E M P L O Y M E N T coronaryheart.com Radiation Protection “Subscribe online for your FREE Copy!!” Interview Patricia Pye - Carolinas Medical Center, NC How to Create Loyal & Motivated Staff Management Atrial Flutter Explained Education Special Edition Site Visit St Mary’s Medical Center, WV September / October 2007 Issue 8

Coronary Heart #8 US
Mar 28, 2016
Coronary Heart Sepember / October 2007
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EMP
LO
YMENT
coronaryheart.com
PLLOOLLOO
Radiation Protection
“Subscribe online
for your
FREE Copy!!”
InterviewPatricia Pye - Carolinas Medical Center, NC
How to Create Loyal & Motivated Staff
Management
Atrial Flutter ExplainedEducation
Special Edition
Site VisitSt Mary’s Medical Center, WV
September / October 2007Issue 8

That’s the beauty of integrated medical information. The images and reports you need are
at your fingertips and accessible, whenever and wherever you need them. When seconds
matter most, you will be glad that Agfa HealthCare created an integrated Cardiovascular
Image and Information Management Solution that organizes the entire cardiology
patient record at a single point of access. Agfa HealthCare is at work in 1 of every 2
hospitals worldwide, and because our solution is designed by cardiologists, you’ll be
operating with greater efficiency in nearly no time at all.
To learn more about our proven multi-department healthcare solutions,
please visit www.agfa.com/healthcare
Agfa and the Agfa rhombus are trademarks of Agfa-Gevaert N.V. or its affiliates. All rights reserved.
What if you couldaccess both an angiogram
and a chest x-ray in lesstime than it takes to read
this sentence?
AGFA2167_Coronary_Ad_FIN.pdf 8/3/07 10:09:50 AM
CORONARYHEART
CONTENTSSeptember / October 2007
Page: 18
2� Cardiac Site Visit‘Princess of Wales Hospital, Wales, UK’
30 Interview‘Patricia Pye - Carolinas Medical Center, NC’
34 EP Education‘Atrial Flutter’
Page: 09
38 Case Study‘LIMA to What?’
39 Radiation Safety in the Workplace
4� Conferences
47 Employment
04 Editorial
0� Latest News
07 Future
08 Websites
08 ECG Quiz
09 Management‘Creating a Motivated and Loyal Sta� ’
12 Radiation Feature‘Radiation Protection - Best Practices’
14 Radiation Feature‘Radiation Protection - Follow-up on High Dose Procedures’
18 Radiation Dose Reduction‘What the Companies Say’
21 Cardiac Site Visit‘St Mary’s Medical Center, WV, USA’
THIS EDITION
Contents
Radiation Dose Reduction Technology
How to Create a Loyal and Motivated Staff
CORONARY HEART ™ 3
From The EditorWell what a busy last couple of months
it has been. A couple of weeks ago I returned from New Zealand where I attended the Cardiac Society of Australia & New Zealand (CSANZ) Annual Conference. Flying in over the snow capped mountains into Christchurch really felt like a scene out of Lord of Th e Rings. Th e conference though was excellent with a well known international faculty and interesting talks. Everybody I spoke with thoroughly enjoyed it, including the companies whom were well represented.
Another thing that has kept us busy has been the change of this publication to a more common USA size, steering away from the metric A4 you have been used to. Our designers also changed the interior of the magazine, providing readers with a fresh new look.
Th e Special Features in this edition are on Radiation Safety. Our readers and writers have provided some very interesting articles on the subject. Special thanks must be given to the Alliance of Cardiovascular Professionals (ACVP) and Healthworks for their assistance.
Disclaimer:Coronary Heart should never be regarded as an authoritative peer reviewed medical journal. Coronary Heart has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing articles obtained from various companies and contributors, it is not possible to confi rm the accuracy of all statements. Therefore it is the reader’s responsibility that any advice provided in this publication should be carefully checked themselves, by either contacting the companies involved or speaking to those with skills in the specifi c area. Readers should always re check claims made in this publication before employing them in their own work environment. Opinions expressed by contributors are their own and not necessarily those of their institution, Coronary Heart Publishing Ltd or the editorial staff .
Coronary Heart Publishing LtdIndependance Wharf
470 Atlantic Avenue, 4th fl oorBoston, MA 02210
United States
Email: [email protected]: +1 (617) 273-8012
Visit us online at www.coronaryheart.com
Director / Chief EditorTim Larner
Clinical EditorDr Rodney Foale
Consulting EditorsDr Richard Edwards
Ms Voncile Hilson-MorrowMr Ian Wright
Mr Stuart Allen
ADVERTISING
Request Media Kits online
CIRCULATION
USA edition8297 Cardiac Professionals
Copyright 2006 by Coronary Heart Publishing Ltd. All rights reserved.
Material may only be reproduced by prior arrangement and with due acknowledgment of
Coronary Heart Publishing. The publication of an advertisement or product review does not imply
that a product is recommended by Coronary Heart Publishing Ltd.
Tim LarnerDirector
- Tim Larner
Clinical Editor
Dr Rodney Foale, FRCP. FACC. FESC. FCSANZ.Clinical Director, Surgery, Cardiovascular Sciences and Critical Care. SMHT.
COVER PHOTO: Group photo of staff at St Mary’s Medical Center, Huntington, WV, USA
EDITORIAL
Special ThanksE
MP
LO
YMENT
coronaryheart.com
PLLOOLLOO
St Mary’s Medical Center, WV
“Subscribe“Subscribe“Subscribe“Subscribe“Subscribe“Subscribe“Subscribe“Subscribe“Subscribe“Subscribe“Subscribe“Subscribeonlineonlineonlineonlineonlineonlineonlineonlineonline
forforforforforyouryouryouryouryouryour
FREEFREEFREEFREEFREEFREECopy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”Copy!!”
InterviewPatricia Pye - Carolinas Medical Center, NC
How to Create Loyal & Motivated Staff
Management
Radiation ProtectionAtrial Flutter Explained
••
Education
Cardiac Site Visit
September / October 2007Issue 8
coronaryheart.com
September / October 2007Issue 8
coronaryheart.com
Princess of Wales Hospital,Bridgend, Wales
September / October 2007Issue 8
EM
PLO
YMENT
UNITED KINGDOM IRELAND
MMPP
LLOOMM
PPLLO
How to Create Loyal & Motivated Staff
Cath Lab Site Visit
Management
Radiation ProtectionAtrial Flutter Explained
from Ian Wright, St Mary’s Hospital, London
••
Education“Subscribe
onlinefor
yourFREE
Copy!!”
UK / Ireland Edition
USA Edition
4 CORONARY HEART ™

What’s New?
LATEST NEWSCAUTION: Some products within this magazine may be restricted to specific regional usage, and may not be available in your region. Always check with the manufacturer to determine availability.
Thrombus Removal Improves Outcome for DES Patients
A recent study that appeared in the Journal of the American
College of Cardiology (JACC), dated August 14, 2007, showed that patients with no thrombus prior to insertion of a Drug Eluting Stent (DES), resulted in lower rates
of subsequent death, repeat heart attack and stent thrombosis.
In a study of 812 heart attack patients receiving a DES, 28% had a large thrombus that created complications, up to two years after treatment. The study also showed that use of the AngioJet thrombectomy unit developed by Possis to remove thrombus provided results similar to those patients without thrombus to begin with.
You can see how the Angiojet works by visiting www.possis.com
Zoll’s See-Thru CPR Technology
Zoll Medical Corporation recently announced FDA approval to
market its ZOLL AED Pro® with See-Thru CPR™ technology. See-Thru CPR basically works by filtering out compression artifacts that occur during chest compressions. This lets rescuers see a patient’s underlying cardiac rhythm during resuscitation efforts and eliminates the need to stop compressions to see if defibrillation was successful. Visit www.zoll.com
Cleveland Clinic Ranks Number 1 in USA....again
According to the 2007 U.S. News & World Report “America’s
Best Hospitals” survey, and for their thirteenth consecutive year, the Cleveland Clinic’s cardiac care has been ranked number one.
The survey also recognized the Cleveland Clinc as the 4th Best Hospital overall, with twelve of the hospital’s specialities ranked in the Top 10, with the rest in the Top 20.
“At Cleveland Clinic, delivering high-quality, patient-centered healthcare is at the heart of everything we do,” said Delos M. “Toby” Cosgrove, M.D., President and CEO of Cleveland Clinic. “I commend our physicians, nurses and all employees for their
tireless dedication and efforts in putting patients first and providing them with high-quality, compassionate healthcare. The U.S. News survey data provides a useful benchmark as we continue to provide world-class medical care.”
The 18 hospitals selected for the magazine’s 2007 Honor Roll, with Cleveland Clinic ranked No. 4,
“displayed the marked breadth of expertise” and high scores in at least six specialties, according to U.S. News.
So with such a great record you may be asking why Coronary Heart hasn’t performed a Site Visit article yet. You will have to wait until next year, as the hospital is currently building a brand new Heart and Vascular Institute due to be open in the Fall 2008.
An Artist’s Impression of the new Cleveland Clinic Heart & Vascular Institute due to be open in the Fall 2008
CORONARY HEART ™ �

LATEST NEWS
What’s New?Endoscopic Ablation System Achieves CE Mark
On August 1, CardioFocus, Inc. announced it had been
awarded the Eurpean CE mark for its Endoscopic Ablation System. The technology delivers therapeutic light energy through a combination of real-time, full color, endoscopic visualization and guidance. This allows for accurate pulmonary vein isolation for the treatment of atrial fibrillation.
The study co-principal investigator Vivek Reddy of the Massachusetts General Hospital said, “Multiple products are being used to pursue a variety of different strategies, but these
are limited by the inability to directly visualize the tissue being ablated.” The CardioFocus system may have solved this problem.
US Clinical investigations are underway.
For interesting online animations and images visit www.cardiofocus.com
SJM Gets FDA Approval for Transseptal Access
St Jude Medical recently announced FDA approval for the ACross™
Transseptal Access System. The device improves control and simplifies the procedure of accessing the left atrium for procedures such as atrial fibrillation ablation, by consolidating the sheath, dilator and needle into a single interlocking handle.
Visit www.sjm.com for more information.
Siemens add IVUS to their Axiom Artis Range
Siemens Medical Solutions have recently integrated
IVUS technology (intravascular ultrasound) in its imaging systems for X-ray angiography. The system is compatible with the entire Axiom Artis family.
The IVUS operating components are installed directly at the catheter table, allowing for sterile working conditions, and images are seen
directly on the monitor in the exam room.
Visit www.siemens.com for more information
The new CardioFocus Endoscopic Ablation SystemCourtesy: CardioFocus
Image courtesy Siemens
� CORONARY HEART ™
FUTURE
Cardiology in the FutureMedical Nanobots Swimming in Your Blood Soon
This could quite easily be from the script of Star Trek; miniature
robots swimming in your bloodstream to repair vessel damage. But this is no longer science fi ction. Researchers from the Technion and the Hebrew University of Jerusalem in Israel have created a model of a miniature robot capable of self-propulsion inside a viscous liquid.
With a diameter of only 1mm the robot consists of a hub from which tiny arms stretch out, allowing the robot to strongly grip the vessel walls. It is then remotely controlled externally. Although it is still in the early stages of development the technology is already seen as a new device for imaging inside the coronary arteries and possibly delivering drugs directly to the aff ected areas.
Australian Discovery May Have The Cure
Leading the news headlines in Australia recently was the report
that medical experts from the Victor Chang Cardiac Research Institute and Sydney’s St Vincent’s Hospital have successfully used adult stem cells from patients to repair their own dead cardiac tissue.
Th e new treatment uses a hormone drug that is already on the market and is commonly used to assist cancer patients recover after chemotherapy. Th e hormone is injected which releases the benefi cial stem cells from their bone marrow into their bloodstream.
To encourage the stem cells to reach the heart the patient is placed on a treadmill. Eventually they create new blood vessels, restoring circulation to dead or dying heart tissue. Amazingly fi rst results have shown the changes to be permanent.
At present second phase human trials of forty patients in
a double-blind, crossover is underway after passing initial safety tests.
If this technology is found to work after
these trials it will change the face
of cardiology forever.
We will keep you updated.
Paper-Thin Batteries for Pacemakers
Researchers at Rensselaer Polytechnic Institute in New York
have developed a new energy device that could dramatically reduce the size of conventional pacemakers. Th e nanoengineered battery is lightweight, ultra thin, completely fl exible and on fi rst appearance looks like a thin piece of black paper.
Th e device has the unique ability to simultaneously act as a high-energy battery and a high-power supercapacitor and the capability to use human blood or sweat to help power the battery.
90% of the product is made-up of cellulose which is found in nearly every type of newspaper. Th is is then infused with aligned carbon nanotubes giving it the black color. Th e result is a battery with no toxic chemicals and environmentally safe.
Due to the fl exibility don’t be surprised if the actual cases of the pacemakers will actually one-day double as the battery, dramatically reducing its size.
Th e project was outlined in the paper “Flexible Energy Storage Devices Based on Nanocomposite Paper” published Aug. 13 in the Proceedings of the National Academy of Sciences.
CORONARY HEART ™ 7
arteries and possibly delivering drugs directly to the aff ected At present second phase human
trials of forty patients in a double-blind, crossover is underway after passing initial safety tests.
If this technology is found to work after
these trials it will change the face
We will keep you updated.
drugs directly to the aff ected areas.
At present second phase human trials of forty patients in
a double-blind, crossover is underway after passing initial safety tests.
If this technology is found to work after
these trials it will
you updated.
Nanobots: Coming to an artery near you.
Beyond BatteriesRensselaer/Victor Push-
parajnear
WEBSITES
Interesting Websites
StopAfi b.org is the new offi cial website for the American
Foundation for Women’s Health. Started by Mellanie True Hills, heart health expert and author of A Woman’s Guide to Saving Her Own Life: Th e HEART Program for Health and Longevity, Mellanie lived with Atrial Fibrillation. After several episodes of AF and near strokes, eventually Hills underwent surgery to cure her condition.
Th e website is designed for patients
and their families providing information about atrial fi brillation symptoms, causes, risks, and treatments, but also about life-saving options such as catheter ablation and minimally-invasive surgical ablation (Mini-Maze), the heart surgery that Hills had.
Th e site is easy to navigate with an appealing layout and doesn’t get bogged down with complex terminology. Th ere is also a great links page for further information.
Visit www.StopAfi b.org
Do you know of a good website? Email us at [email protected] Quiz
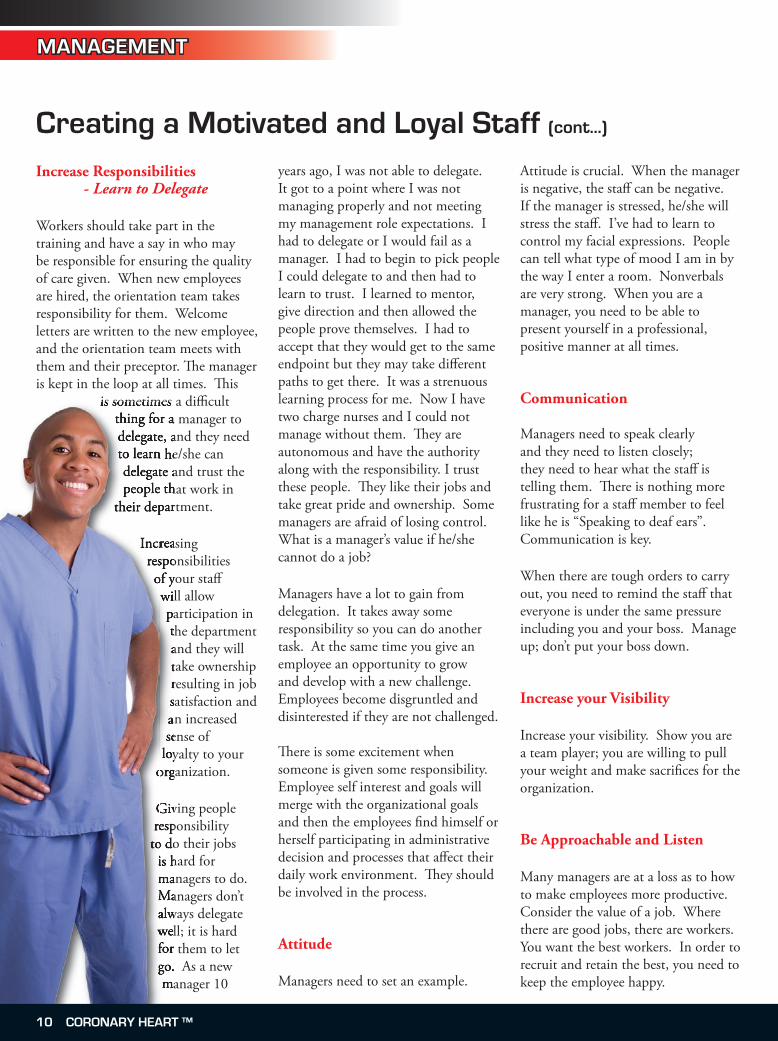
Clue.
77yr female with post CABG intermitant complete heart block. Medtronic ADDRO1 pacemaker
implanted 6 week pacemaker check normal at 2 months post implant attended surgical outpatients and had an episode of collapse. this is the ecg immediately post collapse.
What’s the problem?
Visit coronaryheart.com for answer.
Compiled by: Mr Stuart Allen, Technical Head CRM, Southampton General Hospital, UK
8 CORONARY HEART ™

MANAGEMENT
Creating a Motivated and Loyal Staff
Everyone fi nds value in themselves. Companies that have excelled, teach their
employees that people should be made to feel like they are winners.
Is your approach to your staff as positive as it can be? Do you give positive reinforcement or do you remind them that they are not meeting goals?
Be Supportive
People act in accordance to their image of themselves. If they see themselves as well regarded, they will live up to this standard. A supportive boss is important. Praise, appreciation, respect, new responsibilities, opportunities to learn, authority, and raises, are rewards that play a critical role in your employees’ self esteem and productivity.
People react negatively to attacks on self esteem as a means of self defence, and positively when given positive reinforcement. Th ere is a diff erence between correcting someone and giving someone constructive criticism.
People will surprise you if given the opportunity. Staff that you consider unwilling may emerge with fresh ideas.
Make your expectations clear. Listen and hear suggestions.Consider their new ideas and reward.
You will have some that cannot or will not respond to encouragement
•••
or suggestions. Th ese people should not be exceptions. Goals are set for everyone.
Help Your Staff Grow Authoritarian management has gone by the wayside; newer generations coming into the workforce want to participate and have a say in their work environment. By learning each other’s jobs, there is greater fl exibility. Th ere is room for growth for individuals, which creates a better sense of pride. Newer generations want to participate in meetings and they want to be heard. Shared governance is a new management technique. Managers and staff share in decisions. Opportunity for input exists.
We just obtained Magnet status (an award given by the American Nurses’ Credentialing Center, to hospitals that satisfy a set of criteria designed to measure the strength and quality of their nursing). One of the things that came out of Magnet was “Shared Governance & Unit Councils”. Staff members are voted onto the Unit Council and are the voice of the staff via a suggestion book. Each month there is a council meeting whereby there is a discussion of all issues and possible solutions. Th e chairman of the unit council runs the meeting, not the manager, and everyone takes accountability for the solutions. Th e unit council then communicates back to the staff . It is important that the manager allows this communication to happen, because their input is considered valuable and you are not just going through the motions.
- By Elizabeth Kennedy, Manager Invasive Cardiology, Lankenau and Paoli Hospitals, Main Line Health, Wynnewood, PA
>>
CORONARY HEART ™ 9
MANAGEMENT
Creating a Motivated and Loyal Staff (cont...)
Increase Responsibilities - Learn to Delegate
Workers should take part in the training and have a say in who may be responsible for ensuring the quality of care given. When new employees are hired, the orientation team takes responsibility for them. Welcome letters are written to the new employee, and the orientation team meets with them and their preceptor. Th e manager is kept in the loop at all times. Th is
is sometimes a diffi cult thing for a manager to delegate, and they need to learn he/she can delegate and trust the people that work in
their department.
Increasing responsibilities of your staff will allow participation in the department and they will take ownership resulting in job satisfaction and an increased sense of
loyalty to your organization.
Giving people responsibility
to do their jobs is hard for managers to do. Managers don’t always delegate well; it is hard for them to let go. As a new manager 10
years ago, I was not able to delegate. It got to a point where I was not managing properly and not meeting my management role expectations. I had to delegate or I would fail as a manager. I had to begin to pick people I could delegate to and then had to learn to trust. I learned to mentor, give direction and then allowed the people prove themselves. I had to accept that they would get to the same endpoint but they may take diff erent paths to get there. It was a strenuous learning process for me. Now I have two charge nurses and I could not manage without them. Th ey are autonomous and have the authority along with the responsibility. I trust these people. Th ey like their jobs and take great pride and ownership. Some managers are afraid of losing control. What is a manager’s value if he/she cannot do a job?
Managers have a lot to gain from delegation. It takes away some responsibility so you can do another task. At the same time you give an employee an opportunity to grow and develop with a new challenge. Employees become disgruntled and disinterested if they are not challenged.
Th ere is some excitement when someone is given some responsibility. Employee self interest and goals will merge with the organizational goals and then the employees fi nd himself or herself participating in administrative decision and processes that aff ect their daily work environment. Th ey should be involved in the process.
Attitude
Managers need to set an example.
Attitude is crucial. When the manager is negative, the staff can be negative. If the manager is stressed, he/she will stress the staff . I’ve had to learn to control my facial expressions. People can tell what type of mood I am in by the way I enter a room. Nonverbals are very strong. When you are a manager, you need to be able to present yourself in a professional, positive manner at all times.
Communication
Managers need to speak clearly and they need to listen closely; they need to hear what the staff is telling them. Th ere is nothing more frustrating for a staff member to feel like he is “Speaking to deaf ears”. Communication is key.
When there are tough orders to carry out, you need to remind the staff that everyone is under the same pressure including you and your boss. Manage up; don’t put your boss down.
Increase your Visibility
Increase your visibility. Show you are a team player; you are willing to pull your weight and make sacrifi ces for the organization.
Be Approachable and Listen
Many managers are at a loss as to how to make employees more productive. Consider the value of a job. Where there are good jobs, there are workers. You want the best workers. In order to recruit and retain the best, you need to keep the employee happy.
is sometimes a diffi cult thing for a manager to delegate, and they need to learn he/she can delegate and trust the people that work in
their department.
Increasing responsibilities of your staff will allow participation in the department and they will take ownership resulting in job satisfaction and an increased sense of
loyalty to your organization.
Giving people responsibility
to do their jobs is hard for managers to do. Managers don’t always delegate well; it is hard for them to let go. As a new manager 10
thing for a manager to delegate, and they need to learn he/she can delegate and trust the people that work in
their department.
Increasing responsibilities of your staff
organization.
Giving people responsibility
to do their jobs is hard for managers to do. Managers don’t always delegate well; it is hard for them to let go. As a new
10 CORONARY HEART ™
MANAGEMENT
Creating a Motivated and Loyal Staff (cont...)
It has been proven that most workers will leave their place of employment because of a supervisor. Be approachable and understand where the staff is coming from. Walk the talk. Th is will motivate the staff .
Recognition
Managers need to recognize and appreciate their staff . Positives and public recognition is a great way to show employees you notice their eff orts. Th e employee who does superior work will continue to work at this level when they know it is appreciated and noticed.
Another example of what we do in our department is a “Heart of Gold” board. You are able to write a small note to someone that has gone the extra mile and has made your day a little easier. Positive and public recognition for good behavior or actions goes a long way. Hopefully they will go along for the ride!
Increased TrainingIncreased Salary
It is defi nitely a positive to reward employees for their knowledge. Clinical ladder status employees get an increase in salary according to their level of training.
Maintain Your Authority
While you are taking care of your employees and making them feel valued and appreciated, you need to maintain your authority. Show your employees that you are loyal to them,
your boss, and the organization. If they see the boss has a vested interest in the work place, they will feel confi dent in investing their time and energy as well. Show them you support your boss and you use your boss as a mentor.
Self Evaluation
Evaluate yourself.
Are you approachable? Do you listen and hear, or are you a manager that just runs through the unit and doesn’t really round for outcomes?Do you really care about your employees?
Evaluate your relationships with the people you work with.
How do they view you? Are you open with the people who report to you? Do you give feedback for their ideas after you ask them for participation and suggestions? Are you open minded? Do you try their suggestions or just push them aside?
You need to have an open door policy. Encourage people to come to you. Th is may take time as they need to learn to trust you. Be honest with the people who work with you. I always feel it is better to say someone works “With” you instead of “For” you. I always fi nd a team approach is better.
••
•
••
•
••
Conclusion
In conclusion, these are just some things you can do to create a superior and loyal staff .
Make people feel like they are appreciated and valued. Work with them and credit them for what they do. Participate in staff appreciation activities.
Th e most important thing I feel a manager can do to recruit and retain a loyal and motivated staff is to just treat them the way you would like to be treated, I promise, you will be successful. You are only as successful as the people that work with you!
•
•
•
Th e most important thing I feel a manager can do to recruit and retain a loyal and motivated staff is to just treat them the way you would like to be treated, I promise, you will be successful. You are only as successful as the people that work with you!
Th e most important thing I feel a manager can do to recruit and retain a loyal and motivated staff is to just treat them the way you would like to be treated, I promise, you will be successful. You are only as successful as the people that work with
CORONARY HEART ™ 11
RADIATION FEATURE
Radiation Protection: ‘Best Practices’ for High-Dose Procedures
Now more than ever, healthcare professionals must continually adhere to
standards and policies set forth not only by the organizations in which they practice, but also by external monitoring agencies as well. Due to increasing patient volumes, acuity, and technology, there is a particular need to establish clear care standards in departments such as Radiology, Cardiology, and Nuclear Medicine. Indeed, as in many other specialties, successful Radiologic and Cardiovascular clinicians are challenged to maintain both clinical and regulatory expertise in their day to day practice, which can be difficult as industry advances and new techniques emerge.
Those organizations and departments that are best prepared to meet these challenges have done so through creating a model around Radiation Safety and Protection…a task that might not be so easy. So how can an organization or program develop a policy for radiation protection?
First, clinicians working in a Radiologic environment should ask themselves the following questions...Am I practicing proper Radiation Safety Techniques, not just solely for myself, but for the patient? Do we have an active Radiation Safety Committee? Who is our acting Radiation Safety Officer (RSO)? How often should we be receiving continuing education relative to Radiation Safety and Protection? And, most importantly; what do I need to know and/or do as follow-up for high dose procedures?
For example, in most settings, radiation exposure is reported through a designated Radiation Safety Officer (RSO) to the Radiation Safety Committee and potentially to a State and/or Local Department of Environmental Services. In addition, should a significant “high-dose” exposure resulting in cellular breakdown (such as visible radiation burns) occur, the program may choose to report the incident to the National Council of Radiation Protection and Measurements (NCRP).
This article is intended to raise awareness and provide insight to Radiation Safety practices that clinicians may take for granted, or those that they may not be aware of.
Nurses or Technologists who practice in a controlled environment providing simple X-Rays need adhere to Radiation safety policies and must be cognizant of exposures to the patient as well as to themselves. There are three fundamental radiologic principles: Time, Distance, and Shielding (see figure 1). In Corazon’s experience, these fundamentals of radiation safety are often taken for granted
during simple Radiologic procedures, which can be attributed to the latest technological advances such as digital technologies and the ability for the X-Ray beam to be more focused (inherent automatic collimation). Often, the hustle and bustle of departmental schedules results in neglect or even failure to consider these basic fundamental principles.
In “specialized” settings, such as with Cardiac Catheterizations or Peripheral Vascular Angiograms, the radiation exposure is significantly increased compared to simple X-rays, which is attributed to longer fluoroscopy and multiple cine runs. Consideration must be taken to protect not only those performing the procedures, but also the personnel that may enter this setting at any given time. Typically, the Radiologic Technologist or Physician is accountable to adhering to Radiation Safety and Protection guidelines, but organizations can designate another responsible party. It is vital that these professionals remain cognizant of unnecessary exposure, especially to those individuals of child-bearing age.
The person responsible for maintaining
Radiation Basics: Three Fundamental Principles
Time Reduce the amount of time spent near the radioactive material/source
Distance Increase the distance from the radiation source
Shielding Use appropriate protective shielding whenever possible
- Amy J. Newell, BS, R.T. (R)
12 CORONARY HEART ™
RADIATION FEATURE
safe radiologic practices should ask the following questions:
Is everyone in the room dawning appropriate lead apparel?
Are extra precautions such as Thyroid collar, lead glasses, and portable lead barriers being utilized?
Is there extra lead apparel for ancillary personnel or vendors who may need to enter the procedure?
Is the operator of the flouro pedal providing a verbal notice so that personnel can move at least six feet from the X-ray tube?
Are all personnel in the procedure wearing film badges for individual dosimetry monitoring, and is it being worn in the appropriate location? (On the outside of the Thyroid collar)
Neglect in wearing any of these protective devices is not only unsafe practice, but will not allow for accurate exposure monitoring.
Corazon recommends that organizations performing procedures using Ionizing Radiation have a Radiation Safety Committee. These organizations should also designate an individual to act as the Radiation Safety Officer (RSO). It is through this committee and/or individual that healthcare professionals are monitored, educated, and re-assigned should someone encounter an unexpected “high dose” exposure. Furthermore, this committee or the RSO should be charged with creating and revising policies regarding Radiation protection and safe practices. In many organizations, it is the goal of Radiation Safety Committee to
•
•
•
•
•
adapt and implement the ALARA philosophy (see figure 2). Adherence to the ALARA philosophy should result in “low” to “no” incidence of radiation exposure.
The RSO should also be charged with providing or coordinating radiation safety education to all technical, nursing, and ancillary support personnel who may be involved in these procedures. We advocate that radiation safety and protection education be held annually through classes geared toward the ALARA philosophy and the fundamental principles of Time, Distance, and Shielding. The RSO should include as part of the education component any regulatory changes that are vital to personnel involved in Cardiac Catheterizations and Peripheral Vascular procedures.
In conclusion, Corazon challenges all professionals involved in these procedures to adhere to safe radiation practices, despite the challenges imposed by changing technology, new techniques and staffing shortages. It is also critical to know the reporting “chain of command” within the organization should any personnel fall victim to a “high dose” exposure. In our experience across the country, best practice programs consistently demonstrate the fundamental principles of Time, Distance, Shielding, as well as the ALARA philosophy. Indeed, the more programs that make significant strides in this area, the safer and more effective their Radiology Departments will become.
Referenced: http://www.colorado.edu/EHandS/hpl/RADHandbook/Table_of_Contents.html
Amy is a Senior Consultant at Corazon, a national leader in specialized consulting and recruitment services for cardiovascular program development. Corazon combines strategic business planning, market and financial analysis, feasibility studies, clinical operations, program implementation support, Heart Hospital design, best practice benchmarking, executive search, and staff / leadership education for newly established or existing heart and vascular programs. To contact Amy, email [email protected] or call 412-364-8200. Visit www.corazoninc.com for more information about Corazon.
The ALARA Philosophy
A As
L Low
A As
R Reasonably
A Achievable
CORONARY HEART ™ 13
Radiation Protection
RADIATION FEATURE
A Primer on the “Follow-up of High Dose Fluoroscopy Procedures”
In the last 30 years of practice as a Cardiovascular Technologist in the Cardiac Catheterization
Laboratory, I have seen the technology behind the x-ray equipment advance, from using high dose 90 frames/sec imaging to today’s Digital Flat Panel technology using a mere 15 frames/sec imaging technique.
With the advance of this technology, we have gone from using x-ray (fluoroscopy) as a Diagnostic tool, to using it to do complicated and sometimes prolonged interventional procedures, such as PCI, Ablation, and other procedures that use fluoroscopy to aid in the treatment of patients. As Healthcare providers and thusly patient advocates we must be ever vigilant of the amount of fluoro our patients receive.
As we are not able to see, feel, smell, or hear x-ray we must rely on our equipment settings and thusly the service engineers and radiation physicist to maintain proper dose parameters, to ensure patients are not overly exposed to ionizing radiation. Therefore, a schedule of regular preventative maintenance and calibration is needed to ensure equipment is meeting government regulations.
Even with these protocols in place, one you can still deliver an excessive dose if you don’t pay attention to the total time of fluoroscopy during procedures. Many factors influence the final dose the patient receives, such as; the patients size, small vs obese , the larger the patient the more the x-ray must
adjust to produce high-quality images, the angles used to perform the imaging AP vs lateral which requires more energy to produce high quality images. Other factors that increase the risk of skin injury are,ie: Diabetes, connective tissue collagen disease increase risk along with repeat procedures involving the same area or entry site of the x-ray beam. As you see many factors increase risk, of which not all are mentioned here.
In 1990 the “Safe Medical Devices Act of 1990” was enacted to better track and report injury to patients. With mandatory reporting requirements came verifiable information as to the circumstances of injuries related to fluoroscopic x-ray systems and procedures related to the use of fluoroscopy. The data began to show a relationship between the length of procedures to increased fluoro times, and injuries.
The rest of this article presents a model or set of protocols for pre Procedure, During Procedure, and Post Procedure, for patients having fluoroscopic procedures, the documentation of prolonged fluoro times, and follow-up with the patient, who may have incurred an injury due to the procedure.
PRE PROCEDURE
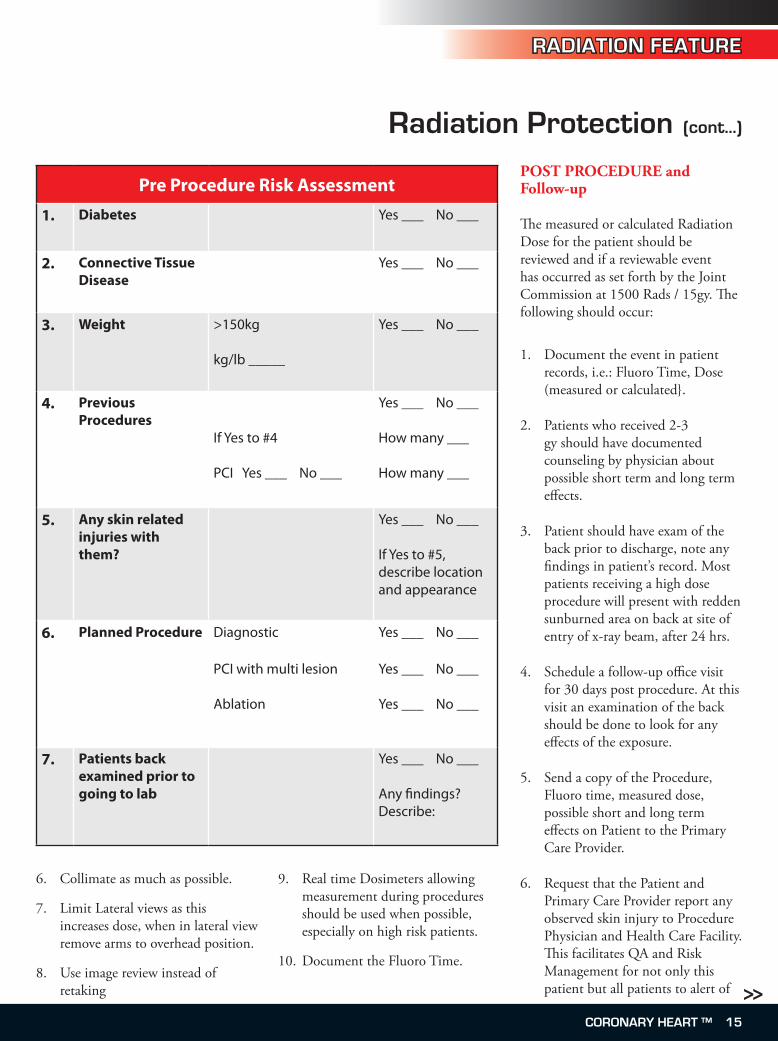
Pre procedure risk assessment and discussion with patient as part of the informed consent process is vitally important. The process should include a pre-check list as exampled below:
The above is just an example of what to include as a risk assessment tool and does not include everything, each Healthcare Facility must develop a tool, using clinical staff, Physicians, and risk management department to cover what you need specifically. The informed consent should also cover this in the listed risks as part of the document. Ensuring the Procedure Physician is made aware of the above will help to reduce the overall procedure risk with better planning as a result.
DURING PROCEDURE
The Procedural Physician and support staff must keep up with the accumulating dose during the procedure using the fluoro time and monitoring the dose rates displayed. Advising the Physician that 75% of 1500 rads dose is approaching gives the operator the time to stop the procedure and evaluate the status and whether to continue or not. Listed below are points to remember keep dose levels low:
Keep patient as far away from x-ray tube as possible.
Lower Image tube as close to patient as possible.
Small Image Magnification and high detail modes should be avoided.
Use variable pulsed fluoroscopy and minimal frame rates.
Limit the amount of time working in one angel with beam entry site unchanged.
1.
2.
3.
4.
5.
- William B. McCurry, RCIS
14 CORONARY HEART ™
RADIATION FEATURE
Radiation Protection (cont...)
Collimate as much as possible.
Limit Lateral views as this increases dose, when in lateral view remove arms to overhead position.
Use image review instead of retaking
6.
7.
8.
Real time Dosimeters allowing measurement during procedures should be used when possible, especially on high risk patients.
Document the Fluoro Time.
9.
10.
POST PROCEDURE and Follow-up The measured or calculated Radiation Dose for the patient should be reviewed and if a reviewable event has occurred as set forth by the Joint Commission at 1500 Rads / 15gy. The following should occur:
Document the event in patient records, i.e.: Fluoro Time, Dose (measured or calculated}.
Patients who received 2-3 gy should have documented counseling by physician about possible short term and long term effects.
Patient should have exam of the back prior to discharge, note any findings in patient’s record. Most patients receiving a high dose procedure will present with redden sunburned area on back at site of entry of x-ray beam, after 24 hrs.
Schedule a follow-up office visit for 30 days post procedure. At this visit an examination of the back should be done to look for any effects of the exposure.
Send a copy of the Procedure, Fluoro time, measured dose, possible short and long term effects on Patient to the Primary Care Provider.
Request that the Patient and Primary Care Provider report any observed skin injury to Procedure Physician and Health Care Facility. This facilitates QA and Risk Management for not only this patient but all patients to alert of
1.
2.
3.
4.
5.
6.
Pre Procedure Risk Assessment
1. Diabetes Yes ___ No ___
2. Connective Tissue Disease
Yes ___ No ___
3. Weight >150kg
kg/lb _____
Yes ___ No ___
4. Previous Procedures
If Yes to #4
PCI Yes ___ No ___
Yes ___ No ___
How many ___
How many ___
5. Any skin related injuries with them?
Yes ___ No ___
If Yes to #5, describe location and appearance
6. Planned Procedure Diagnostic
PCI with multi lesion
Ablation
Yes ___ No ___
Yes ___ No ___
Yes ___ No ___
7. Patients back examined prior to going to lab
Yes ___ No ___
Any findings? Describe:
>>CORONARY HEART ™ 1�
RADIATION FEATURE
Radiation Protection (cont...)
any trends in practice.
All reporting to Hospital Risk Management, JACHO and FDA should be carried out as required here in the United States.
Treatment Plans should be in place to handle effects on patient, and implemented as soon as any adverse reactions are noticed. Standard care for wound in these patients can be from cleaning and applying ointment on the simple case of erythemic reaction to skin grafting on the very worst case scenario.
The above is just a suggested way to follow-up with a High Dose procedure. Using this as starting point develop a protocol for your institution with help from areas to include Nursing, Procedure staff, Risk Management, Radiation Physicist, and Physicians to design a plan that includes Pre procedure assessment, during procedure protocols to minimize exposure, post procedure for documentation and follow-up of patients having a high dose procedure. Here in the U.S. the Joint Commission on Healthcare Organization (JCAHO} has identified tracking a cumulative fluoroscopy dose
7.
8.
of 1500 rads / 15 gy as a”reviewable sentinel event”. From the JCAHO position statement:
2006 Sentinel Event list includes:
Surgery on the wrong individual or wrong body part.
Unintended retention of a foreign object in an individual after surgery or other procedure.
(Unintended) Prolonged fluoroscopy with cumulative dose > 1500 rads (15gy) to a single field, or any delivery of Radiotherapy to the wrong body region or>24% above the planned radiotherapy dose.
This event could be associated with death or major permanent loss of function. Outcomes often do not occur for months or years after the event itself. This event is considered to be preventable. The organization is required to conduct a root cause analysis and is encouraged to voluntarily report the event to the Joint Commission, even though the outcome has not yet become evident. As with all sentinel events, the intent is to analyze. Learn from, and share knowledge about the event, its causes, and strategies for prevention.
•
•
•
As it relates to fluoroscopy, the specification of “1500 rads to a single field” refers to a location on the skin through which the fluoroscopic beam is directed. The issue here is the magnitude of the dose to that portion of the skin that receives the maximum or peak skin dose. This may be the situation that results from using several x-ray beam projections or fields- of-view whose beam areas on the patient’s skin overlap in a specific location to produce a region of highest radiation dose. In fluoroscopically-guided interventional procedures, many different projections or x-ray beam directions are often used, with many overlapping fields-of-view or imaged areas.
Reporting these events should be carried out in a timely manner to all regulatory agencies by the appropriate department in your facility.
Summary
With the importance of fluoroscopy in patients having Interventional procedures, this valuable tool must be used judiciously to optimize patient radiation dose. The Healthcare community, including clinical staff, physicians, manufactures, and regulatory agencies must work together
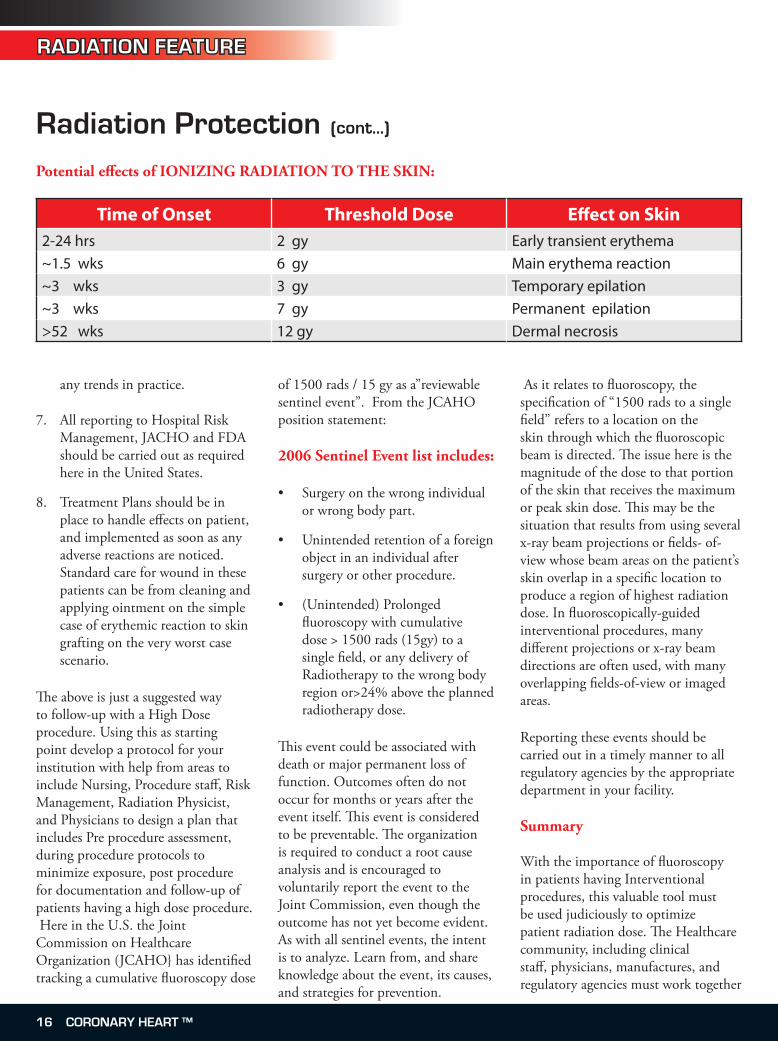
Time of Onset Threshold Dose Effect on Skin2-24 hrs 2 gy Early transient erythema~1.5 wks 6 gy Main erythema reaction~3 wks 3 gy Temporary epilation~3 wks 7 gy Permanent epilation>52 wks 12 gy Dermal necrosis
Potential effects of IONIZING RADIATION TO THE SKIN:
1� CORONARY HEART ™
RADIATION FEATURE
Radiation Protection (cont...)
to bring about education, QA on equipment, procedure processes and reporting events to better care for our patients so as to do no harm. As this article has not covered all the topics and possibilities but is merely an overview to stimulate the mind for you to look at your practice and work processes for ways to improve patient care and thus outcomes in the future. For many articles with pictures and case studies on the internet search for:
RADIATION SKIN INJURY
References
Public Law 101-629, The Safe Medical Devices Act of 1990.
1.
Wagner LK, Eifel PJ, Geise RA, Potential Biological Effects following High X-ray Dose Interventional Procedures, JVIR 1994; 5:71-84
Food and Drug Administration, Important information for Physicians and other Healthcare Professionals; Recording Information in the Patients Medical Record That Identifies the Potential for serious X-ray Induced Skin Injuries Following Fluoroscopically Guided Procedures. September 15, 1995. Rockville, MD, Center for Devices and Radiological Health, FDA, 1995
Stephen Balter, PHD, Interventional Fluoroscopy:
2.
3.
4.
Patient and Staff Safety, as presented at AAPM annual meeting in Minneapolis, Mn. 2007
Trott K. Kummermehr J, Radiation effects in skin, In: Scherer E, Streffer C, Trott K, eds Radio pathology of Organs and Tissues. Berlin: Springer-Verlag, 1991;33-66
Wagner LK, Archer BR, Cohen AM, Management of patient skin does in fluoroscopically guided interventional procedures. JVIR 2000; 11:25-33
Joint Commission on Accreditation of Healthcare Organization 2006
5.
6.
7.
450 Veit RoadHuntingdon Valley, PA [email protected]
Profit from Platinum.You Already Have.
Profit from Platinum.You Already Have.
A used EP Catheter Tiphas VALUE.
Just snip it, ship it and
profit.
Call us for details: 1.800.396.9998
CORONARY HEART ™ 17
RADIATION DOSE
Radiation Dose Reduction
What the companies say
Dose Reduction Technology?
Philips’ SpectraBeam fi ltration is used to reduce patient and staff doses during all fl uoroscopic examinations and some digital acquisition programs. It is always present regardless of patient size. Philips also uses: x-ray tube controlled grid switched pulsed fl uoroscopy, 3.75 and 7.5 pulse rate fl uoroscopy protocols, Last Image Hold (LIH) based beam collimation, fl uoro store, single shot acquisition and radiation shielding technologies to further reduce dose to patients and staff . How does it work?
SpectraBeam pre-fi lters, automatically inserted in the beam, protect patients from low energy radiation. Th is dose reducing fi ltration is integral to the x-ray tube collimator and is a programmable component of Philips’ Xper technology. Based on procedure type, 0.2mm, 0.5mm or 1.0mm Cu equivalent fi lters eliminate non-image forming from the patient. Philips’ grid switched pulse fl uoroscopy removes typical ramps and tails of each pulse to further reduce patient radiation. Th e ability to position x-ray shutters and compensating fi lters on a LIH image, store fl uoro sequences and use high quality single shot digital acquisitions also reduce patient dose.
Dosimetry?
Philips complies with current IEC
and some digital acquisition programs.
single shot acquisition and radiation
SpectraBeam pre-fi lters, automatically inserted in the beam, protect patients
to the x-ray tube collimator and is a programmable component of Philips’ Xper technology. Based on procedure type, 0.2mm, 0.5mm or 1.0mm Cu equivalent fi lters eliminate non-image forming from the patient. Philips’ grid switched pulse fl uoroscopy removes typical ramps and tails of each pulse to further reduce patient radiation. Th e ability to position x-ray shutters and compensating fi lters on a LIH image, store fl uoro sequences and use high quality single shot digital acquisitions
standards. A Dose Area Product (DAP) meter displays real time air kerma (mGy) and accumulated exposure data (mGycm2) on the procedure room monitor. A post procedure Patient Dose Report is available. International Availability?
Philips’ dose control technologies are available in all markets / countries.
Other products available to reduce Dose?
Philips’ new Quick Reference Dose Display provides in progress air kerma (mGy/min), accumulated and predicted skin dose values. A graphical display shows real-time accumulated dose against a 2.5 Gy limit in ten patient skin zones.
Image courtesy Philips
18 CORONARY HEART ™

RADIATION DOSE
Radiation Dose Reduction (cont...)
by automatically selecting all x-ray technique factors and spectral fi ltration according to the selected application protocol and actual patient attenuation, which is measured automatically. AutoExÔ also calculates and displays dose rate and cumulative dose to the patient, in mGy/min and mGy respectively, at the Interventional Reference Point. Dose Reduction Technology?
GEHC employs many key technologies and system features to minimize patient and staff dose per the ALARA (As Low As Reasonably Achievable) principle on the Innova family of products. Th e high continuous power x-ray tube (3.2kW), combined with multiple values of spectral fi ltration, provide an optimally hardened x-ray beam that reduces patient skin dose. Th e GE Flat Panel Detectors have the highest Detective Quantum Effi ciency (DQE) in the industry, particularly in fl uoroscopy, thereby maximizing the imaging information acquired at any exposure level used, which in turn allows for dose reduction.
System features include Virtual collimation; Patient Contouring (automatically mimimizes SID), Fluoro Store; acquisition protocols that can be individually programmed with the desired dose levels, frame rates, and image processing parameters; and image Dynamic Range Management (DRM), which prevents “white- and black-out” areas in the image, thereby reducing retakes.
How does it work?
Th e AutoExÔ exposure control system maximizes the image quality achieved in each of the wide range of dose and fl uoro frame rate choices
Dosimetry?
Dose-Area Product (DAP) is reported in cGy-cm2. Th ese values are displayed for clinican and staff and can be added to the patient electronic data record.
International Availability?
All of the above features are available in all markets globally, albeit
with modifi cations to meet local regulatory requirements.
in all markets globally, albeit with modifi cations to
meet local regulatory requirements.
Image courtesy GE
CORONARY HEART ™ 19

RADIATION DOSE What the companies say
Radiation Dose Reduction (cont...)
Siemens uses a package called CARE- Combined Applications to Reduce Exposure in Cardiac Angiography.
Dose Reduction Technology?
Automatic exposure control provides for optimized exposure conditions without test shots.
Low energy fi ltration with a beam hardening copper fi lter concentrates X-radiation to the useful portion of the spectrum, thus improving image quality. Th e adaptive dose fi lter not only signifi cantly reduces skin dose to the patient, but the scattered radiation to the physician as well.
All Artis Systems have removable grids.
How does it work?
During fl uoroscopy the copper fi lter is always moved into the X-ray beam thereby reducing the skin dose to the patient. Th e automatic dose control of the system calculates the patient’s water equivalent from the actual kV/mA and pulse width values during fl uoroscopy. Depending on this value the appropriate fi lter is automatically moved into the beam during acquisition for the optimum image quality. Th e selection of this fi lter is automatic through the automatic exposure control.
•
•
•
Dosimetry?
Dose-Area Product (DAP) is reported in cGycm². During fl uoroscopy the actual value of skin dose is displayed on the monitor suspension. Th e integral Area Dose Product (fl uoroscopy and radiography) is also displayed at the central system console and on the LCD display on the DCS.
Other products available to reduce Dose?
CAREVISION - provides pulsed fl uoroscopy of 0.5; 1.0; 2.0; 3.0; 4.0; 6.0, 7.5 pps.
FLUORO LOOP – provides the storage and display of dynamic fl uoro sequences, 300 images can be stored
•
•
CAREPOSITION – provides radiation-free positioning via graphic display of the central X-ray beam and image edges in the LIH image on the image monitor.
ECG Triggered Fluoroscopy
International Availability?
Siemens’ dose control technologies are available in all markets / countries.
•
•
CAREVISION - provides pulsed fl uoroscopy of 0.5; 1.0; 2.0; 3.0; 4.0; 6.0, 7.5 pps.
FLUORO LOOP – provides the storage and display of dynamic fl uoro sequences, 300 images can be stored
•
Image courtesy Siemens
20 CORONARY HEART ™
CARDIAC SITE VISIT
St Mary’s Medical Center
St. Mary’s Medical Center, located in Huntington, W.Va., is a 393 bed tertiary care facility that
provides quality, compassionate health care to its surrounding community. Founded in 1924 by the Pallottine Missionary sisters, St. Mary’s has grown to become West Virginia’s second-largest health care facility. As a regional tertiary care facility, St. Mary’s provides advanced care
through its centers of excellence in cardiac, oncology, ER/trauma, and neuroscience services. St. Mary’s is West Virginia’s only Joslin Diabetes Center education affi liate. Th rough its many residency programs and fellowships, St. Mary’s is affi liated with Th e Joan C. Edwards Marshall University School of Medicine. Th e St. Mary’s School of Nursing, School of Medical Imaging, and School of Respiratory Care are also located on the St. Mary’s campus.
Size of the Department:
St.Mary’s has three cath labs and one electrophysiology lab. Th e newest of the three cath labs was designed and equipped for peripheral angiography
and intervention. Adjacent to the cath labs is the Invasive Cardiology Unit, where procedure preparation and recovery is performed. Th is is a 24-bed department consisting of 11 overnight private patient rooms, seven preparation/recovery private rooms, and a six-bed open holding area. Th e department operates 24 hours daily starting at 6 a.m. Monday morning and closing at 11 p.m. Friday night. Th e main goal when designing this unit was to provide patients with the convenience of being prepped, recovered, and discharged from the same room. Th e patients’ satisfaction with the facility and their care are refl ected in the surveys they complete and return.
ADDRESS
MAP
St. Mary’s Medical Center2900 First AvenueHuntington, WV 2�702United States of America
FAST FACTS
Second largest hospital in West Virginia.
3 Cath Labs and 1 EP Lab.
Open 24 Hours.
Over �000 procedures per year.
1.
2.
3.
4.
UNITED STATES OF AMERICA
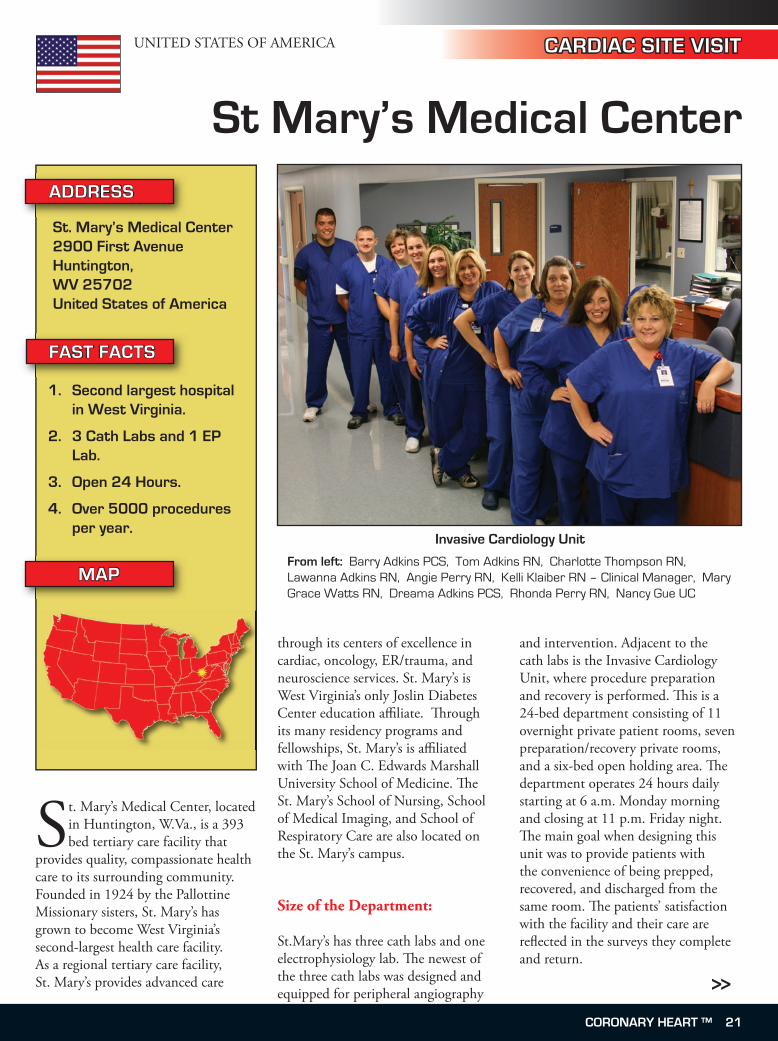
Invasive Cardiology Unit
From left: Barry Adkins PCS, Tom Adkins RN, Charlotte Thompson RN, Lawanna Adkins RN, Angie Perry RN, Kelli Klaiber RN – Clinical Manager, Mary Grace Watts RN, Dreama Adkins PCS, Rhonda Perry RN, Nancy Gue UC
>>
CORONARY HEART ™ 21
St Mary’s Medical Center (cont...)
CARDIAC SITE VISIT
Staff numbers and roles:
Cath Lab / EP Lab 1 – manager 1 – secretary 1 – nurse aide 1 - transcriptionist 11 – RNs 10 – RTs
RNs – Administer all medications. They can circulate, record and scrub during procedures.
RTs – Record and scrub during procedures.
Nurse Aide – Stock supplies, transporting patients.
Secretary – Enter charges, scheduling of procedures, customer relations.
Transcriptionist – Monitor procedure
and equipment charges, transcribe procedure reports.
Invasive Cardiology Unit: 1 – clinical manager 3 – unit clerks 4 – patient care specialists 14 – RNs 1 – part time RN 1 – per diem RN This area is responsible for all patient preparation and recovery. Outpatients requiring overnight stay are cared for here and subsequently discharged. Hemostasis is managed in this area.
Procedures:
Cath lab – diagnostic coronary and peripheral angiography, right heart catheterizations, coronary and peripheral interventions, coronary
brachytherapy, alcohol septal ablations, PFO closures, valvuloplasties, pericardiocentesis, endografts.
EP lab – Electrophysiology studies, ablations, device implants, cardioversions
Equipment:
Witt Hemodynamic Monitoring and Recording Systems, Philips x-ray equipment, EP Med System, Boston Scientific RPM Mapping System, Site Rite, IVUS, Radi Pressure Wire, Polarcath, Angiojet, Rotablator, DES, and BMS.
Day Procedures:
We perform elective outpatient procedures Monday – Friday.
Procedures performed per year:
We performed more than 5,100 procedures last year.
Cross-Training:
The Cath lab staff members are cross-trained to work in the EP Lab if interested. The Cath lab staff and the Invasive Cardiology Unit staff are not cross-trained.
Staffing roles:
Cath lab – charge person – responsible for staff coordination, and facilitating efficient patient flow through the labs.
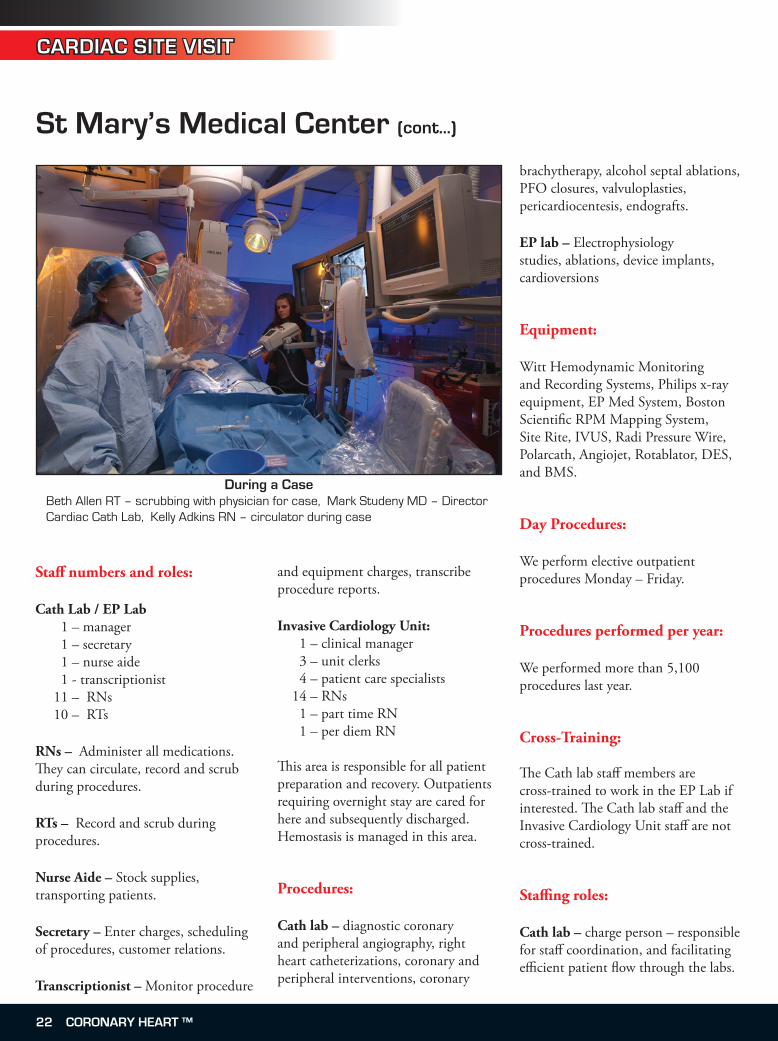
During a CaseBeth Allen RT – scrubbing with physician for case, Mark Studeny MD – Director Cardiac Cath Lab, Kelly Adkins RN – circulator during case
22 CORONARY HEART ™

CARDIAC SITE VISIT
St Mary’s Medical Center (cont...)
RNs – administering all medications and monitoring the patient. They can scrub and complete the required documentation of the procedures.
RTs – one technologist must be in the department for the X-ray equipment to be used. They can scrub, monitor the patient’s hemodynamic status, and complete the required documentation for the procedures. The lead RT position has multiple responsibilities including functioning in the charge role. EP lab – the lead EP position has multiple responsibilities including coordination and direction of staff, developing policies and procedures, monitoring charges for procedures and equipment. Otherwise, RN and RT roles in this room are the same as that in the cath lab.
Surgical Back-up:
We always have cardiovascular surgery back-up available if needed. The need for emergent surgery is very rare. It is usually reserved for unstable high-grade left main stenosis or septal rupture in Acute MI.
Our Cath Lab is available 24 hours every day. We recently joined a national initiative to provide the best chance of survival for STEMI. A Door To Ballon Team was formed to initiate new practices and we have demonstrated GREAT success! Our goal is to open all our STEMI patients’ blocked arteries within 90 minutes of arrival to our ED.
Inventory Management:
The inventory is managed by a dual process. Normal medical supplies (example: solutions, gauze, gloves) are managed by a stockless program. Early each morning a supply clerk, with a handheld device, will check to make sure all items are at par levels. The under par items are then transmitted to our stockless vendor. By mid-morning the under par items are delivered and stocked on the shelves.
For our high dollar items, (example: stents, balloons, guide wires) we have a purchasing agent that is dedicated to the cath lab. The agent works with the staff and doctors on what items and quantities are needed.
We use the Witt System to track item usage. Par levels are set in Witt and ordering is done from the inventory side of the program. Ordering is done every day for replacement of high dollar items.
Hemostasis Management:
The majority of our cases have their sheaths pulled and manual pressure held. Some physicians will use closure devices. The devices that are used most frequently are Angioseal and Perclose. When manual pressure is held there are a couple options available that we consider “hemostatic aides.” The Safeguard and various hemostatic patches are available for use by physician order. If problems with hemostasis occur, we have the Femostop available for use. Managing hemostasis in the Invasive Cardiology Unit allows efficient patient flow to be maintained through the lab. With the exception of those patients that receive a closure device, the majority of patients have their sheaths removed in this area.
Regional Heart Institute
>>
CORONARY HEART ™ 23

CARDIAC SITE VISIT
St Mary’s Medical Center (cont...)
We have a hemostasis management performance improvement project. The day following the procedure a staff member will visit patients, observe forcomplications, and provide instructions on arterial access site care. A sticker is placed on the chart to document the visit and to describe arterial access site findings. If any complications are identified steps are taken to obtain appropriate testing and treatments.
Private cases:
Only physicians that have received privileges can perform procedures in our facility. Unattached patients who present to our ED will have a physician assigned based on a rotating unattached patient list.
Measures implemented to cut costs:
We work to supply our doctors with the best and most up-to-date equipment and supplies on the market. The director of material management and staff diligently work to get the best pricing available on all items. We have the Premier Contract, which is a group of hospitals in West Virginia that meet and work together to get the best pricing for all hospitals. We also try to buy bulk items from companies across division lines to lower their pricing. Consignment is utilized so we do not tie up large amounts of dollars on the shelves. The purchasing agent in the cath lab negotiates with sales representatives regularly to get lowest pricing possible.
Alliances with other hospitals for the treatment of patients:
We accept patients from surrounding hospitals who need treatment or a specialty service that the referring facility may not offer. There is a competitive market for patients in our area so we work very hard on developing good relationships with surrounding facilities. We recently opened a referral center to make the process easier, more efficient and convenient for the referring facility and patient.
Training for new employees:
New employees can expect a 4 – 6 week orientation with a preceptor. The length of orientation depends on the employee’s past experience. There is a competency checklist that must be completed by the end of orientation. The employee will undergo a performance evaluation 90 days after hire.
Continuing education programs for the staff:
Many continuing education opportunities are offered throughout the year. Vendors visiting the cath lab also provide education for staff. Monies are set aside each year to send staff to outside conferences.
Competency checks for staff:
All JCAHO mandatory competencies are evaluated annually by computer testing. There is department specific competency testing that is done by
Cath Lab Staff
From front left: Kelli Klaiber RN – Clinical Manager - Invasive Cardiology Unit, Jill Richbart – Clinical Manager - Cardiac Cath Lab, Marlena Perry RN, Tara Goff RT, Cindy Castle RT, Toni Madden RT, Kim Phillips RT, Mica Hicks RT, Gina Dixon RN, Garon Dent RN, Mark Freeman RN, Sean Wilson RN
24 CORONARY HEART ™
CARDIAC SITE VISIT
St Mary’s Medical Center (cont...)
computer. Any skill that has to be observed is done during planned “Skill’s Days” by the Organizational Development and Learning Department. Th ere are other unit-specifi c competencies that must be completed in the departments.
Training facility for cardiac fellows:
Our hospital is affi liated with Joan C. Edwards Marshall University School of Medicine, which has a cardiology fellowship program.
What is the best part of working at your facility:
Th e foundation upon which Th e Pallottine Missionary Sisters formed St. Mary’s still guides our actions today. At St. Mary’s our core values refl ect what we stand for, what we expect from each other, and what we aspire to be. Th e sisters remain a visible presence in our facility today. Our values will guide us as we continue our tradition of excellence and dedication to provide quality healthcare in ways which respect the God-given dignity of each person and the sacredness of human life.
Th e Values of St. Mary’s Medical Center: Compassion, Hospitality, Respect, Interdependence, Stewardship, Trust.
Huntington is the second largest city in West Virginia and with wide tree-lined
streets and avenues creates a natural “Home Town” feel. The cities history was tied to the railroad and today it is possible to take interesting excusions into the surrounding hills and gorges. Explore the seventy acre Ritter Park where the locals play, or head down to the Harris Riverfront Park where there is a weeklong Summerfest river celebration. With a multi-cultural population of only �0,000, this small city continues to develop with the latest in retail, entertainment, and of course medical facilities.
WHY HUNTINGTON?
CORONARY HEART ™ 2�
CARDIAC SITE VISIT
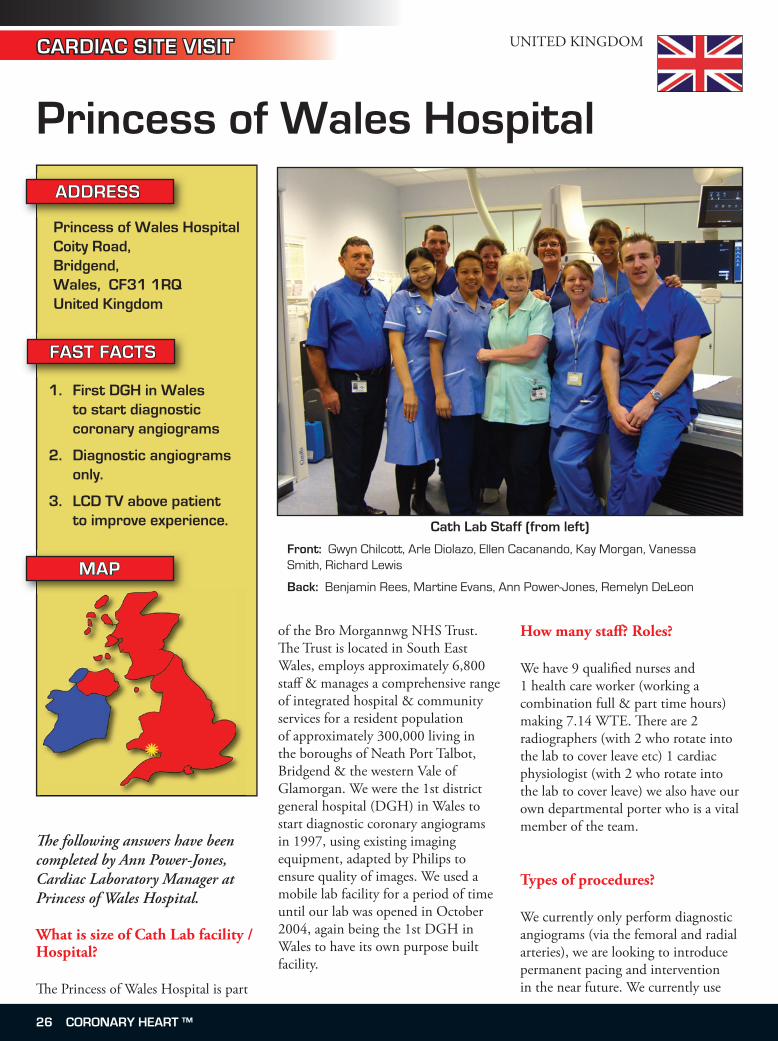
Princess of Wales Hospital
Th e following answers have been completed by Ann Power-Jones, Cardiac Laboratory Manager at Princess of Wales Hospital.
What is size of Cath Lab facility / Hospital?
Th e Princess of Wales Hospital is part
of the Bro Morgannwg NHS Trust. Th e Trust is located in South East Wales, employs approximately 6,800 staff & manages a comprehensive range of integrated hospital & community services for a resident population of approximately 300,000 living in the boroughs of Neath Port Talbot, Bridgend & the western Vale of Glamorgan. We were the 1st district general hospital (DGH) in Wales to start diagnostic coronary angiograms in 1997, using existing imaging equipment, adapted by Philips to ensure quality of images. We used a mobile lab facility for a period of time until our lab was opened in October 2004, again being the 1st DGH in Wales to have its own purpose built facility.
How many staff ? Roles?
We have 9 qualifi ed nurses and 1 health care worker (working a combination full & part time hours) making 7.14 WTE. Th ere are 2 radiographers (with 2 who rotate into the lab to cover leave etc) 1 cardiac physiologist (with 2 who rotate into the lab to cover leave) we also have our own departmental porter who is a vital member of the team.
Types of procedures?
We currently only perform diagnostic angiograms (via the femoral and radial arteries), we are looking to introduce permanent pacing and intervention in the near future. We currently use
ADDRESS
MAP
Princess of Wales HospitalCoity Road, Bridgend, Wales, CF31 1RQUnited Kingdom
FAST FACTS
First DGH in Wales to start diagnostic coronary angiograms
Diagnostic angiograms only.
LCD TV above patient to improve experience.
1.
2.
3.
UNITED KINGDOM
Cath Lab Staff (from left)
Front: Gwyn Chilcott, Arle Diolazo, Ellen Cacanando, Kay Morgan, Vanessa Smith, Richard Lewis
Back: Benjamin Rees, Martine Evans, Ann Power-Jones, Remelyn DeLeon
2� CORONARY HEART ™
CARDIAC SITE VISIT
Princess of Wales Hospital (cont...)
our facility for temporary pacing wire insertion during office hours.
Procedures performed in a year?
Approximately 1300
Types of equipment
Siemens Axiom Artis (Monoplane)GE Mac Lab
Day cases?
All patients are currently performed as day cases. All patients are pre assessed prior to the procedure, during which time bloods are taken, information is given & questions answered so that the patient is prepared for what will happen on the day of the procedure. This has streamlined the service we deliver making things more organised on the day of the angiogram.
Staffing Roles?
We have a mainly traditional lab set up. The qualified nurses rotate between the lab, day case unit and pre assessment clinics & this works well by providing variety within the role. Extended role includes sheath removal. The radiographers are responsible for all the screening as well as ensuring the radiation protection regulations are adhered to, with regular monitoring of screening times & radiation doses. Techs are responsible for the ECG & haemodynamic monitoring & giving vital information to the consultant during the procedure that ensures patient safety.
••
Cross-Training?
One of the radiographers has trained in the scrub skills and assists with cases. We have no formal generic training programme but there is very much a “team ethos” in the department, where everyone works together in between cases, cleaning and preparing the lab for the next patient & this ensures an efficient throughput of patients. Everyone has an appreciation of each others roles and responsibilities within the team.
Surgical back-up
No, if needed we transfer our patients to Morriston Hospital, Swansea which is 30 minutes away by motorway.
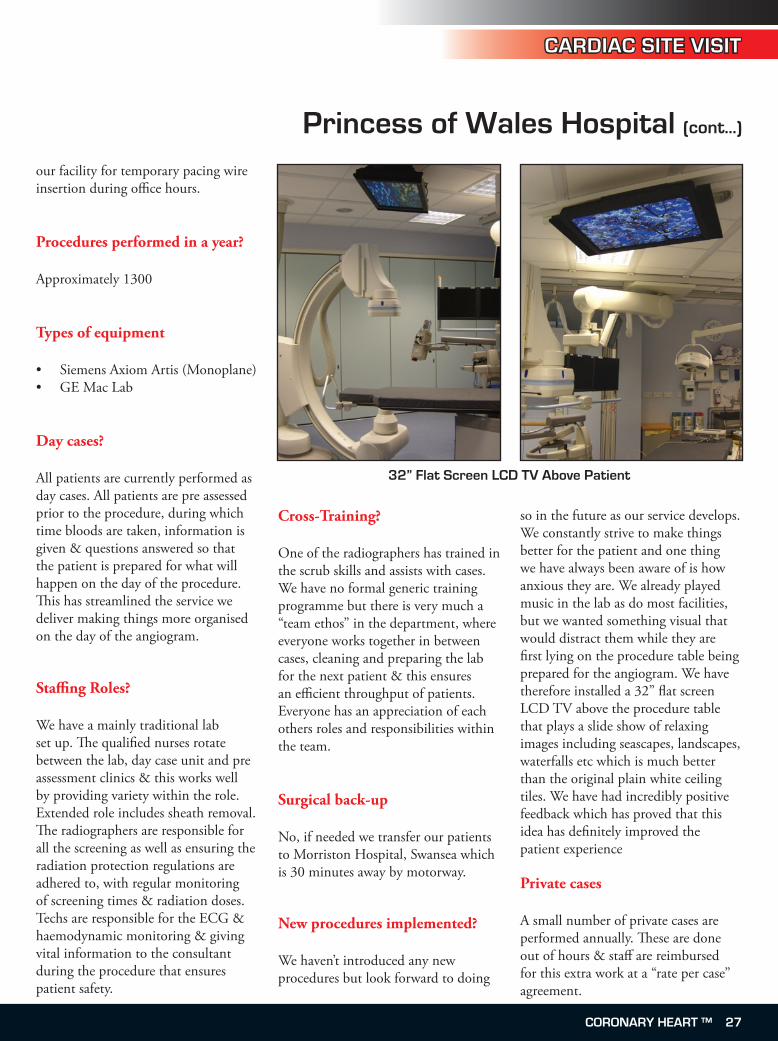
New procedures implemented?
We haven’t introduced any new procedures but look forward to doing
so in the future as our service develops. We constantly strive to make things better for the patient and one thing we have always been aware of is how anxious they are. We already played music in the lab as do most facilities, but we wanted something visual that would distract them while they are first lying on the procedure table being prepared for the angiogram. We have therefore installed a 32” flat screen LCD TV above the procedure table that plays a slide show of relaxing images including seascapes, landscapes, waterfalls etc which is much better than the original plain white ceiling tiles. We have had incredibly positive feedback which has proved that this idea has definitely improved the patient experience
Private cases
A small number of private cases are performed annually. These are done out of hours & staff are reimbursed for this extra work at a “rate per case” agreement.
32” Flat Screen LCD TV Above Patient
CORONARY HEART ™ 27
CARDIAC SITE VISIT
Princess of Wales Hospital (cont...)
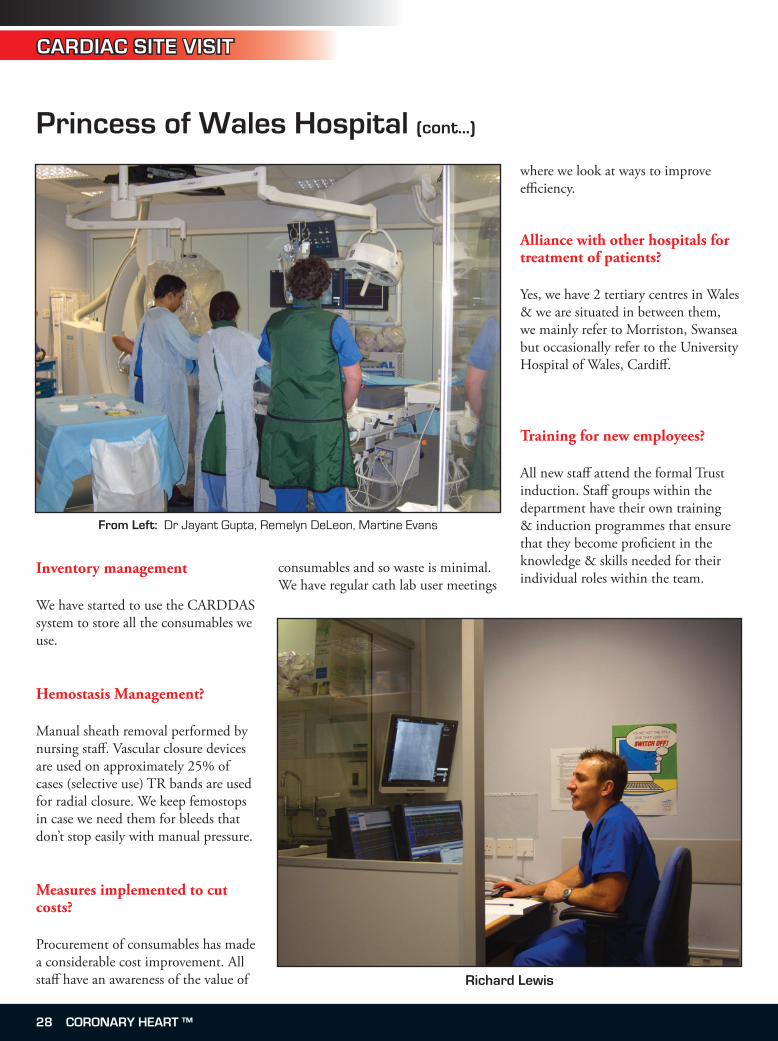
Inventory management
We have started to use the CARDDAS system to store all the consumables we use.
Hemostasis Management?
Manual sheath removal performed by nursing staff. Vascular closure devices are used on approximately 25% of cases (selective use) TR bands are used for radial closure. We keep femostops in case we need them for bleeds that don’t stop easily with manual pressure.
Measures implemented to cut costs?
Procurement of consumables has made a considerable cost improvement. All staff have an awareness of the value of
consumables and so waste is minimal. We have regular cath lab user meetings
where we look at ways to improve efficiency.
Alliance with other hospitals for treatment of patients?
Yes, we have 2 tertiary centres in Wales & we are situated in between them, we mainly refer to Morriston, Swansea but occasionally refer to the University Hospital of Wales, Cardiff.
Training for new employees?
All new staff attend the formal Trust induction. Staff groups within the department have their own training & induction programmes that ensure that they become proficient in the knowledge & skills needed for their individual roles within the team.
From Left: Dr Jayant Gupta, Remelyn DeLeon, Martine Evans
Richard Lewis
28 CORONARY HEART ™
CARDIAC SITE VISIT
Princess of Wales Hospital (cont...)
Continuing education programs for staff ?
All staff are encouraged and supported to attend relevant study days & national conferences. Th e Trust has a programme of mandatory training that all staff attend as well as regular update training in life support etc. We liaise with the tertiary centres and staff receive training in permanent pacing, PCI so that they can learn the skills they will need when these services are introduced into our department. Th ey have also had the opportunity to observe cardiac surgery.
Some of the challenges in the department?
Setting up a new service was quite challenging at the beginning, we were fortunate however not to have any major recruiting problems and the retention of staff has been excellent.
Training facility for cardiac registrars?
Yes
What is the best part of working at your facility?
We have small, motivated & friendly team, where everyone is known by their 1st name (even the consultants!!), and we have a good learning environment with an appreciation of everyone’s role within that team. Th e lab is a happy place with a real “family feel” Everyone has a positive attitude and a dedication to making things better for the patient. We are all looking forward to future developments within the department which will make things even better.
Located on the west coast of the United Kingdom, Wales has a population of approx. 3 million, and has its own National Assembly and language. Famous for its celtic history, stunning scenery, and medieval castles, Wales is a must visit for anybody to the UK.
Worried about the weather? Wales is actually one of the sunniest spots in the UK. So remember to bring your swimmers, hiking gear, and a good camera, because Wales has it all.
Th ings to see and do:
Snowdonia National Park: Th is mountainous region covers 2,142 km² and contains 60km of coastline. Climb or catch a train to the summit of Mt Snowden which is the highest British mountain south of the Scottish Highlands.
Brecon Beacons: Located in the south east, this national park contains old coalmining Valleys, deep caves, and waterfalls. You may even spot a Welsh mountain pony.
Porthcawl: Just south of Bridgend this town is a leading holiday resort. It’s recognised as one of the best surfi ng beaches in Wales, and there is a major golf course nearby.
•
•
•
WHY WALES?
Hiking in the Snowdonia National Park, Wales
Photo: Tim Larner
CORONARY HEART ™ 29
INTERVIEW
Patricia Pye
Patricia Pye is a great leader that is recognized nationally for establishing innovative programs: researched, designed, and created Congestive Heart Failure, Diabetes, Physician/Nurse Collaboration, Standards of Practice, and Critical Care Family Support Programs. Th e motivating force in her career has been the reward that comes from building individuals and teams that grow and succeed in driving positive and innovative changes that impact patient care.
Patricia please provide the readers with an overview of your areas of responsibility.
Th e Carolinas HealthCare System is the largest healthcare system in the Carolinas, and one of the largest
publicly owned systems in the nation. Carolinas HealthCare owns, leases, and manages hospitals, nursing homes, physician practices, home health agencies, radiation therapy hospitals, managed care companies and other healthcare related operations, comprising more than 4,410 licensed beds and approximately 25,300 employees.
Carolinas Medical Center (CMC) is the fl agship facility of Carolinas HealthCare System. As one of North Carolina’s largest hospitals, it serves as the regional referral center for western North Carolina. In addition, a signifi cant number of patients come from South Carolina and all over the Southeast. CMC opened in 1940 and has now expanded to include 861 beds. Th e hospital is one of only fi ve facilities in North Carolina designated as an Academic Medical Center Teaching Hospital and a Level I Trauma Center. It is primarily a tertiary, quaternary referral center.
As Director of Invasive and Non-invasive Cardiovascular Services my responsibilities include the Cath Lab, Cardiology (ECG, Holter, and Stress), the Heart Failure/Heart Transplant Program, and Enhanced External Counterpulsation. Th ere are approximately 100 FTEs covering the 4 departments. Regional outreach responsibilities include some staffi ng of several outlying facilities, training, and the assistance in the development of policy and practice guidelines. Recently I was the driving force behind the implementation of the C-PORT Trial at a remote hospital.
CMC has eight invasive Cath labs (1 peripheral, 1 peripheral/ same day
diagnostic, 3 interventional/diagnostic, 1 pediatric/adult and 2 EP labs). Two of the eight labs have bi-plane capabilities. Pre/Post procedure holding areas are divided into a 10-bed outpatient unit, a 14-bed inpatient/outpatient unit, a 5-bed unit for peripheral vascular, and 1 bed pediatric unit. CMC also has a remote diagnostic Cath lab, with a four bed holding area, in a satellite facility approximately 10 miles away. Approximately 35-50 procedures are completed daily and up to 6 are done each Saturday. A cardiologist is in house 24/7 and cases between the hours 1800-0730 are covered by the on call Cath Lab team.
Th e lab has approximately 70 FTE’s that consist of RCIS, RCP, RTR, RN, CVT, and offi ce support staff . Seniority runs from a few months to 25 years, the average length of service is approximately fi ve years. All CVTs are required to become registered within one year of employment
Th e Heart Failure Program consists of Nurse Practitioners, RNs, Pharmacists and Social Workers. Th ere are approximately 1500 patients currently enrolled in the program. Initiatives such as a Pulmonary Hypertension Clinic and PTT Clinic are underway. We have a Link program which provides very close telephonic follow-up on patients once they are discharged from the hospital. Th e program and its intense follow-up have signifi cantly decreased readmissions.
Th e Enhanced External Counterpulsation program was initiated in 2006. Th e Coordinator of the program is very aggressive in marketing the program. As a result
Patricia M. Pye, RN, MSDirector, Invasive and Non-invasive
Cardiovascular ServicesCarolinas Medical Center, Charlotte,
North Carolina
Interviewed by Ms Voncile Hilson-MorrowCEO Baltimore/Washington Division of Healthworks, Inc.Previous Director of Invasive Cardiology at Washington Heart at the Washington Hospital Center
30 CORONARY HEART ™
INTERVIEW
Patricia Pye (cont...)
we have been at near capacity since its inception.
The Cardiology Department has approximately 25 FTEs comprised of ECG Techs and RNs. The ECG Techs are responsible for all ECGs in the Hospital with the exception of the Emergency Department. The Supervisor of the Department is responsible for the MUSE ECG Management System. Currently all ECGs are read, edited and confirmed on-line with the exception of the Emergency Department which will be on-line by the end of the year. The RNs are responsible for managing both
in/out patient stress exams.
Discuss service excellence within your organization. List any customer service assessment tools used and pertinent results.
Caring, Commitment, Teamwork and Integrity have long been the core values of the System and as such the foundation for Service Excellence. Several years ago the System engaged the Studer Group to enrich an already strong emphasis on excellence. Communications, Safety and Service Recovery were added to the standards.
All the standards are an integral part of everyone’s evaluation. The organization has employed a national firm, PRC (Professional Research Consultants, Inc.), to monitor, report, and rate the organization as compared to other like facilities across the nation. The Invasive and Non-invasive Cardiovascular Service has placed significant emphasis on Service Excellence and as a result has been the winner of the PRC 5 Star Award for Service Excellence 3 years in a row.
Carolinas Medical Center, Charlotte, North Carolina
>>
CORONARY HEART ™ 31

INTERVIEW
Patricia Pye (cont...)
In your view, what are the issues that most affect Cardiovascular Service Lines and what trends will shape cardiovascular departments over the next five years?
The next five years are going to see major changes in the cardiovascular service line. The competition for cardiac and vascular services is on the rise. Services will be in more demand because of the aging population. In order to surpass the competition the hospital must be prepared to react quickly to industry changes. A forward thinking, fast acting strategic plan that includes adequate and functional space planning, enhanced information systems, and advanced technologies will be critical. Emphasis will be placed on growth in the Vascular, Peds, EP and Heart Failure/Heart Transplant arenas. Primary interventions, blending of surgical and percutaneous treatments, more non-invasive diagnostic techniques, shorter bed rest, shorter hospital stay and more evidence based protocols are some of the emerging practices of invasive cardiology. Changes in reimbursement – moving from a charge based to a cost based method will reduce revenues significantly. To be on the leading edge a major focus must be on process improvement, personnel, technology, and facility flexibility.
Are you a visionary? Please explain. I believe that I am a strong visionary in that I have been able to foresee and predict changes that are necessary to position the Departments and hospital for the future. Some of these changes have included: the development of hybrid labs, a regional Code STEMI
program, an enhanced Heart Failure/Heart Transplant program, and an annual Nurse/Specialist Conference (Expanding Horizons) in Hilton Head, South Carolina. Other programs include implementation of a significant cost saving equipment/supply vendor negotiation program, facilities planning, and a productivity incentive program, cross training and required RCIS certification.
Give at least one significant accomplishment that has been achieved at your direction. Please discuss any compelling examples demonstrating that your influence significantly improved patient outcomes.
The accomplishment that I am the most enthusiastic and proud of is the development of a strong team. Each individual has been mentored, coached and motivated to take on new challenges, enhance their education, collaborate, communicate and benchmark against the best practices. The results have been strong individual and team performance and noteworthy accomplishments. Abstracts have been accepted. Poster presentations have been presented at SCA&I and the ACC. Articles have been written and published. The Code STEMI program has resulted in data demonstrating a decrease in mortality to one half the national rate with NRMI validating a 14 minute door to reperfusion time best in the country. Staff has been invited to lecture at national conferences. A regional Heart Failure program has been initiated; and the vendor negotiation program has resulted in multimillion dollar savings for the hospital.
What drives your team? What do you do to initiate, stimulate and reward positive performance?
A Productivity Incentive Program was instituted in 2003 in order to improve the Cath Lab efficiency, productivity and patient, physician and staff satisfaction. It financially recognizes those employees that perform in an exemplary manner. It aligns staff performance with growth and service targets. It is available only if the department meets established productivity and quality goals and the individual meets certain performance standards. A minimum of 32 cases must be completed between 7:30am and 6:00pm five days a week. The over all quality of care must be at 90% or better as measured by PRC (Professional Research Consultants, Inc.). There must be less than a 5% /staff error rate in documentation. If the established criteria are met each staff member receives a case weighted monetary incentive. Results have been noteworthy. Approximately 90% of the cases are completed by 6:00pm. The overall quality of care has exceeded the 90% mark and the Lab has won the 5 Star award for the last 3 years in a row. Overtime has been decreased by 28% and the vacancy rate has decreased to less than 4%. Both physicians and staff have enthusiastically endorsed the program. It has clearly been a win/win solution.
Discuss your experience with Joint Commission Surveys and pertinent results.
The key to successful JCAHO surveys is to be in a natural state of readiness at all times. A last minute surge to
32 CORONARY HEART ™
INTERVIEW
Patricia Pye (cont...)
prepare for and obtain compliance is not only ineff ective but contrary to the spirit of providing safe and eff ective patient care and service excellence. Fundamental to a successful survey is staff knowledge of the standards and their rationale. We have established a monthly tracer program. Th is involves randomly selected staff members who audit each area to determine the level of compliance and bring to management the corrective action that are necessary. Our last JCAHO survey resulted in accolades from the surveyor.
Describe the level of involvement your physician leaders have in your program.
Th ere are regular and close interactions with the physician leaders of each of the programs. Th ese include the Directors of the Cath Lab, Electrophysiology, Pediatrics, Vascular, Research, Heart Failure/Heart Transplant Program, Cardiology, and the Chest Pain Center. Th ere is close teamwork and collaboration amongst the group in order to provide quality, cutting edge, and cost eff ective patient care. Th e physician leadership team is very active and supportive in the major operational issues and strategic planning for their specifi c areas. Open communications and respect for each others point of view have been the key to a win/win environment.
What is your definition of leadership?
Leadership is the ability to mentor, coach and direct people to the achievement of win/win solutions. It requires an individual to be visionary,
operationally astute, and situational. Key to being a successful leader is to be able to get along with and be respected by ones subordinates, peers and management. A leader must be a role model, ethical, fl exible, entrepreneurial, innovative, and able to drive change.
What are the “drivers’ in your career?
My greatest reward is experiencing the successes and achievements of many of those who have worked with me. My overarching goal has always been to make a positive and lasting diff erence.
Inside Humour
CORONARY HEART ™ 33

EP EDUCATION
Atrial Flutter
Atrial fl utter is characterised by rapid but regular atrial depolarisations with a
consistent ECG morphology. In the most common form the inferior leads on the ECG show a p wave with a gradual down-slope followed by a rapid upstroke. Th is is described as a “saw-tooth” appearance and is easily recognised (Fig 1).
Th ere are less common forms of fl utter where the p waves look diff erent (see “less common fl utters”). Th e atrial rate in fl utter is usually around 300 bpm. Clearly it would not be desirable for all these impulses to be conducted to the ventricles, so the AV node comes to the rescue by only conducting a proportion. If the node conducts every other impulse the resulting ventricular rate is 150 bpm. Th is is described as fl utter with 2:1 conduction. 3:1 conduction results in a ventricular rate of 100 bpm, 4:1 conduction in a rate of 75 bpm.
Because of this the heart rare trend in 24 hr tapes of patients with fl utter often show abrupt step-wise changes in rate rather than the gradual changes the sinus node produces. Patients are symptomatic when the rate steps up. Atrial fi brillation may sometimes mimic atrial fl utter but in AF the p wave morphology varies over time and gives rise to a disorganised ventricular rhythm. Occasionally fl utter is conducted in a 1:1 fashion resulting in a very rapid ventricular response which may cause syncope (Fig 2). Th is usually occurs where the atrial rate during fl utter is slightly slower than the typical 300 bpm. Th is slowing can be an undesirable eff ect of anti-arrhythmic medication.
Th ere is some confusion around the use of the terms atrial fl utter and atrial tachycardia. Flutter is a term based primarily on the ECG appearance. As atrial tachycardia describes a fast rhythm arising exclusively in the atria then atrial fl utter represents a subset of atrial tachycardias. However the term
atrial tachycardia is usually reserved for slower tachycardias. Atrial fl utter can be described in electrophysiological terms as a form of macro-reentrant atrial tachycardia.
Fig 1. 12 lead of typical flutter
Fig 2. Flutter with 1:1 conduction
By Mr Ian WrightSt. Mary’s Hospital, London, UK
34 CORONARY HEART ™
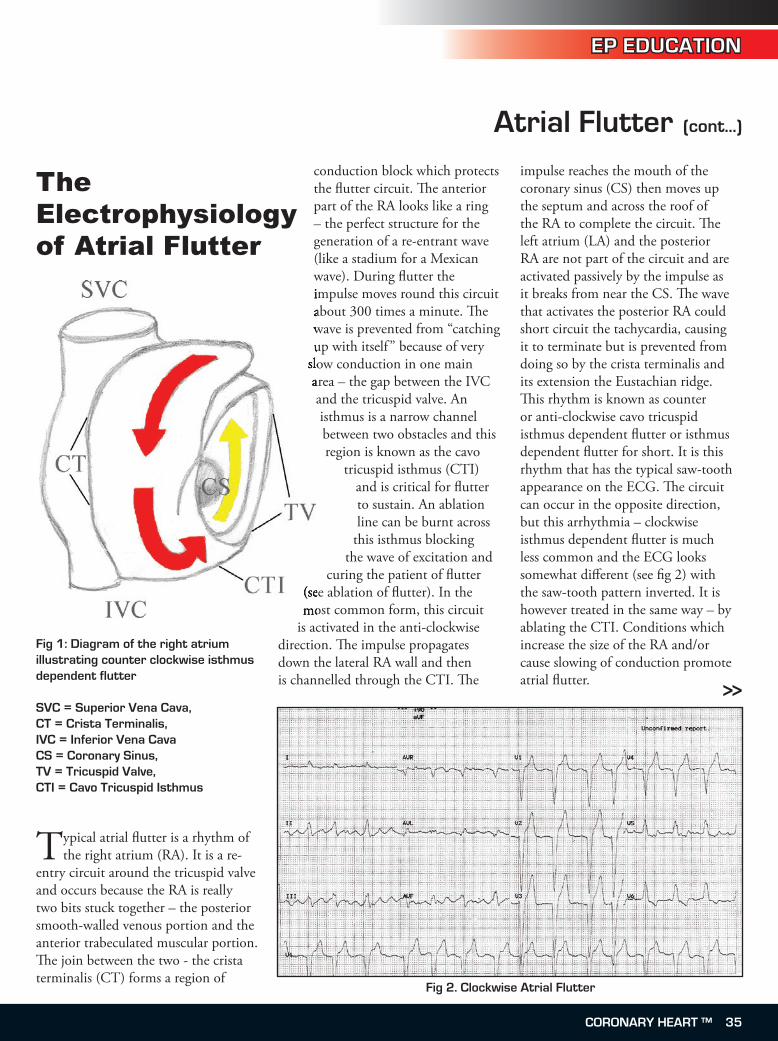
EP EDUCATION
Atrial Flutter (cont...)
Typical atrial fl utter is a rhythm of the right atrium (RA). It is a re-
entry circuit around the tricuspid valve and occurs because the RA is really two bits stuck together – the posterior smooth-walled venous portion and the anterior trabeculated muscular portion. Th e join between the two - the crista terminalis (CT) forms a region of
conduction block which protects the fl utter circuit. Th e anterior part of the RA looks like a ring – the perfect structure for the generation of a re-entrant wave (like a stadium for a Mexican wave). During fl utter the impulse moves round this circuit about 300 times a minute. Th e wave is prevented from “catching up with itself ” because of very
slow conduction in one main area – the gap between the IVC and the tricuspid valve. An isthmus is a narrow channel between two obstacles and this region is known as the cavo
tricuspid isthmus (CTI) and is critical for fl utter to sustain. An ablation line can be burnt across
this isthmus blocking the wave of excitation and
curing the patient of fl utter (see ablation of fl utter). In the most common form, this circuit
is activated in the anti-clockwise direction. Th e impulse propagates down the lateral RA wall and then is channelled through the CTI. Th e
impulse reaches the mouth of the coronary sinus (CS) then moves up the septum and across the roof of the RA to complete the circuit. Th e left atrium (LA) and the posterior RA are not part of the circuit and are activated passively by the impulse as it breaks from near the CS. Th e wave that activates the posterior RA could short circuit the tachycardia, causing it to terminate but is prevented from doing so by the crista terminalis and its extension the Eustachian ridge. Th is rhythm is known as counter or anti-clockwise cavo tricuspid isthmus dependent fl utter or isthmus dependent fl utter for short. It is this rhythm that has the typical saw-tooth appearance on the ECG. Th e circuit can occur in the opposite direction, but this arrhythmia – clockwise isthmus dependent fl utter is much less common and the ECG looks somewhat diff erent (see fi g 2) with the saw-tooth pattern inverted. It is however treated in the same way – by ablating the CTI. Conditions which increase the size of the RA and/or cause slowing of conduction promote atrial fl utter.
Fig 1: Diagram of the right atrium illustrating counter clockwise isthmus dependent flutter
SVC = Superior Vena Cava,CT = Crista Terminalis,IVC = Inferior Vena CavaCS = Coronary Sinus, TV = Tricuspid Valve, CTI = Cavo Tricuspid Isthmus
wave). During fl utter the impulse moves round this circuit about 300 times a minute. Th e wave is prevented from “catching up with itself ” because of very
slow conduction in one main area – the gap between the IVC
(see ablation of fl utter). In the most common form, this circuit
The Electrophysiology of Atrial Flutter
Fig 2. Clockwise Atrial Flutter
>>
CORONARY HEART ™ 3�
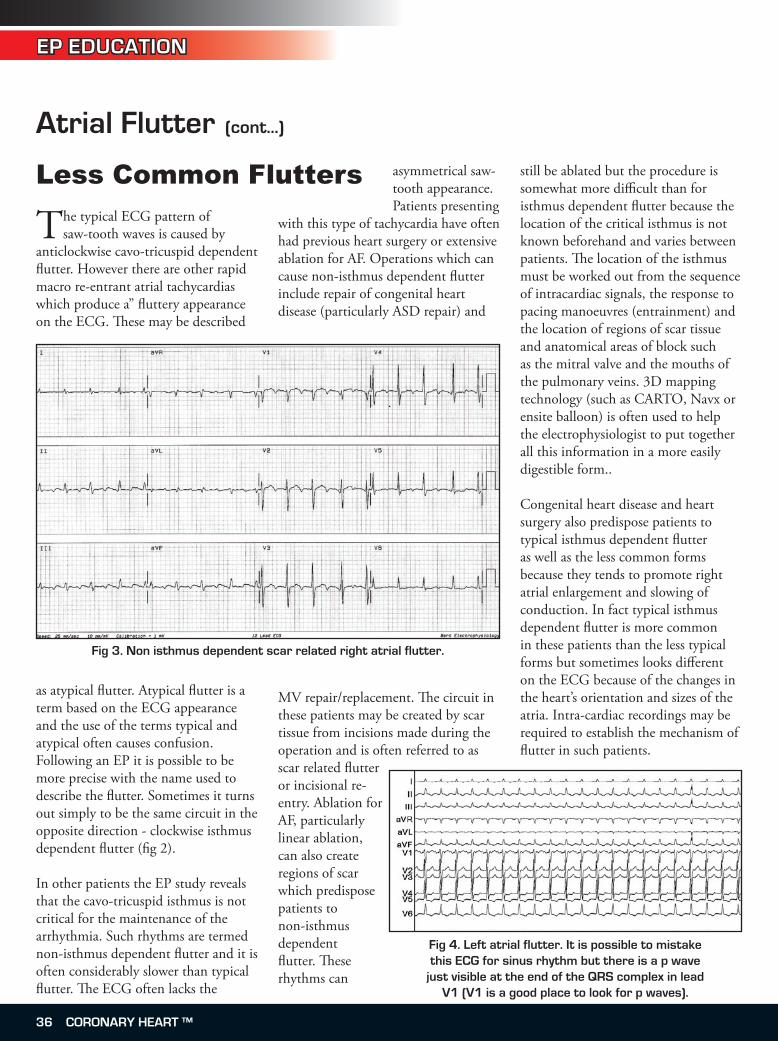
Atrial Flutter (cont...)
EP EDUCATION
The typical ECG pattern of saw-tooth waves is caused by
anticlockwise cavo-tricuspid dependent flutter. However there are other rapid macro re-entrant atrial tachycardias which produce a” fluttery appearance on the ECG. These may be described
as atypical flutter. Atypical flutter is a term based on the ECG appearance and the use of the terms typical and atypical often causes confusion. Following an EP it is possible to be more precise with the name used to describe the flutter. Sometimes it turns out simply to be the same circuit in the opposite direction - clockwise isthmus dependent flutter (fig 2).
In other patients the EP study reveals that the cavo-tricuspid isthmus is not critical for the maintenance of the arrhythmia. Such rhythms are termed non-isthmus dependent flutter and it is often considerably slower than typical flutter. The ECG often lacks the
asymmetrical saw-tooth appearance. Patients presenting
with this type of tachycardia have often had previous heart surgery or extensive ablation for AF. Operations which can cause non-isthmus dependent flutter include repair of congenital heart disease (particularly ASD repair) and
MV repair/replacement. The circuit in these patients may be created by scar tissue from incisions made during the operation and is often referred to as scar related flutter or incisional re-entry. Ablation for AF, particularly linear ablation, can also create regions of scar which predispose patients to non-isthmus dependent flutter. These rhythms can
still be ablated but the procedure is somewhat more difficult than for isthmus dependent flutter because the location of the critical isthmus is not known beforehand and varies between patients. The location of the isthmus must be worked out from the sequence of intracardiac signals, the response to pacing manoeuvres (entrainment) and the location of regions of scar tissue and anatomical areas of block such as the mitral valve and the mouths of the pulmonary veins. 3D mapping technology (such as CARTO, Navx or ensite balloon) is often used to help the electrophysiologist to put together all this information in a more easily digestible form..
Congenital heart disease and heart surgery also predispose patients to typical isthmus dependent flutter as well as the less common forms because they tends to promote right atrial enlargement and slowing of conduction. In fact typical isthmus dependent flutter is more common in these patients than the less typical forms but sometimes looks different on the ECG because of the changes in the heart’s orientation and sizes of the atria. Intra-cardiac recordings may be required to establish the mechanism of flutter in such patients.
Less Common Flutters
Fig 3. Non isthmus dependent scar related right atrial flutter.
Fig 4. Left atrial flutter. It is possible to mistake this ECG for sinus rhythm but there is a p wave
just visible at the end of the QRS complex in lead V1 (V1 is a good place to look for p waves).
3� CORONARY HEART ™
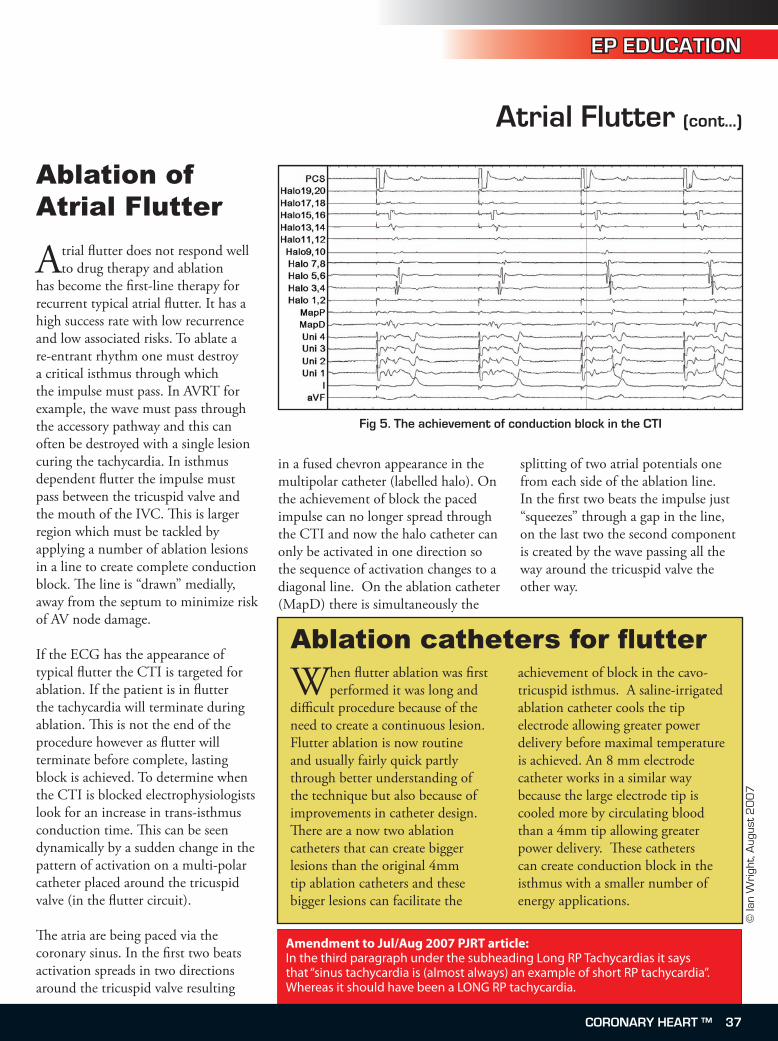
EP EDUCATION
Atrial Flutter (cont...)
Atrial flutter does not respond well to drug therapy and ablation
has become the first-line therapy for recurrent typical atrial flutter. It has a high success rate with low recurrence and low associated risks. To ablate a re-entrant rhythm one must destroy a critical isthmus through which the impulse must pass. In AVRT for example, the wave must pass through the accessory pathway and this can often be destroyed with a single lesion curing the tachycardia. In isthmus dependent flutter the impulse must pass between the tricuspid valve and the mouth of the IVC. This is larger region which must be tackled by applying a number of ablation lesions in a line to create complete conduction block. The line is “drawn” medially, away from the septum to minimize risk of AV node damage. If the ECG has the appearance of typical flutter the CTI is targeted for ablation. If the patient is in flutter the tachycardia will terminate during ablation. This is not the end of the procedure however as flutter will terminate before complete, lasting block is achieved. To determine when the CTI is blocked electrophysiologists look for an increase in trans-isthmus conduction time. This can be seen dynamically by a sudden change in the pattern of activation on a multi-polar catheter placed around the tricuspid valve (in the flutter circuit).
The atria are being paced via the coronary sinus. In the first two beats activation spreads in two directions around the tricuspid valve resulting
in a fused chevron appearance in the multipolar catheter (labelled halo). On the achievement of block the paced impulse can no longer spread through the CTI and now the halo catheter can only be activated in one direction so the sequence of activation changes to a diagonal line. On the ablation catheter (MapD) there is simultaneously the
splitting of two atrial potentials one from each side of the ablation line. In the first two beats the impulse just “squeezes” through a gap in the line, on the last two the second component is created by the wave passing all the way around the tricuspid valve the other way.
Ablation of Atrial Flutter
Fig �. The achievement of conduction block in the CTI
When flutter ablation was first performed it was long and
difficult procedure because of the need to create a continuous lesion. Flutter ablation is now routine and usually fairly quick partly through better understanding of the technique but also because of improvements in catheter design. There are a now two ablation catheters that can create bigger lesions than the original 4mm tip ablation catheters and these bigger lesions can facilitate the
achievement of block in the cavo-tricuspid isthmus. A saline-irrigated ablation catheter cools the tip electrode allowing greater power delivery before maximal temperature is achieved. An 8 mm electrode catheter works in a similar way because the large electrode tip is cooled more by circulating blood than a 4mm tip allowing greater power delivery. These catheters can create conduction block in the isthmus with a smaller number of energy applications.
© Ia
n W
righ
t, A
ugus
t 2
00
7
Amendment to Jul/Aug 2007 PJRT article: In the third paragraph under the subheading Long RP Tachycardias it says that “sinus tachycardia is (almost always) an example of short RP tachycardia”. Whereas it should have been a LONG RP tachycardia.
Ablation catheters for flutter
CORONARY HEART ™ 37
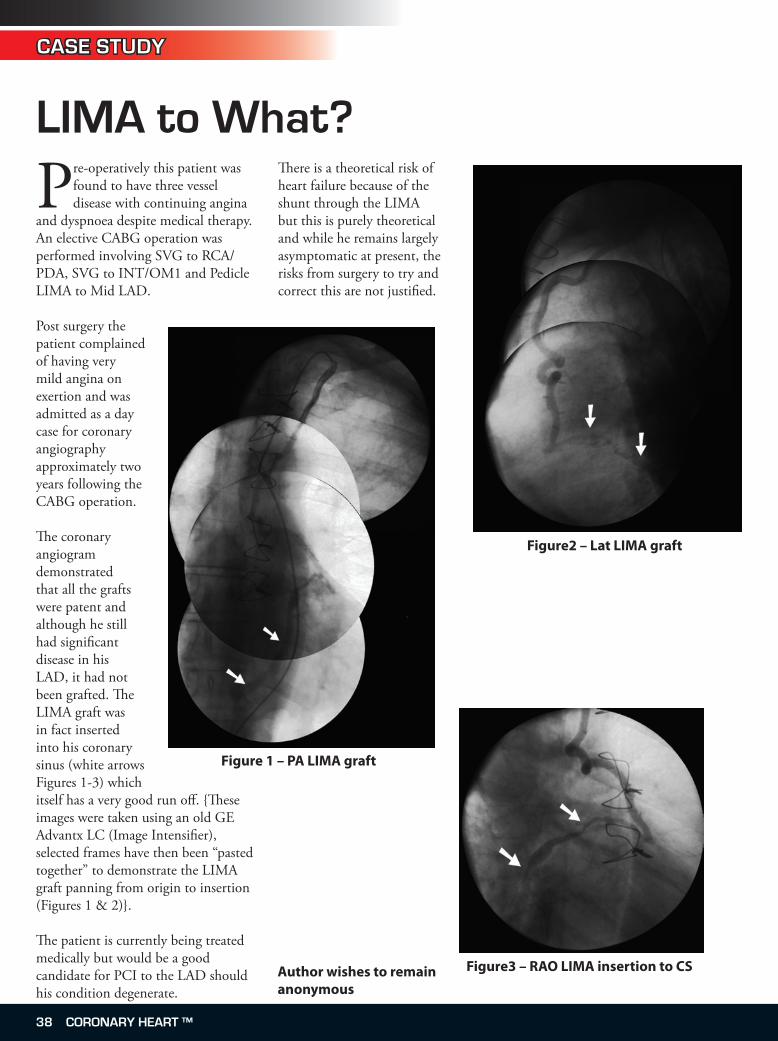
LIMA to What?
Author wishes to remain anonymous
Pre-operatively this patient was found to have three vessel disease with continuing angina
and dyspnoea despite medical therapy. An elective CABG operation was performed involving SVG to RCA/PDA, SVG to INT/OM1 and Pedicle LIMA to Mid LAD.
Post surgery the patient complained of having very mild angina on exertion and was admitted as a day case for coronary angiography approximately two years following the CABG operation.
The coronary angiogram demonstrated that all the grafts were patent and although he still had significant disease in his LAD, it had not been grafted. The LIMA graft was in fact inserted into his coronary sinus (white arrows Figures 1-3) which itself has a very good run off. {These images were taken using an old GE Advantx LC (Image Intensifier), selected frames have then been “pasted together” to demonstrate the LIMA graft panning from origin to insertion (Figures 1 & 2)}.
The patient is currently being treated medically but would be a good candidate for PCI to the LAD should his condition degenerate.
There is a theoretical risk of heart failure because of the shunt through the LIMA but this is purely theoretical and while he remains largely asymptomatic at present, the risks from surgery to try and correct this are not justified.
Figure 1 – PA LIMA graft
Figure2 – Lat LIMA graft
Figure3 – RAO LIMA insertion to CS
CASE STUDY
38 CORONARY HEART ™

RADIATION EDUCATION
Radiation safety is a primary focus in the diagnostic and invasive cardiovascular workplace. As
healthcare providers working with radiation on a daily basis, it is important to examine some of the measures taken to ensure our protection from these harmful waves.
Radiation is considered energy traveling through space. One example of this phenomenon is sunshine which we are exposed to everyday. Sunshine is a form of radiation consisting of many different waves ranging from long wave (infrared) to short wave (ultraviolet). However, most people are aware that too much sunshine can result in adverse effects such as skin cancer. As a result, we control the amount of exposure. Sunscreen, sunglasses, and hats are some of the ways we protect ourselves. The same phenomenon holds true in the workplace. Radiation varies
and limiting ones exposure is of utmost importance.
Radiation sources are normally considered to be natural occurring or man-made in nature. Approximately 82% of radiation exposure occurs as a result of natural occurring radiation. Some examples of naturally occurring radiation are: radon which accounts for about 55%, rocks, and soil. The other 18% are man made. Man made radiation is primarily from industry and healthcare with x-rays being the biggest contributor.
X-rays were discovered by German professor Wilhelm Conrad Roentgen in 1895. These rays were called x-radiation to reflect their unknown origin. This discovery was quickly followed by Henri Becquerel and his discovery of natural radioactivity. During the time of Becquerel’s discovery, Polish scientist Marie Curie became interested in his work and went on to study the Uranium ore. With the help of her husband Pierre, her investigation led to the discovery of Polonium and Radium. By the early 1900s, the study of radiation became a popular topic of interest.
It was noted that while radiation appeared useful, improper handling posed threats to humans. One example surfaced in the death of Thomas Edison’s assistant who died from a radiation- induced tumor. During WWI, the paint used on aircrafts to make them more visible at night, contained radioactive materials. The
women who designed glow-in-the-dark watch handles and faces also improperly handled radioactive materials. By using their mouths to shape the tips of their paint brushes, they unknowingly swallowed small amounts of the radioactive substance. Over a 2-year period, some of these women died. This prompted an investigation which concluded they had all died from radiation or radioactive exposure.
The result of this investigation was the birth of radiation protection. By 1915, the British imposed strict regulations to protect people from over exposure to radiation. These regulations quickly became widespread. In 1928, The Advisory Committee on X-Ray and Radium protection was established. This group served to represent all of the national radiologic groups in the United States. The Advisory Committee on X-ray and Radium subsequently evolved into The Natural Council on Radiation Protection and Measurements (NCRP) in 1929. This group served as educators for individuals who would be exposed to radiation. Their mission was to provide information and offer recommendations on radiation safety. One of their major recommendations was the specification of the maximum amount of radiation allowed. In the workplaces where exposure is eminent, emphasizing the phrase “As Low as Reasonably Achievable” (ALARA) should be paramount. This means keeping the dose as low as possible but still achieving good diagnostic images.
Radiation has two major divisions: Ionizing Radiation and Non-ionizing Radiation.
The following article was made possible in part by an unrestricted educational grant from Bracco Diagnostics Inc. For more information, please visit them at www.bracco.com
- By Dawn Provost-Larmond, AS, BS, M. Ed, RCISHealthworks, Inc.
Radiation Safety in the Workplace
>>
CORONARY HEART ™ 39
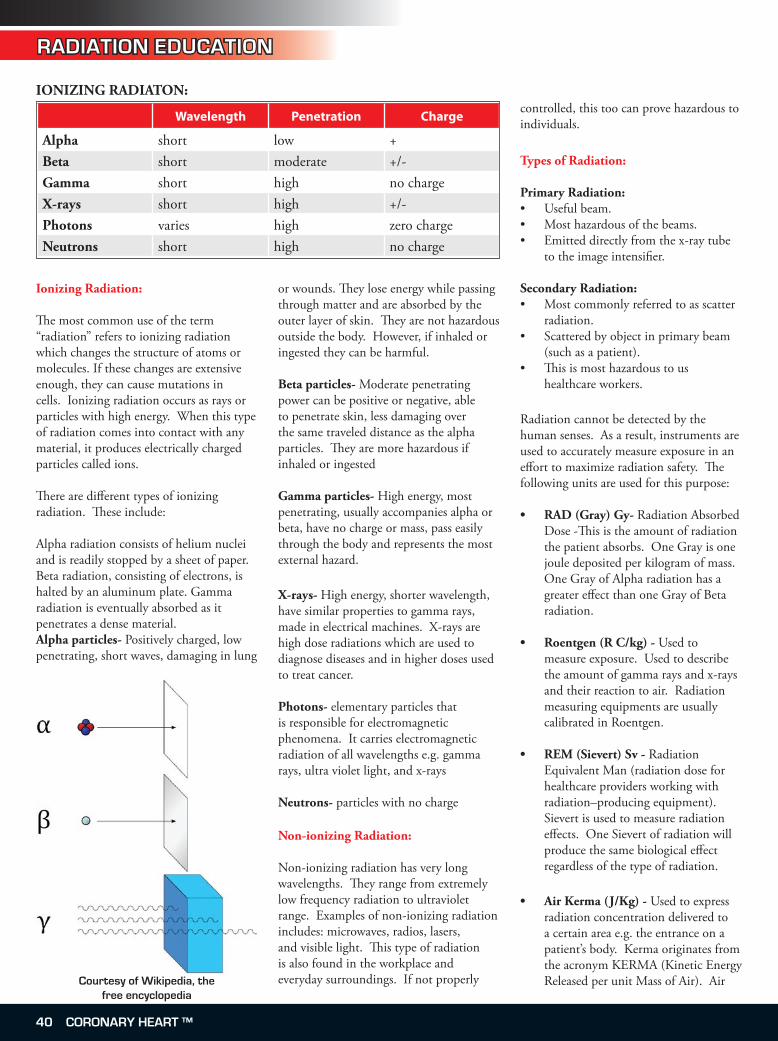
RADIATION EDUCATION
Ionizing Radiation:
The most common use of the term “radiation” refers to ionizing radiation which changes the structure of atoms or molecules. If these changes are extensive enough, they can cause mutations in cells. Ionizing radiation occurs as rays or particles with high energy. When this type of radiation comes into contact with any material, it produces electrically charged particles called ions.
There are different types of ionizing radiation. These include:
Alpha radiation consists of helium nuclei and is readily stopped by a sheet of paper. Beta radiation, consisting of electrons, is halted by an aluminum plate. Gamma radiation is eventually absorbed as it penetrates a dense material.Alpha particles- Positively charged, low penetrating, short waves, damaging in lung
or wounds. They lose energy while passing through matter and are absorbed by the outer layer of skin. They are not hazardous outside the body. However, if inhaled or ingested they can be harmful.
Beta particles- Moderate penetrating power can be positive or negative, able to penetrate skin, less damaging over the same traveled distance as the alpha particles. They are more hazardous if inhaled or ingested
Gamma particles- High energy, most penetrating, usually accompanies alpha or beta, have no charge or mass, pass easily through the body and represents the most external hazard.
X-rays- High energy, shorter wavelength, have similar properties to gamma rays, made in electrical machines. X-rays are high dose radiations which are used to diagnose diseases and in higher doses used to treat cancer.
Photons- elementary particles that is responsible for electromagnetic phenomena. It carries electromagnetic radiation of all wavelengths e.g. gamma rays, ultra violet light, and x-rays
Neutrons- particles with no charge
Non-ionizing Radiation:
Non-ionizing radiation has very long wavelengths. They range from extremely low frequency radiation to ultraviolet range. Examples of non-ionizing radiation includes: microwaves, radios, lasers, and visible light. This type of radiation is also found in the workplace and everyday surroundings. If not properly
controlled, this too can prove hazardous to individuals.
Types of Radiation:
Primary Radiation: Useful beam. Most hazardous of the beams. Emitted directly from the x-ray tube to the image intensifier.
Secondary Radiation: Most commonly referred to as scatter radiation. Scattered by object in primary beam (such as a patient). This is most hazardous to us healthcare workers.
Radiation cannot be detected by the human senses. As a result, instruments are used to accurately measure exposure in an effort to maximize radiation safety. The following units are used for this purpose:
RAD (Gray) Gy- Radiation Absorbed Dose -This is the amount of radiation the patient absorbs. One Gray is one joule deposited per kilogram of mass. One Gray of Alpha radiation has a greater effect than one Gray of Beta radiation.
Roentgen (R C/kg) - Used to measure exposure. Used to describe the amount of gamma rays and x-rays and their reaction to air. Radiation measuring equipments are usually calibrated in Roentgen.
REM (Sievert) Sv - Radiation Equivalent Man (radiation dose for healthcare providers working with radiation–producing equipment). Sievert is used to measure radiation effects. One Sievert of radiation will produce the same biological effect regardless of the type of radiation.
Air Kerma (J/Kg) - Used to express radiation concentration delivered to a certain area e.g. the entrance on a patient’s body. Kerma originates from the acronym KERMA (Kinetic Energy Released per unit Mass of Air). Air
•••
•
•
•
•
•
•
•
Wavelength Penetration Charge
Alpha short low +Beta short moderate +/-Gamma short high no chargeX-rays short high +/-Photons varies high zero chargeNeutrons short high no charge
IONIZING RADIATON:
Courtesy of Wikipedia, the free encyclopedia
40 CORONARY HEART ™
RADIATION EDUCATION
Kerma is another way of saying the absorbed dose in air. It is measured in J/Kg which is equivalent to the radiation unit the Gray (used when measuring the Radiation Absorbed Dose). Air Kerma is beginning to replace the way the absorbed dose was measured. Air Kerma is expressed in SI (International system of Units) units which makes calculations easier.
With technological advancements in radiation, other quantities and units have been introduced. Most of the units discussed previously are considered very useful but limited in that they do not give the total radiation delivered or absorbed by the body. Some of the other units currently being used are:
Surface Integral Exposure (SIE) - Product of the exposure value and the size of the exposed area. R-cm². The SIE gives total radiation to the entire bodyDose Area Product (DAP)- similar to SIE except in the units used (Gy-cm²)CTDI (Computed tomography dose Index)- Used in CT and relies on scatter radiation for calculationMammography Mean Glandular dose- Used in MammographyIntegral Dose-Radiation quantity that is the same as the total energy absorbed by the body. The unit for integral dose is Joules or gram-radCTDLP- Product of CTDI and the area of the body scanned. Measured in rad-cm or Gy-cm
The majority of quantities used in radiation are physical quantities that can be measured. However, one of the primary reasons for monitoring radiation exposure is to correlate its effect on our bodies and tissues. As a result one quantity known as Effective Dose is considered very useful in assessing relative risk to patients and healthcare workers. Effective Dose is more specific as it takes into account specific organs and the areas of the body that are being exposed to radiation. In an effort to make this easier, organs and different body areas have assigned weighing factors to aide in the calculations. The weighting factor for the entire body is 1.
•
•
•
•
•
•
Staff and physicians wear monitoring devices to track the amount of cumulative radiation exposure. This amount is measured in millirem (mrem). Healthcare providers who work in radiation areas are allowed 5 REM/year (5000mrem). The average American receives 360mrem/year from natural background exposure.
Some of the monitoring devices used by healthcare workers are:
Film badges- These are the oldest personal dosimeters. These devices are used to measure whole body radiation exposure. They are made up of three parts: a plastic film holder, radiographic film packet, and assorted metal filters. Film badges are sensitive to doses between 0.1 mSv (10mrem) and 5,000mSv (500 rem). These
•
badges are usually shipped once a month to be read and analyzed.
Optically Stimulated Luminescent Dosimeter- OSL combines the features of the film badges and the thermoluminescent dosimeters. These devices give an accurate reading for exposure as low as 1mrem. Because of its high sensitivity it is recommended for use in tracking exposure of any individual who may be pregnant.
Pocket dosimeters- Most sensitive of all dosimeters. Pocket dosimeters are sensitive to exposures ranging from 0 to 200mR (milliroentgens). One advantage of the pocket dosimeter is the fact that it provides immediate radiation readings. Some disadvan-tages of the pocket dosimeter are: they are expensive, they do not provide any permanent legal records and record-ings can be skewed if the device is dropped.
Rings- TLD ring badges are worn on the hands during the procedure to measure radiation exposure to the extremities.
These devices should be analyzed on a monthly basis to confirm that exposure is less than the maximum allowed dose.There are doses of exposure which are considered permissible without any proven ‘adverse effects’.
•
•
•
Tissue Weighting Factor
Gonads 0.25Breast 0.15Red Bone Marrow 0.12Lung 0.12Thyroid 0.03Bone Surface 0.03Remainder 0.3
(For the remaining organs a value of
0.06 is used for each of the five organs
receiving the highest dose.)
TOTAL 1.0
Maximum Permissible DosagesWhole Body 5 Rem per yearSkin 15 Rem per yearHands 75 Rem per yearForearms 30 Rem per yearOther Organs 15 Rem per yearPregnant Women 0.5 Rem during
gestation period for fetus
Students 0.1 Rem per year
Courtesy of Landauer
>>
Courtesy of Landauer
CORONARY HEART ™ 41
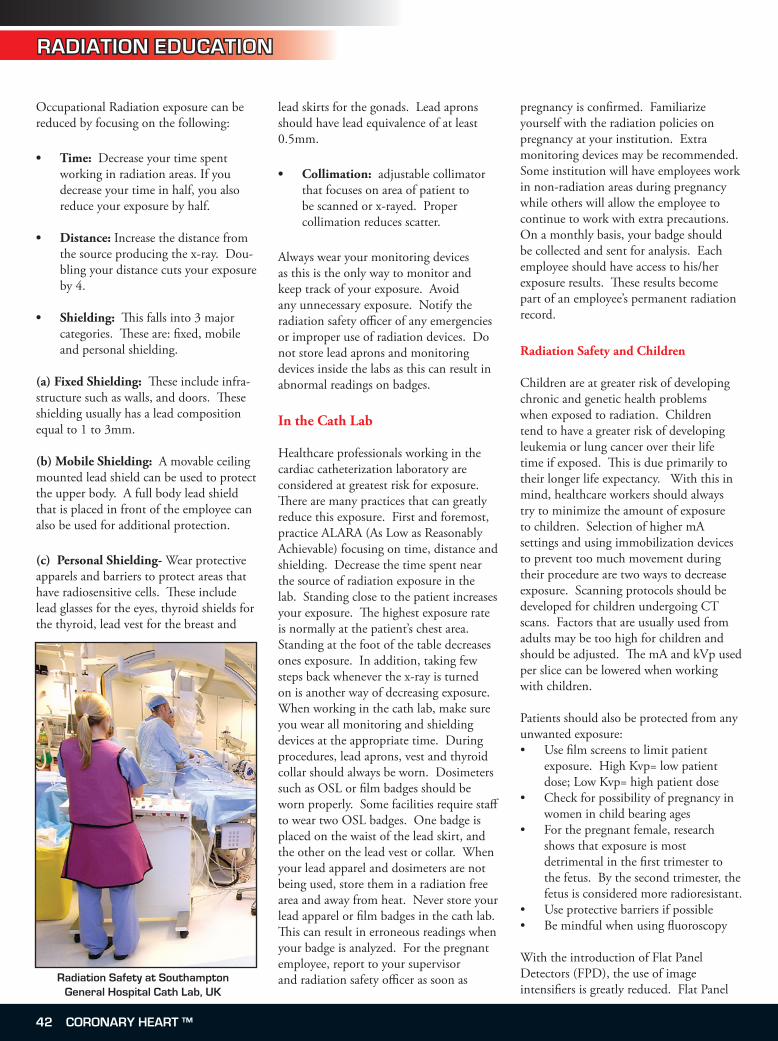
RADIATION EDUCATION
Occupational Radiation exposure can be reduced by focusing on the following:
Time: Decrease your time spent working in radiation areas. If you decrease your time in half, you also reduce your exposure by half.
Distance: Increase the distance from the source producing the x-ray. Dou-bling your distance cuts your exposure by 4.
Shielding: This falls into 3 major categories. These are: fixed, mobile and personal shielding.
(a) Fixed Shielding: These include infra-structure such as walls, and doors. These shielding usually has a lead composition equal to 1 to 3mm.
(b) Mobile Shielding: A movable ceiling mounted lead shield can be used to protect the upper body. A full body lead shield that is placed in front of the employee can also be used for additional protection.
(c) Personal Shielding- Wear protective apparels and barriers to protect areas that have radiosensitive cells. These include lead glasses for the eyes, thyroid shields for the thyroid, lead vest for the breast and
•
•
•
lead skirts for the gonads. Lead aprons should have lead equivalence of at least 0.5mm.
Collimation: adjustable collimator that focuses on area of patient to be scanned or x-rayed. Proper collimation reduces scatter.
Always wear your monitoring devices as this is the only way to monitor and keep track of your exposure. Avoid any unnecessary exposure. Notify the radiation safety officer of any emergencies or improper use of radiation devices. Do not store lead aprons and monitoring devices inside the labs as this can result in abnormal readings on badges.
In the Cath Lab
Healthcare professionals working in the cardiac catheterization laboratory are considered at greatest risk for exposure. There are many practices that can greatly reduce this exposure. First and foremost, practice ALARA (As Low as Reasonably Achievable) focusing on time, distance and shielding. Decrease the time spent near the source of radiation exposure in the lab. Standing close to the patient increases your exposure. The highest exposure rate is normally at the patient’s chest area. Standing at the foot of the table decreases ones exposure. In addition, taking few steps back whenever the x-ray is turned on is another way of decreasing exposure. When working in the cath lab, make sure you wear all monitoring and shielding devices at the appropriate time. During procedures, lead aprons, vest and thyroid collar should always be worn. Dosimeters such as OSL or film badges should be worn properly. Some facilities require staff to wear two OSL badges. One badge is placed on the waist of the lead skirt, and the other on the lead vest or collar. When your lead apparel and dosimeters are not being used, store them in a radiation free area and away from heat. Never store your lead apparel or film badges in the cath lab. This can result in erroneous readings when your badge is analyzed. For the pregnant employee, report to your supervisor and radiation safety officer as soon as
•
pregnancy is confirmed. Familiarize yourself with the radiation policies on pregnancy at your institution. Extra monitoring devices may be recommended. Some institution will have employees work in non-radiation areas during pregnancy while others will allow the employee to continue to work with extra precautions. On a monthly basis, your badge should be collected and sent for analysis. Each employee should have access to his/her exposure results. These results become part of an employee’s permanent radiation record. Radiation Safety and Children
Children are at greater risk of developing chronic and genetic health problems when exposed to radiation. Children tend to have a greater risk of developing leukemia or lung cancer over their life time if exposed. This is due primarily to their longer life expectancy. With this in mind, healthcare workers should always try to minimize the amount of exposure to children. Selection of higher mA settings and using immobilization devices to prevent too much movement during their procedure are two ways to decrease exposure. Scanning protocols should be developed for children undergoing CT scans. Factors that are usually used from adults may be too high for children and should be adjusted. The mA and kVp used per slice can be lowered when working with children.
Patients should also be protected from any unwanted exposure:
Use film screens to limit patient exposure. High Kvp= low patient dose; Low Kvp= high patient doseCheck for possibility of pregnancy in women in child bearing agesFor the pregnant female, research shows that exposure is most detrimental in the first trimester to the fetus. By the second trimester, the fetus is considered more radioresistant.Use protective barriers if possibleBe mindful when using fluoroscopy
With the introduction of Flat Panel Detectors (FPD), the use of image intensifiers is greatly reduced. Flat Panel
•
•
•
••
Radiation Safety at Southampton General Hospital Cath Lab, UK
42 CORONARY HEART ™
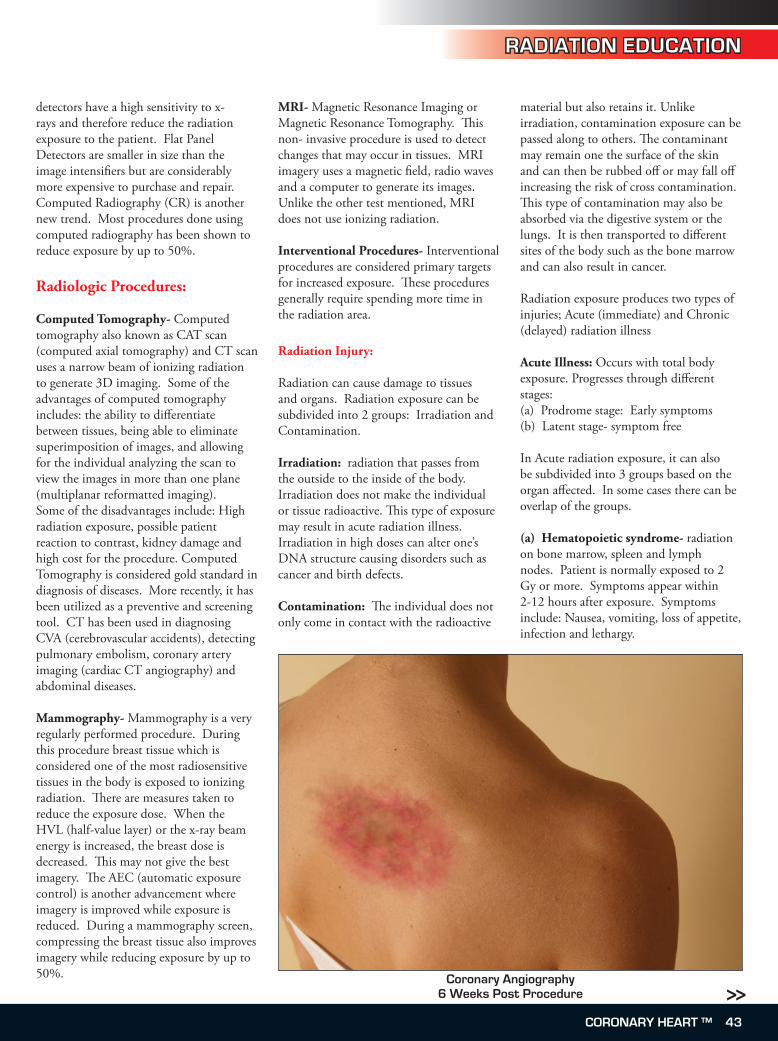
RADIATION EDUCATION
detectors have a high sensitivity to x-rays and therefore reduce the radiation exposure to the patient. Flat Panel Detectors are smaller in size than the image intensifiers but are considerably more expensive to purchase and repair. Computed Radiography (CR) is another new trend. Most procedures done using computed radiography has been shown to reduce exposure by up to 50%.
Radiologic Procedures:
Computed Tomography- Computed tomography also known as CAT scan (computed axial tomography) and CT scan uses a narrow beam of ionizing radiation to generate 3D imaging. Some of the advantages of computed tomography includes: the ability to differentiate between tissues, being able to eliminate superimposition of images, and allowing for the individual analyzing the scan to view the images in more than one plane (multiplanar reformatted imaging). Some of the disadvantages include: High radiation exposure, possible patient reaction to contrast, kidney damage and high cost for the procedure. Computed Tomography is considered gold standard in diagnosis of diseases. More recently, it has been utilized as a preventive and screening tool. CT has been used in diagnosing CVA (cerebrovascular accidents), detecting pulmonary embolism, coronary artery imaging (cardiac CT angiography) and abdominal diseases.
Mammography- Mammography is a very regularly performed procedure. During this procedure breast tissue which is considered one of the most radiosensitive tissues in the body is exposed to ionizing radiation. There are measures taken to reduce the exposure dose. When the HVL (half-value layer) or the x-ray beam energy is increased, the breast dose is decreased. This may not give the best imagery. The AEC (automatic exposure control) is another advancement where imagery is improved while exposure is reduced. During a mammography screen, compressing the breast tissue also improves imagery while reducing exposure by up to 50%.
MRI- Magnetic Resonance Imaging or Magnetic Resonance Tomography. This non- invasive procedure is used to detect changes that may occur in tissues. MRI imagery uses a magnetic field, radio waves and a computer to generate its images. Unlike the other test mentioned, MRI does not use ionizing radiation.
Interventional Procedures- Interventional procedures are considered primary targets for increased exposure. These procedures generally require spending more time in the radiation area. Radiation Injury:
Radiation can cause damage to tissues and organs. Radiation exposure can be subdivided into 2 groups: Irradiation and Contamination.
Irradiation: radiation that passes from the outside to the inside of the body. Irradiation does not make the individual or tissue radioactive. This type of exposure may result in acute radiation illness. Irradiation in high doses can alter one’s DNA structure causing disorders such as cancer and birth defects.
Contamination: The individual does not only come in contact with the radioactive
material but also retains it. Unlike irradiation, contamination exposure can be passed along to others. The contaminant may remain one the surface of the skin and can then be rubbed off or may fall off increasing the risk of cross contamination. This type of contamination may also be absorbed via the digestive system or the lungs. It is then transported to different sites of the body such as the bone marrow and can also result in cancer. Radiation exposure produces two types of injuries; Acute (immediate) and Chronic (delayed) radiation illness
Acute Illness: Occurs with total body exposure. Progresses through different stages:(a) Prodrome stage: Early symptoms(b) Latent stage- symptom free
In Acute radiation exposure, it can also be subdivided into 3 groups based on the organ affected. In some cases there can be overlap of the groups.
(a) Hematopoietic syndrome- radiation on bone marrow, spleen and lymph nodes. Patient is normally exposed to 2 Gy or more. Symptoms appear within 2-12 hours after exposure. Symptoms include: Nausea, vomiting, loss of appetite, infection and lethargy.
>>Coronary Angiography
� Weeks Post Procedure
CORONARY HEART ™ 43

RADIATION EDUCATION
(b) Gastrointestinal syndrome- radiation on the cells that line the digestive tract. Symptoms manifest in 2- 12 hours after exposure to 4Gy. Patient becomes fatigued, loss of appetite, nausea and vomiting, dehydration and infections.
(c) Cerebrovascular Syndrome- Exposure is greater than 20-30 Gy. This syndrome is usually fatal. In minutes, the patient experiences decrease in blood pressure, confusion, vomiting, diarrhea, shock, seizures, coma and death.
Diagnosis:
IrradiationPatients are diagnosed with radiation illness if a patient falls ill after receiving radiation exposure. There is no device to measure radiation exposure in this case. Doctors rely on blood analysis (lymphocytes) to assist with diagnosis. If lymphocytes are lower after 48 hrs post exposure, the radiation exposure is considered worse.
ContaminationA Geiger counter can be used to measure the exposure. Samples from different areas of the body can also be checked for the presence of radioactivity.
To take a look at some case studies involving radiation exposure and related injury, the following website link is available.
http://radiologyresearch.org/radiationsafety/rso_fot_chapter_4.htm
The outcome of a patient post radiation exposure is dependent on:(a) the patients overall health(b) the amount of radiation (dose)(c) the distribution over the body
Patients receiving greater than 6 Gy of radiation at the same time will die. Patients exposed to this level of radiation are monitored very closely. Symptoms are treated as they arise especially if it is irradiation which does not have any emergency treatment. If contamination is suspected, the radioactive material should be removed from the patient
immediately to prevent any further cross contamination. A Geiger counter is used to measure the amount of exposure.There are two categories of health risks associated with radiation exposure:
1. Stochastic Health Effects- results from chronic exposure. These effects occur overtime and are normally from low levels of exposure. Examples of stochastic health effects are: cancer, and genetic mutations
2. Non-Stochastic Health Effects- results from acute exposure. This normally occurs from high levels of radiation with the severity increasing as the exposure increases. Health effects that occurs as a result of acute exposure normally shows up immediately. Examples of Non-Stochastic Health effects are: burns, radiation poisoning, aging and death
Radiation Symbols:
The symbol is usually magenta or black and is usually shown on a yellow background. The sign is always posted wherever radiation is being used or radioactive material is present. This universal symbol has a few versions. Below are pictures of these symbols.
On February 15, 2007, the International Atomic energy Agency and International Organization for Standards introduced a new supplemental international radiation warning symbol. This new symbol was not designed to replace the existing trefoil symbol but to be used as a supplemental symbol. The new symbol shows the original trefoil with waves pointing to a skull and bone and a running figure.
In an effort to keep ourselves and
colleagues safe while working in a radiation environment, we need to pay full attention to all the preventative measures at our disposal. Always remember ALARA (As Low as Reasonable Achievable), remember to decrease our time spent in radiation areas, increase our distance from the source and always shield body areas that are considered radiosensitive. Contact your radiation safety officer and make sure he/she continues to track your monitoring devices on a monthly basis. Always have access to your radiation exposure records and talk to your radiation safety committee if you have issues or concerns.
If you are a healthcare provider who is pregnant and working in these radiation areas, consult your radiation safety department and investigate their policies for practicing while pregnant. It is in our own best interest that we continue to be aware, vigilant and educated about radiation safety and the potential problems if not taken seriously. REFERENCES
A Review of Ionizing Radiation. Gerard J. Celitans. National Education Press. Jan.1973An Introduction to Radiation Protection. 3rd Ed. Martin, A. and Harbison S.A., London: Chapman and Hall, 1986. Atoms, Radiation, and Radiation Protection, 2nd Edition. James E. Turner. Wiley-IntersciencesOSHA Occupational Radiation Safety (Audio book). Daniel Farb. University of Healthcare. Cdr Edition. January 2005)Radiation and Life. Eric J. Hall, professor of Radiology, College of Physicians and Surgeons, Columbia University, New York. http://radiologyresearch.org/radiationsafety/rso_fot_chapter_4.htmhttp://www.osha.gov/SLTC/radiation/National Research Council. Health Effects of Exposure to Low Levels of Ionizing Radiation, BEIR V. Washington, D.C.: National Academy Press, 1990.http://www.nrc.gov/reading-rm/basic-ref/teachers/09.pdf
•
•
•
•
•
•
••
•
Trefoil- international symbol
New International Symbol
44 CORONARY HEART ™

Date Name Location Website / Contact
2007September 5-8 8th Annual New Cardiovascular
HorizonsNew Orleans, LA, USA www.newcvhorizons.com
September 20-22 SICP Annual Conference St Louis, MO, USA www.sicp.com
October 6-10 SICP’s Signature RCIS Review Course at ACE
New York, NY, USA www.sicp.com
October 6-10 ACE: Advances in Cardiac & Endovascular Therapies
New York, NY, USA www.ny-ace.com
October 18-21 American Association of Cardiovascular and Pulmonary Rehabilitation - 22nd Annual Meeting
Salt Lake City, UT, USA www.aacvpr.org
October 20-24 Canadian Cardiovascular Congress 2007
Quebec City, Canada www.css.ca
October 20-25 TCT 2007: Transcatheter Cardiovascular Therapeutics
Washington DC, USA www.tct2007.com
October 21-22 TCT SICP’s Signature RCIS Review Course
Washington, DC www.sicp.com
October 22 Best Practices in Cardiovascular Nursing
Sutter Heart Institute Sacramento, CA
www.sutterheartinstitute.org
October 24-26 Corazon Fall Conference - “Changing Tides in Heart & Vascular Care: Are You Prepared?”
St. Petersburg, FL www.corazoninc.com
October 29-31 Heart Rhythm UK Congress Birmingham, UK www.ukheartrhythm.org.uk
November 4-7 AHA Scientific Sessions Orlando, FL, USA scientificsessions.americanheart.org
November 25-30 RSNA Chicago, IL, USA www.rsna.org
December 12-13 Madrid Arrhythmia Meeting Madrid, Spain www.mamweb.org
2008January 23-25 Advanced Angioplasty 2008 London, UK www.andvancedangioplasty.co.uk
March 29 - April 1 ACC 2008 + i2 Summit Chicago, IL, USA www.acc08.acc.org
May 14-17 Heart Rhythm 2008 - 29th Annual Scientific Sessions
San Francisco, CA, USA www.hrsonline.org
May 28-31 SCAI 31st Annual Scientific Sessions
Las Vegas, NV, USA www.scai.org
CONFERENCES
Conferences / Meetings
CORONARY HEART ™ 4�
Solutions for cardiovascular and imaging services
515 Old Swede Road, Suite C-1, Douglassville, PA 19518Phone 610-385-1227 n Fax 610-385-1229
www.healthworksonline.cc
Let us help you solve your cardiovascular
and imaging challenges.
“When I callHealthworks,I don’t have
to worry aboutquality.”
Charles Minehart, MD, FACCBerks Cardiologists, Ltd.
Pennsylvania
EDUCATIONBoost employee retention and cut the productivity losses that oftenaccompany new hires or service lines with Healthworks clinical education programs, available both onsite and online.
CONSULTING
Resolve challenging service line issues like staffing shortages, quality assurance, inventory control and cath lab planning and construction with expert advice from Healthworks consultants.
STAFFING
Meet your staffing needs with help from our experienced technologists and nurses. Or achieve financial efficiencies of up to 30% when Healthworks manages and staffs your lab. Staffing services are currently available in the Mid-Atlantic region.
To find out more, just call us at 1-610-385-1227 or e-mail [email protected].

CORONARY HEART ™ 47
EMPLOYMENT ADVERTISING
It’s a pleasure to come to a job where you are part of a
team you consider family. In the Cardiovascular Center
physicians and staff work together for the best interest
of our patients.
MelanieCardiac Cath Lab
11 years of service
Please visit to apply online
www.cmc-union.org EOE/AA
At Carolinas Medical Center-Union located in Monroe, North Carolina, we have built one of the best healthcare teams in the region and some of the finest professionals have made their home here. Come see why we’ve recently been named as one of America’s Hospitals of Choice, Employer of Choice and designated as one of the Top 40 Family Friendly Employers in NC for three consecutive years.
Opportunities Cardiovascular Nurse, current NC RN licensure
We are looking for great employees to support our mission and vision to provide excellent care to our community. We invite you to join our growing family.
Plus: Edition 9 Special FeatureCath Lab Design
Make sure you visit our website at www.zest4life.co.nz to view all of our current vacancies, or alternatively send us an enquiry by e-mail to [email protected]
Apply online at www.zest4life.co.nz
New Zealand Allied Health Careers
Cardio/Respiratory Technologist/Technician Waikato Hospital, HamiltonPosition No. 50707-39002 Are you a person of high integrity who enjoys working in a patient focussed and progressive environment, working with a dynamic multi-disciplinary team in a tertiary hospital?
If you are a Cardio / Respiratory Technologist or Technician with relevant qualifi cations and experience in invasive and / or non-invasive investigations we want to hear from you as you may be just the person we are looking for.
The hours are Monday to Friday with a component of on-call over 24hours/7 days. The numbers of hours worked are open to negotiation. A full orientation and opportunities for professional development will be given to the successful applicant.
Waikato Hospital is an innovative, progressive hospital that promotes a supportive and challenging clinical environment with further education opportunities. Hamilton off ers a vibrant, exciting city within a relaxed environment. A variety of outdoor recreation activities, amazing scenic countryside and beautiful beaches are within close travelling distance providing a wonderful lifestyle.
Cath Lab RNDay Shift Monday-Friday,
No weekends, holidays or on call.
Epharta Community Hospital is seeking a full-time Cardiovascular/Angiography Lab RNwho will be responsible for the care of Patients undergoing Diagnostic CardiacCatheterizations, Pacemaker Implantations,Tilt Table Testing and Peripheral Angiogram/Angioplasty procedures.
The qualified candidate must have current PARN licensure and be ACLS certified.Experience in hemodynamic monitoring, EKGinterpretation and moderate sedation is preferred. Critical care experience is required.
Ephrata Community Hospital is a 138-Bed,non-profit health services organization inLancaster County.
www.ephratahospital.org
[email protected] Martin Avenue
PO Box 1002Ephrata, PA 17522
EOE
GLOBAL PHOTO WINNERLancaster General Hospital, PA
(See their department in the next issue)
Truthin evidence-based medicine
Challengeconventional wisdom
Transformyour thinking
Sponsored by
F O U N D A T I O NCARDIOVASCULAR RESEARCH
®
Coronary_Heart_Journal_Ad.indd 1 8/17/07 10:15:03 AM
Related Documents