
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 1/50

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 2/50
COPD:Spirometry
Clare Hawkins, MD, MSProgram Director, San Jacinto Methodist Hospital Family Medicine Residency,Baytown, TX
Isaac M. Goldberg, MDFaculty, San Jacinto Methodist Hospital Family Medicine Residency, Baytown,TX

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 3/50
Educational Objectives
At the end of this presentation, thelearner should be able to …
• Utilize spirometry to diagnose and stageCOPD
• Overcome barriers to the use of officespirometry
• Achieve confidence with spirometryinterpretation

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 4/50
Background
Objective measure of airway function for accuratediagnosis of Chronic Obstructive PulmonaryDisease (COPD)
World Health Organization Global Obstructive LungDisease Consensus/ Evidence guideline (GOLD)
American Thoracic Society (ATS)
European Respiratory Society (ERS)
National Committee for Quality Assurance (NCQA)

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 5/50
Background
Alternate ways to diagnose COPD
Clinical Findings Late- Increased AP diameter, tympanitic chest
-
Signs of respiratory distress Peak flow reading not adequately sensitive or specific
Radiographic findings occur late in disease
CT scanning more accurate, but findings also occur
late in disease

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 6/50
Background
Who should receive spirometry? Early diagnosis relies on the recognition of the clinical
features- Persistent cough
-Chronic sputum production
- Breathlessness on exertion
- Reduction in activity (often attributed to natural aging)
About 20% of COPD patients identified in NHANESstudy with obstruction never smoked
- Only 1/5 were explained by asthma

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 7/50
Background
Other testing considerations Recurrent or chronic respiratory symptoms Occupational exposure to respiratory irritants
Family history of respiratory diseases and symptoms NCQA established use of spirometry as required
quality measure for accurate COPD diagnosis Routine periodic use not recommended

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 8/50
Background
Screening Not recommended in the absence of respiratory
symptoms (dyspnea, cough)
No threshold amount of smoking pack-years forscreening in the absence of respiratory symptoms Not recommended by USPSTF or ACP 2011
Guideline

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 9/50
Background
Family physicians able to do quality spirometry
Quality of care increases with use of spirometry- To prevent overdiagnosis of COPD, attention to quality
spirometry is important
Suggestions to maintain quality of spirometry- Know technique
- Have staff coach the patient
- Do sufficient numbers of tests
-Maintain and calibrate the equipment
- Understand interpretative algorithms

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 10/50
Background
Why do office spirometry? Diagnostic accuracy. 30% of time diagnosis changes.
- Was not COPD; heart failure or asthma
- Was COPD rather than asthma
- If spirometry normal, then expensive meds discontinued
Respect. Patients respect physicians who usetechnology (Future of Family Medicine)
Patient convenience. You can avoid an unnecessaryreferral and additional visit
Diagnostic power: You can connect diagnosticinformation with rest of clinical encounter
Financial benefit to practice.

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 11/50
Equipment
Older volume/time loop- Drum technique from John
Hutchinson 1844
Newer flow/volume loopusing flow transducer- Smaller Machines, Mobile
- Disposable Mouthpiece
No other infection
transmissionprecautions necessary

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 12/50
Equipment
Numerous manufacturers produce quality instruments
Reviews conducted by National Lung Health EducationProgram (NLHEP) regarding appropriateness ofspirometers for office practice- http://www.nlhep.org/spirometer-review-process.html
- Simplicity (fewer numbers)
- Reliability

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 13/50
Equipment
Calibration
Daily calibration must be done with 3 L syringe
Syringe must have accuracy of at least 15 ml
Spirometer must have accuracy of ±105 mL or0.105 L (calibration volume = 2.90 to 3.11)
Calibration log/printouts must be kept
- Date and time of calibration
-Individual performing
- Comments

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 14/50
Technique
Forced expiratory maneuver
Coach patient to get a maximal effort
Six seconds of effort required though most of air pushed
out in the first second Pace of expired air is most important variable; therefore
it should be released with explosive force

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 15/50
Technique
Minimum 6 second exhalation with 2 second plateau
Tracing should have no artifacts
At least 3 acceptable maneuvers (<5 % variation)
- ATS criteria
Empty bladder for females (concern if incontinence)
Can be seated or standing
Nose plug optional

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 16/50
Technique
None of the following should occur: Unsatisfactory start, with excessive hesitation or false start
Air leak
Coughing during the first second Early termination of forced expiration
Glottis closure
Obstructed mouthpiece -
Tongue- False teeth
- Chewing gum

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 17/50
Technique
Reliability
Spirometry overdiagnoses COPD if insufficient effort
Concerns that family physicians will not perform
quality testing and overdiagnose people withobstructive lung disease
Imperative that patients be coached on robust, forcedexpiratory maneuver
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 18/50
Technique
Contraindications
Hemoptysis of unknown origin
Pneumothorax
Unstable cardiovascular status or recent MI or PE Thoracic, abdominal, or cerebral aneurysms
Recent eye, thorax or abdomen surgery

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 19/50
Technique
Barriers Inaccessibility of Equipment Concern patient effort and cooperation are insufficient Difficulty remembering interpretive algorithm
Frustration by ambiguous results Difficulty working 30-minute spirometry into office flow Central location for spirometry versus going room to
room Lack of staff training Poor integration with electronic health record Lack of adequate reimbursement

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 20/50
Measurements
Abbreviation Characteristic measured
FEV1 Forced expired volume in 1 second
FVC Forced vital capacity
FEV1 /FVC
Ratio
Ratio of the above
PEFR Peak expiratory flow rate
FEF 25-75% Forced expiratory flow between 25-75% of the vital
capacity

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 21/50
Measurements
Normal values Individual variation according to age, height, ethnicity
and gender
-Height - Tall people have larger lungs
- Age - Respiratory function declines with age
- Sex - Lung volumes smaller in females
- Race - Studies show Blacks and Asians have smaller lung
volumes (-12%)- Posture - Little difference between sitting and standing;
reduced in supine position

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 22/50
Measurements
Bronchodilator reversibility testing
Beta-agonist
- Short-acting – wait 20 minutes before retesting
-Long-acting – wait 2 hours before retesting
Do not take bronchodilator the day of testing
- Measured reversibility will be limited if the patient isbronchodilated for the pretest.

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 23/50
Measurements
Definition of reversibility
Pre-Bronchodilator
- FEV1/FVC <70% of predicted
Post-Bronchodilator- Increase 12% AND at least 200 cc
Reversibility = Asthma!
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 24/50
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 25/50
Measurements
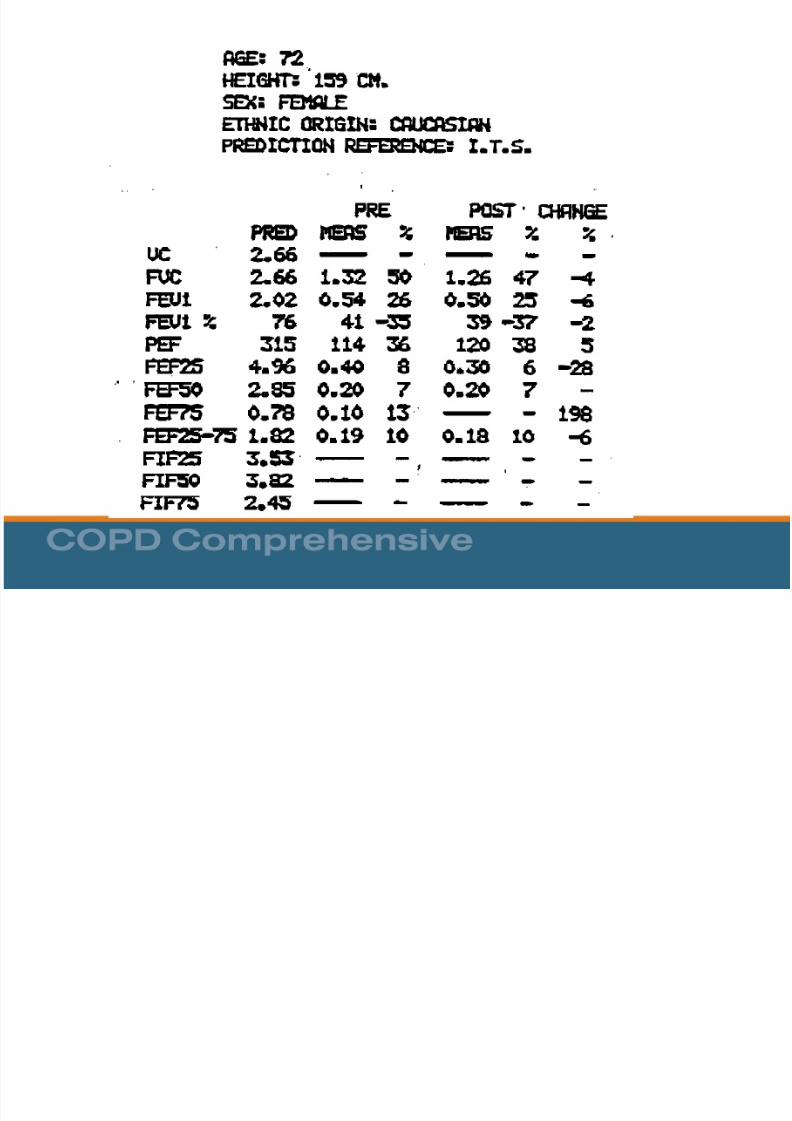
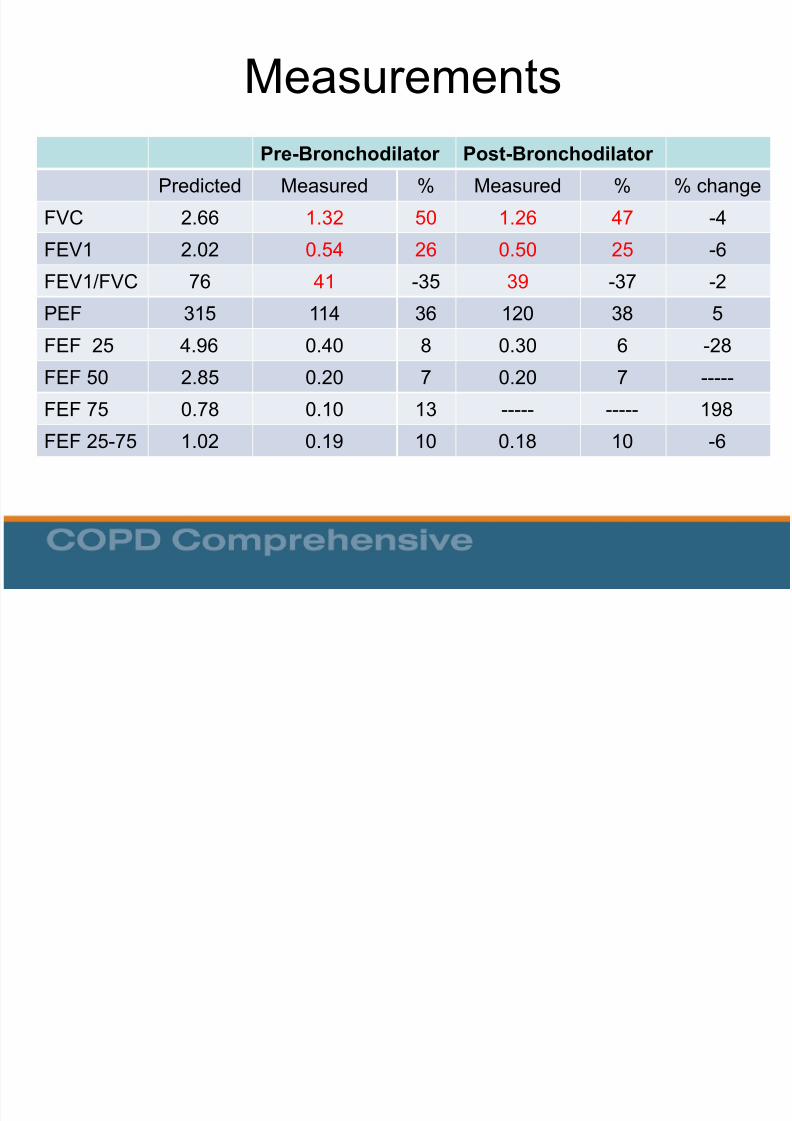
Pre-Bronchodilator Post-Bronchodilator
Predicted Measured % Measured % % change
FVC 2.66 1.32 50 1.26 47 -4
FEV1 2.02 0.54 26 0.50 25 -6
FEV1/FVC 76 41 -35 39 -37 -2
PEF 315 114 36 120 38 5
FEF 25 4.96 0.40 8 0.30 6 -28
FEF 50 2.85 0.20 7 0.20 7 -----
FEF 75 0.78 0.10 13 ----- ----- 198FEF 25-75 1.02 0.19 10 0.18 10 -6
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 26/50
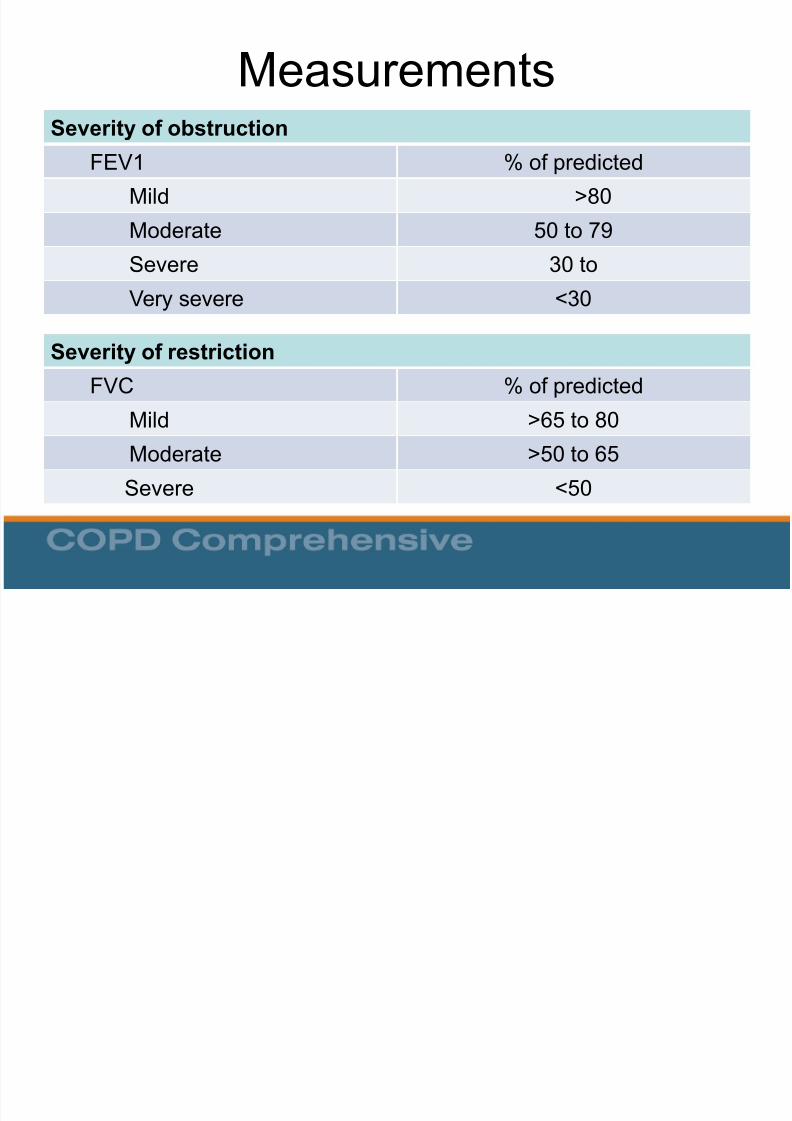
MeasurementsSeverity of obstruction
FEV1 % of predicted
Mild >80
Moderate 50 to 79
Severe 30 to
Very severe <30
Severity of restriction
FVC % of predicted
Mild >65 to 80Moderate >50 to 65
Severe <50
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 27/50
Case Study 1
A 53-year-old white male presents for annualvisit. Although he quit 10 years ago he is aprevious cigarette smoker with a 20 pack-year
history. During the past 12 months, he has had3 episodes of bronchitis. His history of tobaccouse and recent episodes of acute bronchitis leadyou to perform spirometry.
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 28/50
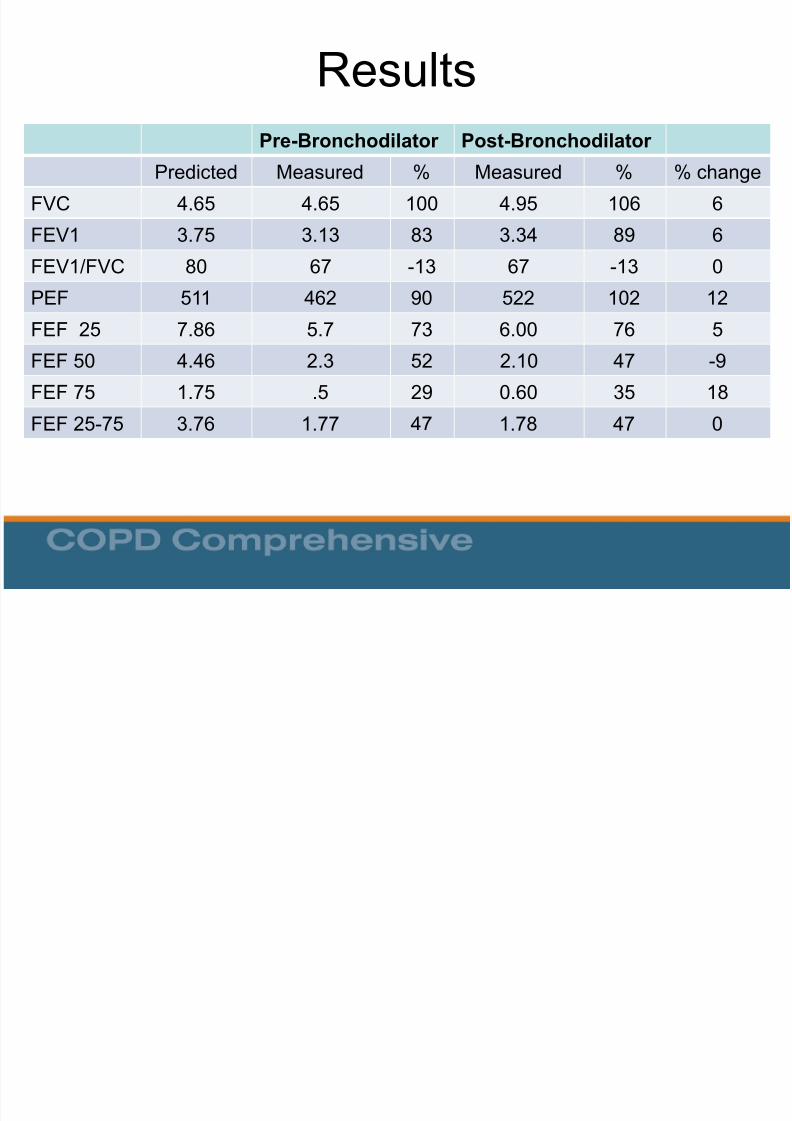
Results
Pre-Bronchodilator Post-BronchodilatorPredicted Measured % Measured % % change
FVC 4.65 4.65 100 4.95 106 6
FEV1 3.75 3.13 83 3.34 89 6
FEV1/FVC 80 67 -13 67 -13 0
PEF 511 462 90 522 102 12
FEF 25 7.86 5.7 73 6.00 76 5
FEF 50 4.46 2.3 52 2.10 47 -9
FEF 75 1.75 .5 29 0.60 35 18
FEF 25-75 3.76 1.77 47 1.78 47 0

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 29/50
Results
Pre-Bronchodilator Post-BronchodilatorPredicted Measured % Measured % % change
FVC 4.65 4.65 100 4.95 106 6
FEV1 3.75 3.13 83 3.34 89 6
FEV1/FVC 80 67 -13 67 -13 0
Is there obstruction?
FEV1/FVC = 67% of predicted; therefore, obstruction present
Is there restriction?FVC = 100% of predicted; therefore, no restriction present

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 30/50
Results
Pre-Bronchodilator Post-BronchodilatorPredicted Measured % Measured % % change
FVC 4.65 4.65 100 4.95 106 6
FEV1 3.75 3.13 83 3.34 89 6
FEV1/FVC 80 67 -13 67 -13 0
What is the severity of obstruction?
FEV1 is 83% of predicted; therefore, the obstruction is mild
Is the obstruction reversible (is reversibility present)?
FEV1 increases from 83% to 89% (6% increase) and increases from 3,130
cc to 3,340 cc (increase of 210 cc)
Interpretation: Mild Obstruction with minimal reversibility: Mild COPD
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 31/50
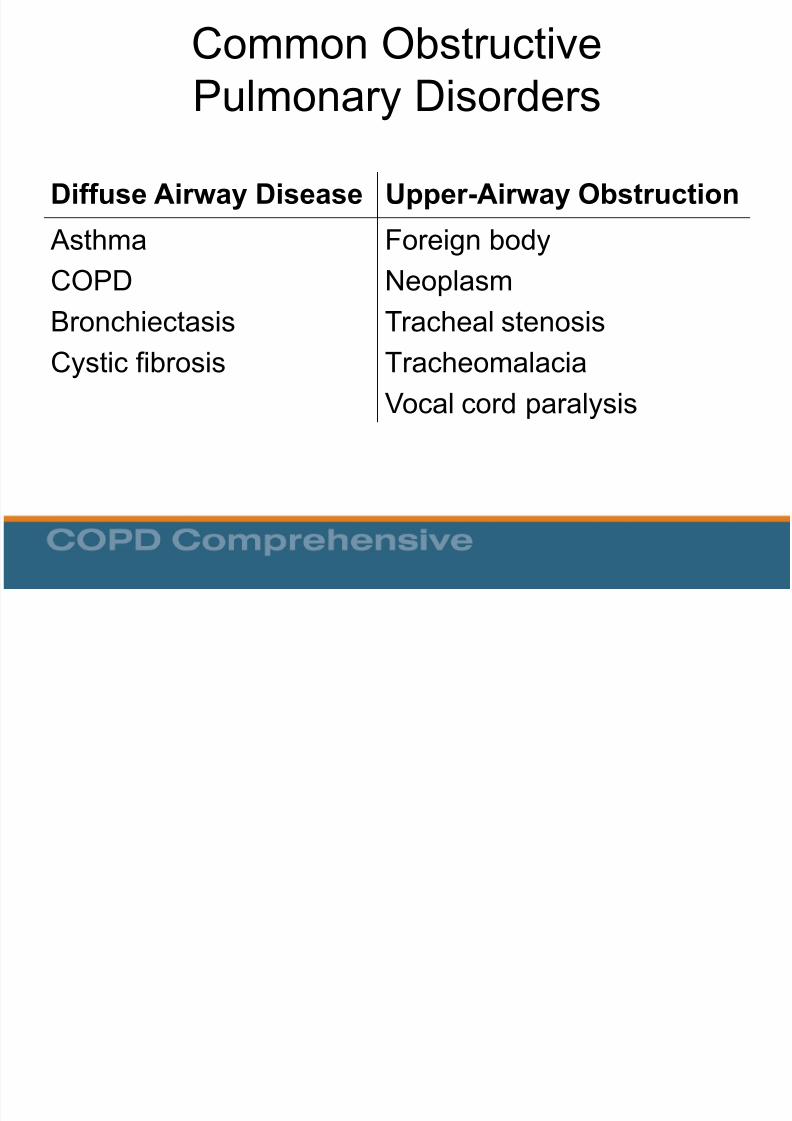
Common ObstructivePulmonary Disorders
Diffuse Airway Disease Upper-Airway Obstruction
Asthma
COPDBronchiectasis
Cystic fibrosis
Foreign body
NeoplasmTracheal stenosis
Tracheomalacia
Vocal cord paralysis

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 32/50
No Yes
Obstructive Defect
Is FVC Low? (<80% pred)
Combined Obstruction &Restriction /or HyperinflationPure Obstruction
Improved FVC withß-agonist
Reversible Obstructionwith ß-agonist
Further Testing withFull PFT’s
SuspectAsthma
SuspectCOPD
Is FEV1 / FVC Ratio Low? (<70%)
Yes
No Yes
No Yes
Diagnostic Flow Diagram for Obstruction
Adapted from Lowry.

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 33/50

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 34/50

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 35/50
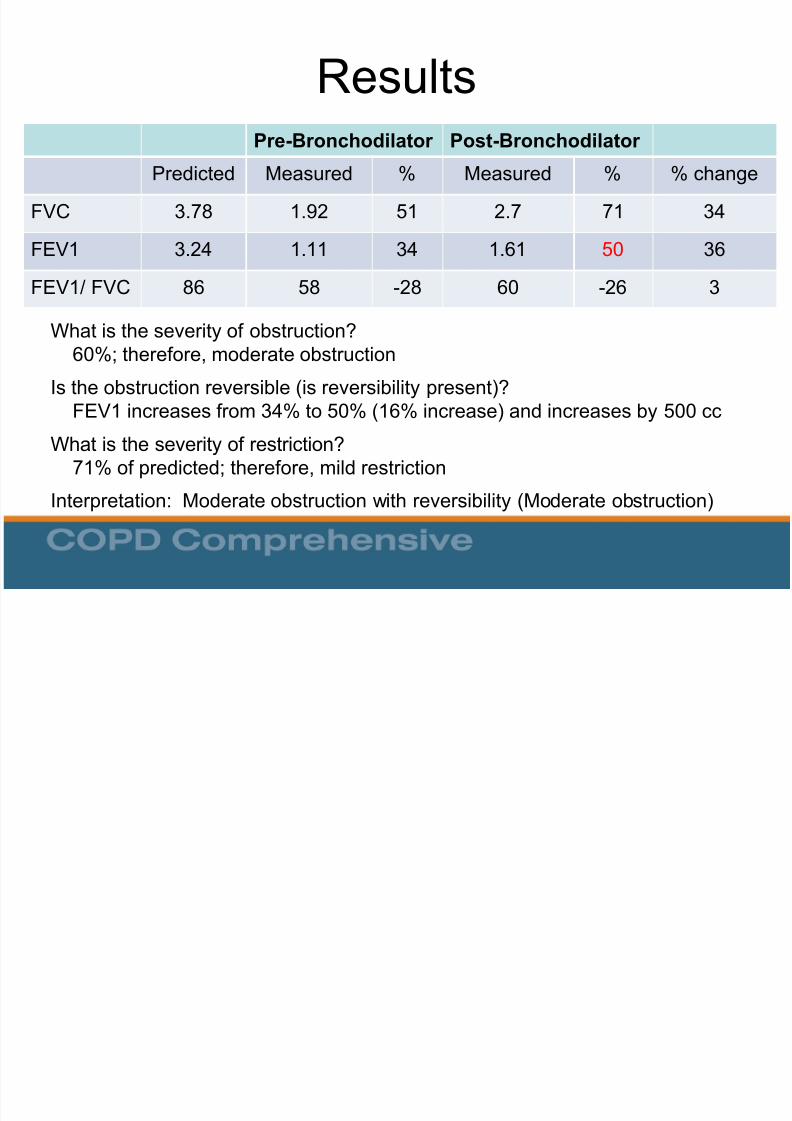
Results
Pre-Bronchodilator Post-Bronchodilator
Predicted Measured % Measured % % change
FVC 3.78 1.92 51 2.7 71 34
FEV1 3.24 1.11 34 1.61 50 36
FEV1/ FVC 86 58 -28 60 -26 3
Obstruction?
FEV1/FVC = 60%; therefore, obstruction present
Restriction?
FVC = 51% of predicted; therefore, restriction present
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 36/50
Results
Pre-Bronchodilator Post-BronchodilatorPredicted Measured % Measured % % change
FVC 3.78 1.92 51 2.7 71 34
FEV1 3.24 1.11 34 1.61 50 36
FEV1/ FVC 86 58 -28 60 -26 3
What is the severity of obstruction?60%; therefore, moderate obstruction
Is the obstruction reversible (is reversibility present)?
FEV1 increases from 34% to 50% (16% increase) and increases by 500 ccWhat is the severity of restriction?
71% of predicted; therefore, mild restriction
Interpretation: Moderate obstruction with reversibility (Moderate obstruction)

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 37/50
Common Restrictive PulmonaryDisorders
Parenchymal Interstitial Lung Diseases
- Fibrosis
- Granulomatosis (TB)
- Pneumoconiosis
- Pneumonitis (lupus)
Loss of Functioning Tissue
- Atelectasis
- Large Neoplasm
- Resection
Pleural Effusion
Fibrosis
Chest Wall
Kyphoscoliosis
Neuromuscular Disease
Trauma
Extrathoracic
Obesity
Abdominal Trauma

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 38/50
No Yes
Is FVC Low?(<80% pred)
Restrictive Defect Normal Spirometry
Further Testing with
Full PFT’s; consider
referral if moderate to
severe
Is FEV1 / FVC Ratio Low? (<70%)
No
Diagnostic Flow Diagram for Restriction
Adapted from Lowry, 1998

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 39/50
Results
Lowry 1998
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 40/50
Results
“Full” Pulmonary Function Testing (PFT’s) Assessment of Oxygenation
- Transcutaneous oxygen saturation
- Arterial blood gasses
Diffusion test to evaluate alveolar exchange (DLCO) Plethysmography
- To objectively assess lung volumes
- Delineate air-trapping versus restriction
May also include Spirometry
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 41/50

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 42/50

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 43/50
Spirometry and Smoking Cessation

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 44/50
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 45/50
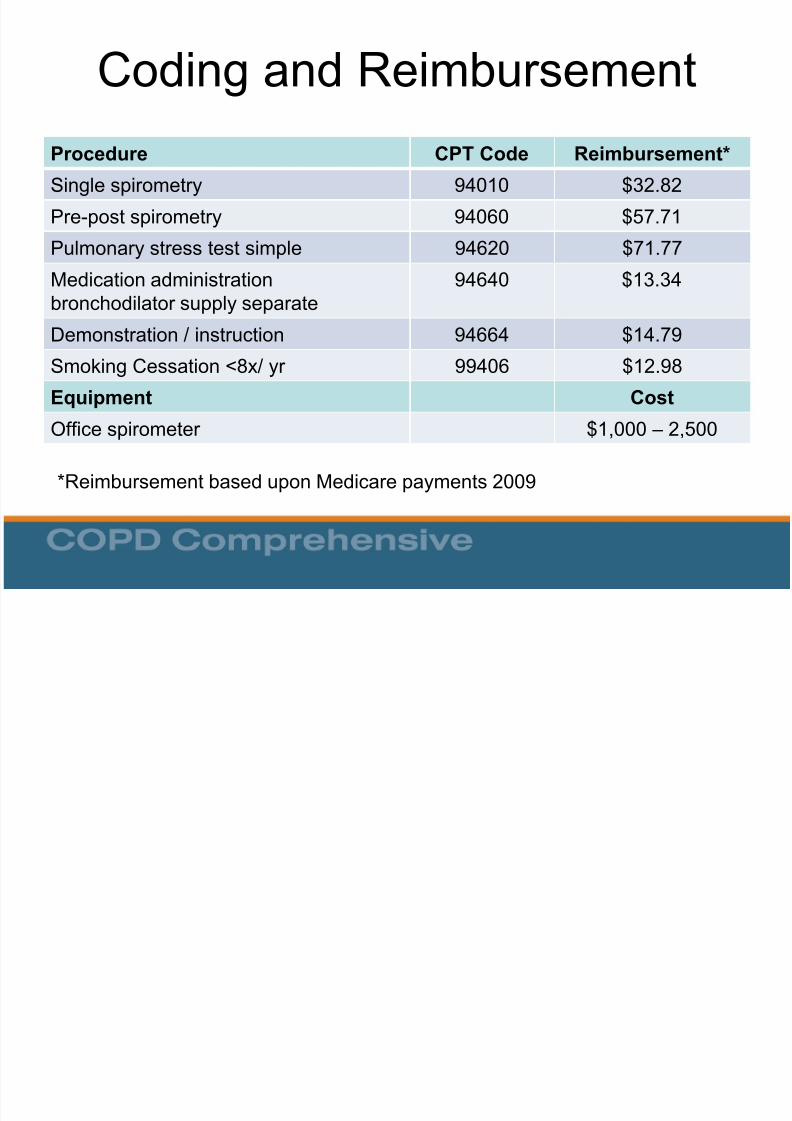
Coding and Reimbursement
Procedure CPT Code Reimbursement*
Single spirometry 94010 $32.82
Pre-post spirometry 94060 $57.71
Pulmonary stress test simple 94620 $71.77
Medication administrationbronchodilator supply separate
94640 $13.34
Demonstration / instruction 94664 $14.79
Smoking Cessation <8x/ yr 99406 $12.98
Equipment Cost
Office spirometer $1,000 – 2,500
*Reimbursement based upon Medicare payments 2009

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 46/50
Estimated Return on Investment
Tests /week (#) Reimbursement/year* ROI $1,995 in weeks
4 $6,864 15
6 $10, 296 10
8 $13,728 710 $17,160 6
15 $25,740 4
20 $34,320 3
25 $42,900 2
*Based upon CPT code 94010

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 47/50
References
• AARC Clinical Practice Guideline. Delivery of aerosols to the upper airway.Respir Care 1996;41(7):629-36
• Belfer M. Office management of COPD in primary care: A 2009 clinicalupdate. Postgraduate Medicine 2009;121(4):82-90.
• Blain EA, Craig TJ. The use of spirometry in a primary care setting. Int JGen Med. 2009; 2: 183 –186.
• Chavez,P.C. and Shokar,N.K. Diagnosis and management of chronicobstructive pulmonary disease (COPD) in a primary care clinic. COPD 2009;6(6): 446-451.
• Enright P. The use and abuse of office spirometry. Prim Care Respir J.2008 Dec;17(4):238-42.
• Fletcher C, Peto R. The natural history of chronic airflow obstruction. BrMed J. 1977;1(6077):1645-1648.
• Ferguson GT et al. Office spirometry for lung health assessment in adults: Aconsensus statement from the National Lung Health Education Program.Respiratory Care 2000;45(5) 513-30

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 48/50
References (continued)
• Grossman E, Sherman S. Telling smokers their "lung age" promotedsuccessful smoking cessation. Evid Based Med. 2008;13(4):104
• Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference valuesfrom a sample of the general US population. Am J Respir Crit Care Med1999;159:179 –187
• History Diagnosis Spirometerhttp://www.umanitoba.ca/libraries/units/health/images/HistoryDiagnosisSpir ometer.jpg
• Jing JY. Should FEV1/FEV6 replace FEV1/FVC ratio to detect airwayobstruction? A metaanalysis. Chest. 2009 Apr;135(4):991-8.
• Johannessen A, et al. Post-bronchodilator spirometry reference values inadults and implications for disease management. Am J Respir Crit CareMed 2006; 173(12):1316-25.
• Kaminsky DA, Marcy TW, Bachand M, Irvin CG. Knowledge and use ofoffice spirometry for the detection of chronic obstructive pulmonary diseaseby primary care physicians. Respir Care. 2005 Dec;50(12):1639-48.
8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 49/50
• Knudson RJ, Slatin RC, Lebowitz MD, Burrows B. The maximal expiratoryflow-volume curve. Normal standards, variability, and effects of age. AmRev Respir Dis 1976;113:587 –600
• Lin KW Screening Spirometry. American Family Physician 2009;80(8) :861-2.
• Lowry, Josiah A Guide to Spirometry for Primary Care Physicians 1998Published by College of Family Physicians of Canada with BoehringerIngelheim
• MacIntyre NR, Selecky PA. Is there a role for screening spirometry? RespirCare. 2010;55(1):35-42 [Review].
• National Committee on Quality Assurance. 2009 Healthcare EffectivenessData and Information Set (HEDIS) performance measures. 2010. Availableat www.ncqa.org/tabid/855/Default.aspx. Accessed August 2010.
• Parkes G, Greenhalgh T, Griffin M, Dent R. Effect on smoking quit rate oftelling patients their lung age: the Step2quit randomised controlled trial BMJ2008;336:598-600.

8/10/2019 copd spiro
http://slidepdf.com/reader/full/copd-spiro 50/50
References (continued)
• Poels PJ, olde Hartman TC, Schermer TR. Qualitative studies to explorebarriers to spirometry use: a breath of fresh air? Respir Care. 2006Jul;51(7):768.
• Rennard S, Vestbo J. COPD: The Dangerous underestimate of 15%. Lancet2006; 367, 1216-1219.
• Spann SJ. Impact of spirometry on the management of chronic obstructiveairway disease. J Fam Pract. 1983 Feb;16(2):271-5.
• Spirometer Review Process (SRP) – Revised.http://www.nlhep.org/spirometer-review-process.html. Accessed, November14th, 2010.
• Wilt TJ, Niewoehner D, Kim C, et al. Use of spirometry for case finding,diagnosis, and management of chronic obstructive pulmonary disease(COPD). Evid Rep Technol Assess (Summ). 2005;(121):1-7 [Review].
• Yawn BP et al. Spirometry can be done in family physicians' offices andalters clinical decisions in management of asthma and COPD. Chest. 2007Oct;132(4):1162-8. Epub 2007 Jun 5.
Related Documents











