Winter Pressures in NHS Scotland 2008-2009 Report for the Emergency Access Delivery Team, Scottish Government Dr Daniel Beckett

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Winter Pressures in NHS Scotland 2008-2009
Report for the Emergency Access Delivery Team, Scottish Government
Dr Daniel Beckett

CONTENTS
CONTENTS.....................................................................................................................2
FIGURES.........................................................................................................................3
TABLES...........................................................................................................................3
WINTER PRESSURES REPORT EXECUTIVE SUMMARY...........................................4
INTRODUCTION..............................................................................................................9
METHODS.....................................................................................................................10
ASSESSMENT OF PRESSURE....................................................................................11
ANALYSIS OF QUALITATIVE DATA...........................................................................17
THE WINTER PLANNING PROCESS.........................................................................................................................18NHS24.................................................................................................................................................................19SCOTTISH AMBULANCE SERVICE.........................................................................................................................20OUT OF HOURS GENERAL PRACTITIONER SERVICES............................................................................................21HOSPITAL ADMISSIONS.........................................................................................................................................23CAPACITY AND DEMAND WITHIN SECONDARY CARE...........................................................................................30HOSPITAL DISCHARGES........................................................................................................................................37
ANALYSIS OF QUANTITATIVE DATA.........................................................................42
LONG TERM TRENDS.............................................................................................................................................42WINTER 2008-2009..............................................................................................................................................43THE 4 HOUR STANDARD FOR ACCESS TO EMERGENCY CARE..............................................................................48PATIENT CHARACTERISTICS..................................................................................................................................50SPECIAL HEALTH BOARD DATA...........................................................................................................................52GP OUT OF HOURS SERVICES................................................................................................................................55
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS.........................................56
SUMMARY............................................................................................................................................................56CONCLUSIONS.......................................................................................................................................................58RECOMMENDATIONS............................................................................................................................................59
APPENDIX 1: QUESTIONNAIRE..................................................................................61
APPENDIX 2: LIST OF INTERVIEWEES......................................................................65
APPENDIX 3: EXAMPLES OF GOOD PRACTICE.......................................................68
APPENDIX 4: FESTIVE MONIES..................................................................................76
2

FIGURES
FIGURE 1. MEAN TEMPERATURE ANOMALY WINTER 2008-2009..................................................................... 15FIGURE 2. WINTER COMPARISON OF MEAN TEMPERATURES FOR SCOTLAND 2006-2007 & 2008-2009............15FIGURE 3. DAYS OF AIR FROST ANOMALY WINTER 2008-2009.......................................................................16FIGURE 4. A&E ATTENDANCES PER DAY VS PROPORTION ADMITTED - DEC 2008-JAN 2009-REDUCED
STAFFING............................................................................................................................................. 24FIGURE 5. A&E ATTENDANCES PER DAY VS PROPORTION ADMITTED - DEC 2008-JAN 2009-FULL STAFFING.....25FIGURE 6. EMERGENCY DEPARTMENT ATTENDANCES AND ADMISSIONS NHS GG&C WINTER 2008-2009........26FIGURE 7. EMERGENCY DEPARTMENT TIME PROFILE DEC 2008 – GOOD PERFORMANCE.................................27FIGURE 8. EMERGENCY DEPARTMENT TIME PROFILE DEC 2008 – POOR PERFORMANCE.................................28FIGURE 9. BEDS OCCUPIED BY PATIENTS ADMITTED AS EMERGENCIES (WEEKLY AVERAGE) .............................31FIGURE 10. BED OCCUPANCY LEVELS FOR CORE AND NON-CORE SITES – APR 2008-MAR 2009.....................35FIGURE 11. DELAYED DISCHARGES - SCOTLAND - JAN 2006-APR 2009.........................................................39FIGURE 12. FIRST A&E OUTPATIENT ATTENDANCES, SCOTLAND, 1998/99 – 2008/09....................................42FIGURE 13. EMERGENCY DEPARTMENT ADMISSIONS VS ALL EMERGENCY ADMISSIONS FEB 2008-JAN 2009.....43FIGURE 14. ATTENDANCES, ADMISSIONS & TRANSFERS FROM CORE EDS WINTER 2008-2009.......................44FIGURE 15. SCOTLAND EMERGENCY & ELECTIVE INPATIENT ADMISSIONS WINTER 2008-2009..........................45FIGURE 16. SCOTLAND EMERGENCY & ELECTIVE INPATIENT ADMISSIONS INC. DAYCASES WINTER 2008-2009
........................................................................................................................................................... 46FIGURE 17 ADMISSION/DISCHARGE PROFILE WITH 4 HOUR BREACHES FROM CORE SITES DEC 2008-JAN 2009
........................................................................................................................................................... 47FIGURE 18. NUMBER OF INPATIENT DISCHARGES PER WK DEC 2008-JAN 2009...............................................48FIGURE 19. PERCENTAGE OF A&E ATTENDANCES MEETING 4 HOUR STANDARD, JULY 2007 TO APRIL 2009
........................................................................................................................................................... 48FIGURE 20. REASONS FOR 4 HOUR BREACHES, DEC 2008-JAN 2009............................................................49FIGURE 21. NUMBER OF 12 HOUR BREACHES, JUNE 07 TO APRIL 09............................................................49FIGURE 22. EMERGENCY ADMISSIONS PER AGE GROUP, FEBRUARY 08-FEBRUARY 09....................................50FIGURE 23. EMERGENCY ADMISSIONS WINTER 2008-2009 SPLIT BY RESPIRATORY/NON-RESP DIAGNOSIS........51FIGURE 24. EMERGENCY ADMISSIONS WINTER 2006-2007 SPLIT BY RESPIRATORY/NON-RESP DIAGNOSIS........51FIGURE 25. SCOTLAND LEVEL MONTHLY EMERGENCY ADMISSIONS FOR ALL DIAGNOSES FEB 08-JAN 09..........52FIGURE 26. NHS24 CALL DEMAND WINTERS 2006-2007 & 2008-2009 AND SUMMER 2008..........................53FIGURE 27. NHS24 WINTER 08/09 TOTAL CALL DEMAND...............................................................................53FIGURE 28 SAS CATEGORY A INCIDENTS BY WEEK, MAINLAND SCOTLAND.....................................................54FIGURE 29. SAS CATEGORY A PERFORMANCE MAINLAND BY SUBDIVISION, DEC 06/JAN 07/DEC 08/JAN 09....54FIGURE 30. GP OUT OF HOURS ACTIVITY......................................................................................................55FIGURE 31. GP OUT OF HOURS PERFORMANCE FOR 1 HOUR HOME VISITS......................................................56
TABLES
TABLE 1. MEAN SCORES GIVEN ON LIKERT QUESTIONS BY CLINICIANS, MANAGEMENT AND GPOOH STAFF…........................................................................................................................................................ ...18
TABLE 2. NHS SCOTLAND EMERGENCY AND ELECTIVE ADMISSIONS DEC 2008 AND JAN 2009 COMPARED WITH THE FIVE YEAR MONTHLY MEAN.............................................................................................................45
3

Winter Pressures Report Executive Summary
Feedback from NHS Health Boards
BACKGROUND
1. In March 2009 the Scottish Government Emergency Access Delivery Team commissioned a report to review the pressures experienced, and response by NHS Scotland during winter 2008-2009.
2. There has been a significant improvement in the 4 hour emergency access waiting times, increasing from 87% in June 2006 to delivery of the current 98% 4 hour HEAT Standard. However, there was a drop in performance in 11 out of the 14 territorial Health Boards against the 4 hour Standard in December 2008 and January 2009. Overall performance for NHS Scotland during these months dipped below 98% (96.7% and 96.5% respectively). Additionally, there was media interest in how well the NHS had handled winter in parts of Scotland, particularly the central belt, with articles about long trolley waits, and hospitals not coping with adverse weather conditions. Recent figures (March 2009) show performance improved to 97.7% with 140,000 attendances (compared with 128,084 in December).
3. The review was undertaken by Dr Daniel Beckett, Acting Consultant in Acute Medicine at the Royal Infirmary of Edinburgh, with support from NSS Information Services Department (ISD) and Scottish Government Analytical Services Directorate (ASD). Each NHS Health Board in Scotland was visited, plus the relevant Special Health Boards, to obtain a wide range of professional and staff perceptions about their local experience of winter using semi-structured one-to-one interviews. Quantitative data and information was provided by ISD and ASD.
4. The report focused upon December and January as these were the months with the poorest performance against the 4 hour Standard. Comparison was made with previous winter performances, particularly 2006-2007 (as 2007-2008 was widely considered to have been atypical)
KEY FINDINGS
5. The key findings from the qualitative and quantitative aspects of this report are summarised below.
Hospital Admissions
6. There was a perception amongst Health Boards that winter 2008-2009 had been ‘busier than previous years’ in terms of total numbers of admissions and that the
4

peak had commenced earlier. Health Boards commented that the age profile of patients admitted over winter appeared to be older, with more patients suffering from respiratory disease resulting in greater lengths of stay. Data from the SMR01 dataset confirmed that, compared with the five year monthly mean, there was a 7.9% increase in all emergency admissions across the NHS in Scotland in December 2008, followed by a 1.8% increase in January 2009 (Figure 16, main report (p46)). Furthermore, there was an 11% increase in the number of patients admitted to hospital with respiratory illness over December and January compared with winter 2006-2007. However in practice this equates to only 2 extra respiratory patients per day across NHS Scotland. There was no evidence for a disproportionate increase in admission of elderly patients or greater length of stay.
Hospital Discharges
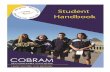
7. Low levels of hospital discharges, particularly over the festive period, were highlighted as a cause for concern by most NHS Health Boards over winter 2008-2009.
8. Figure 18, main report (p48), shows admission/discharge profiles across NHS Scotland (from core sites) plus number of four hour breaches. There is a consistent admission/discharge profile in December, with peaks of admissions at the start of the week, mirrored by a peak of discharges towards the end of the week. Admissions outnumbered discharges every weekend (and on Mondays) with a surge of discharges on Christmas Eve. This was followed by the 11 day holiday period, and for nine of these 11 days, admissions outnumbered discharges. The net effect was that hospitals had high levels of bed occupancy when the elective programme restarted at full capacity on 5 January, resulting in a spike in four hour breaches. The system attempted to return to the previous admission/discharge profile over the following week, but had not recovered by the following Monday, 12 January, and further four hour breaches were noted.
9. Reasons highlighted for this reduction in discharges over the festive period included:
lack of consultant staff in downstream wards; lack of discharge infrastructure over the festive period (e.g. Patient
Transport Services, Allied Health Professionals and social work); and perceived lack of coordination of decision making in the system over the
festive period.
10. Tools for discharge planning, such as Estimated Date of Discharge (EDD), and Nurse Led Discharge (NLD) were used patchily, and in some Health Boards not at all.
11. Health Boards reported almost universal improvement in numbers of delayed discharges, with NHS Scotland achieving zero delayed discharges over 6 weeks by April 2008 and 2009 (although this was not achieved in every month). A small number of Health Boards continued to be challenged by significant numbers of delayed discharges over 6 weeks.
Capacity and Demand Planning
5

12. Nine of the 14 territorial Health Boards have developed an internal tool to predict unscheduled activity, and these were largely found to be accurate. Two Health Boards employed tools to predict discharges based on previous discharge patterns. Despite Health Boards being encouraged to use System Watch, there was little use for medium to long term predictions of activity despite its proven accuracy. Figure 9, main report (p31), shows the System Watch prediction for winter 2008-2009. Activity started to increase early (2 November), but then short term prediction followed well after 2-3 weeks.
13. Eight out of 11 mainland Health Boards opened additional capacity beds in their acute sites this winter. Many Health Boards had difficulties accessing the full complement of community beds, despite the acute site being near, or over-capacity. These difficulties included:
lack of Patient Transport Services; complex referral pathways; and patient choice.
Escalation Plans
14. There was variation between Health Boards in the effectiveness of local escalation plans. Most Health Boards had a bed management escalation plan, but the triggers for escalation varied between predicted activity, actual observed activity, or simply perception of activity. There were reports of managers and clinicians (including primary care) becoming desensitised to red alert. Conversely there were reports of middle management being reluctant to escalate, or senior managers refusing to escalate to red alert.
15. CHP involvement in escalation plans was variable, with one example of an escalation plan being developed by CHP senior management without clear involvement of CHP middle managers, who were not fully sighted on this and were unable to respond when necessary.
Elective Activity
16. Eight of the 14 territorial Health Boards continued with elective work until Christmas Eve and between Christmas and New Year, whereas six Health Boards ran a ‘cancer and urgent only’ service over the festive period. The decrease in elective admissions on 29 December (60% of a ‘normal’ Monday) is shown on Figure 16, main report (p46).
17. The perception in several Health Board areas was that the introduction of the 18 week Referral to Treatment Target, and the disbanding of the Unscheduled Care Collaborative, de-prioritised the 4 hour Standard. Examples of this included:
surgical wards (with staff available) remaining closed over the festive period despite eight hour, or greater, trolley waits in the Emergency Department; and
waiting list initiatives on 5 January despite clear predictions of high levels of unscheduled medical activity.
6

18. Seven Health Boards did not cancel any elective procedures due to lack of beds, five cancelled a small number (<15 each) and two cancelled significantly more.
Staffing
19. Three major staffing challenges over winter were highlighted:
Potential problem with non-clinical staff retention in out of hours GP services because staff employed under Agenda for Change were not paid extra for working unsociable hours over the festive period.
Implementation of Modernising Medical Careers (MMC) and nationalised medical recruitment has led to a number of medical posts, particularly within acute specialities, remaining unfilled.
Many sites did not have sufficient consultants in the hospital to deal with the predicted activity over the two week festive period and to facilitate quicker discharges in down stream wards.
There was a perception of lack of social work availability due to significant amounts of annual leave being taken over the festive period.
Boarding Patients (outliers)
20. Each of Scotland’s 11 mainland Health Boards use boarding of patients outside their own speciality beds as a solution to capacity issues. Over winter 2008-2009 in some sites up to 60% of all medical patients were boarders, occupying more than 10% of the total bed complement. There has been a recent move to board patients from the Admission Unit (and in exceptional circumstances the Emergency Department) before initial consultant review. This should be considered a clinical governance issue.
Recommendations
These recommendations should be considered alongside the many examples of good practice detailed in Appendix 3 to this report.
Health Boards should ensure that their winter planning starts early and that the process includes Community Health Partnerships and Social Work Departments. There should be a clear relationship between the winter plan and pandemic ‘flu plan.
Integral to the winter plan should be the escalation plan. This should involve all stakeholders including Community Health Partnerships. This includes the utilisation of beds in Community Hospitals, and protocols for referral and transfer should be agreed to resolve issues relating to perceived bed ownership.
System Watch should be used systematically for long to medium term predictions of unscheduled activity, and predictions acted upon to create the necessary capacity, in terms of beds and to support initiatives to reduce
7

admissions. Consideration should also be given to the use of System Watch for planning of elective activity over the winter months.
Daily bed meetings should take place at every site, and should occur twice daily during the winter period. Consultant medical staff should have greater awareness of bed management issues, including escalation plans for sites.
Health Boards should undertake more accurate modelling over the festive period to plan elective capacity and optimise the use of bed capacity, including maximising the bed capacity in community hospitals. This may then enable hospitals to reduce the number of elective admissions on the first Monday in January. Further consideration should be given to front loading the first week in January with minor procedures, and back loading with majors. Also medical elective activity (such as clinics and endoscopy lists) could be back loaded during this week.
Medical Directors should ensure that appropriate numbers of consultant medical staff are on site to deal with the predicted activity over the two week festive period.
Health Boards should aim to eliminate boarding of patients as a solution to bed capacity problems. Specifically, the boarding of patients from the Acute Medical Unit and/or Emergency Department should not occur (this includes ‘treat and transfer’ policies, with the exception of tertiary care referrals).
The level of discharges over the holiday period should be improved. This might include:
o increased consultant presence with dedicated discharge ward rounds in downstream wards;
o utilisation of a rapid response team (or equivalent) of AHPs with access to homecare packages without recourse to social work assessment; and
o re-energising and establishing ownership of the Estimated Date of Discharge policy, plus introducing Nurse Led Discharges (NLDs).
o Patients should be discharged early in the day, as this is key to maintaining capacity. Planning of discharge ward rounds should take this into account.
If all the above measures have been undertaken, including consultant review and discharge of downstream patients, and all capacity beds filled (including community beds) then the 98% standard for emergency access of care should be achievable. Health Boards should note that if there are ongoing difficulties then priority should be given to emergency admissions over routine elective procedures. The Scottish Government has, for the last 10 years, made it clear that clinical decision making always trumps routine elective targets.
8

Introduction
1. The National Emergency Access Delivery Team (EADT) works closely with Scottish Government Health Directorates to provide direction and support to NHS Health Boards to:
deliver local improvement trajectories for reducing rates of attendances at the Emergency Department (HEAT target T10);
monitor Health Boards’ performance in relation to the maximum 4 hour wait; and
improve whole systems winter planning.
2. In March 2009 the EADT commissioned a short term review of pressures experienced and response by NHS Scotland over winter 2008-2009. The main driver for this was the dip in performance against the 4 hour Standard for emergency access in December 2008 and January 2009 in some parts of Scotland. Additionally, there had been unfavourable media interest regarding NHS handling of winter pressures, particularly in the central belt, with articles about extended trolley waits, and hospitals unable to cope with the adverse weather
3. The purpose of this review was to:
- provide a description of unscheduled care systems in Scotland over winter, including levels of activity and pressure points from November 2008 – March 2009 (this being defined as the ‘winter period’);
- assess the extent to which the system ‘coped’ or showed signs of strain;- describe the winter planning response, including what worked and what didn’t;- derive lessons for the future, and explore how recommendations may be
implemented; and- identify the extent to which community/primary care can improve the
effectiveness of the whole system of unscheduled care.
4. The review was carried out by Dr Daniel Beckett, Acting Consultant in Acute Medicine at the Royal Infirmary of Edinburgh, with support from NSS Information Services Department and the Scottish Government Analytical Services Directorate. Each NHS Health Board in Scotland was visited, plus the relevant Special Health Boards, to obtain the perceptions of staff using semi-structured one-to-one interviews. Quantitative data and information was provided by ISD and ASD. The Key Learning Points and examples of good practice will be shared with the Service, both at the National Winter Planning Conference (June 2009) and through distribution of this report, in order to inform planning for winter 2009-2010.
9

Methods
Qualitative data
5. All 14 territorial Health Boards across NHS Scotland were visited, plus the relevant Special Health Boards. Seventy interviews, using a semi-structured questionnaire, were undertaken over a 10 week period. All interviews were digitally recorded and transcribed by the author. All data was anonymised following transcription. A minimum of two people from each Health Board were interviewed. These included:
Hospital management, including Chief Executives, Directors of Operations, General Managers and Senior Bed Managers;
Secondary care clinical staff, with the focus on clinical leads for Emergency Medicine and Acute Medicine;
Clinical and management staff from GP out of hours services; Social work representation; and Mental health representation.
The Special Health Boards visited were:
Scottish Ambulance Service; NHS24; Health Protection Scotland (HPS); and NHS Education for Scotland (NES).
The questionnaire can be found in Appendix 1 to this report, and the list of interviewees in Appendix 2.
Quantitative data
6. Information Services Division (ISD) is Scotland's national organisation for health information and statistics (www. isdscotland.org). It collects, analyses and publishes information on health and health care services in Scotland from a wide range of datasets. All datasets adhere to National Data Standards and data collected according to rigorous classifications and rules to ensure they are of consistently high quality.
7. A number of these datasets have been used to support the qualitative findings in this report. These include:
ISD(S)1 - Hospital Activity Statistics
The ISD(S)1 scheme provides routine quarterly aggregate information for monitoring activity in hospitals, health centres and clinics in NHS Scotland. Information collected (on monthly returns) relates to hospital beds, inpatients, outpatients, day cases, day patients, haemodialysis patients, ward attendees, patients seen by AHP's (Allied Health Professionals) and other technical department staff and cancellations.
10

A&E Data Mart
Established in July 2007, this dataset is an aggregate of monthly patient level returns for all attendances submitted by 33 main/major Accident and Emergency departments (core sites) across Scotland. Data included in this report is for new and unplanned attendances at A&E. This data is still being developed. SMR01 - General Acute Inpatient / Day Case Record
Contains patient based data on all inpatient and day case episodes in general and acute wards.
Delayed Discharges
Published quarterly, this comprises a census of NHS hospital in-patients who are "ready for discharge", but whose discharge has been delayed.
The data included in this report is released for management information purposes only and should be treated as restricted information until public release of related data on ISD's website.
In addition, the following organisations also provided data:
ADASTRA: This is the main IT system used to capture information on attendances at Primary Care Out of Hours centres.
NHS24 provided information on call dispositions and callbacks, plus performance against Key Performance Indicators (KPIs).
The Scottish Ambulance Service provided data on activity levels plus performance against KPIs.
Assessment of pressure
8. Assessing pressures in complex healthcare systems can be difficult, and different perspectives are often required as there is no single measure. Monitoring performance against national targets or standards, and recognised clinical outcomes can give an indication of where pressure exists in the system. In addition there are a number of proxy measures, such as the extent of boarding patients, or cancellation of elective activity, which add useful information. The following targets, standards and measures were used to gain an overall picture of the pressures experienced within each NHS Health Board:
1. 4 hour Target/Standard for access of emergency careThis Target specified that from end 2007, no patient will wait more than four hours from arrival to admission, discharge or transfer for emergency treatment. Importantly, the 4 hour Target in Scotland differed from that in England in that it specifically include trolleyed areas in assessment units. This Target was redefined as a HEAT Standard from April 2009 and is widely believed to be a good barometer of ’whole system performance’ in relation to unscheduled care.
11

The Scottish Government monitors monthly performance against this Standard based on daily data. Most NHS Health Boards use the nationally procured EDIS information system to collect the data, while the remaining Health Boards have had their systems’ compliance tested to allow amalgamation and national analysis of data. The mandatory dataset includes patient ID, hospital code, new or return patient, time/date of arrival and discharge, discharge destination, patient flow group and reason for four hour breach.
Often erroneously considered to be purely an Emergency Department Standard, lack of compliance with the 4 hour Standard implies whole system pressure. Simply relying on performance against the 4 hour Standard to assess pressure, however, may be flawed. Variations in delivering the 4 hour Standard may reflect differing admission protocols rather than true differences in performance. If a large proportion of admissions to hospital bypass the Emergency Department (for example direct ward admissions), comparisons with sites that operate a common front door policy may not be valid. This is particularly the case if primary care referrals to hospital are admitted directly to an area of the hospital that is considered, correctly or otherwise, not to be subject to the 4 hour Standard.
2. 12 hour trolley waitsTwelve hour trolley waits in the Emergency Department have significantly decreased since the introduction of the 4 hour Standard for access of emergency care. However, they still occur. There should be no 12 hour trolley waits.
3. Bed occupancyThe optimum bed occupancy rate is considered to be 82-85% by the UK Government1. Hospital bed occupancy rates are measured at midnight and may not reflect activity during the day when bed occupancy may be significantly higher.
4. Cancellation of elective activityThe numbers of operations that are cancelled or postponed for non-clinical reasons are submitted to the Scottish Government. However, different protocols exist between NHS Health Boards on volume of elective activity undertaken over the winter and festive period, and therefore the number of cancellations may not reflect comparable pressures across Health Boards.
5. Number of boarding patientsBoarding patients outside their speciality wards occurs at times of hospital overcrowding, which is associated with increased mortality2. Boarding is widely acknowledged to increase in response to increased system pressures,
1 http://www. publications. parliament. uk/pa/cm200708/cmhansrd/cm080506/debtext/80506-0002. html (Accessed 19 April 2009)
2 Spivrulis, P.C., Da Silva, J.A., Jacobs, I.G. et al. (2006). The association between hospital overcrowding and mortality amongst patients admitted via Western Australian emergency departments. Med J Aust, 184(5); 208-212.
12

and may be associated with increased mortality and length of stay (Prof D. Bell, personal communication, March 2009).
6. Key Performance Indicators for NHS24NHS24 has three service delivery Key Performance Indicators (KPIs) as follows:
KPI 1. Call handlers to answer 90% of calls from patients within 30 seconds
KPI 2. To commence 90% of GP priority calls within 20 minutes KPI 3. To commence 90% of GP routine calls within 60 minutes
The latter two of these KPIs are retrospective and based on real time performance. This allows NHS24 to measure accuracy of call routing, appropriateness of call reason, correct propitiation and clinical outcome.
The percentage of calls handled via the call-back mechanism is also recorded, as is the proportion of calls that are passed to out of hours partners as pre-prioritised calls. There are also clinical KPIs:
All serious and urgent calls must be answered immediately Priority 1, 2 and 3 calls must be dealt with in 1, 2 and 3 hours
respectively
Priority 1 and 2 calls are reported internally. Priority 3 calls are monitored internally but are not reported and do not form part of the external reporting suite.
7. Key Performance Indicators for GP Out of Hours ServicesThe service delivery KPIs for GP out of hours services include the percentage of calls attended to within the one, two or four hour time limit as determined by NHS24. However differences of opinion exist regarding clinical appropriateness of the timeframes advised by NHS24, and also different IT systems are used throughout NHS Scotland (for example Taycare and ADASTRA).
These data are not centrally collated and are reported only for local, internal Health Board review.
8. Key Performance Indicators for the Scottish Ambulance ServiceThe primary service delivery KPI for the Scottish Ambulance Service is the HEAT Standard (previous HEAT Target A3): 'Sustain response times to category A calls (life threatening emergency incidents) at 75% within 8 minutes in mainland Health Boards from March 2009.' Other KPIs not currently integral to the HEAT target structure include:
Improve response times to Category B calls (serious but not life threatening) to 95% within target times by 2009/2010; and
13

Improve response times to all emergency incidents on island NHS Health Boards to 50% within 8 minutes in 2009/2010.
The key performance indicators for the Patient Transport Service are punctuality for appointment and punctuality for pick up of priority patients.
Regarding the Emergency Medical Dispatch Centre (EMDC), the primary KPI is that 95% of all 999 calls directed to the Scottish Ambulance Service should be picked up within 10 seconds.
Meteorological data
9. The Meteorological Office was asked to produce a report comparing winter 2008-2009 with the Long Term Average (LTA) and with winter 2006-2007, as this was used as the comparator winter for hospital activity data.
10. The anomaly maps for temperature indicate that winter 2008-2009 experienced near average temperatures across Scotland (see Figure 1). However, when considering individual months, December had a below average temperature (see Figure 2). Air frost levels were variable when compared with the LTA (see Figure 3). Some central areas and coastal fringes in the east and north-west had a below average number of frost days; however, across the rest of Scotland the number of frost days was greater than average.
Key Learning Point 1: The mean temperature over winter 2008-2009 was in keeping with the Long Term Average, with December being a little colder than expected.
14

Figure 1. Mean temperature anomaly winter 2008-2009
Figure 2: Winter comparison of mean temperatures for Scotland 2006-2007 and 2008-2009
-2.0
0.0
2.0
4.0
6.0
8.0
10.0
12.0
Nov Dec Jan Feb
Tem
pera
ture
°C
WINTER 06/07
WINTER 08/09
LTA 1971-00
15

Figure 3: Days of air frost anomaly winter 2008-2009
16

Analysis of qualitative data
Likert Scale analysis
11. Each interviewee was asked to answer five simple questions, with their answers being recorded in the form of a Likert scale. The questions were as follows:
Question 1
The local health system coped well with winter pressures this year1 2 3 4 5 6 7Disagree Neutral Agree
Question 2
Areas of increased demand were accurately predicted 1 2 3 4 5 6 7Disagree Neutral Agree
Question 3
The Board’s winter plan prepared the local health system for the increased pressure1 2 3 4 5 6 7Disagree Neutral Agree
Question 4
If there were times that the system struggled to cope, was this due to factors within the NHS Health Board (primary/secondary care) or external agencies (e. g. NHS24/local authority services/Scottish Ambulance Service)? 1 2 3 4 5 6 7External Combination Internal
Question 5
If there were times that the system struggled to cope was this due to predictable or unpredictable factors, or a combination?1 2 3 4 5 6 7Predictable Combination Unpredictable
Interviewees were broadly grouped into one of three categories:
hospital management; secondary care clinicians; and representatives of GP out of hours services (both clinical and non-clinical).
17

The mean scores in each category are detailed in Table 1 below.
Table 1. Mean scores given on Likert questions by Clinicians, Management and GPOOH staff.
Question 1 Question 2 Question 3 Question 4 Question 5Clinicians (total)
4. 6 5. 0 4. 5 3. 9 3. 4
Clinicians (A&E)
3. 9 4. 9 4. 1 4. 0 2. 8
Management 5. 3 5. 5 5. 3 4. 3 3. 7GPOOH 5. 7 4. 7 5. 0 3. 4 4. 4
12. The number of participants was too small to allow meaningful statistical analysis of the responses. However, clinicians based in Emergency Departments typically disagreed with the statement that ‘The local health system coped well with winter pressures this year’. In contrast, representatives from the General Practice out of hours services tended to agreed with this statement.
13. Emergency Department clinicians felt that the pressures experienced over the winter were largely predictable, contrasting with GP out of hours representatives who felt these were marginally unpredictable. Perhaps the difference in opinions relates to the fact that predictors of activity in secondary care have become commonplace, driven by the unscheduled care collaborative. However, with the exception of NHS24’s modelling tool derived from Simul8, there are no formalised predictors used by out of hours GP services in Scotland.
Key Learning Point 2: Many of the pressures experienced across NHS Scotland over winter are the same pressures experienced at other times of peak activity throughout the year, and therefore are predictable.
Key Learning Point 3: Areas that Health Boards considered to be good practice, or to have had a positive effect in managing pressures over winter 2008-2009, are highlighted in the text with the Health Board emboldened. A more complete list, with contact details for the relevant people, is found in Appendix 3.
The winter planning process
14. The majority of Health Boards stressed that the concept of winter planning was becoming an outdated one, and that the emphasis should be on all year round capacity management in order to accurately predict demand, and detail contingencies to cope with these pressures. This general approach has been supported by the Scottish Government Health Directorates since 2003, when the Director of Performance Management and Finance wrote to all Health Boards stating:
“In light of the previous 3 years of effective winter planning and performance and the statement made in the 2002 Winter Report, that:
“…in 2003/04 the Department will move away from requiring a specific “winter” plan, leaving local systems to absorb these plans within the broader capacity issues …(but) we must not lose sight of the dangers that winter presents”
The department will not require you to submit a separate winter plan this year, since the previous arrangements, under which Health Boards submitted for the
18

Department’s approval a stand-alone winter plan, are now less necessary because capacity planning is firmly embedded in Health Boards’ normal planning cycles. Generating an additional plan would prove a low value additional burden that would create artificial boundaries in the local planning system and inhibit the seamless year round capacity planning required. ”
15. Almost all Health Boards felt that planning for the two holiday periods had been extremely robust, and had largely delivered to expectations. Many suggested that the focus of planning should be the start of January, when elective activity recommences and bed occupancy is very high.
16. Most Health Boards strived to develop whole system winter plans, involving the local CHPs (Community Health Partnerships) plus other partnership agencies such as NHS24 and the Scottish Ambulance Service in the planning process. Several Health Boards appointed CHP winter planning leads, which was generally felt to have improved the whole systems approach. However, it was felt by the majority of Health Boards that there was a lack of engagement with the local social work department, signified by their non-attendance at winter planning meetings.
17. Examples exist of Health Boards developing winter plans in a sectored manner, with the acute sector and primary care preparing separately. At times of peak pressure this manifested as poor partnership working, as different sectors failed to understand the demands on the whole system. Lack of predefined cross-sectoral roles and responsibilities led to some areas of the service being under severe strain whilst others had excess capacity, for example high acute hospital bed occupancy, whilst local community hospital bed occupancy remained below 70% (see Figure 10, p35).
18. Timescales for starting the winter planning varied between Health Boards from April to November. Some interviewees felt that the development of the winter plan was little more than a paper exercise, and that the plan and contingencies outlined were not utilised or relied upon on at times of pressure. Some interviewees at middle management level would welcome a return to the previous system of winter plans being submitted to the Scottish Government Delivery Directorate for centralised scrutiny, rather than simply confirming that preparations for winter had been developed.
NHS24
19. The NHS24 winter plan included a well defined and rehearsed escalation policy, in partnership with out of hours services and all the territorial Health Boards. For the three weeks over the festive period NHS24 staff rotas were suspended to allow matching of capacity to predicted activity. On days of peak predicted activity, NHS24 was staffed to maximum capacity.
20. The NHS24 modelling tool (derived from Simul8) was utilised to predict activity and was largely perceived to be accurate, with the exception of the weekend of 13/14 December and the two four-day holiday periods. It included HPS data and data from ‘flu spotter practices, and also factored in previous NHS24 activity. Predictions were disseminated to out of hours services as a guide to predicted activity.
19

21. In NHS Greater Glasgow and Clyde co-location of NHS24 with the GP out of hours hub, out of hours mental health service, and Scottish Ambulance Service at Caledonia House in Cardonald was universally acclaimed to improve partnership working. Examples of this include:
On Hogmanay, NHS24 call handlers, who had extra capacity, were able to assist SAS call handlers with non-999 calls, and General Practitioners working for the out of hours service were triaging 999 calls.
Following IT system failure of the out of hours system, General Practitioners were able to sit with NHS24 call-handlers and continue to take pre-prioritised calls until the IT system came back online 12 hours later.
NHS24 plan to co-locate their call centre with the SAS East EMDC.
On Christmas Eve, Health Protection Scotland informed NHS24 of increased ‘flu spotter rates in the community (specifically in Glasgow, Edinburgh and Aberdeen). The GP out of hours services was advised that they could issue anti-viral therapy. This led to a phone conference between the medical director of NHS24 and the directors of the out of hours GP services. The outcome was that NHS24 did not change its telephone advice to patients and did not mention antivirals. Consequently:
Four Health Boards accessed pandemic ‘flu supplies of oseltamivir (Tamiflu), but prescribed very small amounts
Nine Health Boards made the decision that attempting to access and prescribe oseltamivir would put the out of hours system under enormous pressure, and so made a positive decision not to access stocks.
One Health Board was unaware of the email.
The lack of consistency of response from NHS24 and HPS in relation to the same information resulted in local partners taking different courses of action, which caused unnecessary confusion. Scottish Ambulance Service
22. Each Scottish Ambulance Service division contributes to the overarching Scottish Ambulance Service Capacity Management Plan, which is also used for winter planning, and the Scottish Ambulance Service also contributes to territorial Health Boards’ winter plans.
23. Pressures on the Scottish Ambulance Service over the winter are related to increased demand, and adverse weather conditions such as icy roads which can significantly impair Category A response times. A further pressure highlighted at interview was the increasing need for secondary transfer, as some Health Boards increasingly adopt a policy of utilising several sites as a single bed base in order to cope with capacity issues.
24. SAS noted increased activity as early as 3 December, with SAS managers undertaking clinical roles. Activity peaked over Hogmanay and 2 January where, despite all call centres being staffed to maximal levels, on occasion call answering rates were reduced to 15% within the first 30 seconds. Note that co-location of the EMDC with NHS24 and the out of hours centre in Glasgow was advantageous as
20

NHS24 call-handlers handled some of the non-999 SAS activity, and General Practitioners assisted by triaging some of the SAS calls.
25. Throughout December and January there continued to be significant challenges with meeting the KPI for Category A and Category B calls, due to physical lack of room in the East EMDC. During 2009-2010 the East EMDC will quadruple capacity when it co-locates with NHS24 at South Queensferry.
26. The Scottish Ambulance Service achieved delivery of the HEAT A3 target in March 2009, reaching 77.4% of category A calls within 8 minutes on the Scottish mainland. This target has now become a HEAT standard. To achieve this, some SAS divisions were in escalation mode for the entirety of March, employed significant overtime, and sanctioned the use of extra vehicles, particularly in rural areas with longer response times.
Patient Transport Service
Please refer to Hospital Discharges (p37).
Out of hours General Practitioner Services
27. Feedback from the out of hours GP services across Scotland was largely positive, with the vast majority ascribing to the view that the difficulties in ‘coping’ by NHS Scotland over winter 2008-2009 were largely in the acute sector.
28. Winter plans, particularly for the two four day holiday periods, were felt to be robust. One Health Board, as part of their contingency plan, requested that primary care increase capacity in the three days between the holiday periods (29-31 December). This was felt to significantly reduce the pressures subsequently experienced by the out of hours service.
29. NHS24 issued modelling tool data to each Health Board to allow extrapolation and prediction of out of hours GP activity. Few Health Boards found this data helpful, with predictions of activity differing from actual activity by over 50% on occasions. The majority of Health Boards, although not using a formalised predictor of activity, used their own historic data in order to anticipate demand and plan capacity, and found this generally more reliable. There were some examples where activity peaked earlier in winter than expected (for example due to viral respiratory illness over the weekend of 13/14 December) and an increase in capacity for the corresponding weekend next year is planned by some Health Boards.
30. Some Health Boards (predominantly NHS Lothian and NHS Greater Glasgow and Clyde) handle a proportion of not immediate and life-threatening/not serious and urgent calls for NHS24, as pre-prioritised, or untriaged calls, at weekends. Over the two four day holiday periods this is extended to include all out of hours hubs. These calls are dealt with by General Practitioners without the NHS24 algorithm. Many Health Boards employed extra doctors over the Christmas and New Year holidays specifically to increase pre-prioritised call capacity. On two occasions during December weekends (due to IT failure and an unpredicted peak in activity) hubs were asked at exceptionally short notice to provide extra pre-prioritised call capacity, and had to bring in extra staff, or ask staff to work extended hours.
21

31. Once demand for NHS24 clinicians outstrips capacity then calls are handled via call-back, whereby the call-handler decides the triage category of the call and the patient is called back within an allotted time span. This places extra pressures on NHS24 and the out of hours GP service, as it shifts a significant proportion of the workload into the evening, when staff modelling is not matched to this demand. 32. There is an increasing move towards co-location of Emergency Departments and out of hours General Practitioner services to improve patient flow. In 21 out of 28 core hospitals (excluding paediatric hospitals), the two services are co-located. NHS Highland has moved to a fully integrated Emergency Department/GP out of hours service at Raigmore Hospital, with patients being triaged into either service on arrival. Across several NHS Health Boards there are issues with perceived patient ownership by Emergency Departments and GP out of hours services limiting partnership working. However, this winter other Health Boards saw >10% of self-referrals to the Emergency Department being referred to, and dealt with, by the GP out of hours service. In some Health Boards these patients are counted as attendances at both the Emergency Department and the out of hours service, which is inappropriate and inflates the attendance figures. This will be a focus of ongoing work with the Scottish Government HEAT T10 target.
33. There are two models of patient appointments employed by GP out of hours services. Most Health Boards operate a traditional appointments system, where patients are issued an appointment time at the nearest Primary Care Emergency Centre, depending on their NHS24 triage category (i.e. 1 hour, 2 hour or 4 hours). Health Boards operating this policy find this is the most efficient mechanism of controlling surges in demand. NHS Greater Glasgow and Clyde run a ‘no appointments’ system, whereby patients are asked to attend their nearest Primary Care Emergency Centre as soon as possible. The service feels that this eliminates a layer of clinical risk, where there is no delay in seeing patients, and also that patients are less likely to self-present to the Emergency Department whilst waiting for their appointment time. In order to manage surges in demand, a robust escalation policy is in place whereby if the waiting time to see a clinician exceeds one hour, then back up clinicians are called in from home.
34. The impact on in-hours primary care of having easily accessible out of hours primary care is unknown.
35. The Key Performance Indicators (KPIs) for GP out of hours services include percentage of home visits achieved within the 1 hour, 2 hour and 4 hour timeframes triaged by NHS24. However it is the perception of some clinicians that the referral algorithm employed by NHS24 is excessively risk averse, and that many home visits triaged for 60 minutes are inappropriate. Preliminary findings from an audit undertaken by Lothian Unscheduled Care Service along with NHS24 found that only 25% of requests for a 1 hour home visit could be validated, with a proportion being re-triaged as simple home care advice. Further work is currently being undertaken to examine this issue further.
36. Health Boards have differing practices for dealing with KPIs. In some Health Boards it is accepted practice that if a clinician makes telephone contact with a patient within the initial allotted timeframe (e. g. 1 hour), and re-triages him or her to a less urgent category (e. g. within 4 hours), then the 1 hour KPI is classed as having been met if the patient is seen within 4 hours.
22

37. Every Health Board increased GP out of hours services, for both clinical and non-clinical staff, over the festive period to a level they considered to be sufficient to cope with the increase in activity. A minority of Health Boards had difficulty in filling the clinical sessions, and some Health Boards cancelled non-clinical staff annual leave over this period. Several Health Boards noted that with the advent of the European Working Time Directive maximum 48 hour working week in August 2009, it will be difficult to fill clinical sessions for four day holidays in future.
38. Finally, almost all Health Boards flagged up Agenda for Change as posing significant challenges for the provision of out of hours services over the festive period. Non-clinical staff are already paid the unsocial hours enhancement in their salary and this may affect their willingness to work over the festive period.
Hospital admissions
Emergency Medicine
39. Patterns of access for hospital admission vary, with many sites continuing to operate a traditional single front door policy, where all admissions to hospital, including General Practitioner referrals to specialities, are admitted via the Emergency Department. Sites then differ with regard to whether GP referrals are left for specialists to assess in the department, or whether the Emergency Department initiates assessment.
40. Some of the teaching hospitals have adopted a direct admission policy, whereby if a patient presenting to the Emergency Department is deemed to require inpatient assessment, the patient can be transferred to the Acute Medical Unit without traditional referral. Data from NHS Greater Glasgow and Clyde suggests that this does not increase the proportion of patients admitted (of patients presenting with chest pain).
41. Other sites operate a model where General Practitioner referrals are admitted directly to the Acute Medical Unit, bypassing the Emergency Department. Many specialities (particularly haematology/oncology) continue to admit a proportion of patients direct to the speciality ward.
42. NHS Lanarkshire has established an Emergency Response Centre, a single point of contact for primary care to refer patients into secondary care across the entire health board.
43. Emergency Departments across NHS Scotland differs between Health Boards. Some units operate predominantly as a triage and resuscitation unit, booking downstream beds for patients on their arrival in the department, and providing minimal access to diagnostic services. At one site, to improve flow, patients are moved out of the Emergency Department to the Acute Medical Unit after 2 hours, regardless of whether or not a bed is available (in these circumstances they become a ‘corridor wait’). Furthermore, if no beds are available in the Admissions Unit, GP referrals to medicine are also treated as corridor waits but are not subject to the 4 hour Standard, which is not in line with the Scottish Government definition. Other Departments will instigate, and often complete, the diagnostic process, including GP
23

referrals to speciality. Several Emergency Departments have attempted to facilitate this process by opening Clinical Decision Units (CDUs).
44. Of the rural and island Health Boards, NHS Highland runs a fully integrated Emergency Department and GP out of hours service at two sites, where patients are triaged into either service on arrival. NHS Western Isles and NHS Shetland Emergency Departments are staffed primarily by Emergency Nurse Practitioners (ENP), with support from ward based medical staff, and NHS Orkney Emergency Department functions only as a minor injuries unit, with all GP referrals and emergency ambulance patients being admitted directly to the general ward. NHS Borders operates an ENP and GP led Emergency Department, with a Consultant in Emergency Medicine. Finally, NHS Dumfries and Galloway employ two consultants in Emergency Medicine, and will appoint three salaried General Practitioners in the department, working towards integration with GP out of hours.
45. Many Health Boards felt that if the Emergency Department comes under sustained activity pressure, then the default position is to admit a larger proportion of patients, easing congestion in the department, but increasing pressure on inpatient beds. However, data from this winter does not support this concept. Figures 4 and 5 demonstrate the number of attendances to the Emergency Department and proportion of patients admitted over December 2008/January 2009. Figure 4 is from a busy Emergency Department with significant medical staffing challenges, and here there is no impact of attendances on admission rates. Figure 5, from a busy Emergency Department with a full complement of medical staff, suggests that the proportion of patients admitted falls significantly with increasing attendance rate (r = -0. 4, p<0. 0001).
Figure 4.
Source: A&E Data Mart, extracted May 2009
A&E attendances per day vs proportion admitted - Dec 2008- Jan 2009 - Reduced staffing
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
100 120 140 160 180 200 220 240 260 280 300
24

Figure 5.
Source: A&E Data Mart, extracted May 2009
Key Learning Point 4: There is no evidence to support the belief that as Emergency Departments become busier, the proportion of patients admitted increases. Indeed, in well staffed departments the converse may be true.
46. Many Accident and Emergency Departments attempted to increase staffing levels over the winter and festive period. Some Health Boards did not allow nursing staff to take annual leave over the two four-day holidays. Additional junior medical staff were employed by some departments over the festive period, but significant issues with recruiting locum staff were again reported. NHS Lanarkshire employed additional consultant sessions over the winter weekends, and this policy is to be continued indefinitely.
47. As winter initiatives, NHS Lanarkshire and NHS Greater Glasgow and Clyde employed General Practitioners in the Emergency Department, with the aim of seeing patients suitable for primary care. These pilots were well received, with some GPs able to contribute to the overall activity in the department when there was less primary care activity, and more experienced GPs facilitating two-way learning. Other Health Boards are increasingly employing extended role nursing staff functioning as independent clinicians, with one example being MINTS (Major, Minor Illness and Injury Nurse Treatment Service) nurses in NHS Lanarkshire.
48. Many Health Boards (though not all) felt that winter was busier in terms of admissions, particularly over December. Also many clinicians referred to the fact that patients requiring hospital admission appeared to be more elderly and frail, with respiratory illness, a combination frequently associated with an increased length of stay.
A&E attendances per day vs proportion admitted - Dec 2008- Jan 2009 - Full staffing
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
200 220 240 260 280 300 320 340 360 380Attendances
Pro
po
rtio
n a
dm
itte
d
25

49. In the west of Scotland, there were a small number of exceptional days. On 2 December there was an unpredicted overnight freeze. Although the local authorities managed to grit roads, pavements were not gritted, and this resulted in the phenomenon known as ‘slippy Tuesday’. Emergency Department attendances in NHS Greater Glasgow and Clyde were 20% above the highest number ever previously recorded, and 55% above the normal activity. Although this did not translate into an increase in overall admissions of a similar magnitude (see Figure 6), surgical admissions were 75% above the average, and well above predictions for the day. This put extreme pressure on theatre services at a time when the elective programme was running at maximum capacity.
Figure 6.
Source: A&E Data Mart, extracted May 2009
50. NHS Greater Glasgow and Clyde opened Clinical Decision Units (CDUs) at Glasgow Royal Infirmary and the Southern General Hospital as winter initiatives, with patients being jointly managed by Acute and Emergency Medicine. In their experience these units functioned as an effective buffer against the 4 hour Standard, and were invaluable for times when surge management was necessary, such as on 2 December. Data from the Southern General Hospital showed that the CDU:
reduced the number of patients breaching the 4 hour Standard (now 98% for flow 2 and 3 patients and 99% for minor injuries);
reduced the length of stay for particular patient groups (for example chest pain); and
discharged 87% of patients without recourse to admission to a ward bed.
Originally undertaken as a winter initiative, the CDU has been adopted on a recurring basis by the board, opening from Monday to Thursday. Emergency Department Time Profiles
Emergency Department attendances and admissionsNHS Greater Glasgow and Clyde winter 2008-2009
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Total A&E attendances Admissions to same hospital Other ( not admitted) Transfers (admissions to other hospital)
26

51. In addition to the percentage of four hour breaches, analysis of the Emergency Department admission/discharge time profile can yield information regarding stability of the whole system. In a stable system deigned to assess, treat and admit or discharge patients timeously, the time profile should reflect a skewed distribution, with the majority of patients admitted or discharged within three hours.
52. Figure 7 is a four hour time profile from an Emergency Department of a well performing site during December 2008, and as can be seen, the distribution is skewed to the left. However in a department with a significant exit block, the peak of admissions/discharges would be shifted significantly to the right. This can be seen in Figure 8, which is an Emergency Department time profile from a poorly performing site over December 2008. Note that the peak time for patients to be moved out of the department (admitted to hospital or discharged) was 3 hours 55 minutes.
Figure 7.
Source: A&E Data Mart, extracted May 2009
Figure 8.
Emergency Department time profile Dec 2008Good performance
0
5
10
15
20
25
30
35
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00
Waiting Time (Hours)
No
. o
f A
tten
dan
ces
27

Source: A&E Data Mart, extracted May 2009
Staffing Issues
53. Staffing levels in Emergency Departments across Scotland vary widely, with consultant cover being a particular issue for certain Health Boards with split site working. The past year, and particularly winter, has seen increasing challenges for Emergency Medicine (and other acute specialities including acute medicine, acute surgery, paediatrics and obstetrics and gynaecology) in terms of filling rota slots. There have been two main reasons for this. If speciality trainees drop out of rotation then, because recruitment is now nationally driven and occurs annually, there can be a delay of many months before the post is refilled. Secondly, many trainees on General Practitioner Vocational Training Schemes (GPVTS) are taking maternity leave (approximately 75% of medical graduates are now female). As trainees are changing placements every four months, this has meant that departments have been left with very short notice regarding staffing deficiencies. One district general hospital was given only four months notice that 3 out of 4 GPVTS trainees (37% of the total of Emergency Medicine junior staff) would not be undertaking their placements in December.
54. These staff shortages are compounded by the fact that Emergency Departments (and other specialities) find it difficult to employ locum staff, as doctors previously willing to undertake FTSTA posts have moved further afield, or entered GP training. Large central belt teaching hospitals are able to employ clinical assistants on an ad hoc basis, but this is rarely feasible outside Edinburgh and Glasgow. Several Health Boards have now amalgamated the funding available for FTSTA posts and established new consultant posts in Emergency Medicine and/or Acute Medicine.
55. Health Boards highlighted the perception that junior medical staff working in Emergency Medicine are increasingly more risk averse, and this can impact on attendance/admission ratios, particularly in sites with limited consultant presence.
Emergency Department time profile Dec 2008Poor performance
0
5
10
15
20
25
30
35
40
45
50
0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00
Waiting Time (Hours)
No
. o
f A
tten
dan
ces
28

This is a year-long problem, not specific to winter, but may be exacerbated by the increased volume of patients during this season.
56. These points were discussed with NHS Education for Scotland (NES). It was felt that Health Boards had been slow to adapt and restructure their workforce in accordance with the long-predicted fall in junior medical staff, resulting from implementation of the European Working Time Directive (EWTD). With regards to recruiting middle grade staff, the running of two recruitment rounds per year in specialities struggling to fill posts would be unlikely to improve matters, as the problem is a lack of applicants.
57. Furthermore, the difficulty in recruiting short or long term locums is thought to be largely a result of recent changes in immigration and employment laws, and is unlikely to change. However, more formal appointments for Training Programme Directors of GPVTS schemes are currently being made, increasing the likelihood of future employers being notified well in advance should a trainee intend to take maternity leave.
58. Finally the issue of junior doctors being perceived as less experienced, and therefore potentially more risk averse, was raised, and it was agreed that in the United Kingdom there had been challenges in implementing the EWTD and a resultant shortening in training. NES is focused on rethinking significant areas of training, increasing its intensity, and making service experience more telling.
59. There were also significant staffing issues with unfilled slots in junior doctor rotas in acute medicine, particularly outside Glasgow and Edinburgh. One Health Board also had critical issues with nursing staff shortage in the Acute Medical Unit over the festive period, despite suspending all annual leave, with off-duty nursing staff asked to remain ‘on-call’ at home.
60. There was little change to consultant physician working patterns over the winter with some exceptions:
NHS Lanarkshire increased to a two tier system of consultant receiving at one site (0900-1600, 1600-2300) and noticed a significant increase in the number of discharges and improvement in patient flow. This is now a permanent arrangement. Additionally, extra consultant physician sessions were employed over winter weekends and the festive period to discharge patients from downstream wards, with the aim that each patient was reviewed every 24 hours.
NHS Greater Glasgow and Clyde doubled the number of on-call consultant physicians at some sites at times of peak predicted activity.
NHS Lothian consultant physicians on-call worked until midnight during weekends of high activity.
Alternatives to admission
61. There were many acute medicine driven initiatives offering alternatives to hospital admission this winter. NHS Tayside developed an assessment room for ambulatory care and rapid assessment. Approximately 20% of GP referrals for admission were triaged into this service, saving 200 admissions per month. NHS Lothian successfully piloted a Mon-Fri daily rapid access medical clinic (via the Bed
29

Bureau) embedded within the MAU and offered to the GP at the point of referral. However NHS Greater Glasgow and Clyde found uptake of a similar clinic was disappointing, when offered as a stand-alone service. NHS Shetland consultant physicians offered an outreach service to care homes on the islands over the festive period, guaranteeing a review within 24 hours within the care home, as an admission avoidance initiative. Originally funded by EADT festive monies, this is still ongoing, funded by the Health Board.
62. NHS Lanarkshire has introduced the Emergency Access Programme Health Board, which is looking to redesign access to emergency care using a whole systems model. There are six streams, including:
primary care in hours; primary care out of hours; emergency care redesign; inpatient capacity management; information and performance management; and emergency response centre for NHS Lanarkshire.
The six work streams are underpinned by the Acute Access Action Group (AAAG) which consists of senior clinicians and managers from primary and secondary care. This group met weekly over the winter period to discuss four hour breaches and significant issues relating to access to emergency care.
Capacity and demand within secondary care
Predictors of activity
63. Nine out of Scotland’s 14 territorial NHS Health Boards have an internally developed tool for predicting unscheduled activity. The majority of these Health Boards also predict elective activity, although in every case the unscheduled activity predictor is considered to be more accurate, largely due to poor IT interface with surgical services. The predictors were largely developed during the Unscheduled Care Collaborative, are based on the previous six weeks’ activity and are used to accurately predict between two and 14 days in advance. One Health Boards’ predictor was found to consistently under-predict as it was based solely on data from winter 2007-2008, widely acknowledged to have been a quieter year.
64. The ISD predictor tool, System Watch, was used patchily throughout the NHS over winter, with most Health Boards preferring to rely on the internal predictor. A minority of Health Boards inputted System Watch into their own predictor tool. Reasons for lack of uptake of System Watch include:
perceived inaccuracy, particularly for smaller Health Boards; broad definition of medical admissions (e. g. including neurology) leading to
over-prediction; perceived complexity; and lack of awareness of its existence.
65. NHS Lothian used System Watch four months in advance to predict the number of capacity beds that would be required in January. The prediction was 140 beds, and the actual number required was 148; a difference of only 6%. NHS Forth
30

Valley also used System Watch, alongside its own predictor tool, in order to model elective activity, maximising elective activity at times of predicted low unscheduled activity, and running minimal elective activity (plus out-sourcing to external agencies) during the first three weeks of January when unscheduled activity was predicted to be high. There were no breaches of the 18 week RTT target.
66. Figure 9 demonstrates the System Watch prediction for August 2008-August 2009. It demonstrates activity beginning to increase at the start of November (earlier than predicted) but the short term prediction improves in accuracy after 2-3 weeks.
Key Learning Point 5: System Watch has a proven track record of accurate long, medium and short term prediction of unscheduled demand. All Health Boards should use System Watch routinely to predict activity, in line with current Government recommendations.
Figure 9.
Source: System Watch, accessed 9 June 2009
Bed meetings
67. Four Health Boards across Scotland do not hold daily bed meetings in their main hospital, even over the winter period (despite unscheduled care recommendations). Of the remaining 10 Health Boards, all sites had bed meetings at least once daily, with the vast majority holding them twice daily (and some three times daily over the winter period). Increasingly Health Boards are using their sites as a single bed base, alternating the admitting hospital and transferring patients depending on pressures within the whole system. If this has not been adequately planned in
31

advance with the Scottish Ambulance Service, it potentially results in pressure on Patient Transport Services and delays to patient transfer.68. The importance ascribed to bed meetings varies across the country. At one large teaching hospital site, which does not utilise a predictor and does not employ bed managers, bed meetings are described as entirely reactive with no forward planning and no ownership of patient flow. NHS Greater Glasgow and Clyde, however, monitors real time bed occupancy, whilst the bed management team at NHS Lothian assesses the actual empty bed base every morning and then looks at predicted admissions/discharges against actual admissions/discharges every two hours to determine bed status.
69. NHS Greater Glasgow and Clyde proactively employed an extra bed manager over the busy winter months, at the Western Infirmary. Furthermore, an additional bed manager was situated at the Victoria Infirmary twice weekly. Although this initiative was felt to have worked well, improving dynamic capacity management, interviewees felt that in retrospect the staff could have been employed four weeks earlier, in December, allowing a period of acclimatisation before the busy period.
70. NHS Lanarkshire has implemented a twice daily conference call between all three acute sites, during which the bed occupancy and escalation status of each site is discussed, and thus the escalation status of the Health Board is determined. The escalation status is then relayed to other stakeholders including primary care via email or text message. At times of peak activity over the winter this conference call included representatives from the out of hours GP service.
Key Learning Point 6: Daily bed meetings are necessary at every site. Twice daily bed meetings are necessary at core sites over the winter period.
Escalation plans
71. Each NHS Health Board has an escalation plan, but there is variation in the degree to which they are implemented. The three island Health Boards’ escalation plans are based simply on bed occupancy, and when this reaches maximal level (including all contingency beds) and there are no patients suitable for discharge, then elective activity is postponed. Following this, patients are transferred off the island, to NHS Grampian (NHS Orkney/NHS Shetland) or NHS Highland/NHS Greater Glasgow and Clyde (NHS Western Isles). These escalation plans were not required to be actioned this winter.
72. Nine of the 11 mainland Health Boards in NHS Scotland have a bed management escalation plan. However significant flaws were highlighted in several of these plans; for example one Health Board defined red alert as >100% bed occupancy, yet key areas of the hospital (for example CCU) would as a matter of normality always keep one empty bed, thus removing the ability to escalate to red alert. Another Health Board described misuse of the escalation policy, with district general hospitals closing and transferring admissions to the local teaching hospital, whilst retaining empty beds. Others described fear amongst hospital management to escalate beyond green and only executives on call having the ability to escalate to red alert.
73. There was a lack of knowledge, particularly amongst clinicians, regarding the specific local triggers for escalation. There was also a feeling in some hospital sites
32

that if the escalation plan were adhered to, then the escalation status would be red most of the time. Many interviewees commented that both internal and external stakeholders, particularly primary care, had become desensitised to the local hospital site escalating to status red, and hence little or no action was taken.
74. Community Health Partnership (CHP) involvement in escalation plans was variable between NHS Health Boards. In one Health Board an escalation plan was developed by CHP senior management, however CHP middle managers were not fully sighted on this and so were unable to respond when necessary.
Capacity Beds
75. Eight of the 11 mainland Health Boards (and two of the three island Health Boards) opened additional bed capacity in the main sites over winter 2008-2009. Only three acute sites opened previously closed wards, which were considered to be ‘winter wards’.
Other responses adopted by acute sites included:
opening wards normally closed at the weekend (predominantly ENT); opening closed surgical wards over the festive period; overnight utilisation of day-case unit beds; endoscopy unit beds; day hospital beds; and ad-hoc beds placed where possible in wards – for example in dayrooms.
The latter four of these are associated with an increase in clinical risk.
Some specific sites experienced bed reductions, for example:
23 beds closed in October at an acute elderly medicine site as a consequence of the Vale of Leven report; and
closure of some Community Hospitals and centralisation of services to improve patient care, however with reduced capacity on the acute site.
76. Concerns were raised about medical staff no longer having sufficient awareness of bed management. Indeed the perception of one senior clinician at a large teaching hospital was of the local system having ‘no pressure on beds over the winter. . . as elective activity is significantly scaled down. . . and therefore there are limitless beds to decant (board) into’. In reality this site did not postpone elective cases despite trolley waits in the Emergency Department, and medical wards were asked to accommodate extra capacity beds in non-clinical areas.
Key Learning Point 7: Consultant medical staff should have greater awareness of bed management issues. This includes Health Board and site escalation status and triggers.
77. The majority of the mainland Health Boards highlighted the under-use of bed capacity in Community Hospitals. This was a particular problem for larger, rural Health Boards where day-time bed occupancy in the acute sites was often reported to be approaching 100%, whilst in the affiliated Community Hospitals was as low as
33

65%. There were several factors identified as limiting factors in flow from the acute sector to community beds:
Availability of Patient Transport Services:
highlighted as a particular problem in transporting patients from the Emergency Department, when by definition only limited notice could be given to the Scottish Ambulance Service (though numerically the numbers of transfers from Emergency Departments and Acute Medicine Units is far smaller than from downstream wards).
Complex referral processes and pathways:
need for patients to be accepted for transfer to the community bed base by either General Practitioners or Medicine for the Elderly Consultants;
subsequent delays in review, or the referral process itself was rate limiting (for example the need for written referrals); differing practices for accepting patients for transfer (e.g. one community hospital would accept only one admission per day, regardless of bed occupancy); and some community hospitals will not routinely accept admissions out of hours, and are reliant on the out of hours service when they do.
Patient choice:
Large rural Health Boards may have community hospitals in sparsely populated areas many miles, and several hours travel, from the acute site. These sites tend to be under-utilised, predominantly due to patient choice.
78. Figure 10 illustrates bed occupancy at both core and non-core sites. Core sites are the 33 major hospitals within the Health Board that submit Emergency Department data to ISD. Non-core sites represent community hospitals, or hospitals with small Emergency Departments/Minor Injury Units only. Note that the graphed daytime bed occupancy of all Health Boards is less than the >100% at core sites during the winter which was reported by some. Reasons for this discrepancy include:
bed occupancy being measured at midnight; no electives at weekends; zero length stays; and day-case patients being seen in inpatient facilities.
Figure 10.
34

Source: ISD(S)1 Hospital Activity Statistics
Key Learning Point 8: Bed capacity in community hospitals was significantly under-utilised this winter.
Elective procedures
79. Differing policies on elective activity over the festive period were evident. Over the two week holiday period (22 December – 4 January), six Health Boards planned in advance to reduce elective activity to a ‘cancers and urgent only’ service, whereas eight Health Boards continued with a full elective programme until Christmas Eve, and then resumed it for the three days between holiday periods (one Health Board at 80% of capacity).
80. NHS Lanarkshire and NHS Highland front-loaded the week beginning 5 January with minor elective surgery to reduce surgical bed utilisation. For winter 2009-2010 NHS Lanarkshire is planning to back-load medical elective activity (such as clinics and endoscopy lists) for the first two weeks of January. NHS Borders continued to run a ‘cancers and urgent only’ service from 20 December - 12 January without triggering any 18 week RTT breaches. Finally NHS Forth Valley used System Watch to model its elective activity programme (see Predictors of Activity, p.30).
81. NHS Scotland is committed to delivering ‘a whole journey waiting time target of 18 weeks from general practitioner referral to treatment. . . by 2011’3. Health Boards pointed out that implementation of this target could potentially be seen as conflicting with the 4 hour Standard for access of emergency care, with emergency and elective patients vying for a finite number of beds. Interviewees from a significant minority of Health Boards stated that since the disbanding of the Unscheduled Care
3 NHS Improvement Plan : Putting people at the heart of public services. DOH, June 2004
Bed Occupancy levels for core and non-core sitesApr 2008-Mar 2009
70%
72%
74%
76%
78%
80%
82%
84%
86%
Apr-
08
May
-08
Jun-
08
Jul-0
8
Aug-
08
Sep-
08
Oct
-08
Nov
-08
Dec
-08
Jan-
09
Feb-
09
Mar
-09
% Bed Occupancy at core sites % Bed Occupancy at non-core sites
35

Collaborative and the reclassification of the 4 hour HEAT Target to a Standard of care, there had been a noticeable reduction in focus on emergency care, manifested by systems prioritising planned elective care in the following situations:
closure of surgical wards over the festive period (as elective activity was significantly reduced) and refusal to reopen them to accept medical patients, despite four and eight hour breaches in the Emergency Department;
Health Boards planning waiting list initiatives on 5 and 12 January despite predictions of very high unscheduled medical activity and high bed occupancy;
a Chief Executive refusing to sanction the postponement of non-urgent elective procedures despite the presence of excess trolley waits in the Emergency Department; and
the perception that there is 2% ‘room for manoeuvre’ within the 4 hour Standard, but that the 18 week RTT target is absolute.
Key Learning Point 9: In some Health Boards there was a reluctance to postpone elective procedures even when pressures in emergency care were rising.
Cancelled elective procedures
82. Over the winter period, all the island Health Boards and four of the mainland Health Boards did not cancel elective work due to lack of hospital beds. Five Health Boards cancelled activity in very small numbers (less than 15 cases each) and two Health Boards cancelled significantly more.
In one Health Board there was an increase in emergency orthopaedic admissions in early December, resulting in postponement of some elective surgery. This then put pressure on the 18 week RTT target over the winter period, resulting in waiting list initiatives in early January.
A second Health Board had a significant norovirus outbreak in late January/February, closing beds, which led to the cancellation of a number of electives.
Boarding patients
83. All 11 mainland Health Boards relied on a policy of boarding patients this winter. The largest patient group boarded were medical patients, though a minority of Health Boards also boarded surgical, orthopaedic and medicine of the elderly patients at different stages.
84. Few Health Boards have written protocols for boarding patients. Most aim to board stable patients with an established discharge date from the downstream wards. However the reluctance of wards to nominate patients for boarding was noted. Indeed one interviewee commented that it was not unusual for wards to fail to identify a single patient to board overnight, yet have a significant number of discharges before midday the following day. Failure to do this leads to an increase in boarding of patients from assessment wards or the Emergency Department. Although most sites stated that boarders were identified during daylight hours by consultant staff, in practice at times of pressure boarders should be identified by junior medical staff, nursing staff or bed managers at any time, and from any area of the hospital. A minority of Health Boards utilised ‘treat and transfer’ policies. For similar reasons, patients from the Acute Medical Unit (and rarely the Emergency Department) were
36

transferred in preference to stable ward patients, and not infrequently they were transferred to boarding beds in the receiving hospital.
85. Both boarding of patients and ‘treat and transfer’ policies are considered by the Scottish Government to be poor practice. This is especially the case when patients are boarded from Emergency Departments and Acute Medical Units. As part of the review, systems were asked how they would cope if the Scottish Government challenged the NHS in Scotland to eradicate or minimise the boarding of patients. 86. Many Health Boards struggled with this concept, highlighting that hospitals cannot run at >95% bed occupancy and accommodate seasonal variation in speciality admissions without boarding. However five Health Boards provided data that demonstrated a reduction in boarding, with NHS Greater Glasgow and Clyde having reduced boarding by over 70% since 2007, primarily by focusing on proactive discharge planning. Most Health Boards stated that their bed configuration was historical and not related to current patient need. NHS Highland significantly reduced boarding by reconfiguring 12 beds from surgery/obstetrics to medicine.
87. The method of recording boarding patient numbers varies between Health Boards. One Health Board only records boarders from Monday to Thursday. Data was in fact only available from selected sites from some Health Boards, and the format differed, meaning that comparison between Health Boards was not possible. Nonetheless, in a Health Board with a self-acknowledged problem with boarding patients, in January 2009 an unacceptably high proportion (up to 60%) of medical patients on one site were subject to boarding, accruing 5290 total boarded bed days for the month for the board, a total of 2.7 boarded days per bed in January. In contrast, NHS Highland recorded only 0.3 boarded days per bed in January.
Key Learning Point 10: All mainland Health Boards rely on a policy of boarding patients at times of increasing system pressure. The degree of boarding between Health Boards differs greatly, and some Health Boards have reduced boarding significantly. There has been an increasing move to board patients from Acute Medical Units, or Emergency Departments, before consultant review. Boarding must be reviewed and minimised.
Hospital discharges
Discharge planning
88. Different discharge planning models are in use across Health Boards in Scotland:
seven Health Boards primarily use Estimated Date of Discharge (EDD); two Health Boards primarily use Traffic Lights; two Health Boards use a hybrid model of Traffic Lights and EDD; one Health Board uses EDD aligned with Jonah’s theory of constraints; and two Health Boards have no discharge planning protocols.
In general Health Boards reported that Estimated Date of Discharge was variably employed across the organisation. Some reported that all patients were assigned an EDD on admission, but that discharge planning deteriorated once the patient was
37

transferred to an inpatient ward. However other Health Boards reported the opposite experience, where there was little or no discharge planning in the AMU, but a greater appreciation of the role of EDD on the wards, particularly in elderly medicine and surgery. Many Health Boards commented there was no ownership of the EDD, with consultant medical staff having little or no interest.
89. Regardless of which system was employed, there were significant doubts about accuracy of predictions. Managers commented on large numbers of patients with a ‘red’ traffic light being discharged at short notice, particularly from medical wards. Despite a general appreciation that morning discharges improve patient flow, and initiatives such as ‘two before ten’ being lauded as good ideas, this continues to be an issue for almost all Health Boards, with the median time of discharge at some sites being 6pm. Reasons highlighted included reluctance to use discharge lounges, risk averse junior medical staff awaiting consultant ratification of discharge, and delays in pharmacy supplying discharge medication.
Key Learning Point 11: Discharging patients early in the day is key to maintaining capacity.
90. NHS Lothian and NHS Grampian include the EDD as an integral part of the hospital bed management system and each patient must have an EDD within 24 hours of admission. However this data is not used as part of bed management predictions, being considered too unreliable. NHS Dumfries and Galloway re-piloted EDD with charge nurse and consultant ownership on a single medical ward as part of a rapid improvement event, and saw a significant improvement in length of stay.
Delayed discharges
91. NHS Scotland met the Scottish Government target of zero delayed discharges (>6 weeks in hospital after being declared medically fit) on the census date in April 2008 and April 2009, but not on other months (Figure 11). The target for zero delayed discharges in short stay beds was also met. The majority of Health Boards noted significant improvement in numbers of patients in delay. However large numbers of patients delayed <6 weeks continued to present significant challenges to a small number of Health Boards.
92. It was noted that although the zero target was met on the census dates, there were significant numbers of patients in the system over 6 weeks that were coded 71X (exercising statutory right of choice where an interim placement is not reasonable or possible) or 9 (complex discharges).
Figure 11.
38

Source: Delayed discharge census
93. Some Health Boards’ experience was of patients’ assessment of need being delayed until the six week target was threatened, thus allowing resource concentration on patients nearing the six week trigger. This was not the experience of any of the local authority representatives interviewed.
94. The rural and island Health Boards felt they had a particular problem of patient choice of care home. In low density populations, care homes are few in number and generally widely spread. Patients, perhaps not unreasonably, are not keen to live in homes many miles from (or indeed on separate islands from) their families. Furthermore, at the time of writing, there are currently no available care home beds in two of the three island Health Boards. Physical lack of carers was identified as a significant problem particularly for, but not limited to, the rural and island Health Boards.
Festive period discharges
95. Over the festive period, hospital discharges fell significantly across all Health Boards. This largely represents a fall in discharges from downstream wards, rather than from Acute Medical Units. Several reasons were highlighted:
A marked drive to discharge patients in the days immediately preceding Christmas. Patients remaining in hospital over Christmas are those who are not medically fit for discharge.
A common observation was the lack of social work availability over the festive period. Most Health Boards could restart care packages if a patient was admitted and discharged over the festive period (as the carers had not been re-allocated), but it proved very difficult to restart care packages over the festive period if patients had been admitted days earlier. Health Boards were generally unable to order new home care packages over the festive period.
Over the festive period, there was a reduced consultant presence on the downstream wards and in some cases patients did not have a medical review for four days. Some Health Boards attempted to minimise this problem. NHS Lanarkshire employed extra consultant physician sessions over the festive
Delayed discharges - Scotland - Jan 2006-Apr 2009
0200400600800
1000120014001600
Jan06
Apr06
Jul06
Oct06
Jan07
Apr07
Jul07
Oct07
Jan08
Apr08
Jul08
Oct08
Jan09
Apr09
Census month
No
of
pat
ien
ts
> 6 weeks
< 6 weeks
39

period and during the winter weekends, to ensure every patient in a downstream ward could be seen daily to identify potential discharges. There remains a historical reticence amongst some medical staff to discharge patients under the care of a different consultant.
Allied Health Professional support over the festive period varied across NHS Scotland. Many Health Boards were limited to on-call physiotherapy only. NHS Greater Glasgow and Clyde’s IRIS (Interdisciplinary Response and Intervention Service) and DART (Discharge and Rehabilitation Team) were available for six out of the eight festive days but reported that demand for their early supported discharge services was very low. The reasons for this were unclear, but may have been related to staff being unaware of their availability during the festive period. NHS Greater Glasgow and Clyde also piloted a winter initiative of the Emergency Department being able to restart homecare packages, as often they were cancelled before a decision was made to admit the patient to hospital. This was not felt to have been successful, as patients were often admitted too late to restart packages the same day. NHS Ayrshire and Arran rapid response team ran over the festive period, funded by festive monies from EADT.
The lack of diagnostics was not felt to be a significant rate limiting step, with most radiology departments running a weekend, or extended weekend, service over the festive period. NHS Fife ensured that investigations to support discharge, such as echocardiography and exercise tolerance testing, were timetabled at least every 48 hours over the festive period; however this is still longer than the average.
Patient Transport Service
96. The capacity of Patient Transport Services, particularly after 1700 in the evening and at weekends, was noted as being a significant barrier to discharge by almost every Health Board interviewed. The majority of PTS resources are targeted to match the operational requirements of non emergency outpatient models. As such, availability of PTS ambulances was perceived to be a particular problem in some Emergency Departments (and to a lesser extent, Acute Medical Units).
97. One Emergency Department kept a log of calls to the regional Patient Transport Service that remained unanswered after 120 minutes. The lack of a PTS ambulance was the underlying reason for 3 out of the 5 12 hour trolley waits in one Health Board over winter 2008-2009. Other Health Boards dealt with this issue by admitting the patient to wait for PTS.
98. Capacity and availability of Patient Transport Services was also a major rate limiting step in the transfer of patients from acute sites to community hospitals, particularly for rural or semi-rural Health Boards with the majority of bed capacity in primary care.
99. Several Health Boards funded increased capacity in PTS as an integral part of their winter plans. Other Health Boards purchased their own vehicles. In addition to this, at least four Health Boards employed private ambulance companies to transfer patients to peripheral hospitals. NHS Highland developed evening and weekend PTS by utilising their mental health ambulance, with joint funding between SAS and the acute division.
40

100. The Scottish Ambulance Service is acutely aware of the above issues and has highlighted the development of PTS as a key focus for 2009. It was suggested that some Health Boards may have developed a degree of automatic over-reliance on PTS when alternate transport modalities may be just as appropriate.
101. Recent data from patient satisfaction surveys has shown that a significant number of patients (>80%) who travel to hospital in a PTS vehicle for planned care regularly utilise private and public transport for non health related journeys. NHS Highland has a contract with the regional council taxi company, employing taxi drivers who undertake school runs (and thus have Disclosure Scotland clearance).
Social work
102. A lack of availability of social work for patient assessment or homecare provision was identified by Health Boards as a common issue, not just over the festive period but also in the lead up to Christmas and the New Year. A small number of Health Boards were informed by their corresponding social work departments that if complex discharges were not highlighted by mid-December then the discharge would not be supported until after the New Year.
103. Many social work employees take leave over the festive period, although measures have been taken by some Councils to prevent excess annual leave being taken at this time. Even when services have been provided during the festive period (for example increased availability of homecare managers and rapid response teams) then engagement has been minimal, suggesting a need for improved advance communication.
104. Nurses from the acute sector in NHS Greater Glasgow and Clyde can order homecare up to four times daily, seven days per week via a telephone hotline, without recourse to either occupational therapy or social work assessment. Nursing staff have found this significantly facilitates rapid discharge, with patients then being re-assessed in their home environment and the homecare package adjusted as necessary.
105. However, initial evidence has suggested that nursing staff are over-ordering, and this has led to some capacity issues in the community and delays in re-assessment. As a result of this a focused programme of nurse education is being introduced. Homecare ordering was also extended to 7 days per week over the winter for the non-acute sector (with patients being assessed in the normal manner) although demand for this was minimal.
106. Also in NHS Greater Glasgow and Clyde, a pilot of joint equipment stores (which are already in existence in other Health Boards) under the name ‘EquipU’ was undertaken. Equipment could be ordered from the EquipU website by hospital occupational therapists or nursing staff, and could be ready within 24 hours for urgent discharges.
107. Finally, social work reported the increasing issue of patients being discharged, primarily from the acute sector, without their care packages being restarted. This causes significant stress and distress to patients and their families. Additionally, the feeling persists amongst social work staff that the NHS is an increasingly risk averse
41

organisation, and that there are under-utilised opportunities for patients to be discharged to wait at home for a package of care (in cases when they will be receiving it for the first time).
Analysis of quantitative data
Long term trends
108. To understand the data presented on activity levels in NHS Scotland over winter 2008-2009, it is important to contextualise them with activity over a number of years. However it is difficult to use long-term trends as direct comparators, as there has been a significant shift in the model of service delivery in recent years. Data demonstrates that Emergency Department attendances in Scotland have been increasing year on year since 2004-2005, rising by about 50,000 per annum in these 3 years (Figure 12).
Figure 12.
109. The data for the above chart has been taken from ISD(S) 1 data to show historical trends. ISD Scotland were asked to develop a secure A&E Data Mart to serve as a repository for A&E data submissions, which was implemented in July 2007; from this time several NHS Health Boards have asked that this data source be used to complete the ISD(S)1 return.
110. A number of reasons have been suggested to underlie this increase in Emergency Department attendances:
public expectation; perceived accessibility of the Emergency Department; perceived inaccessibility of Primary Care services, particularly in hours; public awareness campaigns (e.g. FAST, dial 999 for chest pain); and NHS24 policies that are perceived by some to be risk averse.
42

111. Many of the reasons belying the increase in hospital attendances are equally applicable when attempting to understand the increase in admissions. Further important factors include:
the changing age demographic of the population; the improved management of chronic conditions, leading to an increasing
number of patients with chronic disease in the community; and a deterioration in social infrastructure and family support for elderly relatives.
Winter 2008-2009
112. Figure 13 shows monthly emergency admissions to hospital from February 2008 - January 2009. Note that admissions in December 2008 (the busiest month) are only 8% above the level in June/July (traditionally the quietest months). Admissions through the Emergency Department constituted 75% of total emergency admissions. The remaining 25% were admitted through Acute Medical Units or directly to wards.
Figure 13.
Source: A&E admissions from A&E Data Mart, Scotland emergency inpatient admissions from SMR01 linked catalog, updated 30 May 2009
113. In trying to assess whether winter 2008-2009 was a ‘busier’ year for the NHS in Scotland, then, different comparators were used:
winter 2006-2007 (winter 2007-2008 was widely perceived to have been atypical with regard to its low level of activity); and
comparison with composite means of activity from previous winters: 2003-2004, 2004-2005, 2005-2006, 2006-2007 and 2007-2008.
Emergency Department admissions vs all emergency admissionsFeb 2008-Jan 2009
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
Feb-
08
Mar
-08
Apr-
08
May
-08
Jun-
08
Jul-0
8
Aug-
08
Sep-
08
Oct
-08
Nov
-08
Dec
-08
Jan-
09
ED admissions All emergency admissions
43

114. Figure 14 gives an overall picture of activity in the Emergency Department across NHS Scotland over the winter (November to January) of 2008-2009. Attendances at the Emergency Department per day varied from 2509 (Christmas Day) to 4676 (2 December). Admissions to hospital from the ED varied from 835 (Christmas Day) to 1297 (29 December).
Figure 14.
Source: A&E Data Mart, extracted May 2009
115. Figure 15 shows emergency and elective admissions to hospital in Scotland over December 2008 and January 2009, and compares numbers with the five year mean for admissions in December and January. The graph demonstrates several spikes of activity, with some 400 patients per day above the five year mean level for December (a 30% increase). Overall emergency admissions to hospital in December were 7.9% above the five year monthly mean. There was a smaller 1.8% increase in emergency admissions in January, compared with the five year monthly mean.
Attendances, admissions and transfers from core Emergency Departmentswinter 2008-2009
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Total A&E attendances Admissions to same hospital Other ( not admitted) Transfers (admissions to other hospital)
44

Figure 15.
Source: SMR01 linked catalog, updated 2 May 2009
Table 2. NHS Scotland emergency and elective admissions Dec 2008 and Jan 2009 compared with the five year monthly mean
Emergency
Elective
2008/09 5yr mean Change 2008/09 5yr mean ChangeDecember 1471 1363 +7.9% 486 482 +0.8%January 1395 1369 +1.8% 528 561 -5.8%Total 2866 2732 +4.9% 1014 1043 -2.8%
Key Learning Point 12: Overall emergency admissions to hospital in Scotland were 8% higher in December 2008 compared with the monthly five year mean.
116. All admissions (including day-cases) to hospital over January/December 2008-2009 are seen in Figure 16. The lack of elective activity at weekends and the two four day holiday periods is clear. In the three days between the holiday periods, activity resumed at about 75% of normal for day cases, and about 60% for admitted surgery.
Scotland emergency and elective inpatient admissions winter 2008-2009
0
200
400
600
800
1000
1200
1400
1600
1800
2000
1st D
ec3r
d D
ec5t
h D
ec7t
h D
ec9t
h D
ec11
th D
ec13
th D
ec15
th D
ec17
th D
ec19
th D
ec21
st D
ec23
rd D
ec25
th D
ec27
th D
ec29
th D
ec31
st D
ec2n
d Ja
n4t
h Ja
n6t
h Ja
n8t
h Ja
n10
th J
an12
th J
an14
th J
an16
th J
an18
th J
an20
th J
an22
nd J
an24
th J
an26
th J
an28
th J
an30
th J
an
Emergency admissions 5-year-monthly-average Elective admissions 5-year-monthly-average
45

Figure 16.
Source: SMR01 linked catalog, updated 2 May 2009
Key Learning Point 13: Admitted elective activity in NHS Scotland on 22 December was 70% of a normal Monday, and on 29 December was 60% of a normal Monday.
117. Simply looking at numbers of attendances and admissions to hospital does not truly reflect the level of pressure that a system is under. Assuming that there are no rate limiting steps in patient flow; that the bed complement is adequate in both number and configuration, and that numbers of discharges at least equal numbers of admissions (i.e. the system has adequately planned capacity), then the system should remain stable, almost regardless of the demand placed upon it. Unfortunately this is rarely the case, and pressures in any or all of these areas are transmitted to the point of entry, resulting in four hour breaches in the Emergency Department, a marker of whole systems pressure.
118. This is highlighted in Figure 17, which shows admission/discharge profiles across NHS Scotland (from core sites) plus number of four hour breaches. There is a consistent admission/discharge profile in December, with peaks of admissions at the start of the week, mirrored by a peak of discharges towards the end of the week. Admissions outnumbered discharges every weekend (and on Mondays) with a surge of discharges on Christmas Eve. This was followed by the 11 day holiday period, and for nine of these 11 days, admissions outnumbered discharges.
119. The net effect was that hospitals were at high levels of bed occupancy when the elective programme restarted at full capacity on 5 January, resulting in a spike in four hour breaches. The system attempted to return to the previous
Scotland emergency and elective inpatient admissions including daycases winter 2008-2009
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Emergency Admissions Elective Admissions Elective daycases Emergency Daycases
46

admission/discharge profile over the following week, but had not recovered by the following Monday, 12 January, and further four hour breaches were noted.
Figure 17.
Source: SMR01 linked catalog, updated 2 May 2009
120. The well recognised large spike in hospital discharges on Christmas Eve does not compensate for the sustained lack of discharges for the following 11 days, evidenced by the low weekly discharge averages (Figure 18).
Key Learning Point 14: On 9 out of the 11 days of the festive period, admissions exceeded discharges, leaving hospitals with high bed occupancy and vulnerable for the restart of elective activity.
NHS Scotland admission/discharge profile with 4 hour breaches from core sites Dec 2008-Jan 2009
0
500
1000
1500
2000
2500
3000
3500
1st D
ec3r
d D
ec5t
h D
ec7t
h D
ec9t
h D
ec11
th D
ec13
th D
ec15
th D
ec17
th D
ec19
th D
ec21
st D
ec23
rd D
ec25
th D
ec27
th D
ec29
th D
ec31
st D
ec2n
d Ja
n4t
h Ja
n6t
h Ja
n8t
h Ja
n10
th J
an12
th J
an14
th J
an16
th J
an18
th J
an20
th J
an22
nd J
an24
th J
an26
th J
an28
th J
an30
th J
an
Number of Inpatient Admissions Number of Inpatient Discharges Number of 4 hour breaches
47

Figure 18.
Source: SMR01 catalog, updated 2 May 2009
The 4 Hour Standard for access to emergency care121. Although the largest number of 4 hour breaches occurred on 5 January, underperformance against the 4 hour Standard began in December (Figure 19). Figure 19.
. Source: A&E Data Mart, extracted May 2009
Number of inpatient discharges per weekDec 2008-Jan 2009 - by week ending date
0 2000 4000 6000 8000 10000 12000 14000 16000 18000
w k1 7th Dec
w k2 14th Dec
w k3 21st Dec
w k4 28th Dec
w k5 4th Jan
w k6 11th Jan
w k7 18th Jan
w k8 25th Jan
w k9 1st Feb
number of inpatient discharges
48

122. The major reasons for breaching the 4 hour Standard can be seen in Figure 20. 40% of breaches were caused by ‘wait for a bed’, the largest single category. The next largest category was ‘wait for first assessment’, the cause of 17% of breaches. According to Health Boards, waits for first assessment were caused by a combination of staffing challenges within Emergency Departments, and also overcrowding in the department when there was an exit block to patients leaving the department.
Figure 20.
Worryingly, there was an increase in the number of patients waiting for more than 12 hours on a trolley in the Emergency Department in December 2008 and January 2009 (Figure 21).
Figure 21.
Source: A&E Data Mart, extracted May 2009 (Fig. 21 & 22)
Reasons for 4 hour breaches Dec 2008-Jan 2009
0
500
1000
1500
2000
2500
3000
3500
Wai
t fo
r B
ed
Wai
t fo
r 1s
tA
sses
smen
t
Wai
t fo
rS
peci
alis
t
Clin
ical
reas
ons(
s)
Wai
t fo
r in
itial
A&
Etr
eatm
ent
Wai
t fo
rdi
agno
stic
ste
st(s
)
Oth
er
Not
kno
wn
Reason
No
. o
f B
rea
ch
ers
49

Patient characteristics
123. Along with the absolute number of patients being admitted to hospital, the admitting diagnosis, age and subsequent length of stay of the patients also impact on system capacity. Winter traditionally sees an increase in admission of elderly patients, and patients with respiratory diagnoses, both independently associated with an increase in length of stay.
124. Figure 22 depicts emergency admissions per age group from February 2008 to February 2009 in Scotland. Compared with summer (June-July 2008) there was an absolute increase of 12.5% in admissions of patients aged >70 years in December 2008/January 2009. The proportion of patients admitted being >70 years also changed from 33.4% to 34.8% from summer to winter.
However comparing winter 2008-2009 with winter 2006-2007, there was only an increase of 1.8% in number of patients >70 years admitted as an emergency. Also the proportion of patients admitted >70 years was similar (34.7% vs 34.8%).
Key Learning Point 15: Patients admitted as an emergency over winter 2008-2009 tended to be older that those admitted over summer 2008. However there was no difference in age profiles between emergency admissions in winter 2008-2009 and winter 2006-2007.
Figure 22.
Source: SMR01 linked catalog, accessed May 2009
125. Diagnostic codes on discharge were used to look at proportion of patients admitted to hospital with respiratory illness over winter 2008-2009, and compared with winter 2006-2007. Respiratory illnesses included, but were not limited to, upper and lower respiratory tract infections, pneumonia and influenza. Figures 23 and 24 show that, compared with winter 2006-2007, there was a small increase in patients admitted with respiratory illness from mid-December to early January. The mean number of patients admitted to hospital per week with a respiratory diagnosis from the
50

end of November to the start of February in 2008-2009 was 1701, compared with 1530 in 2006-2007, an increase of 11%. However in practice this equates to only 2 extra respiratory patients per day across NHS Scotland. Figure 23.
Source: SMR01 linked catalog, updated 2 May 2009.Respiratory diagnosis is based on the main ICD-10 diagnosis J01-J99Figure 24.
Source: SMR01 linked catalog, updated 2 May 2009Respiratory diagnosis is based on the main ICD-10 diagnosis J01-J99
Emergency admissions winter 2008-2009split by respiratory/non-respiratory diagnosis
0
2000
4000
6000
8000
10000
12000
Respiratory Admissions Non-respiratory admissions
Emergency admissions winter 2006-2007split by respiratory/non-respiratory diagnosis
0
2000
4000
6000
8000
10000
12000
Respiratory Admissions Non-respiratory admissions
51

Key Learning Point 16: Compared with winter 2006-2007 there was an 11% increase in patients admitted with respiratory disease over winter (December-January) 2008-2009. However in practice this equates to only a small number of patients in total.
126. Figure 25 looks at length of stay of patients admitted to hospital in Scotland as an emergency from February 2008 to January 2009. There was a 4% increase in number of patients staying in hospital >1 week from in December/January compared with June/July. However this is in keeping with the overall increase in admission to hospital, as the proportion of patients staying for >1 week was the same in June/July (26.4%) as in December/January (26.7%).
Figure 25.
Source: SMR01 linked catalog updated 2 May 2009. Analysis based on start date of a continuous inpatient stay
Key Learning Point 17: There was no disproportional increase in length of stay seen in patients admitted over winter 2008-2009 compared with summer 2008.
Special Health Board data
NHS24
127. NHS24 activity over winter 2006-2007 and winter 2008-2009 is displayed in Figure 26 below, with summer 2008 as a comparator. The festive period in 2006-2007 was busier than in 2008-2009. There was little seasonal variation in demand between non-holiday winter periods and the summer period.
52

Figure 26.
Source: NHS24
128. Figure 27 demonstrates that as demand on NHS24 increased over winter 2008-2009, a greater proportion of calls was passed to out of hours partners as pre-prioritised calls (from 5.2% of all calls during the week ending 2nd November to 11.3% in week ending 28 December). Bearing in mind that the total number of calls also increased during this period, this equated to an extra 4000 pre-prioritised calls. The proportion of total calls handled as call-backs also increased from 22.2% to 26.1% over the same time period, equating to an extra 7000 calls.Figure 27.
Source: NHS24
NHS24 Call demand Winters 2006-2007 & 2008-2009 and Summer 2008
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22week
no
of
calls
oct 06 mar 07 may 08 sep 08 oct 08 mar 09
Christmas week New Year week
53

Key Learning Point 18: As demand on NHS24 increased, a greater proportion of calls were passed out to GP out of hours services as pre-prioritised calls. There was a proportionally smaller increase in calls handled as outbound calls (call-backs).
Scottish Ambulance Service
129. Figure 28 shows Category A incidents by week, comparing winters 2006-2007 and 2008-2009. Over winter 2008-2009, there were 19.6% more incidents in December than in January. There was a 2% increase in activity over winter 2008-2009 compared with winter 2006-2007.
130. Figure 29 shows SAS performance in mainland Health Boards against the Category A calls Key Performance Indicator over winter (December/January) 2008, as compared with winter 2006-2007. All Health Boards demonstrated an improvement in winter 2008-2009 compared with winter 2006-2007.
Figure 28.
Figure 29.
Source: Orcon. Data extracted 29 May 2009, 1 June 2009 and 10 June 2009 (figures 28 & 29)
Category A incidents by week, mainland Scotland
54

GP out of hours services
131. Overall NHS Scotland data for activity of GP out of hours services is not available due to:
differences in IT systems being used (e. g. ADASTRA and Taycare); and potential inaccuracies in ADASTRA data from some Health Boards who did not
make it available for analysis.
Figure 30 shows out of hours GP activity in a single Health Board over winter 2008-2009, compared with summer 2008 and winter 2006-2007. Compared with winter 2006-2007, activity was 6.8% higher, and compared with summer 2008, activity was 29.7% higher.
Figure 30.
Source: ADASTRA Software Ltd
132. Figure 31 shows the same out of hours service performance against the 1 hour home visit KPI. Despite the nearly 30% increase in activity from summer to winter, there was no discernible drop in performance.
Key Learning Point 19: GP out of hours activity in one Health Board increased by 30% from summer 2008 to winter 2008-2009, with no drop in performance against the major KPI. Emergency hospital admissions increased by 8% from summer 2008 to winter 2008-2009.
55

Figure 31.
Summary, Conclusions and Recommendations
Summary
133. What is clear from both the national quantitative data and local enquiry is that pressure at the front door of the acute hospital is now felt all year round, although there remain some seasonal differences in acute hospital admissions. There is evidence, however, that the case-mix of patients admitted to hospital over winter 2008-2009 demonstrated a small increase in respiratory illness compared with winter 2006-2007. There was no evidence that patients admitted over winter 2008-2009 were older than in previous winters, or had a proportionally greater length of stay.
134. Figure 17 clearly demonstrates a consistent system throughout December, with admissions peaking at the start of the week, mirrored by a peak in discharges at the end of the week. Weekends demonstrated lesser activity but with admissions consistently greater than discharges. Throughout December, there was a considerable number of breaches, but this should be interpreted in the context of an 8% increase in admissions in December compared with the five year mean for that month (Figure 15).
135. The system then moved into a period of great instability, the festive period. This was characterised by a large volume of discharges on Christmas Eve followed by 9 out of 11 days where admissions exceeded discharges. This resulted in hospitals running at high levels of bed occupancy and being very vulnerable on 5
56

January, when the majority of sites recommenced their elective programs at full capacity. This resulted in a spike in four hour breaches and 12 hour trolley waits, and although the system quickly reverted to the previous admission/discharge profile, and admissions in January were similar to previous years, the system still had not recovered by the following Monday and a further spike in four hour breaches was observed.
136. The 11 day festive period is characterised by a lack of discharges. Primary reasons for this include:
a perceived lack of pressure on the system; reduced medical staff in downstream wards (senior and junior); and disruption of the normal discharge infrastructure including allied health
professionals and social care.
137. For five out of every seven years NHS Scotland will experience two four-day holiday periods within 11 days. This puts a large amount of pressure on NHS24 and the General Practitioner out of hours services. Over winter 2008-2009 these services coped well, with robust winter plans drawn up months in advance, and generally effective contingency plans. Data from one Health Board suggested that demand for GP out of hours service in winter 2008-2009 was 30% above that in the summer; with no discernible drop in performance indicators. The 8% increase in the number of hospital admissions resulted in a significant drop in performance against emergency care performance indicators. This is despite secondary care having access to accurate predictors of unscheduled care activity.
138. Although perceptions do persist regarding the potential risk adversity of NHS24 policies increasing strain on the out of hours service and Scottish Ambulance Service, increased partnership working between these stakeholders was noted and is encouraging.
139. Other significant factors that impacted on the NHS ability to cope with winter (defined as December to March) pressures included:
minimal use of long term predictive data; a reduction in numbers of, and perceived experience of, junior medical staff; difficulties with accessing the community bed base; and in some Health Boards, delayed discharges (both over and under 6 weeks).
140. In the majority of Health Boards the elective programme was recommenced at full capacity on 5 January. Many Health Boards felt that the 4 hour Standard and 18 week Referral to Treatment Target were competing, rather than complementary. Examples of this included keeping surgical wards closed over the festive period despite the presence of medical patients in the Emergency Department, and Health Boards undertaking waiting list initiatives on 5 January despite sites having high bed occupancy, with high levels of unplanned medical admissions predicted. Some managers across the system felt that a loss of corporate memory since the end of the Unscheduled Care Collaborative had manifested itself as de-prioritisation of the 4 hour Standard, as compared with current HEAT Targets.
141. Clinicians and junior managers in many Health Boards described the health system as being increasingly target driven. Objective evidence of this is seen with
57

the zero delayed discharges on the census dates in April, but at no other time, and the peak of discharges from the Emergency Department after 3 hours and 50 minutes. Although the intentions of such targets are unquestionably to improve patient care, we must bear in mind the findings of the Investigation into Mid-Staffordshire NHS Foundation Trust4 which asks trusts to ensure that a focus on elective work and targets is not to the detriment of emergency admissions.
Conclusions
The findings of this report are that over winter 2008-2009:
The staff of NHS Scotland worked exceptionally hard and delivered high quality healthcare to the population of Scotland.
Emergency admissions to hospital in December were 8% above the five year monthly mean, with a proportional increase in admissions of elderly patients, but no evidence of a disproportionate increase in length of stay. There was a small increase in respiratory illness compared with winter 2006-2007.
The NHS moved to an unstable admission/discharge profile over the 11 day festive period, with a significant fall in the number of discharges and a resultant increase in bed occupancy. This was compounded by a return to full elective activity on 5 January, in many instances driven by the 18 week Referral to Treatment Target.
In some Health Boards, routine elective work (and the 18 week Referral to Treatment Target) is being prioritised over emergency admissions (and the 4 hour Standard for access of emergency care).
All mainland Health Boards in Scotland used the boarding of patients outside their speciality wards as a solution to capacity issues. Increasingly patients are being boarded from Admission/Assessment Units, and in exceptional circumstances the Emergency Department. This should be considered an issue of clinical governance.
Delayed discharges, generally under six weeks, presented a significant challenge for some Health Boards this winter. Although numbers of delayed discharges >6 weeks have reduced significantly, there remain discrepancies in numbers reported to ISD, and actual numbers in hospital due to issues with coding.
Bed capacity in the community was significantly under-utilised this winter.
Winter pressure is something of a misnomer. The pressures experienced are rarely due to winter per se, but are more a result of the NHS’ (and partners’) management of the Christmas and New Year holiday periods.
4 http://www.rcn.org.uk/__data/assets/pdf_file/0004/234976/Healthcare_Commission_report.pdf58

Quoting one consultant in Emergency Medicine, “winter pressures are only winter pressures because we choose to make them thus, by closing down the system for two weeks at a time of increasing activity”.
Recommendations
These recommendations should be considered alongside the many examples of good practice detailed in Appendix 3 to this report.
Health Boards should ensure that their winter planning starts early and that the process includes Community Health Partnerships and Social Work Departments. There should be a clear relationship between the winter plan and pandemic ‘flu plan.
Integral to the winter plan should be the escalation plan. This should involve all stakeholders including Community Health Partnerships. This includes the utilisation of beds in Community Hospitals, and protocols for referral and transfer should be agreed to resolve issues relating to perceived bed ownership.
System Watch should be used systematically for long to medium term predictions of unscheduled activity, and predictions acted upon to create the necessary capacity, in terms of beds and to support initiatives to reduce admissions. Consideration should also be given to the use of System Watch for planning of elective activity over the winter months.
Daily bed meetings should take place at every site, and should occur twice daily during the winter period. Consultant medical staff should have greater awareness of bed management issues, including escalation plans for sites.
Health Boards should undertake more accurate modelling over the festive period to plan elective capacity and optimise the use of bed capacity, including maximising the bed capacity in community hospitals. This may then enable hospitals to reduce the number of elective admissions on the first Monday in January. Further consideration should be given to front loading the first week in January with minor procedures, and back loading with majors. Also medical elective activity (such as clinics and endoscopy lists) could be back loaded during this week.
Medical Directors should ensure that appropriate numbers of consultant medical staff are on site to deal with the predicted activity over the two week festive period.
Health Boards should aim to eliminate boarding of patients as a solution to bed capacity problems. Specifically, the boarding of patients from the Acute Medical Unit and/or Emergency Department should not occur (this includes ‘treat and transfer’ policies, with the exception of tertiary care referrals).
The level of discharges over the holiday period should be improved. This might include:
o increased consultant presence with dedicated discharge ward rounds in downstream wards;
59

o utilisation of a rapid response team (or equivalent) of AHPs with access to homecare packages without recourse to social work assessment; and
o re-energising and establishing ownership of the Estimated Date of Discharge policy, plus introducing Nurse Led Discharges (NLDs).
o Patients should be discharged early in the day, as this is key to maintaining capacity. Planning of discharge ward rounds should take this into account.
If all the above measures have been undertaken, including consultant review and discharge of downstream patients, and all capacity beds filled (including community beds) then the 98% standard for emergency access of care should be achievable. Health Boards should note that if there are ongoing difficulties then priority should be given to emergency admissions over routine elective procedures. The Scottish Government has, for the last 10 years, made it clear that clinical decision making always trumps routine elective targets.
Appendix 1: Questionnaire
The local health system coped well with winter pressures this year
1 2 3 4 5 6 7
60

Disagree Neutral Agree
Areas of increased demand were accurately predicted
1 2 3 4 5 6 7
Disagree Neutral Agree
The board’s winter plan prepared the local health system for the increased pressure
1 2 3 4 5 6 7
Disagree Neutral Agree
If there were times that the system struggled to cope, was this due to factors within the NHS board (primary/secondary care) or external agencies (e.g. NHS24/local authority services/Scottish Ambulance Service)?
1 2 3 4 5 6 7
External Combination Internal
If there were times that the system struggled to cope was this due to predictable or unpredictable factors, or a combination?
1 2 3 4 5 6 7
Predictable Combination Unpredictable
What were the main pressures your health system experienced during the winter of 2008/2009? When and where did they develop?
Overall, how well did your system cope with these pressures?
What would are you planning to do differently in winter 2009/2010
Pre Winter planning and escalation
Did you feel there is adequate support from the Scottish Government (financial or otherwise) for winter planning?
61

How were festive monies from the Scottish Government allocated, and what were the benefits gained?
Escalation plan
Within the winter plan was there an escalation plan?
When was it last updated?
Was the escalation plan rehearsed? (practical or table top only)
Who has the authority to enable the escalation plan?
Is there a predefined ‘trigger’ for enabling the escalation plan?
Was the escalation plan auctioned?
Knowledge of capacity and demand planning
Was use made of predictive and monitoring tools in planning for winter?
Use of capacity and demand planning
Did the predictive and monitoring tools accurately predict pressures on capacity and demand?
Specific actions to support increased capacity
What were the arrangements for the provision of extra medical staff? Were they appropriate and sufficient?
What were the arrangements for the provision of extra nursing/AHP/pharmacy staff? Were they appropriate and sufficient?
Were extra capacity beds identified? Were they used?
Were additional diagnostic services made available?
Was there a hospital manager on-site? Of what seniority? How many days per week (and hours per day)?
How often were bed meetings held? Were formal reports produced thereafter?
Was there a planned increase in OOHGP capacity for the winter (and festive) periods? Was it delivered?
62

What was the health board policy on elective procedures over the winter and festive periods? Were there any unplanned cancellations?
Did you have boarding patients? What would be the impact of implementing a policy to eliminate the practice of boarding patients?
Was there a special mechanism for discharge facilitation employed?
External agencies
Was access to local authority services problematic over the winter/festive periods?
Was there a planned increase in access to local authority service? Did this happen?
And finally…
Are you carrying out a local review of what happened this winter?
Furthermore additional questions (specific to an individual health board or stakeholder within that health board) are expected to be raised by analysis of the 2 week data regarding performance, and also by critical analysis of that health board’s winter planning strategy document.
Data will be obtained through a combination of System Watch, ISD and local enquiry
The datasets that will be analysed over the first 2 week period in January include (but are not limited to)
Emergency Department attendances per 100,000 population (referenced against a 10 year period)
Performance against the 4 hour standard
Number (and reasons for) of 12 hour breaches
NHS24 activity
999 calls
Contact with GP OOH services
Occupied bed days/LOS
Admissions to hospital (emergency/elective)
Presence or absence of boarding patients (outliers)
Delayed discharges
63

4 hour profile
Attendance/Admission ratio
Appendix 2: List of interviewees
Health Board Name Designation
NHS Ayrshire and Arran David Chung Clinical Director – Urgent/Emergency Care
NHS Ayrshire and Arran Liz Moore Health Care Director – Integrated Care & Emergency
64

Services
NHS Borders Philip Lunts Head of Service Improvement
NHS Borders Jacques Kerr A&E consultant
NHS Borders Sheena MacDonald GP and Associate Medical Director
NHS Borders Lynne Huckerby Unscheduled Care Operational Manager
NHS Dumfries and Galloway John Burns Chief Executive
NHS Dumfries and Galloway Jeff Ace Winter Planning Lead
NHS Dumfries and Galloway David Pedley A&E consultant
NHS Fife Janette BroganInterim Lead Nurse for Primary Care Emergency Service (PCES)
NHS Fife Colin Dewar Consultant, A&E
NHS Fife Andrea Wilson Director, Clinical Delivery Department
NHS FifeYvonne McCallion
Integrated Admission and Discharge Manager, Operational Division
NHS Fife Rob Cargill Clinical Director for Medicine
Fife Council Rona Laing Older People’s Service, Social Work Department
NHS Forth Valley Ian Aitken General Manager Medicine, Emergency Care & Rehabilitation Unit
NHS Forth Valley Lorna Henry Service Manager for Speciality Medicine
NHS Forth Valley Deirdre Anderson Service Manager OOH + Winter Planning
NHS Forth Valley Norman Peden Associate Medical Director
NHS Forth Valley Karen MacLure Service Manager Acute & Emergency Care
NHS Grampian Irene Jessiman Operational Support Manager
NHS Grampian Nick Fluck Medical Lead Acute Services
NHS Grampian Fiona MacKenzie Lead Nurse Acute Services
NHS Grampian George McLean Head of OOH
NHS Grampian Pauline Strachan Deputy Medical Director and Head of Primary Care
NHS Greater Glasgow and Clyde
Joan Barr Service Manager OOH
NHS Greater Glasgow and Clyde
Grant Archibald Director, Emergency Care & Medical Services
65

NHS Greater Glasgow and Clyde
Alastair Ireland Clinical lead of A&E City Wide
NHS Greater Glasgow and Clyde
David Stewart Associate Medical Director
NHS Greater Glasgow and Clyde
Fiona Bernklow Bed management
NHS Greater Glasgow and Clyde
Kevin BegbieInformation Manager, Unscheduled Care Collaborative
NHS Greater Glasgow and Clyde
Norrie Gaw Clinical Director, GEMS OOH
NHS Greater Glasgow and Clyde
Calum McLeod Head of Mental Health
Glasgow City Council Nick KempeHead of Strategic Management and Disability, Local Authority
NHS Highland Iona McGauran Nurse Manager for Medical Directorate
NHS Highland Richard Bennie Manager in Emergency Department
NHS Highland Lorraine Beigley HUB Manager
NHS Highland Stuart Caldwell Head of Service Redesign
NHS Lanarkshire Rosemary Lyness Director of Acute Services
NHS Lanarkshire Mary Thom Bed Management
NHS Lanarkshire Alan Lawrie Director of South Lanarkshire CHP
NHS Lanarkshire Veronica Devlin Emergency Access Programme Manager
NHS LanarkshireJohn Keaney
Clinical Director for Medical Directorate, Hairmyres Hospital
NHS Lothian Andy Jackson Associate Director of Strategic Planning
NHS Lothian Alisdair Gray Clinical Lead for Emergency Medicine
NHS Lothian Casey Stewart Clinical Director for Medicine
NHS Lothian Brian Montgomery Associate Medical Director
NHS Lothian Marion Storrie Clinical Director of LUCS
NHS Lothian Angela Tuohy Bed Management
NHS Orkney Rhoda Walker Director of AHP, Nursing, Planning & Performance
NHS Orkney Mark Clouston Head of Performance and Delivery
NHS Orkney Peter Gent Acute Services Manager
NHS Shetland Simon Bokor- Director of Clinical Services
66

Ingram
NHS Shetland Ken Graham Medical Director
NHS Tayside Carol Goodman Head of Capacity and Flow
NHS Tayside Joyce Meikle Medical Director OOH
NHS Tayside Arun Chaudhuri Acute Receiving Physician
NHS Tayside Meg Park Clinical Team Manager/Senior Nurse
NHS Tayside Shobhan Thakore Clinical Lead, A&E Services
Dundee City Council Stewart Watt Older people service manager
NHS Western Isles Sheena Wright Interim Nurse Director/ Chief Operating Officer
NHS Western Isles Brian Michie Interim Medical Director
NHS Western Isles Gordon Jamieson Chief Executive
NHS24 Janice Houston Associate Director of Operation and Nursing
Scottish Ambulance Service Peter Connor Head of Ambulance Services - Edinburgh
Scottish Ambulance Service Grant Leslie General Manager of EMDC
NHS Education for Scotland Mike Watson Medical Director of NES
Health Protection Scotland Jim McMenamin Consultant Epidemiologist
67

Appendix 3: Examples of good practice
The following are examples of good practice highlighted by NHS Boards during the visits across Scotland. Some were specific winter initiatives, and some were simply initiatives in order to improve aspects of system working. Contact details are provided for each initiative, and protocols, where available, are provided.
The initiatives can be divided into several main categories:
A. Winter Planning
B. Out of Hours GP services
C. Emergency Medicine
D. Medicine
E. Predictions of Capacity and Demand
F. Bed Management
G. Elective Activity
H. Discharges and Social Work
I. Mental Health
J. Emergency Access
A. Winter Planning
Most (though not all) Boards developed whole system winter plans with varying input from local authorities and CHPs. NHS Greater Glasgow and Clyde was perhaps the most all-encompassing of the large Boards, involving input from primary care and social work via the CHCP model.
Of the smaller Boards, NHS Borders also adopted an excellent whole system approach.
Of the hybrid rural/urban Boards, NHS Ayrshire and Arran produced a whole systems winter plan that was notable for its engagement with the three local authority services, each of whom appointed a lead for winter planning.
68

B. Out of Hours GP Services
In many Boards, but not all, the Emergency Departments and GPOOH centres are co-located. The experiences of this are largely positive, with some Emergency Departments transferring up to 15% of self-referrals to the Primary Care Emergency Centre.
NHS Borders implemented a novel scheme of primary care input into secondary care, whereby experienced General Practitioners would assess and discharge in-patients. This model was employed predominantly at periods of peak pressure, such as throughout January. In a single sweep of in-patients in the Borders General Hospital in January, 21 patients were identified who could be discharged with support or transferred that day.Sheena MacDonald ([email protected])
NHS Ayrshire and Arran out of hours GP service introduced a ‘Single Point of Contact’ (SPOC) for people contacting the service, in order to signpost them to services that were available and accessible out of hours (including community care). This could involve:
starting a new homecare package; restarting a homecare package; and arranging a GP to revisit vulnerable patients at home.
The main aim in developing SPOC was to facilitate home care support, enabling those clinically appropriate groups of patients to remain at home, prevent their admission to hospital and support their early discharge.Liz Farquhar ([email protected])
In NHS Greater Glasgow and Clyde the hubs for NHS24, SAS and GPOOH services (including mental health OOH services) are co-located and this facilitates partnership working during times of peak demand.
On Hogmanay, NHS24 call handlers, who had extra capacity, were able to assist SAS call handlers with non-999 calls, and General Practitioners working for the out of hours service were triaging 999 calls.
Following IT system failure of the out of hours system, General Practitioners were able to sit with NHS24 call-handlers and continue to take pre-prioritised calls until the IT system came back online twelve hours later.
Janice Houston ([email protected])
NHS Fife operated a ‘see and treat’ paramedic vehicle staffed by an extended role paramedic and an Emergency Nurse Practitioner. This vehicle attended both 999 calls (70% of activity) and GP out of hours calls (30% of activity). 60% of the patients they saw remained at home and the proportion of 999 calls being transported to the Emergency Department fell from 91% to 37%.Janette Brogan ([email protected])
NHS Lothian employed paramedic practitioners as part of its out of hours clinical workforce, functioning as independent practitioners. Furthermore, collaborative work is being undertaken between Lothian Unscheduled Care Service and the Scottish Ambulance Service to reduce hospital admissions, whereby if a patient is deemed not
69

to require transfer to hospital then the assessing paramedic can refer them directly to the out of hours GP service. Marion Storrie ([email protected])
NHS Greater Glasgow and Clyde arranged with primary care, through the GP sub-committee, to increase the number of appointments available to patients on the days between the festive periods (i.e. 29/30/31 December) so that the second four day holiday would be less demanding. This was considered to have worked well. Norrie Gaw ([email protected])
NHS Tayside staffed their Minor Injury Units with GPs for walk-in clinics over the festive periods. This was considered to have worked very well, and GPs saw up to 30 patients in any one session. This was considered to have reduced the local workload on the Emergency Department and NHS24.Joyce Meikle ([email protected])
NHS Western Isles utilised the District Nurse out of hours service (which is embedded within the GP out of hours service) to provide a revisiting service (more than once per night if necessary) for patients that the General Practitioners were concerned about leaving at home. This service operates 365 nights per year and is considered to have prevented a significant number of admissions.Brian Michie ([email protected])
C. Emergency Medicine
NHS Greater Glasgow and Clyde opened up Clinical Decision Units (CDUs), aligned with the Emergency Departments in the Southern General Hospital, Glasgow Royal Infirmary and Stobhill Hospital. Patients were jointly managed between Emergency Medicine and Acute Medicine. These units were considered invaluable in maintaining patient flow and achieving the 4 hour Standard during times of greatest demand, particularly at Stobhill hospital. The CDU at the Southern General Hospital was initially a winter initiative, but has been adopted on a recurring basis by the NHS Board, functioning from Monday to Thursday. The local experience is that this unit has:
significantly improved surge management in the Emergency Department; reduced the number of patients breaching the 4 hour Standard (now 98% for
flow 2 and 3 patients and 99% for minor injuries); reduced the length of stay for particular patient groups (for example chest
pain); and allowed 87% of patients to be discharged without recourse to admission to a
ward bedAlastair Ireland ([email protected])
NHS Lanarkshire employed extra consultant sessions in Emergency Medicine over the festive periods and over the winter weekends, funded from Health Board festive monies. This was considered so successful in terms of flow through the patient departments that weekend working has now continued routinely. John Keaney ([email protected])
NHS Dumfries and Galloway are due to appoint three salaried General Practitioners who will work in the Emergency Department overnight, and also see primary care
70

patients. This is considered locally to be a cost effective manner of establishing an out of hours middle grade Emergency Department rota.David Pedley ([email protected])
D. Medicine
NHS Lanarkshire employed extra consultant physicians over the winter weekends to specifically do ward rounds on the downstream wards to discharge patients. This was also employed over the festive period, in an effort to ensure that each patient in a downstream ward was seen every 24 hours. Veronica Devlin ([email protected])
NHS Lanarkshire have also moved to a two tier physician on-call rota at Wishaw General Hospital (0900-1600, 1600-2300) and have noted significant improvements in patient flow, and a reduction in medical admissions. Veronica Devlin ([email protected])NHS Lanarkshire piloted a system where respiratory specialist nursing staff see referrals to medicine (from the Emergency Department or General Practitioner) with COPD in the Emergency Department or assessment unit, and directly discharge them home with support.Veronica Devlin ([email protected])
In NHS Fife consultant physicians ensured every patient in a downstream bed was reviewed at least every 48 hours over the festive holidays. Furthermore, arrangements were made so that investigations to facilitate discharge (e.g. echocardiography, exercise tolerance tests, DVT clinics) were available at least every 48 hours over the festive periods. Rob Cargill ([email protected])
NHS Greater Glasgow and Clyde doubled the number of on-call physicians at busy sites at times of peak demand, for example 5th-7th January. Grant Archibald ([email protected])
NHS Tayside employed clinical assistants to work within the admissions unit and set up an ‘Assessment Room’, into which they streamlined appropriate patients (ambulatory care, rapid access out-patient clinic patients). They estimate this has saved 8 admissions per day (20% of total activity). Carol Goodman ([email protected])
NHS Tayside have successfully established a short stay ward for medical admissions with a predicted LOS of <72 hours. Carol Goodman ([email protected])
NHS Shetland consultant physicians provided an outreach service to care homes in the area over the holiday periods. Patients were guaranteed to get a consultant review in the care home setting within 24 hours. Originally funded by EADT festive monies, this has been a success in preventing admissions and is still ongoing, now funded by the NHS Board. Simon Bokor-Ingram ([email protected])E. Predictions of Capacity and Demand
71

NHS Lothian used Systemwatch as early as September to predict activity levels in January. Proactive efforts were then made to put contingencies in place to be able to open the predicted number of beds when needed, particularly in primary care. Alongside contingency planning to open capacity beds, efforts were also focused on admission avoidance initiatives, effectively delivering ‘bed equivalents’. The predicted number of extra beds needed was 140, the actual number of actual beds needed was 148. Andy Jackson ([email protected])Throughout the winter period, NHS Forth Valley utilised Systemwatch along with their internal predictor two weeks in advance. Elective activity was then aligned to this prediction, with pre-loading of elective activity in early December and running minimal elective activity in early January. There was some out-sourcing of elective activity to external providers. All 18 week RTT targets were met. Ian Aitken ([email protected])
Both NHS Lothian and NHS Lanarkshire have discharge predictors based on previous activity rather than on expected date of discharge. Both predictors are used on a daily basis along with predicted admissions to proactively manage bed capacity. Angela Tuohy ([email protected])Veronica Devlin ([email protected])
F. Bed Management
NHS Greater Glasgow and Clyde proactively employed an extra bed manager at the Western Infirmary over the busy winter months. Furthermore, an additional bed manager was situated at the Victoria Infirmary twice weekly. Although this initiative was felt to have worked well, improving the dynamic capacity management, with retrospect the staff could have been employed four weeks earlier, in December, allowing a period of acclimatisation before the busy period. Fiona Bernklow ([email protected])
NHS Lanarkshire has twice daily bed meetings and a twice daily conference call between all three sites, at which the escalation status per site and for the Board overall is decided. This is then relayed by text/GP to primary care. Veronica Devlin ([email protected])
The bed management team at NHS Lothian assess the actual empty bed base every morning and then look at predicted admissions/discharges against actual admissions/discharges every two hours to determine bed status. This is then escalated if necessary. Angela Tuohy ([email protected])
G. Elective activity
Most Boards had a 2 week ‘cancers and urgent’ service and then went back to full activity on Monday 5 January. This caused significant problems in many areas on 5 January. Other Boards adopted a different approach.
NHS Borders had a three week ‘cancers and urgent only’ policy, restarting the elective programme on 12 January. There were no 18 week RTT breaches.
72

Rachel Bacon ([email protected])NHS Forth Valley utilised Systemwatch along with its own internal predictor two weeks in advance. Elective activity was then aligned to this prediction, with pre-loading of elective activity in early December and running minimal elective activity in early January. There was some out-sourcing of elective activity to external providers. All 18 week RTT targets were met. Ian Aitken ([email protected])
NHS Lanarkshire front loaded the week of 5 January with minors (mainly day case surgery) to ease pressures on in-patient beds. Veronica Devlin ([email protected])
H. Discharges/Social work
Rapid response teams (generally a hospital social worker with guaranteed access to care packages) worked well across many Boards, particularly when engaged over the festive periods. Additionally, many Boards purchased extra capacity from the SAS Patient Transport Service.
NHS Highland utilised their mental health ambulance as additional PTS in the evenings and at weekends. This was joint funded between SAS and the NHS Board.Iona McGuaran ([email protected])
NHS Greater Glasgow and Clyde implemented a system whereby nursing staff from the acute sector could telephone a ‘hotline’ and set up care packages up to four times daily, seven days per week. Patients did not need to be reviewed by a social worker or occupational therapist. This has facilitated discharge significantly. Nick Kempe ([email protected])
NHS Greater Glasgow and Clyde increased homecare ordering from 5 to 7 days per week over the winter period.Nick Kempe ([email protected])
NHS Greater Glasgow and Clyde also use joint equipment stores (EquipU) with internet based ordering that can be accessed by nursing staff, or occupational therapy staff. Equipment can be provided within 24 hours from the order being placed.Nick Kempe ([email protected])
Due to local pressures which arose, NHS Dumfries and Galloway are now putting in place care packages and charging back the costs to the social work department. Patients do not have to wait to be assessed by a social worker. The local experience is that the care packages are delivered more consistently with the re-enablement model than previously. Jeff Ace ([email protected])
NHS Fife employed an extra discharge support nurse over the winter period so that both hospital sites would be covered. Yvonne McCallion ([email protected])
73

In NHS Lothian the Estimated Date of Discharge (EDD) is an integral part of the bed management IT system; each patient needs to have an active EDD entered, and it is a mandatory requirement that it is updated for each patient daily. Angela Tuohy ([email protected])
In NHS Grampian the homecare co-ordinator visits the MAU on a daily basis (5 days per week) and supports early discharges from the department. Irene Jessiman ([email protected]) NHS Lanarkshire increased the working of discharge teams from 5 days to 7 days per week over the winter period. Veronica Devlin ([email protected])
NHS Lothian has introduced the IMPACT team (Improving Anticipatory Care and Treatment). This team have a caseload of patients with chronic conditions, whom are managed at home. If the patients are admitted, the IMPACT team can expedite discharge and provide increased support at home. Brian Montgomery
In NHS Lothian all Occupational Therapists can access 7 hours homecare per week without recourse to social worker assessment. A pilot study is ongoing regarding extending this to 14 hours per week. Claire Gordon ([email protected])
NHS Lothian employed a roving AHP team specifically for winter/boarding patients. The team, consisting of senior PT, senior OT, and PT assistant was based in the winter ward, but provided dedicated outreach to boarding medical patients (it was felt that ward AHPs were unable to sufficiently prioritise boarding patients rehabilitation). It was Health Board funded with three months of non-recurring money.Iain Duguid ([email protected])
NHS Tayside purchased 23 beds from a private care home, and used these for Intermediate Care patients. Rehabilitation was provided by NHS Tayside physiotherapy and occupational therapy staff, and care was provided by the care home staff. This initiative was utilised for patients with a predicted length of stay of <42 days, and significantly eased bed pressures in the acute sector.Carol Goodman ([email protected])
NHS Tayside employed physiotherapists and occupational therapists in the AMAU over all four public holidays and four weekend days, enabling and facilitating discharge.Carol Goodman ([email protected])
I. Mental Health
NHS Greater Glasgow and Clyde involved their addictions service in festive planning. They proactively contacted their most vulnerable patients and also ensured that prescriptions were filled in advance etc. Calum MacLeod ([email protected])
74

NHS Highland introduced extra alcohol liaison nurses (Community Psychiatric Nurses) in the Emergency Department at Raigmore hospital. This extra resource was deployed at the end of January, when attendances to the ED by patients with alcohol dependency are historically at their highest.Stuart Caldwell ([email protected])
NHS Grampian used festive monies to place Community Psychiatric Nurses in the GPOOH centres. They felt that this improved patient flow, as patients with mental health problems can be time consuming for GPs to deal with, and CPNs generally have more experience with this patient group.Pauline Strachan ([email protected])
J. Emergency Access
NHS Lanarkshire has established an Emergency Response Centre – a single point of contact for primary care to refer patients into secondary care across the entire Health Board. Veronica Devlin ([email protected])
NHS Lanarkshire has introduced the Emergency Access Board, which is looking to redesign access to emergency care using a whole systems model. There are six streams, including:
Primary care in-hours Primary care out-of-hours Emergency care redesign In-patient capacity management Information and performance management Emergency response centre for NHS Lanarkshire
The six work streams are underpinned by the Acute Access Action Group (AAAG) which consists of senior clinicians and managers from primary and secondary care. This group met weekly over the winter period to discuss four hour breaches and significant issues relating to access to emergency care. Veronica Devlin ([email protected])
75

Appendix 4: Festive monies
Each of the 14 health boards were invited to submit bids for festive monies. The aim of these initiatives was primarily to strengthen primary care out of hours services over the festive periods. A brief summary of the successful bids and initiatives follows.
NHS Ayrshire and Arran increased the working hours of their rapid response teams to include winter weekend and festive period working. These teams worked in the acute sector and highlighted patients for early supported discharge. Additional district nursing staff were employed within each local authority area to increase capacity, supporting additional referrals from the rapid response team. This initiative was felt to have had a significant positive impact over the winter.
Festive monies were also used to help establish the Single Point Of Care (SPOC) for the GP out of hours centre, ADOC. Based at the out of hours hub, and using 12 years of ADASTRA data as its infrastructure, this service is designed to facilitate home care support, enabling patients to remain at home, and supporting early discharge. It can also be used to arrange out of hours GP revisiting. Referrals are taken from:
the rapid response service; the Emergency Department; North, East and South Ayrshire Councils; and General Practitioners.
NHS Borders implemented a scheme of telephone follow up (and revisit if necessary) for patients who had been visited by the GP out of hours service. This was well received by clinicians and patients, with only 3% of patients who were telephoned/revisited subsequently requiring hospital admission.
Festive monies were also used to implement a novel scheme of primary care input into secondary care, whereby experienced General Practitioners would assess and discharge inpatients. This model was employed predominantly at periods of peak pressure, mainly in January. In a single sweep of inpatients in the Borders General Hospital in January, 21 patients were identified who could be discharged with support or transferred that day. However there were some challenges regarding consultant physician acceptance of this initiative, and ultimately it was used reactively rather than proactively.
NHS Dumfries and Galloway implemented a scheme over the festive period to follow up patients considered to be at risk of hospital admission/readmission. This involved employing an extra GP over the festive periods, to make telephone contact in the first instance and undertake a home visit if considered necessary. There were differing opinions between clinicians and managers regarding the effectiveness of this initiative.
NHS Fife implemented a telephone contact system, proactively contacting patients in the community with complex needs who were referred by either primary or secondary care. Although no data is available, anecdotal evidence suggested that this was successful as a tool to avoid admission and will be undertaken again next year. Formal evaluation should be undertaken over winter 2009-2010.
76

NHS Forth Valley used a telephone contact system (and follow up home visit if necessary) over the festive period for patients with complex needs in the community. Referrals could be made by GPs, but this service was not well used, generating only four referrals. This was largely felt to be due to late implementation.
NHS Grampian undertook three separate festive monies initiatives:
General Practitioners within the Emergency Department at Aberdeen Royal Infirmary to see patients with conditions more appropriately treated by primary care. This was generally considered to have worked well, and both GP and ED patients were seen.
Additional District Nurse capacity was provided over winter weekends. This was perceived to have worked well, particularly in supporting palliative care patients in the community.
Community Psychiatric Nurses (CPNs) were employed by the GP out of hours service. This initiative was felt to have worked particularly well, with positive feedback from clinicians, managers and patients.
NHS Greater Glasgow and Clyde employed a General Practitioner within the Emergency Department at Glasgow Royal Infirmary for 17 weeks. This was well received by managers and clinicians. It was noted, however, that GRI does not have a large problem with patients attending with ‘primary care’ problems. Thus when there were no patients in the department who were more appropriate to be seen by a General Practitioner, the majority of GPs were happy to see Emergency Department patients. Some of the more experienced GPs felt less able to see Emergency Department patients, but instead contributed to the department by providing valuable two-way learning.
Festive monies were also used to provide a ‘back-up’ doctor for the GP out of hours service at the Royal Alexandra Hospital in Paisley, as Clyde recently made the move to a no appointment system, necessitating the need for additional capacity in the event of a surge in activity.
NHS Highland undertook four initiatives:
Lochaber Vulnerable Patient Support. Six beds in one ward of the Community Hospital were staffed as GP led Intermediate Care beds over the festive period. Patients identified as at risk of admission over the festive period had a short admission in a rehabilitation unit to avoid a long admission in an acute hospital.
Community Detoxification. An extra CPN was employed from late January in the Emergency Department to provide support to people who presented with chronic substance abuse. This support then continued in the community, avoiding admission.
Increased capacity for the Integrated Care Team from December–March, supporting early discharge and avoiding admission.
The Ambulance Service Town Centre Initiative provided on scene facilities for severely intoxicated individuals, preventing attendance at the Emergency Department.
77

All these initiatives were felt to have worked well, and avoided attendances and admissions to hospital.
NHS Lanarkshire planned a GP out of hours revisiting and telephone review of patients considered to be at risk of hospital admission due to exacerbation of chronic health problems. Palliative Care patients were also targeted. Referrals were accepted from hospital discharge teams and General Practitioners, through pre-determined referral criteria. Although considered to be a good initiative, it was under-utilised and next year a more focused initiative to avoid admission from care homes is planned.
NHS Lothian undertook initiatives to extend planned review by the Lothian Unscheduled Care Services (LUCS). This included taking referrals from the Emergency Department along with referrals from primary care. This worked well with referrals from primary care but there were very few referrals from the Emergency Department, perceived to be due to lack of knowledge of the scheme.
In addition to this a protocol was developed for direct referral of patients from the Scottish Ambulance Service to LUCS (for home visits) allowing paramedics to leave a greater number of patients at home. Uptake of this scheme was small but has been continued with funding from the NHS Board. It is hoped that up to 20% of 999 calls will ultimately be referred to LUCS.
NHS Orkney extended out of hours GP services at Balfour Hospital and on 10 of the outlying inhabited islands for the four public holidays. This involved a combination of extended hours and running drop-in clinics. Using SPARRA data, patients deemed at risk of admission were contacted proactively by telephone over the festive periods. These initiatives worked well.
NHS Shetland offered a consultant physician outreach service to care homes on the islands. Referrals were made by General Practitioners and the patients seen within 24 hours. This was considered to have worked extremely well and is now in place funded by the board.
NHS Tayside implemented a dedicated out of hours GP call-back (and revisiting) service over the festive period to support recently discharged patients, and allowed General Practitioners greater flexibility to keep patients at home.
Local drop in clinics were held in six Minor Injury Units across Tayside, Perthshire and Angus, staffed by General Practitioners for four hours per day over the four day festive weekends. This was considered locally to have worked well, with a perceived reduction in demand on NHS24, the Emergency Department, the out of hours GP service and primary care when they returned to work.
NHS Western Isles did not submit any bids for funding.
78
Related Documents