Cord Blood Transplantation: from the basics to what’s new 2013 Hematopoietic Stem Cell Transplant for Advanced Practice Providers Governor Hotel, Portland, Oregon September 20, 2013 Dr. Shernan Holtan, MD

Cord Blood Transplantation: from the basics to what’s new 2013 Hematopoietic Stem Cell Transplant for Advanced Practice Providers Governor Hotel, Portland,
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cord Blood Transplantation:
from the basics to what’s new2013 Hematopoietic Stem Cell Transplant for Advanced Practice
ProvidersGovernor Hotel, Portland, Oregon
September 20, 2013Dr. Shernan Holtan, MD

Milestones in the History of Cord Blood Transplantation
Early Milestones in the History of Cord Blood Transplantation (CBT)
• 1988: first CBT performed in 5-y/o boy with Fanconi Anemia • CB donor was patient’s HLA-identical sibling, identified by prenatal testing to be
unaffected by FA• Established proof of principle:
• Hematopoietic reconstitution can be achieved using umbilical cord blood hematopoietic stem cells
• 1990: first HLA-mismatched CBT performed in 30-month old boy with ALL in CR2
• 1992, 1993: initiation of cord blood banking programs• 1993: first unrelated donor CBT in 3-y/o boy with T-ALL
• 1996: Kurtzberg et al and Wagner et al reported first series of unrelated donor CBTs

Early Milestones in the History of Cord Blood Transplantation (CBT)
• 1995: first CBT performed in adult patient with leukemia• Experience reported in 1996, with 4 adults >21 years old
• 2005: first large series of double CBTs reported• Transplanted between 2000-2003, pioneered by the University of Minnesota
• Double CBT now the standard of care for many adult CBT programs
• More than 20,000 CBTs have been performed to date• Initial transplants limited to children, now adults• HLA-mismatched, unrelated setting, single vs double cord unit transplants• Worldwide inventory of CB units >500,000• NMDP estimates >95% patients can find at least 1 potential 4/6-matched CB
unit

www.marrow.org

Cord Blood as an Alternate Stem Cell Source – Pro’s and Con’s
• Extends donor pool • Lack of donor attrition• Shortened time to transplant• No safety risks for mother or child
with CB collection• HLA-mismatch well tolerated• Thought to be lower incidence of
(chronic) GVHD- May be more treatment-responsive?
• Delay in engraftment• Neutrophils• Platelets
• Risk of graft failure• Limited cell dose
• Total nucleated cell dose• CD34+ cell dose
• Viral reactivations and infections post transplant
• Delayed immune reconstitution• No DLI available
Benefits of CB Concerns with CB
Engraftment after CBT
• Early analyses described delay in engraftment in 562 patients undergoing CBT1
• Neutrophil recovery (>500) : median 28 days• Graft failure in 28%
• Platelet recovery ( >50,000): median 90 days• Tolerable degree of acute and chronic GVHD
• 23% grade III/IV acute and 25% chronic
• Identified factors important to CB engraftment:• Cell dose/kg body weight
• Total nucleated cell dose• CD34+ cell dose
• Degree of HLA-match
1. Rubinstein P et al. NEJM 1998.
Delayed Engraftment after CBT• ANC recovery delayed after single unit CBT:
• Pediatric patients1:• ANC >500: day 32 with CBT versus day 18 for BMT• Platelets >20,000: day 81 with CBT versus day 29 for BMT
• Adult patients2:• ANC >500: day 27 for CBT versus day 18-20 for BMT• Platelets >20,000: day 60 for CBT versus day 29 for BMT
1. Rocha V et al. Blood 2001.2. Laughlin MJ et al. NEJM 2004.
Historical Comparison of CB vs BMT
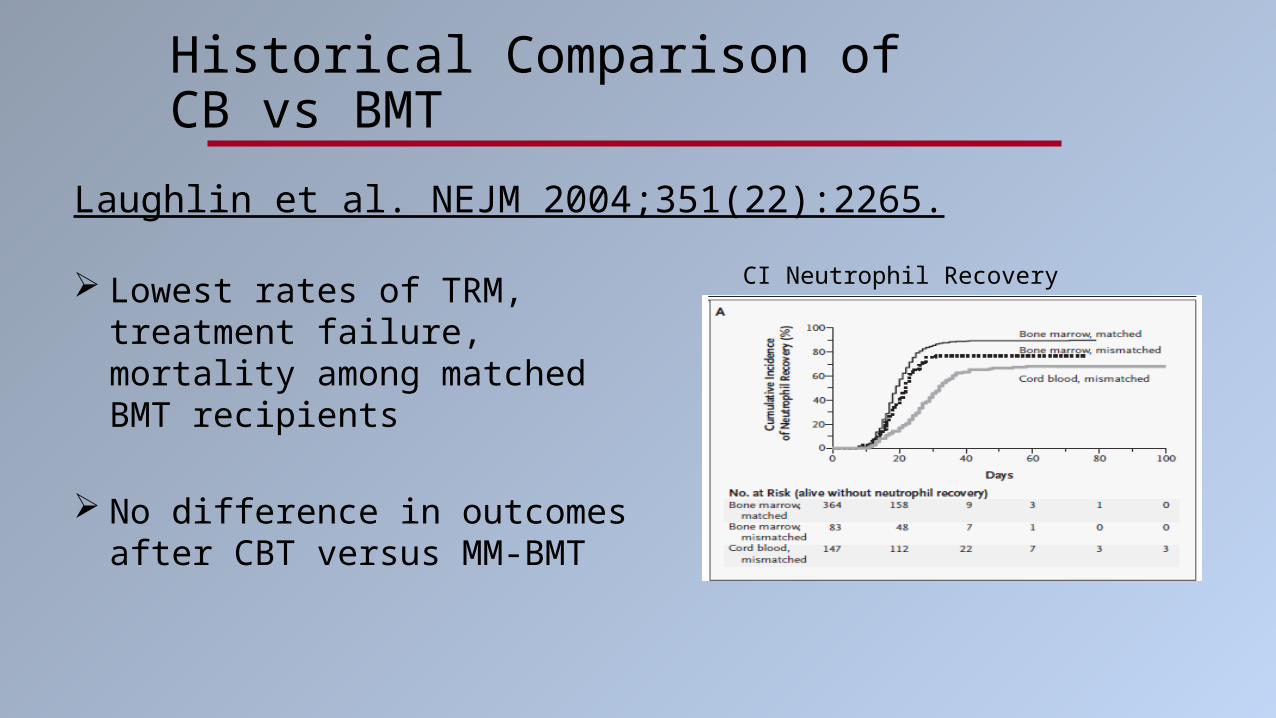
Laughlin et al. NEJM 2004;351(22):2265.
CI Neutrophil Recovery Lowest rates of TRM, treatment failure, mortality among matched BMT recipients
No difference in outcomes after CBT versus MM-BMT

Contributors to Delayed Engraftment
• HLA-match• Cell dose:
• 10-fold lower cell dose with CBT1
• BM or PBSC transplant: 2x10^6 CD34+ cells/kg• Cord blood transplant: 1.37x10^5 CD34+ cells/kg for single cord
• Conditioning regimen2,3
• GVHD prophylaxis2
• Inherent difference with CB HSC compared to other stem cell sources?• Impaired homing versus engraftment
1. Gluckman E et al. Exp Hematol 2004.2. Locatelli F et al. Blood 2003.3. Gluckman E et al. BBMT 2007.

How to Improve Delayed Engraftment after CBT?
How to Improve Delayed Engraftment after CBT?Development of Double Cord Blood Unit Transplantation

• 23 patients, median age 24 (13-53)• 2 CB units given:
• 10 (43%) patients received 4/6-matched units• 11 (48%) patients received at least one 5/6-match• 2 (9%) patients received at least one 6/6-match
• Infused cell doses:• Median cryopreserved TNC/kg = 4.8 x 10^7/kg• Median infused TNC/kg = 3.5 x 10^7/kg• Median infused CD34+/kg = 4.9 x 10^5/kg

• Ablative conditioning:• 120 mg/kg Cyclophosphamide• TBI 1320 cGy• ATG Fludarabine 75 mg/m2
• GVHD prophylaxis:• Cyclosporine• Methylprednisone MMF
• All 21 evaluable patients achieved sustained neutrophil engraftment
• Median of 23 days (range 15-41)• Complete donor chimerism
• 76% with single donor dominance by day 21• 100% by day 100
• No secondary graft failure
• Day 180 CI of platelet engraftment (>50,000) was 71%

Demonstrated feasibility and safety of double CB unit transplantation as a means to improve engraftment
Established standard ablative conditioning regimen with Cy/Flu/1320 TBI
• GVHD prophylaxis: CSA/MMF
This regimen continues to be standard of care ablative conditioning regimen for younger adult patients

Delayed Engraftment after CBT• ANC recovery delayed after single unit CBT:
• Pediatric patients1:• ANC >500: day 32 with CBT versus day 18 for BMT• Platelets >20,000: day 81 with CBT versus day 29 for BMT
• Adult patients2:• ANC >500: day 27 for CBT versus day 18-20 for BMT• Platelets >20,000: day 60 for CBT versus day 29 for BMT
1. Rocha V et al. Blood 2001.2. Laughlin MJ et al. NEJM 2004.3. Barker JN et al. Blood 2005.
• Double unit CBT3:• ANC >500: day 23• CI of platelet engraftment to >50,000 was 71% by day 180

How to Improve Delayed Engraftment after CBT?Other Ways to Improve Engraftment?
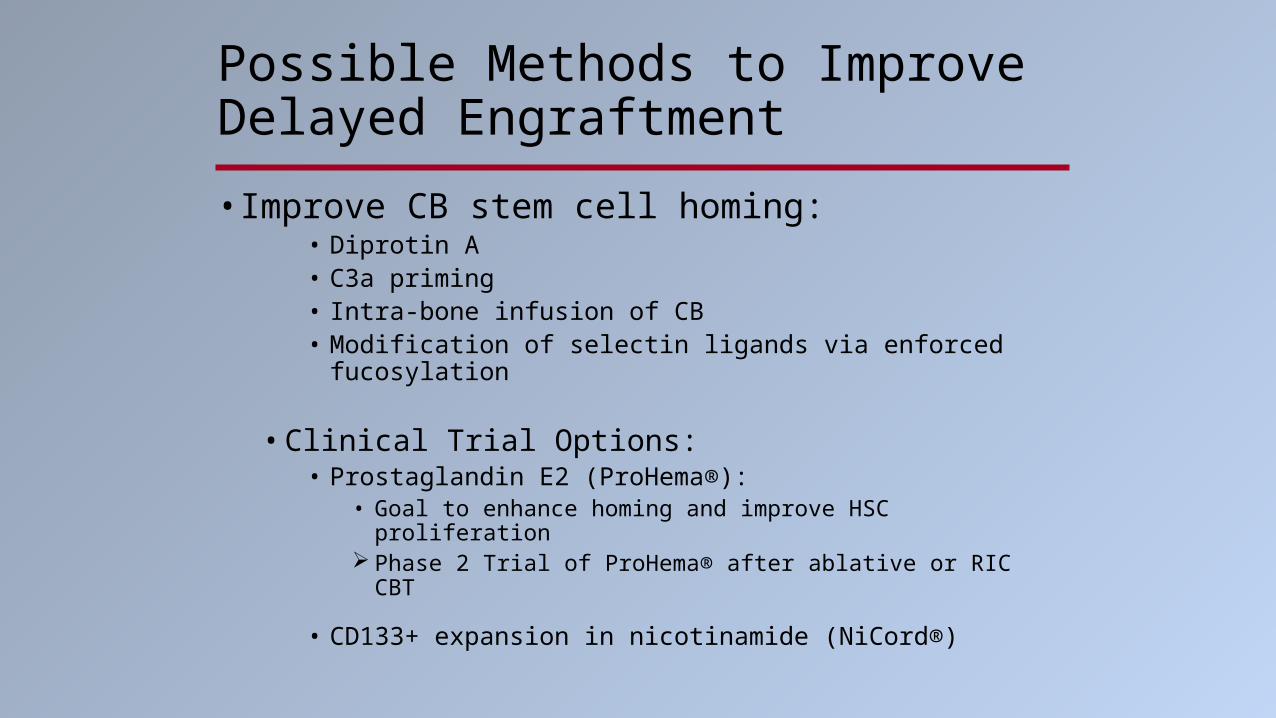
Possible Methods to Improve Delayed Engraftment
• Improve CB stem cell homing: • Diprotin A • C3a priming • Intra-bone infusion of CB • Modification of selectin ligands via enforced fucosylation
• Clinical Trial Options:• Prostaglandin E2 (ProHema®):
• Goal to enhance homing and improve HSC proliferation Phase 2 Trial of ProHema® after ablative or RIC CBT
• CD133+ expansion in nicotinamide (NiCord®)

Possible Methods to Improve Delayed Engraftment
• Overcome the limitation in cell dose:• Double cord blood transplant
• Coinfusion of third party donor cells• Haploidentical donor cells
• Ex vivo expansion of CB stem/progenitor cells• Seattle group: Notch ligand expanded CB progenitor cells
ANC recovery at day 12 versus 25 days for historical cohort
• MD Anderson / Baylor: Ex vivo expansion via mesenchymal cell co-cultures
ANC recovery at day 15 versus day 24 for CIBMTR matched cohort
NEJM 2012;367:2305.

Post-CBT ComplicationsImmune Reconstitution after CBT
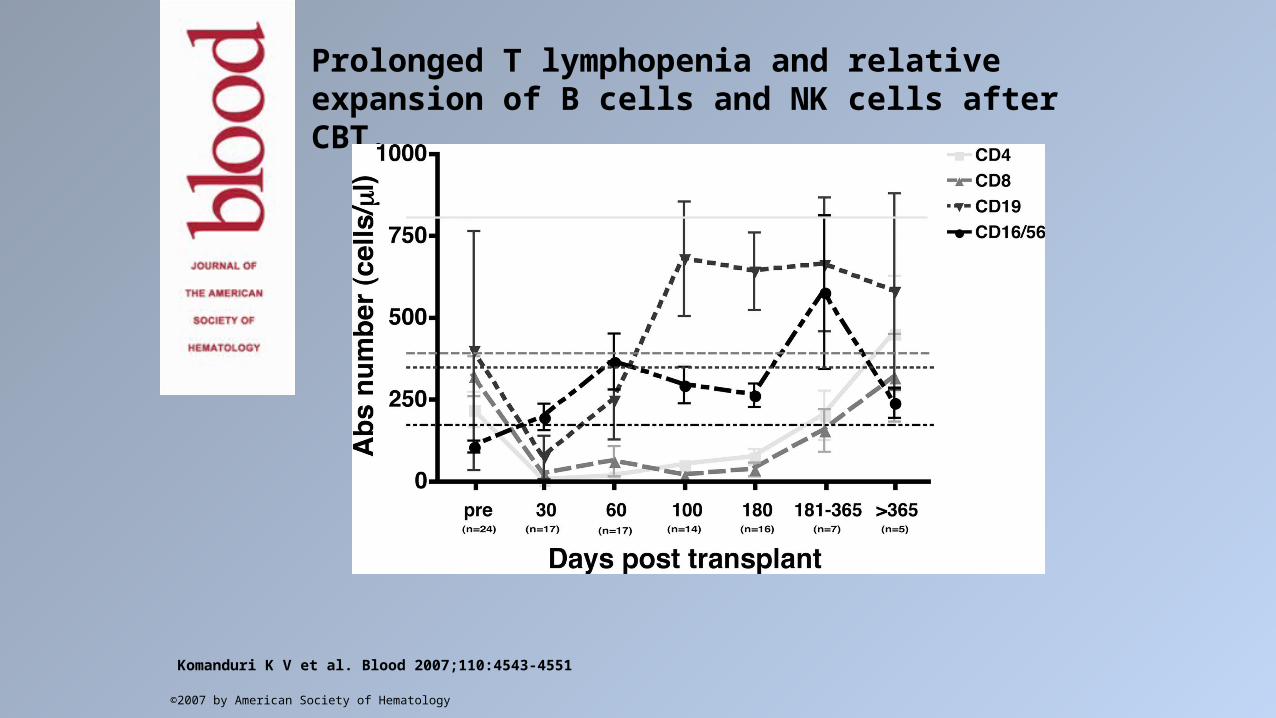
Prolonged T lymphopenia and relative expansion of B cells and NK cells after CBT.
Komanduri K V et al. Blood 2007;110:4543-4551
©2007 by American Society of Hematology

Thymic regeneration failure after CBT.
Komanduri K V et al. Blood 2007;110:4543-4551
©2007 by American Society of Hematology

Post-CBT ComplicationsInfectious Complications
CMV Reactivation after CBT
• High rate of CMV reactivation• Reported rates between ~21% up to 100% 1-2
• Incidence of CMV disease 6-21%2
• Development of disease may be trend for inferior outcomes3
• While there is early CD4+ CD8+ T-cell response to CMV, in correlative studies these T-cells failed to achieve sufficient numbers in vivo to control CMV reactivations4
• Optimal anti-CMV prophylaxis, surveillance, and treatment remain areas of active debate
CBT patients likely require higher level of surveillance as well as treatment/prophylaxis strategies
1. Takami A et al. Haematologica 2005.2. Walker CM et al. BBMT 2007.3. Beck JC et al. BBMT 2010.4. McGoldrick et al. Blood 2013.
Other Infectious Complications after HCT?
• Epstein-Barr virus• Adenovirus disease• Fungal infections
• RIC study found invasive fungal infection in 14/128 patients2
• 13/14 with probable invasive pulmonary aspergillosis• 3-year CI of invasive aspergillosis was 10.2%
• Median onset of IFI was day 20 (range 1-82)• Mortality rate of IFI was 86%• Multivariate analysis revealed steroids >0.2 mg/kg was a significant risk factor for
invasive aspergillosis
1. Sauter C et al. BBMT 2011.2. Miyakoshi et al. BBMT 2007.

Benefits of CBT Enhanced Graft-Versus-Leukemia Effect?
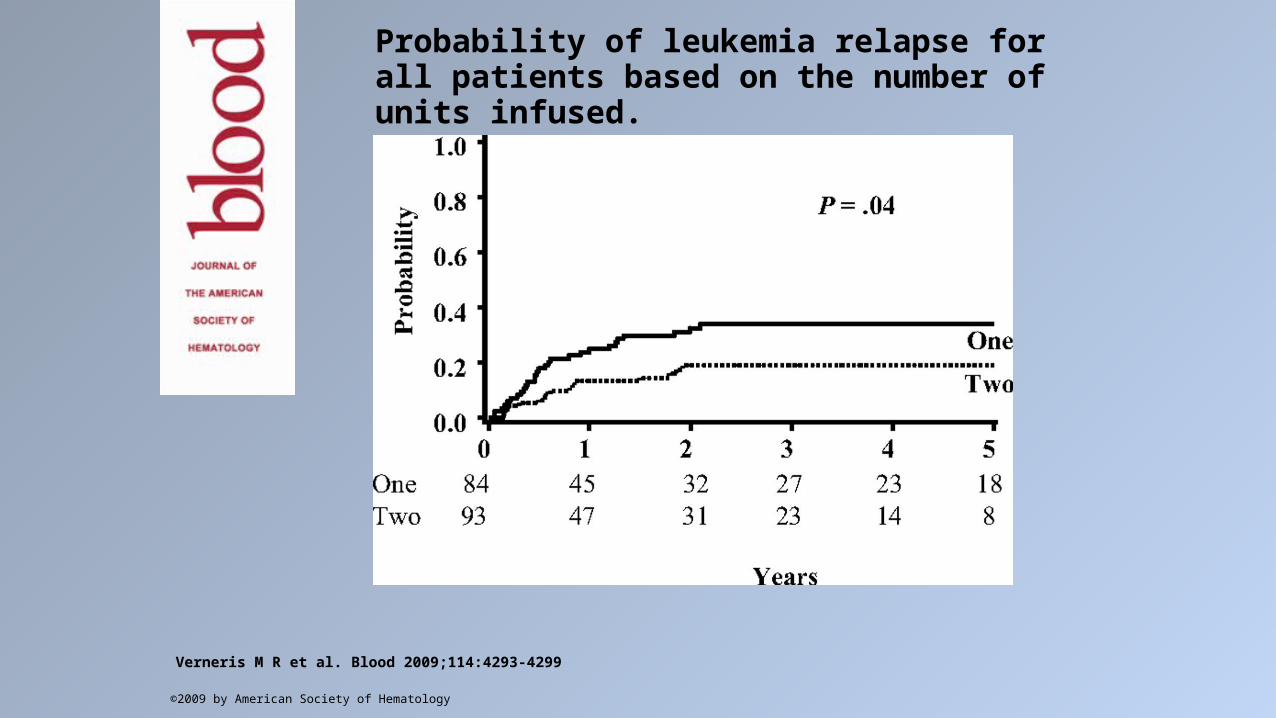
Probability of leukemia relapse for all patients based on the number of units infused.
Verneris M R et al. Blood 2009;114:4293-4299
©2009 by American Society of Hematology

Verneris M R et al. Blood 2009;114:4293-4299
©2009 by American Society of Hematology

Analysis of risk factors for outcomes after unrelated cord blood transplantation in adults with lymphoid malignancies: a study by the Eurocord-Netcord and lymphoma working party
of the European group for blood and marrow
transplantation.
J Clin Oncol. 2009 Jan 10;27(2):256-63. Epub 2008 Dec 8.Rodrigues CA, Sanz G, Brunstein CG, Sanz J, Wagner JE, Renaud M, de Lima M, Cairo MS, Fürst S, Rio B, Dalley C, Carreras E, Harousseau JL, Mohty M, Taveira D, Dreger P, Sureda A, Gluckman E, Rocha V.

Sideri et al. Haematologica 96(8);2011.

Brunstein C G et al. Blood 2010;116:4693-4699
©2010 by American Society of Hematology
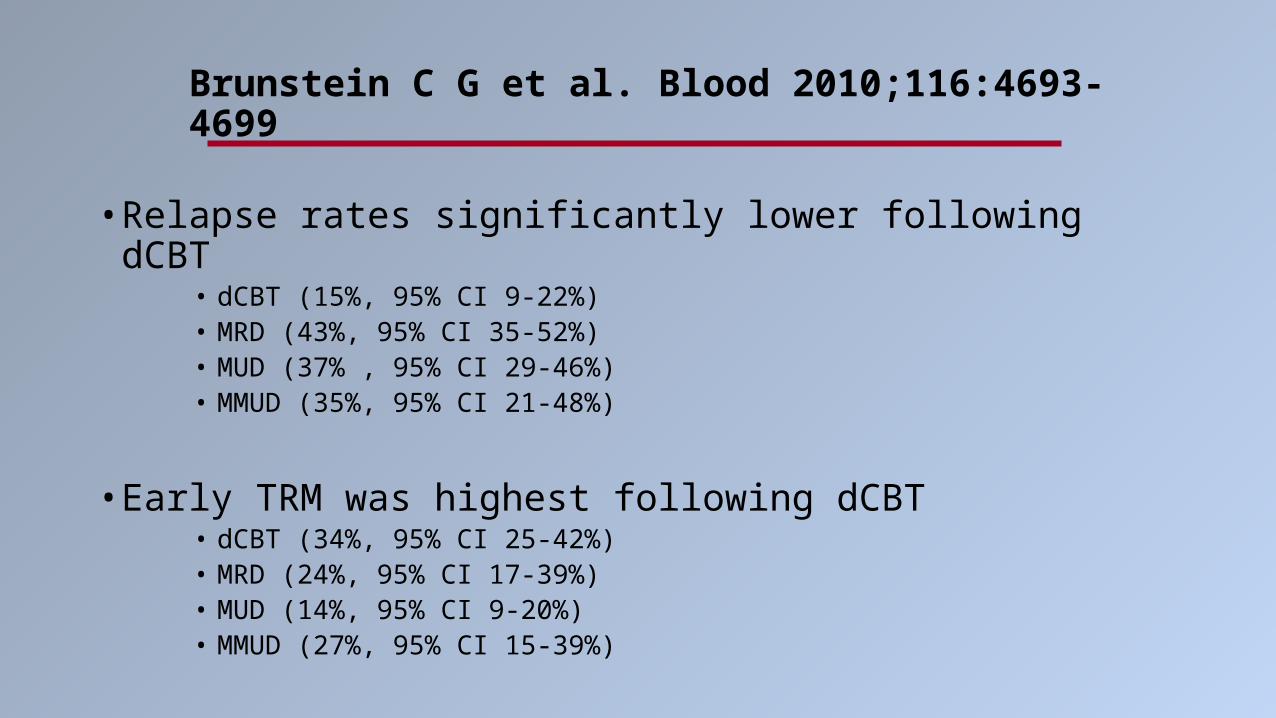
• Relapse rates significantly lower following dCBT• dCBT (15%, 95% CI 9-22%)• MRD (43%, 95% CI 35-52%)• MUD (37% , 95% CI 29-46%)• MMUD (35%, 95% CI 21-48%)
• Early TRM was highest following dCBT• dCBT (34%, 95% CI 25-42%)• MRD (24%, 95% CI 17-39%) • MUD (14%, 95% CI 9-20%)• MMUD (27%, 95% CI 15-39%)
Brunstein C G et al. Blood 2010;116:4693-4699

Pro’s / Con’s of Double CBT
• Double CBT associated with higher incidence of acute GVHD (58% vs 39% double vs single)
• Not higher TRM or chronic GVHD for single versus double CBT
• TRM after onset of acute GVHD significantly lower in double CBT compared to single CBT
• 20% vs 39% at 1-year
• Lower leukemia relapse for patients with good disease status in CR1, CR2
Sideri et al. Haematologica 2011.
MacMillan et al. Blood 2009

How to Extend CBT to Older Patient Population?
How to Extend CBT to Older Patient Population?Reduced Intensity Conditioning Regimens
• Reduced intensity conditioning:• Fludarabine 200 mg/m2• Cyclophosphamide 50 mg/kg• TBI 200 cGy
• GVHD prophylaxis with CSA/MMF• Required > 3 x 10^7 TNC/kg

• 110 patients, median age 51 years (17-69)• 85% received double CBT• HLA-match:
• 124 (61%) 4/6-match
• Median infused doses:• TNC/kg = 3.7 x 10^7• CD34/kg = 4.7 x 10^5• CD3/kg = 1.1 x 10^7

• Neutrophil engrafted in 92% of patients• Median of 12 days (0-32)• No difference between recipients of 1 versus 2 units
• CI of sustained engraftment 85%• Primary graft failure = 7; secondary graft failure = 8
• CI of platelet recovery by day 180 = 65%• Occurred at median of 49 days
• Double unit chimerism detectable in marrow of 43% of patients at day 21, 9% at day 100, 0% at 1-year
Optimal Reduced Intensity Regimen
• Remains an area of active investigation• Melphalan-containing regimens• TBI/Fludarabine• Treosulfan• ATG-containing regimens

Benefits of CBT Less, or More Treatment-Responsive Graft-Versus-Host Disease?

Chronic GVHD after CBT
• Relatively mismatched donor source with CBT• Reported increased incidence of acute GVHD after dCBT
• Literature has suggested a potentially lower overall incidence of chronic extensive GVHD after CBT
• Reported incidences vary widely:• 10-20% to 89% after ablative single and double CBT• ~12% to 40% after reduced intensity CBT

Chronic GVHD after CBT
• Mechanisms for the potential difference in chronic GVHD after CBT, compared with other stem cell sources, remain to be defined.
• CB T-cells have been reported to have greater immune tolerance to HLA-mismatch, generally thought to be due to the overall immaturity of the immune cells
• Decreased cytotoxicity of cord blood CD8+ T-cells• Impaired allogeneic activation with subsequent decreased production of interferon-γ• Defective Th1 responses of CB T-cells related to differential expression and activation of
transcription factors• Impaired cord blood dendritic cell maturation and cytokine production
Response Rate to Treatment of Chronic GVHD after CBT
• Arora et al. evaluated presentation and response to treatment in 170 patients with chronic GVHD
• Complete response (CR): resolution of all reversible signs and symptoms of cGVHD.
• Partial response (PR): improvement in 1 or more organs of involvement and no evidence of worsening in any organ.
• Progression: defined as worsening in 1 or more organs of involvement to be more severe than at baseline.
• Compared URD, predominately HLA-matched marrow (n=123), versus CBT (n=47)
Arora M et al. BBMT 2007.

Response Rate to Treatment of Chronic GVHD after CBT
• Higher response rates among recipients of CBT• Similar incidence and timing of discontinuation of
immunosuppression• Higher NRM after chronic GVHD following URD
transplant • 27% versus 11% (URD versus CB) at 1-year (p=0.055)
Time Point URD Response Rate CB Response Rate p value
2-months 48% 74% 0.005
6-months 49% 78% 0.001
1-year 51% 72% 0.03
2-years 47% 70% 0.05
Arora M et al. BBMT 2007.

Historical Classification of Chronic GVHD
Limited_ Localized skin involvement or_ Hepatic dysfunction due to chronic GVHD, or_ Localized skin involvement and hepatic dysfunction
Extensive • Generalized skin involvement, or_ Findings of limited chronic GVHD plus
· Aggressive hepatitis, bridging necrosis, cirrhosis, or· Ocular sicca, or · Oral involvement, or· Involvement of any other organ
Shulman, Sullivan, Weiden et al. Am J Med. 1980; 69:204Slide courtesy of Dr. Mary Flowers.

2005 NIH Consensus Criteria for Classification of Chronic GVHD
• Proposed new criteria for the diagnosis and classification of chronic GVHD for clinical trials
• Goals were to:(1) Establish criteria for diagnosis of the disease, emphasizing the distinction
between acute and chronic GVHD(2) Define criteria for scoring the severity of clinical manifestations in affected
organs(3) Propose categories describing the overall severity of the disease and the
indications for treatment
Filipovich AH et al. BBMT 2005.
NIH consensus criteria have been evaluated in the conventional donor setting in several large series. In the CBT setting, NIH consensus criteria have only been evaluated prospectively in 1 study of CBT patients.
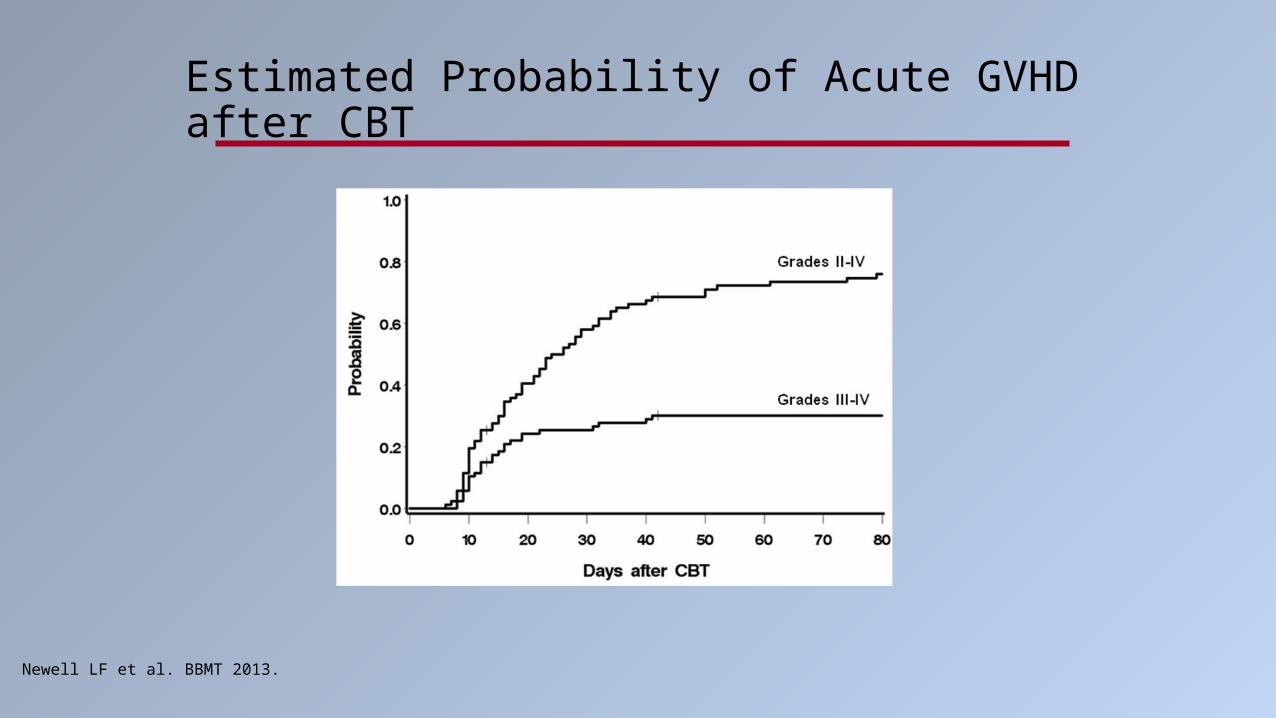
Estimated Probability of Acute GVHD after CBT
Newell LF et al. BBMT 2013.
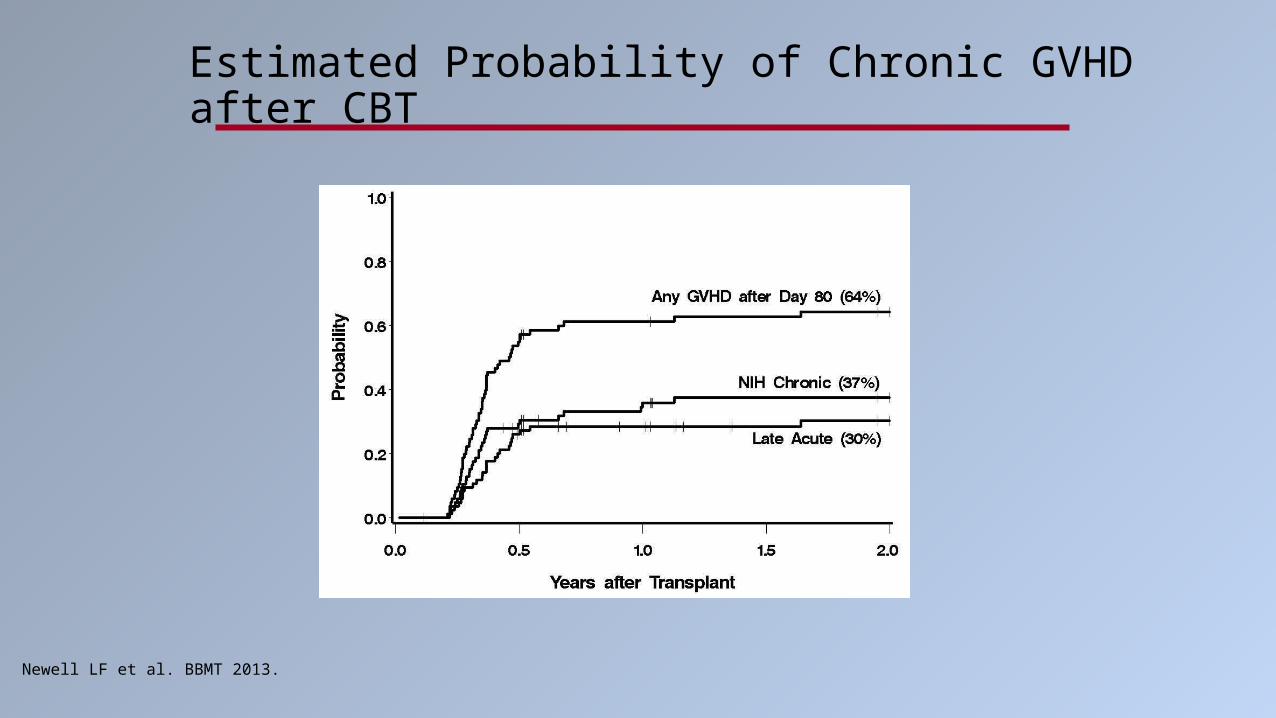
Estimated Probability of Chronic GVHD after CBT
Newell LF et al. BBMT 2013.
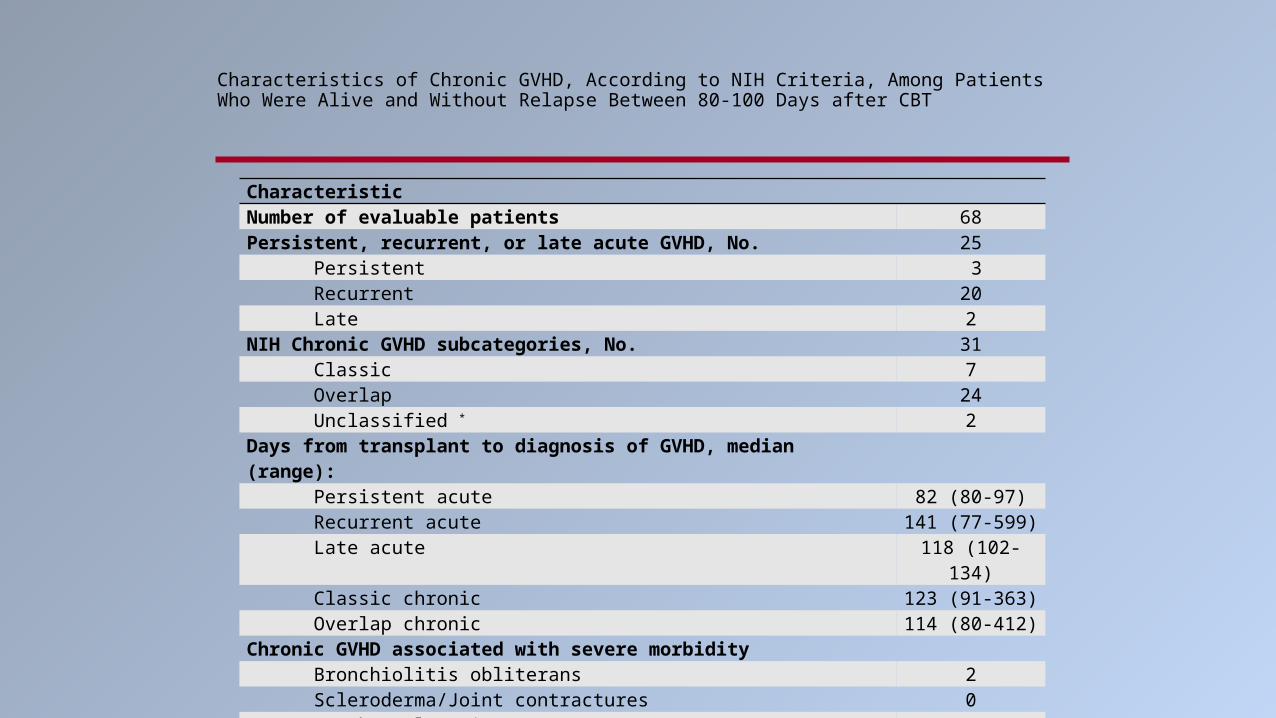
Characteristics of Chronic GVHD, According to NIH Criteria, Among Patients Who Were Alive and Without Relapse Between 80-100 Days after CBT
CharacteristicNumber of evaluable patients 68Persistent, recurrent, or late acute GVHD, No. 25 Persistent 3 Recurrent 20 Late 2NIH Chronic GVHD subcategories, No. 31 Classic 7 Overlap 24 Unclassified * 2Days from transplant to diagnosis of GVHD, median (range): Persistent acute 82 (80-97) Recurrent acute 141 (77-599) Late acute 118 (102-134) Classic chronic 123 (91-363) Overlap chronic 114 (80-412)Chronic GVHD associated with severe morbidity Bronchiolitis obliterans 2 Scleroderma/Joint contractures 0 Esophageal stricture 1 Serositis 5* Treated with immunosuppression for cryptogenic organizing pneumonia at day 123 post-transplant (n=1), and for anasarca at day 309 after transplant (n=1).

Probability of Discontinuation of Immunosuppression

Financial Costs of CBT

Comparison of CBT vs MRD Transplant
• U Minnesota group compared costs of HCT within first 100 days:• MRD: n=67 ablative, n=54 nonmyeloablative• CBT: n=63 ablative, n=110 nonmyeloablative
• Comparable 100-day probabilities of overall survival, TRM• Delayed ANC recovery with CBT• Greater incidence of graft failure with CBT
• Median cost per day survived:• $1016 for ablative MRD• $2082 for ablative CBT• $612 for nonmyeloablative MRD• $1156 for nonmyeloablative CBT
Majhail et al. BBMT 2009.

Comparison of CBT vs MRD Transplant
• Factors associated with higher costs within first 100 days in multivariate analysis:
• Graft failure• Need for dialysis• Mechanical ventilation• Ablative CBT
• Longer inpatient stay with associated costs (i.e. pharmacy, room, blood draws, etc)• Due to longer time to engraftment
Authors connote that this study did not address long-term costs of CBT: Given potential for less (severe) / more treatment responsive GVHD after CBT, will
this translate into lower costs over an extended period of time?
Majhail et al. BBMT 2009.

Cost Effectiveness of Single vs Double CBT in France
• Adult patients, acute leukemia in CR, 2002-2009, n=134• In myeloablative setting:
• Similar total cost• Greater cost of CB units for doubles• Increased hospitalizations for singles (increased infections, increased relapse)
• In RIC setting:• Higher total cost for double CBT
• Greater cost of CB grafts with doubles• Increased hospitalizations for GVHD with doubles
Rocha V et al, 2012 International Cord Blood Symposium
Future Directions in CBT

How to Select CB Units?• Traditionally based on HLA-match, TNC/kg cell dose, unit quality
• HLA-A and –B typing at antigen level, high resolution typing for HLA-DRB1 alleles• Minimum 4/6-matched, each > 1.5 x 10^7 TNC/kg
• 6/6-match: minimum single unit dose required > 3 x 10^7/kg• 5/6-match: > 4 x 10^7/kg• 4/6-match: > 6 x 10^7/kg
Ongoing studies on benefit of further high resolution typing, effect of HLA-C matching
How to Select CB Units?• Higher CD34+ viability
• Part of benefit of double CBT is increased likelihood of transplanting at least 1 good unit• Not all banks are the same
• Lower CD34+ viability from less commonly used banks (range 36-94% versus >70-90% with commonly used banks)
• CD34 dose important for engraftment, not necessarily for single donor dominance• Unit-unit match, patient-unit match no effect
• Speed of neutrophil engraftment related to CD34+ dose• Potential dose-dependent effect TNC, CD3+

Other Factors ?• Effect of HLA-C matching: Eapen et al. The Lancet Oncology
2011;12(13):1214.• More significant for 6/6-matched CBT
TRM 9% with C-match vs. 26% with C-MM
• Also for 5/6-matched CBT TRM 32% with C-match vs. 44% for C-MM
• NIMA: • Improved NRM, LFS ?
• Donor-specific antibodies: • Associated with increased TRM, decreased engraftment

Future Questions / Directions
• Number of CB units to infuse• Is double CBT the standard for adult patients
• Ideal conditioning regimens• Ablative regimens• RIC regimens
• Third party donor cells?• Manipulation of CB stem cells
• Generation of NK cells, CMV specific T-cells, etc
• Novel methods to improve homing / engraftment• PGE2-modulation• Fucosylation• CD26/DPP4 inhibition• Copper chelation
Questions?
Related Documents