Connecting Care Our story so far…… Finnish Health ICT Conference May 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Connecting Care
Our story so far……
Finnish Health ICT Conference
May 2016

Andy Kinnear – 4 roles
• Connecting Care Programme Director – The BNSSG Digital Transformation programme
• Director of Digital Transformation – South, Central and West CSU
• Local Delivery Advisor – NHS Digital (formerly Health and Social Care Information Centre)
• Chair of BCS Health & Care Executive – British Computer Society
Also:
• 25 years NHS experience
• Member of George Freeman MP’s Digital Cabinet
• CIO Network member
• Long suffering Crewe Alexandra fan ;-)
Andy Kinnear

Background, History & Governance

BRISTOL

description
what is BNSSG?
• Map The current
footprint for
Connecting Care
is the Bristol,
North Somerset
and South
Gloucestershire
Health and Social
Care community
Approx 1.2m
people
Approx £1.2bn
health and social
care spend

Connecting Care is the Bristol, North Somerset and South Gloucestershire [BNSSG] programme, dedicated to using technology to support -
• Better information sharing between local health and social care organisations
• Joining up information to ensure care is focused around the individual and their needs
• Improving better, safer and more joined-up care
• Supporting increased efficiency in the delivery of health and social care services
• Ensuring that the people who are providing care have the information they need, when they need it
what is Connecting Care?
Our first focus has been the delivery of a shared ‘view only’ electronic
patient record
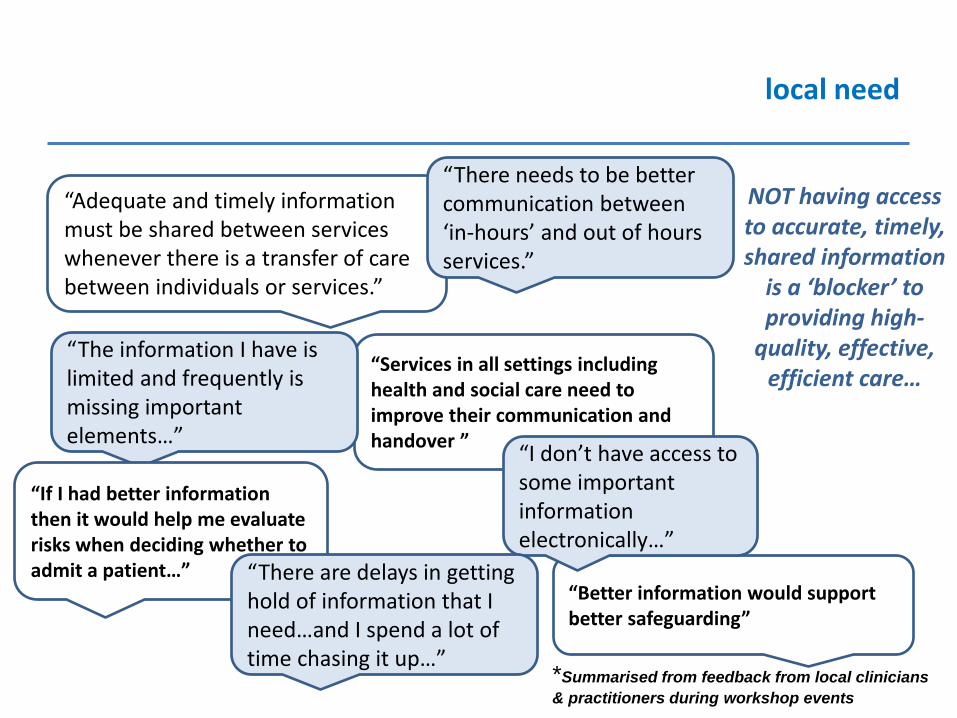
local need
“Adequate and timely information must be shared between services whenever there is a transfer of care between individuals or services.”
“Services in all settings including health and social care need to improve their communication and handover ”
“The information I have is limited and frequently is missing important elements…”
“Better information would support better safeguarding”
“I don’t have access to some important information electronically…”
“If I had better information then it would help me evaluate risks when deciding whether to admit a patient…” “There are delays in getting
hold of information that I need…and I spend a lot of time chasing it up…”
*Summarised from feedback from local clinicians
& practitioners during workshop events
NOT having access to accurate, timely, shared information
is a ‘blocker’ to providing high-
quality, effective, efficient care…
“There needs to be better communication between ‘in-hours’ and out of hours services.”

national drivers

strategic alignment
5 year forward view: “Most countries have been slow to recognise and
capitalise on the opportunities presented by the information revolution……the
NHS has oscillated between two opposite approaches to information technology
adoption.....the result has been
systems that don’t
talk to each other
and a failure to
harness the shared
benefits that come
from interoperable
systems…..In
future we intend to
take a different
approach”

project approach
• 2011 Original Vision
• 2012 Procurement
• 2013 Staged approach
– First stage (pilot) started in March 2013. Key deliverables:
• A working system for 500 users
• Evaluation of benefits
• Stage one themed on urgent & unplanned care
• 2014 A business case for the second stage started
Dec 2014 (next 5-7 years)
FYFV PUBLISHED
• 2015 & beyond = GROWTH
Stage two will extend the breadth & depth (10,000 more users, more information sharing, more organisations, more functionality, more more more more….)

the partnership

• Demographics • Laboratory • Radiology • Encounters • Allergies • Diagnosis
Clinical Data Repository Rhapsody Integration Engine
Pathology &
radiology - tbc
EMIS
GPs and
Community
Health
organisations Mental
health (RiO)
• Authentication • Patient Privacy & Consent • Relationships • Audit Logs
• Patient Search • Patient Lists • Patient Summary • Timeline
Presentation
Integration
Source Systems
Security & Privacy Patient Record
• Medications • Problems • Procedures
Portal
Connecting Care Clinical Portal
Master Patient Index
MiG
PAS Systems
(Weston
Cerner, NBT
Lorenzo,
UHB
Medway)
Adult Social
Care (Swift
N Som & S
Glos, Liquid
Logic -
Bristol)
End Of Life
(Adastra)
Children’s
Social Care
(Liquid
Logic N
Som &
Bristol, Capita – S
Glos)
Out Of
Hours
(Adastra)

some facts & figures
Over 1 million records shared
17 health & social care organisations in partnership
13 + different IT systems linked from both health & social care (and growing!)
Over 800k informing letters sent to all local residents as part of a wider IG
First stage project delivered in 9 months – live since December 2013
Currently have 1600 users….plan to expand to 4,000 this year – and up to 10,000 +

Benefits

benefits
Out of hours care
• Saves appointments and visits • Saves admissions • Safer prescribing • Improved quality of consultation
Pharmacy
• Safer prescribing – provides access to allergy and GP prescribing information
• Saves time – reduces the amount of time calling GP practices • Safer communication - reduces errors
Hospitals/ A&E
• Safer care – patient background, context and medications • Saves times – reduces time trying to find out information • Reduces risks – where patients unable to inform clinicians about
relevant information/fax errors etc.

benefits…
Community Care
• Saves time in triage and assessment • Saves time – reduces the amount of calls to GPs • Saves unnecessary home visits • Supporting risk management and safeguarding
Social Care
• Supporting referral management • Saves time in triage and assessment • Informs assessments & care planning • Saves installation and equipment costs • Supports risk management and safeguarding
General Practice
• Reduces burden on practice administrators • Supports risk management and safeguarding • Increased confidence in better care being provided outside of the
practice • Immediate access to GP records (new registrations)

User Evaluation of Stage One showed:
• 50% saved time calling other organisations
• 71% saved a call to a GP
• 50% saved time and saw improvements in triage and analysis
• The number of faxes requested/received dropped sharply - 86% less in NBT pharmacy and 75% less in UHB pharmacy
• 12% stated without Connecting Care they would have made an (unnecessary / inappropriate) referral to another service
• 17% stated that avoiding duplication was one of the main benefits of Connecting Care for them and their team
• 25% said that Connecting Care had helped to improve care planning
enhancing safer and better care

benefits…
“Massive difference in
time spent accessing information. On average [I can] access the GP record within 30 seconds compared with 15-20 minutes taken via telephone or via fax” Critical Care Pharmacist Manager UHB “3 cases identified
on Connecting Care today that were already allocated to a health practitioner (BCH OT or IMCS OT) so did not require referrals to BCC OT”. Occupational Therapist Bristol City Council
“I now use Connecting Care on almost every case I deal with it (approx. 25 cases per shift). It always makes a difference and adds value. Every shift, acute admissions are avoided.” Doctor (out of hours)
“Have been able to identify trends which have then resulted in swifter [safeguarding] interventions…one case where concerns would not have increased without Connecting Care…” Social Worker Safeguarding team
“Connecting Care is brilliant…I use it to triangulate information from service users, to find out about other services involved so that I can contact them to inform my assessments” Bristol social worker
“it has enabled us to commence discharge planning earlier in the patients stay to help prevent delays later on.” Discharge Nurse
“Unable to obtain a medication history or allergy status from the patient….accurately confirmed through Connecting Care …” Pharmacist, NBT
““Information about the patient’s diagnoses has helped our team decide which type of therapy to offer the patient” UHB

benefits…
“On Monday I managed to obtain details for 22 patients on Connecting Care, I saved a huge amount of time as I didn’t need to phone the GPs and wait for the faxes to arrive” Acute
Pharmacist
“I used Connecting Care to find vital information for the diabetes nurses . The information logged by district nurses is a goldmine of information. We saved 20 minutes on the telephone and managed to find the reason for patients insulin being discontinued” Discharge Nurse
“In cases where we are dealing with a person who is being supported by Rapid Response and the district nurses, Connecting Care comes in to its own. All the notes from visits are documented and it can save at least 30-40 minutes on duty cases of this nature” Social Worker “The extra patient detail
is useful when deciding to stop drugs such as anti-platelets and it helps to identify risk factors” Doctor
Having access to accurate, timely,
shared information is no longer a
‘blocker’ to providing high-
quality, effective, efficient care…
“Without Connecting Care today I couldn’t have done my job.” Pharmacist
“Connecting Care has been really helpful tonight. Could not do without it. Particularly in the case of an old lady with XX who I could not reach on the phone. Without Connecting Care this would have resulted in a visit and probably her door being broken down. But with CC I was able to work out that all that should of been done, had been done.” OOH Doctor

potential financial benefits
Prevented
Admissions 10,000 users could see annual saving of £1,036,288 from inappropriate admissions prevented, by using information in Connecting Care
Based on a Department of Health reference cost 2012/13 of £1,436 for a unplanned admission and only the same rate of stated admissions prevented in the pilot
Reducing
duplicate
assessment
Reducing duplicate assessments
10,000 users could see a annual saving of £179,520 on stopping the duplication of assessments as a result of using information in Connecting Care
Based on cost savings if the same rate of stated admissions prevented during the pilot continues – based on £60 for an average cost of a face to face assessment by a community nurse - Department of Health reference cost 2012/13

potential financial benefits
Time saving 10,000 users could see an annual saving of £155,278 of ‘people time’ as Connecting Care users spend much less time calling other organisations for information Based on salary cost savings if only one call per week per user is saved where the medium salary between NHS bands 7 to 8 is used.
Reducing
wasted home
visits
10,000 users could see a annual saving of £68,000 on stopping unnecessary home visits as a result of using information in Connecting Care Based on cost savings if the same rate of stated home visits prevented during the pilot continues – based on £60 for an average cost of a face to face assessment by a community nurse - Department of Health reference cost 2012/13

Our Vision

vision
Our vision:
• Original vision – achieved (2014)
• Revisited in Spring 2015
• Co-produced the vision for 2020.
• 67 interviews:
– Leading clinicians
– Public representatives
– Care professionals
– Executives
– Key managers
– CIOs and Informatics professionals
• Signed off in August 2015

vision
We are a diverse group of organisations united by a common purpose and a common vision. Our common purpose is to serve the million people in Bristol, North Somerset and South Gloucestershire by meeting their need for health care and social care.
Our common vision is that, by sharing information securely and effectively, we will make a lasting contribution to the health, well-being and opportunity of our population.
3 Acute Trusts
3 Acute Trusts
3 Community Providers
3 Local Authorites
2 Mental Health Trusts
Out of Hours Provider
100 + GP Practices
Ambulance Service
3 Clinical Commissioning Groups
AHSN, NHS England, Central and South West CSU

vision - platform
Connecting Care Technology Platform
Citizen / Patient
Driven Apps
Connecting Care
Analytics Hub
Online guidance –
NICE, NHS
Choices &
Council Websites
Health &
Social Care
Apps
Connecting
Care Portal
Telecare/Health
Devices/
Wearables
My ‘Circle of
Care’
Personal Health Record
Research
Health & Social Care Organisational Systems e.g.
- EMIS (GPs & Community Health)
- Lorenzo /Medway/ Cerner/ CliniSys etc.
- RIO
- Liquid Logic / Swift
- Adastra
Etc.
Data Sources
For citizens
Secondary usesFor Health &
social care
professionals
Wider
connectivity
With thanks to Leeds City Council

‘Herding Cats’

behaviours
The ‘herding cats’ challenge –
Connecting Care and shared record programmes are characterised by:
• Multiple organisations with Multiple agenda
• Multiple clinical or care professions with Multiple priorities
• Multiple system suppliers with Multiple commercial interests
But
ONE public, ONE citizen, ONE patient
behaviours
The ‘herding cats’ challenge –
Recognise and work on the different elements –
• Political dimension
• Personal dimension
• Human behaviours
• Organisational behaviours
• Interests, motivations and blockers
• Time and timing

5 reasons we have been successful so far…..
1. Line of business systems that ‘share’
• You cannot share paper data easily • Good electronic ‘line of business’ systems that share
data are critical
2. Integration Partner • Integration is tricky. Find a software partner who ‘gets it’
3. Money…locally owned money!
• Invest locally….seek national money too, but make your local organisations put skin in the game
4. People….local talented people
• Hire really talented project people….we did, we do, we always will
5. SPIRIT • Overrides everything else • Stamp on ‘organisationally centric’ thinking at every
single opportunity. • Command the morale high ground that the
patients/citizens best interest occupies

Reasons to be cheerful…….or
“Why England is finally getting its e-Health
strategy right”

The Digital Transformation ‘engines’ THEORY….
NHS England - Vision & Strategy
- Money
- Leadership
‘
‘Locals’
- Design
- Delivery
- Timetable
HSCIC - Standards
- National systems
- Delivery
Suppliers - Products
- Innovation
- Repeatability
Our Patients
Our Public

The Digital Transformation ‘engines’ THEORY….
NHS England - Vision & Strategy
- Money
- Leadership
‘
‘Locals’
- Design
- Delivery
- Timetable
HSCIC - Standards
- National systems
- Delivery
Suppliers - Products
- Innovation
- Repeatability
Our Patients
Our Public
Requires people to lead, act, think and
behave DIFFERENTLY

The Digital Transformation ‘engines’ PRACTICE….
NHS England - FYFV, Personalised Healthcare 2020
- NIB investment, CSR settlement (£1bn)
- NIB, Digital Cabinet
‘
‘Locals’
- Connecting Care –like Programme, investment & governance
- Digital Roadmap development & delivery
HSCIC - Open API layer, Code4Health
- SCR, E-RS, SUS, Spine etc
- Partnership with local delivery
Suppliers - Orion Health
- Strategic Partnership as leading EMEA reference site
- Opportunity to exploit international learning
Our Patients
Our Public

NHS England….

£4.2bn will be spent on NHS technology over the next 5 years
£1.8bn to create a paper-free NHS and interoperability for
clinicians
£1bn on infrastructure, cyber security and data consent.
£750m on transforming out of hospital care, including digital primary
care, medicines, social care digitalisation and digital urgent & emergency care
£400m to enable the NHS to become digital, including a new nhs.uk
website, apps, free Wi-Fi and telehealth
£250m for data for outcomes and research

HSCIC….


Locals - 2014
Oxfordshire Shared Record
Hampshire Shared Record
Connecting Care

Locals - 2016
Oxfordshire Shared Record
Hampshire Shared Record
Connecting Care
SIDER
Dorset Care
Record
JUYI
Single view of
the citizen
Berkshire West – Connected Care
Berkshire East – Share my care

Suppliers
5 principles of the Interoperability Charter:
• We will make available to other suppliers, the NHS and Local Authorities, the
technical specifications of our interfaces without charge
• Where there is customer demand we agree to co-operate without charge with
other suppliers in developing interfaces
• We will not reinvent the wheel and will use internationally recognised standards
where relevant
• We will only charge reasonable and proportionate fees to the end user
organisation for Licencing, Implementation and Support services required for the
interfaces.
• Where new interfaces and enhancement to existing enhancements to existing
interfaces are required, we will not charge twice for the same software
development

Creating a common and open set of APIs to support information sharing across health and care
Defining the key clinical
information
sharing needs.
Prioritising the key APIs.
Group members e.g. CCIOs,
CIOs, Vanguard, Pioneers,
PMCFs,
NHS England.
Outlining the accreditation
approach for APIs.
Group members e.g.
TechUK, CIOs, suppliers,
HSCIC.
Defining the key underpinning
components and policies, e.g.
security and authentication.
Group members e.g. HSCIC,
suppliers, CIOs, TechUK, NHS
England.
Establishing and creating the
required APIs based on clinical
information sharing needs.
Group members e.g. suppliers,
innovators, CCIOs, CIOs, NHS
England, HSCIC.
Made up of the above organisations, the
Project Board
is responsible for the assurance and
governance process.
Links to existing
communities and
signposts tools
and products.

On top of that…..


Other evidence
Starting now and lasting until forever, your health and
healthcare will be determined, to a remarkable and
somewhat disquieting degree, by how well the technology
works.
Bob Wachter, The Digital Doctor.
Clinically led improvement, enabled by new technology, is
transforming the delivery of health care and our
management of population health. Yet strategic decisions
about clinical transformation and the associated investment
in information and digital technology can all too often be a
footnote to NHS board discussions. This needs to change.
Nuffield Trust

Domain Descriptions
A. Self-Care and Prevention: We will deliver the online services that patients need to take control of their own care, which will reduce the pressure on front line services.
B. Urgent and Emergency Care: We will help to deliver the national urgent and emergency care strategy by providing the digital infrastructure, algorithms and pathways we require.
C. Transforming General Practice: We will use technology to free GPs from time consuming administrative tasks and provide patients with online services.
D. Integrated Care: We will better inform clinical decision making across all health and care settings by enabling and enhancing the flow of patient information.
E. Digital Medicines: We will enable and improve pharmacy decision making and outcomes by providing patients and prescribers with streamlined digital services.
F. Elective Care: We will improve referral management and provide an improved treatment choice for patients by automating referrals across the NHS.
45
G. Paper free at the point of care: We will create an NHS “paper free at the point of care” by driving up levels of digital maturity and by enabling the NHS workforce to better utilise the benefits of digital technology.
H. Data Outcomes for Research and Oversight: We will deliver the health and care information and insight which is fundamental to informed policy making, commissioning and regulation by improving information collections, analysis and reporting.
I. Infrastructure: We will enable information to move safely and securely across all health and care settings by providing robust and future-proofed national systems and networks.
J. Public Trust and Security: We will provide the means for citizens to set their consent preferences. We will provide confidence that clinical and citizen information is held safely and securely and protect health and care systems from external threats.

Linking Programmes to Outcomes
Citizen Identity NHS.UK Health Apps Assessment & Uptake (inc wearables) Widening Digital Participation
Digital Referrals
5
Integrated Care – Business Change Integrated Care – Interoperability and Architecture Social Care Integration Personal Health Record
Digitising Community Pharmacy Pharmacy Supply Chain and Secondary Uses Integrating Pharmacy Across Care Settings 19
18
17
20
Driving Digital Maturity Digital Child Health Digital Diagnostics Workforce and Professional Capabilities
21
General Practice Operational Systems and Services Adopting Existing Technologies in General Practice Technology for General Practice Transformation GP Data for Secondary Uses
10
9
6
12
4
29
3
2
1
Clinical Triage Platform Patient Relationship Management Access to Service Information Out of Hospital Care
National Data Services Development Data Content (inc. GP data, PLICS and PCOMS) Innovative uses of Data
25
26
Self Care and Prevention
Integrated Care
Elective Care
Infrastructure
Digital Medicines
Paper Free at Point of Care
Data Outcomes for Research and Oversight
Urgent and Emergency Care
Transforming General Practice C
B
H
G
A
I
D
E
F
Cyber-Security National Opt-Out Model
Public Trust and Security
Digital Interoperability Platform and Spine NHSmail2 HSCN WiFi
11
13
14
15
16
22
23
24
27
30
31
32
33
7
8
28
J
46

The Digital Transformation ‘engines’ emerging reality….
SOME people ARE leading, acting, thinking and
behaving DIFFERENTLY…..
…..Its time for the rest to do the same

Questions
Andy Kinnear - Programme Director
T: 0117 900 2552 M: 07967 005871
Andy_Kinnear
Related Documents











