CONTACT DERMATITS OPD CASE PRESENTATION

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CONTACT DERMATITS
OPD CASE PRESENTATION

IDENTIFYING DATA
A.B., 68/M, Roman Catholic, Married, from San Juan City who consulted SJMC-OPD, Dermatology Clinic on January 6, 2010 for
the 1st time.

CHIEF COMPLAINT
Pruritic Rash on Nape x 1 Month

TEMPORAL PROFILE
- Perfume - Rash - Ointment

• PAST MEDICAL HISTORY 2000: Hypertension St II, controlled,
maintained on Amlodipine 10mg/t 1 tab OD (-) DM, BA, COPD (-) allergies to food or drugs
• FAMILY HISTORY Hypertension, DM – maternal side
• SOCIAL HISTORY Stopped smoking 10 years ago Non alcoholic beverage drinker No history of drug abuse

PHYSICAL EXAMINATIONGeneral Survey Conscious, coherent, ambulatory, Not in distressVital signs BP: 130/80 HR: 86 RR: 19 To: 36.8°C
Skin Brown, Warm, moist, good skin turgorErythematous, maculopapular rashes with irregular border on right nape area, ~3inches widest diameterErythematous, maculopapular rashes with irregular border on right & left shoulders, ~2inches widest diameterErythematous maculopapular rash with irregular border on chest, ~6inches widest diameter




PHYSICAL EXAMINATIONHEENT Normocephalic, atraumatic, anicteric sclera, pink palpebral
conjunctivae, non periorbital edema, no cervical lymphadenopathies
Chest/lungs Equal Chest Expansion, Clear Breath sounds, no retractions
CVS Adynamic precordium, normal rate, regular rhythm, distinct S1 and S2, no murmurs
Abdomen Flat, soft, normoactive bowel sounds, liver span ~4cm right subcostal margin, nonpalpable spleen, no mass nor tenderness noted, tympanitic upon percussion
Genitalia Grossly male external genitalia, papule on right testes, no penile discharge, SMR 4
Extremities Full and equal pulses, no edema, no cyanosis

NEUROLOGIC EXAMINATIONMSE IntactCN I Able to identify test substanceCN II 3-4 mm EBRTL, (+) ROR, OUCN III, IV, VI Full and intact EOM’sCN V Intact V1-V3CN VII No facial asymmetryCN VIII Intact gross hearingCN IX, X Uvula midlineCN XI Good shoulder shrugCN XII Tongue midline, no fasciculationsMotor 5/5 in allSensory 100% intact in allDTR’s ++ in allPathologic reflex No Babinski, no clonusCerebellar No nystagmus notedMeninges Supple neck

SALIENT POINTS
• 68/M• Pruritic rash on nape• No known food nor drug
allergies• No Bronchial asthma
• History of perfume application
• Erythematous, maculopapular rashes with irregular border on nape area, shoulders, chest

INITIAL DIAGNOSIS
Allergic Contact Dermatitis

DIFFERENTIAL DIAGNOSIS
• Irritant contact dermatitis• Lichen simplex chronicus• Asteatotic Eczema• Atopic Dermatitis
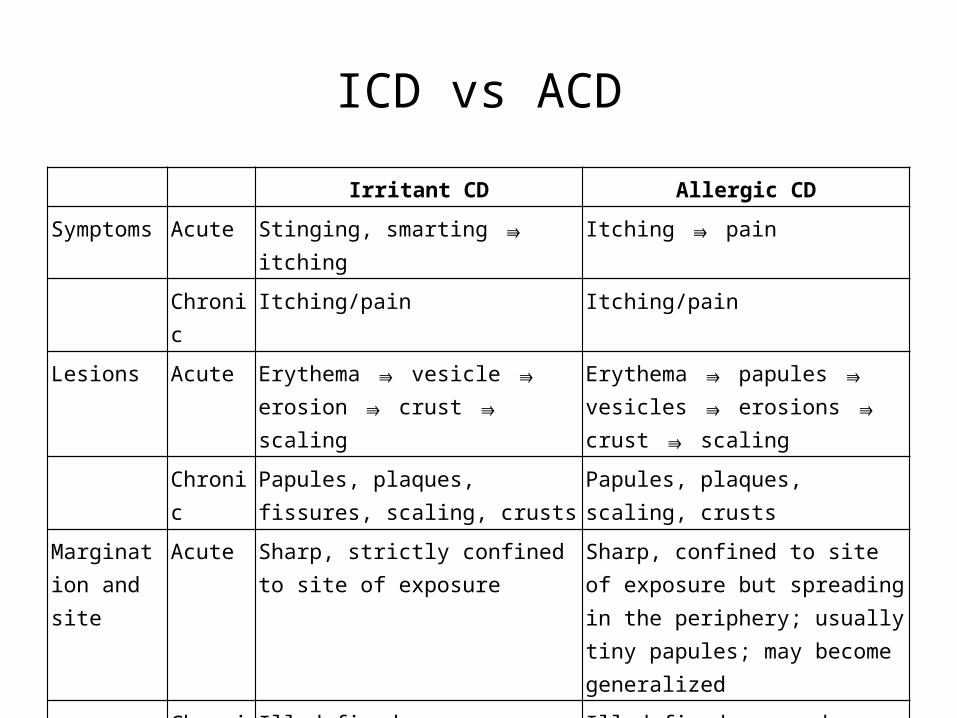
ICD vs ACD
Irritant CD Allergic CD
Symptoms Acute Stinging, smarting itching ⇛ Itching pain ⇛
Chronic Itching/pain Itching/pain
Lesions Acute Erythema vesicle erosion ⇛ ⇛ ⇛crust scaling⇛
Erythema papules vesicles ⇛ ⇛ ⇛erosions crust scaling ⇛ ⇛
Chronic Papules, plaques, fissures, scaling, crusts
Papules, plaques, scaling, crusts
Margination and site
Acute Sharp, strictly confined to site of exposure
Sharp, confined to site of exposure but spreading in the periphery; usually tiny papules; may become generalized
Chronic Ill-defined Ill-defined, spreads

ICD vs ACD
Irritant CD Allergic CD
Evolution Acute Rapid (few hours after exposure) Not so rapid (12 to 72 h after exposure)
Chronic Months to years of repeated exposure
Months or longer; exacerbation after every reexposure
Causative agents
Dependent on concentration of agent and state of skin barrier; occurs only above threshold level
Relatively independent of amount applied, usually very low concentrations sufficient but depends on degree of sensitization
Incidence May occur in practically everyone Occurs only in the sensitized

FINAL DIAGNOSIS
ALLERGIC CONTACT DERMATITIS

PATHOGENESIS
• Classic Type IV Hypersensitivity Reaction• antigen is taken up by Langerhans cells in the epidermis,
which process the antigen and migrate from the epidermis to the draining lymph nodes, where they present the processed antigen in association with MHC class II molecules to T cells that then proliferate.
• Sensitized T cells leave the lymph node, enter the blood circulation, home to the skin, and, after being presented by Langerhans cells with the same specific antigen, produce and mediate the release by other cells of a variety of cytokines.
• Thus, all the skin becomes hypersensitive to the contact allergen and will react wherever the specific allergen is represented.


ALLERGENS
Allergen Principal Sources of Contact
Nickel sulfate Metals, metals in clothing, jewelry, catalyzing agents
Neomycin sulfate Usually contained in creams, ointments
Balsam of Peru Topical medications
Fragrance mix Fragrances, cosmetics
Thimerosal Antiseptics
Sodium gold thiosulfate Medication
Formaldehyde Disinfectant, curing agents, plastics
Quaternium-15 Disinfectant
Cobalt chloride Cement, galvanization, industrial oils, cooling agents, eyeshades
Bacitracin Ointments, powder

TYPES OF ACDACUTE Well-demarcated erythema and edema on which are superimposed
closely spaced, nonumbilicated vesicles, and/or papules in severe reactions, bullae, confluent erosions exuding serum, and crusts
SUBACUTE Plaques of mild erythema showing small, dry scales, sometimes associated with small, red, pointed or rounded, firm papules.
CHRONIC Plaques of lichenification (thickening of the epidermis with deepening of the skin lines in parallel or rhomboidal pattern), scaling with satellite, small, firm, rounded or flat-topped papules, excoriations, erythema, and pigmentation.

CHARACTERISTICSARRANGEMENT Initially, confined to area of contact with allergen [e.g., earlobe
(earrings), dorsum of foot (shoes), wrist (watch or watch-band), collar-like (necklace), lips (lipstick)]. Often linear, with artificial patterns, an "outside job." Plant contact often results in linear lesions (e.g., Rhus dermatitis). Initially confined to site of contact, later spreading beyond.
EXTENT Isolated, localized to one region or generalized
PATTERN Random or on exposed areas

COURSE
• EVOLUTION• ACUTE
– Erythema papules vesicles erosions crusts scaling.
• CHRONIC– Papules scaling lichenification
excoriations– Chronic inflammation with thickening,
fissuring, scaling, and crusting results

LABORATORY
• Complete blood count• Dermatopathology• Patch tests

PLAN
• Identify and remove the etiologic agent• Termination of Exposure• Topical Therapy
Related Documents











