Contrast Induced Nephropathy: Contrast Induced Nephropathy: Predictors, Prevention, and Predictors, Prevention, and Management Management Columbia University Medical Center Columbia University Medical Center Cardiovascular Research Foundation Cardiovascular Research Foundation Roxana Mehran, MD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Contrast Induced Nephropathy: Contrast Induced Nephropathy: Predictors, Prevention, and Predictors, Prevention, and
Management Management
Columbia University Medical CenterColumbia University Medical CenterCardiovascular Research FoundationCardiovascular Research Foundation
Roxana Mehran, MD

Disclosures:Disclosures:Research Grant to CRF: Tyco, Research Grant to CRF: Tyco, GuerbertGuerbert
Consultant/ Advisory Board:Consultant/ Advisory Board:FlowMedicaFlowMedica
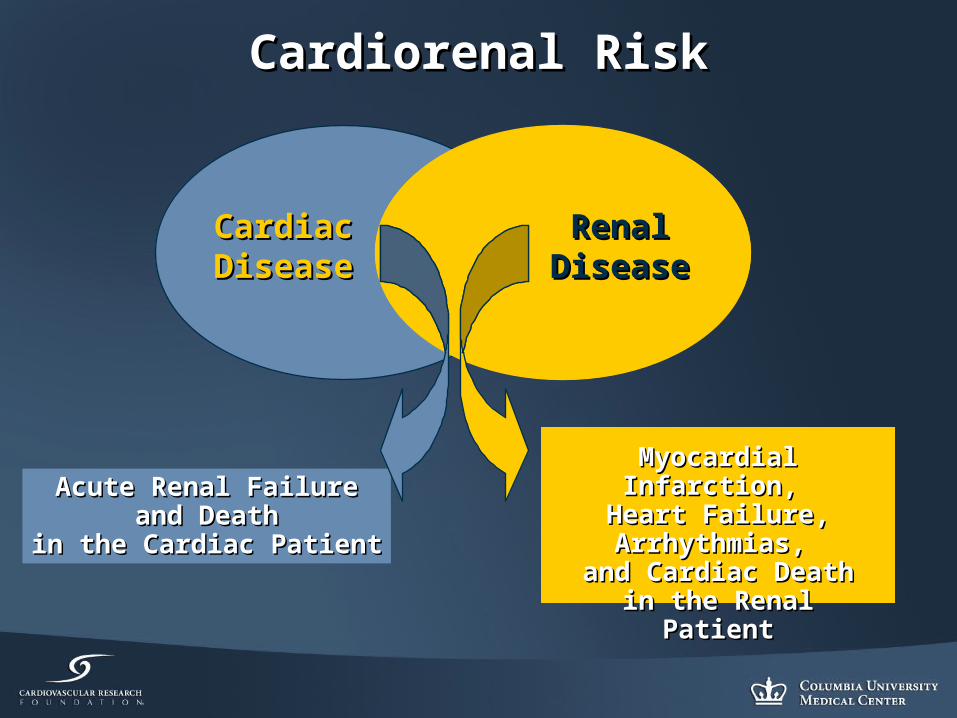
Cardiorenal RiskCardiorenal Risk
CardiacCardiacDiseaseDisease
RenalRenalDiseaseDisease
Acute Renal FailureAcute Renal Failureand Deathand Death
in the Cardiac Patientin the Cardiac Patient
Myocardial Infarction, Myocardial Infarction, Heart Failure, Heart Failure, Arrhythmias, Arrhythmias,
and Cardiac Death in and Cardiac Death in the Renal Patientthe Renal Patient

How to Assess Renal Function?How to Assess Renal Function?
Abbreviated Modification of Diet in Renal Disease equations (MDRD) equation:
eGFR, ml/min/1.73 m2= 186 x (Serum Creatinine [mg/dL]) -1.154 x (Age-0.203x (0.742 if female) x (1.210 if African American)
(140- age) x Body Weight [kg]* Creatinine Clearance, ml/min =
* Multiple by 0.8 in female
Cockcroft-Gault equation:
Serum Creatinine mg/dL] x 72

Predictors of All-Cause Mortality Predictors of All-Cause Mortality to 7 Years BARI Trial + Registryto 7 Years BARI Trial + Registry
Szczech L. et al., Szczech L. et al., CirculationCirculation 2002; 105:2253-8. 2002; 105:2253-8.
RRRR 95% CI95% CI PP
CKD (baseline Cr > 1.5 mg/dl)CKD (baseline Cr > 1.5 mg/dl) 2.312.31 1.63-3.281.63-3.28 <0.001<0.001
Sex, female vs. maleSex, female vs. male 0.910.91 0.75-1.100.75-1.10 0.320.32
Race, black vs. non-blackRace, black vs. non-black 1.401.40 1.04-1.891.04-1.89 0.0280.028
Age, yAge, y 1.051.05 1.04-1.061.04-1.06 <0.001<0.001
Diabetes mellitusDiabetes mellitus
Oral hypoglycemicsOral hypoglycemics 1.631.63 1.29-2.061.29-2.06 <0.001<0.001
InsulinInsulin 1.801.80 1.26-2.581.26-2.58 <0.001<0.001
PTCS vs. CABGPTCS vs. CABG 1.041.04 0.87-1.250.87-1.25 0.670.67
Interaction between PTCA and Interaction between PTCA and insulin-treated diabeticsinsulin-treated diabetics
1.731.73 1.11-2.691.11-2.69 0.020.02
Smoking historySmoking history
Prior tobacco usePrior tobacco use 1.301.30 1.06-1.591.06-1.59 0.010.01
Tobacco use at baselineTobacco use at baseline 1.821.82 1.42-2.331.42-2.33 <0.001<0.001

Risk Factors for CINRisk Factors for CIN
Patient-related Risk FactorsPatient-related Risk Factors
• Renal insufficiencyRenal insufficiency
• Diabetes mellitus withDiabetes mellitus withrenal insufficiencyrenal insufficiency
• AgeAge
• Volume depletionVolume depletion
• HypotensionHypotension
• Low cardiac outputLow cardiac output
• Class IV CHFClass IV CHF
• Other nephrotoxinsOther nephrotoxins
• Renal transplantRenal transplant
• Hypoalbuminemia (<35 g/l)Hypoalbuminemia (<35 g/l)
Procedure-related Risk FactorsProcedure-related Risk Factors
• Multiple contrast media Multiple contrast media injection within 72 hrsinjection within 72 hrs
• Intra-arterial injection siteIntra-arterial injection site
• High volume of contrast mediaHigh volume of contrast media
• High osmolality of contrast High osmolality of contrast mediamedia

RiskRiskScoreScore
RiskRiskof CINof CIN
Risk ofRisk of
DialysisDialysis
≤ ≤ 55 7.5%7.5% 0.04%0.04%
6 to 106 to 10 14.0%14.0% 0.12%0.12%
11 to 11 to 1616 26.1%26.1% 1.09%1.09%
≥ ≥ 1616 57.3%57.3% 12.6%12.6%
Mehran et al. JACC 2004;44:1393-1399.
Hypotension
IABP
CHF
Age >75 years
Anemia
Diabetes
Contrast media volume
Risk Factors
5
5
5
4
3
3
Integer Score
1 for each 100 cc3
Scheme to Define CIN Risk ScoreScheme to Define CIN Risk Score
Serum creatinine > 1.5mg/dl 4
eGFR <60ml/min/1.73 m2
2 for 40 – 604 for 20 – 40
6 for < 20eGFR < 60ml/min/1.73 m2 =186 x (SCr)-1.154 x (Age)-0.203
X (0.742 if female) x (1.210 if African American)
Calculate
OR

Prognostic significance of the proposed risk score for CIN extended to prediction of 1-year mortality. (Red bars = development dataset; blue bars =
validation dataset.)
CIN Risk Score & 1-year MortalityCIN Risk Score & 1-year Mortality
31.2 33.3
15.5
5.51.9 2.0
5.7
13.5
0
5
10
15
20
25
30
35
Low Moderate High Very High
1-y
ea
r m
ort
alit
y
31.2 33.3
15.5
5.51.9 2.0
5.7
13.5
0
5
10
15
20
25
30
35
Low Moderate High Very High
1-y
ea
r m
ort
alit
y
Risk Groups:Risk Score: ≤5 6 to 10 11 to 15 ≥16
Mehran et al. JACC 2004;44:1393-1399.

Preventive TrialsPreventive Trials
HydrationHydration

Optimal Hydration RegimenOptimal Hydration Regimen
Mueller et al Mueller et al Arch Intern MedArch Intern Med 2002 2002
1937 Patients Screened
317 Ineligible or No Consent
685 for Primary End Point Analysis
698 for Primary End Point Analysis
1620 Randomized
809 Received 0.9% Saline
124 Excluded From Primary End Point Analysis
Repeat Catheterization (n=78)Incomplete Data (n=46)
811 Received 0.45% Sodium Chloride
113 Excluded From Primary End Point Analysis
Repeat Catheterization (n=59)Incomplete Data (n=53)Bypass Grafting (n=1)

Optimal HydrationOptimal Hydration0.9% NS vs 0.45% NS0.9% NS vs 0.45% NS
P=.35P=.35
0
1
2
3
CN Mortality Vascular
Inc
ide
nc
e,
%
0.9% Saline0.45% Sodium Chloride
P=.93P=.93
P=.04P=.04
Mueller et al Mueller et al Arch Intern MedArch Intern Med 2002 2002

Prevention of CIN with Prevention of CIN with Sodium BicarbonateSodium Bicarbonate
Merten GJ et al. Merten GJ et al. JAMAJAMA, 2004;291:2328-2334, 2004;291:2328-2334
Patients With Baseline Serum Creatinine >1.8 mg/dlPatients With Baseline Serum Creatinine >1.8 mg/dlwho Underwent Contrast Exposure (Iopamidol in All) who Underwent Contrast Exposure (Iopamidol in All)
N=137N=137
Sodium Chloride Sodium Chloride Hydration (154 mEq/L of Hydration (154 mEq/L of
Sodium Chloride)Sodium Chloride)N=68N=68
Sodium Bicarbonate Sodium Bicarbonate Hydration (154 mEq/L of Hydration (154 mEq/L of
Sodium Bicarbonate)Sodium Bicarbonate)N=69N=69
Primary endpoint: increase in serum creatinine ≥25% Primary endpoint: increase in serum creatinine ≥25% within 2 days post-exposurewithin 2 days post-exposure

Prevention of CIN with Sodium Prevention of CIN with Sodium Bicarbonate: ResultsBicarbonate: Results
EndpointsEndpoints
Sodium Sodium
ChlorideChloride
N=59N=59
Sodium Sodium BicarbonateBicarbonate
N=60N=60
P P valuevalue
Incidence of CIN (%)Incidence of CIN (%) 13.6%13.6% 1.7%1.7% 0.020.02
Incidence of CIN Incidence of CIN (↑SCr 0.5 mg/dL)(↑SCr 0.5 mg/dL)
11.9%11.9% 1.7%1.7% 0.030.03
Merten GJ et al. Merten GJ et al. JAMA,JAMA, 2004;291:2328-2334 2004;291:2328-2334

REMEDIAL Trial REMEDIAL Trial
Saline + NAC Saline + NAC N=118N=118
Bicarbonate + NAC Bicarbonate + NAC N=117N=117
Saline+AA+NAC Saline+AA+NAC N=116N=116
7 excluded7 excluded
Pts with eGFR<40 Pts with eGFR<40 N=393 N=393
Randomized N=351Randomized N=351
Excluded N=42Excluded N=42
NAC = NAC = NN-acetylcysteine, AA = ascorbic acid-acetylcysteine, AA = ascorbic acid
9 excluded9 excluded9 excluded9 excluded
107 included 107 included into analysisinto analysis
108 included 108 included into analysisinto analysis
111 included 111 included into analysisinto analysis
Briguorio C. et al, Briguorio C. et al, CirculationCirculation 2007 2007
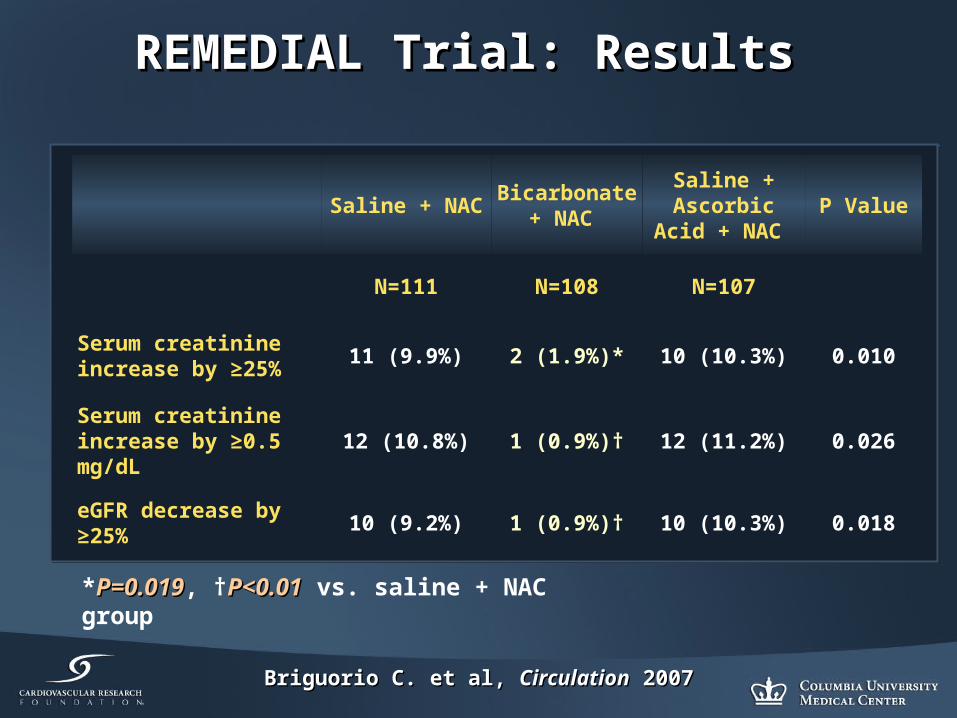
REMEDIAL Trial: Results REMEDIAL Trial: Results
Saline + NAC Bicarbonate +
NAC
Saline + Ascorbic Acid
+ NAC P Value
N=111 N=108 N=107
Serum creatinine increase by ≥25%
11 (9.9%) 2 (1.9%)* 10 (10.3%) 0.010
Serum creatinine increase by ≥0.5 mg/dL
12 (10.8%) 1 (0.9%)† 12 (11.2%) 0.026
eGFR decrease by ≥25%
10 (9.2%) 1 (0.9%)† 10 (10.3%) 0.018
*P=0.019P=0.019, †P<0.01P<0.01 vs. saline + NAC group
Briguorio C. et al, Briguorio C. et al, CirculationCirculation 2007 2007

MEENAMEENA
DesignDesign• DESIGN: Prospective,
randomized, parallel-group, single-center clinical evaluation of two hydration strategies for patients undergoing coronary angiography
• OBJECTIVE: To compare the incidence of CIN between periprocedural hydration with sodium bicarbonate vs. sodium chloride (0.9%, normal saline)
• PRIMARY ENDPOINT: Decrease in estimated GFR by ≥ 25% within 4 days of coronary angiography
• DESIGN: Prospective, randomized, parallel-group, single-center clinical evaluation of two hydration strategies for patients undergoing coronary angiography
• OBJECTIVE: To compare the incidence of CIN between periprocedural hydration with sodium bicarbonate vs. sodium chloride (0.9%, normal saline)
• PRIMARY ENDPOINT: Decrease in estimated GFR by ≥ 25% within 4 days of coronary angiography
353 patients enrolled between January 2006 and January 2007
353 patients enrolled between January 2006 and January 2007
236 patients assigned to sodium
chloride
236 patients assigned to sodium
chloride
178 patients assigned to sodium
bicarbonate
178 patients assigned to sodium
bicarbonate
156 evaluable patient
156 evaluable patient
Brar, S et. al., i2/ACC 2007
147 evaluable patient
147 evaluable patient
22 excluded
22 excluded
28 excluded
28 excluded
Hydration ProtocolHydration Protocol•3 mL/kg for 1 hr before the procedure•1.5 mL/kg during and for 4hrs post-procedure
Hydration ProtocolHydration Protocol•3 mL/kg for 1 hr before the procedure•1.5 mL/kg during and for 4hrs post-procedure
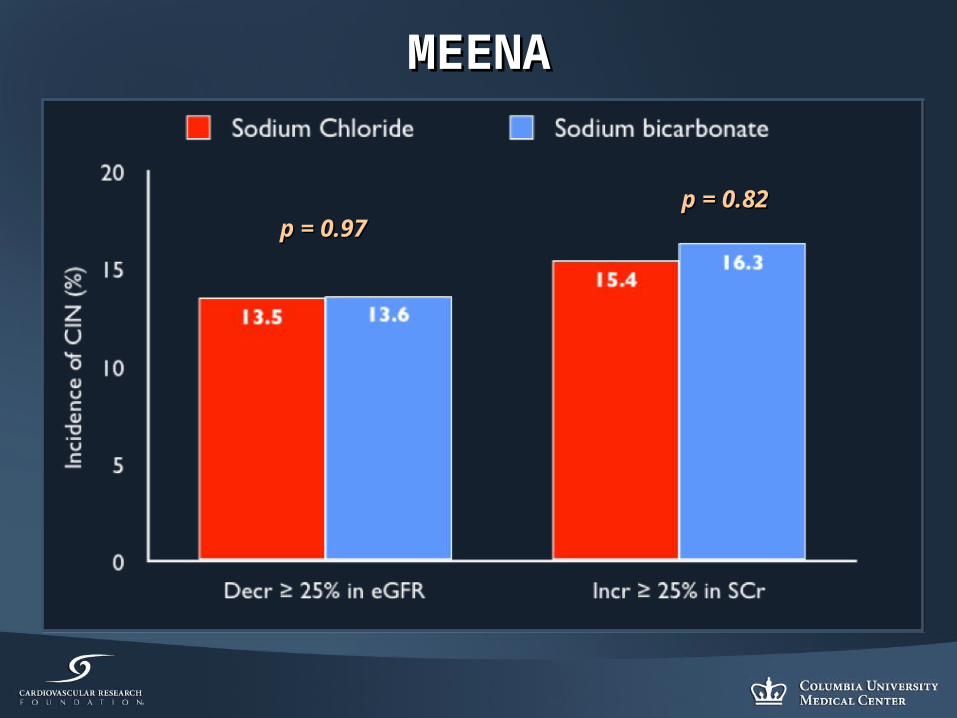
MEENAMEENA
p = 0.97p = 0.97p = 0.82p = 0.82

Sodium BicarbonateSodium BicarbonateStudyStudy NN
(Saline, Bicarb)(Saline, Bicarb)ProcedureProcedure Baseline Baseline
FunctionFunction(mL/min/(mL/min/1.73m2)1.73m2)
Fluid protocolFluid protocol CIN rate CIN rate (%)(%)
pp
RANDOMIZEDRANDOMIZED
BrarBrar 353 353 (175, 178)(175, 178)
CardiacCardiac 48484848
SalineSalineBicarbonateBicarbonate
13.613.613.513.5
0.970.97
BriguoriBriguori 219219(108, 111)(108, 111)
Cardiac Cardiac PeripheralPeripheral
32323535
SalineSalineBicarbonateBicarbonate
9.99.91.91.9
0.020.02
MertenMerten 119 119 (59, 60)(59, 60)
Cardiac Cardiac PeripheralPeripheral
45454141
SalineSalineBicarbonateBicarbonate
13.713.71.71.7
0.020.02
Masuda*Masuda* 5959(29, 30)(29, 30)
Emergency Emergency cardiaccardiac
39394040
SalineSalineBicarbonateBicarbonate
353577
0.010.01
NON-RANDOMIZEDNON-RANDOMIZED
CARECARE 414414(246, 168)(246, 168)
CardiacCardiac 50505050
Bicarbonate Bicarbonate (-NAC)(-NAC)Bicarbonate Bicarbonate (+NAC)(+NAC)
10.610.6
11.911.9
NSNS

N-ACETYLCYSTEINE (NAC)N-ACETYLCYSTEINE (NAC)

CIN: Effect of n-AcetylcysteineCIN: Effect of n-Acetylcysteine
• Prospective, randomizedProspective, randomized
• 83 high risk patients83 high risk patients CrCl < 50 ml/minCrCl < 50 ml/min Diabetes 33%Diabetes 33%
• IV CONTRAST for CT (75 IV CONTRAST for CT (75 ml of Low Osmolar CM)ml of Low Osmolar CM)
• n-AC 600 bid x 2 days pre-n-AC 600 bid x 2 days pre-
• CIN definition: creatinine CIN definition: creatinine increase of 0.5 mg/dl increase of 0.5 mg/dl
• Hydration with 0.45% @ 1 Hydration with 0.45% @ 1 ml/kg/h x 24 hml/kg/h x 24 h
21%
2%
0%
5%
10%
15%
20%
25%
Control (42) AC (41)
CIM
(%
)
Tepel Tepel NEJMNEJM 2000 2000
p= 0.01p= 0.01
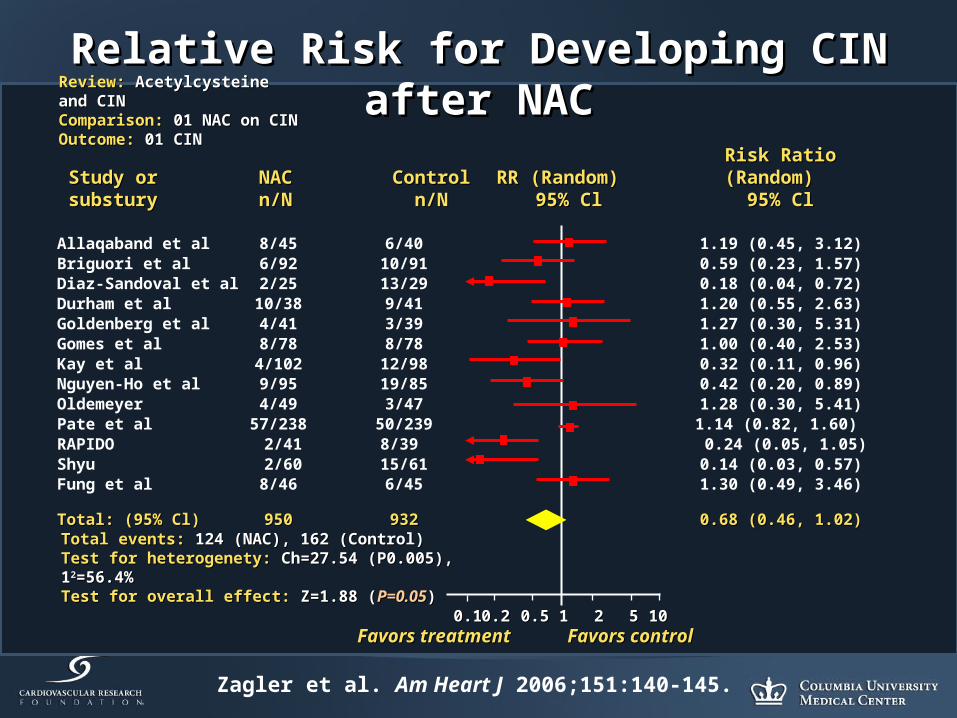
Zagler et al. Am Heart J 2006;151:140-145.
Relative Risk for Developing CIN after NACRelative Risk for Developing CIN after NAC
Risk Ratio (Random) Risk Ratio (Random) 95% Cl95% Cl
0.10.1 11 1010Favors treatmentFavors treatment Favors controlFavors control
0.20.2 0.50.5 22 55
RR (Random) RR (Random) 95% Cl95% Cl
ControlControln/Nn/N
NACNACn/Nn/N
Study or Study or substurysubstury
Review: Review: Acetylcysteine and CINAcetylcysteine and CINComparison: Comparison: 01 NAC on CIN01 NAC on CINOutcome: Outcome: 01 CIN01 CIN
Total events: Total events: 124 (NAC), 162 (Control)124 (NAC), 162 (Control)Test for heterogenety: Test for heterogenety: Ch=27.54 (P0.005), 1Ch=27.54 (P0.005), 122=56.4%=56.4%Test for overall effect: Test for overall effect: Z=1.88 (Z=1.88 (P=0.05P=0.05))
Allaqaband et al 8/45 6/40 1.19 (0.45, 3.12)Briguori et al 6/92 10/91 0.59 (0.23, 1.57)Diaz-Sandoval et al 2/25 13/29 0.18 (0.04, 0.72)Durham et al 10/38 9/41 1.20 (0.55, 2.63)Goldenberg et al 4/41 3/39 1.27 (0.30, 5.31)Gomes et al 8/78 8/78 1.00 (0.40, 2.53)Kay et al 4/102 12/98 0.32 (0.11, 0.96)Nguyen-Ho et al 9/95 19/85 0.42 (0.20, 0.89)Oldemeyer 4/49 3/47 1.28 (0.30, 5.41)Pate et al 57/238 50/239 1.14 (0.82, 1.60) RAPIDO 2/41 8/39 0.24 (0.05, 1.05)Shyu 2/60 15/61 0.14 (0.03, 0.57)Fung et al 8/46 6/45 1.30 (0.49, 3.46)
Total: (95% Cl)Total: (95% Cl) 950950 932932 0.68 (0.46, 1.02)0.68 (0.46, 1.02)

Meta-analysis: High vs.Meta-analysis: High vs.Low Osm Contrast MediaLow Osm Contrast Media
• 39 Trials - 5146 patients39 Trials - 5146 patients
• CIN > 0.5 mg/dlCIN > 0.5 mg/dl
• CIN in 7% of all patientsCIN in 7% of all patients
• CIN in 30% of CRI CIN in 30% of CRI patientspatients
• For CRI, NNT=8 (treat 8 to For CRI, NNT=8 (treat 8 to prevent 1 CIN case)prevent 1 CIN case)
• Low osmolal group Low osmolal group included Ioxaglate included Ioxaglate (Hexabrix); Iodixanol (Hexabrix); Iodixanol (Visipaque) not studied(Visipaque) not studied
Barrett and Carlisle Barrett and Carlisle J Am Soc NephrolJ Am Soc Nephrol 92; 92;
1.0
0.61
0.0
0.2
0.4
0.6
0.8
1.0
1.2
High Osm Low Osm
Rel
ativ
e R
isk
of
CIN

The NEPHRIC StudyThe NEPHRIC Study
Nephrotoxicity in High-risk PatientsNephrotoxicity in High-risk Patientsa Double Blind Randomized Multicentre a Double Blind Randomized Multicentre Study of Iso-osmolar and Low-osmolar Study of Iso-osmolar and Low-osmolar
Non-ionic Contrast MediaNon-ionic Contrast Media
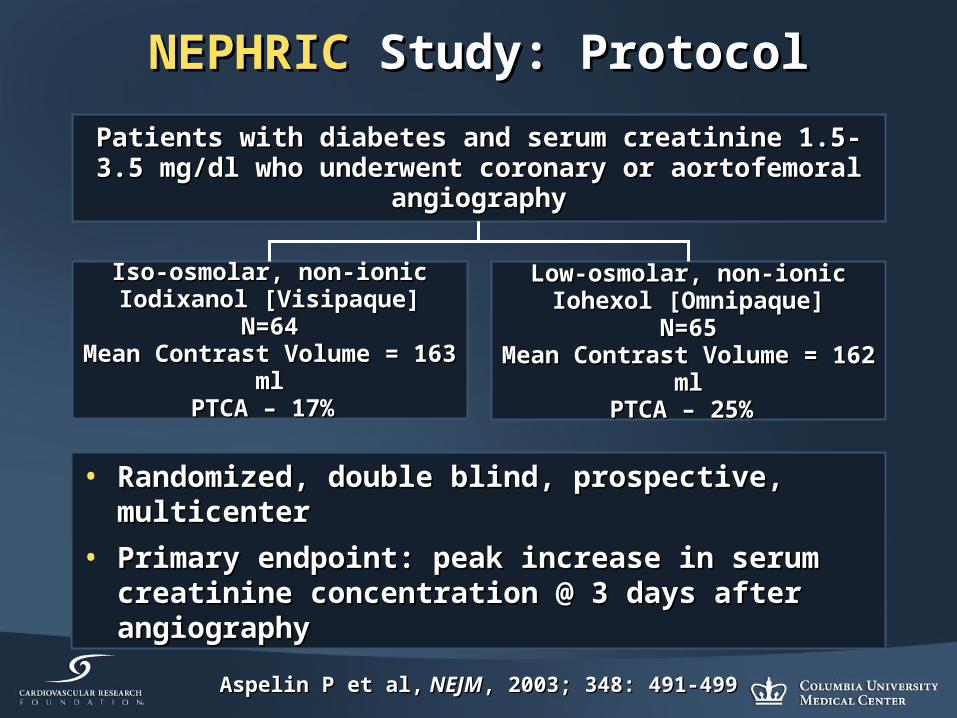
NEPHRICNEPHRIC Study: Protocol Study: Protocol
• Randomized, double blind, prospective, multicenterRandomized, double blind, prospective, multicenter
• Primary endpoint: peak increase in serum creatinine Primary endpoint: peak increase in serum creatinine concentration @ 3 days after angiographyconcentration @ 3 days after angiography
Patients with diabetes and serum creatinine 1.5-3.5 mg/dl who Patients with diabetes and serum creatinine 1.5-3.5 mg/dl who underwent coronary or aortofemoral angiographyunderwent coronary or aortofemoral angiography
Iso-osmolar, non-ionicIso-osmolar, non-ionicIodixanol [Visipaque]Iodixanol [Visipaque]
N=64N=64Mean Contrast Volume = 163 mlMean Contrast Volume = 163 ml
PTCA – 17% PTCA – 17%
Low-osmolar, non-ionicLow-osmolar, non-ionicIohexol [Omnipaque]Iohexol [Omnipaque]
N=65N=65Mean Contrast Volume =Mean Contrast Volume = 162 ml162 ml
PTCA – 25% PTCA – 25%
Aspelin P et al,Aspelin P et al, NEJM NEJM, 2003; 348: 491-499, 2003; 348: 491-499

Primary Endpoint –Primary Endpoint –Peak Increase in Scr from Baseline to Day 3Peak Increase in Scr from Baseline to Day 3
(µmol/l) (µmol/l) p=0.002p=0.002
Iodixanol Iodixanol (Visipaque)
Iohexol Iohexol (Omnipaque)
n=62n=62 n=64n=64
MeanMean 11.2 ±19.711.2 ±19.7 41.5 ± 68.641.5 ± 68.6
MinimumMinimum - 19.0- 19.0 - 21.0- 21.0
MaxMax 74.074.0 331.0331.0
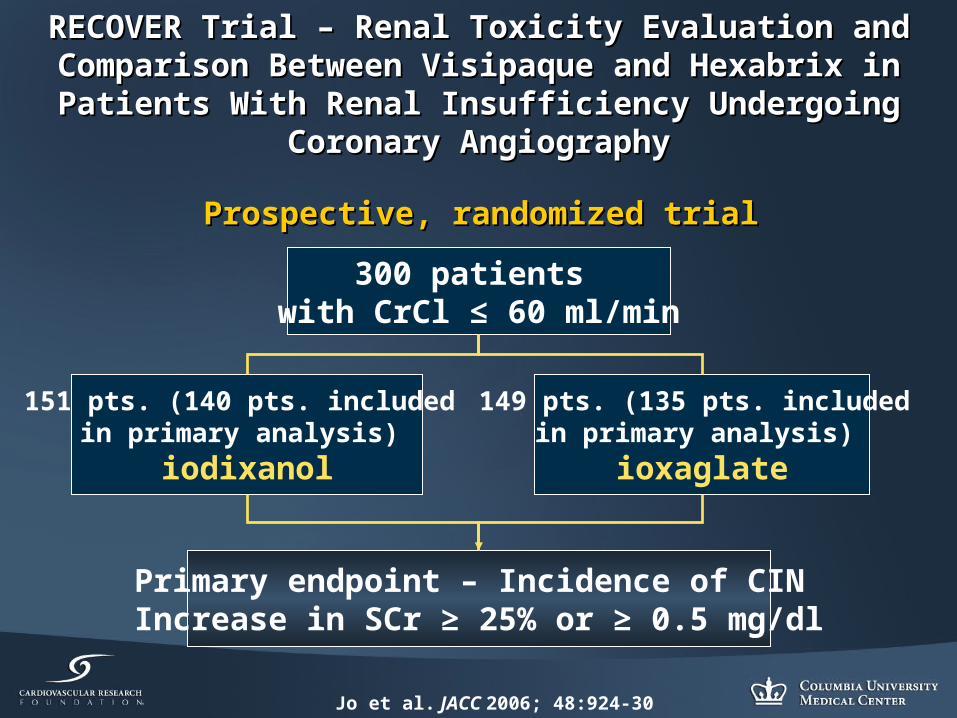
RECOVER Trial – Renal Toxicity Evaluation and Comparison RECOVER Trial – Renal Toxicity Evaluation and Comparison Between Visipaque and Hexabrix in Patients With Renal Between Visipaque and Hexabrix in Patients With Renal
Insufficiency Undergoing Coronary AngiographyInsufficiency Undergoing Coronary Angiography
Jo et al. JACC 2006; 48:924-30
Prospective, randomized trialProspective, randomized trial
300 patients with CrCl ≤ 60 ml/min
149 pts. (135 pts. included in primary analysis)
ioxaglate
151 pts. (140 pts. included in primary analysis)
iodixanol
Primary endpoint – Incidence of CIN Increase in SCr ≥ 25% or ≥ 0.5 mg/dl

RECOVER Trial – Incidence of CIN RECOVER Trial – Incidence of CIN
Jo et al. JACC 2006; 48:924-30
17.0%
7.9%
0.0%
10.0%
20.0%
CIN
ioxaglate
iodixanol
P=0.021P=0.021
N=300

24.2%16.2%
0%
10%
20%
30%
Ioxaglate Iodixanol
ICON ICON TTrialrial
Patients Patients wwith ith cchronic hronic rrenal enal iinsufficiencynsufficiencyuundergondergoinging PCI PCI wwith at ith at lleast 150cc of east 150cc of ccontrast ontrast vvolumeolume
Patients Patients wwith ith cchronic hronic rrenal enal iinsufficiencynsufficiencyuundergondergoinging PCI PCI wwith at ith at lleast 150cc of east 150cc of ccontrast ontrast vvolumeolume
IoxaglateIoxaglateN=74N=74
IoxaglateIoxaglateN=74N=74
IodixanolIodixanolN=71N=71
IodixanolIodixanolN=71N=71
NN=130=130
P=0.26P=0.26
Incidence of CIN
Mehran R. et al, Transcatheter Cardiovascular Therapeutics. 2006.

Renal Failure in Patients Undergoing Coronary Renal Failure in Patients Undergoing Coronary Procedures using Iso-osmolar or Low-osmolar Procedures using Iso-osmolar or Low-osmolar
Contrast MediaContrast Media
Liss et al. Kidney International 2006
Contrast Contrast media (CM)media (CM) CM propertiesCM properties NN Time periodTime period
IodixanolIodixanol iso-osmolar, nonionic, iso-osmolar, nonionic, 45 48545 485 2000-20032000-2003
IoxaglateIoxaglate low-osmolar, nonionic, low-osmolar, nonionic, 12 44012 440 2000-20032000-2003
• Swedish Coronary Angiography and Angioplasty Registry• Swedish Hospital Discharge Registry

Rehospitalization with Renal Failure as a Rehospitalization with Renal Failure as a Primary Diagnosis Primary Diagnosis
Liss et al. Kidney International 2006
0.02% 0.03%
0.10%0.07%
0.20%
0.30%
0.00%
0.10%
0.20%
0.30%
0.40%
Within 1 w eek Within 1 month Within 3months
Ioxaglate
Iodixanol P<0.001P<0.001P<0.001P<0.001
P<0.001P<0.001P<0.001P<0.001
P=0.022P=0.022P=0.022P=0.022

Start of Dialysis after Coronary Start of Dialysis after Coronary Angiography or PCI Angiography or PCI
Liss et al. Kidney International 2006
0.00%0.02%
0.10%
0.02%
0.10%
0.20%
0.00%
0.05%
0.10%
0.15%
0.20%
0.25%
Within 1 week Within 1 month Within 3 months
Ioxaglate
Iodixanol
P=0.098P=0.098P=0.098P=0.098
P=0.010P=0.010P=0.010P=0.010
P=0.009P=0.009P=0.009P=0.009

1-year Follow-up 1-year Follow-up
Liss et al. Kidney International 2006
* Groups differ in time period !
CMCM N of ptsN of pts
iodixanoliodixanol 54 61654 616
ioxaglateioxaglate 24 47924 479
* * iohexoliohexol 6 8546 854
Renal failureRenal failure Iodixanol
Iohexol
Ioxaglate
f
Time (years)
%
6
5
4
3
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12
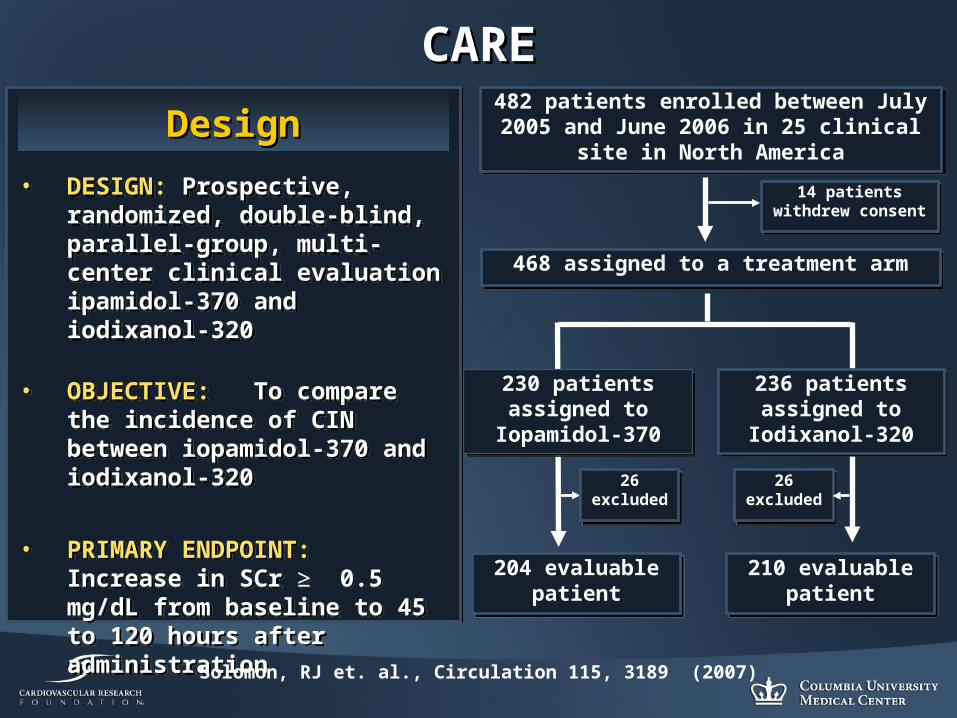
CARECARE
DesignDesign
• DESIGN: Prospective, randomized, double-blind, parallel-group, multi-center clinical evaluation ipamidol-370 and iodixanol-320
• OBJECTIVE: To compare the incidence of CIN between iopamidol-370 and iodixanol-320
• PRIMARY ENDPOINT: Increase in SCr ≥ 0.5 mg/dL from baseline to 45 to 120 hours after administration
• DESIGN: Prospective, randomized, double-blind, parallel-group, multi-center clinical evaluation ipamidol-370 and iodixanol-320
• OBJECTIVE: To compare the incidence of CIN between iopamidol-370 and iodixanol-320
• PRIMARY ENDPOINT: Increase in SCr ≥ 0.5 mg/dL from baseline to 45 to 120 hours after administration
482 patients enrolled between July 2005 and June 2006 in 25 clinical site in North
America
482 patients enrolled between July 2005 and June 2006 in 25 clinical site in North
America
14 patients withdrew consent
14 patients withdrew consent
468 assigned to a treatment arm468 assigned to a treatment arm
236 patients assigned to
Iodixanol-320
236 patients assigned to
Iodixanol-320
230 patients assigned to
Iopamidol-370
230 patients assigned to
Iopamidol-370
204 evaluable patient
204 evaluable patient
Solomon, RJ et. al., Circulation 115, 3189 (2007)
210 evaluable patient
210 evaluable patient
26 excluded
26 excluded
26 excluded
26 excluded

CARECARE
p = 0.39p = 0.39 p = 0.44p = 0.44 p = 0.15p = 0.15

CARECARE
p = 0.11p = 0.11 p = 0.37p = 0.37 p = 0.20p = 0.20
Diabetic SubgroupDiabetic Subgroup

Conclusions (1)Conclusions (1)
• CRI is one of the most important independent CRI is one of the most important independent predictors of poor outcome post PCIpredictors of poor outcome post PCI
• CIN remains a frequent source of acute renal CIN remains a frequent source of acute renal failure and is associated with increased morbidity failure and is associated with increased morbidity and mortality, and higher resource utilizationand mortality, and higher resource utilization
• Several factors predispose patients to CINSeveral factors predispose patients to CIN
• Preventive measures pre procedure, as well as Preventive measures pre procedure, as well as careful post procedure management should be careful post procedure management should be routine in all patientsroutine in all patients

Conclusions (2)Conclusions (2)
• Hydration pre-PCI (12 hours recommended)Hydration pre-PCI (12 hours recommended)
• D/C nephrotoxic drugs (NSAIDS, antibiotics, etc)D/C nephrotoxic drugs (NSAIDS, antibiotics, etc)
• Role of n-acetylcysteine is disputableRole of n-acetylcysteine is disputable
• No Role for IV FenoldopamNo Role for IV Fenoldopam
• Sodium bicarbonate may be useful, but need more definitive Sodium bicarbonate may be useful, but need more definitive data data
• Limit contrast agent volumeLimit contrast agent volume
• Low-osmolar agents are better than high-osmolarLow-osmolar agents are better than high-osmolar
Within non-ionic contrast, the data are contradictory Within non-ionic contrast, the data are contradictory
• Role of local drug delivery for prevention of CIN requires Role of local drug delivery for prevention of CIN requires further investigationfurther investigation
• Role of Cooling Therapy is being examined: COOL CIN StudyRole of Cooling Therapy is being examined: COOL CIN Study
Related Documents











