COPP MODULE COMMON OFFICE PRACTICE PEDIATRIC PROBLEMS [A MODULE OF IAP TAMILNADU STATE CHAPTER 2017]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

COPP MODULE
COMMON OFFICE PRACTICE PEDIATRIC PROBLEMS[A MODULE OF IAP TAMILNADU STATE CHAPTER 2017]

TEAM• Scientific advisors Dr P Ramachandran, Dr S Balasubramanian
• Conveners Dr S Thirumalai Kolundu, Dr Sunil Srinivasan
• Scientific Coordinator Dr A Somasundaram
• Academic coordinators Dr S Narmada, Dr R.V Dhakshayani
• Academic committee [MODERATORS]• Dr NC Gowrishankar,• Dr T N Manohar,• Dr K Nedunchelian,• Dr Rema Chandramohan,• Dr R Somasekar,• Dr S Thangavelu,• Dr V V Varadarajan

• 1.Dr.R.V.Dhakshayani• 2.Dr.Hemchand K
Prasad• 3. Dr.E.Mahender• 4.Dr.S.Mangalabharathi• 5.Dr.C.Manigandan• 6.Dr.S.Manikumar• 7.Dr.S.Giridar• 8.Dr.S.Narmada• 9.Dr.R.Selvan
• 10.Dr.A.Somasundaram• 11.Dr.P.Sudhakar• 12.Dr.Sudharsana
Skanda• 13.Dr.N.Suresh• 14.Dr.So.Sivabalan• 15.Dr.S.Srinivas• 16.Dr.Venkateswaran• 17.Dr.C.Vijayabhaskar• 18.Dr Palaniraman• 19.Dr B.Sumathi

Dr. S. Srinivas MBBS DCH DNB (PED) MNAMS PDCC (PED GASTRO)
FELLOWSHIP IN PED GASTRO (AUSTRALIA)
• Consultant Pediatric gastroenterologist, Apollo Children’s Hospital & KKCTH
• Prizes and Awards– Karthikeyan Memorial Gold Medal for Pediatrics 1996 as an undergraduate– Represented my college in the inter-zonal round of the National Undergraduate Quiz conducted by
the Indian Academy of Pediatrics 1996– Certificate of Best performance in Otorhinolaryngology– Distinction in the subject of Anatomy during the Undergraduate University Exams– Second prize in the Annual Pediatric Postgraduate National Nephrology Exam 2000
• Research activities– postgraduate thesis on ‘The Gastrointestinal and Neurological manifestations of DH Fever’– Was involved in research project on ‘Bone Mineral Density in children with Inflammatory
Bowel Disease’ during my stint as fellow at Royal Childrens Hospital, Melbourne
• 6 peer reviewed research articles• Co authored 4 chapters• Multiple papers presented at National and International Pediatric
Gastroenterology Conferences

Dr. SRINIVAS SConsultant Pediatric Gastroenterologist
Moderator
Dr. T.N.Manohar
CONSTIPATION

WHAT IS CONSTIPATION
Difficulty & delay in passing stools resulting in significant distress lasting for more than 2 weeks.
The definition is subjective & involvesü Stool frequencyü Stool consistencyüDifficulty in passage

ETIOLOGY OF CHILDHOOD CONSTIPATION
• 5 - 10% : Organic causes• 90 - 95% : Functional constipation_______________________________________• In infantile onset of constipation – always
suspect an organic cause strongly
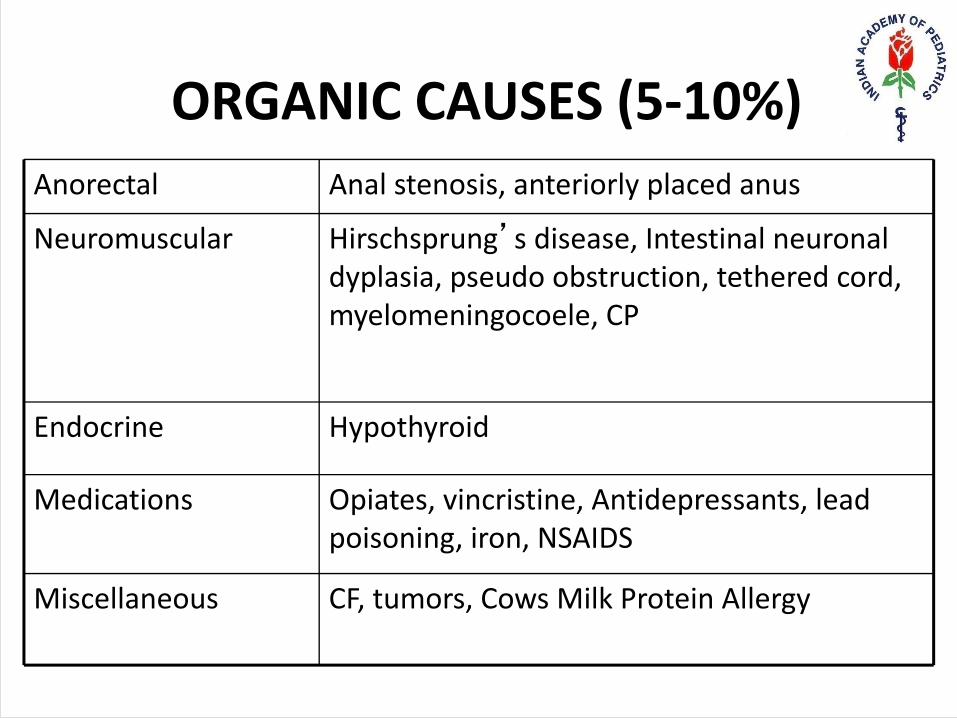
ORGANIC CAUSES (5-10%)Anorectal Anal stenosis, anteriorly placed anus
Neuromuscular Hirschsprung’s disease, Intestinal neuronal dyplasia, pseudo obstruction, tethered cord, myelomeningocoele, CP
Endocrine Hypothyroid
Medications Opiates, vincristine, Antidepressants, lead poisoning, iron, NSAIDS
Miscellaneous CF, tumors, Cows Milk Protein Allergy

WHEN TO SUSPECT ORGANIC CAUSE?
• Age of onset < 1 year• Delayed passage of meconium• Absence of withholding• Absence of fecal soiling• Bladder dysfunction• No response to conventional therapy• Clinical clues like growth retardation,• Abdominal wall, perineum, lumbosacral and lower limb
examination suggests abnormality

FUNCTIONAL CONSTIPATION
Functional constipation refers to a form of chronic
constipation in children (i.e. symptoms > 2 months)
AND
there are no demonstrable anatomic, physiologic or
histopathological abnormalities to explain the same.

EPIDEMIOLOGY
• Age: peak toddlers and preschool children. Shortly after toilet training.
• Sex: More in boys than girls.• All social classes• 30% may continue to have symptoms beyond puberty
A TYPICAL HISTORY
• 3 yr old boy with constipation since 1 yr of age• Hard stools – often pellet like• H/O fear of defecation – often stands and stools,
withholding manoeuvres• H/O fecal soiling• Multiple doctor consults• Intermittent use of laxatives• Not toilet trained

PREDISPOSING FACTORS FOR THE ONSET
• Minor illness, prolonged recumbency• Drugs• Dietary factors: Low fiber, low fluid intake and milk rich
diet. Recent change in formula/ diet• Other causesLack of toilet trainingSchool environmentNot enough time to potty before going to school
Remember all chronic constipation starts acutely !!
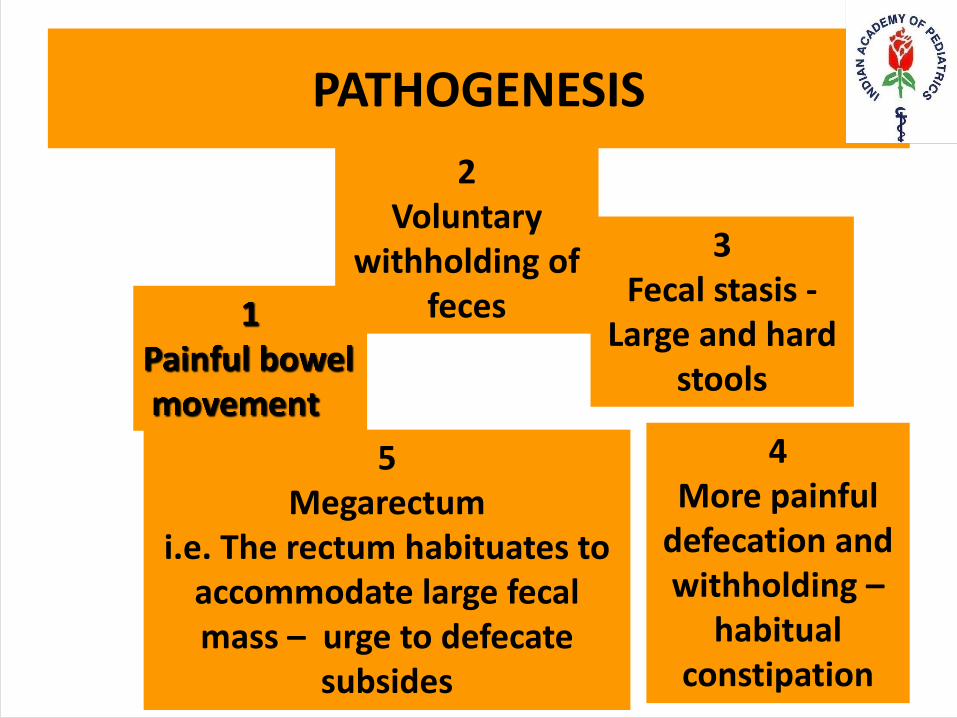
PATHOGENESIS2
Voluntary withholding of
feces
3Fecal stasis -
Large and hard stools
4More painful
defecation and withholding –
habitual constipation
5Megarectum
i.e. The rectum habituates to accommodate large fecal mass – urge to defecate
subsides
CLINICAL EXAMINATION
Growth chart: no FTT Abdomen: soft, no organomegaly but some resistance/
fecal mass in hypogastrium and LIF Peri anal region: Fissure at 12 o clock. Normal peri anal wink and sensations. Tightens his anal sphincter PR: not to be done in the presence of painful fissure Spine: No tuft of hair or skin dimples

INVESTIGATIONS
• Seldom required• Plain X ray abdomen: Obese – thick abdominal wall and
where PR not possible• USG abdomen: if you suspect voiding dysfunction or
history of UTI• Thyroid profile - not needed unless there is clinical
suspicion

MANAGEMENT OF CONSTIPATION
• Education• Disimpaction• Maintenance• Follow up• Evaluation of refractory patients

EDUCATION
• Spend time with the patient & entire family/ caregivers
• Explain physiological basis of constipation and soiling
• Explain the concept of secondary mega rectum and
hence the need for long term laxatives & follow-up
• Need for comprehensive bowel training program
• Optimum dose is unpredictable, so need for frequent
meetings initially.

DISIMPACTION
1. First line therapy is PEG – polyethylene glycol
2. Enema - painful, less preferred option. Certainly not to be used
on a regular basis or in presence of a fissure.
3. Digital disimpaction preferably under anaesthesia - very rarely
needed in a small minority of children who fail to disimpact
with PEG.
Positioning For Enema
HOSPITAL BASED PROTOCOL
• PEG solution as lavage 25 ml/ kg/ hr orally or through N/G tube
• End- point: Clear rectal effluent
• Caution: Watch for bloating, fluid overload, vomiting and electrolyte imbalance
HOME BASED PROTOCOL
• 1.5-2 g/kg/day of PEG twice a day x 3-5 days orally till the passage of liquid stools
DISIMPACTION WITH PEG

LAXATIVES
• Lactulose/ PEG/ stimulant laxatives • It does not matter what you use• They all soften stools• Ensure pain free defecation• Ensure regular bowel movements• Do not ensure cure• Toilet training and behaviour modification is vital

MAINTENANCE - LAXATIVES
CHOICE OF LAXATIVESInfants PEG/Lactulose/ Lactitol
Children > 1 yr Polyethylene glycol / Lactulose/ Lactitol
DOSEPolyethylene glycol (PEG) 0.5 g - 1 g/kg/day
Lactulose 1-2 ml/kg/day
Lactitol 1-3 ml/kg/day
All are osmotic laxatives. Hence the higher doses of laxatives can result in abdominal bloat, cramps and flatulence

WHEN TO USE STIMULANT OR IRRITANT LAXATIVES
Stimulant laxatives are used only as rescue therapy for
2-3 days to tide over an acute or sudden episode of
constipation while being compliant on regular laxative
therapy
Eg. Bisacodyl (oral/rectal), Sodium picosulphate, Senna.

TREATING A PAINFUL FISSURE
• Avoid enemas/Digital examnination.
• 2% xylocaine jelly or coconut oil may be used topically for pain relief.
• SITZ bath offers some pain relief

BEHAVIORAL MODIFICATION
1) Routine toilet sitting twice daily§ 5 -10 min after meals - utilize gastrocolic reflex§ Develop a regular habit, conditioning§ Maintain a stool diary/ chart to ensure compliance
2) Positive reinforcement• Reward Method / No punishment
3) A small proportion of adamant toddlers may remain resistant to toilet training
DIET MODIFICATION
ü Plenty of fluids and water
ü Restrict milk intake only in kids who are milk guzzlers
ü High fiber diet - adequate green leafy veg and fruits
ü Fiber requirement in gms / day = age in years + 5
ü Diet modification alone without laxatives is insufficient .

FIBRE CONTENT IN DIET
One fruit 100gm = 2-3 g Fibre
One Fruit 200 gm = 4-6 g Fibre
50 gm GLV = 4 g Fibre
One 100gm = 4-6 g Fibre

FOLLOW UP
§ Initially: weekly, then fortnightly, then monthly till stooling is normal.
§ Stool diary is helpful§ Start reducing dose gradually only after the child is
toilet trained and remains symptom free for a minimum period of 8 wks
§ No abrupt stoppage of treatment § Commonest cause of recurrence is premature
withdrawal of laxatives § Outcome is better if we intervene early

THANK YOU
Related Documents











