Contaminated Product Water as the Source of Phialemonium curvatum Bloodstream Infection among Patients Undergoing Hemodialysis • Author(s): Carol Y. Rao , ScD, Constance Pachucki , MD, Salvatore Cali , MPH, Mangai Santhiraj , MPH, Kathi L. K. Krankoski , BS, Judith A. Noble‐Wang , PhD, David Leehey , MD, Subhash Popli , MD, Mary E. Brandt , PhD, Mark D. Lindsley , ScD, Scott K. Fridkin , MD, Matthew J. Arduino , DrPH Source: Infection Control and Hospital Epidemiology, Vol. 30, No. 9 (September 2009), pp. 840- 847 Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiology of America Stable URL: http://www.jstor.org/stable/10.1086/605324 . Accessed: 08/04/2011 18:10 Your use of the JSTOR archive indicates your acceptance of JSTOR's Terms and Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's Terms and Conditions of Use provides, in part, that unless you have obtained prior permission, you may not download an entire issue of a journal or multiple copies of articles, and you may use content in the JSTOR archive only for your personal, non-commercial use. Please contact the publisher regarding any further use of this work. Publisher contact information may be obtained at . http://www.jstor.org/action/showPublisher?publisherCode=ucpress. . Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printed page of such transmission. JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaborating with JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology. http://www.jstor.org

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Contaminated Product Water as the Source of Phialemonium curvatum Bloodstream Infectionamong Patients Undergoing Hemodialysis • Author(s): Carol Y. Rao , ScD, Constance Pachucki , MD, Salvatore Cali , MPH, Mangai Santhiraj, MPH, Kathi L. K. Krankoski , BS, Judith A. Noble‐Wang , PhD, David Leehey , MD, SubhashPopli , MD, Mary E. Brandt , PhD, Mark D. Lindsley , ScD, Scott K. Fridkin , MD, Matthew J.Arduino , DrPHSource: Infection Control and Hospital Epidemiology, Vol. 30, No. 9 (September 2009), pp. 840-847Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiology ofAmericaStable URL: http://www.jstor.org/stable/10.1086/605324 .Accessed: 08/04/2011 18:10
Your use of the JSTOR archive indicates your acceptance of JSTOR's Terms and Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's Terms and Conditions of Use provides, in part, that unlessyou have obtained prior permission, you may not download an entire issue of a journal or multiple copies of articles, and youmay use content in the JSTOR archive only for your personal, non-commercial use.
Please contact the publisher regarding any further use of this work. Publisher contact information may be obtained at .http://www.jstor.org/action/showPublisher?publisherCode=ucpress. .
Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printedpage of such transmission.
JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology.
http://www.jstor.org

infection control and hospital epidemiology september 2009, vol. 30, no. 9
o r i g i n a l a r t i c l e
Contaminated Product Water as the Source of Phialemoniumcurvatum Bloodstream Infection among Patients
Undergoing Hemodialysis
Carol Y. Rao, ScD; Constance Pachucki, MD; Salvatore Cali, MPH; Mangai Santhiraj, MPH; Kathi L. K. Krankoski, BS;Judith A. Noble-Wang, PhD; David Leehey, MD; Subhash Popli, MD; Mary E. Brandt, PhD; Mark D. Lindsley, ScD;
Scott K. Fridkin, MD; Matthew J. Arduino, DrPH
objective. We investigated a cluster of cases of bloodstream infection (BSI) due to the mold Phialemonium at a hemodialysis centerin Illinois and conducted a cohort study to identify risk factors.
design. Environmental assessment and cohort study.
setting. A hemodialysis center in a tertiary care hospital.
methods. A case patient was defined as a person who underwent dialysis at the center and had a blood sample that tested positive forPhialemonium curvatum on culture. We reviewed microbiology and medical records and tested water, surface, and dialysate samples byculture. Molds isolated from environmental and clinical specimens were identified by their morphological features and confirmed bysequencing DNA.
results. We identified 2 case patients with BSI due to P. curvatum. Both became febrile and hypotensive while undergoing dialysis onthe same machine at the same treatment station, although on different days. Dialysis machines were equipped with waste handling optionports that are used to discard dialyzer priming fluid. We isolated P. curvatum from the product water (ie, water used for dialysis purposes)at 2 of 19 treatment stations, one of which was the implicated station.
conclusion. The source of P. curvatum was likely the water distribution system. To our knowledge, this is the first report of patientsacquiring a mold BSI from contaminated product water. The route of exposure in these cases of BSI due to P. curvatum may be relatedto the malfunction and improper maintenance of the waste handling option ports. Waste handling option ports have been previouslyimplicated as the source of bacterial BSI due to the backflow of waste fluid into a patient’s blood line. No additional cases of infectionwere noted after remediation of the water distribution system and after discontinuing use of waste handling option ports at the facility.
Infect Control Hosp Epidemiol 2009; 30:840-847
From the Divisions of Healthcare Quality Promotion (C.Y.R., J.A.N.-W., S.K.F., M.J.A.) and of Foodborne, Bacterial, and Mycotic Diseases (M.E.B.,M.D.L.), Centers for Disease Control and Prevention, Atlanta, Georgia; and Edward Hines, Jr. Veterans Affairs Hospital, Hines (C.P., M.S., K.L.K.K., D.L.,S.P.), and the University of Illinois at Chicago School of Public Health, Chicago (S.C.), Illinois.
Received November 20, 2008; accepted April 20, 2009; electronically published July 17, 2009.� 2009 by The Society for Healthcare Epidemiology of America. All rights reserved. 0899-823X/2009/3009-0004$15.00. DOI: 10.1086/605324
In 2005, there were 314,162 people with end-stage renal dis-ease who were undergoing maintenance hemodialysis therapyin the United States.1 Patients receiving chronic hemodialysisare at increased risk of developing a bloodstream infection(BSI) as a result of repeated vascular access.2,3 The environ-mental sources associated with clusters of cases of BSI includethe following: contamination of dialysate, medication, or wa-ter used for dialysis purposes (hereafter referred to as productwater); inadequate disinfection of water treatment or distri-bution systems; and improper maintenance procedures.4-7 Al-though cases of BSI due to gram-positive bacteria are com-mon among patients undergoing hemodialysis, cases of BSI
that are unrelated to catheter use and due to molds areuncommon.8
We investigated 2 cases of Phialemonium curvatum fun-gemia among 60 patients who were undergoing hemodialysis;these 2 cases occurred in late November 2005 at the EdwardHines, Jr. Veterans Affairs (VA) Hospital, which is located 12miles west of downtown Chicago in Hines, Illinois. Phiale-monium is a mold isolated from soil, sewage, air, and water.9
Infections with this mold are extremely rare; 18 human caseshave been described in the published literature (ie, cutaneousor endovascular cases of endocarditis, endophthalmitis, peri-tonitis, fungemia, cyst, osteomyelitis, and/or pulmonary gran-

p. curvatum bsi as a result of hemodialysis 841
ulomas).10-20 In our investigation, we report the third outbreakof P. curvatum BSI and the second associated with hemodi-alysis in the greater Chicago metropolitan area.10,15,21
methods
Case Definition and Ascertainment
We defined a case patient as a person who underwent he-modialysis treatment at the Hines VA Hospital and had ablood sample that tested positive for P. curvatum on cultureduring the period from October 31 through December 21,2005 (hereafter referred to as the investigation period). Wereviewed the hospital’s infection control surveillance data andclinical microbiology laboratory records for information onmolds isolated during the investigation period. Dialysis staffobtained blood samples from all patients who underwenthemodialysis on December 9 and 10 and on December 20and 21, 2005, for culture. We interviewed case patients andconducted a medical record review.
Assessment of Infection Control Procedures
We interviewed staff, reviewed the maintenance and cleaningschedules of the dialysis machines and the water distributionsystem, and observed treatment processes and procedures,including the preparation and administration of medication.We reviewed the logs of microbiological testing results forboth product water and dialysate for the past year and themachine service logs for the past 6 months.
Environmental and Ventilation Assessments
We visually inspected the hemodialysis unit and the on-sitelong-term care unit, including the product water distributionsystem and the heating, ventilating, and air-conditioning sys-tems. We estimated the air exchange rate in the main roomof the hemodialysis unit. We disassembled a dialysis machine(Cobe Centry System 3; Gambro Healthcare) suspected ofmalfunctioning or being improperly maintained, and we ob-tained samples from various internal and external surfacesusing moistened sterile swabs for fungal culture analysis. Weobtained samples from surfaces in the hemodialysis unit andthe ventilation system, and we collected product water fromhemodialysis treatment stations and from various points inthe water distribution system using a clean-catch method(approximately 800-mL volume collected per sample).
Clinical and Environmental Samples for Fungal Analysis
The on-site clinical microbiology laboratory at the hospitalplaced patients’ blood samples in standard aerobic and an-aerobic bottles (BacT/ALERT culture media; bioMerieux)with incubation at 35�C for 7 days. The Phialemonium isolateswere subcultured onto Sabouraud dextrose agar slants andsent to the Centers for Disease Control and Prevention inAtlanta, Georgia, for confirmation.
We shipped the environmental samples overnight to theCenters for Disease Control and Prevention. We streakedswab samples onto potato dextrose agar plates. We filteredwater samples through membrane filters (pore size, 0.45 mm;diameter, 47 mm) that were placed directly onto potato dex-trose agar plates. These plates were incubated at ambientroom temperature (ie, ∼23�C). Fungal growth was observedover a 14-day period.
The suspected Phialemonium isolates recovered from eitherclinical or environmental samples were analyzed by sequenc-ing the ribosomal internal transcribed spacer (ITS) regionusing ITS5 and ITS4 primers and the BigDye TerminatorCycle Sequencing kit (Applied Biosystems). We analyzed se-quences with a genetic analyzer (ABI PRISM 310; AppliedBiosystems).
Retrospective Cohort Study
To determine risk factors for fungemia, we abstracted avail-able dialysis log records for sessions that occurred during theinvestigation period. We collected the following data: patientdemographic characteristics, machine and station used, nameof dialysis technician, type of vascular access, time (ie, shift)that dialysis took place, and therapy schedule. Because thesensitivity of blood culture for P. curvatum is unknown, wealso evaluated the following clinical indicators for fungemia:fever (ie, a temperature of 138�C) and hypotension (ie, asystolic blood pressure reading of !90 mm Hg) that occurredduring a session. Blood pressure was monitored every 30minutes during the dialysis session, and an aural temperaturewas taken at the beginning and end of each session.
Statistical Methods
Data were entered into JMP, version 5.01 (SAS), and analyzedusing SAS, version 9.12 (SAS). We examined the frequenciesof visits across treatment stations and the patterns of dialysismachine use. To examine risk factors for infection, we used ageneralized estimating equation method (PROC GENMOD)with a stationary Toeplitz correlation structure to account forpossible correlation between repeated observations from anindividual patient.
results
Case Descriptions
From the 60 patients who were undergoing chronic dialysis(dialyzed 3 times per week) in the hemodialysis unit, weidentified 2 case patients. The demographic and clinical char-acteristics of the case patients are shown in Table 1. Both casepatients became febrile and hypotensive while undergoinghemodialysis on machine 14 at station 5. Patient A’s catheter(PermCath; Kendall Healthcare) tested negative on culture.

842 infection control and hospital epidemiology september 2009, vol. 30, no. 9
table 1. Demographic and Clinical Characteristics of the 2 Case Patients with Bloodstream Infection Due toPhialemonium curvatum at Edward Hines, Jr. Veterans Affairs Hospital in Hines, Illinois, in 2005
Characteristic Patient A Patient B
Age Late 60s Late 70sSex Male MalePlace of residence On-site long-term care unit On-site long-term care unitDuration of hemodialysis 4 months 3 monthsReason for hemodialysis End-stage renal disease secondary
to diabetic nephropathyEnd-stage renal disease and ne-
phrectomy for renal cellcarcinoma
Immunosuppression Noa Nob
Dialysis access Double-lumen silastic catheter Arteriovenous fistulaDays of dialysis Monday, Wednesday, and Friday Monday, Wednesday, and FridayDialysis shift Afternoon Afternoonc
Initial symptoms Low-grade temperature (x37.8�C[x100�F]); hypotensive whileon dialysis; loss ofconsciousness
Febrile soon after dialysis (37.5�C[99.4�F]); hypotensive whileon dialysis
Date of symptom onset and blood draw Nov 25 Nov 28Blood culture results Positive for fungal elements Positive for fungal elementsDialysis treatment machine used at
symptom onsetMachine 14 Machine 14
Dialysis treatment water tap used atsymptom onset
Water tap 3A Water tap 3A
a With a white blood cell count of cells/L on November 26, 2005.953.1 # 10b With a white blood cell count of cells/L on November 28, 2005.911.4 # 10c Except for November 25 and 28, 2005, when he was switched to the morning shift.
Environmental and Ventilation Assessments
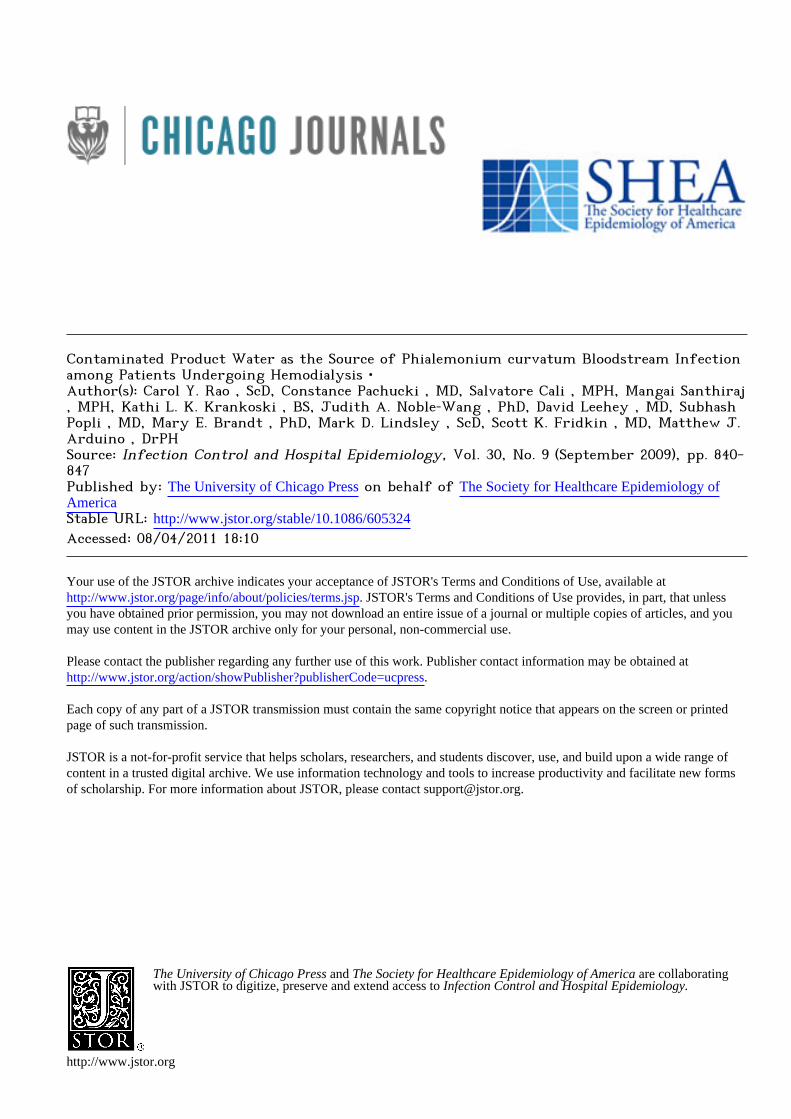
Figure 1 is a diagram of the 17 treatment stations, the 19product water taps, the product water distribution system,and the ventilation supply and exhaust registers of the he-modialysis unit.
Water treatment. First, municipal water undergoes supple-mental chlorination at a separate facility on the hospital cam-pus. At the hemodialysis unit, the water is treated by softening,carbon adsorption, and reverse osmosis. The treated water isstored in a reverse-osmosis holding tank; water leaving thetank is polished by deionization and filtered through a 0.2-mmfilter before distribution to the individual treatment stations.Unused product water recirculates back into the reverse-os-mosis holding tank. As originally designed, the system was adirect feed system. Several years before this outbreak, a con-tractor retrofitted the system, forming an indirect feed loopdistribution system. The water distribution system, however,is not in a continuous loop and included several dead ends,multiple branches, and long runs of piping (Figure 1). A con-tractor sanitizes the distribution system biannually with Minn-care (Minntech). The last sanitization occurred approximately5 months before the outbreak.
Building ventilation system. The hemodialysis unit is onthe sixth floor of a 15-story building. Conditioned air is sup-plied by 2 rooftop air handling units with 3 sets of filters.Air is not recirculated. The air exchange rate on December14, 2005, in the main treatment room of the hemodialysis
unit was approximately 2 air changes per hour, which wasbelow the recommended guideline of 6–7 air changes perhour for healthcare facilities.22
Assessment of Infection Control Procedures
Hemodialysis procedures. All medications, with the excep-tion of heparin, are premeasured and packaged by the phar-macy. Heparin was administered from multidose bottles. Ingeneral, barrier protection procedures (ie, the use of mask,gown, and gloves) and appropriate antisepsis were followed.Chloroprep (Enturia) or isopropyl alcohol was used to cleanand disinfect the vascular access site or the area around thecatheter. The duration of antiseptic contact ranged from 20seconds to 1 minute.
Water sampling and laboratory analysis procedures. Thestaff members of the hemodialysis unit conduct monthly mi-crobiological testing of water from all 19 water taps and ofdialysate from all 22 machines in the unit. The reported sam-pling and analysis methods, however, were not in accordancewith the Association for the Advancement of Medical In-strumentation (AAMI) guidelines.23 For example, the dialysistechnicians wiped the water taps with bleach and then col-lected approximately 100 mL of product water. For the anal-ysis of water and dialysate on culture, samples of 100 mL ofproduct water (AAMI guidelines recommend 500 mL) wereplated onto trypticase soy agar, a general-purpose mediumused for determining bacterial contamination, and incubated
p. curvatum bsi as a result of hemodialysis 843
figure 1. Diagram of the hemodialysis unit and schematic of the water distribution system of the Edward Hines, Jr. Veterans AffairsHospital in Hines, Illinois (not drawn to scale). Phialemonium curvatum was isolated from water samples from water taps 2B and 3A.Station 5 was the treatment station where the 2 case patients underwent dialysis. RO, reverse osmosis.
for 48 hours at 35�C. Bacterial colony-forming units (cfu)were enumerated and calculated per milliliter. From Januaryto December 2005, 1 of 223 water samples and 4 of 252dialysate samples were above the AAMI standard of 200 cfu/mL; none of these samples were from machine 14, which wassuspected of causing these cases of BSI.
A contractor performed monthly preventive maintenanceof the water treatment system and quarterly endotoxin andchemical analyses on product water. Samples taken in January,June, and September 2005 met acceptable AAMI limits forendotoxin and chemicals.
Dialysis machines. The 22 dialysis machines (numberedfrom 4 to 26) were Cobe Centry System 3 dialysis machines;all but one had been retrofitted with waste handling optionports in 1998–1999. Staff members did not follow the man-ufacturer’s recommendations regarding routine disinfectionor safety checks for backflow of these ports.24 The machinesundergo an acid-bleach cleaning with a final water rinse ev-ery evening. In the morning, the technicians do test runs andthen start priming the first dialyzer with saline. Every Sat-urday night, the dialysate lines are filled with a disinfectant(Actril; Minntech) until Monday morning. Dialyzers are notreused. A review of the dialysis machines’ annual preventivemaintenance service records showed that, in the previous 12months, the service representative noted that 5 machines (in-
cluding machine 14) had a “yeast infiltrate” in the tubing inthe waste handling option port and that this tubing had tobe replaced (this information was included in the December16, 2005, record for machine 14).
Clinical and Environmental Microbiology
Fungal elements were detected in the blood samples obtainedfrom patients A and B on the days they became symptomaticwhile undergoing dialysis (Table 1). Molecular sequencingconfirmed that the isolates recovered from the case patients’blood samples were isolates of P. curvatum (type 4 with var-iable nucleotides at key alignment positions in the ITS ofthymidine at 65, a gap at 83, thymidine at 84, and cytosineat 456). Both patients’ isolates had identical ITS sequences.
Fungi were detected on a variety of environmental surfacesin the hemodialysis unit and in the building ventilation sys-tem (Table 2). The waste handling option port and associat-ed tubing on the machine 14 were replaced before our in-vestigation and were unavailable for inspection. Samples ob-tained from the replacement tubing of the waste handlingoption port from machine 14 yielded yeast (Candida tropi-calis) on culture (Table 2).
We obtained samples of water from various points in thewater treatment room, from all 17 treatment stations and
844 infection control and hospital epidemiology september 2009, vol. 30, no. 9
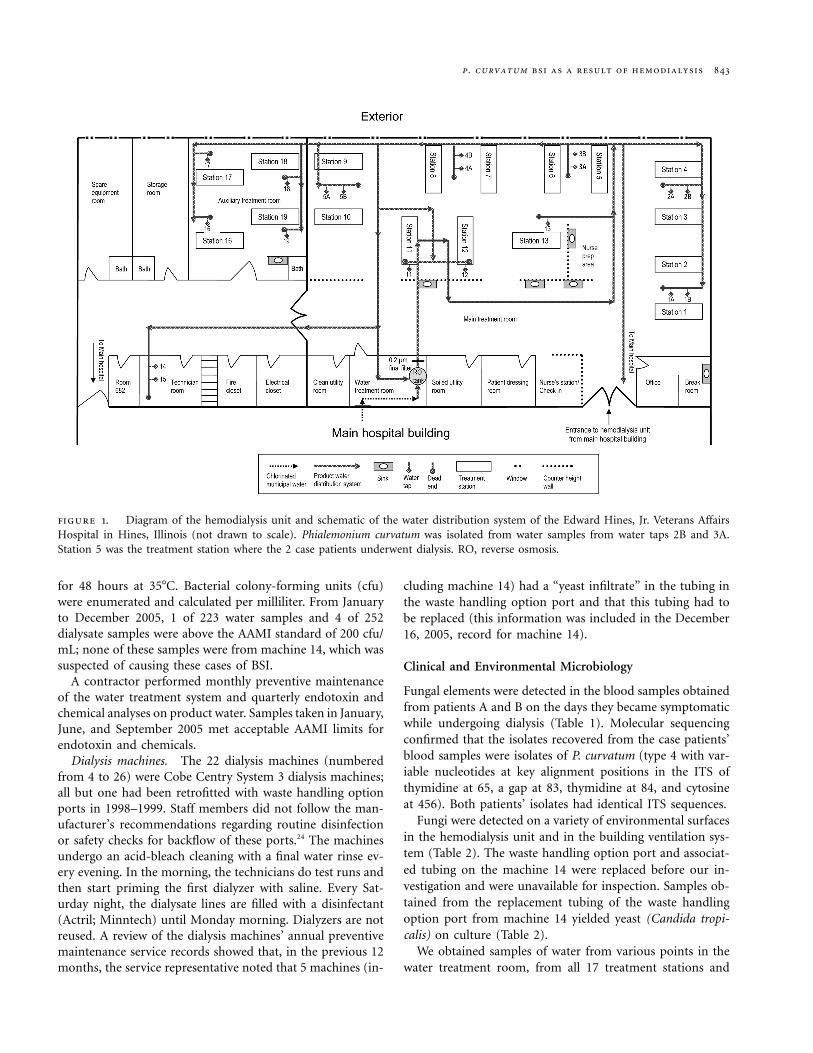
table 2. Culture Yielding Molds and Yeasts from Environmental Samples in the Hemodialysis Unit and in the Building VentilationSystem at Edward Hines, Jr. Veterans Affairs Hospital in Hines, Illinois, in 2005
Sample locationDate ofsample
No. ofsamples
Sampletype
Type(s) of mold and yeastdetected on culture
Air handling units Dec 12 8 Dry swab All samples with hyaline nonsporulating molds; yeasts;Aspergillus, Penicillium, and/or Cladosporium species
Drain from water tap 3 Dec 12 2 Dry swab 2 samples with Fusarium solani speciesAir handling units from on-site
long-term care unitDec 16 2 Wet swab Alternaria, Epicoccum nigrum, Trichoderma, and/or
Cladosporium species; 7 hyaline nonsporulatingmolds
Unit air filters from dialysis unit Dec 16 5 Wet swab Hyaline nonsporulating molds; Alternaria, Penicillium,and/or Cladosporium species
Machine 14 waste handling optionport (implicated dialysis machine)
Dec 12 7 Wet swab 2 samples with Candida tropicalis in the new wastehandling option port tubing; all other samples neg-ative for fungi
Water room (after final filtration) Dec 12and 21
2 Water No mold growth detected
Municipal water from on-site long-term care unit
Dec 16 2 Water No mold growth detected
Water tap 3A (implicated treatmentstation)
Dec 12 1 Water Phialemonium curvatum, nonsporulating molds, andCladosporium species
All water taps Dec 21 18 Water Molds recovered from water taps 1A, 1B, 2A, 2B, 4A,4B, 5A, 12, 15, 16, 17, 18, and 19 (hyaline nonspo-rulating molds and unidentified pigmented molds);P. curvatum recovered from water tap 2B and F. so-lani recovered from water tap 16
Water room (recirculated water) Dec 21 1 Water Hyaline molds detected in recirculated water returningto water treatment room
Water taps Dec 29 5 Water All samples negative for molds after disinfection ofwater distribution system on Dec 22
from 2 water taps in the technician’s room. The water samplescollected in the water treatment room after a final filtrationbut before distribution to the treatment stations were negativefor fungi on culture. However, fungi were detected in 14 ofthe water samples from the treatment stations (Table 2). Prod-uct water samples from water taps 3A and 2B grew P. cur-vatum on culture by the fifth day of incubation. The ITSsequencing for both environmental isolates matched the ITSsequence of the 2 clinical P. curvatum isolates. The entirewater distribution system was sanitized on December 22,2005. No molds were detected in water samples on December29 (Table 2).
Risk Factors for BSI: Retrospective Cohort Study
During the investigation period, 60 patients received chronicdialysis treatment. The patients were all men (median age,60.1 years). Of these 60 patients, 29 (48.3%) used a catheterfor vascular access. These 60 patients received a total of 1,159dialysis sessions during the investigation period, both in thehemodialysis unit and at other hospital units.
Of these 1,159 dialysis sessions, patients became febrile 6times (0.5%) and hypotensive 214 times (18.5%) while un-dergoing dialysis. Two patients became both febrile and hy-potensive during 3 dialysis sessions (0.26%). One of these
patients was the index case (patient A). Patient B becamefebrile soon after his dialysis session.
We examined incidents of hypotension in relation to sta-tion, product water tap, machine use, and session schedule(Table 3). There were too few febrile incidents for statisticalmodeling. Because adjacent treatment stations could be at-tached to either adjacent water taps (eg, station 5 could beattached to water tap 3A or 3B), we combined adjacent watertaps for the statistical analysis. Although not statistically sig-nificant, patients became hypotensive more often when un-dergoing dialysis while attached to water taps 2A or 2B (ie,in treatment stations 3 and 4) or water taps 3A or 3B (ie, intreatment stations 5 and 6) ( ). No other risk factorP p .08(Table 3) showed a trend.
discussion
Little is known about the ecology of the Phialemonium genus,especially with regard to it being the cause of human infec-tions. Environmental sources of pathogenic Phialemoniumspecies have been reported.10-14,16-18,21,20 The routes of exposurefor these reported infections were hypothesized to be airbornespores settling into open wounds, onto medical devices priorto implantation (eg, catheters and heart valves), onto skin

p. curvatum bsi as a result of hemodialysis 845
table 3. Data on Incidents of Hypotension Among Patients Un-dergoing Dialysis at Edward Hines, Jr. Veterans Affairs Hospital inHines, Illinois, in 2005, in Relation to Station, Product Water Tap,Machine Use, and Session Schedule
Risk factor(s)
Proportion (%)of dialysis sessionsin which patients
experiencedhypotensiona Pb
Dialysis machineMachine 14 13/39 (33.3) .15Others 147/841 (17.5)
Water tapTaps 2A, 2B, 3A, and 3B 59/264 (22.3) .08Others 154/886 (17.4)
Dialysis shiftMonday, Wednesday, and Friday 110/693 (15.9) .22Tuesday, Thursday, and Saturday 104/449 (23.2)
Dialysis sessionMorning 115/572 (20.1) .56Afternoon 87/524 (16.6)
Patient age!60 years old 126/596 (21.1) .22x60 years old 88/560 (15.7)
Overall frequency 214/1,156 (18.5) NA
note. NA, not available.a With a systolic blood pressure reading of !90 mm Hg.b Using repeated-measured analysis of the 60 patients who were undergoingchronic dialysis (dialyzed 3 times per week) in the hemodialysis unit.
prior to injection, and into fluids prior to injection. We iden-tified 2 patients with Phialemonium fungemia who were un-dergoing dialysis treatment on the same machine that wasattached to a water tap contaminated with P. curvatum. TheITS sequence of the isolate recovered from the patient andthat of the isolate recovered from a water sample were iden-tical. These isolates have the same ITS sequence (ie, type 4)as the isolates recovered from patients from the previous he-modialysis outbreak in the Chicago area in 2001–2002.15,21 TheITS sequencing results indicate that the clinical and environ-mental isolates are different from those isolates identified inother parts of the world.18 There are no analytical methods tofurther differentiate P. curvatum strains from within the samegeographic region.
Because P. curvatum was isolated from samples of bothpatient blood and product water, we believe that the sourceof the mold was most likely biofilms in the product waterdistribution system. This system at the Hines VA Hospitalhas dead-end pipes, long runs of piping, and unused taps,all which cannot be adequately disinfected.23 Although notstatistically significant, the retrospective cohort study impliesthat the product water was a factor; patients undergoingdialysis on machines attached to the 2 contaminated watertaps were more likely to experience hypotension than werepatients undergoing dialysis on machines attached to the wa-ter taps ( ). In other studies, contamination of theP p .08
product water distribution system has been implicated in he-modialysis-related bacterial infections.5,7,25,26
Although the product water distribution system was thelikely source, product water does not come into direct con-tact with a patient’s blood under proper dialysis procedures.Molds are too large to pass through the dialysis membrane.We believe that reflux of contaminated product water fromthe waste handling option port into the blood line duringthe priming process was the most likely route of exposure.Several observations support this theory. First, unintendedbackflow of waste fluid from waste handling option ports hasbeen associated with several previous outbreaks of BSI.27-31 Asurvey of 290 US hemodialysis units found that only 14% ofthese units regularly performed the manufacturer’s recom-mended backflow check.32 Second, hemodialysis unit staff didnot routinely disinfect or check the competency of the wastehandling option ports. Third, in November 2004, there were3 patients undergoing dialysis at the Hines VA Hospital whodeveloped a BSI due to Enterobacter cloacae. E. cloacae wasisolated from samples of the dialysate and the mix line tubingof the patients’ dialysis machine. This previous outbreak ofinfection illustrates a precedent regarding the failure of theseparation of the extracorporeal circuit and dialysate path atthis hemodialysis unit.
Other possible sources and routes of exposure are unlikely.Because 1 case patient received dialysis with a catheter andthe other with an arteriovenous fistula, we do not believethat dialysis access type was the common route of exposureas in the previous outbreak associated with dialysis.15 We didnot find P. curvatum in any other environmental samples. He-modialyzers were not reused; therefore, cross-contaminationfrom improperly disinfected dialyzers could not have occurred.Dialyzer membrane malfunction is a possibility. We ruled outthe multidose bottles of heparin as the source because onewould have expected to see cases of infection in adjacent treat-ment stations during the same shift (horizontal time course)rather than during different shifts on the same station (verticaltime course). Technician error may be a risk factor. We couldnot examine fungemia in relation to specific technicians be-cause many dialysis log records were incomplete.
There were limitations to our investigation. We used non-specific clinical indicators of infection (ie, incidents of feverand hypotension) to investigate factors associated with in-fections, because we had limited statistical power with only2 case patients. In addition, we could not test the originalwaste handling option port assembly of machine 14 for P.curvatum contamination because it had been removed andwas not available for testing. Dialysis machine tubing, how-ever, is susceptible to fungal growth.31 In the machine main-tenance records, the service representative noted “yeastlike”debris in the tubing of several machines in the year prior tothe outbreak, including machine 14. Phialemonium speciescan grow in the form of sporodochia, which can look mac-roscopically similar to yeast growth.15
To our knowledge, we have described the first report of

846 infection control and hospital epidemiology september 2009, vol. 30, no. 9
dialysis product water as the environmental source of BSIdue to pathogenic P. curvatum. Molds and yeasts were com-monly found in surveys of dialysis water quality.33-35 In routinesampling and analysis of dialysis water and dialysate, however,mold growth may be missed because the AAMI microbialguidelines only require a 48-hour incubation period.23 In ourinvestigation, P. curvatum required 4–5 days of incubation tobe detected in the environmental culture samples. In futureinvestigations of mold BSIs, laboratory analytical protocolsshould be modified to accommodate the longer incubationperiods needed to detect mold growth.
The Centers for Disease Control and Prevention recom-mend that the containers used for the priming solutionshould be discarded or should be disinfected before reuse.36
A 2002 survey of US hemodialysis centers showed that useof nondisposable containers (including waste handling optionports) for priming the dialyzer was associated with an increasein cases of hepatitis C infection.37 Cases of BSI associated withthe use of a waste handling option port were first reportedover 10 years ago.32 The cases of BSI in this outbreak weremost likely due to a combination of factors, including P. curva-tum biofilm formation in the water distribution system, failureto perform a waste handling option port competency check todetect backflow, and malfunction and improper disinfectionof the waste handling option port. All of these factors musthave been present in close temporal proximity for an infectionto have occurred. On the basis of the available evidence ofcases of BSI associated with the use of a waste handling optionport, the use of a waste handling option port should be dis-couraged unless educational sessions are instituted for endusers regarding proper quality assurance, use, disinfection, andmaintenance of waste handling option ports.
acknowledgments
We thank Dr. David Kleinbaum for statistical guidance, Drs. Craig Conoverand Kathleen Ritger for scientific assistance, and Ms. Shirley McClinton, Ms.Karen Stamey, and the Hines VA Hospital dialysis technicians for technicalassistance.
Financial support. S.C. was supported by cooperative agreement U50/CCU524174-01 from the Centers for Disease Control and Prevention.
Potential conflicts of interest. All authors report no conflicts of interestrelevant to this article.
Address reprint requests to Carol Y. Rao, ScD, Division of HealthcareQuality Promotion, Centers for Disease Control and Prevention, 1600 CliftonRoad, Mailstop A-35, Atlanta, GA 30333 ([email protected]).
The findings and conclusions are those of the authors and do not nec-essarily represent the official position of the Centers of Disease Control andPrevention.
references
1. US Renal Data System (USRDS) 2007 annual data report: atlas of chronickidney disease and end-stage renal disease in the United States. Bethesda,MD: National Institutes of Health, National Institute of Diabetes andDigestive and Kidney Diseases; 2007.
2. Taylor G, Gravel D, Johnston L, Embil J, Holton D, Paton S.; Canadian
Nosocomial Infection Surveillance Program; Canadian Hospital Epide-miology Committee. Incidence of bloodstream infection in multicenterinception cohorts of hemodialysis patients. Am J Infect Control 2004; 32:155–160.
3. Hoen B, Paul-Dauphin A, Hestin D, Kessler M. EPIBACDIAL: A mul-ticenter prospective study of risk factors for bacteremia in chronic he-modialysis patients. J Am Soc Nephrol 1998; 9:869–876.
4. Oie S, Kamiya A, Yoneda I, et al. Microbial contamination of dialysate andits prevention in haemodialysis units. J Hosp Infect 2003; 54:115–119.
5. Tokars JI, Arduino MJ, Alter MJ. Infection control in hemodialysis units.Infect Dis Clin North Am 2001; 15:797–812.
6. Grohskopf LA, Roth VR, Feikin DR, et al. Serratia liquefaciens blood-stream infections from contamination of epoetin alfa at a hemodialysiscenter. N Engl J Med 2001; 344:1491–1497.
7. Jackson BM, Becksague CM, Bland LA, Arduino MJ, Meyer L, JarvisWR. Outbreak of pyrogenic reactions and gram-negative bacteremia ina hemodialysis center. Am J Nephrol 1994; 14:85–89.
8. Tokars JI, Miller ER, Stein G. New national surveillance system for he-modialysis-associated infections: initial results. Am J Infect Control 2002;30:288–295.
9. Gams W, McGinnis MR. Phialemonium, a new anamorph genus in-termediate between Phialophora and Acremonium. Mycologia 1983; 75:977–987.
10. Gavin PJ, Sutton DA, Katz BZ. Fatal endocarditis in a neonate caused bythe dematiaceous fungus Phialemonium obovatum: case report and reviewof the literature. J Clin Microbiol 2002; 40:2207–2212.
11. Guarro J, Nucci M, Akiti T, et al. Phialemonium fungemia: two docu-mented nosocomial cases. J Clin Microbiol 1999; 37:2493–2497.
12. Heins-Vaccari EM, Machado CM, Saboya RS, et al. Phialemonium cur-vatum infection after bone marrow transplantation. Rev Inst Med TropSao Paulo 2001; 43:163–166.
13. King D, Pasarell L, Dixon DM, McGinnis MR, Merz WG. A pheohyphomy-cotic cyst and peritonitis caused by Phialemonium species and a reevaluationof its taxonomy. J Clin Microbiol 1993; 31:1804–1810.
14. McGinnis MR, Gams W, Goodwin MN. Phialemonium obovatum infec-tion in a burned child. J Med Vet Mycol 1986; 24:51–55.
15. Proia LA, Hayden MK, Kammeyer PL, et al. Phialemonium: an emergingmold pathogen that caused 4 cases of hemodialysis-associated endovas-cular infection. Clin Infect Dis 2004; 39:373–379.
16. Schønheyder HC, Jensen HE, Gams W, et al. Late bioprosthetic valveendocarditis caused by Phialemonium aff. curvatum and Streptococcussanguis: a case report. J Med Vet Mycol 1996; 34:209–214.
17. Scott RS, Sutton DA, Jagirdar J. Lung infection due to opportunistic fungus,Phialemonium obovatum, in a bone marrow transplant recipient: an emerg-ing infection with fungemia and Crohn disease–like involvement of thegastrointestinal tract. Ann Diagn Pathol 2005; 9:227–230.
18. Strahilevitz J, Rahav G, Schroers HJ, et al. An outbreak of Phialemoniuminfective endocarditis linked to intracavernous penile injections for thetreatment of impotence. Clin Infect Dis 2005; 40:781–786.
19. Zayit-Soudry S, Neudorfer M, Barak A, Loewenstein A, Bash E, Siegman-Igra Y. Endogenous Phialemonium curvatum endophthalmitis. Am J Oph-thalmol 2005; 140:755–757.
20. Dan M, Yossepowitch O, Hendel D, Shwartz O, Sutton DA. Phialemon-ium curvatum arthritis of the knee following intra-articular injection ofa corticosteroid. Med Mycol 2006; 44:571–574.
21. Clark T, Huhn GD, Conover C, et al. Outbreak of bloodstream infectionwith the mold Phialemonium among patients receiving dialysis at a he-modialysis unit. Infect Control Hosp Epidemiol 2006; 27:1164–1170.
22. Centers for Disease Control and Prevention. Guidelines for environ-mental infection control in health-care facilities: recommendations ofCDC and the Healthcare Infection Control Practices Advisory Com-mittee (HICPAC). MMWR Recomm Rep 2003; 52(RR-10):1–44.
23. Association for the Advancement of Medical Instrumentation. ANSI/AAMI RD52:2004: dialysate for hemodialysis. Arlington, VA: Associationfor the Advancement of Medical Instrumentation; 2004.
24. GAMBRO Renal Care Products. COBE Waste Handling Option (WHO):

p. curvatum bsi as a result of hemodialysis 847
instructions for use with the COBE Centrysystem 3 family of dialysis de-livery systems. Lakewood, CO: GAMBRO Renal Care Products, Inc.; 1999.
25. Jornet AR, Garcia AG, Mariscal D, et al. An outbreak of gram-negativebacteremia (GNB), especially Enterobacter cloacae, in patients with long-term tunnelled haemodialysis catheters. Nefrologia 2003; 23:333–343.
26. Azadian BS, Beck A, Curtis JR, et al. Disseminated infection with Myco-bacterium chelonei in a haemodialysis patient. Tubercle 1981; 62:281–284.
27. Block C, Backenroth R, Gershon E, et al. Outbreak of bloodstream in-fectious associated with dialysis machine waste ports in a hemodialysisfacility. Eur J Clin Microbiol Infect Dis 1999; 18:723–725.
28. Wang SA, Levine RB, Carson LA, et al. An outbreak of gram-negativebacteremia in hemodialysis patients traced to hemodialysis machinewaste drain ports. Infect Control Hosp Epidemiol 1999; 20:746–751.
29. Olver WJ, Webster C, Clements H, Weston V, Boswell T. Two cases ofEnterococcus faecalis bacteremia associated with a hemodialysis ma-chine. J Infect Dis 1999; 179:1312–1312.
30. Jochimsen EM, Frenette C, Delorme M, et al. A cluster of bloodstreaminfections and pyrogenic reactions among hemodialysis patients tracedto dialysis machine waste-handling option units. Am J Nephrol 1998; 18:485–489.
31. Arnow PM, Garcia-Houchins S, Neagle MB, Bova JL, Dillon JJ, Chou
T. An outbreak of bloodstream infections arising from hemodialysisequipment. J Infect Dis 1998; 178:783–791.
32. Centers for Disease Control and Prevention. Outbreaks of gram-negativebacterial bloodstream infections traced to probable contamination ofhemodialysis machines—Canada, 1995; United States, 1997; and Israel,1997. MMWR Morb Mortal Wkly Rep 1998; 47:55–59.
33. Arvanitidou M, Spaia S, Velegraki A, et al. High level of recovery of fungifrom water and dialysate in haemodialysis units. J Hosp Infect 2000; 45:225–230.
34. Klein E, Pass T, Harding GB, Wright R, Million C. Microbial and en-dotoxin contamination in water and dialysate in the central United States.Artif Organs 1990; 14:85–94.
35. Bambauer R, Schauer M, Jung WK, Daum V, Vienken J. Contaminationof dialysis water and dialysate. A survey of 30 centers. ASAIO J 1994; 40:1012–1016.
36. Centers for Disease Control and Prevention. Recommendations for pre-venting transmission of infections among chronic hemodialysis patients.MMWR Recomm Rep 2001; 50(RR-5):1–43.
37. Finelli L, Miller JT, Tokars JI, Alter MJ, Arduino MJ. National surveillanceof dialysis-associated diseases in the United States, 2002. Semin Dial2005; 18:52–61.
Related Documents