Platinum Priority – Collaborative Review – Prostate Cancer Editorial by XXX on pp. x–y of this issue Contemporary Role of Salvage Lymphadenectomy in Patients with Recurrence Following Radical Prostatectomy Firas Abdollah a, *, Alberto Briganti b , Francesco Montorsi b , Arnulf Stenzl c , Christian Stief d , Bertrand Tombal e , Hein Van Poppel f , Karim Touijer g a Vattikuti Urology Institute and VUI Center for Outcomes Research Analytics and Evaluation, Henry Ford Hospital, Detroit, MI, USA; b Department of Urology, Vita-Salute University, San Raffaele, Milan, Italy; c Department of Urology, Eberhard-Karls-University Tuebingen, Tuebingen, Germany; d Department of Urology, Ludwig-Maximilians-University, Klinikum Grosshadern, Munich, Germany; e Service d’Urologie, Cliniques universitaires Saint Luc, Universite ´ catholique de Louvain, Brussels, Belgium; f Department of Urology, Leuven Cancer Institute, Universitair Ziekenhuis Gasthuisberg, Leuven, Belgium; g Urology Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, NY, USA EUROPEAN UROLOGY XXX (2014) XXX–XXX available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted March 17, 2014 Published online ahead of print on March 26, 2014 Keywords: Lymph node excision Lymphatic metastasis Neoplasm recurrence local/surgery Prostate-specific antigen/blood Prostatectomy Prostatic neoplasms/surgery Salvage therapy Treatment outcome Abstract Context: Prostate cancer (PCa) patients with isolated clinical lymph node (LN) relapse, limited to the regional and/or retroperitoneal LNs, may represent a distinct group of patients who have a more favorable outcome than men with progression to the bone or to other visceral organs. Some data indirectly denote a beneficial impact of pelvic LN dissection on survival in these patients. Objective: To provide an overview of the currently available literature regarding salvage LN dissection (SLND) in PCa patients with clinical relapse limited to LNs after radical prostatec- tomy (RP). Evidence acquisition: A systematic literature search was conducted using the Medline, Embase, and Web of Science databases to identify original articles, review articles, and editorials regarding SLND. Articles published between 2000 and 2012 were reviewed and selected with the consensus of all the authors. Evidence synthesis: Contemporary imaging techniques, such as 11C-choline positron emis- sion tomography and diffusion-weighted magnetic resonance imaging, appear to enhance the accuracy in identifying LN relapse in patients with biochemical recurrence (BCR) and after RP. In these individuals, SLND can be considered as a treatment option. The currently available data suggest that SLND can delay clinical progression and postpone hormonal therapy in almost one-third of the patients, although the majority will have BCR. An accurate and attentive preoperative patient selection may help improve these outcomes. The most frequent complication after SLND was lymphorrhea (15.3%), followed by fever (14.5%) and ileus (11.2%). It is noteworthy that all examined cohorts originated from retrospective single-institution series, with limited sample size and short follow-up. Consequently, the current findings cannot be generalized and warrant further investigation in future prospective trials. Conclusions: The current data suggest that SLND represents an option in patients with disease relapse limited to the LNs after RP; however, more robust data derived from well-designed clinical trials are needed to validate the role of SLND in this selected patient population. Patient summary: Salvage lymph node dissection (SLND) represents a treatment option in for patients with prostate cancer relapse limited to the lymph nodes; however, more robust data derived from well-designed clinical trials are needed to validate the role of SLND in this selected patient population. # 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Vattikuti Urology Institute and VUI Center for Outcomes Research Analytics and Evaluation, Henry Ford Hospital, 2799 W. Grand Blvd., Detroit, MI 48202-2689, USA. E-mail address: fi[email protected] (F. Abdollah). EURURO-5594; No. of Pages 11 Please cite this article in press as: Abdollah F, et al. Contemporary Role of Salvage Lymphadenectomy in Patients with Recurrence Following Radical Prostatectomy. Eur Urol (2014), http://dx.doi.org/10.1016/j.eururo.2014.03.019 http://dx.doi.org/10.1016/j.eururo.2014.03.019 0302-2838/# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X
ava i lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
EURURO-5594; No. of Pages 11
Platinum Priority – Collaborative Review – Prostate CancerEditorial by XXX on pp. x–y of this issue
Contemporary Role of Salvage Lymphadenectomy in Patients with
Recurrence Following Radical Prostatectomy
Firas Abdollah a,*, Alberto Briganti b, Francesco Montorsi b, Arnulf Stenzl c, Christian Stief d,Bertrand Tombal e, Hein Van Poppel f, Karim Touijer g
a Vattikuti Urology Institute and VUI Center for Outcomes Research Analytics and Evaluation, Henry Ford Hospital, Detroit, MI, USA; b Department of Urology,
Vita-Salute University, San Raffaele, Milan, Italy; c Department of Urology, Eberhard-Karls-University Tuebingen, Tuebingen, Germany; d Department of
Urology, Ludwig-Maximilians-University, Klinikum Grosshadern, Munich, Germany; e Service d’Urologie, Cliniques universitaires Saint Luc, Universite
catholique de Louvain, Brussels, Belgium; f Department of Urology, Leuven Cancer Institute, Universitair Ziekenhuis Gasthuisberg, Leuven, Belgium; g Urology
Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, NY, USA
Article info
Article history:
Accepted March 17, 2014Published online ahead ofprint on March 26, 2014
Keywords:
Lymph node excision
Lymphatic metastasis
Neoplasm recurrence
local/surgery
Prostate-specific antigen/blood
Prostatectomy
Prostatic neoplasms/surgery
Salvage therapy
Treatment outcome
Abstract
Context: Prostate cancer (PCa) patients with isolated clinical lymph node (LN) relapse, limitedto the regional and/or retroperitoneal LNs, may represent a distinct group of patients who havea more favorable outcome than men with progression to the bone or to other visceral organs.Some data indirectly denote a beneficial impact of pelvic LN dissection on survival in thesepatients.Objective: To provide an overview of the currently available literature regarding salvage LNdissection (SLND) in PCa patients with clinical relapse limited to LNs after radical prostatec-tomy (RP).Evidence acquisition: A systematic literature search was conducted using the Medline,Embase, and Web of Science databases to identify original articles, review articles, andeditorials regarding SLND. Articles published between 2000 and 2012 were reviewed andselected with the consensus of all the authors.Evidence synthesis: Contemporary imaging techniques, such as 11C-choline positron emis-sion tomography and diffusion-weighted magnetic resonance imaging, appear to enhancethe accuracy in identifying LN relapse in patients with biochemical recurrence (BCR) andafter RP. In these individuals, SLND can be considered as a treatment option. The currentlyavailable data suggest that SLND can delay clinical progression and postpone hormonaltherapy in almost one-third of the patients, although the majority will have BCR. Anaccurate and attentive preoperative patient selection may help improve these outcomes.The most frequent complication after SLND was lymphorrhea (15.3%), followed by fever(14.5%) and ileus (11.2%). It is noteworthy that all examined cohorts originated fromretrospective single-institution series, with limited sample size and short follow-up.Consequently, the current findings cannot be generalized and warrant further investigationin future prospective trials.Conclusions: The current data suggest that SLND represents an option in patients with diseaserelapse limited to the LNs after RP; however, more robust data derived from well-designedclinical trials are needed to validate the role of SLND in this selected patient population.Patient summary: Salvage lymph node dissection (SLND) represents a treatment option in forpatients with prostate cancer relapse limited to the lymph nodes; however, more robust dataderived from well-designed clinical trials are needed to validate the role of SLND in thisselected patient population.
# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Vaand Evaluation, Henry FordE-mail address: firas.abdoll
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
http://dx.doi.org/10.1016/j.eururo.2014.03.0190302-2838/# 2014 European Association of Urology. Published by Elsevier
ttikuti Urology Institute and VUI Center for Outcomes Research AnalyticsHospital, 2799 W. Grand Blvd., Detroit, MI 48202-2689, USA.
[email protected] (F. Abdollah).
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019
B.V. All rights reserved.

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X2
EURURO-5594; No. of Pages 11
1. Introduction
In contemporary surgically treated prostate cancer (PCa)
patients, the rate of biochemical recurrence (BCR) after
radical prostatectomy (RP) may reach 40% [1–4]. A
postoperative increase in prostate-specific antigen (PSA)
level is an index of tumor relapse, which could be localized
or systemic. Traditionally, salvage radiotherapy is offered to
patients with a suspected localized pelvic recurrence,
whereas hormonal therapy is offered to those with systemic
spread of the disease [5]. However, current advances in
clinical imaging techniques have allowed the identification
of a new group of patients with a unique relapse pattern.
These are patients with ‘‘systemic’’ disease progression,
which is limited to the regional and/or retroperitoneal
lymph nodes (LNs). These patients will be referred to as
patients with clinical LN relapse.
Patients with isolated clinical LN relapse may represent a
distinct group of patients who have a more favorable
outcome compared with men with progression to the bone
or to other visceral organs [6]. Recent reports found that
some of these patients may benefit from favorable cancer-
control outcomes when surgically treated [7,8]. This finding
is in line with previous retrospective data showing that
extended pelvic LN dissection (ePLND) could offer favorable
cancer control outcomes in PCa with LN invasion (LNI) at RP,
especially when the LNI volume is low (two or fewer
positive nodes) [9,10]. It is interesting to note that the
favorable impact of RP and ePLND held true even in patients
who did not receive adjuvant hormonal therapy after
surgery. Such data indirectly denote a beneficial impact of
pelvic LN dissection (PLND) on survival in these individuals.
However, it is not possible to directly apply these findings to
patients with post-RP clinical LN relapse, because the latter
represent a distinct clinical setting. Nevertheless, it may be
hypothesized that at least some patients with evidence of
limited clinical LN relapse after RP can benefit from salvage
LN dissection (SLND).
It is noteworthy that clinical LN relapse can be the
direct consequence of a suboptimal PLND at initial
treatment. Indeed, during the last two decades, the
majority of surgically treated PCa patients received either
a limited PLND (only obturator fossa) or no PLND at all
during initial treatment [11]. This finding was confirmed
in contemporary patients, in whom PLND was omitted in
28.5% and 18.2% of patients with respectively intermedi-
ate- and high-risk tumors treated with open RP, and in
49.5% and 32.7% of patients treated with robotic-assisted
RP, respectively [12]. These findings imply that even when
there are clear clinical indications, PLND is not always
performed. It appears that the introduction of laparo-
scopic and robot-assisted RP has significantly contributed
to the increased omission of PLND [12]. This situation may
translate to a higher proportion of patients with clinical
LN relapse in the coming years, which further points out
the necessity of working out an optimal treatment
strategy in these individuals. We reviewed the data
regarding the currently highly controversial procedure
of SLND in patients with clinical LN relapse after RP.
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
2. Evidence acquisition
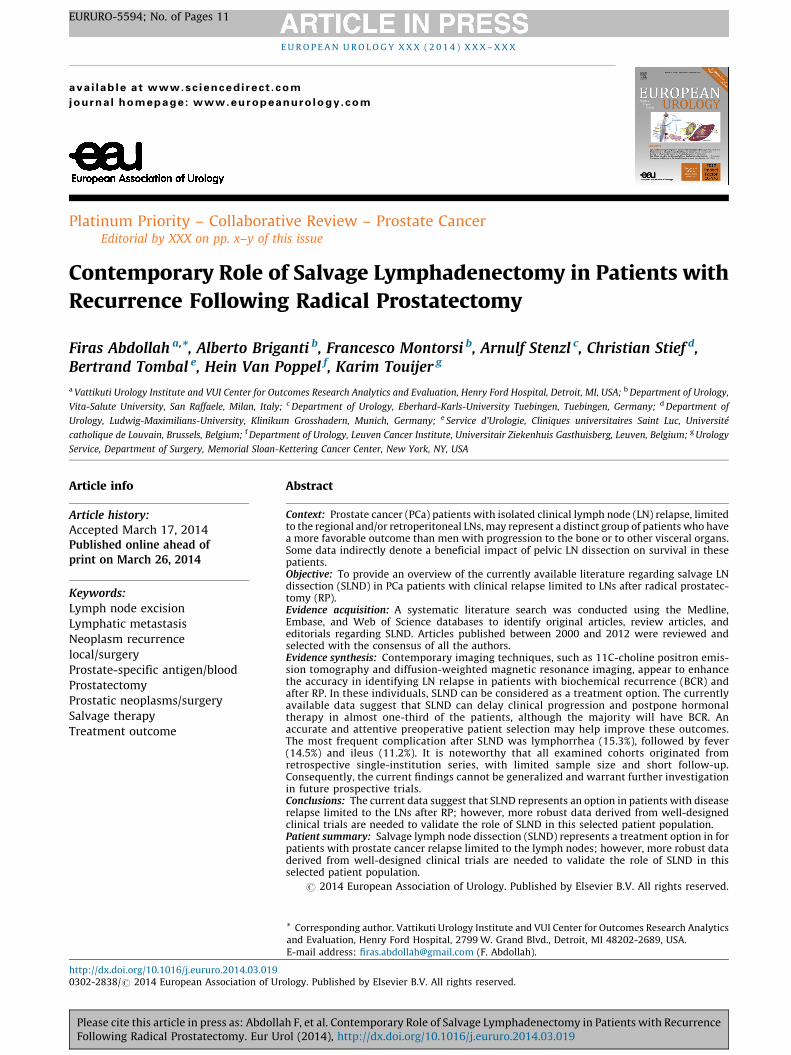
We performed a literature search in December 2012 using
the Medline, Embase, and Web of Science databases. We
identified original articles, review articles, and editorials
addressing the role of SLND in PCa. Articles written in any
language other than English were excluded. The following
limits were used: humans; and gender (male). Keywords
included prostate cancer, salvage lymphadenectomy, salvage
lymph node dissection, and salvage lymph node excision. All
titles were screened, and studies were excluded if obviously
irrelevant. If there was any doubt concerning the eligibility
of a study, abstracts—and if necessary, the full text—were
examined. Additional references were identified from the
reference lists of these articles (Fig. 1). It is noteworthy that
all included articles consisted of case series, which
represent level 4 evidence.
To identify publications that address the evolution of
imaging techniques and their role in the management
of patients with PCa relapse, additional sources were
gathered by including the following keywords, arranged
in variable combinations: prostate cancer, positron emission
tomography (PET), computed tomography (CT), choline,
magnetic resonance imaging (MRI), diffusion-weighted MRI,
PSA, biochemical relapse, restaging, and recurrence.
3. Evidence synthesis
3.1. Diagnosis and staging of lymph node relapse after radical
prostatectomy
Cross-sectional imaging techniques, such as computed
tomography (CT) and magnetic resonance imaging (MRI),
have shown poor ability to detect LN metastasis
in patients with PCa [13] because a volumetric measure
(ie, LN diameter) was traditionally used to define LNI
status. This drawback limited the use of these imaging
techniques in the preoperative staging work-up. Howev-
er, in recent years, several developments and improve-
ments were introduced to the traditional imaging
techniques that escalated their performance as LN staging
procedures. In the current review, we focused on two
relatively novel imaging techniques that are increasingly
recognized as promising staging tools for clinical LN
relapse.
3.1.1. 11C-Choline positron emission tomography/computed
tomography scan
The theory beyond the use of the 11C-choline positron
emission tomography (PET)/CT scan is that tumor cells have
a higher turnover of essential cell membrane components,
such as phosphatidylcholine. After uptake by tumor cells,
radioactive choline is phosphorylated in high concentration
and built into the cell membrane, which allows its detection
by the PET scan. Since the introduction of 11C-choline
PET/CT, several reports have tried to evaluate its role as a
staging procedure in PCa patients with BCR after initial
radical treatment with curative intent [14–26]. These reports
showed a sensitivity that ranged between 38% and 98%. This
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019
[(Fig._1)TD$FIG]
109 publica�ons iden�fied throughPubMed database search using the
following terms: prostate cancer,salvage lymphadenectomy, salvagelymph node dissec�on, and salvage
lymph node excision
Addi�onal 3 publica�ons were iden�fiedthrough search in the references of the 109
publica�ons
Poten�ally relevant 112 ar�cles or abstracts
45 ar�cles were excluded forduplicate
67 ar�cles were assessed for eligibility
60 ar�cles were excluded for:Dated before January 2000 (n = 16)Unrelated (n = 34)Case reports/review/comments (n = 5)Non-English (n = 5)
7 ar�cles were included in the systema�c review
Elegibility
Includ
edScreen
ing
Iden
�fica�o
n
----
Fig. 1 – The review process.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 3
EURURO-5594; No. of Pages 11
wide range might be mainly attributed to the heterogeneity
of the examined cohorts.
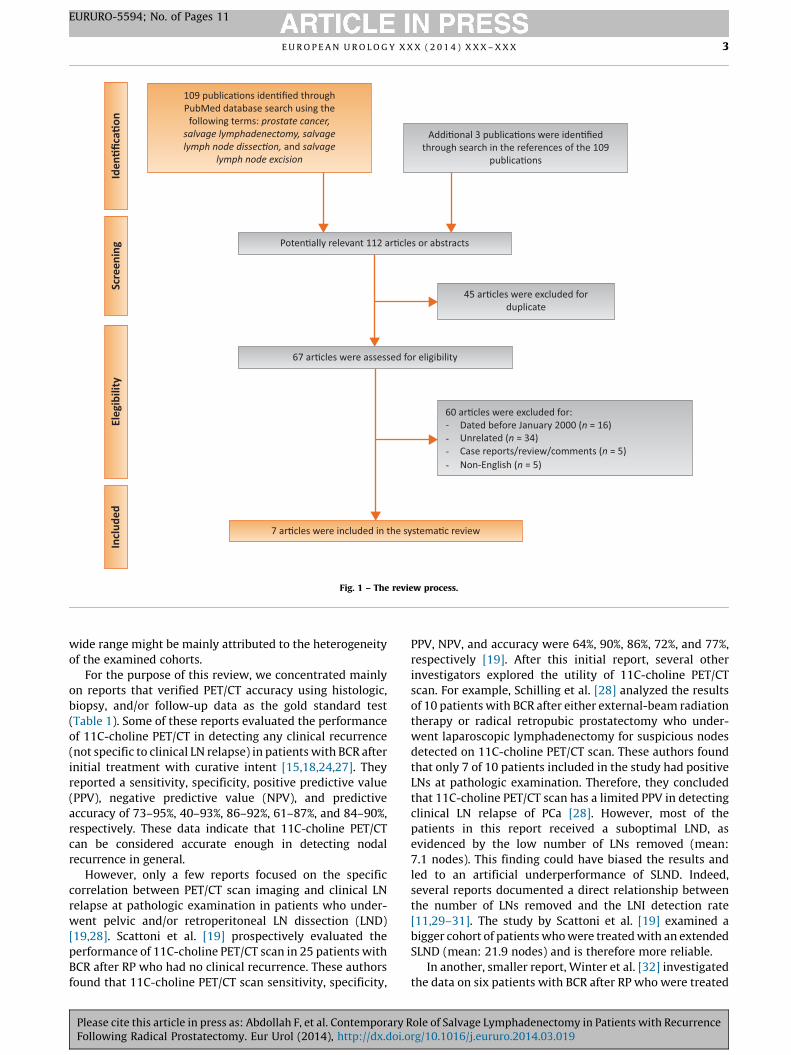
For the purpose of this review, we concentrated mainly
on reports that verified PET/CT accuracy using histologic,
biopsy, and/or follow-up data as the gold standard test
(Table 1). Some of these reports evaluated the performance
of 11C-choline PET/CT in detecting any clinical recurrence
(not specific to clinical LN relapse) in patients with BCR after
initial treatment with curative intent [15,18,24,27]. They
reported a sensitivity, specificity, positive predictive value
(PPV), negative predictive value (NPV), and predictive
accuracy of 73–95%, 40–93%, 86–92%, 61–87%, and 84–90%,
respectively. These data indicate that 11C-choline PET/CT
can be considered accurate enough in detecting nodal
recurrence in general.
However, only a few reports focused on the specific
correlation between PET/CT scan imaging and clinical LN
relapse at pathologic examination in patients who under-
went pelvic and/or retroperitoneal LN dissection (LND)
[19,28]. Scattoni et al. [19] prospectively evaluated the
performance of 11C-choline PET/CT scan in 25 patients with
BCR after RP who had no clinical recurrence. These authors
found that 11C-choline PET/CT scan sensitivity, specificity,
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
PPV, NPV, and accuracy were 64%, 90%, 86%, 72%, and 77%,
respectively [19]. After this initial report, several other
investigators explored the utility of 11C-choline PET/CT
scan. For example, Schilling et al. [28] analyzed the results
of 10 patients with BCR after either external-beam radiation
therapy or radical retropubic prostatectomy who under-
went laparoscopic lymphadenectomy for suspicious nodes
detected on 11C-choline PET/CT scan. These authors found
that only 7 of 10 patients included in the study had positive
LNs at pathologic examination. Therefore, they concluded
that 11C-choline PET/CT scan has a limited PPV in detecting
clinical LN relapse of PCa [28]. However, most of the
patients in this report received a suboptimal LND, as
evidenced by the low number of LNs removed (mean:
7.1 nodes). This finding could have biased the results and
led to an artificial underperformance of SLND. Indeed,
several reports documented a direct relationship between
the number of LNs removed and the LNI detection rate
[11,29–31]. The study by Scattoni et al. [19] examined a
bigger cohort of patients who were treated with an extended
SLND (mean: 21.9 nodes) and is therefore more reliable.
In another, smaller report, Winter et al. [32] investigated
the data on six patients with BCR after RP who were treated
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019
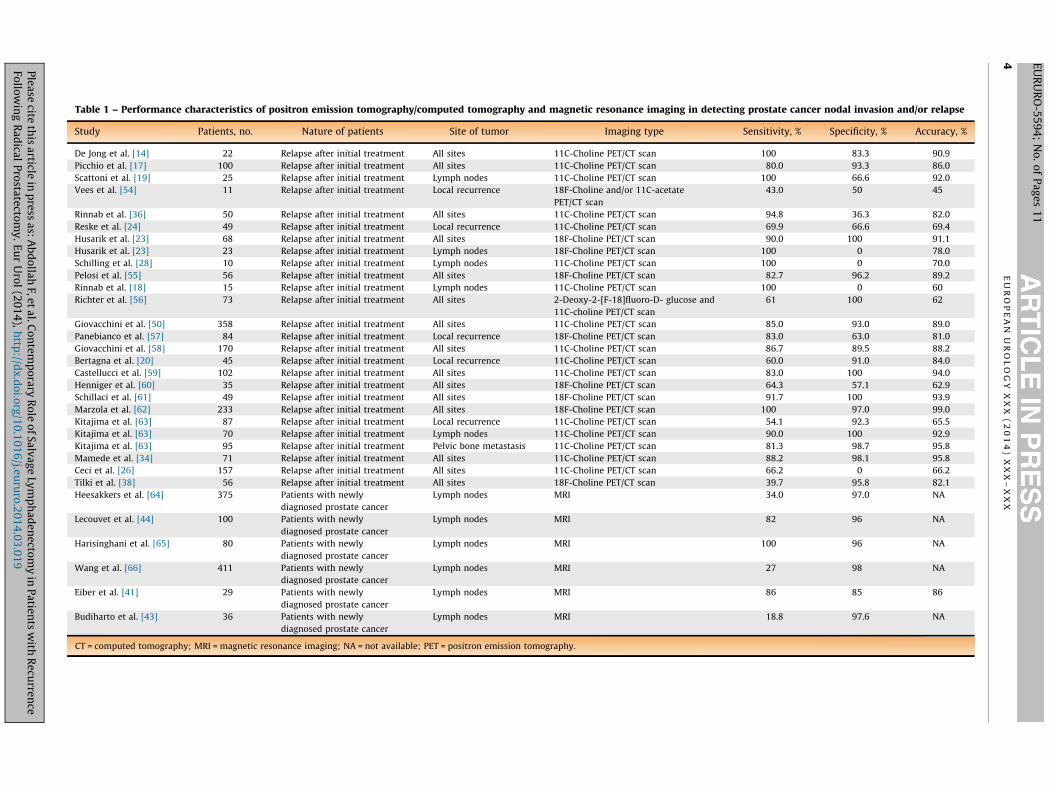
Table 1 – Performance characteristics of positron emission tomography/computed tomography and magnetic resonance imaging in detecting prostate cancer nodal invasion and/or relapse
Study Patients, no. Nature of patients Site of tumor Imaging type Sensitivity, % Specificity, % Accuracy, %
De Jong et al. [14] 22 Relapse after initial treatment All sites 11C-Choline PET/CT scan 100 83.3 90.9
Picchio et al. [17] 100 Relapse after initial treatment All sites 11C-Choline PET/CT scan 80.0 93.3 86.0
Scattoni et al. [19] 25 Relapse after initial treatment Lymph nodes 11C-Choline PET/CT scan 100 66.6 92.0
Vees et al. [54] 11 Relapse after initial treatment Local recurrence 18F-Choline and/or 11C-acetate
PET/CT scan
43.0 50 45
Rinnab et al. [36] 50 Relapse after initial treatment All sites 11C-Choline PET/CT scan 94.8 36.3 82.0
Reske et al. [24] 49 Relapse after initial treatment Local recurrence 11C-Choline PET/CT scan 69.9 66.6 69.4
Husarik et al. [23] 68 Relapse after initial treatment All sites 18F-Choline PET/CT scan 90.0 100 91.1
Husarik et al. [23] 23 Relapse after initial treatment Lymph nodes 18F-Choline PET/CT scan 100 0 78.0
Schilling et al. [28] 10 Relapse after initial treatment Lymph nodes 11C-Choline PET/CT scan 100 0 70.0
Pelosi et al. [55] 56 Relapse after initial treatment All sites 18F-Choline PET/CT scan 82.7 96.2 89.2
Rinnab et al. [18] 15 Relapse after initial treatment Lymph nodes 11C-Choline PET/CT scan 100 0 60
Richter et al. [56] 73 Relapse after initial treatment All sites 2-Deoxy-2-[F-18]fluoro-D- glucose and
11C-choline PET/CT scan
61 100 62
Giovacchini et al. [50] 358 Relapse after initial treatment All sites 11C-Choline PET/CT scan 85.0 93.0 89.0
Panebianco et al. [57] 84 Relapse after initial treatment Local recurrence 18F-Choline PET/CT scan 83.0 63.0 81.0
Giovacchini et al. [58] 170 Relapse after initial treatment All sites 11C-Choline PET/CT scan 86.7 89.5 88.2
Bertagna et al. [20] 45 Relapse after initial treatment Local recurrence 11C-Choline PET/CT scan 60.0 91.0 84.0
Castellucci et al. [59] 102 Relapse after initial treatment All sites 11C-Choline PET/CT scan 83.0 100 94.0
Henniger et al. [60] 35 Relapse after initial treatment All sites 18F-Choline PET/CT scan 64.3 57.1 62.9
Schillaci et al. [61] 49 Relapse after initial treatment All sites 18F-Choline PET/CT scan 91.7 100 93.9
Marzola et al. [62] 233 Relapse after initial treatment All sites 18F-Choline PET/CT scan 100 97.0 99.0
Kitajima et al. [63] 87 Relapse after initial treatment Local recurrence 11C-Choline PET/CT scan 54.1 92.3 65.5
Kitajima et al. [63] 70 Relapse after initial treatment Lymph nodes 11C-Choline PET/CT scan 90.0 100 92.9
Kitajima et al. [63] 95 Relapse after initial treatment Pelvic bone metastasis 11C-Choline PET/CT scan 81.3 98.7 95.8
Mamede et al. [34] 71 Relapse after initial treatment All sites 11C-Choline PET/CT scan 88.2 98.1 95.8
Ceci et al. [26] 157 Relapse after initial treatment All sites 11C-Choline PET/CT scan 66.2 0 66.2
Tilki et al. [38] 56 Relapse after initial treatment All sites 18F-Choline PET/CT scan 39.7 95.8 82.1
Heesakkers et al. [64] 375 Patients with newly
diagnosed prostate cancer
Lymph nodes MRI 34.0 97.0 NA
Lecouvet et al. [44] 100 Patients with newly
diagnosed prostate cancer
Lymph nodes MRI 82 96 NA
Harisinghani et al. [65] 80 Patients with newly
diagnosed prostate cancer
Lymph nodes MRI 100 96 NA
Wang et al. [66] 411 Patients with newly
diagnosed prostate cancer
Lymph nodes MRI 27 98 NA
Eiber et al. [41] 29 Patients with newly
diagnosed prostate cancer
Lymph nodes MRI 86 85 86
Budiharto et al. [43] 36 Patients with newly
diagnosed prostate cancer
Lymph nodes MRI 18.8 97.6 NA
CT = computed tomography; MRI = magnetic resonance imaging; NA = not available; PET = positron emission tomography.
EU
RO
PE
AN
UR
OL
OG
YX
XX
(2
01
4)
XX
X–
XX
X4 E
UR
UR
O-5
59
4;
No
.o
fP
ag
es
11
Ple
ase
citeth
isa
rticlein
pre
ssa
s:A
bd
olla
hF,e
ta
l.Co
nte
mp
orary
Ro
leo
fS
alv
ag
eLy
mp
ha
de
necto
my
inP
atie
nts
with
Re
curre
nce
Follo
win
gR
ad
ical
Pro
state
ctom
y.
Eu
rU
rol
(20
14
),h
ttp://d
x.d
oi.o
rg/1
0.1
01
6/j.e
uru
ro.2
01
4.0
3.0
19

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 5
EURURO-5594; No. of Pages 11
with dissection of the suspicious LNs. In that report, all
metastasis-suspicious LNs at PET/CT scan revealed metas-
tases of PCa at pathologic examination. Ten additional
removed LNs, which had not been considered suspicious at
preoperative imaging, did not show recurrence of PCa.
Therefore, the authors concluded that 11C-choline PET/CT
scan represents a useful tool for the detection of PCa LN
relapse. A similar set of patients was examined by Martini
et al. [33], who found that LN relapse was histologically
confirmed in six of eight patients with positive preoperative
11C-choline PET/CT scans. Thus, the authors concluded that
this imaging technique could be useful in selecting optimal
candidates for SLND.
The ability of 11C-choline PET/CT scan to detect clinical
LN relapse appears to be affected by several factors,
including preimaging PSA level, as well as hormonal and
chemotherapy status [14,22,34–36]. Initial reports argued
against the use of 11C-choline PET/CT scan to detect
recurrence in patients with a PSA <5.0 ng/ml because of the
high false-negative results in these individuals [14].
However, these findings were not corroborated in subse-
quent reports that observed a high reliability of 11C-choline
PET/CT scan in detecting tumor recurrence, even in patients
with very low PSA values (ie, <0.5 ng/ml) [22,34,36].
Nonetheless, it appears that PSA kinetics, rather than the
absolute PSA value, should be used to guide the decision to
perform a PET/CT scan. This is especially true for patients
with low PSA values. For example, Castellucci et al. reported
that PSA doubling time (PSA DT) was the only independent
predictor of a positive scan in patients with a PSA level
<2 ng/ml [22]. Likewise, Mamede et al. observed that PSA
DT and hormonal treatment were the only significant
predictors of positive scans in patients with a PSA level
<0.5 ng/ml [34].
In summary, it appears that 11C-choline PET/CT scan
represents a reliable and valid tool for restaging PCa
patients with BCR after initial treatment with curative
intent. However, given the heterogeneity of the currently
available data and the small number of patients exam-
ined, larger studies are warranted to confirm these
promising results. Similar performance characteristics
were reported when 18F-choline was used to detect PCa
relapse (Table 1).
In an interesting report, Passoni et al. [37] studied the
performance characteristics of 11C-choline PET/CT in
patients with BCR after RP who harbored a single suspected
positive LN metastasis. A total of 46 patients were included,
and all received an SLND. Of them, 38 patients (83%)
harbored a positive LN at pathologic examination. However,
only 16 patients (35%) had a pathologic LN metastases
exclusively limited to the nodes indicated by the PET/TC,
and only 11 patients (24%) had an involvement of a single
LN. Based on these findings, the authors concluded that the
performance of 11C-choline PET/CT in detecting a single
positive LN at SLND is poor. Similar results were observed
when 18-fluoroethylcholine PET/CT was used to identify
clinical LN relapse [38]. Therefore, when an SLND is planned
based on PET/CT findings, it must be extended, regardless of
the number of positive LNs on preoperative imaging.
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
3.1.2. Diffusion-weighted magnetic resonance imaging
In diffusion-weighted MRI (DW-MRI), the Brownian motion
of water protons (molecular diffusion) in biologic tissue is
depicted. Normally, the extracellular and intraductal water
molecules are moving freely in all directions. Therefore,
within the peripheral zone in a healthy prostate, the so-
called apparent diffusion coefficient (ADC), which is
measured by DW-MRI, has high values. Conversely, lower
ADC values are observed in cases of PCa growth [39,40].
Regarding LN staging, DW-MRI seems to have favorable
performance characteristics. Eiber et al. [41] examined the
data on 29 PCa patients (118 LNs were analyzed) who were
investigated with DW-MRI. The performance of DW-MRI in
detecting LNI was calculated using histologic and/or follow-
up data as the standard of reference. These authors used an
ADC cut-off of 1.30 � 10�3 and reported that the sensitivity,
specificity, and discrimination accuracy of this cut-off to
detect LNI were 86%, 85% and 86%, respectively. In a
subsequent report, the same group of authors confirmed
their previous findings in 14 additional PCa patients (55 LNs
were analyzed) [42]. In this report, patients with LNI had
statistically significantly higher ADC values than their
counterparts without LNI (mean ADC: 1.60 � 0.24 vs
1.09 � 0.23 � 10�3, p < 0.001) [42]. Based on these findings,
the authors proposed ADC measured by DW-MRI as a novel
potential imaging biomarker.
Unfortunately, these encouraging results were not
confirmed in other series. Specifically, in a cohort of 36
PCa patients treated with RP and anatomically extended
PLND, Budiharto et al. [43] reported that the sensitivity,
specificity, PPV, and NPV of DW-MRI to detect LNI were 19%,
98%, 46%, and 92%, respectively. These differences in DW-MRI
performance characteristics between the Budiharto et al.
[43] report and the other two aforementioned reports [41,42]
might originate from differences in patient selection criteria
and study design methodology. Indeed, patients described
by Budiharto et al. [43] had a preoperative LNI risk of 10% to
35% according to the Partin tables. Although these patients
harbor high LNI risk, they do not necessarily represent all the
ideal candidates for PLND. It may be argued that these
selection criteria have artificially undermined the perfor-
mance characteristics of DW-MRI. However, given that
Budiharto et al. [43] did not provide a specific ADC cut-off,
a direct comparison of the results of this report with the
previous two studies [41,42] was not possible. Nevertheless,
the major advantage of DW-MRI, when acquired whole-
body, might be the exclusion of the presence of occult bone
metastases with more specificity and sensitivity than with
technetium Tc 99m bone scintigraphy or 11C-choline PET/CT
[44]. Other studies investigating the role of MRI in detecting
LNI are reported in Table 1.
Similar to PET/CT scan, the performance characteristics
of DW-MRI might also be affected by several variables, such
as preimaging PSA value and/or PSA kinetics. However, to
date, there is a paucity of data that examine the impact of
these variables on the accuracy of DW-MRI to detect LNI.
In an interesting study, Thoeny et al. [45] analyzed the
data on 802 removed LNs and reported that the combina-
tion of ultrasmall superparamagnetic particles of iron oxide
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X6
EURURO-5594; No. of Pages 11
(USPIO)–enhanced MRI and DW-MRI allowed the achieve-
ment of optimal performance characteristics in detecting
LNI (sensitivity: 80%; specificity: 87%; PPV: 67%; NPV: 93%;
and accuracy: 90%). In a recent report, the same group of
authors updated their results examining the data on 2993
removed nodes. Fifty-four nodes harbored a metastasis, and
the majority of metastases (93%) were �5 mm in diameter.
The sensitivity, specificity, PPV, NPV, and accuracy of the
procedure were 58%, 83%, 58%, 84%, and 76%, respectively.
As such, the authors concluded that USPIO-enhanced MRI is
accurate in detecting even small metastases. Several USPIO
contrasts had been recently approved in the United States,
Europe, and Japan [46]. However, these contrasts need
further investigation before they can be implemented in
urologic clinical practice.
It is noteworthy that virtually all the aforementioned
reports that discussed the performance of DW-MRI focused
on LN staging in PCa before primary treatment. As such, the
reliability of the technique in detecting clinical LN relapse
after primary treatment is still unknown and warrants
investigation.
3.2. Salvage lymph node dissection in prostate cancer patients
with clinical lymph node relapse after radical prostatectomy
3.2.1. Rationale
The therapeutic benefit of LND has been already established
for several tumors. For example, in the urologic field, LND
represents an important component in the treatment of
patients with testis, penile, and bladder cancer [47,48].
Conversely, the therapeutic role of LND in treating PCa is
still controversial. However, observational data have
showed that PLND might be associated with more favorable
survival rates in PCa patients [9,10], especially when they
harbor a low LNI burden (defined as a maximum of one or
two positive nodes). A recently published randomized trial
showed that at a median follow-up of 74 mo, extended
PLND (in comparison with standard PLND) can significantly
improve the BCR-free rate by 13% and 20% in patients with
intermediate- and high-risk PCa, respectively [49]. Unfor-
tunately, during the last two decades, most patients were
treated with an anatomically limited PLND [11]. Approxi-
mately 30% of patients received no PLND at all [11]. This
situation has certainly resulted in a suboptimal LN
pathologic staging [29–31] and might have contributed to
an increasing risk of clinical LN relapse.
With the development of novel imaging techniques, the
identification of PCa patients with a clinical LN relapse after
primary treatment with RP has become feasible [19,28,32,
41,42,45]. However, these patients are considered by most
experts to harbor a systemic disease, and systemic treatment
with hormonal therapy is recommended in this setting [50].
Some investigators have put forth the provocative hypothesis
that this pattern of recurrence might not necessarily
represent a systemic disease and have suggested that surgical
treatment with SLND might be beneficial in these men
[7,8,32]. The technique, outcomes, morbidity, and mortality
of such a surgical procedure—namely, SLND—represent the
focus of the following part of this review.
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
3.2.2. Surgical technique and anatomic limits of salvage lymph node
dissection in prostate cancer patients with clinical lymph node relapse
after radical prostatectomy
The currently available literature does not allow an accurate
identification of a standardized SLND surgical technique.
However, some hints can still be derived from the existing
data. Generally speaking, the extent of SLND and its
anatomic limits can be guided by the results of 11C-choline
PET/CT scan and/or other preoperative staging imaging. In
patients with clinical LN relapse limited to the pelvic zone, it
is preferable to perform an SLND that includes the fibrofatty
tissue along the external iliac vein, with the distal limit at
the deep circumflex vein and femoral canal. Proximally,
SLND can be extended to include all the LNs along the
common iliac vessels up to the aortic bifurcation. All
fibrofatty tissue within the obturator fossa should also be
removed. Likewise, presacral LNs and LNs located laterally
and medially to the internal iliac artery must be excised
[51].
In patients with retroperitoneal clinical LN relapse at
preoperative imaging and/or in patients with positive
common iliac nodes at intraoperative frozen section
analysis, SLND can be extended to the retroperitoneal
region. This procedure usually consists of the excision of all
nodal tissue located between the renal artery (cranially) and
aortic bifurcation (caudally). Medial and lateral limits
usually consist of the midline of the vena cava and right
ureter, as well as the midline of the aorta and left ureter.
Sometimes it might be necessary to remove the inter-
aortocaval LNs as well. It is of note that clinical LN relapse
may involve several nodes other than those indicated by
the PET/CT scan [37,38]. Thus, some surgeons prefer to
perform a pelvic and retroperitoneal LND upfront, regard-
less of the positive zone on the scan. However, unless clearly
indicated by the preoperative imaging, it might be wise to
avoid LND in areas that were included in the primary LND
and/or included in adjuvant/salvage radiotherapy treat-
ment. Trying to dissect these nodes might be extremely
tedious, and such dissection is unlikely to uncover the
presence of malignancy.
The aforementioned description of SLND closely agrees
with the personal experience of the authors. However, it is
noteworthy that the description is based on currently
available expert opinion, which consists mainly of retro-
spective small institutional studies. The correct technique
of SLND, the anatomic limitations, and the exact indications
are controversial subjects that warrant future investigation.
3.2.3. Cancer control outcomes in patients treated with salvage
lymph node dissection
Data regarding the oncologic outcomes of SLND in patients
with clinical LN relapse are continuously growing. However,
the number of patients treated with this technique, as well
as the available follow-up, is still limited. One of the first
reports that addressed this end point examined the data on
15 patients affected by BCR after primary PCa therapy
associated with 11C-choline PET/CT scan evidence of nodal
recurrence [18]. In this report, all patients had at least one
PET/CT scan with positive LN and no evidence of local
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019
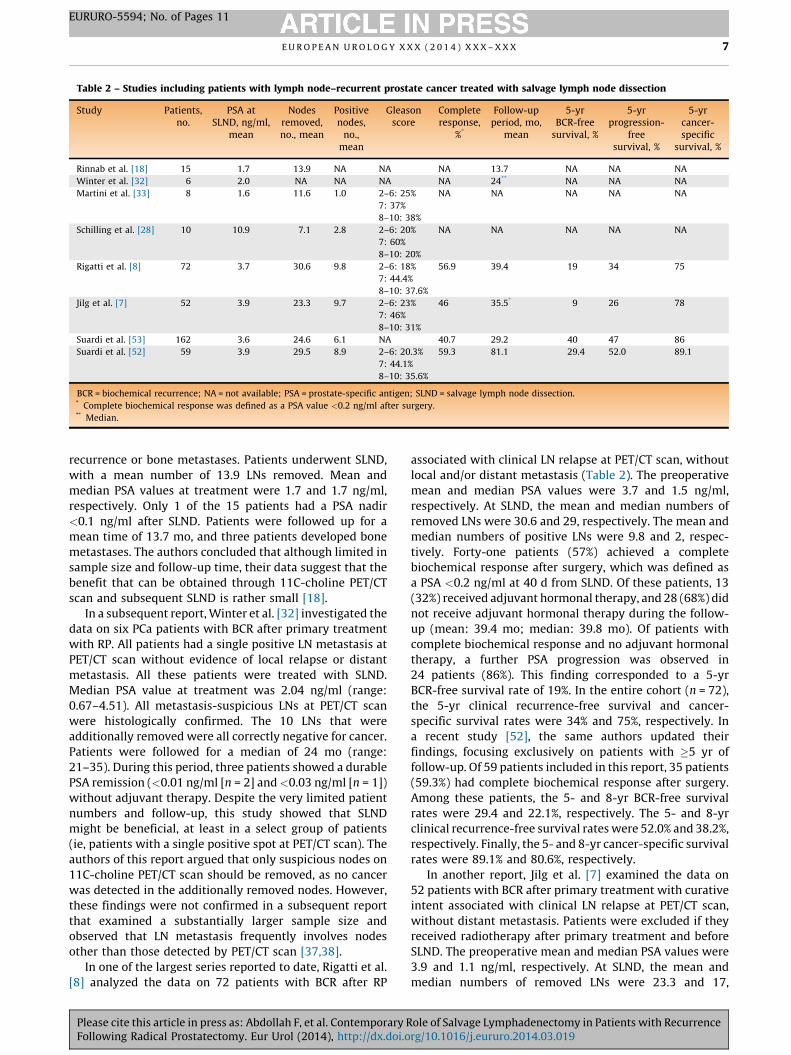
Table 2 – Studies including patients with lymph node–recurrent prostate cancer treated with salvage lymph node dissection
Study Patients,no.
PSA atSLND, ng/ml,
mean
Nodesremoved,no., mean
Positivenodes,
no.,mean
Gleasonscore
Completeresponse,
%*
Follow-upperiod, mo,
mean
5-yrBCR-free
survival, %
5-yrprogression-
freesurvival, %
5-yrcancer-specific
survival, %
Rinnab et al. [18] 15 1.7 13.9 NA NA NA 13.7 NA NA NA
Winter et al. [32] 6 2.0 NA NA NA NA 24** NA NA NA
Martini et al. [33] 8 1.6 11.6 1.0 2–6: 25%
7: 37%
8–10: 38%
NA NA NA NA NA
Schilling et al. [28] 10 10.9 7.1 2.8 2–6: 20%
7: 60%
8–10: 20%
NA NA NA NA NA
Rigatti et al. [8] 72 3.7 30.6 9.8 2–6: 18%
7: 44.4%
8–10: 37.6%
56.9 39.4 19 34 75
Jilg et al. [7] 52 3.9 23.3 9.7 2–6: 23%
7: 46%
8–10: 31%
46 35.5* 9 26 78
Suardi et al. [53] 162 3.6 24.6 6.1 NA 40.7 29.2 40 47 86
Suardi et al. [52] 59 3.9 29.5 8.9 2–6: 20.3%
7: 44.1%
8–10: 35.6%
59.3 81.1 29.4 52.0 89.1
BCR = biochemical recurrence; NA = not available; PSA = prostate-specific antigen; SLND = salvage lymph node dissection.* Complete biochemical response was defined as a PSA value <0.2 ng/ml after surgery.** Median.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 7
EURURO-5594; No. of Pages 11
recurrence or bone metastases. Patients underwent SLND,
with a mean number of 13.9 LNs removed. Mean and
median PSA values at treatment were 1.7 and 1.7 ng/ml,
respectively. Only 1 of the 15 patients had a PSA nadir
<0.1 ng/ml after SLND. Patients were followed up for a
mean time of 13.7 mo, and three patients developed bone
metastases. The authors concluded that although limited in
sample size and follow-up time, their data suggest that the
benefit that can be obtained through 11C-choline PET/CT
scan and subsequent SLND is rather small [18].
In a subsequent report, Winter et al. [32] investigated the
data on six PCa patients with BCR after primary treatment
with RP. All patients had a single positive LN metastasis at
PET/CT scan without evidence of local relapse or distant
metastasis. All these patients were treated with SLND.
Median PSA value at treatment was 2.04 ng/ml (range:
0.67–4.51). All metastasis-suspicious LNs at PET/CT scan
were histologically confirmed. The 10 LNs that were
additionally removed were all correctly negative for cancer.
Patients were followed for a median of 24 mo (range:
21–35). During this period, three patients showed a durable
PSA remission (<0.01 ng/ml [n = 2] and<0.03 ng/ml [n = 1])
without adjuvant therapy. Despite the very limited patient
numbers and follow-up, this study showed that SLND
might be beneficial, at least in a select group of patients
(ie, patients with a single positive spot at PET/CT scan). The
authors of this report argued that only suspicious nodes on
11C-choline PET/CT scan should be removed, as no cancer
was detected in the additionally removed nodes. However,
these findings were not confirmed in a subsequent report
that examined a substantially larger sample size and
observed that LN metastasis frequently involves nodes
other than those detected by PET/CT scan [37,38].
In one of the largest series reported to date, Rigatti et al.
[8] analyzed the data on 72 patients with BCR after RP
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
associated with clinical LN relapse at PET/CT scan, without
local and/or distant metastasis (Table 2). The preoperative
mean and median PSA values were 3.7 and 1.5 ng/ml,
respectively. At SLND, the mean and median numbers of
removed LNs were 30.6 and 29, respectively. The mean and
median numbers of positive LNs were 9.8 and 2, respec-
tively. Forty-one patients (57%) achieved a complete
biochemical response after surgery, which was defined as
a PSA <0.2 ng/ml at 40 d from SLND. Of these patients, 13
(32%) received adjuvant hormonal therapy, and 28 (68%) did
not receive adjuvant hormonal therapy during the follow-
up (mean: 39.4 mo; median: 39.8 mo). Of patients with
complete biochemical response and no adjuvant hormonal
therapy, a further PSA progression was observed in
24 patients (86%). This finding corresponded to a 5-yr
BCR-free survival rate of 19%. In the entire cohort (n = 72),
the 5-yr clinical recurrence-free survival and cancer-
specific survival rates were 34% and 75%, respectively. In
a recent study [52], the same authors updated their
findings, focusing exclusively on patients with �5 yr of
follow-up. Of 59 patients included in this report, 35 patients
(59.3%) had complete biochemical response after surgery.
Among these patients, the 5- and 8-yr BCR-free survival
rates were 29.4 and 22.1%, respectively. The 5- and 8-yr
clinical recurrence-free survival rates were 52.0% and 38.2%,
respectively. Finally, the 5- and 8-yr cancer-specific survival
rates were 89.1% and 80.6%, respectively.
In another report, Jilg et al. [7] examined the data on
52 patients with BCR after primary treatment with curative
intent associated with clinical LN relapse at PET/CT scan,
without distant metastasis. Patients were excluded if they
received radiotherapy after primary treatment and before
SLND. The preoperative mean and median PSA values were
3.9 and 1.1 ng/ml, respectively. At SLND, the mean and
median numbers of removed LNs were 23.3 and 17,
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X8
EURURO-5594; No. of Pages 11
respectively. Mean and median numbers of positive LNs
were 9.7 and 4, respectively. Complete biochemical
response, defined as a PSA value <0.2 ng/ml after surgery,
was achieved in 24 of 52 cases (46%). In 27 of 52 cases (52%),
adjuvant radiotherapy was performed after SLND. A mean
dose of 50.8 Gy (standard deviation [SD]: 3.6) was applied
per patient externally in the anatomic region in which
positive LNs had been confirmed histologically. In six
patients, based on PET/CT findings with additional evidence
of local PCa recurrence in prostatic fossa, a mean dose of
68.7 Gy (SD: 2.39) was locally applied. The median follow-
up of this cohort was 35.5 mo. A total of 24 patients (46%)
had complete biochemical response after surgery, followed
by 1-yr BCR-free survival of 71.8%. In the entire cohort
(n = 52), the 5-yr clinical recurrence-free survival and
cancer-specific survival rates were 26% and 78%, respec-
tively.
Finally, in the only multi-institutional report available to
date, Suardi et al. [53] examined the data from five tertiary
referral centers of 162 patients affected by BCR after RP
associated with nodal recurrence detected at either 11C-
choline PET/TC scan or conventional imaging. The preoper-
ative mean and median PSA values were 3.6 and 1.9 ng/ml,
respectively. At SLND, the mean and median numbers of
removed LNs were 24.6 and 20.0, respectively. The mean
and median number of positive LNs were 6.1 and 2,
respectively. A total of 132 patients (81%) were found to
harbor a pathologically confirmed clinical LN relapse, and
66 patients (41%) achieved a complete biochemical
response after surgery [53].
Taken together, the current data denote that SLND is
feasible and can be used as an option to treat patients with
clinical LN relapse after primary treatment with RP.
However, a significant proportion of patients treated with
this technique will invariably progress to BCR after surgery.
Nonetheless, at 5 yr, approximately 9–19% of these patients
will remain free from BCR, and approximately 26–34% will
remain free from clinical recurrence. These data indicate
that the benefit of SLND in the majority of cases would be to
prolong survival and/or to postpone hormonal therapy, but
not to achieve a complete cure. However, whether or not
this survival benefit would compare preferentially with the
current standard of care (ie, hormonal therapy) is still
unknown because of the lack of comparative data between
these two treatment modalities. Nonetheless, given the
limited survival benefit of hormonal therapy, SLND might
represent a supplementary, and not a substitutive, treat-
ment option.
3.2.4. The importance of patient selection
Despite the limited data available, it appears that SLND
could be beneficial only in a select group of patients. This
idea highlights the importance of correct patient selection
before surgery. Rigatti et al. [8], as well as Jilg et al. [7],
defined several factors that can be helpful in identifying the
best candidates for SLND. Rigatti el al [8] observed that the
5-yr clinical recurrence-free survival was higher for patients
with a preoperative PSA value <4 ng/ml compared with
patients with a PSA �4 ng/ml (48% vs 13%; log-rank:
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
p = 0.004). Conversely, the 5-yr clinical recurrence-free
survival was lower for patients with positive nodes in the
retroperitoneum compared with patients with positive
nodes in the pelvis only (11% vs 53%; p < 0.001). These data
were confirmed in the multivariable analyses, in which
preoperative PSA >4 ng/ml (hazard ratio [HR]: 2.13;
p = 0.03) and the presence of retroperitoneal uptake at
PET/CT scan (HR: 2.92; p = 0.004) were independent
predictors of clinical progression after surgery. Additionally,
Jilg et al. [7] defined a Gleason score of 8–10 (HR: 3.5;
p = 0.03) as an independent predictor of clinical progres-
sion.
Several postoperative factors, including complete bio-
chemical response, the location of positive LNs at SLND, and
the number of positive LNs at SLND, were established as
independent predictors of clinical progression [7,8]. Al-
though these variables can be helpful for postoperative risk
classification and patient counseling, they cannot be used in
selecting the best candidates for surgery preoperatively.
In summary, correct patient selection for SLND is
essential to achieve acceptable cancer control outcomes
and avoid unnecessary morbidity in a significant proportion
of patients. Patients with a low PSA value (<4 ng/ml), well
to moderately differentiated tumor (Gleason score �7), and
a clinical LN relapse limited to the pelvis only might
represent the ideal candidates for SLND. However, a larger
sample size and more homogenous cohorts are necessary to
allow the development of a multivariable tool that can
improve the accuracy of patient selection. Larger cohorts
may allow the identification of other survival predictors. For
example, clinical experience suggests that patients with
biochemical progression despite hormonal therapy are at a
higher risk of mortality. These individuals could not benefit
from SLND. Likewise, age might represent another impor-
tant factor that influences SLND outcomes, while most of
the currently available reports included young and highly
selected patients. Thus, it might be difficult to evaluate the
impact of these factors using the currently available
literature. Older patients might benefit from treatment
modalities other than surgery, such as intensity-modulated
radiation therapy, for the management of clinical LN
relapse. However, data regarding the long-term outcomes
of this modality are scarce and beyond the scope of this
review.
3.2.5. Complications associated with salvage lymph node dissection
Two studies used a systematic way to report the data
regarding postoperative morbidity and mortality in patients
treated with SLND [7,8] Complications were stratified
according to Clavien classification. It is encouraging to
note that most of the reported complications were mild.
Indeed, the most frequent complication was lymphorrhea
(15.3%), followed by fever (14.5%) and ileus (11.2%). High-
grade (Clavien 3b) complications were rare and consisted of
ureteral injury in one case (0.8%) and the necessity of
surgical reintervention in two cases (1.6%). Other complica-
tions, such as lymphoceles and limb lymphedema, might
also occur after SLND. However, these complications were
not reported by the previous two studies [7,8]. This
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 9
EURURO-5594; No. of Pages 11
situation might stem from the fact that these morbidities are
frequently mild and self-limiting. Nonetheless, they should
be considered, and patients should be informed accordingly.
To date, no postoperative mortality was reported after SLND
[7,8]. These data denote that this procedure is feasible and
has an acceptable safety profile. However, larger studies are
warranted to validate these observations. It is noteworthy
that these data originate from tertiary care centers and might
not be generalizable to the community setting. However, we
believe that for the time being, such a delicate and
experimental surgical procedure should be offered only in
high-volume centers and by expert surgeons.
4. Conclusions
The current data, although limited, indicate that PSA
kinetics, especially PSA DT, should guide the decision to
perform PET/CT scan and/or DW-MRI in patients with
suspected clinical LN relapse. For the majority of patients,
SLND might help in postponing hormonal therapy. Indeed,
about half of patients treated with SLND will have an
immediate complete postoperative biochemical response,
and roughly one-third of these patients will remain free
of biochemical relapse for 5 yr. Patients with a PSA value
<4 ng/ml, Gleason score �7, and clinical LN relapse limited
to the pelvis might benefit the most from this procedure.
However, these findings still need to be validated using
rigorous methodology and prospective randomized data.
Author contributions: Firas Abdollah had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Abdollah, Briganti, Montorsi, Stenzl, Stief,
Tombal, Van Poppel, Touijer.
Acquisition of data: Abdollah, Touijer.
Analysis and interpretation of data: Abdollah, Briganti, Montorsi, Stenzl,
Stief, Tombal, Van Poppel, Touijer.
Drafting of the manuscript: Abdollah, Touijer.
Critical revision of the manuscript for important intellectual content:
Briganti, Montorsi, Stenzl, Stief, Tombal, Van Poppel, Touijer.
Statistical analysis: None.
Obtaining funding: None.
Administrative, technical, or material support: None.
Supervision: Briganti, Montorsi, Stenzl, Stief, Tombal, Van Poppel, Touijer.
Other (specify): None.
Financial disclosures: Firas Abdollah certifies that all conflicts of interest,
including specific financial interests and relationships and affiliations
relevant to the subject matter or materials discussed in the manuscript
(eg, employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
References
[1] Han M, Partin AW, Pound CR, Epstein JI, Walsh PC. Long-term
biochemical disease-free and cancer-specific survival following
anatomic radical retropubic prostatectomy: the 15-year Johns
Hopkins experience. Urol Clin North Am 2001;28:555–65.
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
[2] Simmons MN, Stephenson AJ, Klein EA. Natural history of biochem-
ical recurrence after radical prostatectomy: risk assessment for
secondary therapy. Eur Urol 2007;51:1175–84.
[3] Suardi N, Porter CR, Reuther AM, et al. A nomogram predicting long-
term biochemical recurrence after radical prostatectomy. Cancer
2008;112:1254–63.
[4] Roehl KA, Han M, Ramos CG, Antenor JA, Catalona WJ. Cancer
progression and survival rates following anatomical radical retro-
pubic prostatectomy in 3,478 consecutive patients: long-term
results. J Urol 2004;172:910–4.
[5] National Comprehensive Cancer Network clinical practice guide-
lines (NCCN Guidelines). Prostate cancer. Version 1.2014. National
Comprehensive Cancer Network Web site. http://www.nccn.org/
professionals/physician_gls/f_guidelines.asp. Accessed January 31,
2014.
[6] Giovacchini G, Picchio M, Gracia-Parra R, et al. [11C]Choline PET/CT
predicts prostate cancer-specific survival in patients with biochem-
ical failure during androgen deprivation therapy. J Nucl Med
2014;55:233–41.
[7] Jilg CA, Rischke HC, Reske SN, et al. Salvage lymph node dissection
with adjuvant radiotherapy for nodal recurrence of prostate cancer.
J Urol 2012;188:2190–7.
[8] Rigatti P, Suardi N, Briganti A, et al. Pelvic/retroperitoneal salvage
lymph node dissection for patients treated with radical prostatec-
tomy with biochemical recurrence and nodal recurrence detected
by [11C]choline positron emission tomography/computed tomog-
raphy. Eur Urol 2011;60:935–43.
[9] Briganti A, Karnes JR, Pozzo LFD, et al. Two positive nodes represent
a significant cut-off value for cancer specific survival in patients
with node positive prostate cancer: a new proposal based on a two-
institution experience on 703 consecutive N+ patients treated with
radical prostatectomy, extended pelvic lymph node dissection and
adjuvant therapy. Eur Urol 2009;55:261–70.
[10] Abdollah F, Schmitges J, Sun M, et al. A critical assessment of the value
of lymph node dissection at radical prostatectomy: a population-
based study. Prostate. In press. http://dx.doi.org/10.1002/pros.21376
[11] Abdollah F, Sun M, Thuret R, et al. Decreasing rate and extent of
lymph node staging in patients undergoing radical prostatectomy
may undermine the rate of diagnosis of lymph node metastases in
prostate cancer. Eur Urol 2010;58:882–92.
[12] Gandaglia G, Trinh QD, Hu JC, et al. The impact of robot-assisted
radical prostatectomy on the use and extent of pelvic lymph node
dissection in the ‘‘post-dissemination’’ period. Eur J Surg Oncol. In
press. http://dx.doi.org/10.1016/j.ejso.2013.12.016
[13] Briganti A, Abdollah F, Nini A, et al. Performance characteristics of
computed tomography in detecting lymph node metastases in
contemporary patients with prostate cancer treated with extended
pelvic lymph node dissection. Eur Urol 2012;61:1132–8.
[14] DeJong I, Pruim J, Elsinga P, Vaalburg W, Mensink H. C-Choline
positron emission tomography for the evaluation after treatment of
localized prostate cancer. Eur Urol 2003;44:32–9.
[15] Giovacchini G, Picchio M, Briganti A, et al. [11C] Choline positron
emission tomography/computerized tomography to restage pros-
tate cancer cases with biochemical failure after radical prostatec-
tomy and no disease evidence on conventional imaging. J Urol
2010;184:938–43.
[16] Krause BJ, Souvatzoglou M, Tuncel M, et al. The detection rate of
[11C]choline-PET/CT depends on the serum PSA-value in patients
with biochemical recurrence of prostate cancer. Eur J Nucl Med Mol
Imaging 2008;35:18–23.
[17] Picchio M, Messa C, Landoni C, et al. Value of [11C]choline-positron
emission tomography for re-staging prostate cancer: a comparison
with [18F]fluorodeoxyglucose-positron emission tomography. J
Urol 2003;169:1337–40.
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X10
EURURO-5594; No. of Pages 11
[18] Rinnab L, Mottaghy FM, Simon J, et al. [11C]Choline PET/CT
for targeted salvage lymph node dissection in patients with bio-
chemical recurrence after primary curative therapy for prostate
cancer: preliminary results of a prospective study. Urol Int 2008;
81:191–7.
[19] Scattoni V, Picchio M, Suardi N, et al. Detection of lymph-node
metastases with integrated [11C]choline PET/CT in patients with
PSA failure after radical retropubic prostatectomy: results con-
firmed by open pelvic-retroperitoneal lymphadenectomy. Eur Urol
2007;52:423–9.
[20] Bertagna F, Abuhilal M, Bosio G, et al. Role of 11C-choline positron
emission tomography/computed tomography in evaluating patients
affected by prostate cancer with suspected relapse due to prostate-
specific antigen elevation. Jpn J Radiol 2011;29:394–404.
[21] Breeuwsma AJ, Pruim J, van den Bergh ACM, et al. Detection of local,
regional, and distant recurrence in patients with PSA relapse after
external-beam radiotherapy using (11)C-choline positron emission
tomography. Int J Radiat Oncol Biol Phys 2010;77:160–4.
[22] Castellucci P, Fuccio C, Nanni C, et al. Influence of trigger PSA and
PSA kinetics on 11C-choline PET/CT detection rate in patients with
biochemical relapse after radical prostatectomy. J Nucl Med
2009;50:1394–400.
[23] Husarik DB, Miralbell R, Dubs M, et al. Evaluation of [(18)F]-choline
PET/CT for staging and restaging of prostate cancer. Eur J Nucl Med
Mol Imaging 2008;35:253–63.
[24] Reske SN, Blumstein NM, Glatting G. [11C]Choline PET/CT imaging
in occult local relapse of prostate cancer after radical prostatec-
tomy. Eur J Nucl Med Mol Imaging 2008;35:9–17.
[25] Fuccio C, Castellucci P, Schiavina R, et al. Role of 11C-choline PET/CT
in the re-staging of prostate cancer patients with biochemical
relapse and negative results at bone scintigraphy. Eur J Radiol
2012;81:e893–6.
[26] Ceci F, Castellucci P, Mamede M, et al. (11)C-Choline PET/CT in
patients with hormone-resistant prostate cancer showing bio-
chemical relapse after radical prostatectomy. Eur J Nucl Med Mol
Imaging 2013;40:149–55.
[27] Mitchell CR, Lowe VJ, Rangel LJ, Hung JC, Kwon ED, Karnes RJ.
Operational characteristics of 11 C-choline PET/CT for prostate
cancer patients with biochemical recurrence following initial treat-
ment. J Urol 2013;189:1308–13.
[28] Schilling D, Schlemmer HP, Wagner PH, et al. Histological verifica-
tion of 11C-choline-positron emission/computed tomography-
positive lymph nodes in patients with biochemical failure after
treatment for localized prostate cancer. BJU Int 2008;102:446–51.
[29] Abdollah F, Sun M, Thuret R, et al. Lymph node count threshold for
optimal pelvic lymph node staging in prostate cancer. Int J Urol
2012;19:645–51.
[30] Briganti A, Chun FK, Salonia A, et al. Critical assessment of ideal
nodal yield at pelvic lymphadenectomy to accurately diagnose
prostate cancer nodal metastasis in patients undergoing radical
retropubic prostatectomy. Urology 2007;69:147–51.
[31] Heidenreich A, Varga Z, Von Knobloch R. Extended pelvic
lymphadenectomy in patients undergoing radical prostatectomy:
high incidence of lymph node metastasis. J Urol 2002;167:1681–6.
[32] Winter A, Uphoff J, Henke RP, Wawroschek F. First results of
[11C]choline PET/CT-guided secondary lymph node surgery in
patients with PSA failure and single lymph node recurrence after
radical retropubic prostatectomy. Urol Int 2010;84:418–23.
[33] Martini T, Mayr R, Trenti E, et al. The role of C-choline-PET/
CT-guided secondary lymphadenectomy in patients with PSA fail-
ure after radical prostatectomy: lessons learned from eight cases.
Adv Urol 2012;2012:601572.
[34] Mamede M, Ceci F, Castellucci P, et al. The role of 11C-choline PET
imaging in the early detection of recurrence in surgically treated
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
prostate cancer patients with very low PSA level <0.5 ng/mL. Clin
Nucl Med 2013;38:e342–5.
[35] Muller SA, Holzapfel K, Seidl C, Treiber U, Krause BJ, Senekowitsch-
Schmidtke R. Characterization of choline uptake in prostate cancer
cells following bicalutamide and docetaxel treatment. Eur J Nucl
Med Mol Imaging 2009;36:1434–42.
[36] Rinnab L, Mottaghy FM, Blumstein NM, et al. Evaluation of [11C]-
choline positron-emission/computed tomography in patients with
increasing prostate-specific antigen levels after primary treatment
for prostate cancer. BJU Int 2007;100:786–93.
[37] Passoni NM, Suardi N, Abdollah F, et al. Utility of [C]choline PET/CT
in guiding lesion-targeted salvage therapies in patients with pros-
tate cancer recurrence localized to a single lymph node at imaging:
results from a pathologically validated series. Urol Oncol 2014;32,
38.e9-16.
[38] Tilki D, Reich O, Graser A, et al. 18F-Fluoroethylcholine PET/CT
identifies lymph node metastasis in patients with prostate-specific
antigen failure after radical prostatectomy but underestimates its
extent. Eur Urol 2013;63:792–6.
[39] Somford DM, Futterer JJ, Hambrock T, Barentsz JO. Diffusion and
perfusion MR imaging of the prostate. Magn Reson Imaging Clin
North Am 2008;16:685–95, ix.
[40] Seitz M, Shukla-Dave A, Bjartell A, et al. Functional magnetic
resonance imaging in prostate cancer. Eur Urol 2009;55:801–14.
[41] Eiber M, Beer AJ, Holzapfel K, et al. Preliminary results for charac-
terization of pelvic lymph nodes in patients with prostate cancer by
diffusion-weighted MR-imaging. Invest Radiol 2010;45:15–23.
[42] Beer AJ, Eiber M, Souvatzoglou M, et al. Restricted water diffusibility
as measured by diffusion-weighted MR imaging and choline uptake
in (11)C-choline PET/CT are correlated in pelvic lymph nodes in
patients with prostate cancer. Mol Imaging Biol 2011;13:352–61.
[43] Budiharto T, Joniau S, Lerut E, et al. Prospective evaluation of 11C-
choline positron emission tomography/computed tomography and
diffusion-weighted magnetic resonance imaging for the nodal
staging of prostate cancer with a high risk of lymph node metasta-
ses. Eur Urol 2011;60:125–30.
[44] Lecouvet FE, El Mouedden J, Collette L, et al. Can whole-body
magnetic resonance imaging with diffusion-weighted imaging re-
place Tc 99m bone scanning and computed tomography for single-
step detection of metastases in patients with high-risk prostate
cancer? Eur Urol 2012;62:68–75.
[45] Thoeny HC, Triantafyllou M, Birkhaeuser FD, et al. Combined ultra-
small superparamagnetic particles of iron oxide-enhanced and
diffusion-weighted magnetic resonance imaging reliably detect
pelvic lymph node metastases in normal-sized nodes of bladder
and prostate cancer patients. Eur Urol 2009;55:761–9.
[46] Wang YX. Superparamagnetic iron oxide based MRI contrast
agents: current status of clinical application. Quant Imaging Med
Surg 2011;1:35–40.
[47] Stenzl A, Cowan NC, De Santis M, et al. Treatment of muscle-
invasive and metastatic bladder cancer: update of the EAU guide-
lines. Eur Urol 2011;59:1009–18.
[48] Pizzocaro G, Algaba F, Horenblas S, et al. EAU penile cancer guide-
lines 2009. Eur Urol 2010;57:1002–12.
[49] Ji J, Yuan H, Wang L, Hou J. Is the impact of the extent of lymphadenec-
tomy in radical prostatectomy related to the disease risk? A single
center prospective study. J Surg Res 2012;178:779–84.
[50] Giovacchini G, Picchio M, Coradeschi E, et al. Predictive factors of
[(11)C]choline PET/CT in patients with biochemical failure after
radical prostatectomy. Eur J Nucl Med Mol Imaging 2010;37:301–9.
[51] Joniau S, Van den Bergh L, Lerut E, et al. Mapping of pelvic lymph
node metastases in prostate cancer. Eur Urol 2013;63:450–8.
[52] Suardi N, Gandaglia G, Gallina A, et al. Long-term outcomes of salvage
lymph node dissection for clinically recurrent prostate cancer:
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 11
EURURO-5594; No. of Pages 11
results of a single-institution series with a minimum follow-up
of 5 years. Eur Urol. In press. http://dx.doi.org/10.1016/j.eurur0.
2014.02.011
[53] Suardi N, Karnes J, Joniau S, et al. Salvage lymph node dissection for
patients treated with radical prostatectomy with biochemical recur-
rence and imaging-detected nodal metastases. J Urol 2013;189:
e317–8.
[54] Vees H, Buchegger F, Albrecht S, et al. 18F-Choline and/or 11C-acetate
positron emission tomography: detection of residual or progressive
subclinical disease at very low prostate-specific antigen values
(<1 ng/mL) after radical prostatectomy. BJU Int 2007;99:1415–20.
[55] Pelosi E, Arena V, Skanjeti A, et al. Role of whole-body 18F-choline
PET/CT in disease detection in patients with biochemical relapse after
radical treatment for prostate cancer. La Radiol Med 2008;113:
895–904.
[56] Richter JA, Rodriguez M, Rioja J, et al. Dual tracer 11C-choline and
FDG-PET in the diagnosis of biochemical prostate cancer relapse
after radical treatment. Mol Imaging Biol 2010;12:210–7.
[57] Panebianco V, Sciarra A, Lisi D, et al. Prostate cancer: 1HMRS-DCEMR
at 3T versus [(18)F]choline PET/CT in the detection of local prostate
cancer recurrence in men with biochemical progression after radical
retropubic prostatectomy (RRP). Eur J Radiol 2012;81:700–8.
[58] Giovacchini G, Picchio M, Scattoni V, et al. PSA doubling time for
prediction of [(11)C]choline PET/CT findings in prostate cancer
patients with biochemical failure after radical prostatectomy.
Eur J Nucl Med Mol Imaging 2010;37:1106–16.
[59] Castellucci P, Fuccio C, Rubello D, et al. Is there a role for (1)(1)C-
choline PET/CT in the early detection of metastatic disease in
Please cite this article in press as: Abdollah F, et al. Contemporary RFollowing Radical Prostatectomy. Eur Urol (2014), http://dx.doi.o
surgically treated prostate cancer patients with a mild PSA increase
<1.5 ng/ml? Eur J Nucl Med Mol Imaging 2011;38:55–63.
[60] Henninger B, Vesco P, Putzer D, et al. [18F]Choline positron emission
tomography in prostate cancer patients with biochemical recurrence
after radical prostatectomy: influence of antiandrogen therapy—a
preliminary study. Nucl Med Commun 2012;33:889–94.
[61] Schillaci O, Calabria F, Tavolozza M, et al. Influence of PSA, PSA
velocity and PSA doubling time on contrast-enhanced 18F-choline
PET/CT detection rate in patients with rising PSA after radical
prostatectomy. Eur J Nucl Med Mol Imaging 2012;39:589–96.
[62] Marzola MC, Chondrogiannis S, Ferretti A, et al. Role of 18F-choline
PET/CT in biochemically relapsed prostate cancer after radical pros-
tatectomy: correlation with trigger PSA, PSA velocity, PSA doubling
time, and metastatic distribution. Clin Nucl Med 2013;38:e26–32.
[63] Kitajima K, Murphy RC, Nathan MA, et al. Detection of recurrent
prostate cancer after radical prostatectomy: comparison of 11C-
choline PET/CT with pelvic multiparametric MR imaging with
endorectal coil. J Nucl Med 2014;55:223–32.
[64] Heesakkers RA, Hovels AM, Jager GJ, et al. MRI with a lymph-node-
specific contrast agent as an alternative to CT scan and lymph-node
dissection in patients with prostate cancer: a prospective multi-
cohort study. Lancet Oncol 2008;9:850–6.
[65] Harisinghani MG, Barentsz J, Hahn PF, et al. Noninvasive detection
of clinically occult lymph-node metastases in prostate cancer. New
Engl J Med 2003;348:2491–9.
[66] Wang L, Hricak H, Kattan MW, et al. Combined endorectal and
phased-array MRI in the prediction of pelvic lymph node metastasis
in prostate cancer. AJR Am J Roentgenol 2006;186:743–8.
ole of Salvage Lymphadenectomy in Patients with Recurrencerg/10.1016/j.eururo.2014.03.019
Related Documents