Constipation with Colonic Inertia A Manifestation of Systemic Disease? ALAIN WATIER, GHISLAIN DEVROEDE. ANDRIZ DURANCEAU, MOHAMED ABDEL- RAHMAN, COLETTE DUGUAY, MARCELLE D. FORAND, LI~ON TI~TREAULT, PIERRE ARHAN, JACQUES LAMARCHE, and MOSTAFA ELHILALI Transit of radiopaque markers was delayed in the ascending colon of 51 females and 3 males treated for severe idiopathic constipation. Onset of symptoms was between age i0 and 20 in more than half of the patients. Eighteen percent had previously undergone unnecessary laparotomy for large bowel pseudoobstruction. Stool frequency ranged from 1 stool e~)ery three days to 1 every 2 months. Twenty-six percent suffered from fecal incontinence. In addition, 30% had orthostatic hypotension and 15% galactorrhea of idiopathic origin. Patients had a higher than normal anal pressure (P < 0.001). They all had a rectoanal inhibitory reflex, but it was abnormal in 76%. In the upper esophageal sphincter, resting pressure was higher (P < 0.02), and coordination poorer (P < 0.05) than in normal control subjects. Incidence of spontaneous tertiary contractions in the body of the esophagus was greater than normal (P < 0.03). In the lower esophageal sphincter, resting pressure was lower (P = 0.001) and gastroesophageal gradient weaker (P = 0.05). Closing pressure of the sphincter was lower (P < 0.001) and coordination less adequate (P < 0.02). After subcutaneous injection of 0.035 mg/kg bethanechol, urinary bladder intraluminal pressure increased by over 15 cm 1420 in 31% of patients but never did in controls, and average maximal pressure was greater (P < 0.025). Time taken to reach peak pressure was shorter (P < 0.01). This study provides evidence that patients who suffer from constipation with colonic inertia also have abnormal function in other hollow viscera. The high incidence of extraintestinal symptoms provides further suggestion of the existence of one or more underlying systemic diseases. In order to have a more objective appraisal of the sympt0m of constipation, radiopaque markers may be used to study segmental colonic transit times (1- 4). This study was designed to describe constipated From the Centre de recherche en pathophysiologie digestive, drPartements de Chirurgie grnrrale et d,Urologie, Facult6 de Mrdecine, Universit6 de Sherbrooke, Sherbrooke, Qurbec, Canada; Drpartement de Chirurgie, Facult6 de Mrdecine, Uni- versit6 de Montrral, Montrral, Qurbec, Canada; and Drparte- ments de i~hysiologieet de Chirurgi e prdiatrique, Centre Hospi- taller Necker-Enfants-Malades, Paris, France. Partly supported by the following granting agencies: CRM (Canada) (MT-3511); CRL INSERM (77:2-1857); la sous-com- mission franco-qurbrcoise pour les accords de la santr; le Centre de Recherche Mrdicale de l'Universit6 de Sherbrooke (CRMUS). Address for reprint requests: Dr. Ghislain Devroede, Drparte- ment de Chirurgie grnrrale, Centre Hospitalier Universitaire, Sherbrooke, J1H 5N4, Qurbec, Canada. Manuscript received June 23, 1981; revised manuscript re- ceived April 20, 1983; accepted June 14, 1983. patients who suffer from colonic inertia, where the entire colon fails to propel contents, and to test the hypothesis that their constipation may be a manifes- tation of otherwise asymptomatic systemic disease. MATERIALS AND METHODS Between January 1, 1969, and January 1, 1979, 54 patients (51 females, 3 males) (aged 12-76), evaluated for constipation of idiopathic origin, were found to have Colonic inertia. Clinical Evaluation. A meticulous clinical and radiologi- cal evaluation led to the exclusion of known causes of constipation (4), including scleroderma and underlying disease. Lactose tolerance was evaluated as normal from history and dietary trial. Patients were instructed to eat a high-residue diet (29.9 g dietary fibers per day) and encouraged to defectate at regular intervals. They recorded their bowel habit for one Digestive Diseases and Sciences, Vol. 28, No. ll (November 1983) 0163-2116/83/1100-1025503.00/0 1983 Plenum Publishing Corporation 1025

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Constipation with Colonic Inertia A Manifestation of Systemic Disease?
A L A I N W A T I E R , G H I S L A I N D E V R O E D E . ANDRIZ D U R A N C E A U , M O H A M E D A B D E L - R A H M A N , C O L E T T E D U G U A Y , M A R C E L L E D. F O R A N D , LI~ON TI~TREAULT, P I E R R E
A R H A N , J A C Q U E S L A M A R C H E , and M O S T A F A E L H I L A L I
Transit o f radiopaque markers was delayed in the ascending colon of 51 females and 3 males treated for severe idiopathic constipation. Onset o f symptoms was between age i0 and 20 in more than half o f the patients. Eighteen percent had previously undergone unnecessary laparotomy for large bowel pseudoobstruction. Stool frequency ranged from 1 stool e~)ery three days to 1 every 2 months. Twenty-six percent suffered from fecal incontinence. In addition, 30% had orthostatic hypotension and 15% galactorrhea of idiopathic origin. Patients had a higher than normal anal pressure (P < 0.001). They all had a rectoanal inhibitory reflex, but it was abnormal in 76%. In the upper esophageal sphincter, resting pressure was higher (P < 0.02), and coordination poorer (P < 0.05) than in normal control subjects. Incidence of spontaneous tertiary contractions in the body o f the esophagus was greater than normal (P < 0.03). In the lower esophageal sphincter, resting pressure was lower (P = 0.001) and gastroesophageal gradient weaker (P = 0.05). Closing pressure of the sphincter was lower (P < 0.001) and coordination less adequate (P < 0.02). After subcutaneous injection of 0.035 mg/kg bethanechol, urinary bladder intraluminal pressure increased by over 15 cm 1420 in 31% of patients but never did in controls, and average maximal pressure was greater (P < 0.025). Time taken to reach peak pressure was shorter (P < 0.01). This study provides evidence that patients who suffer from constipation with colonic inertia also have abnormal function in other hollow viscera. The high incidence of extraintestinal symptoms provides further suggestion of the existence o f one or more underlying systemic diseases.
In order to have a more object ive appraisal o f the sympt0m of constipation, radiopaque markers may be used to study segmental colonic transit times (1- 4). This study was designed to describe constipated
From the Centre de recherche en pathophysiologie digestive, drPartements de Chirurgie grnrrale et d,Urologie, Facult6 de Mrdecine, Universit6 de Sherbrooke, Sherbrooke, Qurbec, Canada; Drpartement de Chirurgie, Facult6 de Mrdecine, Uni- versit6 de Montrral, Montrral, Qurbec, Canada; and Drparte- ments de i~hysiologie et de Chirurgi e prdiatrique, Centre Hospi- taller Necker-Enfants-Malades, Paris, France. �9 Partly supported by the following granting agencies: CRM
(Canada) (MT-3511); CRL INSERM (77:2-1857); la sous-com- mission franco-qurbrcoise pour les accords de la santr; le Centre de Recherche Mrdicale de l'Universit6 de Sherbrooke (CRMUS).
Address for reprint requests: Dr. Ghislain Devroede, Drparte- ment de Chirurgie grnrrale, Centre Hospitalier Universitaire, Sherbrooke, J1H 5N4, Qurbec, Canada.
Manuscript received June 23, 1981; revised manuscript re- ceived April 20, 1983; accepted June 14, 1983.
patients who suffer f rom colonic inertia, where the entire colon fails to propel contents , and to test the hypothesis that their const ipat ion may be a manifes- tation of otherwise asymptomat ic systemic disease.
MATERIALS AND METHODS
Between January 1, 1969, and January 1, 1979, 54 patients (51 females, 3 males) (aged 12-76), evaluated for constipation of idiopathic origin, were found to have Colonic inertia.
Clinical Evaluation. A meticulous clinical and radiologi- cal evaluation led to the exclusion of known causes of constipation (4), including scleroderma and underlying disease. Lactose tolerance was evaluated as normal from history and dietary trial.
Patients were instructed to eat a high-residue diet (29.9 g dietary fibers per day) and encouraged to defectate at regular intervals. They recorded their bowel habit for one
Digestive Diseases and Sciences, Vol. 28, No. l l (November 1983)
0163-2116/83/1100-1025503.00/0 �9 1983 Plenum Publishing Corporation
1025

WATIER ET AL
month during which no laxatives or enemas were al- lowed. None produced more than 3 stools/week during this trial period.
Colon and Anorectal Motility Studies. Data on radi- opaque marker transit times through the gastrointestinal tract were obtained in these patients and in age- and sex- matched healthy adults. Subjects ingested 20 markers (cut sections of radiopaque Levin tube) and a plain film of the abdomen was taken daily for a maximum of 8 days while they continued their dietary regimen. Markers were counted in three segments of large bowel: right and left colon, and rectum (1, 2). All patients had a number of markers in the right colon exceeding normal range at least during one day of the trial: this was a prerequisite for inclusion in the study. Mean segmental transk time was calculated with the following formula, as previously de- scribed (3).
i ~, ni t(i + I) - - t ( i - 1 )
t = g i = l
where: t = mean transit time; N = total number of markers; ni = number of markers in a given site, on a given day; t = t ime of film taking; 1 = time interval between films (in this study 24 hr); and i t o j = days.
Anorectal manometry was performed (1). Stools if present in the rectum were evacuated with saline enemas the day before. Pressures were recorded at rest and immediately after distension of a rectal balloon for 3 sec with 5-50 cc of air. This induced in all patients a relaxation of the upper anal canal (rectoanal inhibitory reflex). Thus Hirschsprung's disease Was ruled out. The reflex was analyzed in terms of amplitude and duration (relaxation and contraction time). Amplitude and dura- tion of the rectoanal contractile reflex were also mea- sured. Data were compared to normal values obtained in matched healthy subjects.
EsOphageal Motility Studies. EsOphageal motility stud- ies were performed in 47 of these patients (age 42 -+ 2; X - SE) and 40 asymptomatic controls (age 27 -+ 1) matched for sex, during fasting conditions and without prior medication.
The three-lumen (1.5 mm ID) polyethylene tube (USCI No. 1100) ended laterally (orifice diameter: 0.8 mm) With the opening 5 cm apart in a radial orientation. A Harvard infusion pump perfused saline continuously into the tube at a rate of 3.8ml/min/lumen for the distal sphincter and esophageal body and 7.6ml/min/lumen for the proximal sphincter area. Pharyngea l function was recorded through a water-filled but unperfused lumen. The pres- sures sensed by the column of water in the motility tube were transmitted to external transducers (Hewlett:Pack- ard 1280) placed at head level and recorded on a four- channel polygraph (Hewlett-Packard 7754A). All pres- sureS were recorded in mm Hg and compared to the atmospheric zero reference point. Calibration of the recording system was done before and after each study.
The tube was passed through the nose and th e subjects placed in the supine position. Stomach pressure was recorded, followed by ten pull-throughs. Two milliliters Of water were given as a bolus to induce volUntary swallow- ing. The lower esophageal sphincter pressure was record-
ed through two separate ports having two different orien- tations. The tube was then pulled back to selectively record ten swallows in the distal 10 cm of the esophagus, ten swallows in the proximal 10 cm of the esophageal body, and ten swallows in the upper esophageal sphincter area. The tube orifice recording the upper esophageal sphincter zone was always facing the posterior Wall of the pharynX. Paper speed was at 1 mm/sec for the body and lower esophageal sphincter area, and 5 mm/sec for the upper esophageal sphincter area. Duration of the record- ing varied from 40 to 60 min.
The manometric tracings were interpreted without knowledge of clinical findings. The upper esophageal sphincter recording was analyzed for resting pressure and coordination, which was termed normal when peak pharyngeal contraction corresponded to the nadir of upper esophageal sphincter relaxation and when the latter entirely encompassed the duration of pharyngeal contraction. Both proximal and distal halves of the esophageal body were analyzed for resting pressure, p e a k contraction pressure, and coordination following voluntary deglutition. The incidence and amplitude of secondary and spontaneous tertiary waves was mea- sured. The lower esophageal sphincter area was studied for its absolute resting and closing pressure. The differ- ence between gastric and lower esophageal sphincter resting pressure gave the lower esophageal sphincter gradient. Relaxation of the lower esophageal sphincter was termed normal when the sphincter Pressure fell to within 5 mm Hg of resting intragastric pressure. Relax- ation time was recorded. Coordination was termed nor: real when the relaxation period of the lower esophageal sphincter entirely encompassed the duration of the esophageal contraction.
Bladder Motility Studies. Between January 1, 1979 and January 1, 1980, 16 of these female patients (age 40 --- 9; -+ SD; range 28-51) with colonic inertia and 12 aSymptom- atic female volunteers (age 27 - 4; X -+ SD; range 19-36; P = NS) underwent urodynamic Studies. None had undergone surgery involving the peritoneal floor of the pelvis. This precaution made sure that pelvic nerves had not been damaged. The cohort represents the entire clinical experience of one year with this syndrome and was not therefore selected on the basis of possible urinary symptoms.
A urethral catheter (size 16 French CR Bard Co. No. 102V) was introduced to investigate bladder function.. It was perfused with sterile normal saline (0.9% Nac1), by gra'city, from a 1000-ml receptacle located 100 cm above the subject, at a rate of 20 ml/min. The bladder pressure was monitored via an unperfused epidural Catheter (19 gauge; Deseret Company), connected to a Bentley Tran- tec physiologic pressure transducer (model 800). Signals were passed through a bridge amplifier (Honeywell Accu- data No. 113) and recorded on a recorder (Honeywell No. 540).
Before each study, subjects voided and residual urine was measured. They were then examined twice. First, a conventional c~,stometrogram was done: volume at first desire of voiding, maximal bladder capacity (as deter- mined by the desire of the Subject to terminate the examination because of pain), and pressure-volume rela-
1026 Digestive Diseases and Sciences, Vol. 28, No. 11 (November 1983)
C O N S T I P A T I O N W I T H C O L O N I C I N E R T I A
t i o n s h i p w e r e r e c o r d e d . T h e b l a d d e r w a s t h e n e m p t i e d and t h e r e s p o n s e to t he s u b c u t a n e o u s in j ec t ion o f 0.035 mg/kg b e t h a n e c h o l , wh i l e it c o n t a i n e d 100 ml o f sa l ine , w a s e v a l u a t e d (5, 6). P r e s s u r e w a s a n a l y z e d b e f o r e and at m a x i m a l r e s p o n s e to d rug in j ec t ion . T i m e t a k e n to r e a c h th is p e a k p r e s s u r e f r o m i n j e c t i o n w a s n o t e d .
S t a t i s t i c a l Analys is . S ta t i s t i ca l ana ly s i s o f c l in ica l d a t a w a s d o n e b y ch i s q u a r e c o r r e c t e d a c c o r d i n g to Y a t e s (7). W h e n t h e e x p e c t e d v a l u e s w e r e s m a l l e r t h a n f ive in m o r e t h a n 25% o f t he ce l l s , c o m p a r i s o n s w e r e m a d e t w o by t w o , u s ing F i s h e r ' s e x a c t p r o b a b i l i t y t e s t (8). S t u d e n t ' s t t e s t w a s d o n e to c o m p a r e mo t i l i t y da t a , e x c e p t w h e n t h e r e w a s h e t e r o g e n e i t y o f v a r i a n c e , w h e r e a B e h r e n s - F i s h e r t t e s t w a s u s e d (9). C o r r e l a t i o n coef f i c i en t s w e r e a l so ca l cu l a t ed . D a t a a re e x p r e s s e d as m e a n and s t a n d a r d error.
RESULTS
Clinical Evaluation. Stool frequency averaged 1.6 _+ 0.2 stools per week (range from 1 stool every 3 days to 1 stool every 2 months).
Onset of disease was between age I0 and 20 in over half (58%) of those who remembered how long they had been constipated. Partial intestinal obstruction had led to hospitalization in One third of the patients (2.2 admissions per patient) and lapa- rotomy performed for large bowel obstruction but with no finding (pseudoobstruction) in one fifth (1.6 per patient). Release of intraabdominal "adhe- sions" was done in another fifth.
Twenty-six percent complained of sporadic fecal incontinence and had not undergone prior anorectal surgery. Four patients complained of having bouts of watery colorless diarrhea, unaccompanied by stools. Fecalomas (stools present in the rectum of different consistency than those produced sponta- neously) were present in only four patients and
melanosis coli was only found in five at proctosig- moidoscopy.
Galactorrhea for which no etiology could be found occurred in 15% of patients. Fasting prolactin levels were normal. Orthostatic hypotension was confirmed on examination at least once in 30% of patients. Cerebral functions, cranial nerve testing, motor reflex and sensory function, and gait and stance were all normal.
During episodes of acute abdominal pain, air- fluid levels and distension of the colon mimicking obstruction was a common finding (18 patients).
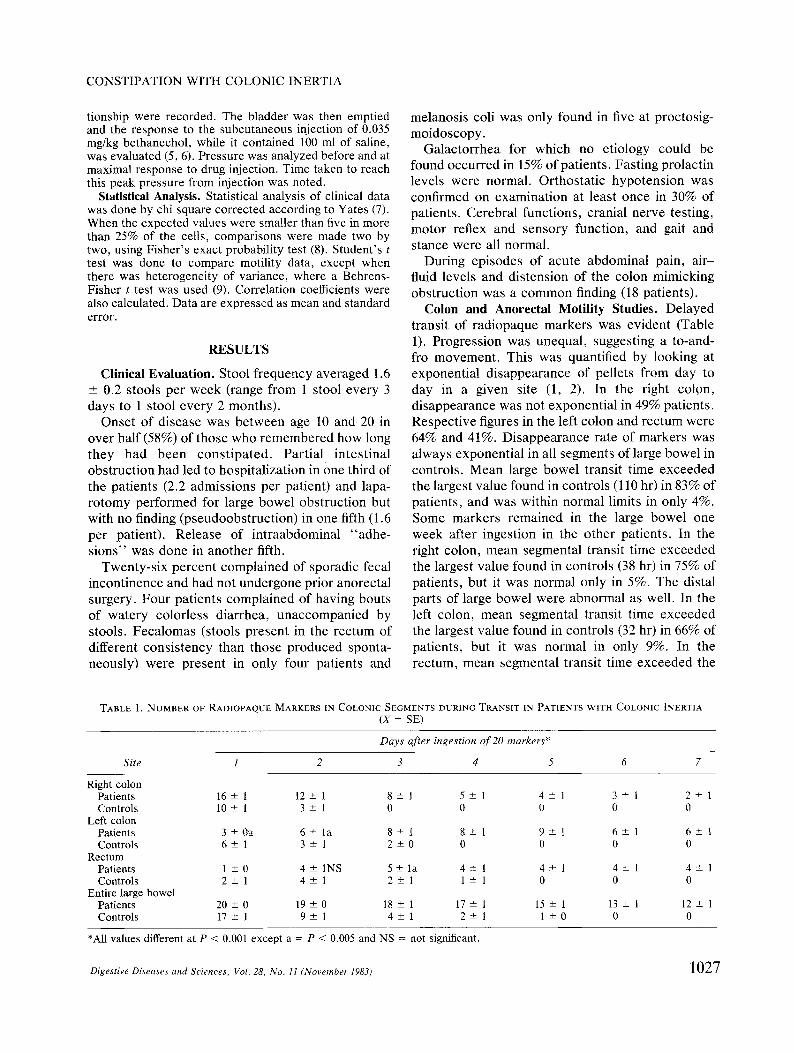
Colon and Anorectal Motility Studies. Delayed transit of radiopaque markers was evident (Table 1). Progression was unequal, suggesting a to-and- fro movement. This was quantified by looking at exponential disappearance of pellets from day to day in a given site (1, 2). In the right colon, disappearance was not exponential in 49% patients. Respective figures in the left colon and rectum were 64% and 41%. Disappearance rate of markers was always exponential in all segments of large bowel in controls. Mean large bowel transit time exceeded the largest value found in controls (110 hr) in 83% of patients, and was within normal limits in only 4%. Some markers remained in the large bowel one week after ingestion in the other patients. In the right colon, mean segmental transit time exceeded the largest value found in controls (38 hr) in 75% of patients, but it was normal only in 5%. The distal parts of large bowel were abnormal as well. In the left colon, mean segmental transit time exceeded the largest value found in controls (32 hr) in 66% of patients, but it was normal in only 9%. In the rectum, mean segmental transit time exceeded the
TABLE 1. NUMBER OF RADIOPAQUE MARKERS IN COLONIC SEGMENTS DURING TRANSIT IN PATIENTS WITH COLONIC INERTIA (2 • SE)
Days after ingestion o f 20 markers*
Site 1 2 3 4 5 6 7
Right colon Patients 16-+ 1 12-+ 1 8-+ 1 5-+ 1 4-+ 1 3-+ 1 2 • 1 Controls 10 • 1 3 + 1 0 0 0 0 0
Left colon Patients 3 • 6 • l a 8 • 1 8+- 1 9-+ 1 6+- 1 6-+ 1 Controls 6 • 1 3 • 1 2 -+ 0 0 0 0 0
Rectum Patients 1 -+ 0 4-+ 1NS 5 • la 4 • 1 4 • 1 4_+ 1 4_+ 1 Controls 2 • 1 4-+ 1 2-+ 1 1 • 1 0 0 0
Entire large bowel Patients 20 -+ 0 19 -+ 0 18 -- 1 17 • 1 15 • 1 13 -+ 1 12 • 1 Controls 17 • 1 9-+ 1 4-+ 1 2-+ 1 1 • 0 0 0
*All values different at P < 0.001 except a = P < 0.005 and NS = not significant.
Digestive Diseases and Sciences, Vol. 28, No. II (November 1983) 1027
W A T I E R ET A L
largest value found in controls (44 hr) in 23% of patients, but it was normal in only 6%.
Upper anal canal (72 + 4 cm H20) and lower anal canal resting pressures (50 -+ 3 cm H 20) were significantly higher in patients (P < 0.001). Control values were, respectively, 57 + 4 cm H20 for the upper and 33 -+ 4 cm H20 for the lower anal canal. There was no quantitative difference in parameters of the rectoanal inhibitory reflex. However, 76% of patients had an abnormal rectoanal inhibitory reflex (at least one value outside of the normal range). The rectoanal contractile reflex was similar in patients and controls.
Esophageal Motility Studies. Resting pressure of the upper esophageal sphincter was greater in pa- tients with colonic inertia (62.5 _+ 3.9 mm Hg) than in controls (50.3 --- 2.7 mm Hg) (P < 0.02). Coordi- nation of the sphincter with pharyngeal contraction was poorer in patients (94 --_ 2 vs 99%; P < 0.05).
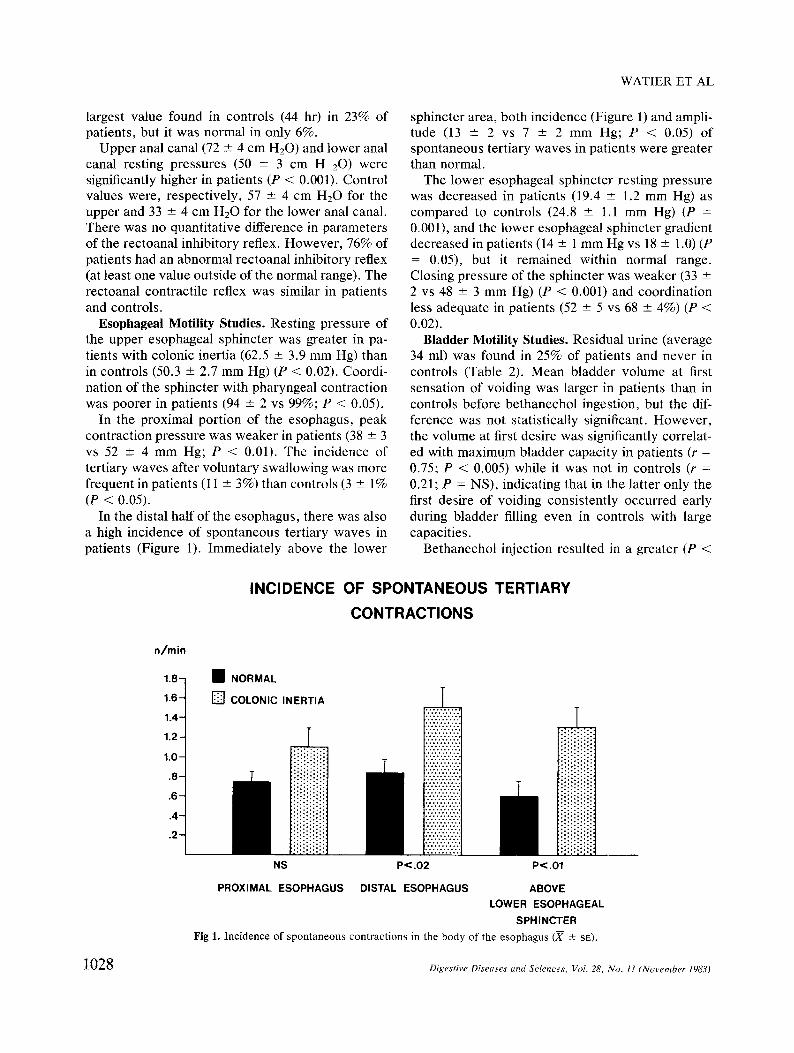
In the proximal portion of the esophagus, peak contraction pressure was weaker in patients (38 -+ 3 vs 52 --- 4 mm Hg; P < 0.01). The incidence of tertiary waves after voluntary swallowing was more frequent in patients (11 -+ 3%) than controls (3 -+ 1% (P < 0.05).
In the distal half of the esophagus, there was also a high incidence of spontaneous tertiary waves in patients (Figure 1). Immediately above the lower
sphincter area, both incidence (Figure 1) and ampli- tude (13 --- 2 vs 7 -+ 2 mm Hg; P < 0.05) of spontaneoo s tertiary waves in patients were greater than normal.
The lower esophageal sphincter resting pressure was decreased in patients (19.4 --_ 1.2 mm Hg) as compared to controls (24.8 +- 1.1 mm Hg) (P = 0.001), and the lower esophageal sphincter gradient decreased in patients (14 -+ 1 mm Hg vs 18 -+ 1.0) (P = 0.05), but it remained within normal range. Closing pressure of the sphincter was weaker (33 -+ 2 vs 48 _+ 3 mm Hg) (P < 0.001) and coordination less adequate in patients (52 -+ 5 vs 68 --- 4%) (P < 0.02).
Bladder Motility Studies. Residual urine (average 34 ml) was found in 25% of patients and never in controls (Table 2). Mean bladder volume at first sensation of voiding was larger in patients than in controls before bethanechol ingestion, but the dif- ference was not statistically significant. However, the volume at first desire was significantly correlat- ed with maximum bladder capacity in patients (r = 0.75; P < 0.005) while it was not in controls (r = 0.21; P = NS) , indicating that in the latter only the first desire of voiding consistently occurred early during bladder filling even in controls with large capacities.
Bethanechol injection resulted in a greater (P <
INCIDENCE OF SPONTANEOUS TERTIARY
CONTRACTIONS
n/min
1"8 1 1.6
1.4
1.2
1.0
�9 NORMAL [ ] COLONIC INERTIA
, . . . . . . . . . , ~~176176
, . . . . . . . . . , , . . - . , , . . . ~ , . .% , , . , . . , , , . . . , , . , . . , , , . , . . , , , , . , , . , , . . , , , , . , , , , , , . . , . , . , , , , ~
!iiii!i!i!ii , , , . , . . . , . , , . . . . . o . . . , .
, . , . , . . ~ , .
NS PROXIMAL ESOPHAGUS
. . . . . . . .
. . - . . . - ~ - ,
, . ~176 .~
P<.02 DISTAL ESOPHAGUS
.','!-'.'4 iiiiiii:i:~ ::::::::::~
iiiiiiii;i;~ ::::::::i::~
P<.01 ABOVE
LOWER ESOPHAGEAL SPHINCTER
Fig 1. Incidence of spontaneous contractions in the body of the esophagus (X • SE).
1028 Digestive Diseases and Sciences, VoL 28, No. l l (November I983)

CONSTIPATION WITH COLONIC INERTIA
TABLE 2, URODYNAMIC STUDIES IN PATIENTS WITH COLONIC INERTIA (X + SE)
Controls Patients
Bladder capacity (ml) 585 + 46 550 -+ 4 Vo!ume at first desire (ml) 185 -+ 27 231 -+ 41 Bladder pressure before bethane- 2.8 -+ 0.5 2.8 -+ 0.4
chol injection (cm HzO) Bladder pressure after be thanechol 8.5 +- 0.5 11.5 _+ 1"
injection (cm H20) Time to reach the m a x i m u m re- 19.8 -+ 1.2
sponse (min) 17.4 -+ 7t
*P < 0.025. +P < 0.01.
0.025) and quicker (P < 0.01) increase in pressure in the bladder of patients than controls. A positive supersensitive test (increase in intravesical pressure of 15 cm H20 over the control pressure before injection) (5, 6) occurred in 31% of patients but not in controls.
Clinical Management. Because the etiology of
colonic inertia is not known, the clinical manage- ment of this group of patients was not the subject of a prospective trial. The overwhelming majority were treated conservatively. However, because of the severity of symptoms, nine patients underwent total colectomy with an ileorectal anastomosis. In one patient (Figure 2), a granuloma was found in the Auerbach plexus. In another, the pathologist re- ported hyperganglionosis (Figure 2), but a diagnosis of multiple endocrine neoplasia syndrome, type 2b (10-12), could not be established. In a third (Figure 2), the pathologist described patchy disappearance of neurons with inflammation of the plexuses and increase in the number of Schwann cells from anus to cecum.
DISCUSSION
The majority of patients whose idiopathic consti- pation is associated with stagnation of feces in the
Fig 2. Auerbach p lexuses in the colon of three patients with colonic inertia. A: Presence of a granuloma, H&E, x 160. B: Presence of a large number of neurons , H&E , x 160. C: Inf lammation of bowel plexus with decrease in the number of neurons and increase in the
number of Schwann cells, H&E, x 160.
Digestive Diseases and Sciences, Vol. 28, No~ 11 (November 1983) 1029
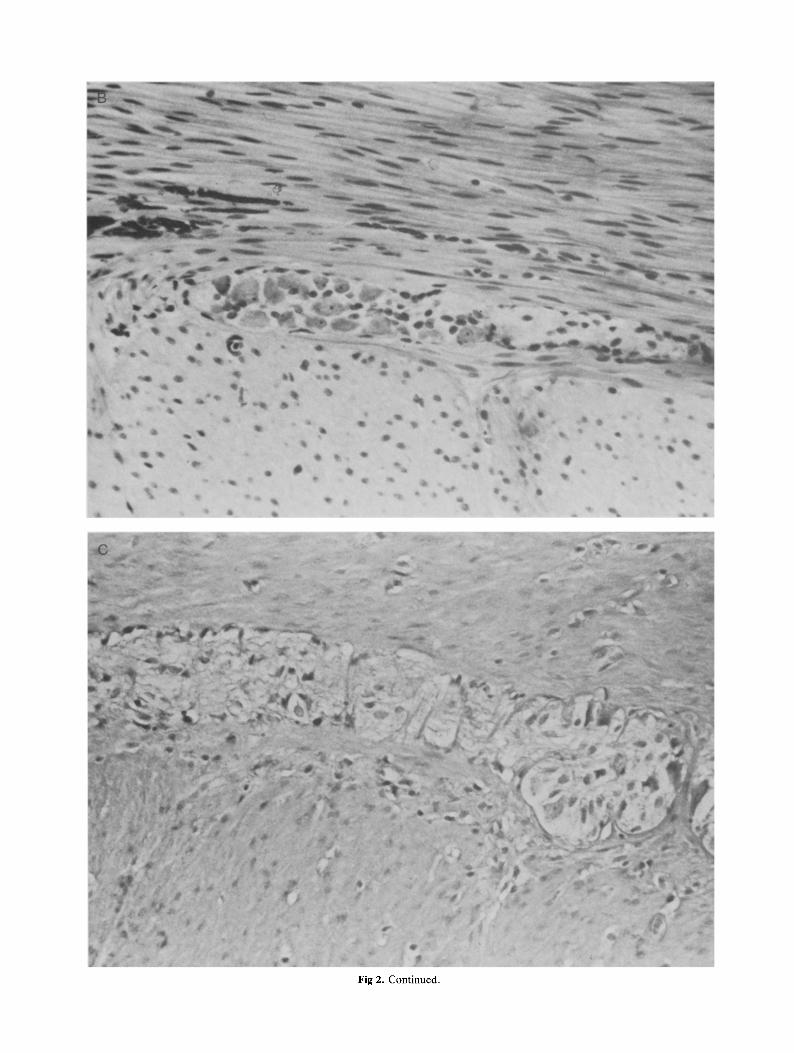
Fig 2. Continued.

CONSTIPATION WITH COLONIC INERTIA
ascending colon have functional abnormalities in the esophagus and the bladder as well: their consti- pation thus is not the symptom of a purely Colonic disease. In this study, the upper esophageal sphinc- ter was hypertonic and uncoordinated~ motility in the body of the esophagus uncoordinated, and gastroesophageal pressure barrier decreased: The bladder contracted faster and stronger in response to bethanechol injection. Segmental colonic transit time was prolonged in all sites, and the anal canal was hypertonic and Uncoordinated. Thus at least three hollOw viscera were not normal in this group of patients. The high incidence of galactorrhea and orthostatic hypotension further suggest one or more underlying systemic diseases.
The.results ofthis Study do not provide a means to go beyond these initial conclusions to establish the precise nature of the disease(s). Nonetheless, h!stologic findings in some of the few patients who underwent colectomy were revealing. The presence of a granuloma cannot be disputed but that of an excess or a paucity of neurons in the plexuses is an observation which is difficult to quantify, the more so because we do not know the range of normal Values. Nevertheless, the association of a paucity of neurons and increase in Schwann cells has been reported in some patients with chronic idiopathic intestinal pseudoobsti'ucti0n (13, 14). In primary autonomic insufficiency and in Shy-Drager syn- drome, constipation, urinary functional abnormali- ties and symptoms, and posturai hypotension may be associated (15-19), as they are in patients with colonic inertia.
The overwhelming pred0minance of women (51 to 3) in this study is striking. Our experience with constipation is almost limited to women, and we have no reason to suspect this is related to self- selection or referral pattern. The high incidence of galactorrhea suggests pituitary-hypothalamic dys- function. However, in the patients with this symp- tom, prolactin levels under fasting and TRH-stimu- fated conditions were normal, and there was no pituitary microadenoma. Finally, the psychologic aspect of colonic inertia deserves some consider- ation. In this study, no effort was made to screen patients in this regard; however, none was psychot- ic, and none was taking any mood-altering drug. Overall, there is a distifict possibility that more than one disease is responsible for the syndrome.
Many patients in this Series underwent unneces- sary laparotomy for what was thought erroneously to be large bowel obstruction. Thus, colonic inertia
may be part of a clinical spectrum including chronic idiopathic intestinal pseudoobstruction (19). Since patients in this study had no evidence of intestinal malabsorption, the small bowel function was proba- bly normal (20,24). Several reports (25-35) describe a number of esophageal motor abnormalities in patients with pseudoobstruction: achaiasia or dif- fuse spasm (29, 32); loss of propulsive force in the body Of the esophagus (26, 27, 33-35); and sponta- neous tertiary activity in the body of the esophagus (261 29, 32). The lower esophageal sphincter was described as normal (26-28, 31, 25), hypertensive (29-32), or hyp0tensive (25, 26, 33, 34). The pattern in patients with Colonic inertia was definitely not that of achalasia or diffuse spasm, and the most significant abnormality was the high incidence of spontaneous tertiary contractions, mainly in the distal esophagus and in the area immediately proxi- mal to the lower esophageal sphincter. Sphincteric function was also abnormal. Resting pressure of the Upper esophageal sphincter was greater in patients, and it was uncoordinated with pharyngeal contrac- tion. This suggests the existence of a striated mus- cle problem perhaps Conducive to dysphagia as in the globus syndrome. Conversely, a weaker gastro- esophageal sphincter creates conditions favorable to the occurrence of gastroesophageal reflux. Ab- normal function of the proximal portion of the esophagus confirms the underlying existence of striated muscle abnormal activity in patients with colonic inertia.
Colorectal and bladder functional abnormalities often coexist (36-42). In this study, residual urine was present in One quarter of patients who had no evidence of obstruction or infection. First urge to void in normal subjects was perceived early during bladder filling, irrespective of maximum bladder capacity. In contrast, patients showed a significant Correlation between capacity and volume at first desire tO void: this represents a sensory defect that necessitates larger fluid volumes to stimulate the desire to void. Such a sensory toss is a reliable symptom of detrusor paresis, and the absence of frank urological Symptoms does not exclude the presence Of even severe neurogenic dysfunction (6, 43). The bethanechol supersensitivity test (5) in the bladder is based on Cannon's law of denervation which implies that a denervated organ becomes hypersensitive to its previously present neurotrans- mitter (44). A rise in pressure of 15 cm of water above baseline in response to injection is consid- ered as the limit between normal and abnormal
Digestive Diseases and Sciences, Vol. 28, No. 11 (November 1983) i03 1

WATIER ET AL
response. This was found in 31% of patients and suggests target organ denervation.
It would be interesting to perform a study such as this in patients where feces stagnate in the more distal parts of the large bowel only. However, in these, congenital lesions such as hypoganglionosis are difficult to recognize. Furthermore, spasticity in the sigmoid accounts for the pathogenesis of the irritable bowel syndrome, and this is highly com- mon in the s0-called "normal" population (45). Half the patients included in this study had an excess of markers in the right part of the bowel, not on the basis of sluggish propulsion but reflux from the distal bowel; the latter group may have Suffered from a severe form of irritable bowel, and this should certainly be looked at in future studies. Finally, there are embryological, anatomical, histo- logical, and functional differences between right and left colon. All these features are a source of much greater heterogeneity in patients with consti- pation where feces are delayed in the distal bowel only and make an overall analysis of these more difficult at this stage of our knowledge. These limitations preclude us from identifying colonic inertia as a mechanism of constipation completely separate from anorectal outlet obstruction or hind- gut dysfunction, but, conversely, when markers do stagnate in the ascending colon, evidence is provid- ed by this study that there is little likelihood that the underlying disease is limited to the colon alone.
ACKNOWLEDGMENTS
We thank Drs. Bernard Perey and Hugh Scott for reviewing this manuscript.
REFERENCES
1. Martelli H, Devroede G, Arhan P, Duguay C, Dornic C, Faverdin C: Some parameters of large bowel motility in normal man. Gastroenterology 75:612-618, 1978
2. Martelli H, Devroede G, Arhan P, Duguay C: Mechanisms of idiopathic constipation: outlet obstruction. Gastroenterol- ogy 75:623-631, 1978
3. Arhan P, Devroede G, Jehannin B, Lanza M, Faverdin C, Dornic C, Persoz B, Tetreault L, PerCy B, Pellerin D! Segmental colonic transit time. Dis Colon Rectum 24:625- 629, 1981
4. Devroede G: Constipation: Mechanisms and management. In Gastrointestinal Disease Pathophysiology Diagnosis Man- agement, 2nd ed. MH Sleisenger, JS Fordtran (eds). Phila- delphia, WB Saunders, Company, 1978, pp 368-387
5. Lapides J, Friend CR, Ajemian EP, Reus WF: A new test for neurogenic bladder. J Urol 88:245-247, i962
6. Glahn BE: Neurogenic bladder diagnosed pharmacologically
on the basis of denervation sensitivity. Scand J Urol Nephrol 4:13-24, 1970
7. Siegel S: Nonparametric Statistics for the Behavioral Sci- ences. New York, McGraw-Hill, 1956, pp 64, 104-111
8. Siegel S: Nonparametric Statistics for the Behavioral Sci- ences. New York, McGraw-Hill; 1956, pp 96-104
9. Winer B J: Statistical Principles in Experimental Design, 2nd ed. New York, McGraw-Hill, 1971, pp 41-44.
10. Nezelof C, Guy-Grand D, Thonine E: Les mrgacrlons avec hyperplasie des plexus myentrriques. Une entit6 anatomo- clinique, ~ propos de 3 cas. Presse Med 78:1501-1506, 1970
11. Carney JA, Go VL, SizemOre GW, Hayles AB: Alimentary tract ganglioneuromatosis. A major component of the syn- drome of multiple endocrine neoplasia, type 2b. N Engl J Med 295:128%129i, 1976
12. Carney JA, Hayles AB: Alimentary tract manifestations of multiple endocrine neoplasia, type 2B. Mayo Clin Proc 52:543-548, 1977
13. Dyer NH, Dawson AM, smith BF, Todd IP: Obstruction of bowel due to lesion in the myenteric plexus. Br Med J 1:686- 689, 1969
14. Phat VN, Chousterman M, Block F, Petite JP, Camilleri JP: Lrsions des plexus myenidriques dans la pseudo-obsti'uction intestinale chronique idiopathique et certaines maladies grn- 6rales. Ann Anat Path (Paris) 23:131-142, 1978
15. Hickler RB, Thompson GR, Fox LM, Hamlin JT III: Suc- cessful treatment of orthostatic hypotension with 9-alpha- fluoro-hydrocortisone. N Engl J Med 261:788-791, 1959
16. Ziegler MG, Lake CR, Kopin IJi The sympathetic-nervous system defect in primary orthostatic hypotension. N Engl J Med 296:293-297, 1977
17. Shy GM, Drager GA: A neurological syndrome associated with orthostatic hypotension: A clinical-pathologic study. Arch Neurol 2:511-527, 1960
18. Caronna J J, Plum F: Cerebrovascular regulation in pregang- lionic and postganglionic autonomic insufficiency. Stroke 4:12-19, 1973
19. Faulk DL, Anuras S, Christensen J: Chronic intestinal pseudo=obstruction. Gastroenterology 74:922-931, 1978
20. Ogilvie H: Large-intestine colic due to sympathetic depriva- tion: A new clinical syndrome. Br Med J 2:671-673, 1948
21. Caves PK, Crockard HA: Pseudo-obstruction of the large bowel. Br Med J 2:583-586, 1970
22. Wanebo H, Mathewson C, Conolly B: Pseudo=obstruction of the colon. Surg Gyneco Obstet 133:44-48, 1971
23. Spira IA, Wolff WI: Colonic pseudo-obstruction following termination of pregnancy and uterine operation. Am J Obstet Gynecol 126:7-12, 1976
24. Bachulis BL, Smith PE: Pseudo-obstruction of the colon. Am J Surg 136:66-72, 1978
25. Maldonado JE, Gregg JA, Green PA, Brown AL: Chronic idiopathic intestinal pseudo-obstruction. Am J Med 49:203- 212, 1970
26. Moss AA, Goldberg HI, Brotman M: Idiopathic intestinal pseudo-obstruction. Am J Roentgenol 115:312-317, 1972
27: Philippon MMF, Goujon G: Pseudo-obstruction intestinale chronique idiopathique. Arch Fr Mal Appar Dig 61:145-160, 1972
28. Lukie BE, Sanders MG: Chronic idiopathic intestinal pseu- do-obstruction with maiabsorption, a scleroderma-like disor- der. Can Med Assoc J 109:1222-1227, 1973
29. Schuffier MD, Pope CE: Esophageal motor dysfunction in
1032 Digestive Diseases and Sciences, Vol. 28, No. 1! (November 1983)

CONSTIPATION WITH COLONIC INERTIA
idiopathic intestinal pseudo-obstruction. Gastroenterology 70:677-682, 1976
30. Schuffier MD, Lowe MD, Bill AH: Studies of idiopathic intestinal psuedo-obstruction. I. Hereditary hollow visceral myopathy: Clinical and pathological studies. Gastroenterol- ogy 73:327-338, 1977
31. Schuffler MD, Pope CE: Studies of idiopathic intestinal pseudo-obstruction. II. Hereditary hollow visceral myopa- thy: Family studies. Gastroenterology 73:339-344, 1977
32. Sulli,)an MA, Snape WJ, Matarazzo SA, Petrobuki RJ, Jeffries G, Cohen S: Gastrointestinal myoelectrical activity in idiopathic intestinal pseudo-obstruction. N Engl J Med 297:233-238, 1977
33. Byrne WJ, Cipel L, Euler AR, Halpin TC, Ament ME: Chronic idiopathic intestinal pseudo-obstruction syndrome in children-clinical characteristics and prognosis. Pediatr 90:585-589, 1977
34. Lipton AB, Knauer CM: Pseudo-obstruction of the bowel. Therapeutic trial of metoclopramide. Am J Dig Dis 22(3):263-265, 1977
35. Euler AR, Ament ME: Esophageal motor dysfunction in idiopathic pseudo-obstructi0n. Gastroenterology 71:712, 1977
36. Bradley WE: Autonomic neuropathy and the genitourinary system. J Urol 119:29%302, 1978
37. Ellenberg M: Diabetic neurogenic vesical dysfunction. Arch Intern Med 117:348-354, 1966
38. Goyal RK, Spiro HM: Gastrointestinal manifestations of diabetes mellitus. Med Clin North Am 55:1031-1044, 1971
39. Dorfman LE, Bailey J, Smith JP: Sub-clinical neurogenic bladder in children. J Urol 101:48-54, 1969
40. Shopfner CE: Urinary tract pathology associated with con- stipation. Radiology 90:865-877, 1968
41. Williams DI, Hirst G, Doyle D: The occult neuropathic bladder. J Pediatr Surg 9(1):35-41, 1974
42. Mix LW: Occult neuropathic bladder. Urology 10:1-9, 1977 43. Glahn BE: The neurogenic factor in vesical dysfunction
following radical hysterectomy for carcinoma of the cervix. Scand J urol Nephrol 4:107-116, 1970
44. Cannon WB, Rosenblueth A: The Supersensitivity of Dener- vated Structures; A Law of Denervation. New York, Mac- millan, 1949
45. Thompson WS, Heaton KW: Functional bowel disorders in apparently healthy people. Gastroenterology 79:283-288, 1980
Digestive Diseases and Sciences, Vol. 28, No. II (November 1983) 1033
Related Documents







![WallFlex Colonic Stent - Boston Scientific- US · WallFlex ™ Colonic Stent Visualization Expertise in combining stent materials has resulted ... (BTS). “The WallFlex™ [Colonic]](https://static.cupdf.com/doc/110x72/5ae601bc7f8b9a8b2b8ca931/wallflex-colonic-stent-boston-scientific-us-colonic-stent-visualization-expertise.jpg)



