Osteoporosis Osteoporosis – Concepts, Diagnosis, Concepts, Diagnosis, T t t T t t Treatments Treatments Johann Herberth, MD PhD MPH CCD FACP FASN Division of Nephrology, Bone and Division of Nephrology, Bone and Mineral Metabolism Mineral Metabolism University of Kentucky University of Kentucky Content Content Definition and epidemiology Definition and epidemiology Primary and secondary risk factors Primary and secondary risk factors Bone pathophysiology Bone pathophysiology Division of Nephrology, Bone and Mineral Metabolism Division of Nephrology, Bone and Mineral Metabolism Diagnostic approach Diagnostic approach Universal prevention Universal prevention Pharmacologic treatment options Pharmacologic treatment options “Bones of glass and a heart of stone” “Bones of glass and a heart of stone” Definition; NIH Consensus Definition; NIH Consensus Conference Conference “A skeletal disorder characterized by compromised “A skeletal disorder characterized by compromised bone strength… bone strength… Division of Nephrology, Bone and Mineral Metabolism Division of Nephrology, Bone and Mineral Metabolism …predisposing to an increased risk of fracture.” …predisposing to an increased risk of fracture.” Strength = Density + Quality Strength = Density + Quality Dempster et al J Bone Miner Res 1986 Epidemiology of Osteoporosis Epidemiology of Osteoporosis 8 mio. Women, 2 mio. Men have osteoporosis 8 mio. Women, 2 mio. Men have osteoporosis 34 mio. have low bone mass 34 mio. have low bone mass In the US, 50% of women and 25% of men In the US, 50% of women and 25% of men >50 yo. will suffer an osteoporosis related >50 yo. will suffer an osteoporosis related Division of Nephrology, Bone and Mineral Metabolism Division of Nephrology, Bone and Mineral Metabolism fracture fracture 300.000 hip 300.000 hip 400.000 wrist / forearm 400.000 wrist / forearm 550.000 vertebrae 550.000 vertebrae 810.000 other 810.000 other NOF 2002 Chrischilles et al, Arch Intern Med 1991 Burge et al, J Bone Miner Res 2007 Economic Burden (per year) Economic Burden (per year) $25.3 billion by 2025 $25.3 billion by 2025 $50 billion by 2050 $50 billion by 2050 $17 billion direct medical costs $17 billion direct medical costs Division of Nephrology, Bone and Mineral Metabolism Division of Nephrology, Bone and Mineral Metabolism >400.000 hospital admission >400.000 hospital admission ~2.5 mio. physician visits ~2.5 mio. physician visits >180.000 nursing home admissions >180.000 nursing home admissions Burge et al, J Bone Miner Res 2007 Ray et al, J Bone Miner Res 1997 NOF, Osteoporosis Int 1998 Risk Factors Risk Factors

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Osteoporosis Osteoporosis ––
Concepts, Diagnosis, Concepts, Diagnosis, T t tT t tTreatmentsTreatments
Johann Herberth, MD PhD MPH CCD FACP FASN
Division of Nephrology, Bone and Division of Nephrology, Bone and Mineral MetabolismMineral Metabolism
University of KentuckyUniversity of Kentucky
ContentContent Definition and epidemiologyDefinition and epidemiology
Primary and secondary risk factorsPrimary and secondary risk factors
Bone pathophysiologyBone pathophysiology
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Diagnostic approachDiagnostic approach
Universal prevention Universal prevention
Pharmacologic treatment optionsPharmacologic treatment options
“Bones of glass and a heart of stone”“Bones of glass and a heart of stone”
Definition; NIH Consensus Definition; NIH Consensus ConferenceConference
“A skeletal disorder characterized by compromised “A skeletal disorder characterized by compromised bone strength…bone strength…
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
…predisposing to an increased risk of fracture.”…predisposing to an increased risk of fracture.”
Strength = Density + QualityStrength = Density + Quality
Dempster et al J Bone Miner Res 1986
Epidemiology of OsteoporosisEpidemiology of Osteoporosis
8 mio. Women, 2 mio. Men have osteoporosis8 mio. Women, 2 mio. Men have osteoporosis 34 mio. have low bone mass34 mio. have low bone mass In the US, 50% of women and 25% of men In the US, 50% of women and 25% of men
>50 yo. will suffer an osteoporosis related >50 yo. will suffer an osteoporosis related
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
50 yo su e a osteopo os s e ated50 yo su e a osteopo os s e atedfracturefracture 300.000 hip300.000 hip 400.000 wrist / forearm400.000 wrist / forearm 550.000 vertebrae550.000 vertebrae 810.000 other810.000 other
NOF 2002Chrischilles et al, Arch Intern Med 1991Burge et al, J Bone Miner Res 2007
Economic Burden (per year)Economic Burden (per year)
$25.3 billion by 2025$25.3 billion by 2025
$50 billion by 2050$50 billion by 2050
$17 billion direct medical costs$17 billion direct medical costs
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
>400.000 hospital admission>400.000 hospital admission
~2.5 mio. physician visits~2.5 mio. physician visits
>180.000 nursing home admissions>180.000 nursing home admissions
Burge et al, J Bone Miner Res 2007Ray et al, J Bone Miner Res 1997NOF, Osteoporosis Int 1998
Risk FactorsRisk Factors

Primary Risk FactorsPrimary Risk Factors
Caucasian / Asian backgroundCaucasian / Asian background
WomenWomen
Age / Postmenopausal statusAge / Postmenopausal status
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Menopause < age 45Menopause < age 45
Small body habitusSmall body habitus
Hx. low trauma fracture in 1Hx. low trauma fracture in 1stst degree relativedegree relative
Primary Risk FactorsPrimary Risk Factors
Dementia / impaired visionDementia / impaired vision
FallsFalls
Low physical activityLow physical activity
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Alcohol intakeAlcohol intake
SmokingSmoking
Low lifelong calcium intakeLow lifelong calcium intake
Secondary Risk FactorsSecondary Risk Factors
GI disorders leading to malabsorption (bariatric GI disorders leading to malabsorption (bariatric surgery, inflammatory dz., celiac dz. etc.)surgery, inflammatory dz., celiac dz. etc.)
EndocrineEndocrine Hyperparathyroidism (primary or secondary)Hyperparathyroidism (primary or secondary)
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Hyperparathyroidism (primary or secondary)Hyperparathyroidism (primary or secondary) Hyper/hypothyroidismHyper/hypothyroidism HypercortisolismHypercortisolism HyperprolactinemiaHyperprolactinemia AcromegalyAcromegaly HypogonadismHypogonadism
Secondary Risk FactorsSecondary Risk Factors
Liver disease (biliary sclerosis, autoimmune and Liver disease (biliary sclerosis, autoimmune and alcoholic hepatitis, sclerosing cholangitis)alcoholic hepatitis, sclerosing cholangitis)
Rheumatoid arthritis and other autoimmune Rheumatoid arthritis and other autoimmune diseasesdiseases
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Renal diseaseRenal disease TransplantationTransplantation IDDMIDDM Dietary disorders (anorexia etc.)Dietary disorders (anorexia etc.)
Less Common Secondary Risk Less Common Secondary Risk FactorsFactors
Ankylosing spondylitisAnkylosing spondylitis
COPDCOPD
EndometriosisEndometriosis
Lymphoma/LeukemiaLymphoma/Leukemia
Multiple MyelomaMultiple Myeloma
AmyloidosisAmyloidosis
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
HemophiliaHemophilia
HemochromatosisHemochromatosis
HypophosphatasiaHypophosphatasia
Osteogenesis imperfectaOsteogenesis imperfecta
SarcoidosisSarcoidosis
MedicationsMedications Glucocorticoids (PO and Glucocorticoids (PO and
inhaled)inhaled)
GrH AgonistsGrH Agonists
DepoDepo--ProveraProvera
LongLong--term heparin / term heparin / coumadincoumadin
PPIPPI
SSRISSRI
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
ImmunosuppressantsImmunosuppressants
AnticonvulsantsAnticonvulsants
Cytotoxic drugsCytotoxic drugs
LithiumLithium

Mas
s Peak Bone Mass
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
20 50 60 80
Age in Years
Bo
ne
M
10 40 70 9030
Active Growth
Type II Loss
Rapid Type I Loss
Continuing Loss
Type II Loss
Vertebral vs. HipVertebral vs. Hip Clinically evident: 25Clinically evident: 25--30%30% Future risk vertebral Future risk vertebral
fracture: 5fracture: 5--foldfold Future risk hip fracture: Future risk hip fracture:
22 foldfold
Excess mortality: 31% Excess mortality: 31% men, 17% womenmen, 17% women
Able to walk without Able to walk without assistance 6 months assistance 6 months later: 15%later: 15%
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
22--foldfold Patients with additional Patients with additional
fracture in 3 years: 50%fracture in 3 years: 50% Excess mortality: 30%Excess mortality: 30%
Recovers prefracture Recovers prefracture status: 20%status: 20%
Nursing home care: 30%Nursing home care: 30%
Lindsay et al JAMA 2001Black et al J Bone Miner Res 1999Hasserius et al Calcif Tissue Int 2005
Forsen et al Osteoporosis Int 1999Van Balen et al Disabil Rehabil 2003
Glucocorticoids and FractureGlucocorticoids and Fracture
2 59
5.18
3
4
5
6
actu
re
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Van Staa et al Rheumatology 2000
1.17 1.1 0.99
1.551.36
1.04
1.77
2.59
1.64
1.19
2.27
0
1
2
all
fore
arm hip vert
all
fore
arm hip vert all
fore
arm hip vert
RR
fra
Orcel Joint Bone Spine 2005
<2.5mg 2.5 – 7.5mg >7.5mg
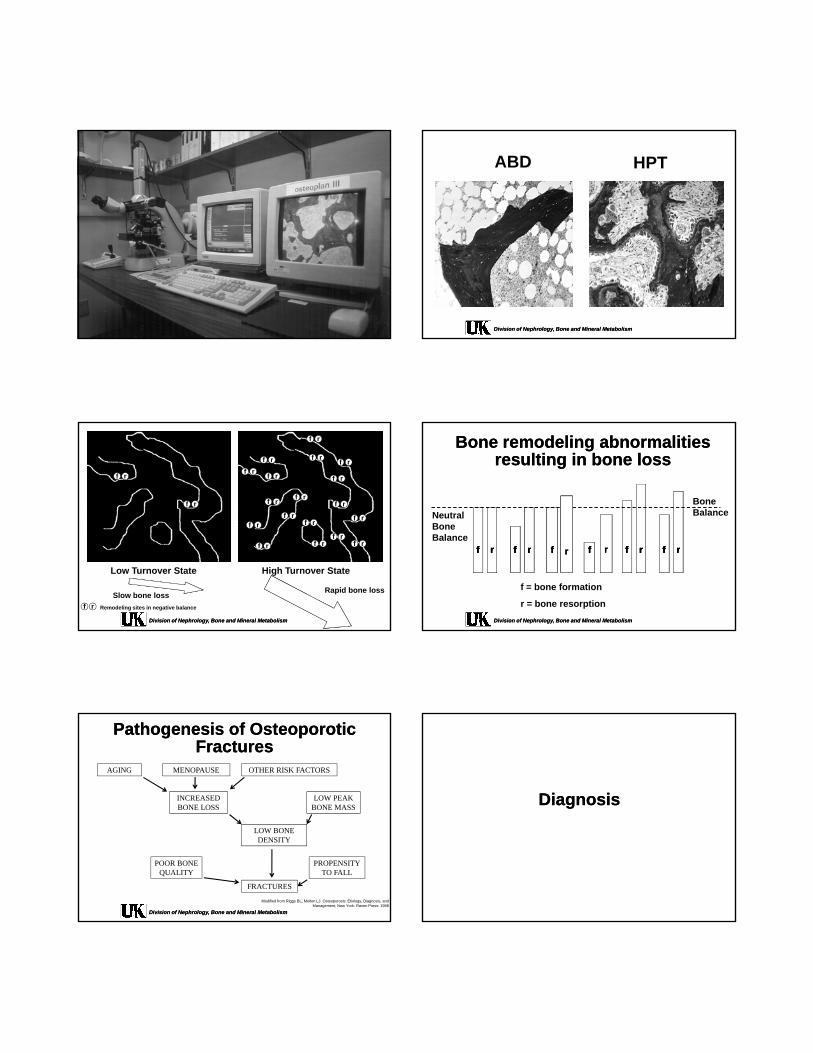
Bone PathophysiologyBone Pathophysiology
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
ABD HPT
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
f r
f r
f r
f r
f r
f r
f rf r
f r
f rf r
f r
f r
f r
f rf r
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
f r
f r
f rf rf r
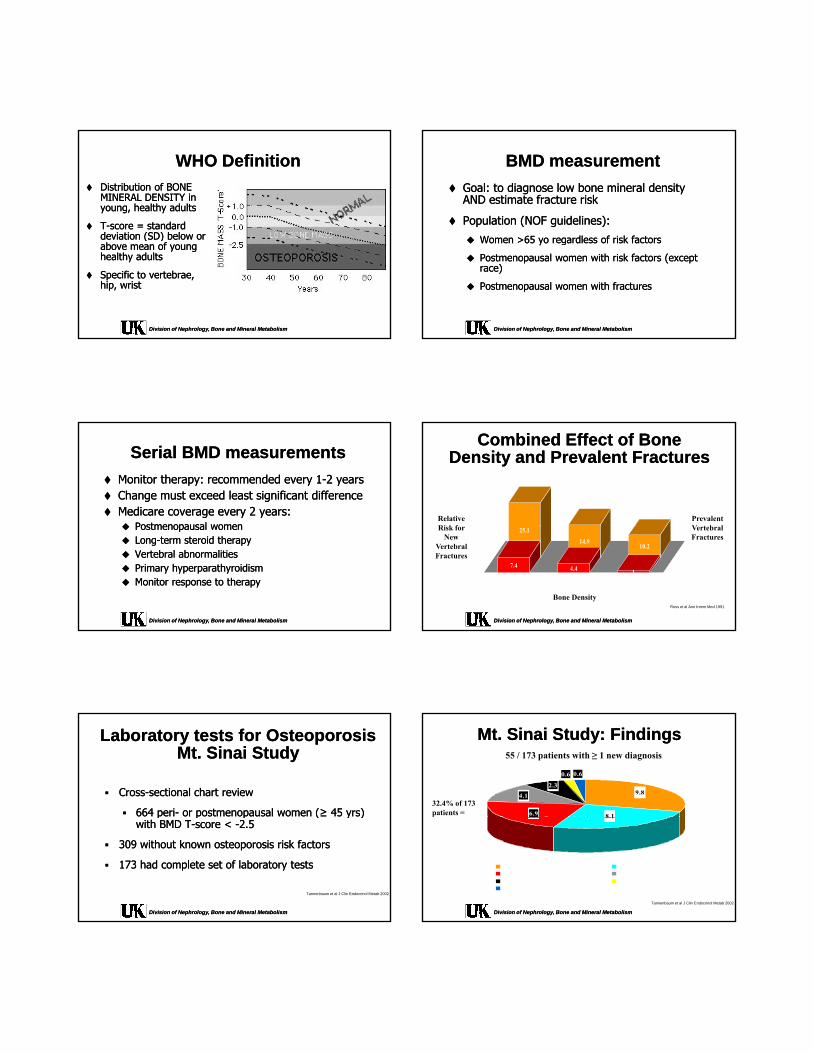
f r Remodeling sites in negative balance
Low Turnover State
Slow bone lossRapid bone loss
High Turnover State
Bone remodeling abnormalities Bone remodeling abnormalities resulting in bone lossresulting in bone loss
Bone BalanceNeutral
Bone
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Bone Balance
ffff rrrr ffff rrrr ffff rrrr ffff ffff rrrr ffff rrrr
f = bone formation
r = bone resorption
rr rr
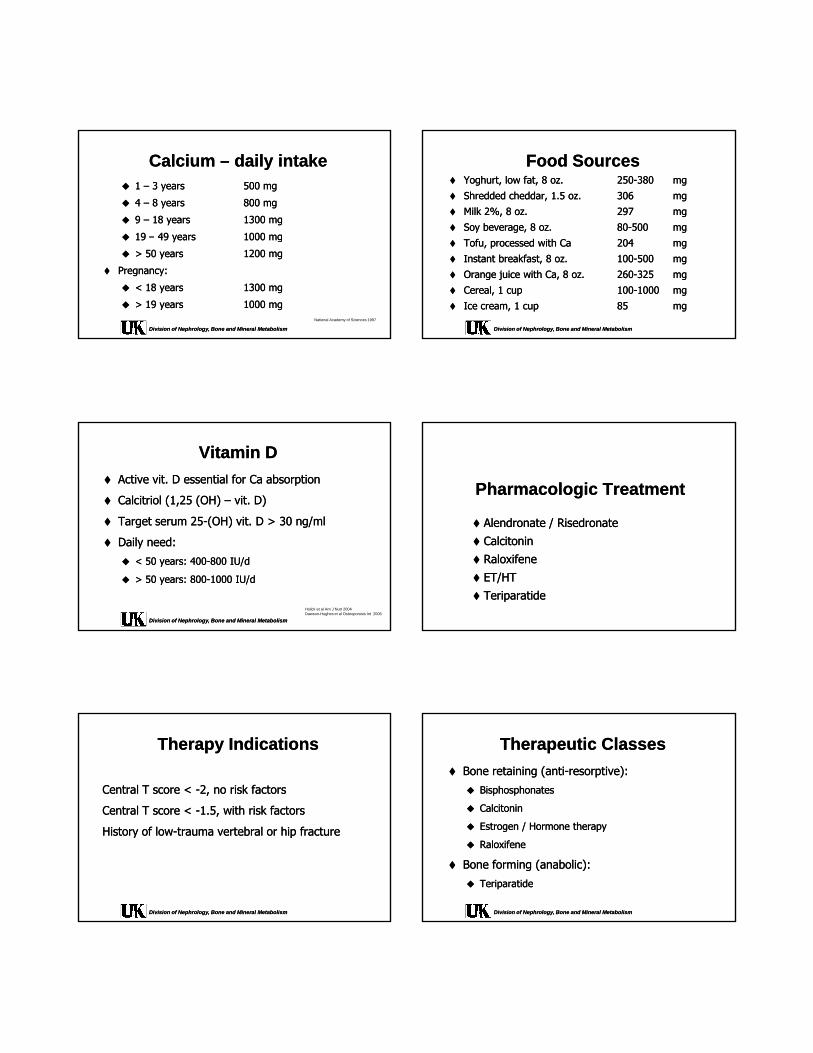
Pathogenesis of Osteoporotic Pathogenesis of Osteoporotic FracturesFractures
AGING MENOPAUSE OTHER RISK FACTORS
INCREASEDBONE LOSS
LOW PEAK BONE MASS
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Modified from Riggs BL, Melton LJ. Osteoporosis: Etiology, Diagnosis, and Management, New York: Raven Press: 1998
LOW BONEDENSITY
POOR BONEQUALITY
FRACTURES
PROPENSITYTO FALL
DiagnosisDiagnosis
WHO DefinitionWHO Definition
Distribution of BONE Distribution of BONE MINERAL DENSITY in MINERAL DENSITY in young, healthy adultsyoung, healthy adults
TT--score = standard score = standard deviation (SD) below ordeviation (SD) below or
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
deviation (SD) below or deviation (SD) below or above mean of young above mean of young healthy adultshealthy adults
Specific to vertebrae, Specific to vertebrae, hip, wristhip, wrist
BMD measurementBMD measurement
Goal: to diagnose low bone mineral density Goal: to diagnose low bone mineral density AND estimate fracture riskAND estimate fracture risk
Population (NOF guidelines):Population (NOF guidelines):
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Women >65 yo regardless of risk factorsWomen >65 yo regardless of risk factors
Postmenopausal women with risk factors (except Postmenopausal women with risk factors (except race)race)
Postmenopausal women with fracturesPostmenopausal women with fractures
Serial BMD measurementsSerial BMD measurements
Monitor therapy: recommended every 1Monitor therapy: recommended every 1--2 years2 years Change must exceed least significant differenceChange must exceed least significant difference Medicare coverage every 2 years:Medicare coverage every 2 years:
Postmenopausal womenPostmenopausal women
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Postmenopausal womenPostmenopausal women LongLong--term steroid therapyterm steroid therapy Vertebral abnormalitiesVertebral abnormalities Primary hyperparathyroidismPrimary hyperparathyroidism Monitor response to therapyMonitor response to therapy
Combined Effect of Bone Combined Effect of Bone Density and Prevalent FracturesDensity and Prevalent Fractures
25
30
Relative Ri k f
Prevalent V t b l
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
25.1
14.910.2
7.4 4.4 10
5
10
15
20
Lowest Third Middle Third Highest Third
None
One
Risk for New
Vertebral Fractures
Vertebral Fractures
Bone DensityRoss et al Ann Intern Med 1991
Laboratory tests for OsteoporosisLaboratory tests for OsteoporosisMt. Sinai StudyMt. Sinai Study
CrossCross--sectional chart review sectional chart review
664 peri664 peri-- or postmenopausal women (or postmenopausal women (≥≥ 45 yrs) 45 yrs)
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
pp p p (p p ( y )y )with BMD Twith BMD T--score < score < --2.52.5
309 without known osteoporosis risk factors309 without known osteoporosis risk factors
173 had complete set of laboratory tests173 had complete set of laboratory tests
Tannenbaum et al J Clin Endocrinol Metab 2002
Mt. Sinai Study: FindingsMt. Sinai Study: Findings
0.60.6
8.1
9.82.3
4.1
6.9
55 / 173 patients with ≥ 1 new diagnosis
32.4% of 173 patients =
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
8.1
Hypercalciuria MalabsorptionHyperparathyroidism Vitamin D deficiencyExogenous hyperthyroidism Hypocaciuric hypercalcemiaCushing's disease
Tannenbaum et al J Clin Endocrinol Metab 2002

Suggested Screening Tests for Suggested Screening Tests for Contributory Causes of OsteoporosisContributory Causes of Osteoporosis 2424--hour urine:hour urine:
Ca, creatinine and NaCa, creatinine and Na
Serum:Serum:
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Ca, P, creatinine, alkaline phosphatase, albumin, Ca, P, creatinine, alkaline phosphatase, albumin, PTH and 25PTH and 25--OH vitamin D, TSH, SPEPOH vitamin D, TSH, SPEP
Moderate cost, misses only rare causes of secondary Moderate cost, misses only rare causes of secondary osteoporosisosteoporosis
Turnover marker???Turnover marker???
Universal Preventive MeasuresUniversal Preventive Measures
Fracture PreventionFracture Prevention
Risk prevention (falls, balance etc.)Risk prevention (falls, balance etc.)
Weight bearing + muscle strength exercisesWeight bearing + muscle strength exercises
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Weight bearing + muscle strength exercisesWeight bearing + muscle strength exercises
Smoking cessation, EtOH avoidanceSmoking cessation, EtOH avoidance
Exercise guidelinesExercise guidelines
AvoidAvoid
Forward flexion of spineForward flexion of spine
Bending forward from the waistBending forward from the waist
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Twisting / jerking of spineTwisting / jerking of spine
One foot to remain on the groundOne foot to remain on the ground
Balance trainingBalance training
Face countertop and hold on with both handsFace countertop and hold on with both hands
Bend one leg and bring foot behind bodyBend one leg and bring foot behind body
Count to 5Count to 5
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Then repeat withThen repeat with
One hand holding onOne hand holding on
FingertipFingertip
Without holding onWithout holding on
Closed eyesClosed eyes
General fall preventionGeneral fall prevention
HandrailsHandrails
Wear shoes with low heelsWear shoes with low heels
Sufficient lighting, use flash lightSufficient lighting, use flash light
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Rubber mat in showerRubber mat in shower
SkidSkid--proof carpets / rugsproof carpets / rugs
Cordless phoneCordless phone
Emergency service / neighborsEmergency service / neighbors
Calcium Calcium –– daily intakedaily intake 1 1 –– 3 years3 years 500 mg500 mg
4 4 –– 8 years8 years 800 mg800 mg
9 9 –– 18 years18 years 1300 mg1300 mg
1919 4949 10001000
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
19 19 –– 49 years49 years 1000 mg1000 mg
> 50 years> 50 years 1200 mg1200 mg
Pregnancy:Pregnancy:
< 18 years< 18 years 1300 mg1300 mg
> 19 years> 19 years 1000 mg1000 mgNational Academy of Sciences 1997
Food SourcesFood Sources Yoghurt, low fat, 8 oz.Yoghurt, low fat, 8 oz. 250250--380 380 mgmg
Shredded cheddar, 1.5 oz.Shredded cheddar, 1.5 oz. 306 306 mgmg
Milk 2%, 8 oz.Milk 2%, 8 oz. 297 297 mgmg
Soy beverage, 8 oz.Soy beverage, 8 oz. 8080--500 500 mgmg
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Tofu, processed with CaTofu, processed with Ca 204 204 mgmg
Instant breakfast, 8 oz.Instant breakfast, 8 oz. 100100--500 500 mgmg
Orange juice with Ca, 8 oz.Orange juice with Ca, 8 oz. 260260--325 325 mgmg
Cereal, 1 cupCereal, 1 cup 100100--1000 1000 mgmg
Ice cream, 1 cupIce cream, 1 cup 85 85 mgmg
Vitamin DVitamin D
Active vit. D essential for Ca absorptionActive vit. D essential for Ca absorption
Calcitriol (1,25 (OH) Calcitriol (1,25 (OH) –– vit. D)vit. D)
Target serum 25Target serum 25--(OH) vit. D > 30 ng/ml(OH) vit. D > 30 ng/ml
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
gg ( ) g/( ) g/
Daily need:Daily need:
< 50 years: 400< 50 years: 400--800 IU/d800 IU/d
> 50 years: 800> 50 years: 800--1000 IU/d1000 IU/d
Holick et al Am J Nutr 2004Dawson-Hughes et al Osteoporosis Int 2005
Pharmacologic TreatmentPharmacologic Treatment
Alendronate / RisedronateAlendronate / Risedronate Alendronate / RisedronateAlendronate / Risedronate
CalcitoninCalcitonin
RaloxifeneRaloxifene
ET/HTET/HT
TeriparatideTeriparatide
Therapy IndicationsTherapy Indications
Central T score < Central T score < --2, no risk factors2, no risk factors
Central T score < Central T score < --1.5, with risk factors1.5, with risk factors
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
History of lowHistory of low--trauma vertebral or hip fracturetrauma vertebral or hip fracture
Therapeutic ClassesTherapeutic Classes
Bone retaining (antiBone retaining (anti--resorptive):resorptive):
BisphosphonatesBisphosphonates
CalcitoninCalcitonin
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Estrogen / Hormone therapyEstrogen / Hormone therapy
RaloxifeneRaloxifene
Bone forming (anabolic):Bone forming (anabolic):
TeriparatideTeriparatide

BisphosphonatesBisphosphonates
FDA approved:FDA approved: AlendronateAlendronate
RisedronateRisedronate
IbandronateIbandronate
Early in the morningEarly in the morning
8 oz. tap water8 oz. tap water
NPO for 30 min (Alendronate, NPO for 30 min (Alendronate, Risedronate) or 60 min Risedronate) or 60 min
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
ZolendronateZolendronate
Binds irreversibly to Binds irreversibly to hydroxyhydroxy--appatite at the appatite at the osteoclastosteoclast--bone bone interfaceinterface
))(Ibandronate)(Ibandronate)
Upright for 30 minUpright for 30 min
Alendronate IndicationsAlendronate Indications
Osteoporosis prevention (5 mg QD, 35 mg qweek)Osteoporosis prevention (5 mg QD, 35 mg qweek)
Postmenopausal womenPostmenopausal women
Osteoporosis treatment (10 mg QD, 70 mg qweek)Osteoporosis treatment (10 mg QD, 70 mg qweek)
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Postmenopausal womenPostmenopausal women
MenMen
SteroidSteroid--induced in men and womeninduced in men and women
Alendronate Alendronate –– GIO 2 yearsGIO 2 years
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Saag et al N Engl J Med 1998
Risedronate IndicationsRisedronate Indications
Osteoporosis prevention (5 mg QD, 35 mg qweek)Osteoporosis prevention (5 mg QD, 35 mg qweek)
Postmenopausal womenPostmenopausal women
SteroidSteroid--induced in men and womeninduced in men and women
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Osteoporosis treatment (10 mg QD, 70 mg qweek)Osteoporosis treatment (10 mg QD, 70 mg qweek)
Postmenopausal womenPostmenopausal women
MenMen
SteroidSteroid--induced in men and womeninduced in men and women
Risedronate Risedronate –– 1 year1 year
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Harris et al JAMA 1999
CalcitoninCalcitonin
Reduces vertebral fracturesReduces vertebral fractures
Not shown to reduce nonNot shown to reduce non--vertebral fracturesvertebral fractures
Indication: postmenopausal (>5 years) womenIndication: postmenopausal (>5 years) women
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Indication: postmenopausal (>5 years) women Indication: postmenopausal (>5 years) women who are unable to tolerate other treatmentswho are unable to tolerate other treatments
Nasal spray or SQ Nasal spray or SQ

Calcitonin Calcitonin –– 5 years5 years
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral MetabolismChesnut et al Am J Med 2000
Cumulative percentage of participants with at least one new fracture per year. Number ofparticipants with follow-up radiographs (placebo = 270, 100 IU = 273, 200 IU = 287, 400IU = 278). The asterisk indicates P <0.05 versus placebo.
RaloxifeneRaloxifene
Selective ESelective E22 receptor modulatorreceptor modulator
Agonist on boneAgonist on bone
Antagonist on breast + uterusAntagonist on breast + uterus
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Osteoporosis preventionOsteoporosis prevention
Postmenopausal womenPostmenopausal women
Osteoporosis treatmentOsteoporosis treatment
Postmenopausal womenPostmenopausal women
Raloxifene Raloxifene –– 5 years5 years
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism Ettinger et al JAMA 1999
Reduction in new vertebral fractures among women (n=6828)
Raloxifene Raloxifene –– Breast CancerBreast Cancer
MORE: 4 years Raloxifene = 72% reduction MORE: 4 years Raloxifene = 72% reduction breast cancer in incidencebreast cancer in incidence
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
CORE: 8 years Raloxifene = 66% reduction in CORE: 8 years Raloxifene = 66% reduction in breast cancer incidence breast cancer incidence
Cauley et al Breast Cancer Res Treatment 2001Martino et al, J Nat Cancer Inst 2004
Women’s Health InitiativeWomen’s Health Initiative
ET: Conj Estrogen (PremarinET: Conj Estrogen (Premarin®®))
HT: Conj Estrogen + Medroxyprogesterone HT: Conj Estrogen + Medroxyprogesterone acetate (Premproacetate (Prempro®®))
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
acetate (Premproacetate (Prempro ))
FDA believes that findings of the WHI study FDA believes that findings of the WHI study apply to all ET/HT combinationsapply to all ET/HT combinations
WHI WHI –– Fracture, CADFracture, CAD
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Writing Group for the Women’s Health Initiative, JAMA 2002

WHI WHI –– Cancer DataCancer Data
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Writing Group for the Women’s Health Initiative, JAMA 2002
WHI limitationsWHI limitations
Looked at 0.625 mg qd EE and 2.5 mg MPALooked at 0.625 mg qd EE and 2.5 mg MPA
Not investigated other formulationsNot investigated other formulations
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
No distinction between estrogen and progestinNo distinction between estrogen and progestin
Transdermal application?Transdermal application?
ET/HT ET/HT –– FDA RecommendationsFDA Recommendations
ET/HT IS approved to PREVENT osteoporosisET/HT IS approved to PREVENT osteoporosis
Consider nonConsider non--estrogen preparations firstestrogen preparations first
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
“smallest dose for shortest time”“smallest dose for shortest time”
Weigh benefit and risks (DVT, CAD, breast Weigh benefit and risks (DVT, CAD, breast cancer)cancer)
Teriparatide = PTH (1Teriparatide = PTH (1--34)34)
First 1First 1--34 aminoacids of the PTH molecule34 aminoacids of the PTH molecule
SQ QDSQ QD
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Max use for 2 yearsMax use for 2 years
Decreases vertebral AND nonDecreases vertebral AND non--vertebral vertebral fractures after mean 18 months treatmentfractures after mean 18 months treatment
Teriparatide IndicationsTeriparatide Indications
LOW TURNOVER bone disease!LOW TURNOVER bone disease! Postmenopausal women osteoporosisPostmenopausal women osteoporosis MenMen
Primary osteoporosisPrimary osteoporosis
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Hypogonadal osteoporosisHypogonadal osteoporosis High riskHigh risk
Previous osteoporotic fracturePrevious osteoporotic fracture Multiple risk factorsMultiple risk factors TT--score <score <--33 Intolerant to other therapiesIntolerant to other therapies
Teriparatide WarningsTeriparatide Warnings
HypercalcemiaHypercalcemia
Paget’s diseasePaget’s disease
Children / adolescentsChildren / adolescents
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
PregnancyPregnancy
Bone cancer (esp. osteosarcoma)Bone cancer (esp. osteosarcoma)
Cancer history (esp. with bone metastasis Cancer history (esp. with bone metastasis potential) or radiation to bonepotential) or radiation to bone

RANKL/RANK/OPG SystemRANKL/RANK/OPG System
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
RealReal--World Obstacles in the World Obstacles in the Management of OsteoporosisManagement of Osteoporosis
Insufficient rates of diagnosisInsufficient rates of diagnosis
Low awareness the necessity to treatLow awareness the necessity to treat
Low persistence: patient stops taking Low persistence: patient stops taking
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
p p p gp p p gmedicationmedication
Poor compliance: patient does not follow Poor compliance: patient does not follow dosing instructionsdosing instructions
Siris et al Mayo Clin Proc. 2006
Probability of fracture in 24 months in bisphosphonate-treated patients
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
Siris et al Mayo Clin Proc. 2006
MPR = medication possession ratio
““Bones of Glass Bones of Glass and and
a Heart of Stonea Heart of Stone””
Aortic Calcifications and Bone Loss Aortic Calcifications and Bone Loss (157 women)(157 women)
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism Schulz et al JCEM 2004;
Coronary Calcifications and Bone Coronary Calcifications and Bone VolumeVolume
(38 dialysis patients)(38 dialysis patients)30 yr old pt
50 yr old pt
75 yr old pt
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
75 yr old pt
Adragao, Herberth et al Clin J Am Soc Nephrol 2009.

ConclusionConclusion Osteoporosis pervasive health problem of major proportions Osteoporosis pervasive health problem of major proportions
incurring enormous healthcare expendituresincurring enormous healthcare expenditures
Underdiagnosed and undertreated Underdiagnosed and undertreated
Different types of bone loss requires different therapeutic Different types of bone loss requires different therapeutic
Division of Nephrology, Bone and Mineral MetabolismDivision of Nephrology, Bone and Mineral Metabolism
yp q pyp q papproachesapproaches
Therapies for high turnover might be harmful to patients Therapies for high turnover might be harmful to patients with low turnoverwith low turnover
Prevention and treatment of osteoporosis not only desirable Prevention and treatment of osteoporosis not only desirable for prevention of fractures but possibly also for slowing for prevention of fractures but possibly also for slowing progression of vascular calcifications progression of vascular calcifications
Thank YouThank You
Related Documents




![Presence of Sarcopenia in Senescence Accelerated Mouse ...€¦ · induced osteoporotic bone. Bone. 2010;46:1299-305. [2] Guo AY; Leung KS; Qin JH; Chow SK; CheungWH*. Effect of low-magnitude](https://static.cupdf.com/doc/110x72/600eb838bfc6b86d2d3c4425/presence-of-sarcopenia-in-senescence-accelerated-mouse-induced-osteoporotic.jpg)



![Dental implant placement in focal osteoporotic bone marrow ... · mechanical pattern of bone at an implant site [20]. As in this case, we recommend augmenting the FOBMD with bone](https://static.cupdf.com/doc/110x72/5fb6ae363ba6310b6b5c0e1b/dental-implant-placement-in-focal-osteoporotic-bone-marrow-mechanical-pattern.jpg)


