks during the preceding year and less than sixweeks lifetime, as assessed by interview of the patient and oneof his/her key relatives, as well as review of the availablemedical records. The trialwas conducted in accordancewith theDeclaration of Helsinki, Good Clinical Practice and nationalregulatory requirements. Patientswere assessed at baseline andthen randomly assigned via a centralized, computerized onlinerandomization system to open-label treatment with haloperi-dol, 1 to 4 mg/day, (N=103); amisulpride, 200 to 800 mg/day,(N=104); olanzapine, 5 to 20 mg/day, (N=105); quetiapine,200 to 750 mg/day, (N=104); or ziprasidone, 40 to 160 mg/day, (N=82). Mood stabilizers, benzodiazepines, antidepres-sants, and anticholinergics were allowed before and during thetrial. Additional antipsychotics were not permitted.
The current report relies on data gathered at baseline(between 4 weeks before and 1 week after randomization)

106 S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
for all clinical and demographic variables, while neuropsy-chological assessment was carried out when patients wereable to fully cooperate, either before randomization or withinthe following month. Of the 498 patients included in EUFEST,40 were missing baseline testing and 4 completed 2 or fewerof the 5 cognitive tests at baseline, and were thereforeexcluded from further analysis. The remaining 454 patientsincluded in the analysis had valid data and completed all tests(n=407) or at least 3 of the 5 neurocognitive tests (n=47).The sample analyzed in the present report (n=454) includesthe one described in Davidson et al (2009) dealing with theeffects of antipsychotic treatment on neurocognitive impair-ment (n=286).
Two-hundred-twenty healthy subjects, comparable withpatients for age, sex, race and parents education,were recruitedfrom the community, through flyers, in the countries contrib-uting to EUFEST. Exclusion criteria were: 1) a DSM-IV Axis Idiagnosis, as assessed with the Mini-Plus; 2) alcohol orsubstance abuse/dependence in the last year; 3) use ofpsychoactive drugs in the last two weeks; and 4) a first degreerelative with a psychotic disorder.
The Mini-Plus also allows the assessment of the Axis-IIantisocial personality disorder, which was not present in anysubject.
In each Country, the number of recruited healthy subjectswas proportional to the number of enrolled patients (e.g.,Romania 50 and 108, The Netherlands 11 and 20, respectively).
Demographic information included gender, age, race,current occupation, living status and education of subjectsand their parents. Recreational use of psychoactive substanceswas recorded and frequency and quantity scored. Baselinedata on diagnoses, present treatment setting and medicationhistory were recorded for patients. Psychopathological eval-uation included the Positive and Negative Syndrome Scale(PANSS, Kay et al., 1987), the Clinical Global Impression (CGI,Guy, 2000) and the Calgary Depression Scale for Schizophre-nia (CDSS, Addington et al., 1992).
An add-on study to assess the duration of untreatedpsychosis was started in the second year of the EUFEST study.All patients recruited from that time on (n=206) wereevaluated by the Symptom Onset in Schizophrenia (Perkinset al., 2000).
2.2. Neuropsychological assessment
A short neurocognitive test battery, focusing on processingspeed, motor dexterity, verbal memory and cognitive flexi-bility was used. Validated versions of the tests were availableand in commonuse in the countrieswhere the trial took place.
The following cognitive tests were administered:
The Rey Auditory Verbal Learning Test, a list learning task inwhich participants are read a list of words, and are thentested for what they have learned by recall. Six trials areadministered. Performance measures were the total numberof correctly recalled words in trials I to V (verbal learning)and in the delayed recall trial VI (secondary verbal memory)(Rey, 1964).
As in Bulgaria no officially validated translation of theRAVLT was available, this assessment was not carried out inthat Country.
Trail Making A & B, in which participants must first drawlines to connect consecutively numbered circles on one worksheet (Part A), and then connect the same number ofconsecutively numbered and lettered circles on another work-sheet by alternating between the two sequences (Part B). Theseare tests of complex visual scanning, motor speed and abilityto shift strategy (Reitan and Wolfson, 1993). Performancemeasures were the time to complete Part A and the Flexibilityindex (time to complete Part B–time to complete Part A).
The Purdue Pegboard, a task inwhichparticipantsmust placepegs in the holes of a board. It tests motor speed andmotor co-ordination and is sensitive to subtle motor dysfunction. Theperformancemeasure was the number of pegs correctly placedby the dominant hand within 30 s (Costa et al., 1963).
The Digit-Symbol Coding, a test in which the participant has120 s to move through a grid of 133 numbers (1 to 9) and pairthemwith the correct symbol by using a key consisting of ninesymbol-digit pairs. This test is part of the Wechsler AdultIntelligence Scale III (WAIS-III) andmeasures processing speed,symbolic representational abilities, visualmotor skill/dexterity,attention/concentration, visual perception of abstract stimuliand short-term visual memory. The performance measure wasthe number of correct symbols drawn within 120 s (Wechsler,1974).
The short cognitive battery ensures practicality of admin-istration for a large, multi-site, international, multi lingualantipsychotic clinical trial. Since lengthy testing is not alwaysacceptable to patients, the tests selected constitute a compro-mise between the comprehensiveness of the test battery andthe need to reduce the amount of missing data. The tests wereadministered at baseline and after 6 months of treatment(±3 weeks). In patients in whom the severity of psychosis atbaseline was such that cognitive testing was not feasible, thetesting could be postponed until the end of the first month ofthe trial. Tests were administered by psychologists andpsychiatrists trained at investigators meetings to administerthe specified tests. No formal assessment of the inter-raterreliability was deemed necessary, but previous experience inneuropsychological testing of schizophrenia patients wasrequired.
2.3. Statistical analyses
A preliminary assessment of data distribution revealed asignificant departure from normality for the time to completethe Trail Making test (both Part A and Part B) and for DUP.Individual values were then log-transformed to achieve anormal distribution. The transformed Trail Making valueswere inverted so that for all cognitive measures high scoresindicated better performance. All neuropsychological mea-sures were standardized to create Z-scores using the meansand standard deviations of the healthy control group.
Psychopathological ratings on PANSS items were com-bined to calculate three dimensions of schizophrenia symp-tomatology: psychomotor poverty, reality distortion anddisorganization, according to the method derived by Harriset al. (1999) (see also Lucas et al., 2004). Items summed tocalculate each dimension include: 1) blunted affect, emo-tional withdrawal, social withdrawal, poor rapport and lackof spontaneity for Psychomotor Poverty; 2) conceptual

107S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
disorganization, grandiosity, excitement and lack of abstractthinking for Disorganization; and 3) suspiciousness, delu-sions, hostility and hallucinatory behavior for RealityDistortion.
A preliminary descriptive analysis revealed that recrea-tional substances mostly used by both patients and controlsincluded tobacco smoking, alcohol and cannabis. For each ofthem the frequency and quantity were scored and werecompared amonggroups. For all other investigated substancesthe frequency of use in either group was unremarkable.
Groupcomparisons ondemographic and/or clinical variableswere carried out by means of Student t-test for independentsamples or Pearson χ2 as appropriate, with Bonferroni correc-tion for multiple comparisons.
Multivariate analysis of variance (MANOVA) on standard-ized test scores was used to investigate group differences oncognitive indices,with diagnosis (patients/controls) andgenderas between factors and neuropsychological test aswithin factor.Multivariate analysis of covariance (MANCOVA)was carried outto assess the effects of possible moderating variables, such asyears of education attained. As a further control for the effects ofage and years of education, a multiple regression analysis wascarried out on healthy controls test scores. The MANCOVA wasthen repeated on residual scores (i.e., the difference betweenthe observed scores and those predicted by subjects' age andeducation), with gender as a covariate.
Tukey's HSD procedure for unequal group size was usedfor post-hoc comparisons only when a significant main effector interaction had been found in the multivariate test.
Pearson's two-tailed testwasused to investigate correlationsbetween baseline cognitive indices and psychopathologicaldimensions or duration of untreated psychosis, with Bonferronicorrection for multiple comparisons. To control for the eventualinfluence of acute symptoms on correlations between neuro-cognitive indices and psychopathology, correlation analyseswere also carried out on data gathered at 6 month follow-up.
Associations between neurocognitive performance andpsychosocial functioning were investigated using the analysisof variance (ANOVA), with diagnosis and living or occupationstatus as grouping factors, neuropsychological test as withinfactor and test scores as dependent variable.
Multiple regression models were used to quantify theamount of variance in cognitive functioning explained bypsychopathological variables, after controlling for severalpotential confounders (e.g., smoking and substance use).
3. Results
3.1. Subjects
The 454 patients included in the analysis did not differ fromsubjects excluded on any demographic or clinical variable.
Among patients included in the analysis, 186 (40.97%)received adiagnosis of schizophreniformdisorder, 240 (52.86%)of schizophrenia and28 (6.17%) of schizoaffective disorder; 146(32.16%) were antipsychotic-naïve (AN).
At baseline 69 (15.19%) were receiving an antipsychotic,25 of them (36.23%) a first-generation antipsychotic (FGA)and 44 (63.76%) a second-generation antipsychotic (SGA), 25(5.51%) were on anticholinergic drugs, 129 (28.41%) receivedbenzodiazepines (55 among the AN), 5 (1.10%) antidepres-
sants (1 among the AN) and 6 (1.32%) mood stabilizers. Two-hundred fifty-four (54.4%) were smokers, 112 (24.7%) usedcannabis and 166 (36.6%) used alcohol. The mean duration ofuse was 9.8 (SD=5.8) months for tobacco, 7.0 (SD=4.8) forcannabis and 9.0 (SD=5.6) for alcohol.
3.2. Sociodemographic characteristics and substance use
Sociodemographic characteristics of patients and healthycontrols are reported in Table 1. The two groups did not differfor age, gender ratio, race (the majority of subjects wereCaucasian) and highest education level attained by subjects'parents. Patients were less educated, lived alone less fre-quently and fewer of them were employees or students withrespect to healthy comparison subjects (Table 1). A largerproportion of patients were smokers and used recreationaldrugs (Table 1). The number of cigarettes smoked per daywashigher in patients (t=4.89, DFs=612, p<0.000001), as wasthe daily use of cannabis (t=−2.86, DFs=612, p<0.0044).
3.3. Neuropsychological results
MANOVA revealedmain effects of diagnosis and gender andinteractions between these two factors and cognitive mea-sures; there was no interaction between gender and diagnosis(Table 2). Post-hoc tests revealed significant differencesbetween patients and controls on all cognitive indices (p valuesranging from 0.000018 to 0.000073). Results did not changewhen controlling for age and level of education, by bothcovariate and residual scores analyses (Table 2).
Mean raw scores and Z-scores for cognitive measures arereported in Table 3.Mean effect sizes (in z score units, reflectingthe number of standard deviations below the comparisongroup means) ranged from −0.88 to −1.73 (95% CIs from−1.85 to −0.77), with digit-symbol coding showing thelargest effect size. The same pattern was observed for theresidual scores: mean effect sizes ranged from−0.86 to−1.71(95% CIs from−1.83 to−0.75), with largest effect size for thedigit-symbol coding.
3.4. Effect of previous antipsychotic exposure on neurocognitiveimpairment
In order to control for previous exposure to antipsychotictreatment, aMANCOVAwas carried out on cognitivemeasures,including healthy controls and patients grouped as AN(n=120) or previously treated (n=282). Subjects with oneor more missing variables were excluded from the MANCOVAanalysis (26 AN and 26 previously treated patients). Asignificant effect of diagnosis (Hotelling t-square=0.82,F=40.69, DFs=12, 1198, p<0.000001) and a test×diagnosisinteraction (Hotelling t-square=0.17, F=10.44, DFs=10,1200, p<0.000001) were found. Previously treated patientsdiffered from healthy controls on all cognitive measures (post-hoc p from 0.00015 to 0.00004), while AN subjects differed onall measures (p from 0.04 to 0.00004), except the flexibilityindex (p=0.24). The two patient subgroups were not differenton any cognitive measure (p from 0.984 to 0.9999). Cognitiveprofiles are illustrated in Fig. 1.
The two patients subgroups did not differ in terms ofdemographic characteristics and alcohol or substance use

Table 1Demographic and clinical characteristics of the study sample.
Patients (N=454) Healthy controls (N=220) T or χ2 P
Sociodemographic characteristicsAge (years) 25.9 (5.6) 26.0 (5.4) −0.2 0.8410Women 181/454 (39.9%) 98/220 (44.6%) 1.3 0.2476White 429/454 (94.5%) 212/219 (96.8%) 3.8 0.2809Education (years) 12.4 (2.9) 14.3 (2.8) −7.9 0.000001 a
Highest parents'education level(professional training or better)
236/447 (52.8%) 124/220 (56.4%) 0.75 0.3848
Living alone 62/451 (13.7%) 72/220 (32.7%) 33.3 0.00001 a
Employed or students 211/454 (46.5%) 199/210 (94.8%) 141.7 0.0001 a
Inpatient status 408/454 (89.9%) – – –
Clinical ratings Mean (SD) rangePANSSTotal 87.98 (20.28) 36–187 – – –
Psychomotor poverty 14.85 (6.15) 5–32 – – –
Disorganization 9.79 (3.60) 4–23 – – –
Reality distortion 14.65 (3.93) 4–24 – – –
CDSS total 5.22 (5.01) 0–23 – – –
CGI score 4.82 (0.78) 2–7 – – –
GAF score 40.22 (13.38) 7–91 – – –
Alcohol/substance useSmoking 247/454 (54.4%) 72/220 (32.7%) 27.9 0.00001 a
Cigarettes/day 8.36 (10.36) 0–60 4.02 (6.58) 0–25 5.67 0.000001 a
Alcohol 166/454 (36.6%) 101/220 (45.9%) 5.4 0.02Glasses/week 2.53 (8.27) 0–99 1.70 (2.89) 0–15 1.44 0.15Cannabis 112/454 (24.7%) 10/220 (4.5%) 40.5 0.00001 a
Joints/week 0.44 (1.96) 0–30 0.01 (0.07) 0–0.7 3.21 0.001
Data are n/N (%) or mean (SD), unless otherwise indicated. Denominators change because of incomplete data. PANSS = Positive And Negative Symptoms Scale;CDSS = Calgary Depression Scale for Schizophrenia; CGI = Clinical Global Impression; GAF = Global Assessment of Functioning.
a Survived Bonferroni-correction (threshold p=0.0045). The absence of substance abuse or dependence in the last year was an inclusion criterion only forhealthy controls.
Table 2MANOVA and MANCOVA effects on neurocognitive indices.
Effect or interaction Hotelling t-SQR F DFs P
MANOVA main effects and interactionsDiagnosis 0.76 76.68 6, 602 0.000001Gender 0.06 6.44 6, 602 0.000001Diagnosis×gender 0.01 1.27 6, 602 0.268816Neurocognitive measure 0.17 20.70 5, 603 0.000001Neurocognitive measure×diagnosis 0.16 19.80 5, 603 0.000001Neurocognitive measure×gender 0.05 5.52 5, 603 0.000055Neurocognitive measure×diagnosis×gender 0.01 1.24 5, 603 0.287748
MANCOVA effects and interactionsYears of education 0.16 16.01 6, 601 0.000001Diagnosis 0.65 64.62 6, 601 0.000001Gender 0.06 6.12 6, 601 0.000003Diagnosis×gender 0.01 1.17 6, 601 0.321964Neurocognitive measure 0.04 4.93 5, 602 0.000199Neurocognitive measure×years of education 0.04 4.74 5, 602 0.000294Neurocognitive measure×diagnosis 0.16 19.80 5, 602 0.000001Neurocognitive measure×gender 0.05 5.97 5, 602 0.000021Neurocognitive measure×diagnosis×gender 0.01 1.22 5, 602 0.298261
Normative analysis on residual scoresDiagnosis 1.06 117.63 6, 664 0.000001Gender 0.01 0.60 6, 664 0.728850Diagnosis×gender 0.01 0.75 6, 664 0.607357Neurocognitive measure 0.09 11.55 5, 665 0.000000Neurocognitive measure×diagnosis 0.09 12.10 5, 665 0.000000Neurocognitive measure×gender 0.00 0.48 5, 665 0.788844Neurocognitive measure×diagnosis×gender 0.01 0.72 5, 665 0.606017
Residual scores=observed values−values predicted by subjects' age and education, based on regression analyses in healthy controls.
108 S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114

Table 3Mean raw and Z-scores on neurocognitive tests.
Scores for FE subjects Scores for HC subjects
Mean (SD) Z-score N 95% CI Mean (SD) n
Trail Making A (time) a −52.18 (34.86) −1.42 454 −1.54/−1.30 −27.87 (12.23) 218Flexibility Index (Trail Making B-A time) a −69.40 (73.29) −0.88 450 −0.99/−0.77 −33.29 (21.99) 218WAIS DC (total correct) 50.65 (19.56) −1.73 447 −1.85/−1.62 77.30 (15.37) 220Purdue pegboard (total pegs with dominant hand) 12.39 (2.81) −1.67 440 −1.80/−1.55 15.94 (2.12) 220RAVLT learning index (total correct on trials I–V) 42.65 (11.79) −1.12 431 −1.24/−1.00 53.16 (9.39) 211RAVLT secondary memory (total correct on Delayed Recall trial) 8.87 (3.49) −1.36 426 −1.49/−1.22 12.17 (2.43) 211
FE = First episode; HC =Healthy Controls; WAIS DC=Wechsler Adult Intelligence Scale Digit-symbol Coding; RAVLT = Rey Auditory Verbal Learning Test. CI =Confidence intervals.
a Trail Making A (time) and Flexibility index (Trail Making B-A time) were inverted so that higher scores indicated better performance as for all other tests.
109S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
(Table 4). Not naïve patients had a higher disorganizationscore and were more often hospitalized than naïve patients(Table 4). As a control analysis, a MANCOVA was carried outon neuropsychological indices with naïve and inpatient statusas grouping factors and disorganization score as covariate.Neither a significant effect of naïve or inpatient status(Hotelling t-square=0.03, F=1.90, DFs=6, 391, p<0.08;Hotelling t-square=0.01, F=0.80, DFs=6, 391, p<0.568,respectively), or a significant interaction test×naïve status ortest×inpatient status (Hotelling t-square=0.02, F=1.37,DFs=5, 392, p<0.2364; Hotelling t-square=0.01, F=0.74,DFs=5, 392, p<0.595, respectively) were found.
Fig. 1. Cognitive impairment in first episode patients with schizophrenia with limitedNeuropsychological measures were standardized to create Z-scores using the meanAdult Intelligence Scale Digit-symbol Coding; RAVLT = Rey Auditory Verbal Learniwere inverted so that higher scores indicated better performance as for all other te
3.5. Associations of neurocognitive impairment with psychosocialfunctioning and psychopathological variables
ANOVA showed a significant main effect of the living statuson neuropsychological performance (F=6.12, DFs=1605,p<0.01), but no significant interaction with the diagnosis(F=0.81, DFs=1605, p=0.3691). These results indicate thatsubjects living alone had a better neurocognitive performance,irrespective of the diagnosis. For the occupation status atbaseline, ANOVA did not show any significant effect (F=2.38,DFs=1595, p=0.1236) or interaction (F=0.40, DFs=1595,p=0.5274).
exposure to antipsychotic drugs (Not Naïve) or antipsychotic-naïve (Naïve).s and standard deviations of the healthy control (HC). WAIS DC = Wechslerng Test. Trail Making A (time) and Flexibility index (Trail Making B-A time)sts.

Table 4Demographic and clinical characteristics of not naïve and naïve patients.
Not naïve patients (N=308) Naïve patients (N=146) T or χ2 P
Sociodemographic characteristicsAge (years) 25.9 (5.6) 25.9 (5.6) −0.001 0.9991Women 129/308 (41.9%) 52/146 (35.6%) 1.6 0.1205White 291/308 (94.5%) 138/146 (94.5%) 2.1 0.5539Education (years) 12.4 (2.9) 12.6 (3.0) −0.97 0.3334Highest parents' education level(professional training or better)
153/303 (50.5%) 83/144 (57.6%) 1.99 0.0945
Living alone 40/307 (13.0%) 22/144 (15.3%) 0.42 0.3053Employed or students 138/308 (44.8%) 73/146 (50.0%) 1.1 0.1747Inpatient status 288/308 (93.5%) 120/146 (82.2%) 20.02 0.0001 a
Clinical ratings Mean (SD) rangePANSSTotal 89.93 (20.99) 39–187 84.51 (18.51) 36–137 2.65 0.0083Psychomotor poverty 14.96 (6.32) 5–32 14.62 (5.81) 5–28 0.54 0.5854Disorganization 10.16 (3.77) 4–23 9.01 (3.09) 4–17 3.20 0.0015 a
Reality distortion 14.96 (4.01) 5–24 13.99 (3.09) 4–17 2.47 0.0137CDSS total 4.82 (5.06) 0–23 5.83 (4.57) 0–21 −2.03 0.0425CGI score 4.83 (0.79) 2–7 4.80 (0.75) 2–6 0.38 0.7037GAF score 38.97 (13.51) 7–85 42.84 (12.75) 20 – 91 −2.89 0.0040
Alcohol/substance useSmoking 173/308 (56.2%) 74/146 (50.7%) 1.20 0.3198Cigarettes/day 8.60 (10.48) 0–60 7.87 (10.12) 0–50 0.70 0.4843Alcohol 100/308 (32.5%) 66/146 (45.2%) 6.93 0.01Glasses/week 2.26 (7.92) 0–99 3.10 (8.95) 0–90 −1.01 0.3122Cannabis 80/308 (26.0%) 32/146 (21.9%) 0.88 0.4123Joints/week 0.48 (2.28) 0–30 0.34 (1.08) 0–5 0.74 0.4572
Data are n/N (%) or mean (SD), unless otherwise indicated. Denominators change because of incomplete data. PANSS = Positive And Negative Symptoms Scale;CDSS = Calgary Depression Scale for Schizophrenia; CGI = Clinical Global Impression; GAF = Global Assessment of Functioning.
a Survived Bonferroni-correction (threshold p=0.0024).
110 S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
Pearson coefficients of correlations between PANSS scoresand cognitive measures are summarized in Table 5. Realitydistortion was negatively correlated with each cognitivemeasure, except Purdue Pegboard index; Disorganization wasweakly associatedwith learning/memory index andmarginallycorrelated with the flexibility index; no significant associationwas found between Psychomotor Poverty and cognitive scores.In antipsychotic-naïve subjects no association between psy-chopathological dimensions and cognitive indices survived theBonferroni correction, while subjects previously exposed toantipsychotics showed the same pattern observed in thewhole group (Pearson r ranging from −.24 to−.28 for Realitydistortion and from −.15 to −.16 for Disorganization).
3.6. Effect of acute psychotic state on associations betweenneurocognitive impairment and psychopathology
To rule out the possibility that correlations observed in oursample were due to an acute psychotic state interfering withpatients' performanceon cognitive tests, a correlational analysiswas also carried out in thepatient subgroupwho completed theneuropsychological evaluation at baseline and after 6 monthsof treatment when both psychopathological dimensions andcognitive performance had improved.
Patients who completed both the baseline and 6-monthtesting and thosewho completed only the baseline testing didnot differ on demographic, clinical or neuropsychologicalvariables (p values ranging from .11 to .90).
Reality distortion was associatedwithmost of the cognitiveindices both at baseline and at 6-month follow-up (Table 6).
Significant correlations after sixmonths of treatmentwere alsoobserved between cognitive indices and the other psychopath-ological dimensions (psychomotor poverty and disorganiza-tion), as reported in Table 6.
Treatment induced changes in psychopathology and cogni-tive scores for the same sample (n=286), data concerningtheir association, as well as raw scores for neuropsychologicalevaluation at baseline and 6-month assessments can be foundin Davidson et al. (2009).
3.7. Association of neurocognitive impairment with duration ofuntreated psychosis
In the subgroup of patients in which both the duration ofuntreated psychosis and neurocognitive functioning had beenevaluated, DUP (mean±SD=182.07±156.7 days, median130; range 1–691) showed no association with any cognitivemeasure (r from −0.001 to 0.093; p from 0.992 to 0.216).
3.8. Results of multiple regression analyses
Results of multiple regressions analyses are presented inTable 7. Gender, years of education and severity of realitydistortion were independently associated with cognitive func-tioning in this large sample of first episode patients, aftercontrolling for age, depressive symptomatology, tobacco smok-ing and cannabis use. The amount of variance explained by theseverityof realitydistortionwasonlymodest and ranged from3%(for the indices offlexibility and secondary verbalmemory) to 7%(for the index of visual scanning and motor speed).
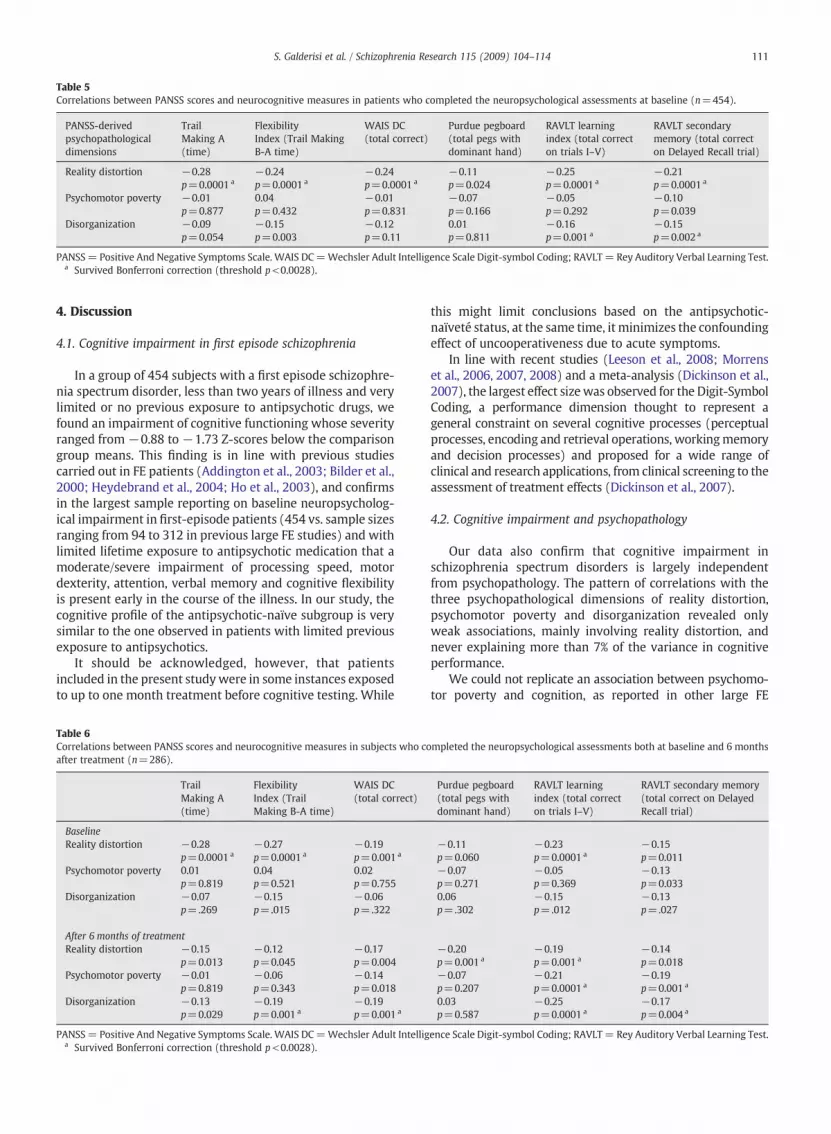
Table 5Correlations between PANSS scores and neurocognitive measures in patients who completed the neuropsychological assessments at baseline (n=454).
PANSS-derivedpsychopathologicaldimensions
TrailMaking A(time)
FlexibilityIndex (Trail MakingB-A time)
WAIS DC(total correct)
Purdue pegboard(total pegs withdominant hand)
RAVLT learningindex (total correcton trials I–V)
RAVLT secondarymemory (total correcton Delayed Recall trial)
Reality distortion −0.28 −0.24 −0.24 −0.11 −0.25 −0.21p=0.0001 a p=0.0001 a p=0.0001 a p=0.024 p=0.0001 a p=0.0001 a
Psychomotor poverty −0.01 0.04 −0.01 −0.07 −0.05 −0.10p=0.877 p=0.432 p=0.831 p=0.166 p=0.292 p=0.039
Disorganization −0.09 −0.15 −0.12 0.01 −0.16 −0.15p=0.054 p=0.003 p=0.11 p=0.811 p=0.001 a p=0.002 a
PANSS= Positive And Negative Symptoms Scale. WAIS DC=Wechsler Adult Intelligence Scale Digit-symbol Coding; RAVLT= Rey Auditory Verbal Learning Test.a Survived Bonferroni correction (threshold p<0.0028).
111S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
4. Discussion
4.1. Cognitive impairment in first episode schizophrenia
In a group of 454 subjects with a first episode schizophre-nia spectrum disorder, less than two years of illness and verylimited or no previous exposure to antipsychotic drugs, wefound an impairment of cognitive functioning whose severityranged from −0.88 to −1.73 Z-scores below the comparisongroup means. This finding is in line with previous studiescarried out in FE patients (Addington et al., 2003; Bilder et al.,2000; Heydebrand et al., 2004; Ho et al., 2003), and confirmsin the largest sample reporting on baseline neuropsycholog-ical impairment in first-episode patients (454 vs. sample sizesranging from 94 to 312 in previous large FE studies) and withlimited lifetime exposure to antipsychotic medication that amoderate/severe impairment of processing speed, motordexterity, attention, verbal memory and cognitive flexibilityis present early in the course of the illness. In our study, thecognitive profile of the antipsychotic-naïve subgroup is verysimilar to the one observed in patients with limited previousexposure to antipsychotics.
It should be acknowledged, however, that patientsincluded in the present studywere in some instances exposedto up to one month treatment before cognitive testing. While
Table 6Correlations between PANSS scores and neurocognitive measures in subjects who coafter treatment (n=286).
TrailMaking A(time)
FlexibilityIndex (TrailMaking B-A time)
WAIS DC(total correct)
BaselineReality distortion −0.28 −0.27 −0.19
p=0.0001 a p=0.0001 a p=0.001 a
Psychomotor poverty 0.01 0.04 0.02p=0.819 p=0.521 p=0.755
Disorganization −0.07 −0.15 −0.06p=.269 p=.015 p=.322
After 6 months of treatmentReality distortion −0.15 −0.12 −0.17
p=0.013 p=0.045 p=0.004Psychomotor poverty −0.01 −0.06 −0.14
p=0.819 p=0.343 p=0.018Disorganization −0.13 −0.19 −0.19
p=0.029 p=0.001 a p=0.001 a
PANSS= Positive And Negative Symptoms Scale. WAIS DC=Wechsler Adult Intelliga Survived Bonferroni correction (threshold p<0.0028).
this might limit conclusions based on the antipsychotic-naïveté status, at the same time, it minimizes the confoundingeffect of uncooperativeness due to acute symptoms.
In line with recent studies (Leeson et al., 2008; Morrenset al., 2006, 2007, 2008) and a meta-analysis (Dickinson et al.,2007), the largest effect sizewas observed for the Digit-SymbolCoding, a performance dimension thought to represent ageneral constraint on several cognitive processes (perceptualprocesses, encoding and retrieval operations, workingmemoryand decision processes) and proposed for a wide range ofclinical and research applications, from clinical screening to theassessment of treatment effects (Dickinson et al., 2007).
4.2. Cognitive impairment and psychopathology
Our data also confirm that cognitive impairment inschizophrenia spectrum disorders is largely independentfrom psychopathology. The pattern of correlations with thethree psychopathological dimensions of reality distortion,psychomotor poverty and disorganization revealed onlyweak associations, mainly involving reality distortion, andnever explaining more than 7% of the variance in cognitiveperformance.
We could not replicate an association between psychomo-tor poverty and cognition, as reported in other large FE
mpleted the neuropsychological assessments both at baseline and 6 months
Purdue pegboard(total pegs withdominant hand)
RAVLT learningindex (total correcton trials I–V)
RAVLT secondary memory(total correct on DelayedRecall trial)
−0.11 −0.23 −0.15p=0.060 p=0.0001 a p=0.011−0.07 −0.05 −0.13p=0.271 p=0.369 p=0.0330.06 −0.15 −0.13p=.302 p=.012 p=.027
−0.20 −0.19 −0.14p=0.001 a p=0.001 a p=0.018−0.07 −0.21 −0.19p=0.207 p=0.0001 a p=0.001 a
0.03 −0.25 −0.17p=0.587 p=0.0001 a p=0.004 a
ence Scale Digit-symbol Coding; RAVLT= Rey Auditory Verbal Learning Test.
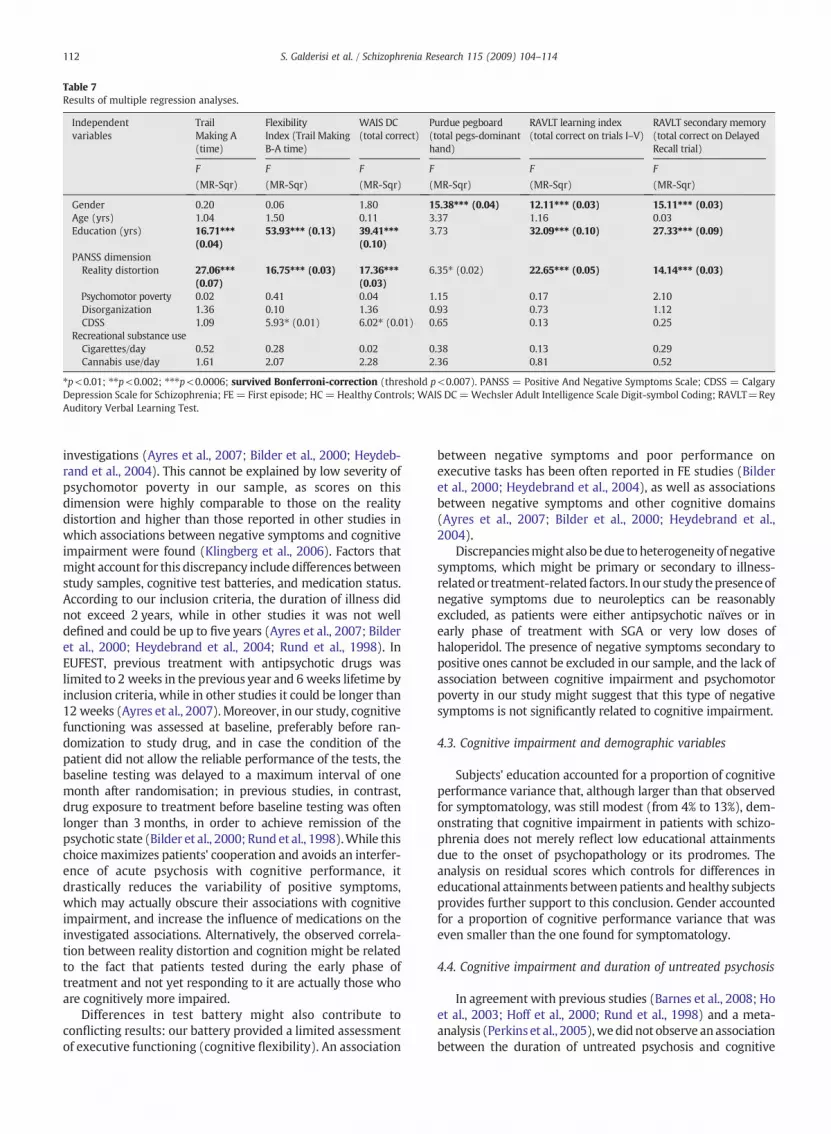
Table 7Results of multiple regression analyses.
Independentvariables
TrailMaking A(time)
FlexibilityIndex (Trail MakingB-A time)
WAIS DC(total correct)
Purdue pegboard(total pegs-dominanthand)
RAVLT learning index(total correct on trials I–V)
RAVLT secondary memory(total correct on DelayedRecall trial)
F F F F F F
(MR-Sqr) (MR-Sqr) (MR-Sqr) (MR-Sqr) (MR-Sqr) (MR-Sqr)
Gender 0.20 0.06 1.80 15.38⁎⁎⁎ (0.04) 12.11⁎⁎⁎ (0.03) 15.11⁎⁎⁎ (0.03)Age (yrs) 1.04 1.50 0.11 3.37 1.16 0.03Education (yrs) 16.71⁎⁎⁎
(0.04)53.93⁎⁎⁎ (0.13) 39.41⁎⁎⁎
(0.10)3.73 32.09⁎⁎⁎ (0.10) 27.33⁎⁎⁎ (0.09)
PANSS dimensionReality distortion 27.06⁎⁎⁎
(0.07)16.75⁎⁎⁎ (0.03) 17.36⁎⁎⁎
(0.03)6.35⁎ (0.02) 22.65⁎⁎⁎ (0.05) 14.14⁎⁎⁎ (0.03)
Psychomotor poverty 0.02 0.41 0.04 1.15 0.17 2.10Disorganization 1.36 0.10 1.36 0.93 0.73 1.12CDSS 1.09 5.93⁎ (0.01) 6.02⁎ (0.01) 0.65 0.13 0.25
Recreational substance useCigarettes/day 0.52 0.28 0.02 0.38 0.13 0.29Cannabis use/day 1.61 2.07 2.28 2.36 0.81 0.52
⁎p<0.01; ⁎⁎p<0.002; ⁎⁎⁎p<0.0006; survived Bonferroni-correction (threshold p<0.007). PANSS = Positive And Negative Symptoms Scale; CDSS = CalgaryDepression Scale for Schizophrenia; FE = First episode; HC = Healthy Controls; WAIS DC=Wechsler Adult Intelligence Scale Digit-symbol Coding; RAVLT=ReyAuditory Verbal Learning Test.
112 S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
investigations (Ayres et al., 2007; Bilder et al., 2000; Heydeb-rand et al., 2004). This cannot be explained by low severity ofpsychomotor poverty in our sample, as scores on thisdimension were highly comparable to those on the realitydistortion and higher than those reported in other studies inwhich associations between negative symptoms and cognitiveimpairment were found (Klingberg et al., 2006). Factors thatmight account for this discrepancy include differences betweenstudy samples, cognitive test batteries, and medication status.According to our inclusion criteria, the duration of illness didnot exceed 2 years, while in other studies it was not welldefined and could be up to five years (Ayres et al., 2007; Bilderet al., 2000; Heydebrand et al., 2004; Rund et al., 1998). InEUFEST, previous treatment with antipsychotic drugs waslimited to 2 weeks in the previous year and 6 weeks lifetime byinclusion criteria, while in other studies it could be longer than12 weeks (Ayres et al., 2007). Moreover, in our study, cognitivefunctioning was assessed at baseline, preferably before ran-domization to study drug, and in case the condition of thepatient did not allow the reliable performance of the tests, thebaseline testing was delayed to a maximum interval of onemonth after randomisation; in previous studies, in contrast,drug exposure to treatment before baseline testing was oftenlonger than 3 months, in order to achieve remission of thepsychotic state (Bilder et al., 2000; Rund et al., 1998).While thischoicemaximizes patients' cooperation and avoids an interfer-ence of acute psychosis with cognitive performance, itdrastically reduces the variability of positive symptoms,which may actually obscure their associations with cognitiveimpairment, and increase the influence of medications on theinvestigated associations. Alternatively, the observed correla-tion between reality distortion and cognition might be relatedto the fact that patients tested during the early phase oftreatment and not yet responding to it are actually those whoare cognitively more impaired.
Differences in test battery might also contribute toconflicting results: our battery provided a limited assessmentof executive functioning (cognitive flexibility). An association
between negative symptoms and poor performance onexecutive tasks has been often reported in FE studies (Bilderet al., 2000; Heydebrand et al., 2004), as well as associationsbetween negative symptoms and other cognitive domains(Ayres et al., 2007; Bilder et al., 2000; Heydebrand et al.,2004).
Discrepanciesmight also bedue toheterogeneity of negativesymptoms, which might be primary or secondary to illness-relatedor treatment-related factors. Inour study thepresenceofnegative symptoms due to neuroleptics can be reasonablyexcluded, as patients were either antipsychotic naïves or inearly phase of treatment with SGA or very low doses ofhaloperidol. The presence of negative symptoms secondary topositive ones cannot be excluded in our sample, and the lack ofassociation between cognitive impairment and psychomotorpoverty in our study might suggest that this type of negativesymptoms is not significantly related to cognitive impairment.
4.3. Cognitive impairment and demographic variables
Subjects' education accounted for a proportion of cognitiveperformance variance that, although larger than that observedfor symptomatology, was still modest (from 4% to 13%), dem-onstrating that cognitive impairment in patients with schizo-phrenia does not merely reflect low educational attainmentsdue to the onset of psychopathology or its prodromes. Theanalysis on residual scores which controls for differences ineducational attainments betweenpatients andhealthy subjectsprovides further support to this conclusion. Gender accountedfor a proportion of cognitive performance variance that waseven smaller than the one found for symptomatology.
4.4. Cognitive impairment and duration of untreated psychosis
In agreement with previous studies (Barnes et al., 2008; Hoet al., 2003; Hoff et al., 2000; Rund et al., 1998) and a meta-analysis (Perkins et al., 2005),wedidnot observe anassociationbetween the duration of untreated psychosis and cognitive

113S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
impairment, thus failing to support the hypothesis raised byLappin et al. (2007) that small sample size and small range ofillness severity (in our sample the PANSS total score rangedfrom 36 to 187) may explain previous negative findings. Thepossibility that the inclusion criterion of a two-year maximumlength of psychosis reduced the DUP variability, thus obscuringeventual relationships, cannotbe ruledout, although intuitivelyone would think that the shorter the duration of symptoms is,the more accurate the determination of DUP should become.
4.5. Cognitive impairment and substance use
Cannabis use and nicotine smoking were not associatedwith cognitive impairment in patients. EUFEST did not excludepatients with substance (ab)use, as we intended to gatherinformation on the influence that such substances may exert onclinical andcognitive aspects of schizophrenia spectrumpatients.Previous studies investigating this influence have reportedconflicting findings (Addington and Addington 1997; Cleghornet al., 1991; Pencer andAddington 2003; Serper et al., 2000; Sevyet al., 1990); however, most of them found no additionalcognitive impairment indrugabusers orno relationshipbetweendrug abuse and cognition (Addington and Addington 1997;Cleghorn et al., 1991; Pencer and Addington 2003; Rund et al.,2004). Discrepant findingsmight be due to the type of substanceused (for cocaine abuse an association is found more frequentlythan for alcohol or cannabis), to the age of subjects (a negativeimpact of substance abuse on cognition is generally found afterprolonged use, thus young subjects are less likely to showdetrimental effects) and to the level of abuse. In our sample,subjects were young, cocaine use was rare, and for both alcoholand cannabis the amount of substance used was not very high.
5. Conclusions
In conclusion, in a large sample of FE patients, with a shortduration of illness and limited exposure to drug treatment, thecomparisonwith a large groupof healthy subjects demonstratedthat amoderate/severe cognitive impairment is already presentearly in the course of the illness, involves several domains ofcognition, is largely independent frompsychopathology and hasno association with the duration of untreated psychosis.
Role of funding sourceThis work was funded by the European Group for Research in
Schizophrenia (EGRIS) with grants from AstraZeneca, Pfizer and Sanofi-Aventis. Neither the EGRIS nor any sponsor had any further role in studydesign; in the collection, analysis and interpretation of data; in the writing ofthe report; and in the decision to submit the paper for publication.
ContributorsAll authors participated in the conception and design of the study, in the
critical revision of the manuscript and provided the final approval of theversion to be published. SG and AM analyzed and interpreted the data anddrafted the manuscript.
Conflict of interestsSG received fees for educational programmes or advisory boards from
AstraZeneca, Innova-Pharma, Bristol-Myers Squibb, Janssen-Cilag.MD has received research grant support, travel support, speaker fees, or
consultancy fees from JNJ, Pfizer, Lundbeck, Teva, BioLineRx, Eli Lilly, Sanofi-Aventis, Roche, Servier, and Tangent Data.
RSK has received grants, honoraria for education programmes, or servedas consultant for Astellas, AstraZeneca, BMS, Eli Lilly, Janssen-Cilag, Pfizer,Roche, and Sanofi-Aventis.
AM received fees for educational programmes by AstraZeneca, Innova-Pharma, Bristol-Myers Squibb, Janssen-Cilag.
JKR has acted as a consultant or as a speaker for the following companies:Adamed-Poland, AstaZeneca, Bristol-Myers-Squibb, Eli Lilly, Janssen-Cilag,Lundbeck, Organon, Pfizer, Sanofi-Aventis and Servier.
JL has received speaker's honoraria, travel grants, or consultancy feesfrom Eli Lilly, Bristol-Myers Squibb, Lundbeck, and Servier. JL was a memberof the advisory boards of Eli Lilly and Bristol-Myers Squibb and he is a facultymember of the Lundbeck Institute (Lundbeck Neuroscience Foundation).
JJL-I ismemberof the scientific committee of Fundacion Lilly (Spain),Wyethmember of the global strategy consultant board, and board member of theLundbeck Neuroscience Foundation (LINF). He has attended several meetingsfinanced by Eli Lilly, Bristol-Myers Squibb, GlaxoSmithKline, and Lundbeck.
JP has received consultancy fees and research grants from and participatedin clinical trials sponsored by AstraZeneca, Sanofi-Aventis, Eli Lilly, Pfizer, andJanssen-Cilag.
LGH has received investigator's fees from Cephalon; speaker's honorariaform Bulgarian National Association of General Practicioners, Lundbeck, andEli Lilly; sponsorship for congresses from Bristol-Myers Squibb, Janssen-Cilag, Sanofi-Aventis, Lundbeck and Pfizer.
WWF has received research grants from BMS/Otsuka, Eli Lilly, Janssen-Cilag, and Servier; honoraria for educational programmes from AstraZenecaand Pfizer; speaking fees from AstraZeneca, BMS/Otsuka, Janssen-Cilag, andPfizer; and advisory board honoraria fromAstraZeneca, BMS/Otsuka, Janssen-Cilag, Servier, and Wyeth.
HB, MDG, SD had no conflict of interest.
AcknowledgmentsProf. Michail Gheorghe died on 28-03-2008 in a car accident.We thank all patients andhealthy volunteerswhoparticipated in the study.
References
Addington, D., Addington, J., Maticka-Tyndale, E., Joyce, J., 1992. Reliabilityand validity of a depression rating scale for schizophrenics. Schizophr.Res. 6 (3), 201–208.
Addington, J., Addington, D., 1997. Substance abuse and cognitive function-ing in schizophrenia. J. Psychiatry Neurosci. 22 (2), 99–104.
Addington, J., Brooks, B.L., Addington, D., 2003. Cognitive functioning in firstepisode psychosis: initial presentation. Schizophr. Res. 62 (1–2), 59–64.
Amminger, G.P., Edwards, J., Brewer, W.J., Harrigan, S., McGorry, P.D., 2002.Duration of untreated psychosis and cognitive deterioration in first-episode schizophrenia. Schizophr. Res. 54 (3), 223–230.
Ayres, A.M., Busatto, G.F., Menezes, P.R., Schaufelberger, M.S., Coutinho, L.,Murray, R.M., McGuire, P.K., Rushe, T., Scazufca, M., 2007. Cognitivedeficits in first-episode psychosis: a population-based study in São Paulo.Brazil Schizophr. Res. 90 (1–3), 338–343.
Barnes, T.R., Leeson, V.C., Mutsatsa, S.H., Watt, H.C., Hutton, S.B., Joyce, E.M.,2008.Durationofuntreatedpsychosis and social function:1-year follow-upstudy of first-episode schizophrenia. Br. J. Psychiatry 193 (3), 203–209.
Bilder, R.M., Goldman, R.S., Robinson, D., Reiter, G., Bell, L., Bates, J.A.,Pappadopulos, E., Willson, D.F., Alvir, J.M., Woerner, M.G., Geisler, S., Kane,J.M., Lieberman, J.A., 2000. Neuropsychology of first-episode schizophrenia:initial characterization and clinical correlates. Am. J. Psychiatry 157 (4),549–559.
Braw, Y., Bloch, Y., Mendelovich, S., Ratzoni, G., Gal, G., Harari, H., Tripto, A.,Levkovitz,Y., 2008.Cognition inyoungschizophreniaoutpatients: comparisonof first-episode with multiepisode patients. Schizophr. Bull. 34 (3), 544–554.
Cleghorn, J.M., Kaplan, R.D., Szechtman, B., Szechtman, H., Brown, G.M.,Franco, S., 1991. Substance abuse and schizophrenia: effect on symptomsbut not on neurocognitive function. J. Clin. Psychiatry 52 (1), 26–30.
Costa, L.D., Vaughan Jr., H.G., Levita, E., Farber, N., 1963. Purdue Pegboard as apredictor of the presence and laterality of cerebral lesions. J. Consult.Psychol. 27, 133–137.
Davidson, M., Galderisi, S., Weiser, M., Werbeloff, N., Fleischhacker, W.W.,Keefe, R.S., Boter, H., Keet, I.P.M., Prelipceanu, D., Rybakowski, J.K., Libiger,J., Hummer, M., Dollfus, S., López-Ibor, J.J., Hranov, L.G., Gaebel, W.,Peuskens, J., Lindefors, N., Riechler-Rössler, A., Kahn, R.S., 2009. Cognitiveeffects of antipsychotic drugs in first-episode schizophrenia and schizo-phreniform disorder: a randomised, open-label clinical trial (EUFEST).Am. J. Psychiatry 166, 675–682.
Dickinson, D., Ramsey, M.E., Gold, J.M., 2007. Overlooking the obvious: a meta-analytic comparison of digit symbol coding tasks and other cognitivemeasures in schizophrenia. Arch. Gen. Psychiatry 64 (5), 532–542.
Fleischhacker, W.W., Keet, I.P., Kahn, R.S., EUFEST Steering Committee, 2005.The European First Episode Schizophrenia Trial (EUFEST): rationale anddesign of the trial. Schizophr. Res. 78 (2–3), 147–156.
114 S. Galderisi et al. / Schizophrenia Research 115 (2009) 104–114
Green, M.F., Kern, R.S., Heaton, R.K., 2004. Longitudinal studies of cognitionand functional outcome in schizophrenia: implications for MATRICS.Schizophr. Res. 72 (1), 41–51.
Guy, W., 2000. Clinical Global Impressions (CGI) Scale. In: RushJr. Jr., A.J.,Pincus, H.A., First, M.B., Blacker, D., Endicott, J., Keith, S.J., Phillips, K.A.,Ryan, N.D., Smith, G.R., Tsuang, M.T., Widiger, T.A., Zarin, D.A. (Eds.),Handbook of Psychiatric Measures. American Psychiatric Association,Washington, pp. 100–102.
Harris, A.W., Williams, L., Gordon, E., Bahramali, H., Slewa-Younan, S., 1999.Different psychopathological models and quantified EEG in schizophre-nia. Psychol. Med. 29 (5), 1175–1181.
Heydebrand, G., Weiser, M., Rabinowitz, J., Hoff, A.L., DeLisi, L.E., Csernansky,J.G., 2004. Correlates of cognitive deficits in first episode schizophrenia.Schizophr. Res. 68 (1), 1–9.
Ho, B.C., Alicata, D., Ward, J., Moser, D.J., O'Leary, D.S., Arndt, S., Andreasen, N.C.,2003. Untreated initial psychosis: relation to cognitive deficits and brainmorphology in first-episode schizophrenia. Am. J. Psychiatry 160 (1),142–148.
Hoff, A.L., Sakuma, M., Razi, K., Heydebrand, G., Csernansky, J.G., DeLisi, L.E.,2000. Lack of association between duration of untreated illness andseverity of cognitive and structural brain deficits at the first episode ofschizophrenia. Am. J. Psychiatry 157 (11), 1824–1828.
Kahn, R.S., Fleischhacker,W.W., Boter, H., Davidson, M., Vergouwe, Y., Keet, I.P.,Gheorghe, M.D., Rybakowski, J.K., Galderisi, S., Libiger, J., Hummer, M.,Dollfus, S., López-Ibor, J.J., Hranov, L.G., Gaebel, W., Peuskens, J., Lindefors,N., Riecher-Rössler, A., Grobbee, D.E., EUFEST study group, 2008. Effective-ness of antipsychotic drugs in first-episode schizophrenia and schizo-phreniform disorder: an open randomised clinical trial. Lancet 371 (9618),1085–1097.
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The positive and negative syndromescale (PANSS) for schizophrenia. Schizophr. Bull. 13 (2), 261–276.
Keefe, R.S., 2008. Should cognitive impairment be included in the diagnosticcriteria for schizophrenia? World Psychiatry 7 (1), 22–28.
Klingberg, S., Wittorf, A., Wiedemann, G., 2006. Disorganization andcognitive impairment in schizophrenia: independent symptom dimen-sions? Eur. Arch. Psychiatry Clin. Neurosci. 256 (8), 532–540.
Kravariti, E., Morris, R.G., Rabe-Hesketh, S., Murray, R.M., Frangou, S., 2007.Comparative profile analysis of cognitive function in recent-onset andchronic patients with adolescent-onset schizophrenia. Schizophr. Res. 94(1–3), 240–244.
Kremen, W.S., Seidman, L.J., Faraone, S.V., Toomey, R., Tsuang, M.T., 2004.Heterogeneity of schizophrenia: a study of individual neuropsychologicalprofiles. Schizophr. Res. 71 (2–3), 307–321.
Lappin, J.M.,Morgan, K.D.,Morgan, C., Dazzan, P., Reichenberg, A., Zanelli, J.W.,Fearon, P., Jones, P.B., Lloyd, T., Tarrant, J., Farrant, A., Leff, J., Murray, R.M.,2007. Duration of untreated psychosis and neuropsychological functionin first episode psychosis. Schizophr. Res. 95 (1–3), 103–110.
Leeson, V.C., Barnes, T.R., Harrison, M., Matheson, E., Harrison, I., Mutsatsa, S.H.,Ron,M.A., Joyce, E.M.,2008. The relationshipbetween IQ,memory, executivefunction, and processing speed in recent-onset psychosis: 1-year stabilityand clinical outcome. Schizophr. Bull. Aug. 4 Electronic publication ahead ofprint.
Lucas, S., Fitzgerald, D., Redoblado-Hodge, M.A., Anderson, J., Sanbrook, M.,Harris, A., Brennan, J., 2004. Neuropsychological correlates of symptomprofiles in first episode schizophrenia. Schizophr. Res. 71 (2–3), 323–330.
Marder, S.R., Fenton, W., 2004. Measurement and treatment research toimprove cognition in schizophrenia: NIMHMATRICS initiative to supportthe development of agents for improving cognition in schizophrenia.Schizophr. Res. 72 (1), 5–9.
Morrens, M., Hulstijn, W., Matton, C., Madani, Y., van Bouwel, L., Peuskens, J.,Sabbe, B.G., 2008. Delineating psychomotor slowing from reducedprocessing speed in schizophrenia. Cogn. Neuropsychiatry13 (6), 457–471.
Morrens, M., Hulstijn, W., Sabbe, B., 2007. Psychomotor slowing inschizophrenia. Schizophr. Bull. 33 (4), 1038–1053.
Morrens, M., Hulstijn, W., Van Hecke, J., Peuskens, J., Sabbe, B.G., 2006.Sensorimotor and cognitive slowing in schizophrenia asmeasured by theSymbol Digit Substitution Test. J. Psychiatr. Res. 40 (3), 200–206.
Norman, R.M., Townsend, L., Malla, A.K., 2001. Duration of untreated psychosisand cognitive functioning in first-episode patients. Br. J. Psychiatry 179,340–345.
Oie, M., Rund, B.R., Sundet, K., Bryhn, G., 1998. Auditory laterality and selectiveattention: normal performance in patients with early-onset schizophrenia.Schizophr. Bull. 24 (4), 643–652.
Pedersen, A., Siegmund, A., Ohrmann, P., Rist, F., Rothermundt, M., Suslow, T.,Arolt, V., 2008. Reduced implicit and explicit sequence learning in first-episode schizophrenia. Neuropsychologia 46 (1), 186–195.
Pencer, A., Addington, J., 2003. Substance use and cognition in earlypsychosis. J. Psychiatry Neurosci. 28 (1), 48–54.
Perkins, D.O., Gu, H., Boteva, K., Lieberman, J.A., 2005. Relationship betweendurationof untreatedpsychosis and outcome infirst-episode schizophrenia:a critical review and meta-analysis. Am. J. Psychiatry 162 (10), 1785–1804.
Perkins, D.O., Leserman, J., Jarskog, L.F., Graham, K., Kazmer, J., Lieberman, J.A.,2000. Characterizing and dating the onset of symptoms in psychoticillness: the SymptomOnset in Schizophrenia (SOS) inventory. Schizophr.Res. 44 (1), 1–10.
Reitan, R.M., Wolfson, D., 1993. The Halstead–Reitan neuropsychological testbattery: theory and clinical interpretation, second ed. NeuropsychologyPress, Tucson.
Rey, A., 1964. L'Examen clinique en psychologie. Presses Universitaires deFrance, Paris.
Rund, B.R.,Melle, I., Friis, S., Larsen, T.K.,Midbøe, L.J., Opjordsmoen, S., Simonsen,E., Vaglum, P., McGlashan, T., 2004. Neurocognitive dysfunction in first-episode psychosis: correlates with symptoms, premorbid adjustment, andduration of untreated psychosis. Am. J. Psychiatry 161 (3), 466–472.
Rund, B.R., Zeiner, P., Sundet, K., Oie, M., Bryhn, G., 1998. No vigilance deficitfound in either young schizophrenic or ADHD subjects. Scand. J. Psychol.39 (2), 101–107.
Serper, M.R., Bergman, A., Copersino, M.L., Chou, J.C., Richarme, D., Cancro, R.,2000. Learning and memory impairment in cocaine-dependent andcomorbid schizophrenic patients. Psychiatry Res. 93 (1), 21–32.
Sevy, S., Kay, S.R., Opler, L.A., van Praag, H.M., 1990. Significance of cocainehistory in schizophrenia. J. Nerv. Ment. Dis. 178 (10), 642–648.
Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E.,Hergueta, T., Baker, R., Dunbar, G.C., 1998. The Mini-InternationalNeuropsychiatric Interview (M.I.N.I.): the development and validationof a structured diagnostic psychiatric interview for DSM-IV and ICD-10.J. Clin. Psychiatry 59 (Suppl 20), 22–33.
Wechsler, D., 1974. Wechsler Adult Intelligence Scale, revised edn. Psycholog-ical Corporation, San Antonio.
Related Documents









![Review Appointment attendance in patients with schizophrenia · 2020-07-17 · or secondary outcome measure in an interventional study [21–24,29]. Rates & correlates of appointment](https://static.cupdf.com/doc/110x72/5fb8572b0a2eef2a43127109/review-appointment-attendance-in-patients-with-schizophrenia-2020-07-17-or-secondary.jpg)

