european journal of pharmaceutical sciences 27 ( 2 0 0 6 ) 37–43 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/ejps Contribution of lymphatic transport to the systemic exposure of orally administered moxidectin in conscious lymph duct-cannulated dogs Anne Lespine a,∗ , Guillaume Chanoit b , Alain Bousquet-Melou c , Elodie Lallemand c , Firas Mohamad Bassissi a , Michel Alvinerie a , Pierre-Louis Toutain c a INRA-UR66, Laboratoire de Pharmacologie-Toxicologie, BP 3, 31931 Toulouse Cedex 9, France b Unit´ e Chirurgie et Anesth´ esiologie, Ecole V´ et´ erinaire de Lyon, 1 Avenue Bourgelat 69280 Marcy l ´ etoile, France c UMR 181, Physiopathologie et Toxicologie Exp´ erimentales INRA/ENVT, 23 Chemin des Capelles, 31076 Toulouse, France article info Article history: Received 18 May 2005 Received in revised form 20 July 2005 Accepted 5 August 2005 Available online 29 September 2005 Keywords: Macrocyclic lactones Moxidectin Lymph duct-cannulated dogs Lymphatic transport Intestinal absorption Lipids Bioavailability abstract Moxidectin, a macrocyclic lactone (ML), is a potent parasiticide widely used in veterinary medicine and currently under development for use in humans. The contribution of the lymphatic route to the intestinal absorption and transport of moxidectin to the systemic cir- culation was evaluated in lymph duct-cannulated dogs. Beagle dogs were operated for lymph duct cannulation and were orally dosed with 38 g of corn oil and moxidectin (0.2 mg/kg, n = 3). The lymph and plasma were collected over 24 h and moxidectin and triglyceride concentra- tions were measured. Similarly, control dogs (n = 5) were dosed orally with moxidectin and oil and subsequently with moxidectin intravenously. Pharmacokinetic parameters were calcu- lated for moxidectin in the plasma of the dogs. Moxidectin readily accumulated in the lymph and reached a plateau 8 h post-administration, paralleling triglyceride appearance. The per- centage of moxidectin recovered in lymph was 22 ± 3% of the total administered dose with 92% being associated with triglyceride-rich particles. The systemic bioavailability of oral moxidectin coadministered with lipid was only 40% in the lymph duct-cannulated dogs compared with 71% in the controls. Our data clearly indicate that the lymphatic transport process contributes significantly to the post-prandial intestinal absorption of moxidectin and subsequently to its systemic bioavailability. The lymphatic transport of moxidectin offers potential strategies based on lipid formulations to improve the bioavailability of MLs when administered orally. © 2005 Elsevier B.V. All rights reserved. 1. Introduction The macrocyclic lactones (MLs) are the most potent parasiti- cides used worldwide for the treatment of both internal and external parasites in animals (McKellar and Benchaoui, 1996). The first to be commercialized ivermectin, a semi-synthetic derivative of the natural product avermectin B1 widely used in ∗ Corresponding author. Tel.: +33 5 61285387; fax: +33 5 61285310. E-mail address: [email protected] (A. Lespine). veterinary medicine, is also used in humans for the treatment of onchocerciasis, lymphatic filariasis and scabies (Molyneux et al., 2003; Dourmishev et al., 1998). Moxidectin is a member of the milbemycin family later registered for several veterinary indications including canine heartworm and gastrointestinal parasites in livestock, and is currently under development for use in humans (Cotreau et al., 2003). 0928-0987/$ – see front matter © 2005 Elsevier B.V. All rights reserved. doi:10.1016/j.ejps.2005.08.003

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 7 ( 2 0 0 6 ) 37–43
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate /e jps
Contribution of lymphatic transport to the systemicexposure of orally administered moxidectin in consciouslymph duct-cannulated dogs
Anne Lespinea,∗, Guillaume Chanoitb, Alain Bousquet-Melouc, Elodie Lallemandc,Firas Mohamad Bassissia, Michel Alvineriea, Pierre-Louis Toutainc
a INRA-UR66, Laboratoire de Pharmacologie-Toxicologie, BP 3, 31931 Toulouse Cedex 9, Franceb Unite Chirurgie et Anesthesiologie, Ecole Veterinaire de Lyon, 1 Avenue Bourgelat 69280 Marcy l′etoile, Francec UMR 181, Physiopathologie et Toxicologie Experimentales INRA/ENVT, 23 Chemin des Capelles, 31076 Toulouse, France
a
A
R
R
A
A
K
M
M
L
L
I
L
B
1
TceTd
0d
r t i c l e i n f o
rticle history:
eceived 18 May 2005
eceived in revised form 20 July 2005
ccepted 5 August 2005
vailable online 29 September 2005
eywords:
acrocyclic lactones
oxidectin
ymph duct-cannulated dogs
ymphatic transport
ntestinal absorption
ipids
ioavailability
a b s t r a c t
Moxidectin, a macrocyclic lactone (ML), is a potent parasiticide widely used in veterinary
medicine and currently under development for use in humans. The contribution of the
lymphatic route to the intestinal absorption and transport of moxidectin to the systemic cir-
culation was evaluated in lymph duct-cannulated dogs. Beagle dogs were operated for lymph
duct cannulation and were orally dosed with 38 g of corn oil and moxidectin (0.2 mg/kg, n = 3).
The lymph and plasma were collected over 24 h and moxidectin and triglyceride concentra-
tions were measured. Similarly, control dogs (n = 5) were dosed orally with moxidectin and oil
and subsequently with moxidectin intravenously. Pharmacokinetic parameters were calcu-
lated for moxidectin in the plasma of the dogs. Moxidectin readily accumulated in the lymph
and reached a plateau 8 h post-administration, paralleling triglyceride appearance. The per-
centage of moxidectin recovered in lymph was 22 ± 3% of the total administered dose with
92% being associated with triglyceride-rich particles. The systemic bioavailability of oral
moxidectin coadministered with lipid was only 40% in the lymph duct-cannulated dogs
compared with 71% in the controls. Our data clearly indicate that the lymphatic transport
process contributes significantly to the post-prandial intestinal absorption of moxidectin
and subsequently to its systemic bioavailability. The lymphatic transport of moxidectin
offers potential strategies based on lipid formulations to improve the bioavailability of MLs
when administered orally.
© 2005 Elsevier B.V. All rights reserved.
. Introduction
he macrocyclic lactones (MLs) are the most potent parasiti-ides used worldwide for the treatment of both internal andxternal parasites in animals (McKellar and Benchaoui, 1996).he first to be commercialized ivermectin, a semi-syntheticerivative of the natural product avermectin B1 widely used in
∗ Corresponding author. Tel.: +33 5 61285387; fax: +33 5 61285310.E-mail address: [email protected] (A. Lespine).
veterinary medicine, is also used in humans for the treatmentof onchocerciasis, lymphatic filariasis and scabies (Molyneuxet al., 2003; Dourmishev et al., 1998). Moxidectin is a memberof the milbemycin family later registered for several veterinaryindications including canine heartworm and gastrointestinalparasites in livestock, and is currently under development foruse in humans (Cotreau et al., 2003).
928-0987/$ – see front matter © 2005 Elsevier B.V. All rights reserved.oi:10.1016/j.ejps.2005.08.003

38 e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 7 ( 2 0 0 6 ) 37–43
The antiparasitic activity of the MLs is related to the pres-ence of an effective concentration for a suitable length oftime in the systemic circulation. Strategies aimed at improvingthe drug exposure are currently being developed to optimizeMLs’ efficacy. The development of oral formulations remainsa challenge which requires a better knowledge of the mech-anisms involved in the intestinal absorption of such drugs.The intestinal lymphatic pathway plays a pivotal role in theabsorption of dietary lipids in the post-prandial period andalso contributes, at least partly, to the absorption of lipophilicxenobiotics. Several drugs have been described that reachthe blood circulation via the lymphatic route by being incor-porated into newly synthesized triglyceride-rich lipoproteinsin the intestine (Porter and Charman, 2001). For these com-pounds the co-administration of lipid increases their systemicexposure.
MLs are highly lipophilic substances that distribute in thecirculating blood associated to the lipoproteins (Bassissi et al.,2004a). Moxidectin is characterized by a large volume of dis-tribution, an extensive elimination in milk during lactation,a remarkably long mean residence time in the host organ-ism (Hennessy and Alvinerie, 2002) influenced by adiposity(Craven et al., 2002) and an interesting long-lasting efficacyof several weeks (Kerboeuf et al., 1995). The oral adminis-tration of ivermectin or moxidectin in humans just after afatty meal leads to a substantial increase in the drug bioavail-ability (Guzzo et al., 2002; Cotreau et al., 2003). Similarly, the
The present study was conducted to evaluate the contri-bution of the lymphatic route to the intestinal absorptionand transport of moxidectin into the systemic circulation. Weused a previously developed model of conscious lymph duct-cannulated dogs to measure the intestinal lymphatic trans-port of the lipophilic drug substrate (Khoo et al., 2001). Thismodel consists in diverting, collecting and analysing the post-prandial lymph after oral drug administration. We determinedthe rate of moxidectin transport into the lymph and comparedthe pharmacokinetics of moxidectin in plasma after oral co-administration of lipid and drug in lymph duct-cannulatedand control Beagle dogs.
2. Materials and methods
2.1. Animals and surgery
The surgical procedure was performed according to thedescription by Khoo et al. (2001). Before surgery, dogs(13.5 ± 0.3 kg) were fasted overnight. Prior to anesthesia, theywere fed a fatty meal to facilitate the identification of thethoracic duct. Dogs were premedicated with an IM injectionof 0.25 mg/kg of Acepromazine (Vetranquil ND, Ceva SanteAnimale, Libourne, France). Antibiotic prophylaxis was carriedout by an i.v. injection of Cefalexine (30 mg/kg, Rilexine ND, Vir-bac, Carros, France) at the time of premedication. After 20 min,
coadministration of lipids increased by two-fold the exposureof rabbits to oral moxidectin (Bassissi et al., 2004b). Mox-idectin (Fig. 1) differs structurally from the avermectins bythe lack of the bis-oleandrosyloxy substitute attached to theC-13 of the macrocyclic ring thus conferring the moleculewith greater hydrophobicity when compared with the aver-mectins. Indeed, moxidectin has a n-octanol/water partitioncoefficient log P of 6.0, while ivermectin log P is about 3.5, witha very low water solubility of 0.006 mg/l (McKellar and Ben-chaoui, 1996). Altogether, these informations indicate thatmoxidectin is a potential candidate for lymphatic intestinaltransport.
Fig. 1 – Chemical structure of moxidectin.
anesthesia was induced with an i.v. injection of thiopental(15 mg/kg, Nesdonal ND, Merial SAS, Lyon, France).
During surgery, anesthesia was maintained by administer-ing halothane (1.5%) and oxygen (approximately 500 ml/kg)via an endotracheal tube, through a closed circuit system.Each dog received an intravenous infusion of lactated-Ringer’ssolution (11 ml/kg/h) during anesthesia and after recovery tomaintain normal hydration. Analgesia was induced by an i.v.injection of 0.1 mg/kg of morphine (Morphine Aguettant, Lyon,France) immediately after the induction of anesthesia, afterextubation and 4 h after recovery from anesthesia if necessary.The thoracic lymph duct was cannulated as followed. The dogwas in right lateral recumbency, and the duct was cannulatedat the upper neck level, after dissection of the sternocephali-cus muscle, distal to the junction of the internal and externaljugular vein where the lymph flows into the systemic circula-tion.
The cannula was heparin-coated sterile tubing (CBAS C50PU Cath 5Fr, round tip, inner diameter: 1.0 mm, outer diameter:1.7 mm; Solomon Scientific, Zevenar, The Netherlands) whichwas externalized by tunelling through the neck muscle andskin at the level of fourth cervical vertebra. During the sameintervention, another catheter was inserted into the jugularvein in the direction of the heart and was connected to thelymph external cannula. This by-pass tubing was maintainedconnected to allow a regular circulation of lymph during therecovery period. The jugular vein catheter enabled blood sam-ples to be taken throughout the experiment. The surgerytime needed for the cannulation of the lymphatic duct wasless than 3 h and the dogs were standing up within 2 h aftersurgery and were allowed to recover for 12 h. All procedureswere approved by the Institutional use and care of animalscommittee.

e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 7 ( 2 0 0 6 ) 37–43 39
2.2. Pharmacokinetics of oral moxidectin in lymphduct-cannulated dogs
After recovery, dogs were orally dosed by intragastric gav-age using a gastro-duodenal feeding tube Levin type (Vygon,France) with 38 g of corn oil. Similarly, a commercial oralformulation of moxidectin (moxidectin solution at 0.1%,Cydectine® 0.1% Fort-Dodge) was then administered intragas-tically at a dose of 0.2 mg/kg corresponding to 2.8–3.0 ml ofmoxidectin formulation. Dogs were placed in a closed cham-ber that allowed them to move and to lay down freely, whilebeing perfused with saline during the experiment. Urine andfaeces were collected. Immediately after drug administrationthe by-pass tubing was disconnected. The lymph cannula tub-ing was placed in heparinised plastic vials for lymph collectionfor 1 h collections over a 24 h period. The lymph volume wasdetermined and the samples were kept at 5–8 ◦C for analysiswithin 24 h. Blood was collected from the jugular vein catheterin heparinised tubes before treatment and 1–4, 6, 8, 10, 12, 18,24 h post-treatment. Plasma was obtained by centrifuging at1500 × g for 15 min at 7 ◦C.
2.3. Lipoprotein separation
Lipoproteins were prepared from lymph fraction collected2 h post-treatment by using a previously described method(Khoo et al., 2001) slightly modified. In brief, the lymph aliquot(diecpuf
2i
Fofc00tt12afsl03
2
Mm
derivative according to the method previously described forplasma (Alvinerie et al., 1995) and was adapted for analysisin lymph and in lipoproteins. The extraction was performedwith 1 ml of sample to which were added 0.25 ml of water and0.75 ml of acetonitrile. After mixing for 20 min, the sampleswere centrifuged at 2000 × g for 2 min and the supernatantsautomatically transferred onto Supelclean LC18 cartridges(100 mg, Supelco, Bellefonte, PA, USA) using a Benchmate IIapparatus (Zymarck, Hopkinton, MA, USA). The eluates wereevaporated to dryness and the residues dissolved in 100 �l of aN-methylimidazole (Aldrich, Milwaukee, USA) solution in ace-tonitrile (50%, v/v) and the derivatization was initiated with150 �l of a trifluoroacetic anhydride (Aldrich, Milwaukee, USA)solution in acetonitrile (33%, v/v). After completion of the reac-tion, an aliquot of the mixture (100 �l) was injected into thechromatography system. The mobile phase of acetic acid (0.2%in water)–methanol–acetonitrile (4/32/64, v/v/v) was pumpedat a flow rate of 1 ml/min through a Supelcosil C18 column,5 �m (150 mm × 4.6 mm; Supelco, Bellefonte, PA, USA) with flu-orescence detection at an excitation wavelength of 355 nmand an emission wavelength of 465 nm (FP-920, Jasco, Tokyo,Japan). The limit of quantification of the technique for the dif-ferent fluids was 0.02 ng/ml with a coefficient of variation of6.95%.
2.6. Triacylglyceride analysis
1 ml) was layered onto a sodium chloride solution (8 ml,= 1.0063 g/ml) and centrifuged at 20 000 × g for 60 min. The
nfranatant was collected and 4 ml (out of 8 ml) were lay-red onto sodium chloride solution (4 ml, d = 1.0063 g/ml) andentrifuged at 39 000 × g for 18 h. Ultracentrifugations wereerformed in a Kontron T1170 ultracentrifuge (Kontron, Italy)sing 60Ti rotor. The upper phases and infranatants collected
rom both centrifugations were analysed for moxidectin.
.4. Pharmacokinetic study of oral and i.v. moxidectinn standard (control) Beagle dogs
ive Beagle dogs (12.1 ± 1.0 kg) were fasted for 12 h. Dogs wererally dosed by intragastric gavage by using a gastro-duodenaleeding tube as described in the previous section with 38 g oforn oil. Similarly, oral formulation of moxidectin (Cydectine®
.1%, Fort-Dodge) was administered intragastically at a dose of
.2 mg/kg corresponding to 2.8–3.0 ml of moxidectin formula-ion. Plasma was collected before (0) and post-treatment athe following time: 0.5, 1, 2, 4, 8, 12, 36, 24, 36, 48, 72, 96,44,192, 240, 288, 336, 408, 480 h. After a wash out period ofmonths, the same dogs were intravenously injected throughcatheter inserted in the left cephalic vein with an injectable
ormulation of moxidectin at a dose of 0.2 mg/kg (moxidectinolution at 1%, Cydectine® 1%, Fort-Dodge). Blood was col-ected by direct venipuncture at the jugular vein level at 0,.033, 0.08, 0.25, 0.5, 1, 2, 4, 8, 12, 24, 48, 72, 96, 144, 192, 240,36, 408, 480 h.
.5. Moxidectin analysis
oxidectin was analysed by high performance liquid chro-atography (HPLC) after derivatization into a fluorescent
Triacylglycerides (TG) were measured in lymph and plasmaby the modified method of Waco (Fossati and Prencipe, 1982),using a commercial enzyme-based colorimetric assay (Triglyc-erides Reagent, ThermoTrace, Australia).
2.7. Data analysis
The data were subjected to non-compartmental analy-sis using the statistical moment approach (Perrier andMayersohn, 1982). The individual areas under the plasmaconcentration–time curve (AUC) were computed using thearithmetic trapezoidal rule from t = 0 to the last measured con-centration (AUC0–24 h) or to infinity (AUC0–infinity).
Mean residence times (MRT) were calculated from t = 0 toinfinity as follows:
MRT = AUMC0–infinity
AUC0–infinity
where AUMC0–infinity is the area under the first moment curvecalculated by using the arithmetic trapezoidal rule.
The peak plasma concentration (Cmax) and time of peakplasma concentration (Tmax) were obtained directly from theplots of plasma concentration versus time for each animal.Plasma clearances (Cltot) were calculated from the ratio of thei.v. administered dose divided by AUC0–infinity obtained for thei.v. route:
Cltot = dosei.v.
AUCi.v.
Distribution volumes (Vss) was the product of Cltot and MRT:
Vss = Cltot × MRT

40 e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 7 ( 2 0 0 6 ) 37–43
Table 1 – Triglyceride and moxidectin recoveries inlymph after oral administration of moxidectin and cornoil to lymph duct-cannulated dogs: moxidectin andtriglyceride were measured in the lymph collected fromtreated-lymph duct-cannulated dogs over a timeperiod of 24 h
Total doseadministered
(TAD)
Recoveryin lymph
(% of TAD)
Triglyceride 38 g 94 ± 3Moxidectin 2935 ± 80 �g 22 ± 3
Data are means ± S.D. of three animals.
The systemic bioavailabilities of oral moxidectin (F) were cal-culated using the ratio of the AUC0–infinity or AUC0–24 h afteroral and after i.v. treatment, corrected by the ratio of the dosesadministered.
The arithmetic means and standard deviations (S.D.) of thedifferent parameters were calculated. Statistical comparisonswere obtained by using the PLSD Fischer test performed withStatview software (Abacus Concepts, Berkeley, CA, USA). Avalue of p < 0.05 was considered significant.
3. Results
Corn oil was administered just before the drug administrationin order to stimulate intestinal lymph secretion. After treat-ment, the lymph flow started immediately and lymph was col-lected throughout the experiment. The integrity of the lymphduct cannulation was evaluated by determining the lymphflow rate, the systemic plasma triglyceride concentration pro-file and the cumulative quantity of triglyceride transported inthe lymph. According to these criteria, data from three dogscould be included in our experiment. Two dogs were excludedbecause of the rapid decrease of the lymph flow rate, due tothe loss of the cannula from the lymphatic duct. The lymphflow rate determined for the other three dogs increased rapidlyand stayed around 40–70 ml/h for the first 8–10 h of the exper-iment. It then slowly decreased to average 20 ml/h for the rest
Fig. 2 – Cumulative lymphatic transport of moxidectin inlymph duct-cannulated dogs: moxidectin was measuredover 24 h in the lymph of thoracic lymph duct-cannulateddogs. Values are the amount of moxidectin recovered inlymph expressed as the percent of the total administereddose (TAD, means ± S.D., n = 3).
The percentage of moxidectin measured in lymph corre-sponded to 22 ± 3% of the total administered dose (Table 1).
The rate of triglyceride and moxidectin transport intolymph is shown in Fig. 3. There was a close parallel betweenthe kinetics of moxidectin and lipid appearance in the lymph.For both molecules, the rate of transport into the lymph wasmaximal from 2.5 to 8 h averaging 3 g/h for triglycerides and60 �g/h for moxidectin. After 8 h, both rates decreased simul-taneously and rapidly.
A lymph aliquot, collected 2 h post-treatment, was submit-ted to two successive ultracentrifugations in order to isolatetriglyceride-containing particles and to determine the mox-idectin distribution. Most of the moxidectin present in lymph(92.7 ± 3.4%) was measured in the cumulated floating fractionscontaining triglyceride-rich particles.
In order to compare moxidectin exposure in lymph ductcannulated and in control dogs, five non-cannulated Bea-gle dogs (controls) were dosed by intragastric gavage with38 g of corn oil and 0.2 mg/kg moxidectin. Two months later,
of the experiment. The total volume of lymph collected withinthe first 12 h was 30–33 ml/kg.The amount of triglyceride recovered in lymph reflects the
mass of ingested lipid and was a good marker of the perfor-mance of lymphatic route diversion. During the experiment,most of the ingested triglyceride was recovered in the col-lected lymph (94 ± 3%, Table 1). Triglyceride concentration inlymph duct-cannulated dog plasma never exceeded 0.6 mMall along the experiment, that is a typical fasted plasmatriglyceride concentration. Indeed, the triglyceride plasmaconcentration measured in fasted control non-cannulateddogs was 0.54 ± 0.08 mM, while 2 h after oral lipid administra-tion the triglyceride concentration was significantly increased(1.82 ± 0.21 mM, p < 0.001, n = 5).
The cumulative transport of moxidectin into the lymphafter lipid and drug administration was followed over a timeperiod of 24 h (Fig. 2). Moxidectin readily accumulated in thelymph and reached a plateau 10 h post-administration. By thistime, most of the drug transport into lymph had been reached.
Fig. 3 – Rate of lymphatic transport of moxidectin (�) andtriglycerides (�) in lymph duct-cannulated dogs:moxidectin and triglyceride were measured in lymph oflymph duct-cannulated dogs over 24 h after treatment.Values are means ± S.D., n = 3.
e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 7 ( 2 0 0 6 ) 37–43 41
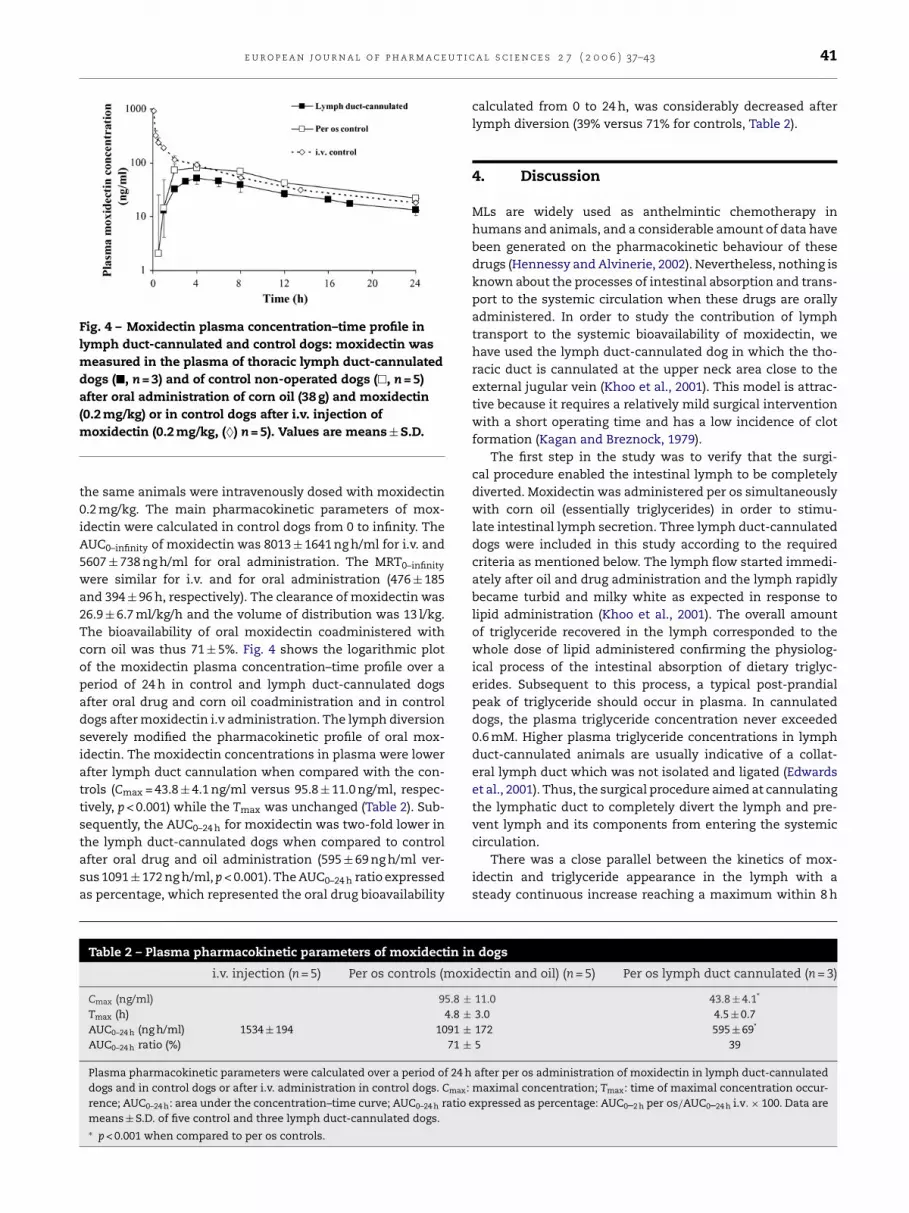
Fig. 4 – Moxidectin plasma concentration–time profile inlymph duct-cannulated and control dogs: moxidectin wasmeasured in the plasma of thoracic lymph duct-cannulateddogs (�, n = 3) and of control non-operated dogs (�, n = 5)after oral administration of corn oil (38 g) and moxidectin(0.2 mg/kg) or in control dogs after i.v. injection ofmoxidectin (0.2 mg/kg, (♦) n = 5). Values are means ± S.D.
the same animals were intravenously dosed with moxidectin0.2 mg/kg. The main pharmacokinetic parameters of mox-idectin were calculated in control dogs from 0 to infinity. TheAUC0–infinity of moxidectin was 8013 ± 1641 ng h/ml for i.v. and5607 ± 738 ng h/ml for oral administration. The MRT0–infinity
were similar for i.v. and for oral administration (476 ± 185and 394 ± 96 h, respectively). The clearance of moxidectin was26.9 ± 6.7 ml/kg/h and the volume of distribution was 13 l/kg.The bioavailability of oral moxidectin coadministered withcorn oil was thus 71 ± 5%. Fig. 4 shows the logarithmic plotof the moxidectin plasma concentration–time profile over aperiod of 24 h in control and lymph duct-cannulated dogsafter oral drug and corn oil coadministration and in controldogs after moxidectin i.v administration. The lymph diversionseverely modified the pharmacokinetic profile of oral mox-idectin. The moxidectin concentrations in plasma were lowerafter lymph duct cannulation when compared with the con-trols (Cmax = 43.8 ± 4.1 ng/ml versus 95.8 ± 11.0 ng/ml, respec-tively, p < 0.001) while the Tmax was unchanged (Table 2). Sub-sequently, the AUC0–24 h for moxidectin was two-fold lower inthe lymph duct-cannulated dogs when compared to controlafter oral drug and oil administration (595 ± 69 ng h/ml ver-sus 1091 ± 172 ng h/ml, p < 0.001). The AUC0–24 h ratio expressedas percentage, which represented the oral drug bioavailability
calculated from 0 to 24 h, was considerably decreased afterlymph diversion (39% versus 71% for controls, Table 2).
4. Discussion
MLs are widely used as anthelmintic chemotherapy inhumans and animals, and a considerable amount of data havebeen generated on the pharmacokinetic behaviour of thesedrugs (Hennessy and Alvinerie, 2002). Nevertheless, nothing isknown about the processes of intestinal absorption and trans-port to the systemic circulation when these drugs are orallyadministered. In order to study the contribution of lymphtransport to the systemic bioavailability of moxidectin, wehave used the lymph duct-cannulated dog in which the tho-racic duct is cannulated at the upper neck area close to theexternal jugular vein (Khoo et al., 2001). This model is attrac-tive because it requires a relatively mild surgical interventionwith a short operating time and has a low incidence of clotformation (Kagan and Breznock, 1979).
The first step in the study was to verify that the surgi-cal procedure enabled the intestinal lymph to be completelydiverted. Moxidectin was administered per os simultaneouslywith corn oil (essentially triglycerides) in order to stimu-late intestinal lymph secretion. Three lymph duct-cannulateddogs were included in this study according to the requiredcriteria as mentioned below. The lymph flow started immedi-
Table 2 – Plasma pharmacokinetic parameters of moxidectin in
oxi
5.8 ±4.8 ±91 ±71 ±
24 h
max:atio e
i.v. injection (n = 5) Per os controls (m
Cmax (ng/ml) 9Tmax (h)AUC0–24 h (ng h/ml) 1534 ± 194 10AUC0–24 h ratio (%)
Plasma pharmacokinetic parameters were calculated over a period ofdogs and in control dogs or after i.v. administration in control dogs. Crence; AUC0–24 h: area under the concentration–time curve; AUC0–24 h rmeans ± S.D. of five control and three lymph duct-cannulated dogs.∗ p < 0.001 when compared to per os controls.
ately after oil and drug administration and the lymph rapidlybecame turbid and milky white as expected in response tolipid administration (Khoo et al., 2001). The overall amountof triglyceride recovered in the lymph corresponded to thewhole dose of lipid administered confirming the physiolog-ical process of the intestinal absorption of dietary triglyc-erides. Subsequent to this process, a typical post-prandialpeak of triglyceride should occur in plasma. In cannulateddogs, the plasma triglyceride concentration never exceeded0.6 mM. Higher plasma triglyceride concentrations in lymphduct-cannulated animals are usually indicative of a collat-eral lymph duct which was not isolated and ligated (Edwardset al., 2001). Thus, the surgical procedure aimed at cannulatingthe lymphatic duct to completely divert the lymph and pre-vent lymph and its components from entering the systemiccirculation.
There was a close parallel between the kinetics of mox-idectin and triglyceride appearance in the lymph with asteady continuous increase reaching a maximum within 8 h
dogs
dectin and oil) (n = 5) Per os lymph duct cannulated (n = 3)
11.0 43.8 ± 4.1*
3.0 4.5 ± 0.7172 595 ± 69*
5 39
after per os administration of moxidectin in lymph duct-cannulatedmaximal concentration; Tmax: time of maximal concentration occur-xpressed as percentage: AUC0–2 h per os/AUC0–24 h i.v. × 100. Data are

42 e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 7 ( 2 0 0 6 ) 37–43
post-gavage. This strongly suggests a similar pathway ofintestinal absorption for both molecules. The cumulativeamount of moxidectin recovered in the intestinal lymph whenstimulated by lipid ingestion represented 22 ± 3% of the totalorally administrated dose in our model. The majority of thedrug was associated with the triglyceride-rich lipoproteins(93 ± 3%) present in the lymph. These results suggest thatduring intestinal absorption, a part of moxidectin is incorpo-rated in the enterocytes into newly synthesized chylomicronsbefore being secreted into lymph and transported into thesystemic circulation. Once in the circulation, the drug maybe transported to the liver to be further secreted into bloodcirculation in association with hepatic lipoproteins or it maybe exchanged between lipoproteins. Indeed, in the systemiccirculation moxidectin is associated with lipoproteins, with85% recovered in the high-density lipoproteins (Bassissi et al.,2004a) which originate mainly from the liver.
A pharmacokinetic study was thus performed over a periodof 20 days with non-cannulated Beagle dogs reproducingclosely the experimental conditions used for cannulated dogsregarding dog breed, weight, maintenance and oral coadmin-istration of moxidectin with corn oil. The moxidectin clear-ance of 27 ml/kg/min was in the range of that reported formoxidectin in cattle (Bousquet-Melou et al., 2004). Such a lowclearance with respect to both the hepatic and renal bloodflows in dogs (about 30 and 20 ml/kg/min, respectively) reflectsthe poor hepatic biotransformation and the very low elimi-
that the administration of oral moxidectin together with afatty meal or a lipid-based formulation substantially improvesthe systemic concentration of the drug (Cotreau et al., 2003;Bassissi et al., 2004b).
Such information enables several strategies to be envisagedfor further improving the oral bioavailability. By improving thedigestibility of lipids (O’Driscoll, 2002; Holm et al., 2003) or byusing excipient generally incorporated in lipid-based formu-lations, we might be able to increase the lymphatic transportof the drug. Nevertheless, a fatty meal is a good enhancer oflymph secretion and certainly remains the most practical wayof augmenting oral drug absorption.
In this study we have used moxidectin because of its higherlipophily when compared with other MLs, probably leadingto a higher rate of intestinal lymphatic absorption. Neverthe-less, previous data showing that ivermectin bioavailability isincreased after a fatty meal intake (Guzzo et al., 2002), suggestthat also ivermectin and probably other MLs are transported bythe lymphatic route. The precise rate of such transport needsto be determined for each ML.
These data clearly indicate that lymphatic transport is acontributing process to the post-prandial oral bioavailabil-ity profile of moxidectin at least in monogastric animals.Such information will help in defining new strategies aimedat increasing the intestinal absorption of MLs and improv-ing their systemic bioavailability when orally administered.Indeed, the administration of the drug with a fatty meal or
r
nation by the kidney reported for MLs. Moreover, it can bededuced from clearance values that hepatic first-pass effectafter oral administration is negligible and is not a limiting fac-tor for oral bioavailability. The long MRT of more than 2 weeksand the large volume of distribution (Vss) are related to thelong persistence of the molecule in the organism and can beassociated to its high lipophilicity. The bioavailability of theoral moxidectin coadministered with lipids was rather high(71%).
In order to evaluate the contribution of the lymphatic routeto the entry of moxidectin into the systemic circulation, themain pharmacokinetic parameters were calculated in non-cannulated dogs over a period of 24 h and compared with thosefrom lymph duct-cannulated dogs. Subsequent to the lymphdiversion, the concentrations of moxidectin in the systemiccirculation were lower with a two-fold reduction in the Cmax
and in the AUC0–24 h when compared to the controls. The drugbioavailability over the first 24 h was only 39% in the lymphduct-cannulated animals compared with 71% in the controls(calculated with the AUC0–24 h). These data confirm that a sub-stantial part of the drug had by-passed the systemic circu-lation and was recovered in the diverted lymph. Absorptioninto the intestinal lymph should thus contribute to around30% of the systemic bioavailable moxidectin. A bioavailabil-ity of 40% reported in the horse was to our knowledge theonly bioavailability reported for oral moxidectin (Afzal et al.,1997). We suggest that the high bioavailability observed in con-trol dogs in our experimental conditions was partly due to theinfluence of lipid coadministration on the drug absorption.
Our data clearly indicate that the lymphatic transportprocess contributes notably to the post-prandial intestinalabsorption of moxidectin and subsequently to its systemicbioavailability and support previous observations showing
new lipid-based formulations would be of considerable bene-fit to the veterinary and clinical use of MLs.
e f e r e n c e s
Afzal, J., Burke, A.B., Batten, P.L., DeLay, R.L., Miller, P., 1997.Moxidectin: metabolic fate and blood pharmacokinetics of14C-labelled moxidectin in horses. J. Agric. Food Chem. 45,3627–3633.
Alvinerie, M., Sutra, J.F., Badri, M., Galtier, P., 1995.Determination of moxidectin in plasma byhigh-performance liquid chromatography with automatedsolid-phase extraction and fluorescence detection. J.Chromatogr. B: Biomed. Appl. 674, 119–124.
Bassissi, M.F., Alvinerie, M., Lespine, A., 2004a. Macrocycliclactones: distribution in plasma lipoproteins of severalanimal species including humans. Comp. Biochem. Physiol.C: Toxicol. Pharmacol. 138, 437–444.
Bassissi, M.F., Lespine, A., Alvinerie, M., 2004b. Enhancement oforal moxidectin bioavailability in rabbits by lipidco-administration. Parasitol. Res. 94 (3), 188–192.
Bousquet-Melou, A., Mercadier, S., Alvinerie, M., Toutain, P.L.,2004. Endectocide exchanges between grazing cattle afterpour-on administration of doramectin, ivermectin andmoxidectin. Int. J. Parasitol. 34, 1299–1307.
Cotreau, M.M., Warren, S., Ryan, J.L., Fleckenstein, L., Vanapalli,S.R., Brown, K.R., Rock, D., Chen, C.Y., Schwertschlag, U.S.,2003. The antiparasitic moxidectin: safety, tolerability, andpharmacokinetics in humans. J. Clin. Pharmacol. 43,1108–1115.
Craven, J., Bjorn, H., Hennessy, D.R., Friis, C., 2002. The effectsof body composition on the pharmacokinetics ofsubcutaneously injected ivermectin and moxidectin in pigs.J. Vet. Pharmacol. Ther. 25, 227–232.

e u r o p e a n j o u r n a l o f p h a r m a c e u t i c a l s c i e n c e s 2 7 ( 2 0 0 6 ) 37–43 43
Dourmishev, A., Serafimova, D., Dourmishev, L., 1998. Efficacyand tolerance of oral ivermectin in scabies. J. Eur. Acad.Dermatol. Venereol. 11, 247–251.
Edwards, G.A., Porter, C.J., Caliph, S.M., Khoo, S.M., Charman,W.N., 2001. Animal models for the study of intestinallymphatic drug transport. Adv. Drug Deliv. Rev. 50, 45–60.
Fossati, P., Prencipe, L., 1982. Serum triglycerides determinedcolorimetrically with an enzyme that produces hydrogenperoxide. Clin. Chem. 28, 2077–2080.
Guzzo, C.A., Furtek, C.I., Porras, A.G., Chen, C., Tipping, R.,Clineschmidt, C.M., Sciberras, D.G., Hsieh, J.Y., Lasseter, K.C.,2002. Safety, tolerability, and pharmacokinetics of escalatinghigh doses of ivermectin in healthy adult subjects. J. Clin.Pharmacol. 42, 1122–1133.
Hennessy, D.R., Alvinerie, M.R., 2002. Pharmacocinetics of themacrocyclic lactones: conventional wisdom and newparadigms. In: Vercruysse, J., Rew, R.S. (Eds.), MacrocyclicLactones in Antiparasitic Therapy. CAB International, pp.97–123.
Holm, R., Porter, C.J., Edwards, G.A., Mullertz, A., Kristensen,H.G., Charman, W.N., 2003. Examination of oral absorptionand lymphatic transport of halofantrine in atriple-cannulated canine model after administration inself-microemulsifying drug delivery systems (SMEDDS)containing structured triglycerides. Eur. J. Pharm. Sci. 20,91–97.
Kagan, K.G., Breznock, E.M., 1979. Variations in the caninethoracic duct system and the effects of surgical occlusiondemonstrated by rapid aqueous lymphography, using anintestinal lymphatic trunk. Am. J. Vet. Res. 40, 948–958.
Kerboeuf, D., Hubert, J., Cardinaud, B., Blond-Riou, F., 1995. Thepersistence of the efficacy of injectable or oral moxidectinagainst Teladorsagia, Haemonchus and Trichostrongylusspecies in experimentally infected sheep. Vet. Rec. 137,399–401.
Khoo, S.M., Edwards, G.A., Porter, C.J., Charman, W.N., 2001. Aconscious dog model for assessing the absorption,enterocyte-based metabolism, and intestinal lymphatictransport of halofantrine. J. Pharm. Sci. 90, 1599–1607.
McKellar, Q.A., Benchaoui, H.A., 1996. Avermectins andmilbemycins. J. Vet. Pharmacol. Ther. 19, 331–351.
Molyneux, D.H., Bradley, M., Hoerauf, A., Kyelem, D., Taylor,M.J., 2003. Mass drug treatment for lymphatic filariasis andonchocerciasis. Trends Parasitol. 19, 516–522.
O’Driscoll, C.M., 2002. Lipid-based formulations for intestinallymphatic delivery. Eur. J. Pharm. Sci. 15, 405–415.
Perrier, D., Mayersohn, M., 1982. Noncompartmentaldetermination of the steady-state volume of distribution forany mode of administration. J. Pharm. Sci. 71, 372–373.
Porter, C.J., Charman, W.N., 2001. Intestinal lymphatic drugtransport: an update. Adv. Drug Deliv. Rev. 50, 61–80.
Related Documents











