coronaryheart.com November / December 200 Issue Building a Heart Centre + 2 Site Visits (UK & USA) - including the Mayo Clinic E M P L O Y M E N T UNITED KINGDOM IRELAND The Easy Read Cardiac Magazine “Now for Cardiologists!” Dr Simon Redwood - Guy’s & St Thomas’ Hospital Special Feature Interview Technological Advances in Lesion Assessment • Education “Subscribe online for your FREE Copy!!” Pacemaker Anatomy - Part 2 •

Coronary Heart #9 UK
Mar 25, 2016
Coronary Heart November / December 2007
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

coronaryheart.com
November / December 200�Issue �
Building a Heart Centre+ 2 Site Visits (UK & USA) - including the Mayo Clinic
November / December 200�Issue �
EMP
LO
YMENT
UNITED KINGDOM IRELAND
The Easy ReadCardiac Magazine“Now for Cardiologists!”
MMPP
LLOOMM
PPLLO
Dr Simon Redwood- Guy’s & St Thomas’ Hospital
Special Feature
Interview
Technological Advances in Lesion Assessment
•Education
“Subscribe online
for your
FREE Copy!!”
Pacemaker Anatomy - Part 2•

Mr Tim LarnerPrevious Cardiology
ManagerQualified Radiographer
Director / Chief Editor
Dr Simon Redwood Director St Thomas’ Hospital
Cath Labs
Chief Clinical Editor
Dr Richard Edwards Consultant Cardiologist
Newcastle General Hospital
Assistant Clinical Editor
Dr Rodney Foale Clinical Director, Surgery,
Cardiovascular Sciences and Critical Care
St Mary’s Hospital
Assistant Clinical Editor
Dr Peter O’Kane Cardiology SpR & Senior
Interventional FellowSt Thomas’ Hospital
Assistant Clinical Editor
Dr Divaka Perera Cardiology SpR
St Thomas’ Hospital
Assistant Clinical Editor
Dr Lucy Blows Cardiology SpR
St Thomas’ Hospital
Assistant Clinical Editor
Mr Stuart Allen Technical Head CRMSouthampton General
HospitalCRM Consulting Editor
Mr Ian Wright Technical Head EPSt Mary’s Hospital
EP Consulting Editor
Ms Voncile Hilson-Morrow CEO Baltimore/Washington
Division of HealthworksPrevious Director of Invasive
Cardiology at Washington Heart at the Washington Hospital Center
Management Consulting Editor
? ??
THE CARDIOLOGY PANEL OF EXPERTS™
OUR LINE-UP for 200�
Designed for the entire cardiology team including Cardiologists.
Various UK & Irish cardiologists give their opinion on one HOT topic each issue.Starting Edition 10 (Jan/Feb 2008)

Contents
CONTENTSNovember / December 200�
CORONARYHEART
CORONARY HEART ™ 3
04 Editorial
0� Latest News
0� Future
0� ECG Quiz +Online Forums
0� Interview‘Dr Simon Redwood - St Thomas’ Hospital’
12 Special Feature‘Building a Heart Centre’
1� Education‘Technological Advances in Lesion Assessment ’
26 Cardiac Site Visit‘Essex Cardiothoracic Centre, UK’
32 Cardiac Site Visit‘Mayo Clinic EP Department, Rochester, MN, USA’
36 Interview‘Mr Douglas Beinborn - Mayo Clinic, USA’
41 Education‘Pacing Anatomy (Part 2) Alternate Pacing Sites - The Atrium’
43 Events Diary & Employment
THIS EDITIONPage: 26
Page: 32
Page: 18

EDITORIAL
From the EditorDear Reader
I am writing this letter to let you know of some innovative changes that have been made by Coronary Heart for 2008. It has been 18 months since our fi rst edition and if you have been with us since the beginning you would be aware of how the magazine has developed and improved during that time.
Our expansion earlier this year into the massive USA market resulted in us publishing two separate versions; USA and UK/Ireland. Th is division has provided us with a major advantage over other publications in the sense we are able to utilise writers in both countries. Th e sharing of experiences and knowledge from both sides of the Atlantic has bought major benefi ts in management and staff education.
After receiving feedback from many of our readers we are introducing two new features in the UK/Ireland edition:
Cardiology Expert Panel: We speak with a variety of cardiologists and get their opinion of the latest hot topic aff ecting their industry.
Interviews: Interviewing a cardiologist and fi nd out their goals and passions, inside and outside the lab.
Additional cardiologist related themes will be implemented throughout the year, such as journal summaries, book reviews, and problem solving cases.
We are also pleased to announce the new Clinical Editor for the UK/Ireland version in 2008 is Dr Simon Redwood. Simon is Senior Lecturer/ Consultant Interventional Cardiologist and Director of the Catheter Labs at St Th omas’ Hospital in London. He is also Lead Clinician for Research and Development within the Directorate and a Council Member of the British Cardiovascular Interventional Society. Add to this several new SpR editors from the Trust and our other leading editors, we are confi dent in our ability to solve any challenge, and stay on top of current issues.
We look forward to working with you all. See you in the fi eld.
•
•
Disclaimer:Coronary Heart should never be regarded as an authoritative peer reviewed medical journal. Coronary Heart has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing articles obtained from various companies and contributors, it is not possible to confi rm the accuracy of all statements. Th erefore it is the reader’s responsibility that any advice provided in this publication should be carefully checked themselves, by either contacting the companies involved or speaking to those with skills in the specifi c area. Readers should always re check claims made in this publication before employing them in their own work environment. Opinions expressed by contributors are their own and not necessarily those of their institution, Coronary Heart Publishing Ltd or the editorial staff .
Coronary Heart Publishing Ltd145 - 157 St John Street
London, EC1V 4PYUnited Kingdom
Email: [email protected]: +44 (0) 207 788 7967
Fax: +44 (0) 207 160 9334
Visit us online at
www.coronaryheart.com
Director / Chief EditorTim Larner
Clinical EditorDr Rodney Foale
Consulting EditorsDr Richard Edwards
Ms Voncile Hilson-MorrowMr Ian Wright
Mr Stuart Allen
ADVERTISINGWendy Rose
Rose Media LtdEmail: [email protected]
CIRCULATION
2013 Cardiac Professionals
Copyright 2006 by Coronary Heart Publishing Ltd. All rights reserved.
Material may only be reproduced by prior arrangement and with due acknowledgment of
Coronary Heart Publishing.The publication of an advertisement or product
review does not imply that a product is recommended by Coronary Heart Publishing Ltd.
Tim LarnerDirector
- Tim Larner
COVER PHOTO (courtesy of Mayo Clinic): Th e Gonda Building. Part of the Mayo Clinic in Rochester, MN, USA
4 CORONARY HEART ™

What’s New?
LATEST NEWS
Hansen Continues International Growth
Since receiving both FDA and CE Mark clearance in
May 2007, Hansen Medical have installed a total of five Sensei™ Robotic Catheter systems in the United States and four in Europe. The installation sites include large teaching sites through to community hospitals because physicians of differing skill level are able to successfully employ this remote catheter navigation system within their practices.
As a bonus for Europe is the ability to provide robotic control of irrigated ablation catheter technology for atrial fibrillation. Hansen stated recently that “The combination of the Sensei system’s ability to accurately position
catheters at targeted cardiac anatomy along with the more effective lesions created by irrigated catheters should have a powerful effect on procedure outcomes.
At present Hansen Medical has two centers of excellence - The Cleveland Clinic, in Cleveland, Ohio, and St. Mary’s Hospital in London.
Visit www.hansenmedical.com for more information
Stereotaxis 93% Success Rate with Niobe
Data given at the recent European Society of Cardiology Congress
(ESC) in Vienna reported a 93% acute success rate in patients treated for atrial fibrillation (AF) with the Niobe® magnetic navigation system.
Dr Xu Chen, M.D., of the Rigshospitalet at the University of Copenhagen presented the findings from 42 patients with AF from which in 93% of these cases the pulmonary veins were fully isolated from the left atrium, eliminating the main cause of the arrhythmia. Each case took on average slightly less than 2 1/2 hours as Dr Chen guided the catheters with
the Niobe magnetic navigation system, controlled from his remote station adjacent to the procedure room. The average exposure time was less than ten minutes.
“We have performed more than 250 total cases with the Stereotaxis system,” said Dr. Chen. “The ESC presentation was based on our first series of complex ablations and since then we have performed an additional 68 complex cases. We have had zero complications, and fluoro time in the last 50 cases has dropped to five minutes
per procedure. Procedures with the Stereotaxis system are faster and far more precise than I could perform with my hands. We are incredibly happy with the system’s performance.”
Visit www.stereotaxis.com for more information
CAUTION: Some products within this magazine may be restricted to specific regional usage, and may not be available in your region. Always check with the manufacturer to determine availability.
Image courtesy Hansen Medical Inc.
Image courtesy Stereotaxis
CORONARY HEART ™ �

LATEST NEWS
What’s New?New ICD from Boston Gains CE Mark
Boston Scientifi c recently announced CE Mark approval
of its CONFIENT™ implantable cardioverter defi brillator (ICD), designed to treat sudden cardiac death (SCD).
Advantages:
An enhanced AV Search Hysteresis feature (reduces unnecessary right ventricular pacing)
Wireless capability (eliminates need for wand and speeds up follow-ups)
Th is device should be available soon for doctors in the UK. Th e device is not available for use in the USA.
•
•
Six Month Results for Triton Side-Branch Stent™
A couple of issues ago we mentioned the Triton Medical
Side-Branch Stent and showed you a diagram of how it worked. Now though the six month results are in from the fi rst in-man study.
Th e results were presented by Dr. Ralf Müller (Helios Heart Center, Siegburg, Germany) and Professor Patrick W.J.C. Serruys (Erasmus Medical Center, Rotterdam, the Netherlands) at the European Bifurcation Club Meeting in Valencia, Spain.
Th e Tryton Side-Branch Stent™
was used in conjunction with a standard drug eluting stent to treat 30 patients with coronary blockages involving large side-branches. After 6 months, none of the patients suff ered from side-branch restenosis.
Triton reported that the core laboratory quantitative analysis reported a late loss of 0.27 ± 0.42 mm in the side branch and 0.12 ± 0.47 mm in the main vessel.
“Th e Core Angiographic Data demonstrates that the hybrid approach, bare metal Tryton Side-Branch Stent used in conjunction with a standard drug eluting stent, provides the same type of restenosis reduction we have seen when drug eluding stents are used to treat standard lesions,” said Professor Serruys, Erasmus Medical Center, the Netherlands. “Th is is the fi rst time, I have seen such promising results in the treatment of bifurcation disease,” added Serruys.
Endeavor® Resolute Receives CE Mark
Medtronic was proud to announce recently they had achieved
the CE mark approval of their new Endeavor® Resolute DES. What makes this stent special? It uses a proprietary new biocompatible polymer called BioLinx ™. Th is polymer has the same biocompatibility as the Endeavor stent’s phosphorylcholine (PC) polymer which has the eff ect of extending the duration of drug exposure in the vessel.
Th e Endeavor® Resolute is not available in the United States.
For more information visit www.medtronic.com
Sonosite Releases New Ultrasound: The M-Turbo
With possibly the coolest name in the imaging industry, Sonosite
has just released their latest creation: Th e M-Turbo. As you would expect with a name like that the processing speed has been thrown into overdrive with a 16-fold increase which the company says ‘generates dramatic improvements in image quality by simultaneously running multiple advanced algorithms.’ An example of this is SonoADAPT™ Tissue Optimization which automatically adjusts imaging parameters depending
on the exam type, making it easier for any cardiologist to not worry about too many buttons to push.
Th e M-Turbo also off ers seamless connectivity for digital image export in a rugged, hand-carried product weighing less than 8 pounds.
Image courtesy Sonosite
6 CORONARY HEART ™

FUTURE
Cardiology in the Future
XTENT Results Very Promising
XTENT, Inc announced follow-up data from their CUSTOM
I and CUSTOM II single-arm prospective studies evaluating the safety and efficacy of its Custom NX® drug-eluting stent.
Custom I: is a 30-patient first-in-man study designed to evaluate the preliminary safety and feasibility of in-situ stent customization. Going for two years.
Custom II: is a 100-patient study designed to evaluate the safety and efficacy of Custom NX for the treatment of long and multiple lesions. Going for one year.
The results for both trials showed no new major adverse cardiac events (MACE), and the incidence of late stent thrombosis for patients treated with the Custom NX was zero percent.
Commercialisation of the Custom NX is expected to commence in Europe in late 2008.
Data from XTENT Inc, as reported at TCT 2008 in Washington, DC.
Stem Cell Advances in Spain
Cardiologists from the University Hospital of Navarre and the
Gregorio Marañón Hospital in Madrid have commenced clinical trials (Phase II) on fifty patients in order to test the efficacy of adult stem sell transplants within the hearts of patients whom have suffered a myocardial infarction and have ventricular dysfunction.
The difference from other studies is the implantation of the cells is via a catheter rather than the traditional open heart approach. The technique is as follows:
Extraction of myoblast cells via a biopsy of muscular tissue from the leg of the patient.
Researchers isolate the adult stem cells.
The cellular units are cultured for a month to obtain sufficient numbers
•
•
•
of cells for transplantation.
The cells are injected in and around the damaged areas of cardiac muscle using a special injection catheter.
One of the major requirements of this trial has been to ensure no other invasive techniques are used on the patients to give more accurate results.
So how do the Cardiologists know where to inject the stem cells?
They use a navigation system known as non-fluoroscopic electroanatomical mapping (CARTO System). This technique is commonly used in EP whereby a three-dimensional reconstruction of the left ventricle provides information relating to the electrical activity anatomically. Where there is no electrical activity, this corresponds with an area of myocardial infarction.
The catheter that is used to inject the stem cells is made up of a very fine
•
needle retractable at its end. The catheter is placed via the femoral artery and once in the left ventricle between 15 and 20 injections of myoblasts are placed. The procedure normally takes between three to four hours to complete.
The aim of the trial is to see if this new treatment is effective and to improve on the cardiac function of patients who have suffered a heart attack.
1-Year Data on Bioabsorbable DES (ABSORB)
Abbott announced today the one-year results from the first
30 patients in their ABSORB trial which is evaluating the safety and performance of a fully bioabsorbable DES. The results demonstrated no stent thrombosis and a low major adverse cardiac event (MACE) rate at 12 months (1 patient, 3.4%, n=29), with no additional MACE, including no re-treatment of a diseased lesion (ischemia-driven target lesion revascularization) since six months for patients who received a bioabsorbable stent. The overall MACE rate in the ABSORB trial at six months was 3.3%, as previously announced in March 2007, with late loss of 0.44mm.
Data obtained from Abbott Vascular, as reported at TCT 2008 in Washington, DC.
Image courtesy Clínica Universitaria. Universidad de Navarra
CORONARY HEART ™ �

ECG Quiz Compiled by: Mr Stuart Allen, Technical Head CRM, Southampton General Hospital, UK
ECG + FORUMS
Website Latest
Online Forums
� CORONARY HEART ™
Cath Lab Forum: D2B
rnaden1 wrote:Hi Cath Lab friends,I am looking for info on door to balloon times for pts and staff. If you established d2b, what are your protocols. I have read that some hospitals have done d2b, but stopped. Thanks Roberta
Respond online
Radiography (RT) Forum: Equipment
ferretpants wrote:I am interested to know what Cardiac cath lab x-ray equipment people are using? Are you happy with it and why/why not?
Respond online
For these and many more questions visit our
FORUMS page on the website at
www.coronaryheart.com
It is free to browse, free to login, and free to post. Join our international community now!!
CLUE:
Patient was admitted for a
non cardiac surgical procedure and reported occasional palpitations. A pacemaker check was requested as a result of this ECG. Patient has a dual chamber pacemaker (implanted 18thms ago). Last pacemaker check 6 months ago was normal.For the answer please visit www.coronaryheart.com and click on Education
Cardiac Nursing Forum: Contrast allergy - what do you do?
veitch57 wrote:I guess we usually aim for steroids and antihistamines. Some go for the night before for steroids if possible. Hmm there is debate about using Omnipaque or Visipaque. Some say either. Both have iodine in them of course so i suspect no difference, I must ask around to see what is the best.
Respond online
� CORONARY HEART ™

INTERVIEWUNITED KINGDOM
CORONARY HEART ™ �
Why did you decide to become an Invasive Cardiologist?
I had a ‘Cardiological upbringing’ which I guess stimulated some interest but when I qualified I was most interested in surgical specialties - I was eventually put off by the FRCS exam (I was never any good at anatomy, except certain bits, but that’s another story….!).
I then decided to do a couple of years of general training with a plan to work in a rural hospital in Africa where I had spent my elective, and at the time the best way to do that was to do a GP training scheme – I applied for several but didn’t get shortlisted for any, so that ended that idea…!
Following an A&E job, I managed to get a 3 year SHO/Reg Medical rotation at the Royal London Hospital which included a lot of Cardiology and realised that it really was what I was interested in.
It was in the early days of angioplasty
and I was fascinated by the prospect of what was a very rapidly developing specialty. The prospect of being able to treat coronary stenoses by anything other than bypass surgery was incredible at the time.
Where did you train?
I went to Medical School at St George’s in sunny Tooting and trained in Cardiology at The Royal London, The Royal Free, St George’s, The Washington Hospital Center and Guy’s and St Thomas’.
What are some of your career highlights?
The early days of stenting were very interesting – at that time, emergency bypass surgery was needed in over 5% of cases and being able to treat dissections with a stent was very novel. I remember presenting one of Dr David Lipkin’s cases at a Grand Round at the Royal Free in 1990 in which we had stented a right coronary using a hand-crimped Palmaz-Schatz
stent. I had diazo slides made and still images where you couldn’t really see anything. Apparently there was a new program called Powerpoint but none of us had it! Nevertheless, the audience were amazed at the case. In those days, of course, patients would stay in for days being intensively anticoagulated with heparin and Dextran overlapping with warfarin for several days. What we didn’t realise was that by giving warfarin we were actually increasing the risk of stent thrombosis!
My most enjoyable and valuable time as a trainee was the time I spent at The Washington Cardiology Center. I was fortunate to learn from some great angioplasty operators (Marty Leon, Kenny Kent, Lowell Satler and Gus Pichard) at a very high volume centre – we used to start in the lab at 6.30am, which took a but of adjusting too! All patients had IVUS, and devices such as the Rotablator, laser, TEC, and directional atherectomy were used on a daily basis, and most patients were in research protocols. I don’t think I realised at the time how lucky I was to be exposed to that environment.
Interview: Dr Simon Redwood
MB BS MD FRCP FACC FSCAI
Senior Lecturer/ Consultant Interventional Cardiologist and Director of the Catheter Labs at St Thomas ‘ Hospital, London.
Honorary Treasurer and Council Member of the British Cardiovascular Interventional Society.
Editorial Board Member for the journal Heart.
Commencing 2008: New Clinical Editor for Coronary Heart.
•
•
•
•
>>CORONARY HEART ™ �

INTERVIEW
Dr Simon Redwood Interview (cont...)
What is your most interesting case?
Difficult question!! I know it sounds a bit sad, but I find most cases interesting, but over the years have been involved in some great cases, both at St Thomas’ and elsewhere.
I was transmitting a case from Glasgow to Advanced Angioplasty a couple of years ago – the patient had a tight calcified distal left main stenosis involving LAD and circumflex which I planned to rotablate. She also had severe right coronary disease which was meant to be treated the day before, but they failed! About 20 mins before we went ‘live’, as I was putting in the sheaths, she got severe chest pain, ST changes and hypotension! After high-dose Immodium and bicycle clips, I put in a balloon pump and rotablated the Circumflex and LAD. By the time we went live she was well and pain free - I don’t think many in the audience realised how much she had tried to die (most were having their lunch at the time!). To top it all, her surname had a similar sounding to “Grotty”, which was very apt given the state of her coronaries!!
What do you believe will be the biggest change in interventional cardiology within the next 5-10 years?
In such a fast moving specialty it’s a bit difficult to predict – if you look back over the last 5-10 years, we had loads of developments, such as Percutaneous Myocardial Revascularization (PMR), brachytherapy, numerous novel stent designs, drug eluting stents, etc.
I think the glory days for angioplasty are over – it is becoming such a common, routine and often outpatient procedure, and the ‘push’ in the UK is for it to be performed ‘locally’
in DGH’s – I don’t entirely agree, having seen so many unexpected complications but I can see the driving force for change. Having said that I could tell you where I would have my angioplasty!!
I think the limitations of angioplasty will become clear once trials such as SYNTAX, CARDia and FREEDOM are reported.
Over the next few years, I think there will be an explosion in structural heart disease developments, in particular percutaneous aortic valve replacement and mitral valve repair.
In the USA, cardiac CT is becoming common with many cardiologists taking specific courses to learn this new modality. The uptake in the UK seems to be a lot slower. Why do you think this is?
In the private sector, cardiac CT has an important role in screening high risk, but apparently asymptomatic, people. The trouble is – what do we do with a high calcium score without symptoms??? At the moment, it doesn’t really have a major role in an NHS setting, which is why I think it hasn’t really taken off in the UK. Having said that, cardiac CT/ MRI is a rapidly developing sub-specialty and will ultimately find its place in non-invasive testing of patients deemed to be high-risk and in patients with known ischemic heart disease (IHD) and recurrent symptoms.
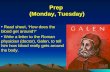
Drug Eluting Stents have been given some bad press lately. What is your opinion, and would you prefer to have a DES or a bare metal stent if you were on the table?
Dr Simon Redwood using a Rotablator at St Thomas’ Hospital
10 CORONARY HEART ™

INTERVIEW
Th ey have received bad press, but to some extent it’s been a bit unfair. We suspected from day one that there was a downside to ‘abolishing’ late loss, and that worry has been realised with a small, but probably signifi cant, increased risk of late stent thrombosis. Th is has made everyone, probably appropriately, to reconsider whether all patients really need DES.
We have to remember that BMS, if properly deployed, will result in restenosis in ‘only’ about 10-15%, which means that 85-90% will remain well. Having said that, DES certainly reduce that risk. Th e key is to recognise which patients are likely to have a recurrence.
Despite the controversy, depending on the lesion characteristics, I would be happy to have a DES, but would also be happy to remain on aspirin and clopidogrel for quite a while!
As the Director of one of the busiest cath labs in the UK, what advice can you give other cardiologists for them to improve workfl ow and enhance their labs positioning in a competitive market?
Working in the cath labs is very much a team based approach and it is very important not to forget the importance of the booking offi ce staff , nurses, radiographers, techs, porters, ward nurses, admin support, etc etc etc. It takes good coordination of everyone to keep workfl ow going – everything can fall down if any one part fails – maintaining motivation is important, and working in a happy environment really helps – in that respect, I am very fortunate at St Th omas’.
Th e competition has certainly changed over the years with a push for patients
to have their procedures locally, as I mentioned earlier. Th ere are still many patients who require more back-up for their procedure and we need to focus on them. I don’t think high risk and complex cases should be performed in a low volume centre, but not everyone agrees with me! In addition, I think there is a great need to increase the amount of research we do into new devices and techniques (for example percutaneous valve repair and replacement), and this is likely to be concentrated in the larger centres, and the reduction in workload should be seen positively as a way of facilitating this.
St Th omas’ recently underwent the installation of new imaging equipment and adjustments to the room design in Lab 5. What was your role during the planning stages?
I was involved in the planning but to be honest, the bulk of the work was done by the radiographers! Th e imaging equipment is so good now that there is little to choose between the main competitors. Sometimes the equipment is too good – it’s frightening to think what we got away with 15 years ago when we couldn’t really see what we were doing!
You are the Head of the Coronary Disease Research Centre. Please explain what this is and how others can be involved?
I have a great interest in clinical research and have spent the last seven years since being appointed trying to build up a research infrastructure at St Th omas. It’s been an uphill struggle but we now have dedicated offi ce space and some excellent and well motivated
research staff . Our ideal aim would be that most patients going through the cath lab were involved in one research study or another, whether it be a commercial study looking at a new stent or technique, or a study as part of a higher degree for one of the research fellows.
As a period of research is (in my view) an essential part of Cardiology training, we are always looking to take on research fellows. Funding for clinical projects has always been an issue but we are now getting to the stage of good support from the Interventional companies and organisations such as the British Heart Foundation. Broadly speaking, our interests are in the fi eld of coronary and myocardial physiology in ischaemic heart disease and we have performed a number of cath lab based studies on, for example, coronary collateral function, ischaemic pre (and post) conditioning, myocardial resistance during ischaemia, etc.
For more information about the Coronary
Disease Research Centre, the various studies
undertaken, and how you can be involved visit the
interactive website at:www.angioplasty.org.uk
CORONARY HEART ™ 11

SPECIAL FEATURE
Many people build a new home. When they do so, they decide what is
important to them and what makes them comfortable. Design generally takes into account what the person or family enjoys or how time is spent. Many questions abound: How many bedrooms? How should we plan the living spaces? What about the kitchen, patio, den and so on? At The University of Kansas Hospital, we followed the same process in building the Center for Advanced Heart Care, a facility dedicated to heart care and heart surgery.
The process of designing and building any structure typically involves working with consultants, architects and construction teams. What made our project different were the careful consideration of each patient area and how they work together, as well as a focus on staff satisfaction and retention, patient comforts, and convenience and caring for both groups.
Only the Beginning
First, the process to determine the right size for the Center for Advanced Heart Care began. A consultant helped determine what would be best for our
organization and our program. Our Business and Strategic Development Department worked carefully to determine capacity projections for both the inpatient and outpatient areas, including the cardiovascular (CV) labs and cardiovascular operating rooms (CVORs).
The architectural firm RTKL, of Dallas, Texas, was chosen through a request for proposal process, as was the nationally recognized, local construction company J.E. Dunn. Owner’s Representative Services, Inc. joined the team to provide construction project management, and the design process was well on its way.
Thoughtful and Functional Design
Right away, the hospital’s clinical and administrative teams had to ask themselves: What is most important for our heart center and our heart program?
Of course, exceptional patient care and safety together are the top priorities. Following closely from an organizational point of view are family and visitor comforts and staff workflows, conveniences, efficiencies
Building A HeartCentreA facility dedicated to heart care
and surgery, as well as outstanding patient outcomes and experiences.
- By Elizabeth Clark, Clinical Director, Cardiovascular Services,The University of Kansas Hospital
12 CORONARY HEART ™

Building A HeartCentre
One of America’s Top Heart Hospitals
- US News & World Report
The University of Kansas Hospital Center for Advanced Heart Care
CORONARY HEART ™ 13

SPECIAL FEATURE
Building A Heart Centre (cont...)
14 CORONARY HEART ™
and comfort. The intention was to provide a great environment in which all staff is supported to provide exceptional patient care.
Design decisions were driven using the guidance of our organizational pillars of quality, service, people, cost and growth. Quality outcomes and care are most important, of course. Design that allowed for superior service, from curbside to bedside, and patient satisfaction were always taken into account. Satisfaction and retention of nursing staff, physicians and other support/ancillary staff were also considered in workflow designs. We determined that the facility should allow for program expansion and growth, so design decisions needed
to be based on that. And, of course, we had to consider how design, flow and equipment selection could be cost efficient and long lasting.
Our internal clinical design team, composed of clinical staff, including nurses and physicians, began meeting with the RTKL architects in 2003. A general scheme had been developed; however, the clinical team provided essential information to create thoughtful and functional patient care areas. Throughout the process, the focus continued to be on patient care and safety, along with efficiency of that care for both nursing staff and physicians.
From the beginning, we determined
it was very important to provide staff respite areas/lounges with generous square footage, natural light and amenities. Staff lounges for five of the seven units in our heart center are located on the corner of the building, providing wonderfully big, beautiful, light-filled areas. All of the lounges contain many staff conveniences that offer some relaxation and rejuvenation as staff members continue to provide great care to patients. We also chose to make the staff areas calm and quiet, providing comfort to those who provide so much comfort to others.
Staff support was and remains an important aspect of the Center for Advanced Heart Care. Early in the process, space was set aside for
The Foyer:The colourful hanging sculpture is called a PulseFlow composed of more than 300 pieces of blown glass.

SPECIAL FEATURE
CORONARY HEART ™ 1�
physician and support staff work areas, and they were designed into each patient care area. These work areas provide computers, phones and storage space in quiet, private locations.
A Focus on Patient Care and Comfort
We paid considerable attention to all patient rooms. Clinical staff made significant contributions to the design, resulting in space that makes sense to staff as they provide care. Patient rooms also feature family areas or zones for family and visitor comfort. Small workspaces with computer access and in-room sleeper sofas are included. There are also six guest suites on the inpatient progressive care units. Suites include attached guest areas for greater privacy, as needed.
A beautifully planned education area for families and patients, located on the second floor, was included to serve as a significant learning and support resource for all patients and families.
Additionally, spaces were specifically planned for the display of art, adding to the building’s beautiful, healing atmosphere. The magnificently spacious entrance to the Center for Advanced Heart Care is filled with light and beauty; natural light and a hanging glass sculpture create a soothing, healing space.
Easy wayfinding also was incorporated into design. Specific colors identify each floor, and related art identifies space, such as waiting areas.
As the design process continued, patient care areas were painstakingly reviewed unit by unit. Another important consideration that upheld the guiding principle of patient safety was the consistency of units from floor to floor. Nurse work areas are similarly
stocked and organized throughout the facility. Universal placement and design allow for safer and more consistent patient care. This concept also allows for physician efficiencies, reducing rounding time spent looking for forms, charts, etc.
An overall look at all areas ensured appropriate and efficient patient care and workflows between areas. All work- and patient flows were specifically detailed and diagramed to ensure that the intended designs would work in practice. These flow diagrams were also used extensively in orientation training for the facility.
Early in the planning, we decided that nursing and supportive care would be decentralized. This meant designing the nurse work areas so they are within steps of the patient beds, allowing nurses to easily see patients and stay close to keep them safe. Architects worked with the clinical team to draw sight lines from each patient’s room to various areas on the unit, ensuring visual lines of sight into each patient’s room from multiple points on the unit
No patient rooms were tucked away out of a nurse’s or other care provider’s sight.
Another of our priorities was to eliminate unnecessary steps for staff to obtain supplies, medications and other patient care items. As a result, plans called for necessary supplies, materials and medicals records to be located at workstations just outside of each patient room. Computers, phones, medications and supplies are only a few steps away from patients. Close-by nutrition centers store the supplies that could not be kept at workstations, including clean supplies and additional medications.
Designing for Advanced Services
Other important aspects of most heart programs were taken into consideration. For example, door-to-balloon time, a performance improvement initiative, is closely monitored. To continue ensuring the ease and speed of care delivery, we
The Foyer:The use of natural light creates a relaxing environment for patients.

SPECIAL FEATURE
Building A Heart Centre (cont...)
16 CORONARY HEART ™
carefully designed a plan for moving patients from ambulance, helicopter or the Emergency Department to the catheterization lab in reduced time. A new state-of-the-art Emergency Department was designed and built on the first level of the Center for
Advanced Heart Care, allowing us to improve door-to-balloon times and quickly transport patients to our cardiac catheterization labs or to the chest pain center, when appropriate.
Also important to the design was the
close proximity of patient care areas. For example, on the second level, which houses the cardiac catheterization and electrophysiology (EP) labs, the floor was laid out to include the labs, the Cardiovascular Treatment and Recovery (which is a prep and recovery area) and the Cardiac Intensive Care Unit. This permits the availability of RNs with a wide scope of competencies (ICU, recovery and procedural), immediate physician availability and ease of movement from one area to another. These efficiencies provide a service-orientation to physicians and patients, along with continued focus on patient care and safety. Help is never far away.
The same concept applies to the cardiothoracic surgery floor. The CVORs and the Cardiothoracic Surgery ICU are housed on a single floor, again providing access to critical care and surgical nurses and to surgeons and anesthesiologists. This floor also has a satellite pharmacy, which serves the CVORs and all ICUs in the heart center and prepares all stat medications for the entire facility.
Cath Lab Floor Plan
Cardiology Inpatient Floor Plan

SPECIAL FEATURE
CORONARY HEART ™ 1�
Cardiac catheterization and EP labs and CVORs are challenging and innovative areas for design. The CV labs, which include the cardiac catheterization and EP labs and the CVORs are big, remarkable areas with state-of-the-art equipment and nurse-designed workstations. The layout was planned with significant physician and staff input. To minimize time spent running for an item, some supply storage is inside the CV labs, as well as a larger stock area.
Equipment selection, a tricky endeavor, could be described in an article of its own. Again, physician input is critical, as is having team members who are well versed or researched in the various equipment and options. It is also important to have someone who is very comfortable with negotiations and contracts. Many questions must be asked to make wise, cost-conscious decisions.
Opening the Heart Center
Design and construction soon were completed. The task of moving in, occupying and opening units, and making them operational soon became the focus of the clinical team. That successful accomplishment is also a story unto itself, for another day.
The University of Kansas Hospital’s Center for Advanced Heart Care opened in October 2006. The major project required the help of hundreds of people – design team, staff, community members, patients and families. We are very proud of our facility. It is a place where excellent, quality care continues to be delivered by a dedicated, committed and caring team. And the quality of care will remain at the heart of its existence.
Patient Rooms:Every patient has a private room, and most have wireless internet access.
Decentralized Nursing Stations:Allowing nurses to be only steps away from their patients.
The University of Kansas HospitalCenter for Advanced Heart Care3901 Rainbow Blvd.Kansas City, KS 66160United States of America
Names and titles from left to right:Mike Kaiser - PA, Shirley Verbenec - CV OR, Lynette Patocka - CV OR, Zann Roach - EP Lab, Chris Buckley - CTS ICU, Lynn Smith - Cath Lab,
Annie Burger - CTS PCU, Kathy Carson - CTS ICU, Gail Schuman - CV Pre/Post, Kate Jones - CTS Nurse Clinician, Andy Hawthorne - CTS ICU,
Anna Werner - CTS PCU

EDUCATION
Technological Advances in Lesion Assessment
For over thirty years, cardiologists and technologists have been looking up at the cardiac cath
lab angiography screen and asking each other, “What do you think?” “What should we do about that lesion?” “Is this stenosis severe enough for the patient to benefi t from intervention?” Th ese questions were followed with multiple views and contrast injections. Unfortunately, the additional radiation exposure and contrast would rarely yield a defi nitive answer to these questions. However, thanks to advances in interventional cardiology, physicians who practice evidence-based medicine have at their disposal two technologies. Th ese technologies can
provide defi nitive answers to questions of lesion signifi cance and direct appropriate medical and interventional therapies. Th e technologies that off er this supporting evidence are Fractional Flow Reserve (FFR) and Intravascular Ultrasound (IVUS). FFR can determine if a suspect lesion is limiting the fl ow of blood to the heart muscle, causing ischemia; while IVUS can diff erentiate the disease pathology, plaque burden and true cross-sectional area of the culprit lesion. Th ese tools serve as guides in interventional therapy, determining stent expansion and apposition in an eff ort to achieve optimal patient results.
Historical Perspective.In 1977, when Andreas Gruntzig, one of the pioneers of modern interventional cardiology, performed the fi rst balloon angioplasty, coronary angiography was the only modality available for lesion assessment. Th us, the angiogram has been integral to cardiological diagnosis. However, the limitations of angiography are well documented. Th e injection of contrast medium into an epicardial vessel provides a lumen gram only. Furthermore, the appearance of that lumen is dependent on the angle at which the lumen is viewed. For instance, an eccentric (elliptical shaped) lesion may appear to have a 75% stenosis in one view, but the orthogonal view of the same area can give an
appearance of only a 25% stenosis (see fi gure 1). In addition, is the worst single view representative of the clinical importance of the narrowing? So, is seeing really believing? Do we send this patient for bypass surgery based solely on the one view in which the left main coronary artery appeared narrowed? For a lesion which cannot be seen well enough to gauge its clinical importance, additional information is needed. 1. Overcoming the limitations of angiography is the reason ischemic stress testing with pressure wire FFR, which measures physiologic impact of lesion severity, and IVUS, which provides an anatomic assessment of lesion severity, were developed. If the angiogram did the job in every case we wouldn’t need these tools.Development of FFR Technology. FFR technology was actually developed by Radi Medical Corporation in conjunction with two European cardiologists, Dr. Nico Pijls and Dr. Bernard De Bruyne. Th e fi rst version was an optical wire released in 1992.
courtesy RA
DI M
edical Systems, Inc.
By Charlene Shellenberger, RN, Clinical Education
Specialist, Healthworks, Inc.
1� CORONARY HEART ™

EDUCATION
Radi’s current pressure wire technology for assessment of FFR celebrates its tenth anniversary this year.
FFR-What is it? By defi nition, FFR is: Maximum achievable blood fl ow to the myocardium supplied by a stenotic artery as a fraction of normal maximum fl ow-pressure distal to the lesion divided by the pressure at the tip of the guide catheter, expressed as pD/pA=FFR. Th us, in the absence of any coronary disease a normal value would be 1.0, as these two pressures would be equal. However, a FFR value of <0.75 identifi es a stenosis associated with inducible ischemia, in other words, the lesion is reducing the fl ow of blood to the myocardium by 25% and is responsible for patient symptoms of chest pain-ischemia. Th is lesion is considered functionally signifi cant and requires interventional therapy. Furthermore, FFR is a lesion specifi c, physiological index determining the hemodynamic severity of intracoronary lesions. FFR can accurately identify lesions responsible for ischemia, which in many cases would have been undetected or not correctly assessed by angiography. Using FFR, the operator can guide intervention to the lesions responsible for the patient’s problem, saving time, cost and optimizing clinical outcome. 2.
How is the Functional Assessment of Coronary Artery Disease with FFR performed? By inserting a specialized 0.014-inch guidewire into the coronary artery, the pressure within the vessel can be accurately measured across a lesion. Two systems are currently available for clinical use: the RADI® Pressure Wire®/RADI Analyzer®, and the Volcano Corporation Smartwire/ ComboMap systems. Vital to this is understanding the physiologic basis of these measurements, a term referred to as hyperemia. When a vessel is in a state of maximum dilation it is said to
be in a state of hyperemia. Hyperemia can be induced in the cath lab with vasodilatory drugs, providing an invasive stress test. ³.
Two drugs have been used to induce hyperemic states in the cath lab, adenosine and paperverine. Adenosine, diluted to 10mcg/cc may be administered intracoronary (IC) starting with 30 mcg in the right coronary or 40 mcg in the left coronary. When given IC, adenosine has a very short half life –about 15 seconds. Adenosine may also be given IV at 140mcg/kg/min. Maximum hyperemia is achieved in one to two minutes. Patients may experience chest pain and/or shortness of breath during the infusion, these symptoms will dissipate quickly after the infusion is discontinued. IV adenosine administration is contraindicated in patients with COPD. IV adenosine administration is preferred by most high-volume RADI institutions (due to the high degree of reproducibility). It is required when performing a pullback of the RADI Pressurewire through multiple lesions within the same vessel, or left main evaluation. Papaverine has been used in the past but suff ers from many complications which include incompatibility with heparin and iodinated contrast agents, prolonged
Q-T interval, and occasionally torsades de pointes.
Th e RADI® Pressure Wire. Th e latest generation RADI® wire, Certus, is a sterile 0.014-inch guide wire with a 3-cm shapeable, radiopaque
tip. Th e wire is hydophyllic to aid placement in tortuous anatomy and hydrophopbic to help maintain wire position during intervention. Th ree microsensors are located 3cm proximal to the distal tip of the wire. Th e fi rst sensor is a silicon plezoresistive microsensor coupled with a Wheatstone bridge. It has a range of 30-300 mmHg and measures FFR. Th e second sensor measures thermodilution derived CFR (Coronary Flow Reserve) which is a measurement of microvasculature fl ow. Th e third microsensor is a temperature sensor. Th e Certus® wire is available in 175-cm and 300-cm lengths. A six foot adapter cable connects the Pressurewire® to the RADI Analyzer® during pressure measurements. Th e cable can be disconnected during wire placement, manipulation and intervention. ⁴. Th e Pressurewire may be placed in a diagnostic catheter or an interventional guide with no sideholes. Patients must be heparinized prior to wire insertion per hospital protocol.
Th e RADI Analyzer®. Th e RADI Analyzer® is a pole-mounted computer system. It may be portable or integrated into the cath lab. Th e Analyzer interfaces with the cardiac cath lab’s hemodynamic monitoring system. It collects and
interprets signals from the guide wire (micromanometer) and arterial
waveform from the guide catheter to be simultaneously displayed on both the RADI Analyzer® and the cath lab hemodynamic screen. Instructions for setup are displayed on the screen. Th e entire process of FFR evaluation (including equipment setup, hyperemia induction and recording) can be
accomplished in fi ve minutes or less. Capitol equipment
cost for a RADI understanding the physiologic basis of
to as hyperemia. When a vessel is in a state of maximum dilation it is said to
Q-T interval, and occasionally torsades de pointes.
Th e RADI® Pressure Wire. Th e latest generation RADI® wire, Certus, is a sterile 0.014-inch guide wire with a 3-cm shapeable, radiopaque
interprets signals from the guide wire (micromanometer) and arterial
waveform from the guide catheter to be simultaneously displayed on both the RADI Analyzer® and the cath lab hemodynamic screen. Instructions for setup are displayed on the screen. Th e entire process of FFR evaluation (including equipment setup, hyperemia induction and recording) can be
accomplished in fi ve minutes or less. Capitol equipment
cost for a RADI
courtesy RADI Medical Systems, Inc.
CORONARY HEART ™ 1�

EDUCATION
Advances in Lesion Assessment (cont...)
20 CORONARY HEART ™
analyzer is about $20,000. Each RADI® Pressure Wire® costs between $600-$700.
DEFER Study. A landmark study that investigated the appropriateness of stenting a functionally nonsignifi cant lesion. 325 patients were referred for PCI of an intermediate stenosis. FFR was measured just prior to the planned intervention. If the FFR was ≥0.75 patients were randomly assigned to deferral (Defer group n=91)(medical therapy with aspirin and statins) or performance (Perform group n=90) of PCI. If FFR <0.75, PCI was performed as planned. Th ere was a fi ve-year follow-up. Th e conclusion of this study was that fi ve year outcomes after deferral of PCI of an intermediate lesion based on FFR >0.75 is excellent. Th e risk of cardiac death or MI related to this stenosis is 1% per year and is NOT decreased by stenting. ⁵. “If it ain’t broke-don’t fi x it!”
Conclusions and Take Home Points about FFR evaluation with RADI Pressurewire system. Functional assessment of ischemia prior to stenting intermediate lesions is mandatory because it determines if a patient will benefi t from PCI or not. FFR evaluation is easy to perform, accurate, lesion-specifi c, quick and the cheapest diagnostic adjunct to non-conclusive angiographic data. Th e immediate and accurate identifi cation of culprit lesions enables easy, complete and eff ective diagnosis and treatment. ⁶⁷. If the stenosis is functionally signifi cant, use IVUS to examine the morphology and composition of the plaque, vessel and lumen size, and lesion length to provide the appropriate interventional therapy for the patient. Currently, only 10% of all cath cases employ FFR as a diagnostic tool to
guide PCI decision making. ²
IVUS Benefi ts vs. Angiography.Intravascular Ultrasound is the only way to evaluate vessel morphology. IVUS can determine the composition of a lesion: soft plaque, fi brous, calcifi ed or fi bro-fatty. IVUS allows insight into the pathophysiology of the plaque formation. Utilization of IVUS gives quantitative measurements of vessel and lumen areas at the stenosis, diameters and lesion length. IVUS provides an evaluation of stent deployment, apposition to the vessel wall, and edge-dissection assessment. Finally, angiography is a 2-D “lumen gram”, while IVUS gives a 3-D, real-time picture of the vessel from the inside out.
IVUS Technology. Th e fi rst human coronary IVUS in the United States was performed in 1987 by Dr. John Hodgson. 8. Th e components of IVUS technology are an ultrasound machine, IVUS catheter, an interface and optional pullback device. Ultrasound machines can either be portable or integrated into the cath lab as a permanent structure. Portability has made great strides in the
last few years, as units used to average about 400-500 pounds and required a strong back and arms to maneuver. Now, the new generation units for both Volcano, (s5), and Boston Scientifi c Corporation, (iLab) weigh about 100 pounds and can be moved with the pressure of one fi nger.
Th ere are two types of IVUS catheters: Mechanical and Phased Array. A mechanical catheter has a central driveshaft and a single transducer mounted at the catheter tip which quickly rotates (1800 rpm) to visualize the entire vessel in crossection. Mechanical transducers provide excellent image quality. However, the disadvantages of the central driveshaft is diminished fl exibility and image distortion termed NURD (Non Uniform Rotational Distortion). Boston Scientifi c utilizes mechanical catheter technology. Phased array catheters consist of multiple transducer elements permanently mounted along the circumference of the catheter tip. Because this catheter has no moving parts or central driveshaft there is greater fl exibility, no NURD, and may be used in the carotids. ⁹. Volcano utilizes phased array technology for
Limitations of Coronary AngiographyCoronary
Cross-section Angiogram Silhouette
X-rays
��%
2�%

EDUCATION
CORONARY HEART ™ 21
their Eagle Eye Gold catheter.
Anatomy of the Coronary Artery from the Inside of the Vessel to the Outside. Coronary arteries are composed of three layers. The INTIMA-innermost layer, only one to two cell layers thick but can greatly enlarge with the deposition of atherosclerotic plaque. The intima is defined by the internal elastic lamina (IEL) and the external elastic lamina (EEL). The MEDIA- middle surrounds the intima with a homogenous layer of smooth muscle cells (40 layers), providing vascular tone to the artery. The ADVENTITIA- outer layer surrounds the media and is composed of fibrous connective tissue which adds external support to the vessel.
Formation of Ultrasound Image. Ultrasound waves transmitted from the transducer will “bounce” back whenever it encounters an interface of different acoustic impedance. Therefore, ultrasound waves will traverse the blood in a vessel with minimal reflection, but will be highly reflected when it meets with the intima, which will be displayed as a single concentric echo. Based on the echo density of the structures of the artery, normal coronary anatomy produces
alternating bright and dark echos: A bright echo from the intima, a dark zone from the media and multiple bright echos from the adventitia. In addition, this explains why calcium, which is very dense and does not allow any penetration of the sounds waves beyond its borders appears bright white (echo dense) with a black shadow behind it (acoustic shadowing).
Atherosclerosis is a wall disease, not a lumen disease as plaque is laid down between the intima and the media. Atherosclerotic vessels may undergo either positive or negative remodeling. Positive remodeling
of the coronary artery is when the vessel grows to accommodate plaque formation in attempt to retain the integrity of the lumen size. Positive remodeling occurs about 80% of the time. Positively-remodeled vessels are composed more of softer plaque and respond more favorably to PCI than does a negatively-remodeled vessel. In negative remodeling, the vessel shrinks as plaque formation encroaches on the vessel lumen. Negative remodeling occurs 20% of the time and can be associated with more difficult PCI revascularization therapies. Remember, with angiography we do not see the plaque, we see only the EFFECTS of the plaque. Visualization of plaque is only possible with IVUS.
IVUS-Guided PCI and Determination of Lesion Significance.The key concept of using IVUS to guide interventional therapy is determining the MLA (Minimal Luminal Area) of the most diseased segment of the vessel. Thus, if the MLA is <4mm² in the proximal third of an epicardial vessel the lesion is considered significant and is justified for intervention. If the left main is being interrogated, an area of <6-7mm² is significant and that patient may
Which is more diagnostic?
Normal angiographic image of RCA
IVUS image of RCA with eccentric plaque
Normal Vessel Dissection
courtesy Volcano Corporation
cour
tesy
Bos
ton
Scie
ntifi
c C
orpo
rati
on

EDUCATION
Advances in Lesion Assessment (cont...)
22 CORONARY HEART ™
be referred for bypass surgery. These MLA parameters correlate with FFR values of <0.75 in determination of hemodynamically and structurally significant lesions.
Heavily calcified lesions. Calcium poses special consideration in guiding therapeutic treatment. Large amounts may require debulking with rotational atherectomy prior to stent placement. The plaque may be modified with a cutting balloon or pre-dilating with a compliant balloon. Nearly all calcified lesions will require post-dilatation with a high-pressure balloon to achieve full stent expansion. It is interesting to note that stable lesions may have a high calcium component. This is due to the deposition of calcium by red blood cells at a time of previous plaque rupture in attempts to repair and give stability to the arterial wall. 10.
Stent Sizing Guided by IVUS. It is important to determine the proximal and distal reference lumen of the target vessel. Reference lumens are the most near “normal” segment adjacent to the stenosis. Aggressive operators may choose to size their stent to the proximal reference which would be larger than the distal reference, as vessels taper in size from proximal to distal. More conservative physicians size the stent to the distal reference, while others take an average of the two sizes.
The MLA of the diseased segment compared to the vessel size of the same segment provides the amount of plaque burden, expressed as a percentage. Plaque burden is not the same as percent stenosis. Percent stenosis is derived by a ratio of the MLA of the diseased segment to the MLA of the proximal reference lumen. The number that appears on the IVUS screen after the determination of the vessel and lumen size with either
manual or automatic edge detection is percent plaque burden.
Key to successful stenting and optimal patient outcomes with IVUS-guided stenting is to adhere to the principle of stenting from normal to normal, with good coverage over the diseased portion of the vessel. 11. Therefore, routine use of a pullback device provides lesion length and is instrumental in choosing stent length and preventing geographic miss and inappropriate stenting. A mechanical pullback device may be set to move at either 0.5mm/sec or 1mm/sec, thus providing quantitative data for lesion length. Detection of edge-dissection post stenting is enhanced when the automatic mechanical pullback is utilized.
IVUS post-stent placement can determine if there is adequate stent strut expansion as well as apposition to the vessel wall. This is of paramount importance in the world of drug eluting stents (DES). Multiple studies have shown optimal deployment of DES is critical to positive patient outcomes. The CRUISE study (Can Routine Ultrasound Influence Stent Expansion) found a 44% reduction in TLR (Target Lesion Revascularization) with IVUS guided post dilatation. This coordinates with a 2006 study by Dr. Ron Waxman at Washington Hospital Center who found that up to 80% of DES may be inadequately deployed. IVUS use can reduce the number of sub-optimally deployed stents, which should positively affect or reduce the risk of restenosis. 12.
Financially, it is better for the patient and the cath lab to place one appropriately sized stent with IVUS guidance than multiple stents due to geographic miss. The STLLR trial showed up to 75% of the time there is some geographic miss. In addition, studies show each episode of restenosis costs an additional $15,000. Finally,
these are monetary costs of restenosis. The emotional cost to the patients and their families cannot be reflected in a monetary value.
Getting the Most From Your Coronary Stent. Utilizing IVUS to assess the lesion pre-stenting and for verification of apposition and expansion post-stenting. Pre-treat the vessel with compliant balloon or debulk if calcium is present as lesion preparation is necessary to optimize stent deployment. Post-dilatation with a non-compliant balloon catheter will ensure good stent expansion and complete apposition. These measures will help reduce the risk of complications associated with coronary stenting such as SAT ( Sub Acute Thrombosis-blood clot), TLR (Target Lesion Revascularization) and restenosis.
Who Benefits the Most from IVUS? The more complex the case, the more IVUS is needed. Any lesion with a known high restenosis rate such as bifurcations, ostial, left main, relatively small vessels in diabetics, and long lesions should be IVUSed. Another group of patients who would also benefit from IVUS are older patients with chronic stable angina. These patients, in most cases, have a lot of calcium build-up. Finally, any case where an unclear angiogram warrants further diagnostic evaluation with IVUS. IVUS would provide the least benefit for a young patient with a short lesion in a large vessel, or, patients with very small vessels 2.0-2.25mm diameter.
Challenges with IVUS- Three Reasons Cited by Physicians NOT to use IVUS.
1. Too much time and or money.a. Actual set up time is 5 minutesb. Actual cost savings as restenosis

EDUCATION
CORONARY HEART ™ 23
and acute problems of thrombosis are reduced.
2. Lack of Clinical Dataa. Nine angiographic vs. IVUS-guided studies performed.b. Eight studies in favor of IVUS-guided stenting and one neutral.c. Studies show IVUS-guided expandable stent implantation have better outcomes both acutely and chronically, CRUISE study.
3. Physicians unable to interpret the image or work the machine, too technically challenging for them.a. Most important to be able to obtain lumen diameter and lumen area.b. Know epicardial vessel MLA <4mm² and left main <6-7mm² require interventional therapy. Differentiate between % plaque burden and % stenosis.c. Well-trained techs and nurses to run the machine making setup faster and interpretation of images more routine will facilitate greater implementation of IVUS technology.
Just announced at TCT 2007, nationwide, 15% of all cath cases use IVUS, up from a previous figure of 10%. However, large research and teaching hospitals, such as Washington Hospital Center, may use IVUS on up to 95% of their cases. It is interesting to note, in Japan IVUS usage is in the range of 65-75%, and SAT rates are lower in Japan than the US. 8.
New and Upcoming Technology with Volcano IVUS. Virtual Histology-VH
VH technology provides a virtual biopsy in the cath lab with real time plaque characterization that correlates with actual histology specimens. VH allows the identification of a vulnerable plaque, or a plaque that is unstable. Intermediate lesions are the unstable lesions. Faulk, in Circulation ’99, stated that 68% of
MI’s are caused by intermediate lesions of 50-70% stenosis. VH technology uses eight spectral parameters to gather information and an algorithm is used to correlate plaque composition with what the ultrasound picks up according to pixels of color: light green = fibro-fatty, dark green = fibrotic, red = necrotic core, white = dense calcium. A plaque is considered vulnerable if there is >10% necrotic core next to the lumen. 12.
AIM- Angio IVUS Mapping. This technology is still in development. However, this will allow the angiogram and the IVUS image to appear together on one screen. The IVUS image is 3-D and the angio will be converted to 3-D as well.
Integrated IVUS. Integrated, or built in, systems for IVUS are available from both Volcano and Boston Scientific companies. Both systems are DICOM compatible and easy to set up with minimal training. The capital cost for an IVUS machine is in the $100,000 range. Each catheter costs between $600-800.
The SIPS trial showed the acute costs associated with IVUS are greater than angiography alone, but the chronic costs are less because patients have better outcomes, less TVR,TLR, SAT and most importantly less MACE (Major Adverse Cardiac Events-death, MI, stroke).
Conclusion-Tying it all Together. This is an exciting time in interventional cardiology. It is a time when adherence to true, evidence-based medicine as physicians guide medical and mechanical treatment of coronary artery disease will make a positive impact on the lives of patients in our cath labs every day. As baby boomers with cardiac risk factors face their inevitable visits to the cardiac cath lab, it will be critical that cardiologists and their teams use evidence-based protocols to thoroughly investigate these patients’ coronary anatomies, using the complete array of tools that are available to them prior to any interventional therapy and treatments. These patients will then leave the interventional suite knowing, with confidence that physicians have taken
IVUS - VHPlaque progression is Associated with Thrombus
courtesy Volcano Corporation

EDUCATION
Advances in Lesion Assessment (cont...)
24 CORONARY HEART ™
the appropriate measures to ensure the best possible outcome. Synergistic use of FFR to determine functional significance of a lesion and IVUS-guided stenting of that lesion will
provide patients with angiographically-moderate lesions definitive evidence to support the decision to the question, “To stent, or not to stent?”
Bibliography
Kern M , MD. Letter from the Editor: Is Seeing Believing? Cath Lab Digest 2006;14(8):4.
www.radi.se/education
Pijls, N. Non-invasive Testing is Not Specific Enough: Why and How to Obtain Objective Signs of Ischemia in the Cath Lab. Cath Lab Digest 2004; 12(10): 12-20. (Weissman, 2007)
Kenneth A. Gorski, RN, RCIS,FSICP. Book Chapter: Functional Assessment of Coronary Artery Disease. Cath Lab Digest 2005;19(9): 8-16.
Pijls, N., Schaardenburgh, P. v., Manoharan, G., & al., e. (2007;49:21). Percutaneous Coronary Intervention of Functionally Nonsignificant Stenosis 5-year Follow-Up of the DEFER study. Jorunal of the American College of Cardiology, 2105-2111.
Fearon W F; Yeung A C; Lee DP et al. Cost-effectiveness of measuring coronary flow reserve to guide coronary interventions. American Heart Journal 2003; 145(5): 882-887.
Pijls NH, De Bruyne B,Peels K, et al. (1996;334). Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. New England Journal of Medicine 1996; 334:11703-1708.
Cath Lab Digest talks with John Hodgson, MD, FSCAL, Professor of Medicine; Chief, Academic Cardiology, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona, about ways stent implantation can be optimized to avoid this complication. Stent Thrombosis: A Wake-Up Call? Cath Lab Digest 2007; 14: 1-10.
Weissman NJ, MD. Techniques and interpretation of Intravascular (Intracoronary) ultrasonography. UpToDate® 2007.
Mintz GS, Leon MB, Popma JJ, et al. Patterns of calcification in coronary artery disease. A statistical analysis of intravascular ultrasound and coronary angiography. Circulation 1995; 9: 1959-1965.
Henry K Lui, MD, Bruce R. Brodie, MD. The Perfect Fit: Getting the Most Out of Your Coronary Stent. Cath Lab Digest 2005; 13(10): 20-26.
El-Shafel A, Kern M. New Techniques for the Evaluation of the Vulnerable Plaque. The Journal of Invasive Cardiology 2002; 14 (3):129-137.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Modality of Investigation
Fractional Flow Reserve (FFR) IVUS
Assessment of: Functional severity of a lesion, examines physiology-inducible ischemia. Lesion specific.
Examine lesion morphology, can determine vessel and lumen diameter, area, and lesion length.
Critical Values FFR <0.75 functionally significant lesion
Minimal Luminal Area MLA for epicardial vessels <4mm²
Left Main <6-7mm²
Manufactures of Technology
RADI® Medical-Pressure Wire®/RADI Analyzer®
Volcano Corporation - Smartwire/ComboMap
Volcano Theraputics- s5-Phased Array Cathether
Boston Scientific Corporation-
iLab- Mechanical Catheter
Medication Requirements
Heparin prior to insertion 30-40units/cc 8.
Adenosine IV-140mcg/kg/min
Adenosine 30mcg in RCA/40 LCA
Heparin prior to insertion 30-40 units/kg
Capital Costs/Catheter cost
$20,000 / $600-700 $100,000 / $600-800
Additional Applications
Carotid, renal, peripheral and CFR (Coronary Flow Reserve)
Volcano & BSC for coronary and peripheral use
Volcano approved for Carotids
Want to learn More? www. teachFFR.comAccess code: RA47W
www.radi.se/education
www.teachivus.com

That’s the beauty of integrated medical information. The images and reports you need are at your
fingertips and accessible, whenever and wherever you need them. When seconds matter most,
you will be glad that Agfa HealthCare created the IMPAX® Cardiovascular Suite that
facilitates point-of-care data collection and anytime, anywhere viewing and management of
integrated images and information. Our patient-centric approach consolidates access to secure
clinical information, supporting cross-modality and legacy equipment data to help you improve
decisions about patient care. Agfa HealthCare is at work in 1 of every 2 hospitals worldwide, and
because our solution is designed by cardiologists, for cardiologists, you’ll be operating with
greater efficiency in nearly no time at all.
To learn more about our proven healthcare IT solutions, please visit
www.agfa.com/healthcare
Agfa and the Agfa rhombus are trademarks of Agfa-Gevaert N.V. or its affiliates. All rights reserved.
PROJECT INFORMATION FILE INFORMATION PRINTING INKS INTERNAL APPROVALSTARGETS/TINTS
Client:
Project:
Docket #:
Live Area:
Final Size:
Print Process:
Colours Available:
Line Screen:
Pre-press/Printer:
Agfa
Access Ad Resize
AGFA2178
N/A
8.125” x 10.875”
Litho
4-CMYK
N/A
Coronary Heart
File Name:
Job Folder Name:
Software/version:
Fonts Used: BosisforAgfa, CharterITCforAgfa
Client is responsible for checking all copy before project prints. Colour separators, pre-press service bureaus and/or printers are responsible for verifying all technical/mechanical specifications, including but not limited to tolerances, registration, accuracy of measurements and construction details before film and plates/cylinders are generated. Any changes to accommodate print requirements must be submitted to client for approval. Milestone makes every reasonable effort to ensure all artwork is error-free; however, we cannot be held responsible for any errors present once client provides final sign-off.
Cyan
101 King Street West, Cambridge, Ontario Canada N3H 1B5 T 519.653.2654 F 519.653.5941 milestoneadvertising.com
M I L E S TO N E A D V E R T I S I N G / D E S I G N
Magenta Yellow Black
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
MILESTONE TEAMADDITIONAL INFORMATION PRODUCTION FILE HISTORY PROOF NUMBER
Production Artist:Production Manager:Proofreader:Designer/Creative Director:Account Director:
October 11, 2007
October 11, 2007
October 11, 2007 2
Artwork Approved:
Production Artist:
Production Manager:
Proofreader:Designer/Creative Director:
Account Director:
Y/N DateInitials
Start Date:
Date Last Modified:
Date Released:
TomDianeDianeHeather/LauraJohn
• This is a digital colour mechanical, no traps have been made. Trapping to be applied by separator.• This proof/PDF is for colour break and content only and may not accurately reflect final printed inks.• Do not open this file with software and version other than that specified.
NOTES:
• This mechanical artwork has been prepared size as - 100%
AGFA2178_AccessAd_CH.ai
AGFA2178 Access Ad Resize
Adobe Illustrator CS3, Macintosh
©2007

Essex CardiothoracicADDRESS
MAP
Cardiac Catheter Labs Essex Cardiothoracic Centre Nethermayne Basildon, Essex SS16 �NL United Kingdom
FAST FACTS
Brand new 100 bed cardiothoracic hospital.
4 Labs: Interventional and EP.
Excellent training for new staff.
Relaxed and friendly working environment.
1.
2.
3.
4.
UNITED KINGDOMCARDIAC SITE VISIT
Centre
26 CORONARY HEART ™
Opened offi cially by the Prime minister Mr Gordon Brown in October 2007
(fi rst case performed July), the Essex Cardiothoracic Centre is one of the nicest departments we have had the pleasure of visiting. Modern and spacious designs are complemented by a friendly and effi cient staff , each with a desire to ensure their department becomes a leader in the industry.
Each morning at 0830 after all of the
staff have performed their morning duties everybody gets together in the staff room for breakfast. Th is allows for an informal meeting to raise issues of concern or just to socialise, a unique situation for any department.
To diff erentiate their department from others they have also named each lab after various cities: London, New York, Paris, and Amsterdam. Naturally London is the EP Lab because everybody has been there and it is not
very exciting compared with the other cities.
We spoke with Dr Nick Robinson and Dr Stuart Harris who were both genuinely impressed with the facility and enthusiastically spoke of the new equipment coming and how wonderful it was to work there.
Lead Nurse, Eliie Gorman gave us a detailed tour of the entire facility and answered the questions we had.

CARDIAC SITE VISIT
CORONARY HEART ™ 2�
Size of the Department:
100 bed dedicated cardiothoracic hospital.11 Day stay beds attached to the cath labs.State of the art cardiothoracic theatres and cath labs.Critical care, cardiothoracic surgery and cardiology wards3 interventional labs – 1 diagnostic lab in the DGH and a shell for another lab.3 cardiothoracic theatres.
Staff numbers and roles:
8 Consultant Cardiologists, 8 Cardiology Registrars, 15 Registered nurses, 8 Radiographers, 7 Cardiac physiologists,
•
•
•
•
•
•
•••••
1 Domestic Assistant.4 Support workers, 2 Admin staff, Waiting list team
The nursing team generally organise the dept as regards daily lists, the running of the day stay and the cath labs. Most of the ordering is undertaken by the nursing team.
The radiographers are responsible for image quality, radiation monitoring, contrast.
The physiologists are responsible for haemodynamics.
Shared duties are patient care; lab throughput, communication and documentation. We also have a member of staff responsible for organisation of social events.
••••
EP Lab Procedure
From left: Abdul Hassan (Cardiac Physiologist), Mark Passey (Lead EP Physiologist), Refai Showkathali (SpR Cardiology), Dr Stuart Harris (EP Consultant).
Cardiac Cath Lab Staff
From left: Dr Nick Robinson, Vicky Hadley (Radiographer), Devika Ghisayawan (Radiographer), Marie Abella (RN), Matthew Varghese (Cardiac Physiologist), Rene Arabia (RN), Chris Puzon (RN), Ellie Gorman (RN), Mark Passey (EP Lead Physiologist), Katy Dean (Cardiac Physiologist)

CARDIAC SITE VISIT
Essex Cardiothoracic Centre (cont...)
2� CORONARY HEART ™
Procedures:
Angiography and angioplasty, Pressure wire analysis, Intravascular coronary ultrasound, Rotablation, EP studies, Radiofrequency ablation, CRT, ICD implantation, Pacing, Cardiac EP Mapping.
Equipment:
IVUS, Pressure wire, Rotablation, Cardiac EP Mapping, Witt haemodynamics, Philips Allura FD10 with 3D cardiac imaging and spin rotation.
Procedures performed per year:
Since opening July 2nd over 450 procedures have been performed. We anticipate performing approximately 1800 PCI and 250 EP procedures per annum.
Day Cases:
A mixture of Day case, overnight stay and interhospital transfers are performed
Cross-Training:
We have one member of staff with the elective angiography generic worker course and 2 members of staff currently undertaking the course. We plan for a further 4 staff to undertake this course next year.
Surgical Back-up:
We have 3 dedicated cardiothoracic theatres on site.
New procedures implemented:
As a new hospital many procedures have been implemented, new integrated care pathways, policies in conscious sedation, infection control, haemostasis, renal complications and diabetes management.
Private Cases:
We do perform private cases, approximately 6 per week, at the end of a consultants list or on a Friday.Private beds will be available in the Cardiothoracic Centre by Christmas run by the healthcare provider Capio.
Alliance with other hospitals for treatment of patients:
We are linked to 5 sites across Essex and our referrals come from all over Essex and beyond.
Inventory Management:
The nursing staff managed the ordering system on a daily basis.
Cath Lab Procedure
From left: Marie Abella (RN) and Dr Nick Robinson

CARDIAC SITE VISIT
CORONARY HEART ™ 2�
Haemostasis Management:
We use the St Jude angioseal device, and on occasions the femostop from RADI, otherwise manual pressure is preferred.
Measures implemented to cut costs:
We are always thinking of measures to cut costs. We are all very conscious of the budgetary constraints.
Some of the challenges in setting up the department:
The whole project has been a challenge from ordering equipment, consumables, employing staff and writing policies and procedures. The biggest challenge was forming an
effective team to work in this new state of the art hospital who were innovative and competent.
Training for new employees:
Competency training on the following areas level appropriate to profession:
Life supportImaging Equipment and archivingRadiation protection and dose monitoringInjector pump trainingIABP trainingSyringe pump trainingInfection control trainingECG monitoringHaemostasisManual handlingRecord Keeping (Caldicott)EP training
•••
•••••••••
Trust mandatory induction and training
Continuing education programs for staff:
We have a Friday breakfast meeting where reps and also educationalists attend and give a short teaching session on a chosen subject. We also encourage staff to go to as many seminars/study days and conferences as possible to broaden their knowledge. We are linked to Anglia Ruskin University and run in house ECG and cardiology courses. Our monthly Audit meeting includes unit performance review and educational lectures.
Competency checks for staff:
Ongoing competencies are undertaken and yearly appraisals are also carried out.
Training facility for cardiac registrars:
Yes we have 8 cardiology registrars who all have a timetable of training for the labs.
What is the best part of working at your facility?
The staff in this hospital and most particularly in the cardiac cath labs are fantastic, everyone works really well and gets along even when under pressure. The camaraderie is extraordinary and everyone who visits comments on this. We spend time as a group outside of the working environment at social events that helps to fuel our team spirit. A good working environment is not only conducive to an effective dept but to patient care.
•
EP Lab Control Room
From left: Abdul Hassan and Franklin Daniel (Cardiac Physiologists) in the EP lab with company reps

CARDIAC SITE VISIT
Essex Cardiothoracic Centre (cont...)
What an amazing place Essex is. Located to the East of London this region is famous for its long coastline and small holiday resorts where you can set sail. Inland expect to find ancient woodland forests near lovely country houses with beautiful gardens.
Culture is also at every turn, with a unique style and colourful dialect famous throughout Britain.
Th ings to see and do:
Southend-on-Sea: Th is costal town is home to the longest pleasure pier in the World - 1.33 miles long. Get to the end via a walkway or rail service.
Chelmsford: Charles Dickens and the Duke of Wellington lived here. See the Grade II listed Hylands House and Gardens, or hire a narrow boat and travel down tranquil waterways.
Basildon: See plenty wildlife at the 120 acre Wat Tyler Country Park, which is also home to the National Motor Boat Museum.
Bring the kids to the annual Teddy Bears Picnic in June.
•
•
•
WHY ESSEX?
Teddy
Best Elements of the Design?
Infection control was a priority.
Side rooms with ensuite for MRSA patients in Day Stay (Recovery).
Large, open corridors and rooms.
Full security protected facility.
Separate back lift for ambulance patients to avoid main entrance and general public.
Automatic Climate Control. Th e labs have sensors that determine when people are working and adjust the temperature accordingly, or turn off when empty.
Separate dedicated anaesthetic unit for patients maintained by theatres.
Prep rooms in each lab. When the main doors are locked, entry is via the prep room only.
•
•
•
•
•
•
•
•
What Could Be Better?
Lead screen in the lab to allow you to walk in without wearing a lead. Particularly useful for surgeons when they need to discuss a case quickly.
A means to protect the patient from visualisation in main corridor (although public not allowed here). Mainly applies to Lab 1.
Electric doors to Roding Ward.
Recovery seating area. At present only designed with trolleys in mind.
TV’s in recovery.
At present dirty utility must go via main corridor.
Shelving in the right places.
•
•
•
•
•
•
•
Essex Cardiothoracic Centre Floor Plan
30 CORONARY HEART ™

www.siemens.co.uk/medical
Siemens has delivered the broadest range of cardiology systems into the UKmarket. The latest, the AXIOM Artis dFC MN, integrates fully with the NIOBEmagnetic navigation system by Stereotaxis, Inc. to support innovative, ground-breaking clinical applications. Magnetic assisted intervention is a unique methodto improve electrophysiology and interventional cardiology workflow andoutcomes.Interventionalist are able to guide magnet-tipped catheters and guidewiresthrough the vessels and chambers of the heart with the utmost precision. Whether in the paediatric or adult environment Siemens is leading the way withtrendsetting innovations to improve outcomes.
Broadest range tomeet your needs
Innovation leadership in cardiac imaging
For further information please contact:
01276 696497 or

The Mayo Clinic- EP Department
ADDRESS
MAP
Mayo Clinic200 First St. S.W.Rochester, MN ���0�United States of America
FAST FACTS
Arguably the world’s most recognized medical institution
Six dedicated EP Labs.
Approximately 26�0 procedures per year.
Stereotaxis Niobe (current) & Hansen (coming soon).
1.
2.
3.
4.
cour
tesy
of
May
o C
linic
“Th e best interest of the patient is the only interest tobe considered.” - Dr Will J. Mayo
UNITED STATES OF AMERICACARDIAC SITE VISIT
32 CORONARY HEART ™
The Mayo Clinic is regarded internationally as one of the top medical
institutions in the world, and has won countless awards for the high levels of service and care. Th is care is supported by advanced programs in medical education and research, utilizing the latest technology medical companies have to off er.
Patients fl y from all over the world to be treated here, however although you would expect to fi nd the Mayo Clinic in the center of a state capital, the reality is vastly diff erent. Th e Mayo is located in the regional city of Rochester surrounded by Amish farming communities in the south-east of Minnesota, one hour from Minneapolis.
Rochester is the third largest city in the state with a population of 94,000, one third of which are employed at the Mayo Clinic. Th e city is also home to one of IBM’s largest facilities, and has long been a fi xture on Money magazine’s “Best Places to Live” index, and was ranked number 67 on the 2006 list. During our visit in September with the sun shining each day, we almost considered moving here.
Th e following pages will provide you with a brief history of how the Mayo Clinic came about, followed by a look inside the world class Electrophysiology Department and an interview with the EP Department manager, Mr Douglas Beinborn. In 2008/09 we hope to return to the Mayo to perform a site visit on the interventional and non-invasive side.

MAYO HISTORY
In 1846, Dr William Worrall Mayo emigrated from England where
he was born, to the United States, training to become a doctor in 1850. In 1864 his family moved to Rochester, after being appointed as a civil war examining surgeon for the Union enrollment board the year prior.
Here Dr Mayo trained his two sons, William J. and Charlie in medicine, first by observing, followed by assisting with autopsies. They both then went on to medical school before returning to their father’s practice. It was however a tornado that ravaged the town in
1863, killing and injuring many that Nuns from the Sisters of St Francis (who acted as nurses), and the Mayo Doctors combined to build the first general hospital in southeastern Minnesota - the 27-bed Saint Marys Hospital which opened in 1889.
Right from the beginning the Mayo was at the forefront of patient care. In 1969 on a trip to New York, Dr W.W. Mayo saw for the first time civilian ambulances transporting patients in the city, amazed that doctors no longer did house calls. He later wrote, “When an accident occurs in any part of the city, there is a dispatch sent ... and the ambulance is on the ground a few minutes after. The injured are picked up, and at once taken to the hospital. Truly this is quite as astonishing as any of the fairy tales.”
Sure enough, once St Marys Hospital was built the Mayo Drs purchased a horse-drawn ambulance from the
Studebaker Company. 1.
As the family practice became bigger and medical knowledge was increasing rapidly, others joined the group. Eventually the team created a new system of health care, with the creation of the USA’s first medical specialities. Dr William Mayo and his sons once said, “no one is big enough to be independent of others.” In other words, medicine has become so complex that it requires a team of physicians, specialists, medical professionals and scientists all working together to provide the absolutely best medical care. ².
Since those days more than eight million people have been treated at Mayo Clinic, and staying true to their word, the patient always comes first.
“The injured are picked up, and at once taken to the hospital. Truly this is quite as astonishing as any of the fairy tales.”
CARDIAC SITE VISITco
urte
sy o
f M
ayo
Clin
iccourtesy of M
ayo Clinic
CORONARY HEART ™ 33
Dr William Worrall Mayo, 1�0�
The Mayo Brothers Dr. Charlie (left) and Dr. Will
1 http://www.mayoclinic.org/news2007-rst/3897.html² http://www.mayoclinic.org/tradition-heritage/mod-el-care.html

CARDIAC SITE VISIT
Mayo Clinic (cont...)
34 CORONARY HEART ™
MAYO CLINIC ELECTROPHYSIOLOGY DEPARTMENT
With the Mayo Clinic in Rochester, MN due to its size
and international interest we have to break away from our traditional site visit articles and separate it into two parts: EP and Cath. In this edition we will look at the EP department which we visited in mid September 2007.
The following questions have been answered by Mr Douglas Beinborn, the EP Department Manager.
Size of the EP Department:
We operate six procedure rooms on a daily basis.
Staff numbers
18 technical staff21 physicians35 RN’s3 mid-level providers4 secretaries4 schedulers
Procedures:
Ablation, Diagnostic EP,
••••••
••
Tilt table studies, Long QT testing, ICD implants including bi-ventricular, PM implants including bi-ventricular, lead extraction, Implantable loop recorders
Equipment:
CartoESIICE Laser extractionPrucka recording Cryo-ablationStereotaxis
•••
•
•
•••••••
Siemens EP Lab with Stereotaxis NiobeThe entire EP department will soon be comprised of all new Siemens imaging equipment.

CARDIAC SITE VISIT
CORONARY HEART ™ 3�
Day Procedures:
Variety of inpatient and outpatient procedures
Procedures performed per year:
900 ablations, 1200 device implants, 350 tilts/long QT tests. 200 EP diagnostic studies.
Cross-Training:
We cross-train within the lab. We share a prep/recovery with the cath lab.
Staffing roles:
We utilize RCIS and CVT’s who perform the same role. We have CRNA’s in four of our procedure rooms who provide deep sedation to general anaesthesia. RN’s are cross-trained to work in the procedure rooms, our clinic, and hospital service.
New procedures implemented:
Epicardial ablation, Tandem heart for complex VT ablation, Carto Sound.
Inventory Management:
We work cooperatively with Mayo Materials Management and a number of our own internal staff to manage our inventories and charging in relation to usage
••••
••
•
Haemostasis Management:
Complex to cover here. Some cases heparin is reversed, most of the time we wait for ACT to be < 180 prior to sheath removal
Measures implemented to cut costs:
Extensive work has been done on materials management. Topics include consignment, utilization rates, automation with reordering, cost negotiation. Currently working on lab efficiencies.
Training for new employees:
Formal orientation process has been developed. Assigned a preceptor with outlines and goals set of the orientee and preceptor
EP training facility for cardiac fellows:
We have four senior fellows each year.
Continuing education programs for staff:
We have core curriculum every Monday that are EP in origin. Ability of staff to attend conferences outside of Mayo.
Competency checks for staff:
BLS, ACLS, Infection control, Safety, Equipment competency,Procedural competencies (recording system, stimulator, device programmers, etc)
What is the best part of working at your facility?
Highly dedicated staff, teamwork, innovation, access to the latest technology, challenging but rewarding work environment.
•
•
••••••
Inserting a Pacemaker

INTERVIEW
36 CORONARY HEART ™
Tell me about the process for upgrading your department?
When we built this lab originally 12 years ago there was a group of nurses, techs, and physicians who helped with the design. Back then we did site visits to different labs, so what we came up with was having three labs connected by one room containing all of our
supplies, and that design has worked well. Now though as we are changing out the floor systems, we get to redesign again, and some of the driving factors are that the cold storage for the old equipment required a bigger space than the new equipment, so we are able to obtain space back from there.
Some other guiding forces are how can we reduce the radiation exposure to our staff? How can we reduce wear and tear? How can we decrease wearing lead as much as what we have in the past, and get the best images possible? So currently in one of the procedure rooms we are doing all of the work inside the room, and we have one procedure room that we are designing for the Hansen Robotics where we are moving all of the equipment outside of the room. Therefore we will be doing the 3D mapping outside of the room, we will be able to do the intra-cardiac echo outside of the room, as well as the stimulator, recording system and ablation system. Those closest to the exposure will be the anaesthesia person and one technician, but they will be far enough away from the fluoro system that the radiation dose drops significantly. In relation to wear and tear, we looked at how we were wearing lead everyday of the week, and can we get our staff to wear it only part of the week.
With the other procedure room that we are replacing we will still be leaving the equipment in the room there. Number one idea was to have 2 EP rooms and have everything in the control room but there was too much of a space
crunch, and it would have been too loud to have two alongside each other. So we are redesigning that room so that the people who are doing the recording system and the ablation box will have it positioned in the room protected by lead. So that once they are behind the lead, they will be able to take off their lead gowns and be better protected.
The other room that we are going to be ramping up significantly is going to be the Stereotaxis room, and that is obviously run from outside of the room, which again is less standing, less wear and tear, and less radiation exposure.
So I think the main thing I see coming up is that we are fortunate to have a number of people who have been working at the Mayo for 20-30 years, and physicians who have been here for 15 years, and I don’t want to say that we are all getting older but obviously how can we better take care of our staff.
That is obviously very important. As a radiographer I have spent many hours in lead during EP cases and it can be difficult for everybody in the lab. It is a real Occupational Health and Safety concern.
Absolutely!
With new technology, radiation exposure is lower, but if we can get them away from there, we will save more wear and tear on the back.
Douglas Beinborn- speaking about the Mayo EP Lab redesign and challenges to be faced in the future.
Mr Douglas Beinborn, MA, RN Department Manager of Heart Rhythm Services, Mayo Clinic,
Rochester
Douglas Beinborn is currently overseeing the redesign of the EP department at the Mayo Clinic in Rochester and explains the process, decisions, and challenges facing one of the world’s leading departments. He spoke with Coronary Heart’s Director and Chief Editor, Tim Larner.

INTERVIEW
CORONARY HEART ™ 3�
What kind of frame rates do you use during procedures?
Two of the three GE rooms have a variable rate of fl ow and a special mag for us and 15fps and low dose, and that will be what we will be using on the new Siemens equipment with 15fps and low.
What kind of input do you have from cardiologists in the design?
We have 2 physicians that work in our department, 2 technicians, and two nurses who sit down with us and go over all of the designs. Th en we take them into the room and show
them where the layout will be and see where the fl uoro sits how we are going to build that section, and see where people are going to be protected during procedures, so we defi nitely get good input from everybody. We sit down with architects, electricians, construction managers, and even our staff get to go over the plan. Th e staff are involved every step of the way.
Do you use Consulting Companies?
Th ere isn’t a specifi c consulting company we use. Th ere are typically local ones who contact us and we use them.
Holistic design for the patients?
Obviously the needs of the patient comes fi rst so we do whatever is needed. I think we have a very comprehensive educational program here for the patients, so before the procedure they are well informed. Th ey are seen by one of our doctors before they have an EP procedure (can be a general cardiologist or one of our doctors who works them up before the procedure). We have nurse educators at both the EP and device side before and after the procedure.
We bring patients in the day before the procedure, so when they arrive in the morning they have been
Interviewed by Tim LarnerDirector/Chief Editor of Coronary HeartPrevious Cardiology Manager, Radiation Safety Officer, and Occupational Health & Safety ManagerExperience in 11 Cath Labs.
Eighteen Bed Recovery Room:Th e display on the ceiling is used to communicate with staff and physicians, acting similar to a paging system. Th ese are located throughout the department.

INTERVIEW
completely worked up so essentially in the morning it is to ensure there has been no change in condition and to answer any last questions. Acts more as a public relations visit by us. Plus if I see them the day before and the day of the procedure we already have an established relationship, which improves their comfort level.
Philips have released their Ambient Suite to improve comfort for the patient, and in our last issue we featured a lab in the UK which had a television above the patient during a procedure. Are you considering employing any unique patient aids?
For our complex ablations we put those
patients under a general anaesthesia. Now for the other rooms we offer music for them, so they can bring their own in on personal players and listen. We honestly haven’t looked at any else other than that.
So many of our patients have general anaesthesia which is unique. For our VT Right Ventricular Outflow tract ones that you need them awake fully so you don’t knock down their Catecholamine’s. But with AF it is so anatomic based that when you find a firing coming from the Right Superior Pulmonary Vein, then we not only isolate that one but we isolate all the veins. We do a thorough ablation line as well. Because although they have firings coming from one pulmonary vein that doesn’t necessarily mean that is the way their normal situation is, so our goal is to do just one procedure and get everything taken care of in one procedure. So for AF they receive a general anaesthetic.
Some companies are offering cash for EP tips. Do you use this service?
Yes, we have utilised it for about 14 years.
Purchasing decisions in the labs?
It happens every year. So for the 2008 budget we met in August to say what our capital equipment needs would be, and what we have to do is anything over $30,000 we have to put it through a committee, part of the capital equipment budget, so if it is anything under $30,000 I can sign off. So what I do is sit down with the physician leaders and both the device, EP and the whole practice and say ‘what do
Douglas Beinborn (cont...)
The Landow Atrium:Located in the Gonda Building. Staff regularly stop by and give an impromptu performance to patients.
3� CORONARY HEART ™

INTERVIEW
we need?’ So next year we have one of our main pacing room will be getting a new fl uoro system, and then we are upgrading some of our 3D mapping systems, and we have put in Hansen Robotics just in case we don’t get it approved this year it is in for next year, and anything for space remodelling. Also an additional procedure room for EP was also put in there.
After that it all gets sent into CV and reviewed by leadership there, where they ask, ‘what is your certainty of needing this equipment?’ Th en they might challenge by saying ‘boy this is only 3 years old, why are you asking for a replacement for that?’ We have never had anything like that but that is the sort of questions. In Echo they may ask what is your breakdown rate, is it new technology, is it superior to what you have, or is it the same platform for what you have. So you have to expect questions. And then the institution will say this is how many millions of dollars they have budgeted for equipment this year. So they may have a budget for $100 million but there may be $170 million that people are asking for. So then you have to ask does it actually need to be replaced. What will happen if it isn’t? Is it a patient care or safety issue?
We are replacing our Prucka systems this year as our communication systems are NT platform which will no longer be supported, and our fl uoro systems are 12 years old so they are in need of replacement. So it is all about checks and balances about how much you really need this equipment.
If it is new technology you have to look at how it conforms to your business plan. Does it require more space? More staff to run it? Does it require physicians? Can you bill for it? Does it speed up cases? Does it improve outcomes? So there are a number of questions you have to answer. Good
checks and balances right there.
How is the rapport between physicians and staff in the Lab?
We have a very unique situation here in that the physicians really value the allied staff . I think EP procedures are a little diff erent from cath Lab
procedures. Cath Lab procedures are quick, but with here particularly the ablations they are longer and technically challenging, and the physicians are very dependant on the rest of the staff . Our staff have a very good working relationship with the physicians, and are a close knit group. Th is has been really the success of our total group
Gonda Building. Opened in 2001 it is linked with two other buildings forming the largest interconnected medical facility of its kind in the world, more than 3.5 million square feet.
CORONARY HEART ™ 3�

INTERVIEW
Douglas Beinborn (cont...)
In the UK I have worked in both public and private hospitals for EP cases. In public hospitals if the patient list hasn’t ended you do the remainder the following day, but in private the staff must stay to complete the list which takes a toll on moral.
I think this is the biggest problem we have coming up is to deal with the demands on our services. If we look at AF it is only going to become a bigger problem, because if you look at statistics now and world wide projections for 2020, they are going to go up drastically, and as people age, more people will need pacemakers. I think everywhere you turn with EP there is significant growth opportunity there.
Another thing we are looking at is how can we improve efficiency and use our expensive rooms to their maximum potential, like can you do an extra case per day with the new equipment. Efficiency is key. You want to do what is best by the patient, but on the other hand if you can do different processes more smoothly and get them in and out of the procedure room more quickly then that is really important.
How is your patient turnover? Can you think of any ways you can improve?
I know we have just hired mid level providers who work on the floors. Sometimes we have patients that come from the ward that aren’t properly prepared that can really slow down the day, so we look at how we can best manage. We use processes whereby we assume 80% of the patients will be straight forward, but when something happens outside the normal we are prepared to handle it. We work backwards to try and work out where
was the holdup and how to improve it for next time.
In the morning our nurse sees them down on the floor and gives them the final education, then a staff nurse from that floor evaluates them, then they come up to our 18 bed recovery area and are seen by a CRNA (Certified Registered Nurse Anesthetist) and have their sites prepped, and if it is an ablation have their groins prepped there. There are many different touches, so we must look at how can we reduce this without reducing quality. Like how many times do you need to ask about medication allergies? So there are always things we can do to improve efficiency.
The best departments have good communications with all areas of the hospital, so any problems that arise can be solved almost immediately, rather than pointing the finger at each other. Prepare for the worst. Hope for the best!!
We even do site visits to other hospitals and here we also bring in a multi-disciplinary groups whom directly affect our workflow and try and say, ‘our goal is to try and have a patient on the table by 0745. How long do you need to bring them in? How long is your process?’ But then there are waits like with transportation, escorting patients to a different area. We
look at the time they are called till the time they get there. What is that time? We are always finding ways to improve.
The Mayo is always regarded as one of the top hospitals in the USA but as you said earlier you will be even visiting the Cleveland Clinic soon to see how they operate.
In the back of my mind I think that wherever I go in any other institution be it a small or big lab there is always a couple of things you can take away, and say ‘boy they really do a good job with this and it would be nice if we can incorporate this in our lab.’ You can gain something from any place you go and watch.
Inside Humour
40 CORONARY HEART ™

EDUCATION
The traditional site of pacing from atrial appendage
is often used when patients receive a permanent pacemaker. Although this site is sufficient to correctly depolarise the atrium the corresponding mechanical contraction may differ significantly from that of intrinsic conduction and may lead to conduction delays .In the atrium pacing sites other than the appendage include the inter-atrial septum which may be elected in the patient with atrial arrhythmias as well as those patients who are candidates for atrial based bi-ventricular pacing with inter atrial conduction delay, thus synchronizing the right and left AV delay.
An understanding of atrial anatomy is of course crucial to be able to select an alternate pacing site. In the picture below (fig 1) you can see the right atrium with the right atrial anterior wall opened. From the right side we are looking into the inter-atrial septum. The superior vena cava is at the top left of this drawing. In the middle runs the Eustachian ridge, the continuation of the terminal crest (crista terminalis) Also visulised is the AV ring with the tricuspid valve, the inferior vena cava and the ostium of the coronary sinus. The Thebesian valve marks the lower part of the coronary sinus ostium, just above the sub-thebesian pouch. The Triangle of Koch is depicted by these landmarks.
Figure 2 shows the right atrium opened with the tricuspid valve in the middle of the picture. this high part of the atrium could be somewhere to pace
from especially as this is a much larger part of the septum. Alternatively why not in or just above the triangle of koch and why not high up in the atrium where there is normal conduction from top to bottom followed by the same direction of contraction?
Well when you turn the heart around (fig 3) you see the venous system entering here in the right atrium. Visualised is the left atrium with the
right pulmonary veins and there is an intra atrial groove between both atria. So when you pace high in the right atrium you will meet the intra atrial groove and you will not pace the right and the left atrium simultaneously. It is better to go down a bit and make your choice of pacing site just above the triangle of Koch. It is the thickest part of the intra atrial septum and as the most anisotropic depolarization of the atrium occurs there, it could be a place where atrial fibrillation is initiated. Pre-excitation by pacing the place of origin of arrhythmias could prevent these arrhythmias to a certain extent.
When positioning a lead in the triangle of Koch on fluoroscopy, a proper knowledge of anatomic position and consequently adequate angulations is very helpful.
In the Figure 4, (next page) in front you is the pulmonary artery, the aortic valve in the middle and the right and the left atrium at the back. The angle of the inter- atrial septum is about 45 degrees, as seen from the frontal side.
Pacing Anatomy Part 2Alternate Pacing Sites – The Atrium
Anatomy:the location of the triangle of Koch
Inferiorvena cava
AV Ring
Ostium Coronary
Sinus
Figure 1
Figure 2
Figure 3
Compiled by: Mr Stuart Allen, Technical Head CRM, Southampton General Hospital, UK
CORONARY HEART ™ 41

EDUCATION
Th e orientation is further clarifi ed in the CT image (fi g 5)
On x ray it may be diffi cult to distinguish between a lead position in the atrial septum and one in the RV septum. Th e pictures and x –rays (Fig 6) show that when in a LAO position, the lead in the Right ventricular septum is well distinguished from the intra-atrial septum lead which is directed posterior. In frontal view proper orientation is much less clear if not impossible.
Next Edition –Alternate Right Ventricular Pacing Sites
Pacing Anatomy Part I available to download at www.coronaryheart.com as part of Edition 6.
Pacing Anatomy - Part 2 (cont...)
Figure 4Anterior Figure �
Figure 6
LAO 4�
Frontal Frontal
After 17 years at Southampton General Hospital, Mr Stuart Allen is heading Down Under to Australia to commence work at the Monash Medical Center. We are assured that he will be missed by all staff at Southampton where he was the Technical Head of CRM. Although he will be located on the other side of the world he will still be contributing for us and still acting as one of our leading consulting editors.
Mr Stuart Allen is Heading to Australia
42 CORONARY HEART ™

EVENTS DIARY
200�
November
ISCP (International Society for Cardiovascular Pharmacotherapy) 200729 November - 1 December, 2007Antalya, TurkeyWeb: www.iscp2007.org
December
Chronic Total Occlusions 4 - Live Course4-5 December, 2007Glenfield Hospital, UKEmail: [email protected]
EuroEcho 20075-8 December, 2007Lisbon, PortugalWeb: www.euroecho.org
200�
January
Advanced Angioplasty23-25 January, 2008London, UKWeb: www.advancedangioplasty.co.uk
February
4th Cardiff Freeman Echocardiography Course5-7 February, 2008Cardiff, UKEmail: [email protected]
March
ACC 2008 + i2 Summit29 March - 1 April, 2008Chicago, IL, USAWeb: www.acc08.acc.org
May
EuroPRevent 20081-3 May, 2008Paris, FranceWeb: www.escardio.org
EuroPCR13-16 May, 2008Barcelona, SpainWeb: www.europcr.com
Heart Rhythm 2008 - 29th Annual Scientific Sessions14-17 May, 2008San Francisco, CA, USAWeb: www.hrsonline.org
XVI World Congress of Cardiology18-21 May, 2008Buenos Aires, ArgentinaWeb: www.worldheart.org
June
BCS Annual Scientific Conference2-5 June, 2008Manchester, UKWeb: www.bcs.com
Arrhythmia Awareness Week 20089-15 June, 2008Email: [email protected]
Heart Failure 2008 Congress14-17 June, 2008Milan, ItalyWeb: www.escardio.org
Cardiostim 200818-21 June, 2008Nice, FranceWeb: www.cardiostim.fr
August
ESC Congress 200830 August - 3 September, 2008Munich, GermanyWeb: www.escardio.org
October
Acute Cardiac Care 200811-14 October, 2008Versailles, FranceWeb: www.escardio.org
To list an event please contact Tim Larner by Email: [email protected] or Fax: +44 (0) 20 7160 9334.To sponsor this diary please contact Wendy Rose by Email: [email protected]
Events Diary
With unsurpassed knowledge of the cardiology industry sector, we are able to offer all the pro’s and con’s of making that move, and the different benefits offered by various companies.
So, if you are even just thinking about making that move and needsome ‘no-pressure’, balanced, informed and free advice, please callus on 01223 550 860.
Go on! How will you know if you don’t ask?
Remtec Selection - the specialists in medical device industry recruitment
For online applications, visit www.remtec.co.uk/register.htmor email: [email protected]
Thinking of a move into the Industry?Need some advice?
www.remtec.co.uk
CORONARY HEART ™ 43

MKT01422_Clinical_Services_1007.indd 1 18/10/07 4:21:51 pm
Related Documents