Coronary bifurcation lesions: To stent one branch or both? A meta-analysis of patients treated with drug eluting stents Giampaolo Niccoli ⁎ ,1 , Giuseppe Ferrante 1 , Italo Porto, Francesco Burzotta, Antonio M. Leone, Rocco Mongiardo, Mario A. Mazzari, Carlo Trani, Antonio G. Rebuzzi, Filippo Crea Institute of Cardiology, Catholic University of the Sacred Heart, Largo Agostino Gemelli, 8, 00168 Rome, Italy Received 18 November 2007; received in revised form 2 September 2008; accepted 12 October 2008 Available online 22 November 2008 Abstract Background: In the treatment of coronary bifurcation lesions (CBL), with drug eluting stents (DES), we sought to compare angiographic and clinical outcomes of a simple strategy of stenting main vessel only with balloon dilatation of the side branch with a complex strategy of stenting both branches. Methods: We performed a meta-analysis of six studies, randomized (three) or prospective observational (three), including 963 patients, that directly compared the simple strategy to the complex strategy, in the treatment of CBL with DES. Results: Final minimal lumen diameter (MLD) of the side branch was significantly smaller in the simple strategy group [WMD − 0.50 mm, 95% CI (− 0.76, − 0.24), p b 0.00001]. The risk of main vessel restenosis [RR 0.66, 95% CI (0.38–1.17), p = 0.16], side branch restenosis [RR 0.62, 95% CI (0.24–1.56), p = 0.31], follow up death [RR 0.60, 95% CI (0.19–1.86), p = 0.38], follow up myocardial infarction [RR 0.71, 95% CI (0.46–1.10), p = 0.13], or target vessel revascularization [RR 0.90, 95% CI (0.56–1.46), p = 0.67] was similar between the two strategies. The simple strategy showed a trend to a lower risk of early myocardial infarction [RR 0.65, 95% CI (0.41–1.05), p = 0.08]. Conclusion: In the treatment of unselected CBL with DES, the complex strategy does not penalize angiographic and clinical outcomes compared to the simple strategy. Further randomized studies are needed to assess the benefit of simple or complex strategy in the treatment of specific subsets of bifurcated lesions. © 2008 Elsevier Ireland Ltd. All rights reserved. Keywords: Coronary bifurcation lesions; Drug eluting stent; Meta-analysis 1. Introduction Coronary bifurcation lesions (CBL), accounting for 15– 18% of coronary angioplasty procedures [1], remain a challenge for the interventional cardiologist. Balloon angioplasty for the treatment of CBL was associated with poor immediate and long term results [2]. Bare metal stents (BMS) have solved some limitations of balloon angioplasty, yet plaque shifting towards the side branch after main vessel stenting has been increasingly recognized as a significant complication of the procedure requiring the use of one or more additional stents in the side branch [3]. Different techniques based on the use of multiple BMS have been described [4]. Non-randomized studies with BMS, however, have suggested improved long term results with a strategy of stenting the main vessel only with balloon dilatation of the side branch (simple strategy) compared to more complex approaches with stenting of both branches (complex strategy) [5–9]. The introduction of drug eluting stents (DES) has been advocated as the final solution in the treatment of CBL, due to their excellent results in both simple and complex lesion subsets [10,11]. International Journal of Cardiology 139 (2010) 80 – 91 www.elsevier.com/locate/ijcard ⁎ Corresponding author. Tel.: +39 06 30154187; fax: +39 06 3055535. E-mail address: [email protected] (G. Niccoli). 1 The authors contributed equally to the paper. 0167-5273/$ - see front matter © 2008 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijcard.2008.10.016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ology 139 (2010) 80–91www.elsevier.com/locate/ijcard
International Journal of Cardi
Coronary bifurcation lesions: To stent one branch or both?A meta-analysis of patients treated with drug eluting stents
Giampaolo Niccoli ⁎,1, Giuseppe Ferrante 1, Italo Porto, Francesco Burzotta, Antonio M. Leone,Rocco Mongiardo, Mario A. Mazzari, Carlo Trani, Antonio G. Rebuzzi, Filippo Crea
Institute of Cardiology, Catholic University of the Sacred Heart, Largo Agostino Gemelli, 8, 00168 Rome, Italy
Received 18 November 2007; received in revised form 2 September 2008; accepted 12 October 2008Available online 22 November 2008
Abstract
Background: In the treatment of coronary bifurcation lesions (CBL), with drug eluting stents (DES), we sought to compare angiographic andclinical outcomes of a simple strategy of stenting main vessel only with balloon dilatation of the side branch with a complex strategy ofstenting both branches.Methods: We performed a meta-analysis of six studies, randomized (three) or prospective observational (three), including 963 patients, thatdirectly compared the simple strategy to the complex strategy, in the treatment of CBL with DES.Results: Final minimal lumen diameter (MLD) of the side branch was significantly smaller in the simple strategy group [WMD −0.50 mm,95% CI (−0.76, −0.24), pb0.00001]. The risk of main vessel restenosis [RR 0.66, 95% CI (0.38–1.17), p=0.16], side branch restenosis [RR0.62, 95% CI (0.24–1.56), p=0.31], follow up death [RR 0.60, 95% CI (0.19–1.86), p=0.38], follow up myocardial infarction [RR 0.71,95% CI (0.46–1.10), p=0.13], or target vessel revascularization [RR 0.90, 95% CI (0.56–1.46), p=0.67] was similar between the twostrategies. The simple strategy showed a trend to a lower risk of early myocardial infarction [RR 0.65, 95% CI (0.41–1.05), p=0.08].Conclusion: In the treatment of unselected CBL with DES, the complex strategy does not penalize angiographic and clinical outcomescompared to the simple strategy. Further randomized studies are needed to assess the benefit of simple or complex strategy in the treatment ofspecific subsets of bifurcated lesions.© 2008 Elsevier Ireland Ltd. All rights reserved.
Keywords: Coronary bifurcation lesions; Drug eluting stent; Meta-analysis
1. Introduction
Coronary bifurcation lesions (CBL), accounting for 15–18%of coronary angioplasty procedures [1], remain a challengefor the interventional cardiologist. Balloon angioplasty for thetreatment of CBLwas associated with poor immediate and longterm results [2]. Bare metal stents (BMS) have solved somelimitations of balloon angioplasty, yet plaque shifting towards
⁎ Corresponding author. Tel.: +39 06 30154187; fax: +39 06 3055535.E-mail address: [email protected] (G. Niccoli).
1 The authors contributed equally to the paper.
0167-5273/$ - see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijcard.2008.10.016
the side branch after main vessel stenting has been increasinglyrecognized as a significant complication of the procedurerequiring the use of one or more additional stents in the sidebranch [3]. Different techniques based on the use of multipleBMS have been described [4]. Non-randomized studies withBMS, however, have suggested improved long term resultswith a strategy of stenting the main vessel only with balloondilatation of the side branch (simple strategy) compared tomorecomplex approaches with stenting of both branches (complexstrategy) [5–9]. The introduction of drug eluting stents (DES)has been advocated as the final solution in the treatment ofCBL,due to their excellent results in both simple and complex lesionsubsets [10,11].
81G. Niccoli et al. / International Journal of Cardiology 139 (2010) 80–91
We performed a meta-analysis of studies that compared asimple strategy with a complex strategy using DES, in orderto assess angiographic and clinical outcomes.
2. Methods
2.1. Search strategy, study selection and data extraction
Two investigators (G.F., G.N.) independently searchedPubmed, EMBASE and CINAHIL for all reports of studies,published from January 2001 to July 2007, comparing asimple strategy to a complex strategy in the treatment ofCBL, by entering the keywords “coronary (bifurcation ORbifurcational) AND stent”. Studies were eligible for inclu-sion in the review if they directly compared, head to head,the simple strategy to the complex strategy and if implanta-tion of DES was performed. Both randomized trials andprospective observational studies were included. Bifurcationlesion was defined as diameter stenosis ≥50% of the mainvessel involving a side branch with a minimal lumendiameter (MLD) ≥2.00 mm. We included studies withavailable clinical follow-up, independently of the presenceof angiographic follow-up. Studies published as abstractwere excluded and all the studies in any language wereeligible for inclusion. Flow diagram showing the process ofstudy selection is shown in Fig. 1.
Two non-blinded reviewers (G.F., G.N.) independentlyextracted the data regarding the endpoints. Disagreementwas resolved by consensus. Data were managed by availablecase analysis and actual treatment.
2.2. End points
Angiographic end-points were: 1) final minimal lumendiameter (MLD) after percutaneous coronary intervention (PCI)
Fig. 1. Flow diagram showing the process of study selection.
of both the main vessel and the side branch; 2) angiographicrestenosis of both the main vessel and the side branch, definedas ≥50% diameter stenosis of the treated lesion.
Clinical end-points were: 1) early (in hospital or 30 day)myocardial infarction (MI); 2) late death or late MI(according to the clinical follow up of each study); 3) targetvessel revascularization (TVR); 4) early stent thrombosisoccurring within 30 days from the index procedure; 5) latestent thrombosis occurring after 30 days from the indexprocedure. MI was defined as elevation of cardiac enzymes≥3 times the upper normal limit, either asymptomatic orwith recurrent ischaemic chest pain associated with newelectrocardiographic changes. The cardiac enzymes,assessed for this purpose, varied among the studies, beingtotal creatine kinase, creatine kinase-MB (mass) or troponinT or I. TVR was defined as repeat PCI or coronary arterybypass graft surgery. Stent thrombosis was defined as anacute coronary syndrome with angiographic documentationof either vessel occlusion or thrombus within or adjacent to apreviously successful implanted stent or, in the absence ofangiographic confirmation, as acute MI in the distribution ofthe treated vessel or death not clearly attributable to othercauses. Numbers of events were obtained from tables andtext in each study.
2.3. Data analysis
Data were expressed as relative risk (RR) and 95%confidence interval (95% CI) for dichotomous variables, andweighted mean difference (WMD) with 95% CI forcontinuous variables. The presence of the heterogeneitybetween studies was evaluated with Cochran Q chi2 test. I2
test was used to evaluate inconsistency. I2 describes thepercentage of total variation across studies that is due toheterogeneity: values of 25%, 50% and 75% correspond tolow, moderate, high I2 [12]. Binary outcomes were combinedwith Mantel Haenszel method according to a fixed effectmodel or with DerSimonian and Laird method according to arandom effect model when heterogeneity between studieswas found [13]. Continuous variables were combined withDerSimonian and Laird method.
A pre-specified subgroup analysis, according to the studydesign (randomized vs observational) was performed foreach endpoint (except for early and late stent thrombosis asdata were available in only four studies for these outcomes).The homogeneity of RR between the two subgroups wasassessed using the interaction test described by Altman andBland [14].
Furthermore, with regard to the angiographic endpoint ofside branch restenosis, which showed significant hetero-geneity, we explored the potential sources of heterogeneityperforming a random metaregression analysis to assess theeffect of the following covariates on the outcome: studydesign (randomized or observational), the duration of followup, the prevalence of the crush technique use in the complexstrategy, the rate of final kissing balloon (as continuous
82 G. Niccoli et al. / International Journal of Cardiology 139 (2010) 80–91
variable) either in the simple or in the complex strategygroup.
A sensitivity analysis was performed, after excludingeach study in turn, before calculating the pooled effect size toassess the relative contribute of less statistically robuststudies included in the meta-analysis.
The presence of selection, performance, attrition, detec-tion and reporting bias was systematically assessed, asrecommended by the Cochrane Collaboration [15]. Publica-tion bias was explored by visual inspection of a funnel plot ofprecision (standard error of logRR) against the treatmenteffect (RR on a logarithmic scale) and using the asymmetrylinear regression of Egger's test [16] and the kendall taucoefficient of correlation of Begg's test [17]. Analyses wereperformed using the Revman 4.2.8 freeware packageprogram (The Cochrane Collaboration, Oxford, England),the statistical software package Stata 9.0 (Stata Corporation,Texas). Statistical level of significance for the summarytreatment effect estimate was a two tailed p valueb0.05.Heterogeneity, publication bias and the test of homogeneitybetween subgroups were considered statistically significantwith a two tailed p value≤0.1.
3. Results
3.1. Study characteristics
Among nine selected studies [18–26], one study [26] wasexcluded due incomplete data regarding the cohort of patientswith true bifurcation lesions, two studies [22,24] were droppedout because the bifurcation lesion was the left main only.Eventually, six studies comparing a simple strategy vs acomplex one were identified and included [18–21,23,25].Main characteristics of the studies are listed in Table 1. Threewere randomized controlled trials (RCT) [18,19,23], threewere prospective case-control studies [20,21,25]. Sirolimuseluting stent was the study stent in five studies [18–21,23],
Table 1Description of the included studies.
Study Studytype
Complex stentingtechnique (%)
Patientnumber
Meanclinical FU(months)
Colombo et al.[18]
RCT MT (63.5)–T (32)–Y (3)–V (1.5) 85 6.4
Nordic et al.[23]
RCT Crush (50)–culotte (21)–other(29)
413 6
Pan et al.[19]
RCT NA 91 11
Assali et al. [21] PO MT (36)–PT (36)–crush (28) 53 12Di Mario
et al. [25]PO Crush (62)–T (19.5)–
V (14.5)–culotte (4)147 12
Ge et al. [20] PO Crush (67)–T, MT (24)–V(6)–culotte (3)
174 9.2
Study column refers to first author (except for the Nordic trial) and year of publicatioMT: modified T stenting; T: T stenting; Y: Y stenting; V: V stenting; PT: provisionaexpressed as means; simple: simple strategy; complex: complex strategy; NA: not
paclitaxel eluting stent was used in the remaining study [25].However, in the Nordic study [23] a few Taxus Express stentswere used in both strategies groups and 1 and 2 bare metalstents were implanted in the simple and complex strategysubgroups, respectively. In two studies [19,21] few left mainbifurcationswere treated (6% and 3.6% in simple and complexstrategy, respectively in one study [19] and 3.6% and 4% in theother study [21]). In the Nordic study [23], the prevalence ofleft main bifurcation was not available, in the remainingstudies no left main bifurcation was treated (however, in thestudy by Colombo et al. [18], although unprotected left mainwas an exclusion criteria, no information is provided withregard to protected leftmain). Themean clinical follow-upwas9.4±2.7months, ranging from 6 to 19.5months. A total of 963patients were included (402 undergoing stenting of the mainvessel only and 561 receiving stenting of both branches). Allprocedures were performed through the radial or femoralapproach using 6–8 French guiding catheters. In each study,patients were on aspirin and clopidogrel. Intravenousunfractionated heparin was administered in the catheterizationlaboratory. The use of platelet IIbIIIa antagonist was similar inpatients treated by the simple strategy compared to patientsreceiving the complex strategy [RR 0.95, 95%CI (0.83–1.08),p=0.42, chi2=6.82, p=0.23, I2=26.7%]. The prevalence offinal kissing balloon was significantly lower in the simplestrategy group compared to the complex one [RR 0.73, 95%CI(0.53–1.00), p=0.05, chi2=44.52, pb0.00001, I2=88.8%].Different techniques for double stent implantation were usedwithin and across studies (Table 1).
3.2. Angiographic end points
MLD of main vessel and side branch was available in allthe included studies. Final MLD of the main vessel wassimilar in patients treated with the simple strategy comparedto those undergoing the complex strategy [WMD −0.05 mm,95% CI (−0.15, 0.04), p=0.30, chi2 =11.56, p=0.04,
Angiographicfollow-up
Diabetes(%)
IIbIIIa blockers(%)
Kissing balloon(%)
Simple Complex Simple Complex Simple Complex
Yes 26 21 36 43 82 90
Yes 13 12 51 51 32 74
Yes 42 39 62 57 60 77
No 25 32 79 92 57 80Yes 18 24 29 20 75 74
Yes 28 15 35 53 43 62
n; RCT = randomized controlled trial; PO = prospective observational study;l T stenting; SKS: simultaneous kissing stenting; follow-up (FU) months areavailable.
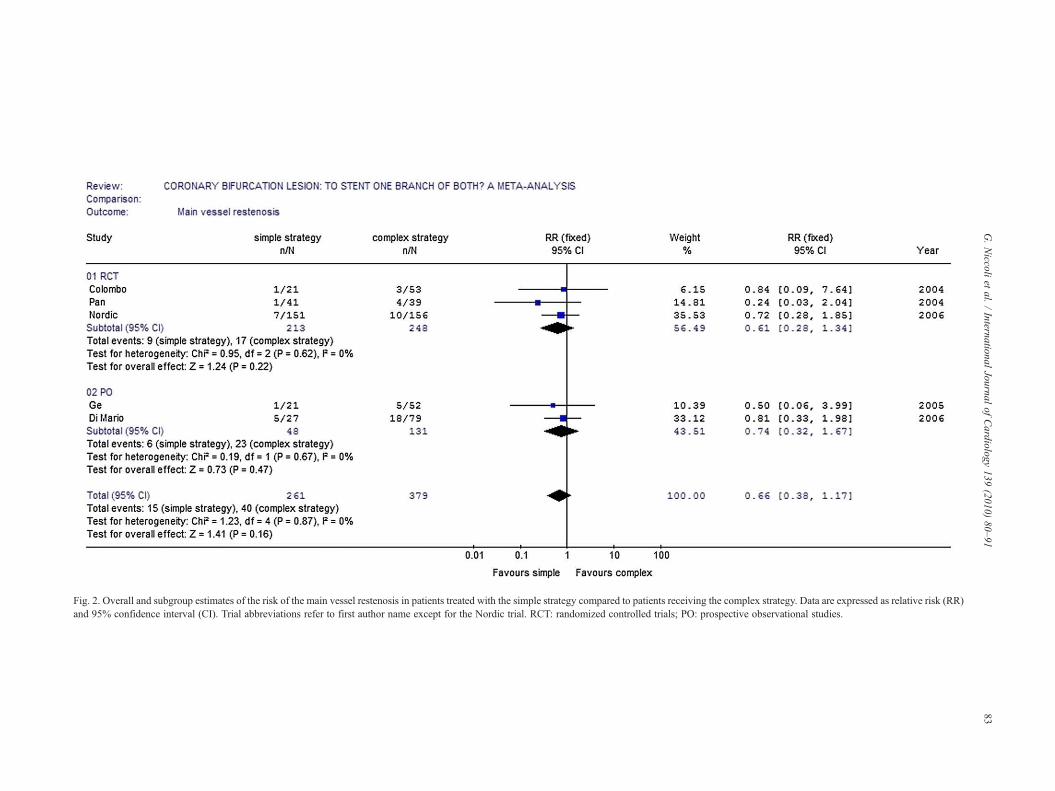
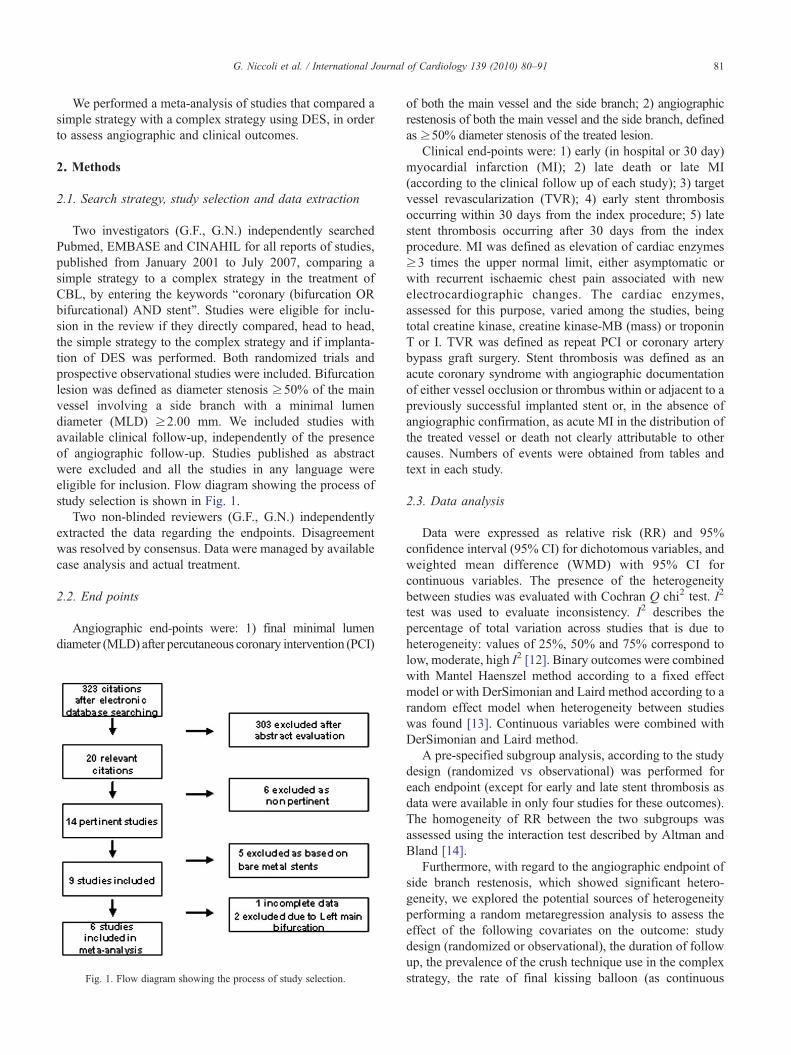
Fig. 2. Overall and subgroup estimates of the risk of the main vessel restenosis in patients treated with the simple strategy compared to patients receiving the complex strategy. Data are expressed as relative risk (RR)and 95% confidence interval (CI). Trial abbreviations refer to first author name except for the Nordic trial. RCT: randomized controlled trials; PO: prospective observational studies.
83G.Niccoli
etal.
/International
Journalof
Cardiology
139(2010)
80–91

84 G. Niccoli et al. / International Journal of Cardiology 139 (2010) 80–91
I2 =57.0%], while final MLD of the side branch wassignificantly smaller in patients treated with the simplestrategy [WMD −0.50 mm, 95% CI (−0.76, −0.24),pb0.00001, chi2 =62.19, pb0.00001, I2 =92.0%]. No pub-lication bias was found for final MLD of both branches(t=1.87, p=0.12, Egger's test; z=0, p=1, Begg's test formain branch, t=0.2, p=0.85 Egger's test; z=0, p=1, Begg'stest for side branch).
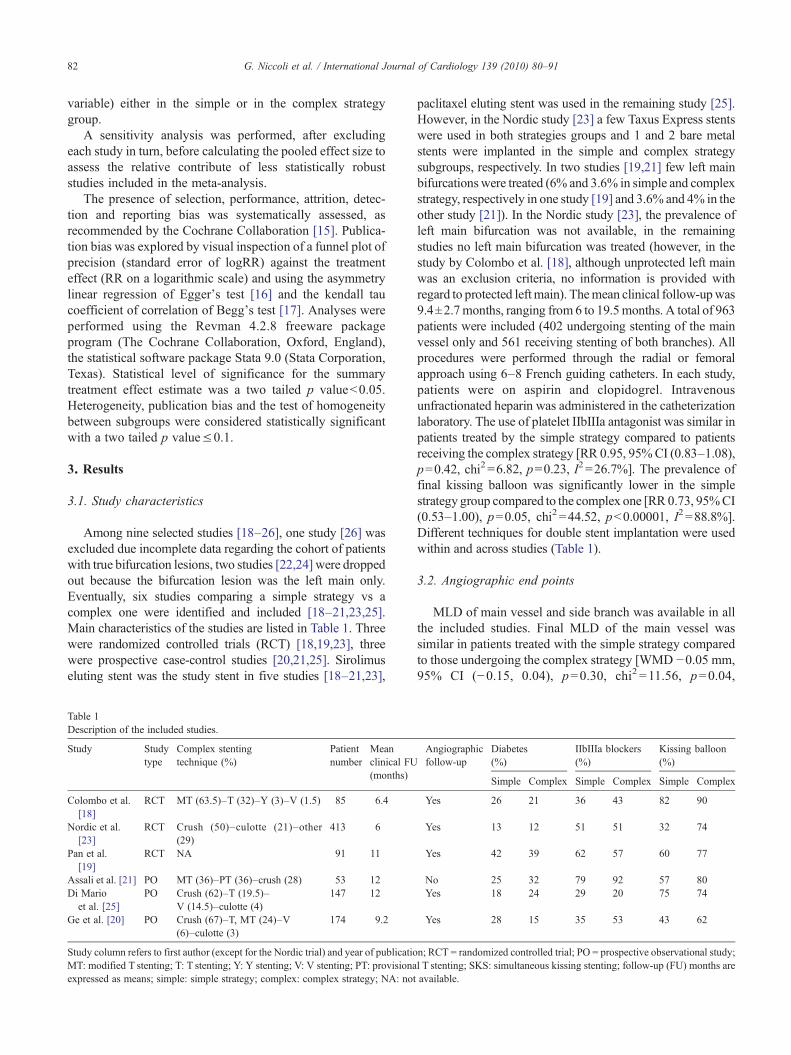
The rate of main vessel and side branch restenosis hasbeen reported in all but one study [20]. At a mean follow upof 7.08±1.35 months, the risk of main vessel restenosis andof side branch restenosis was similar in the simple strategygroup compared to the complex strategy group [RR 0.66,95% CI (0.38–1.17), p=0.16 (Fig. 2) and RR 0.62, 95% CI(0.24–1.56), p=0.31 (Fig. 3), respectively]. Heterogeneityand publication bias were not found for restenosis of themain vessel (chi2 1.23, p=0.87, I2 =0%; and t=−1.49,p=0.23, Egger's test; z=0.73, p=0.46, Begg's test,respectively), while significant heterogeneity (chi2 13.82,p=0.008, I2 =71.1%) and significant publication bias,(t=4.01 p=0.03, Egger's test; t=0.24, p=0.81, Begg'stest) were detected for side branch restenosis.
3.3. Clinical end points
Follow up death, early and follow up MI were assessed inall the included studies. The risk of follow up death [RR 0.60,95% CI (0.19–1.86), p=0.38; chi2 0.27, p=0.99, I2 =0%]was similar in patients treated with the simple strategycompared to those receiving the complex strategy. The risk ofearly MI [RR 0.65, 95% CI (0.41–1.05), p=0.08, chi2 2.76,p=0.6, I2 =0%] tended to be lower in patients treated withmain vessel stenting only compared to patients receivingstenting of both branches (Fig. 4). The risk of follow up MIwas not significantly different [RR 0.71, 95%CI (0.46–1.10),p=0.13; chi2 2.17, p=0.83, I2 =0%, (Fig. 5), and the risk ofTVR was similar [RR 0.90, CI (0.56–1.46), p=0.67, chi2
1.47, p=0.92, I2 =0% (Fig. 6)] in the simple strategy groupcompared to the complex strategy group.
With regard to early stent thrombosis, we excluded thestudy by Pan et al. [19], because of the absence of anydefinition, although a single stent thrombosis event wasreported on day 15 postprocedure in the complex strategygroup, and the Nordic study [23] because the timing of thesingle stent thrombosis, that occurred in the simple strategygroup, was not specified. Thus considering the remaining 4studies, the risk of early stent thrombosis, was notsignificantly different between the simple and the complexstrategy groups [RR 0.39, 95% CI (0.07–2.15), p=0.28,chi2 0.09, p=0.95, I2 =0%] (event rate 0% (0/142) and2.5% (8/317), respectively). Late stent thrombosis wasassessed in the same 4 studies. The risk of this adverse eventwas not significantly different between simple and complexstrategies [RR 0.93, 95% CI (0.10–8.73), p=0.94, chi2 0,p=0.99, I2 =0%] (event rate 0% (0/122) and 0.69% (2/290),respectively).
No heterogeneity was detected for each of the clinicalendpoints. Publication bias was not found for follow-upmortality (t=−0.29 p=0.79 Egger's test; z=0.24 p=0.81,Begg's test), and early stent thrombosis (t=1.94 p=0.30Egger's test; z=0.00 p=1.00 Begg's test), while it wasdetected for early MI (t=−3.34, p=0.04, Egger's test;z=0.24 p=0.81, Begg's test), follow up MI (t=4.41,p=0.01, Egger's test; z=1.50 p=0.13, Begg's test), TVR(t=−1.32 p=0.26, Egger's test; z=1.88 p=0.06, Begg'stest) and late stent thrombosis (t=1.65 p=0.24, Egger's test;z=1.70 p=0.09, Begg's test).
4. Subgroup analysis
4.1. Angiographic end points
Final MLD of the main vessel was similar in the simplestrategy compared to the complex one both in the subgroup ofRCT [WMD −0.04 mm, 95% CI (−0.22, 0.13), p=0.65] andin the subgroup of prospective observational studies [WMD−0.06 mm, 95% CI (−0.16, 0.04), p=0.24] (p for interac-tion=0.84). Final MLD of the side branch was significantlysmaller in the simple strategy group compared to the complexone, in both subgroups [WMD −0.40 mm, 95% CI (−0.63,−0.16), p=0.0009, in RCT subgroup and WMD −0.60 mm,95% CI (−1.16, −0.05), p=0.03, in prospective observa-tional subgroup; p for interaction=0.51].
The risk of main vessel restenosis was similar in thesimple strategy compared to the complex one both in RCTsubgroup [RR 0.61, 95% CI (0.28–1.34), p=0.22], and inprospective observational subgroup [RR 0.74, 95% CI(0.32–1.67), p=0.47 (p for interaction=0.74) (Fig. 2). Therisk of side branch restenosis was similar in the simplestrategy compared to the complex one in the RCT subgroup[RR 0.87, 95% CI (0.30–2.48), p=0.79], while it was lowerin the simple strategy group in the prospective observationalsubgroup [RR 0.33, CI (0.13–0.88), p=0.03], although thisdifference was not statistically significant (p for interac-tion=0.19) (Fig. 3).
4.2. Clinical end points
In RCT subgroup, the risk of early MI was significantlylower in the subgroup of patients treated by the simplestrategy compared to those treated by the complex one [RR0.55, 95% CI (0.31–0.98), p=0.04], while in prospectiveobservational subgroup, it was similar between the twostrategies [RR 0.94, 95% CI (0.40–2.19), p=0.89] (althoughthis difference was not statistically significant, p forinteraction=0.30) (Fig. 4). The risk of follow up MI wassimilar in the simple strategy group compared to the complexstrategy group in both RCT subgroup [RR 0.64, 95% CI(0.37–1.09), p=0.10], and prospective observational sub-group [RR 0.88, 95% CI (0.41–1.90), p=0.74] (p forinteraction=0.50) (Fig. 5). The risk of TVR was similarbetween the two strategies both in RCT subgroup [RR 0.93,
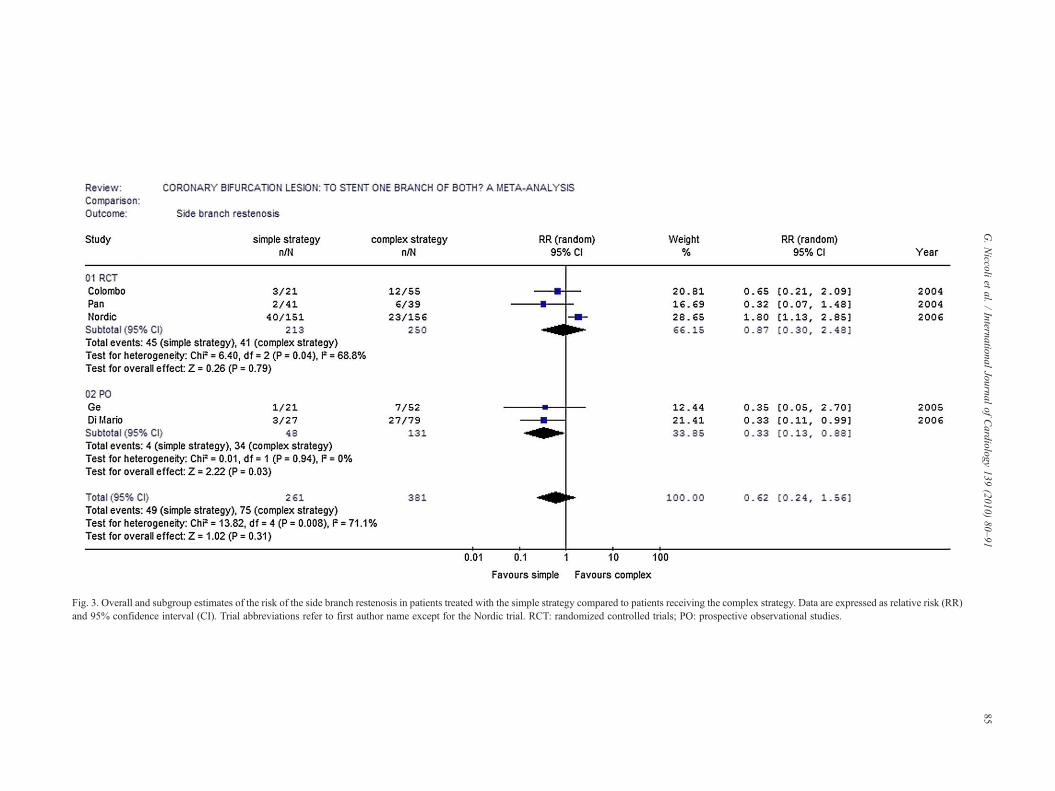
Fig. 3. Overall and subgroup estimates of the risk of the side branch restenosis in patients treated with the simple strategy compared to patients receiving the complex strategy. Data are expressed as relative risk (RR)and 95% confidence interval (CI). Trial abbreviations refer to first author name except for the Nordic trial. RCT: randomized controlled trials; PO: prospective observational studies.
85G.Niccoli
etal.
/International
Journalof
Cardiology
139(2010)
80–91
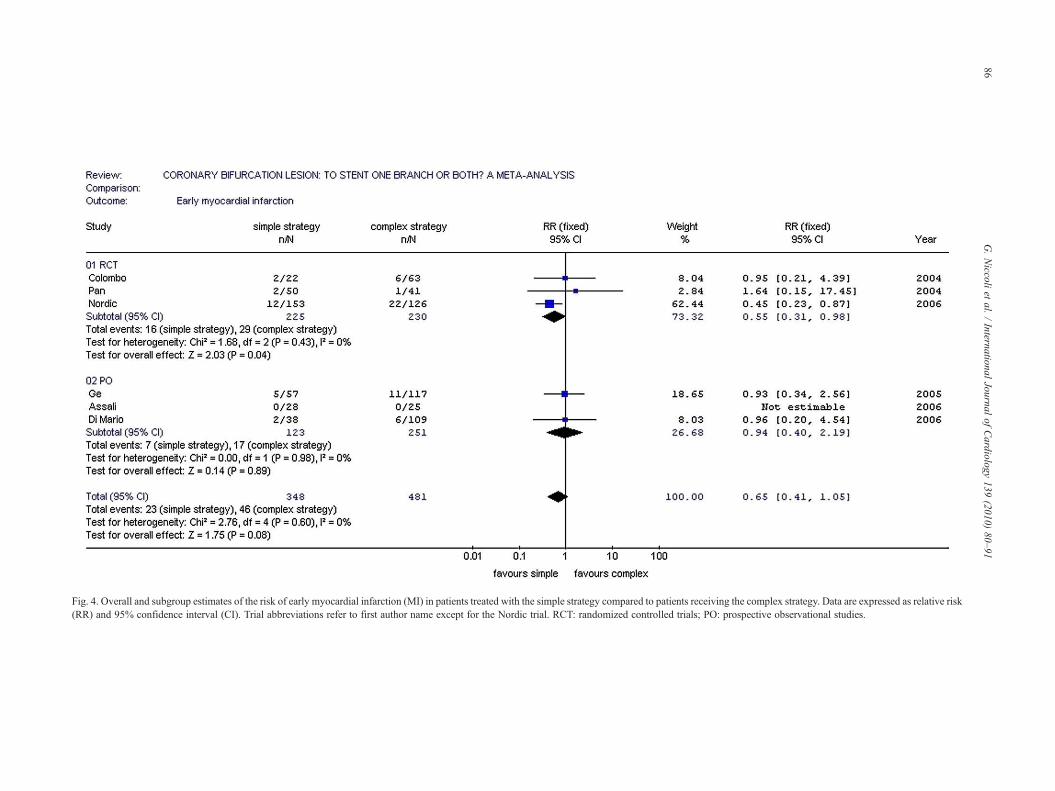
Fig. 4. Overall and subgroup estimates of the risk of early myocardial infarction (MI) in patients treated with the simple strategy compared to patients receiving the complex strategy. Data are expressed as relative risk(RR) and 95% confidence interval (CI). Trial abbreviations refer to first author name except for the Nordic trial. RCT: randomized controlled trials; PO: prospective observational studies.
86G.Niccoli
etal.
/International
Journalof
Cardiology
139(2010)
80–91
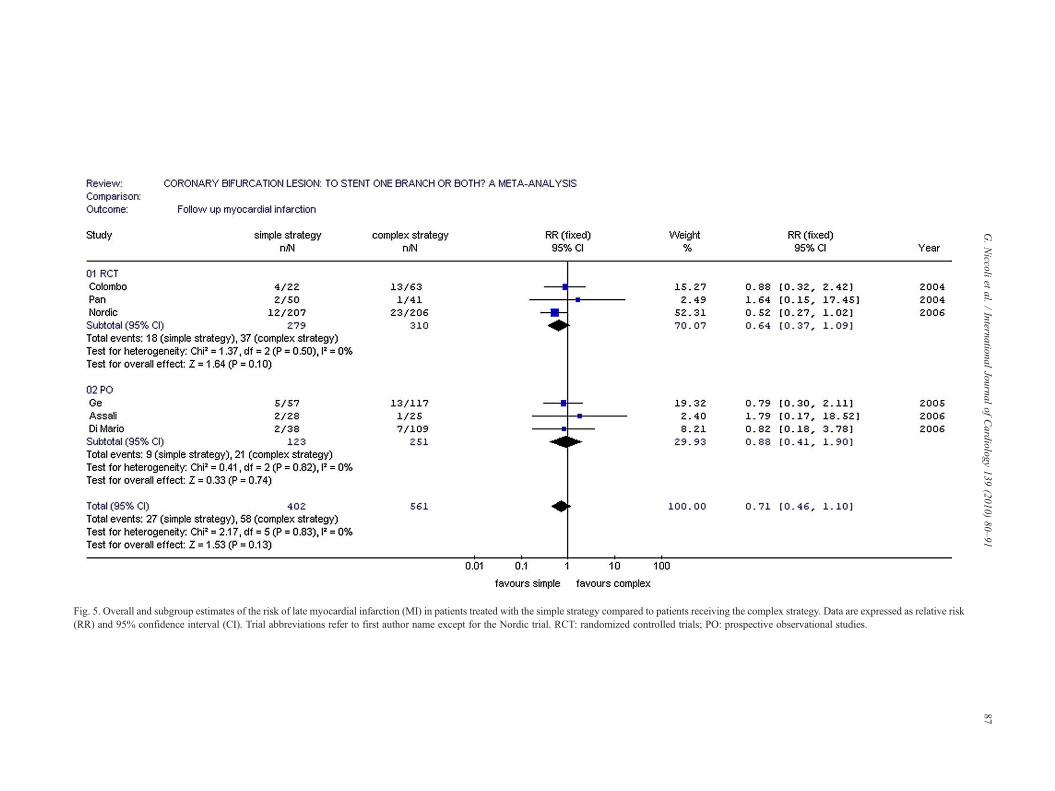
Fig. 5. Overall and subgroup estimates of the risk of late myocardial infarction (MI) in patients treated with the simple strategy compared to patients receiving the complex strategy. Data are expressed as relative risk(RR) and 95% confidence interval (CI). Trial abbreviations refer to first author name except for the Nordic trial. RCT: randomized controlled trials; PO: prospective observational studies.
87G.Niccoli
etal.
/International
Journalof
Cardiology
139(2010)
80–91
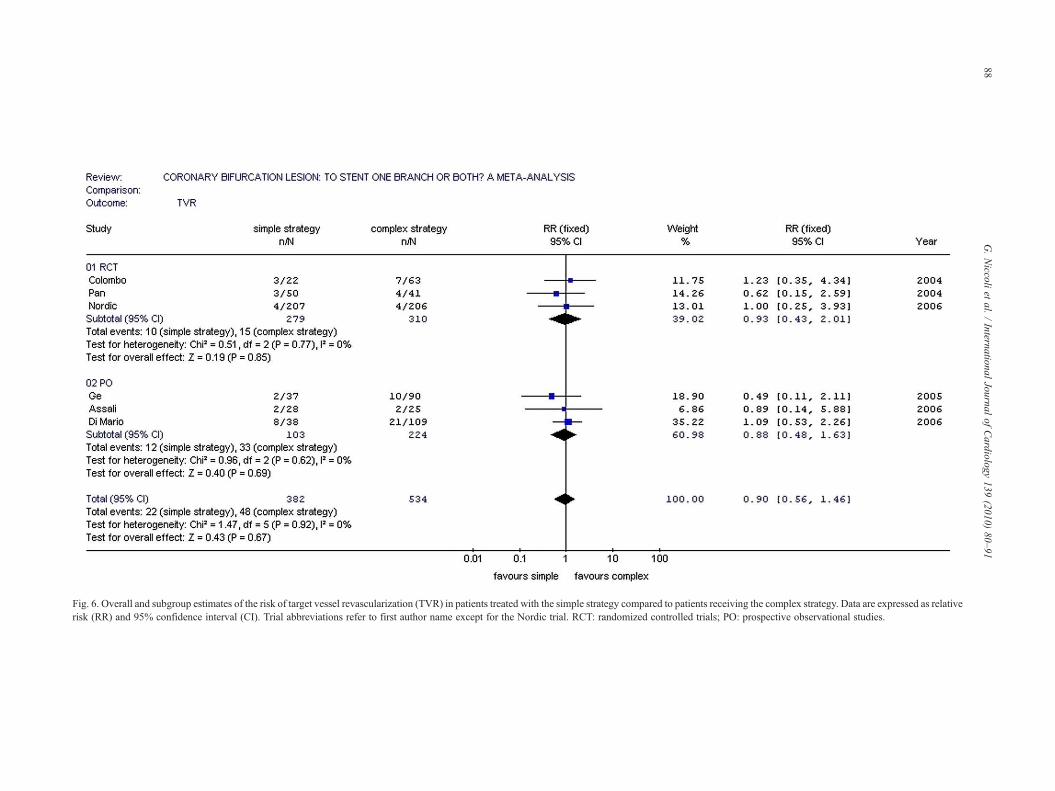
Fig. 6. Overall and subgroup estimates of the risk of target vessel revascularization (TVR) in patients treated with the simple strategy compared to patients receiving the complex strategy. Data are expressed as relativerisk (RR) and 95% confidence interval (CI). Trial abbreviations refer to first author name except for the Nordic trial. RCT: randomized controlled trials; PO: prospective observational studies.
88G.Niccoli
etal.
/International
Journalof
Cardiology
139(2010)
80–91

89G. Niccoli et al. / International Journal of Cardiology 139 (2010) 80–91
95% CI (0.43–2.01), p=0.85] and in prospective observa-tional subgroup [RR 0.88, 95%CI (0.48–1.63), p=0.69] (p forinteraction=0.82) (Fig. 6).
5. Metaregression analysis
We investigated the sources of heterogeneity of the sidebranch restenosis exploring the effect of the followingcovariates on the risk of restenosis (expressed as logarithmRR=y), by random metaregression analysis. The presence ofrandomization of the study (y=1.03⁎ x−1.09; z=1.29,p=0.19), the duration of follow up (y=0.36⁎ x−2.93;z=1.03, p=0.30), the prevalence of crush technique use(y=−0.005⁎x−0.14; z=0.24, p=0.81), the rate of finalkissing balloon in the complex group (y=0.01⁎x−1.25;z=0.18, p=0.86) did not influence the risk of side branchrestenosis. Instead, an increasing rate of final kissing balloonin the simple strategy group reduced the risk of side branchrestenosis (y=−0.03⁎x+1.48; z=−3.1, p=0.002).
6. Sensitivity analysis
The overall summary estimate for any endpoint con-sidered, after excluding each study in turn, showed nosignificant difference compared to the results of mainanalysis (data not shown).
7. Discussion
The main findings of this meta-analysis are that thecomplex strategy is associated to a larger final MLD of theside branch, does not increase the risk of follow upangiographic restenosis, death and MI, and is associated tosimilar risk of TVR compared to the simple strategy, in thetreatment of CBL, in the DES era. Thus, these results show anon penalizing effect of the complex strategy in the treatmentof CBL. Moreover they need to be interpreted consideringthat the most common techniques adopted in the complexstrategy were crush and T stenting, with culotte techniqueperformed in the minority of the patients. The heterogeneityof the techniques and the lack of information on theindividual outcomes, might have diluted the potentialadvantages associated with universal use of a uniquetechnique in the complex strategy and do not allow toidentify the best complex technique for bifurcation stenting.
The introduction of DES consistently lowered the rate ofrepeat revascularization both in simple and complex lesionsubsets [10,11], however bifurcation lesions still remain asubset of lesions with increased in-stent restenosis. Incom-plete ostial coverage of the side branch has been described asa possible cause of restenosis. In fact, DES can exert anoptimal effect on the vessel wall, only if the drug is releasedfor the entire lesion length, allowing complete ostialcoverage [27]. New techniques which effectively allowcomplete ostial coverage, such as the simultaneous kissingstent (SKS) technique [28] and the “crush technique”
[29,30], have been recently associated with good angio-graphic and clinical results in registries. However, a higherprevalence of the crush technique in the complex strategy,did not affect the risk of side branch restenosis, inmetaregression analysis. Excessive metal concentration atthe carina may affect the outcome of crush technique;indeed, mini-crush techniques have been recently associatedwith low side branch restenosis rate [31,32]. The emergingproblem of stent fracture might be involved in DESrestenosis as recently suggested by Lee et al. [33]. Moreover,Aoki et al. [34] reported that stent fractures are often in thelocations that served as hinges during vessel movement inthe cardiac contraction cycle, such as the side branch origin.Other factors associated with in-stent restenosis are thebifurcation angle when using a complex strategy and plaquecomposition at the ostium of the side branch. Indeedincreased cardiac adverse events were observed in patientswith bifurcation angulation ≥50% treated by crushing [35].Pathological studies suggest that coronary ostia are rich inelastic and fibrous tissue [36], thus, higher pressure post-dilatation of DES, which has been recently associated with abetter outcome [37], may be crucial after ostial branchstenting. In our meta-analysis we could not address the roleof bifurcation angle or high pressure post-dilatation, due tothe lack of complete information regarding this issue in theincluded studies.
Metaregression analysis suggested that higher finalkissing balloon rates were associated with reduced risk ofside branch restenosis in the simple strategy group, whereasthey did not influence the risk of side branch restenosis in thecomplex strategy group. This discrepancy may depend onthe relatively overall high rate of the kissing balloon in thecomplex strategy, with small inter-study variability, rangingfrom 62% to 90%, that might not allow further improvementof the restenosis rate. Instead, lower rate of utilization andlarger inter-study variability, from 32 to 82%, were found inthe simple strategy group, compared to the complex one.Interestingly, this inter-study variability was the main sourceof the heterogeneity for the side branch restenosis, atmetaregression analysis. This finding may provide a partialexplanation for the observed reduced risk of side branchrestenosis associated to the complex strategy in the Nordictrial, in contrast to the overall results of this meta-analysis.Of note, in the Nordic trial final kissing balloon wasachieved in 32% only of the patients in the simple strategygroup compared to 74% in the complex group, suggestingthat the lack of a proper use of final kissing balloon in thesimple strategy might be associated to a higher side branchrestenosis rate.
The second finding of our meta-analysis is that the simplestrategy tended to reduce the risk of early MI compared to thecomplex strategy. Multiple mechanisms can be involved.Firstly, longer stent length is known to cause biggerdisplacement of plaque as demonstrated in a volumetricIVUS study [38]. Secondly, overlapping stenting, that hasbeen reported to be associated with higher rate of post-

90 G. Niccoli et al. / International Journal of Cardiology 139 (2010) 80–91
procedural MI in long lesions [39], may play a role also inbifurcation lesions. Previous studies have shown that over-lapping heterogeneous DES, compared to overlapping homo-genous DES, is associated with similar late loss, neointimalhyperplasia and restenosis rate [40], or even with lower lateloss in some cases [41], with no increase in the side effects ofDES [40,41]. Further studies are needed to assess the effect ofoverlapping DES in bifurcation lesions. Finally, although therisk of early stent thrombosis was not statistically differentbetween the two strategies in our meta-analysis, the rate ofearly stent thrombosis was 0% in the simple strategy groupcompared to 2.5% in the complex group, a value significantlyhigher than the 1–1.5% found in previous report [42]. Thus,due to the rare occurrence of stent thrombosis, we cannotdefinitely rule out that it could play a role in the association ofthe complex strategy with a higher early MI risk.
The pre-specified subgroup analysis, according to the studydesign, showed substantial homogeneity between randomizedand prospective observational studies for the relative risk of allthe endpoints, strengthening the results of the meta-analysis.Furthermore, the sensitivity analysis showed that, afterexcluding each study in turn, the initial results of the meta-analysis were confirmed for each endpoint.
8. Study limitations
Our study has several limitations. First, the presence ofrandomization in only three studies increased the risk ofselection and reporting bias. Moreover, the sample size of thestudies was small and in the study of Colombo et al. [18] ahigher cross over rate from the simple strategy to thecomplex one was present. However, subgroup and metare-gression analyses according to study design (randomized vsobservational) showed that this did not influence the resultsof the meta-analysis. Second, publication bias was alsoreported for the risk of side branch restenosis, early andfollow up myocardial infarction, TVR and late stentthrombosis, thus indicating caution before accepting theresults. Third, heterogeneity was found for side branchrestenosis, although we addressed and explained thepotential sources of heterogeneity using subgroup andmetaregression analyses. Fourth, as the follow up durationwas variable across the studies, the actual rates of late stentthrombosis, beyond 6 months, might not have been assessedaccurately. Finally, this is not an individual patient data meta-analysis, thus the effect of other potential confoundingfactors on the outcomes was not addressed.
9. Conclusions
In the treatment of unselected CBL with DES, availabledata show that the selection of a complex strategy isassociated with a larger final MLD of the side branch whilethe simple strategy is associated with a trend toward lowerrisk of early MI. Such differences however, do not translatein any detectable advantage in the clinical outcome at follow-
up. As a consequence, these results indicate a non penalizingeffect of the complex strategy in the treatment of CBL.Further studies should assess the role of complex/simplestrategy in the treatment of specific subgroups of CBL.
Acknowledgments
Giuseppe Ferrante received a research grant from the Eu-ropean Association of Percutaneous Cardiovascular Interven-tions (EAPCI). The authors of this manuscript have certifiedthat they comply with the Principles of Ethical Publishing inthe International Journal of Cardiology [43].
References
[1] Lefevre T, Louvard Y, Morice MC, et al. Stenting of bifurcationlesions: classification, treatments, and results. Catheter CardiovascInterv 2000;49:274–83.
[2] George BS, Myler RK, Stertzer SH, et al. Balloon angioplasty ofcoronary bifurcation lesions: the kissing balloon technique. CatheterCardiovasc Diagn 1986;12:124–38.
[3] Aliabadi D, Tilli FV, Bowers TR, et al. Incidence and angiographicpredictors of side branch occlusion following high-pressure intracor-onary stenting. Am J Cardiol 1997;80:994–7.
[4] Louvard Y, Lefevre T, Morice MC. Percutaneous coronary interventionfor bifurcation coronary disease. Heart 2004;90:713–22.
[5] Assali AR, Teplitsky I, Hasdai D, et al. Coronary bifurcation lesions: tostent one branch or both? J Invasive Cardiol 2004;16:447–50.
[6] Al Suwaidi J, Berger PB, Rihal CS, et al. Immediate and long-termoutcome of intracoronary stent implantation for true bifurcationlesions. J Am Coll Cardiol 2000;35:929–36.
[7] Anzuini A, Briguori C, Rosanio S, et al. Immediate and long-termclinical and angiographic results from Wiktor stent treatment for truebifurcation narrowings. Am J Cardiol 2001;88:1246–50.
[8] Pan M, Suarez de Lezo J, Medina A, et al. Simple and complex stentstrategies for bifurcated coronary arterial stenosis involving the sidebranch origin. Am J Cardiol 1999;83:1320–5.
[9] Yamashita T, Nishida T, Adamian MG, et al. Bifurcation lesions: twostents versus one stent — immediate and follow-up results. J Am CollCardiol 2000;35:1145–51.
[10] Sousa JE, Serruys PW, Costa MA. New frontiers in cardiology: drug-eluting stents: Part I. Circulation 2003;107:2274–9.
[11] Sousa JE, Serruys PW, Costa MA. New frontiers in cardiology: drug-eluting stents: Part II. Circulation 2003;107:2383–9.
[12] Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuringinconsistency in meta-analyses. BMJ 2003;327:557–60.
[13] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control ClinTrials 1986;7:177–88.
[14] Altman DG, Bland JM. Interaction revisited: the difference betweentwo estimates. BMJ 2003;326:219.
[15] http://www.cochrane.org/resources/handbook.[16] Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis
detected by a simple, graphical test. BMJ 1997;315:629–34.[17] Begg CB, Berlin JA. Publication bias: a problem in interpreting
medical data. J R Stat Soc 1988;151:445–63.[18] Colombo A, Moses JW, Morice MC, et al. Randomized study to
evaluate sirolimus-eluting stents implanted at coronary bifurcationlesions. Circulation 2004;109:1244–9.
[19] Pan M, de Lezo JS, Medina A, et al. Rapamycin-eluting stents for thetreatment of bifurcated coronary lesions: a randomized comparison of asimple versus complex strategy. Am Heart J 2004;148:857–64.
[20] Ge L, Tsagalou E, Iakovou I, et al. In-hospital and nine-month outcomeof treatment of coronary bifurcational lesions with sirolimus-elutingstent. Am J Cardiol 2005;95:757–60.
91G. Niccoli et al. / International Journal of Cardiology 139 (2010) 80–91
[21] Assali AR, Assa HV, Ben-Dor I, et al. Drug-eluting stents inbifurcation lesions: to stent one branch or both? Catheter CardiovascInterv 2006;68:891–6.
[22] Kim YH, Park SW, Hong MK, et al. Comparison of simple andcomplex stenting techniques in the treatment of unprotected left maincoronary artery bifurcation stenosis. Am J Cardiol 2006;97:1597–601.
[23] Steigen TK, Maeng M, Wiseth R, et al. Nordic PCI Study Group.Randomized study on simple versus complex stenting of coronaryartery bifurcation lesions: the Nordic bifurcation study. Circulation2006;114:1955–61.
[24] Valgimigli M, Malagutti P, Rodriguez Granillo GA, et al. Single-vesselversus bifurcation stenting for the treatment of distal left main coronaryartery disease in the drug-eluting stenting era. Clinical and angio-graphic insights into the Rapamycin-Eluting Stent Evaluated atRotterdam Cardiology Hospital (RESEARCH) and Taxus-StentEvaluated at Rotterdam Cardiology Hospital (T-SEARCH) registries.Am Heart J 2006;152:896–902.
[25] Di Mario C, Morici N, Godino C, et al. Predictors of restenosis aftertreatment of bifurcational lesions with paclitaxel eluting stents: amulticenter prospective registry of 150 consecutive patients. CatheterCardiovasc Interv 2007;69:416–24.
[26] Tsuchida K, Colombo A, Lefevre T, Oldroyd KG, Guetta V, GuagliumiG, et al. The clinical outcome of percutaneous treatment of bifurcationlesions in multivessel coronary artery disease with the sirolimus-eluting stent: insights from the Arterial Revascularization TherapiesStudy part II (ARTS II). Eur Heart J 2007;28:433–42.
[27] Lemos PA, Saia F, Ligthart JM, et al. Coronary restenosis aftersirolimus-eluting stent implantation: morphological description andmechanistic analysis from a consecutive series of cases. Circulation2003;108:257–60.
[28] Sharma SK. Simultaneous kissing drug-eluting stent technique forpercutaneous treatment of bifurcation lesions in large-size vessels.Catheter Cardiovasc Interv 2005;65:10–6.
[29] Ge L, Airoldi F, Iakovou I, et al. Clinical and angiographic outcomeafter implantation of drug-eluting stents in bifurcation lesions with thecrush stent technique: importance of final kissing balloon post-dilation.J Am Coll Cardiol 2005;46:613–20.
[30] Costa RA, Mintz GS, Carlier SG, et al. Bifurcation coronary lesionstreated with the qcrushq technique: an intravascular ultrasoundanalysis. J Am Coll Cardiol 2005;46:599–605.
[31] Jim MH, Ho HH, Chan AO, Chow WH. Stenting of coronarybifurcation lesions by using modified crush technique with doublekissing balloon inflation (sleeve technique): immediate procedureresult and short-term clinical outcomes. Catheter Cardiovasc Interv2007;69:969–75.
[32] Galassi AR, Colombo A, Buchbinder M, et al. Long-term outcomes ofbifurcation lesions after implantation of drug-eluting stents with the“mini-crush technique”. Catheter Cardiovasc Interv 2007;69:976–83.
[33] Lee MS, Jurewitz D, Aragon J, et al. Stent fracture associated withdrug-eluting stents: clinical characteristics and implications. CatheterCardiovasc Interv 2006;69:387–94.
[34] Aoki J, Nakazawa G, Tanabe K, et al. Incidence and clinical impact ofcoronary stent fracture after sirolimus-eluting stent implantation.Catheter Cardiovasc Interv 2006;69:380–6.
[35] Dzavik V, Kharbanda R, Ivanov J, et al. Predictors of long-termoutcome after crush stenting of coronary bifurcation lesions:importance of the bifurcation angle. Am Heart J 2006;152:762–9.
[36] Boucek RJ, Takeshita R, Brady AH. Microanatomy and intramuralphysical forces within the coronary arteries (man). Anat Rec1965;153:233–41.
[37] Brodie BR, Cooper C, Jones M, et al. Is adjunctive balloonpostdilatation necessary after coronary stent deployment? Final resultsfrom the POSTIT trial. Catheter Cardiovasc Interv 2003;59:184–92.
[38] Porto I, Selvanayagam JB, Van Gaal WJ, et al. Plaque volume andoccurrence and location of periprocedural myocardial necrosis afterpercutaneous coronary intervention: insights from delayed-enhancementmagnetic resonance imaging, thrombolysis in myocardial infarctionmyocardial perfusion grade analysis, and intravascular ultrasound.Circulation 2006;114:662–9.
[39] Chu WW, Kuchulakanti PK, Torguson R, et al. Impact of overlappingdrug-eluting stents in patients undergoing percutaneous coronaryintervention. Catheter Cardiovasc Interv 2006;67:595–9.
[40] Kang WC, Oh KJ, Han SH, Ahn TH, Chung WJ, Shin MS, et al.Angiographic and intravascular ultrasound study of the effects ofoverlapping sirolimus- and paclitaxel-eluting stents: comparison withsame drug-eluting overlapping stents. Int J Cardiol 2007;123:12–7.
[41] Burzotta F, Siviglia M, Altamura L, Trani C, Leone AM, Romagnoli E,et al. Outcome of overlapping heterogenous drug-eluting stents and ofoverlapping drug-eluting and bare metal stents. Am J Cardiol2007;99:364–8.
[42] Ong AT, Hoye A, Aoki J, van Mieghem CA, Rodriguez Granillo GA,Sonnenschein K, et al. Thirty-day incidence and six-month clinicaloutcome of thrombotic stent occlusion after bare-metal, sirolimus, orpaclitaxel stent implantation. J Am Coll Cardiol 2005;45:947–53.
[43] Coats AJ. Ethical authorship and publishing. Int J Cardiol2009;131:149–50.
Related Documents











