Coronary Flow Reserve Measurement Detects Transplant Coronary Artery Disease in Pediatric Heart Transplant Patients Stephan Schubert, MD, Hashim Abdul-Khaliq, MD, PhD, Ernst Wellnhofer, MD, Nicola Erika Hiemann, MD, Peter Ewert, MD, PhD, Hans Brendan Lehmkuhl, MD, Rudolf Meyer, MD, PhD, Oliver Miera, MD, Bjoern Peters, MD, Roland Hetzer, MD, PhD, and Felix Berger, MD, PhD Background: Cardiac allograft vasculopathy (CAV) in patients who have undergone heart transplantation leads to graft dysfunction and is still the major concern for long-term survival. Evaluation of coronary flow velocity reserve (CFR) has been established for diagnosis of CAV. Systemic application of adenosine vs intracoronary testing for CFR has been validated in adults; however, its accuracy in pediatric patients has not yet been proven. Methods: CFR was prospectively measured in 33 clinically asymptomatic pediatric heart transplant recipients. CFR measurements were made in the left anterior descending (LAD) artery using a 0.014-inch Doppler FloWire (Cardiometrics). CFR was defined as the ratio of hyperemic (after adenosine injection) to basal (before adenosine) average peak velocity (APV). Adenosine (Adrekar) was administered by intracoronary (15 or 30 g bolus) and systemic (0.1 mg/kg) injection in each patient. Epicardial CAV was evaluated in coronary angiograms (Stanford criteria) and microvascu- lopathy was diagnosed in endomyocardial biopsies (evidence of luminal stenosis) blinded to clinical data. Results: Thirty-three patients were included in this study. Their median age (range) was 11.9 (1.4 to 17) years and median post-transplant time 4.3 (1 to 11.7) years. Seventeen of the 33 patients had epicardial CAV (mainly peripheral obliterations or B1 and B2 lesions) and microvascular CAV. Epicardial CAV only was found in 4 patients and microvasculopathy only was present in only 1 patient. CFR was significantly reduced in patients with epicardial CAV and microvasculopathy when compared with patients without any signs of CAV: 206 53 vs 276 39 (p 0.001) for the systemic application and 213 50 vs 271 45 (p 0.004) for the intracoronary application. Conclusions: CFR and coronary vasoreactivity to adenosine are decreased in pediatric patients with CAV and correlate with histopathologic and angiographic evidence of microvascular disease. Measurement of CFR with intracoronary and systemic application of adenosine is comparable, while systemic application is necessary for non-invasive measurement of CFR in pediatric patients. J Heart Lung Transplant 2008;27:514 –21. Copyright © 2008 by the International Society for Heart and Lung Transplantation. Cardiac allograft vasculopathy (CAV) is still a major concern in pediatric heart transplant recipients, threat- ening long-term survival in the patients affected. 1–3 CAV is characterized by progressive vascular stenosis, finally leading to acute or chronic ischemia of the graft. Its lesions and its distribution within the coronary arteries are heterogeneous and therefore the risk of angio- graphic underestimation is high. 2,4 Therapeutic options are mainly limited to interventional or surgical ap- proaches to proximal lesions, but CAV frequently also affects intermediate vessels and even leads to luminal stenosis of small intramyocardial coronary arteries, as found in endomyocardial biopsies. 2,4–6 To date, no standard diagnostic procedure has been established that indicates involvement of both epicardial and small intramyocardial blood vessels. Immune-dependent and -independent processes have been demonstrated to play an important role in the development of coronary endothelial dysfunction in the transplanted heart, which is a key event in the development of CAV. 2,7,8 Progressive CAV has been shown to reduce endothelial vasomotor response to physiologic or pharmaceutical stimuli that might indicate small vessel disease. 2,4–6 The coronary flow velocity reserve (CFR) may be tested as described by Doucette et al. 9 It is defined by From the Department of Congenital Heart Defects/Pediatric Cardiol- ogy, Deutsches Herzzentrum Berlin, Berlin, Germany. Submitted November 2, 2007; revised January 31, 2008; accepted February 6, 2008. Reprint requests: Stephan Schubert, MD, Department of Congenital Heart Defects/Pediatric Cardiology, Deutsches Herzzentrum Berlin, Augustenburger Platz 1, Berlin 13353, Germany. Telephone: 49- 30-4593-2800. Fax: 49-30-4593-2900. E-mail: [email protected] Copyright © 2008 by the International Society for Heart and Lung Transplantation. 1053-2498/08/$–see front matter. doi:10.1016/ j.healun.2008.02.005 514 ALLOGRAFT VASCULOPATHY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CCSPB
B
M
R
C
Cceilla
Fo
F
HA3CTj
5
ALLOGRAFT VASCULOPATHY
oronary Flow Reserve Measurement Detects Transplantoronary Artery Disease in Pediatric Heart Transplant Patients
tephan Schubert, MD, Hashim Abdul-Khaliq, MD, PhD, Ernst Wellnhofer, MD, Nicola Erika Hiemann, MD,eter Ewert, MD, PhD, Hans Brendan Lehmkuhl, MD, Rudolf Meyer, MD, PhD, Oliver Miera, MD,joern Peters, MD, Roland Hetzer, MD, PhD, and Felix Berger, MD, PhD
ackground: Cardiac allograft vasculopathy (CAV) in patients who have undergone heart transplantation leads tograft dysfunction and is still the major concern for long-term survival. Evaluation of coronary flowvelocity reserve (CFR) has been established for diagnosis of CAV. Systemic application of adenosinevs intracoronary testing for CFR has been validated in adults; however, its accuracy in pediatricpatients has not yet been proven.
ethods: CFR was prospectively measured in 33 clinically asymptomatic pediatric heart transplant recipients.CFR measurements were made in the left anterior descending (LAD) artery using a 0.014-inchDoppler FloWire (Cardiometrics). CFR was defined as the ratio of hyperemic (after adenosineinjection) to basal (before adenosine) average peak velocity (APV). Adenosine (Adrekar) wasadministered by intracoronary (15 or 30 �g bolus) and systemic (0.1 mg/kg) injection in eachpatient. Epicardial CAV was evaluated in coronary angiograms (Stanford criteria) and microvascu-lopathy was diagnosed in endomyocardial biopsies (evidence of luminal stenosis) blinded to clinicaldata.
esults: Thirty-three patients were included in this study. Their median age (range) was 11.9 (1.4 to 17) yearsand median post-transplant time 4.3 (1 to 11.7) years. Seventeen of the 33 patients had epicardialCAV (mainly peripheral obliterations or B1 and B2 lesions) and microvascular CAV. Epicardial CAVonly was found in 4 patients and microvasculopathy only was present in only 1 patient. CFR wassignificantly reduced in patients with epicardial CAV and microvasculopathy when compared withpatients without any signs of CAV: 206 � 53 vs 276 � 39 (p � 0.001) for the systemic applicationand 213 � 50 vs 271 � 45 (p � 0.004) for the intracoronary application.
onclusions: CFR and coronary vasoreactivity to adenosine are decreased in pediatric patients with CAV andcorrelate with histopathologic and angiographic evidence of microvascular disease. Measurement ofCFR with intracoronary and systemic application of adenosine is comparable, while systemicapplication is necessary for non-invasive measurement of CFR in pediatric patients. J Heart LungTransplant 2008;27:514 –21. Copyright © 2008 by the International Society for Heart and Lung
Transplantation.gapasfsii-pewPvs
ardiac allograft vasculopathy (CAV) is still a majoroncern in pediatric heart transplant recipients, threat-ning long-term survival in the patients affected.1–3 CAVs characterized by progressive vascular stenosis, finallyeading to acute or chronic ischemia of the graft. Itsesions and its distribution within the coronary arteriesre heterogeneous and therefore the risk of angio-
rom the Department of Congenital Heart Defects/Pediatric Cardiol-gy, Deutsches Herzzentrum Berlin, Berlin, Germany.Submitted November 2, 2007; revised January 31, 2008; accepted
ebruary 6, 2008.Reprint requests: Stephan Schubert, MD, Department of Congenital
eart Defects/Pediatric Cardiology, Deutsches Herzzentrum Berlin,ugustenburger Platz 1, Berlin 13353, Germany. Telephone: ��49-0-4593-2800. Fax: ��49-30-4593-2900. E-mail: [email protected] © 2008 by the International Society for Heart and Lungransplantation. 1053-2498/08/$–see front matter. doi:10.1016/
t.healun.2008.02.005
14
raphic underestimation is high.2,4 Therapeutic optionsre mainly limited to interventional or surgical ap-roaches to proximal lesions, but CAV frequently alsoffects intermediate vessels and even leads to luminaltenosis of small intramyocardial coronary arteries, asound in endomyocardial biopsies.2,4–6 To date, notandard diagnostic procedure has been established thatndicates involvement of both epicardial and smallntramyocardial blood vessels. Immune-dependent andindependent processes have been demonstrated tolay an important role in the development of coronaryndothelial dysfunction in the transplanted heart,hich is a key event in the development of CAV.2,7,8
rogressive CAV has been shown to reduce endothelialasomotor response to physiologic or pharmaceuticaltimuli that might indicate small vessel disease.2,4–6
The coronary flow velocity reserve (CFR) may be
ested as described by Doucette et al.9 It is defined by
tbciaowmcctedchMvCa
bdlvh
MS
WaypwUaTtIcdoSunost
E
BaaPscial
M
Fut��b(S(evaiasttemobbwt
ES
Bccsuge
The Journal of Heart and Lung Transplantation Schubert et al. 515Volume 27, Number 5
he ratio between maximum and baseline flow and haseen shown to indicate the functional significance oforonary artery stenosis.9,10 CFR is divided into a phys-ologic reserve, which is stimulated by a physical mech-nism such as coronary occlusion, ischemia inductionr oxygen demand, and a pharmacologic reserve,hich is induced by drug administration. CFR may beeasured using a Doppler guide-wire to measure the
oronary flow at baseline and after intracoronary appli-ation of acetylcholine or nitro-oxygen (NO), as endo-helium-dependent vasodilators, or adenosine, as anndothelium-independent vasodilator.9,11–13 Recentata from a study using an intracoronary Doppleratheter have shown that, at the same dose, adenosineas greater vasodilator potency than dipyridamole.14
oreover, adenosine as an endothelium-independentasodilator has some advantages in the measurement ofFR, such as precise timing, more favorable kineticsnd quick reversibility.10
The aim of this study was to evaluate the relationshipetween CFR, using an endothelium-independent vaso-ilator (adenosine), and angiographic or histopatho-
ogic signs of CAV. We also sought to validate systemics intracoronary application of vasodilator in pediatriceart transplant patients.
ETHODStudy Design
e performed a prospective study with 33 asymptom-tic consecutive heart transplant recipients aged �18ears at time of transplantation. The parents of allatients gave informed written consent and the studyas approved by the ethics committee of Chariténiversity Medicine, Berlin. Exclusion criteria werecute cellular (International Society for Heart and Lungransplantation [ISHLT] Grade �1A) or humoral rejec-
ion on endomyocardial biopsy (evidence of IgG, IgA,gM, C3c, C1q by immunohistochemistry) at time oforonary angiography, focal stenosis in the left anteriorescending (LAD) artery of any degree or Type A lesionf the proximal coronary vessels according to thetanford criteria,15 second-degree or total atrioventric-lar block without pacemaker implantation, hemody-amically significant valvular disease, severe chronicbstructive pulmonary disease, pulmonary hyperten-ion and bronchospasm. Vasoactive drugs were discon-inued 12 to 24 hours before examination in all patients.
Table 1. Demographic Data (Median and Range)
Age (years) Post-tra
With CAV (n � 22) 11.4 (4.7–17.7) 5Without CAV (n � 11) 11.5 (1.4–16.9) 3
CAV, cardiac allograft vasculopathy.
ap � 0.02.picardial CAV
iplane selective angiograms (12.5 frame/s) of coronaryrteries were acquired digitally with standard biplanengiographic X-ray equipment (Integris/LARC System;hilips) using a non-ionic contrast agent and weretored in Dicom format. CAV was scored by a blindedardiologist and pediatric cardiologist with experiencen the detection of CAV.16,17 Epicardial CAV was gradedccording to the Stanford criteria for signs of B1 or B2esions and for peripheral obliterations.15
easurement of CFR
low velocity was always measured in the LAD arterysing a 0.014-inch Doppler FloWire (Cardiometrics) inwo ways: first, before and after intracoronary bolus (15g in 0.3 ml for children �20 kg body weight [BW], 30g in 0.3 ml for children �20 kg BW); and second,efore and after systemic or intravenous bolus injection0.1 mg/kg BW in 1 to 2 ml) of adenosine (Adrekar;anofi-Synthelabo, Germany).9 Coronary flow reserveCFR � PAPV:BAPV) was defined as the ratio of hyper-mic (after adenosine injection) peak average peakelocity (PAPV) divided by the basal (before injection ofdenosine) average peak velocity (BAPV). Percentage ofncrease (%) was defined as ratio · 100. Intracoronarynd systemic application was performed in the sameession, with restitution of normal coronary flow pat-ern to baseline measurement after each injection, sohat a minimum of two injections were performed inach manner and in every patient. Repeated measure-ents were possible due to the short half-life of aden-
sine and any influence of the prior measurement coulde excluded by letting the coronary flow return toaseline after each measurement. Hemodynamic dataere recorded for each patient by standardized moni-
oring.
ndomyocardial Biopsy Harvest and Histopathologictudies
iopsy harvest and tissue preparation were done ac-ording to standard clinical practice at the end oforonary angiographies and after CFR testing as de-cribed elsewhere.2 Microvasculopathy was diagnosedsing hematoxylin–eosin (H&E) staining by a patholo-ist blinded to clinical data and included grading ofndothelial cell swelling and vessel wall thickening
lant time (years) Weight (kg) Height (cm)
(1.6–11.7) 32.5 (11–60) 137 (88–177)(1–11)a 34.6 (8.2–57) 140 (80–176)
nsp
.4
.5

wQ1webcap
S
DrCbSdfdp(sc
RP
Tppti(c(1t
(4vdEanhgwT(i
C
CaaPTatss0
ipcLsB0wp
T
WW
Cf
T
N
WAAM
aa
516 Schubert et al. The Journal of Heart and Lung TransplantationMay 2008
ith regard to evidence of luminal obstruction.5,18 Theuilty phenomenon, as described by Billingham in981, was detected in only 4 of 32 patients togetherith histologic CAV.19,20 To prevent potential residual
ffects of acute cellular rejection on CFR testing, alliopsies with evidence of acute cellular rejection ac-ording to the ISHLT criteria were excluded from thenalysis. In total, 90 biopsies were evaluated (2.9 � 1.3er patient).
tatistical Analysis
escriptive statistics were used (including median andange, mean � standard deviation or standard error).omparative statistical analyses were performed in alinded manner by means of paired and unpairedtudent’s t-test for continuous variables with a normalistribution, regression analysis, Mann–Whitney U-testor metric parameters and not normally distributedata, chi-square test for nominal and ordinal scaledarameters and Fisher’s exact test. SPSS for Windowsrelease 9.0) and STATVIEW (version 5, SAS Institute)oftware were used. p � 0.05 was considered statisti-ally significant.
ESULTSatient Population
hirty-three pediatric patients (16 girls, 17 boys) wererospectively enrolled. All patients underwent heart trans-lantation between 2003 and 2006. Reasons for heartransplantation were dilated cardiomyopathy in the major-ty of patients (n � 21), complex congenital heart diseasen � 8), restrictive cardiomyopathy (n � 2), hypertrophicardiomyopathy (n � 1) and endocardial fibroelastosisn � 1). The median age (range) of the patients was1.9 (1.4 to 17) years and the median post-transplantime was 4.3 (1 to 11.7) years. In 17 patients epicardial
able 2. Hemodynamic Data (Median and Range)
Mean BP (mm Hg) Cardiac index (lit
ith CAV (n � 22) 73 (50–89) 4.1 (2.3–ithout CAV (n � 11) 74 (60–87) 4.0 (2.3–
AV, cardiac allograft vasculopathy; RVEDP, right ventricular end-diastolic presraction.
able 3. Basal and Peak Average Peak Flow of Patients With/Withou
o. BAPV (cm/s)
ithout any CAV (n � 11) 25 � 2a
ngiographic CAV and microvasculopathy (n � 17) 29 � 6ngiographic CAV only (n � 4) 16 � 6icrovasculopathy only (n � 1) 31 � 0
Basal APV was significantly increased in patients with histologic signs of CAVnd intracoronary administration ( bp � 0.001 and cp � 0.004). APV, average p
llograft vasculopathy.angiographic) and microvascular CAV was detected. Inpatients epicardial CAV was seen but without micro-
asculopathy. In only 1 patient was microvasculopathyetected, without angiographic signs of epicardial CAV.leven patients showed no signs of CAV in eitherngiographic or histopathologic analysis. There wereo statistically significant differences in age, weight,eight or hemodynamic parameters between the tworoups (Tables 1 and 2). Only the post-transplant timeas significantly lower in patients without CAV (p � 0.02;able 1). In 3 of 30 patients a temporary atrioventricularAV) block occurred for 2 to 3 seconds, but no therapeuticntervention was necessary.
oronary Flow Velocity and Flow Reserve
oronary flow velocities in the LAD artery at rest (basalverage peak flow � BAPV [cm/s]) and after adenosinedministration (peak average peak flow velocities �
APV [cm/s]) and the calculated CFR ratio are shown inable 3. A CFR increase ([ratio � PAPV:BAPV] · 100)fter adenosine injection was significantly lower in pa-ients with vs without histopathologic and angiographicigns of CAV: 206 � 53 vs 276 � 39 (p � 0.001) for theystemic application and 213 � 50 vs 271 � 45 (p �.004) for the intracoronary application (see Table 3).Basal average peak flow (BAPV) was significantly
ncreased in patients with CAV (see Table 3). Basal oreak average peak flow (BAPV or PAPV) showed noorrelation with left ventricular end-diastolic pressure,V ejection fraction, left atrial pressure or blood pres-ure (BP). CFR showed a weak correlation with meanP (r � 0.41, p � 0.02) and diastolic BP (r � 0.39, p �.02), but no correlation with age, post-transplant time,eight or height. CFR was significantly lower in 1atient with microvasculopathy only (180%) and was
min/m2) RVEDP (mm Hg) LVEDP (mm Hg) LVEF (%)
) 5.3 (2–18) 8.1 (2–20) 69 (60–75)) 4.7 (2–18) 6.7 (2–16) 69 (58–73)
e; LVEDP, left ventricular end-diastolic pressure; LVEF, left ventricular ejection
V (Mean � SD)
temic ADP Intracoronary ADP
APV (cm/s) CFR (%) BAPV (cm/s) PAPV (cm/s) CFR (%)
67 � 10 276b 24 � 3a 64 � 12 271c
63 � 24 206 29 � 9 61 � 23 21344 � 13 256 17 � 7a 44 � 19 26456 � 0 180 30 � 0a 53 � 0 176
� 0.01). aBasal APV vs Peak APV was significantly different for both systemicvelocity; CFR, coronary flow reserve; ADP, adenosine diphosphate; CAV, cardiac
ers/
6.26.0
sur
t CA
Sys
P
(peak

wea
A
Saombepp
S
A(sOsmwT
D
Iwmpt
ciiacasprw
Fl
Fcl
The Journal of Heart and Lung Transplantation Schubert et al. 517Volume 27, Number 5
ithin the normal range in those patients with signs ofpicardial CAV alone (276 � 55%) for both systemicnd intracoronary measurements.
ngiographic and Histopathologic Results
eventeen of 33 patients had signs of epicardial CAV inngiography (B1 or B2 lesions) with/without peripheralbliterations and without macroscopic signs of proxi-al stenosis (Figures 1 and 3). In these 17 patients,
iopsy-proven microvasculopathy was detected in �50ndomyocardial biopsies (median 2.8 biopsies for eachatient). Also, CFR was significantly reduced in everyatient (n � 18) with microvasculopathy (Figure 4).
ystemic vs Intracoronary Application of Adenosine
comparison of intracoronary and systemic applicationsee Figures 2 and 5) of adenosine showed no statisticallyignificant difference for basal average peak flow � BAPV.nly peak APV was slightly higher after systemic adeno-
ine application when compared with intracoronary ad-inistration (64 � 19 vs 59 � 14 cm/s) in all patients,ithout reaching statistical significance (p � 0.07; seeable 3).
ISCUSSION
n the present study, endothelium-independent CFRas tested as a surrogate marker for epicardial andicrovascular CAV in a single-center experience of 33ediatric patients after heart transplantation. We found
igure 1. Angiographic studies from 2 patients. Left: a patient withoesions with an intramyocardial pacemaker electrode (IMEG) in place.
hat patients with evidence of epicardial and microvas- l
ular CAV had a significantly reduced CFR after admin-stration of adenosine, and similar results were obtainedf adenosine was given by systemic or intracoronarypplication. Further, epicardial CAV together with mi-rovasculopathy was predominant in our populationnd diffuse involvement of coronary blood vesselseems to be an important factor in CAV among pediatricatients. We consider systemic testing of CFR to be aeliable diagnostic tool for identifying pediatric patientsith both epicardial and microvascular disease. Normal
igns of CAV; right: signs of CAV with peripheral obliterations and B2
igure 2. Comparison of intracoronary vs systemic adenosine appli-ation showing mean CFR in patients without signs of microvascu-opathy (white boxplots, n � 11) vs those with signs of microvascu-
ut s
opathy (shaded boxplots, n � 17).
vtfaci
sitC
ulpCultcipmnstaplrpw
tmiocdbmta
Ftpc
F(
518 Schubert et al. The Journal of Heart and Lung TransplantationMay 2008
alues for children have been obtained only after correc-ion of transposition of the great arteries, although datarom adults obtained by the same technique are availablend can be used for comparison.13,21 CAV may present asoncentric medial disease in the microvasculature or asntimal disease in the epicardial coronary arteries.2
Coronary microvascular dysfunction has been de-cribed as a reduced response of Doppler-derived CFRn adult and pediatric patients after heart transplanta-ion.9,11,12 Only a small number of studies have testedFR in pediatric patients, mainly in patients who have
igure 3. Patients’ CFR (%) in relation to epicardial CAV according tohe Stanford criteria. Predominantly B1 and B2 lesions are seen inatients with a reduced CFR. Open circles: no CAV (n � 11); shadedircles: CAV (epicardial and microvasculopathy, n � 17).
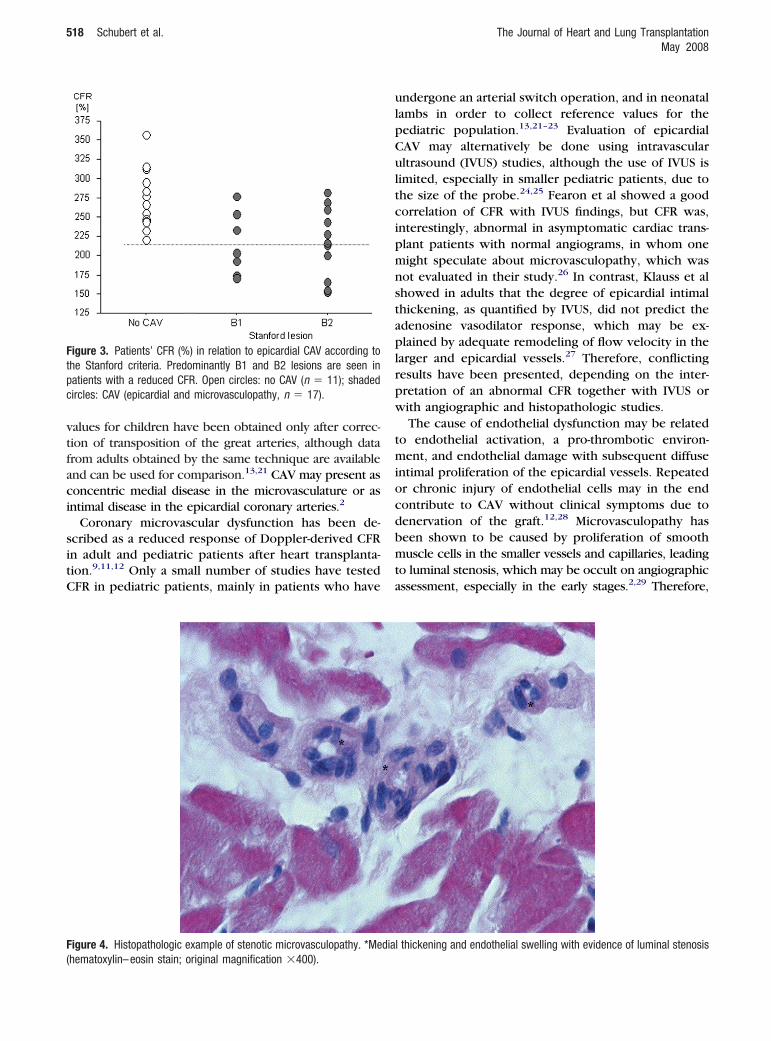
igure 4. Histopathologic example of stenotic microvasculopathy. *Me
hematoxylin–eosin stain; original magnification �400).ndergone an arterial switch operation, and in neonatalambs in order to collect reference values for theediatric population.13,21–23 Evaluation of epicardialAV may alternatively be done using intravascularltrasound (IVUS) studies, although the use of IVUS is
imited, especially in smaller pediatric patients, due tohe size of the probe.24,25 Fearon et al showed a goodorrelation of CFR with IVUS findings, but CFR was,nterestingly, abnormal in asymptomatic cardiac trans-lant patients with normal angiograms, in whom oneight speculate about microvasculopathy, which wasot evaluated in their study.26 In contrast, Klauss et alhowed in adults that the degree of epicardial intimalhickening, as quantified by IVUS, did not predict thedenosine vasodilator response, which may be ex-lained by adequate remodeling of flow velocity in the
arger and epicardial vessels.27 Therefore, conflictingesults have been presented, depending on the inter-retation of an abnormal CFR together with IVUS orith angiographic and histopathologic studies.The cause of endothelial dysfunction may be related
o endothelial activation, a pro-thrombotic environ-ent, and endothelial damage with subsequent diffuse
ntimal proliferation of the epicardial vessels. Repeatedr chronic injury of endothelial cells may in the endontribute to CAV without clinical symptoms due toenervation of the graft.12,28 Microvasculopathy haseen shown to be caused by proliferation of smoothuscle cells in the smaller vessels and capillaries, leading
o luminal stenosis, which may be occult on angiographicssessment, especially in the early stages.2,29 Therefore,
l thickening and endothelial swelling with evidence of luminal stenosis
dia
aiame
emoCbbwem
mipa
ineaaMrw(ai
vaTCbaC
Fow PV
s
The Journal of Heart and Lung Transplantation Schubert et al. 519Volume 27, Number 5
ngiographic and histopathologic evaluations are neededn the post-transplant period to exclude epicardial CAVnd microvasculopathy. However, serial catheterizationay still be complicated in pediatric transplant recipi-
nts.We cannot differentiate between the influence of
picardial and microvascular CAV on CFR measure-ents in this study, because only a small number of
ur patients had epicardial CAV only with normalFR. CFR was significantly reduced in patients withoth signs of epicardial CAV and microvasculopathy,ut it was also significantly reduced in all patientsith microvasculopathy. Additional studies are nec-
ssary to differentiate between epicardial CAV andicrovasculopathy.Nevertheless, there is a need for a non-invasiveethod (e.g., echocardiography or magnetic resonance
maging) to detect CAV, especially in the pediatricopulation, to facilitate post-transplant management
igure 5. Comparison of systemic (A, C) and intracoronary (B, D) applr CFR (ratio: 3.1 vs 2.7). (A) and (B) are from a patient without CAV,ith flow velocity marked at B � basal and P � peak and ratio � PA
ignal (upper panel).
nd to further improve patients’ comfort, which are s
mportant factors. However, alternative methods haveot yet been evaluated in pediatric patients. Redbergt al and Rodrigues et al non-invasively used transesoph-geal echocardiography to test CFR in adults beforend after intravenous administration of adenosine.10,30
uehling et al showed reduced myocardial perfusioneserve and transmural perfusion gradient in patientsith CAV assessed by magnetic resonance imaging
MRI).31 Thus, a non-invasive approach may be possiblend may include transthoracic echocardiographic test-ng of CFR in pediatric patients.
In addition to the influence of epicardial and micro-ascular CAV on CFR, our intention was to compare thepplication of intravenous and intracoronary adenosine.his is needed for future non-invasive measurement ofFR. As we have shown that there is no differenceetween the effects of intracoronary and intravenouspplication of adenosine, non-invasive measurement ofFR using transthoracic echocardiography may be pos-
ion of adenosine shows no significant difference in vascular response(C) and (D) are from a patient with CAV. Average peak velocity (APV)
BAPV calculated. S � systolic and D � diastolic according to the ECG
icatand
:
ible and deserves further study.

S
Iotlecdcprwmpto
medwtisaiC
T
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
520 Schubert et al. The Journal of Heart and Lung TransplantationMay 2008
tudy Limitations
ntracoronary measurements of CFR in healthy childrenf the same age could not be included in our study dueo ethical constraints. Because adenosine is an endothe-ium-independent vasodilator, the present study did notvaluate coronary endothelial function. However, intra-oronary injection of acetylcholine as an endothelium-ependent vasodilator is associated with a high risk oforonary spasms and other serious side effects, asrevious described.11 Nitroglycerine was not appliedoutinely before coronary angiography, and thereforee could not exclude residual effects on CFR measure-ents due to coronary spasm. This was done to avoidossible side effects of nitroglycerine in terms of pa-ients’ safety and to exclude possible underestimationf CFR due to previous vasodilation.In conclusion, intracoronary Doppler flow measure-ent of CFR with adenosine is a good indicator of
ndothelium-independent vasodilator response in chil-ren after heart transplantation and may be performedithout any significant side effects in pediatric heart
ransplant recipients. Reduced CFR after systemic orntracoronary application of adenosine is associatedimilarly with CAV based on biopsy and coronaryngiography, which might be important in future stud-es for establishing a non-invasive diagnostic tool forAV in children.
he authors thank A. Gale (ELS) for editorial assistance.
EFERENCES
1. Pahl E, Naftel DC, Kuhn MA, et al. The impact and outcome oftransplant coronary artery disease in a pediatric population: a9-year multi-institutional study. J Heart Lung Transplant 2005;24:645–51.
2. Hiemann NE, Wellnhofer E, Knosalla C, et al. Prognostic impactof microvasculopathy on survival after heart transplantation:evidence from 9713 endomyocardial biopsies. Circulation 2007;116:1274–82.
3. Pahl E, Fricker FJ, Armitage J, et al. Coronary arteriosclerosis inpediatric heart transplant survivors: limitation of long-term sur-vival. J Pediatr 1990;116:177–83.
4. Johnson DE, Alderman EL, Schroeder JS, et al. Transplant coro-nary artery disease: histopathologic correlations with angio-graphic morphology. J Am Coll Cardiol 1991;17:449–57.
5. Hiemann NE, Wellnhofer E, Abdul-Khaliq H, Hetzer R, Meyer R.Epicardial and microvascular graft vessel disease in children. ActaPaediatr 2004;93(suppl):70–4.
6. Hiemann NE, Wellnhofer E, Hetzer T, Meyer R. Small vesseldisease after heart transplantation: impact of immunologic andnonimmunologic risk factors. Transplant Int 2005;18:908–14.
7. Mills RM Jr, Billett JM, Nichols WW. Endothelial dysfunction earlyafter heart transplantation. Assessment with intravascular ultra-sound and Doppler. Circulation 1992;86:1171–4.
8. Davis SF, Yeung AC, Meredith IT, et al. Early endothelial dysfunc-tion predicts the development of transplant coronary artery
disease at 1 year posttransplant. Circulation 1996;93:457–62.9. Doucette JW, Corl PD, Payne HM, et al. Validation of a Dopplerguide wire for intravascular measurement of coronary artery flowvelocity. Circulation 1992;85:1899–911.
0. Redberg RF, Sobol Y, Chou TM, et al. Adenosine-induced coro-nary vasodilation during transesophageal Doppler echocardiogra-phy. Rapid and safe measurement of coronary flow reserve ratiocan predict significant left anterior descending coronary stenosis.Circulation 1995;92:190–6.
1. Treasure CB, Vita JA, Ganz P, et al. Loss of the coronarymicrovascular response to acetylcholine in cardiac transplantpatients. Circulation 1992;86:1156–64.
2. Gagliardi MG, Crea F, Polletta B, et al. Coronary microvascularendothelial dysfunction in transplanted children. Eur Heart J2001;22:254–60.
3. Oskarsson G, Pesonen E, Munkhammar P, Sandstrom S, Jogi P.Normal coronary flow reserve after arterial switch operation fortransposition of the great arteries: an intracoronary Dopplerguidewire study. Circulation 2002;106:1696–702.
4. Chou TM, Sudhir K, Amidon TM, et al. Comparison of adenosineto dipyridamole in degree of coronary hyperemic response inheart transplant recipients. Am J Cardiol 1996;78:908–13.
5. Gao SZ, Alderman EL, Schroeder JS, Silverman JF, Hunt SA.Accelerated coronary vascular disease in the heart transplantpatient: coronary arteriographic findings. J Am Coll Cardiol1988;12:334–40.
6. Wellnhofer E, Goubergrits L, Kertzscher U, Affeld K. In-vivo coro-nary flow profiling based on biplane angiograms: influence ofgeometric simplifications on the three-dimensional reconstructionand wall shear stress calculation. Biomed Eng Online 2006;5:39.
7. Wellnhofer E, Wahle A, Mugaragu I, et al. Validation of anaccurate method for three-dimensional reconstruction and quan-titative assessment of volumes, lengths and diameters of coronaryvascular branches and segments from biplane angiographic pro-jections. Int J Card Imaging 1999;15:339–53.
8. Hiemann NE, Meyer R, Wellnhofer E, et al. Correlation of angio-graphic and immunohistochemical findings in graft vessel diseaseafter heart transplantation. Transplant Proc 2001;33:1586–90.
9. Gopal S, Narasimhan U, Day JD, et al. The Quilty lesion enigma:focal apoptosis/necrosis and lymphocyte subsets in human car-diac allografts. Pathol Int 1998;48:191–8.
0. Joshi A, Masek MA, Brown BA Jr, Weiss LM, Billingham ME.“Quilty” revisited: a 10-year perspective. Hum Pathol 1995;26:547–57.
1. Hauser M, Bengel FM, Kuhn A, et al. Myocardial blood flow and flowreserve after coronary reimplantation in patients after arterial switchand ross operation. Circulation 2001;103:1875–80.
2. Oskarsson G, Pesonen E, Gudmundsson S, et al. Coronary flowreserve in the newborn lamb: an intracoronary Doppler guidewire study. Pediatr Res 2004;55:205–10.
3. Gagliardi MG, Adorisio R, Crea F, et al. Abnormal vasomotorfunction of the epicardial coronary arteries in children five toeight years after arterial switch operation: an angiographic andintracoronary Doppler flow wire study. J Am Coll Cardiol 2005;46:1565–72.
4. Nicolas RT, Kort HW, Balzer DT, et al. Surveillance for transplantcoronary artery disease in infant, child and adolescent heart trans-plant recipients: an intravascular ultrasound study. J Heart LungTransplant 2006;25:921–7.
5. Kuhn MA, Jutzy KR, Deming DD, et al. The medium-termfindings in coronary arteries by intravascular ultrasound ininfants and children after heart transplantation. J Am CollCardiol 2000;36:250 – 4.
6. Fearon WF, Nakamura M, Lee DP, et al. Simultaneous assessmentof fractional and coronary flow reserves in cardiac transplant
recipients. Circulation 2003;108:1605–10.
2
2
2
3
3
The Journal of Heart and Lung Transplantation Schubert et al. 521Volume 27, Number 5
7. Klauss V, Ackermann K, Henneke KH, et al. Epicardial intimalthickening in transplant coronary artery disease and resistancevessel response to adenosine: a combined intravascular ultra-sound and Doppler study. Circulation 1997;96:II-159–64.
8. Pietra B, Boucek M. Coronary artery vasculopathy in pediatriccardiac transplant patients: the therapeutic potential of immuno-modulators. Paediatr Drugs 2003;5:513–24.
9. Hiemann NE, Wellnhofer E, Meyer R, et al. Prevalence of graft
vessel disease after paediatric heart transplantation: a singlecentre study of 54 patients. Interact Cardiovasc Thorac Surg2005;4:434 –9.
0. Rodrigues AC, Frimm CDE, Bacal F, et al. Coronary flow reserveimpairment predicts cardiac events in heart transplant patients withpreserved left ventricular function. Int J Cardiol 2005;103:201–6.
1. Muehling OM, Wilke NM, Panse P, et al. Reduced myocardialperfusion reserve and transmural perfusion gradient in hearttransplant arteriopathy assessed by magnetic resonance imaging.
J Am Coll Cardiol 2003;42:1054–60.
Related Documents











