ConnectiCare 2017 Small Group plans

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ConnectiCare 2017 Small Group plans

311-800-723-2986
Welcome to ConnectiCare
This guide includes information about ConnectiCare’s 2017 Small Group plans. We’re pleased to offer you a wide range of plan options. A wider choice of plans helps you control costs and meet the needs of your employees.
With ConnectiCare, you can count on the personalized service and easy access to care that sets us apart from other health plans, and that have helped make us:
• The #1 health plan for Connecticut small businesses1
• The most recommended health plan in Connecticut2
• In the top tier of America’s health plans3
This year, ConnectiCare celebrates 35 years of helping make Connecticut a healthier place to live and work. We understand the needs of Connecticut businesses and individuals because we live and work in the same communities that we serve. This allows us to bring our members new, easier ways to get care and service, including:
• New way to get care at CliniSanitas Medical Centers, only for ConnectiCare members
• New Passage plans that give your employees everyday care for just $5 a visit (see pages 6-9 for details)
• New ConnectiCare center in Manchester
Take a look at all we have to offer in this guide, then give ConnectiCare or your broker a call. We’re here to help you find the ConnectiCare plan that’s right for you and your employees.
Thank you again for considering ConnectiCare.
Sincerely,
Terri GuidoneVice President, Sales & Account Management ConnectiCare, Inc. & Affiliates
331-800-723-29861-800-723-29862
Benefits your employees needAll ConnectiCare plans include the benefits your employees need to stay healthy, including:
Free preventive care4 for covered services like their annual checkup, screenings and more
Telemedicine through MDLIVE®5 – virtual doctor visits from home, office or on the go
Emergency and urgent care anywhere in the world
Prescription drug benefits
Vision benefits
Extras that don’t cost extraYour employees will get more than just health insurance, they’ll have access to discounts and savings that can make a big difference!
Vision Discount Program Your employees can save hundreds of dollars each year with discounts of up to 30% on frames, lenses and prescription contacts purchased from a participating optician.
Healthy Alternatives ProgramThis program gives your employees discounts up to 30% on health and wellness products and services, from acupuncture to exercise classes and more.
College Tuition Rewards®6
Your employees can save thousands on college tuition, earning up to one full year’s tuition at more than 340 private colleges and universities. Find out more at tuitionrewards.com/cci.
RX
ConnectiCare center in Manchester
Opening in October, 2016, our new center is a place where your employees can get help with making informed decisions about their coverage and care. And, starting in 2017, we’ll offer more ways to help them stay well with preventive care like flu shots and health assessments, plus healthy lifestyle events and seminars led by experts.
New, easier ways to get care and service
Primary care: family medicine, internal medicine, pediatrics and gynecology
Urgent care/walk-in including observation units
Specialists: cardiology, dermatology, orthopedics and more
Onsite laboratory and diagnostics
Care programs: diabetes, COPD, asthma, weight management and more
CliniSanitas Medical Centers, only for ConnectiCare membersThese medical centers offer ConnectiCare members one convenient place to get primary care, see specialists, get lab work, urgent care, and customer service for their ConnectiCare plan. With Spanish and English speaking staff, easy-to-schedule appointments and convenient hours, CliniSanitas really makes it easier to get care. Three centers will open in the fall of 2016 in Newington, Orange and Bridgeport.

351-800-723-29861-800-723-29864
Plan options ConnectiCare offers small businesses three basic plan types:
Plan Type Description Network
Passage HMO plans
NEW plans that can give members a better value and a simple pathway to the services they need. With a Passage plan, a member selects a primary care doctor from the Passage network and lets him/her guide their care – including getting a referral to see a specialist.
Separate Passage network including more than 1,000 primary care doctors, thousands of specialists and EVERY hospital in CT.
Choice HMO & POS plans
Plans that let members manage their care their way, with access to our broad network and the freedom to see a specialist without a referral.
Extensive regional network that includes all of CT and bordering sections of MA, NY and RI.
FlexPOS plans Plans that give members the most flexibility, with coverage for both in-network and out-of-network medical services.
Extensive regional network PLUS the PHCS Healthy Directions National Network. With PHCS, members have access to in-network care no matter where they are in the United States.
Metal LevelsOur Small Group plans are categorized by “metal level” or tier. The metal level is based on how much of the total health care costs the plan pays versus what members pay out-of-pocket. Listed below are descriptions for premium ranges and out-of-pocket costs for each metal level.
Metal Level Premiums Your Out-of-Pocket Costs Plan Pays*
Bronze plans Lowest Highest 60%
Silver plans Moderate Moderate 70%
Gold plans Higher Lower 80%
Platinum plans Highest Lowest 90%
*Average amount plan pays for covered services
ExampleThe Smith Family has an HSA-compatible planIn-Network Deductible: $5,000 Individual/$10,000 FamilyIn-Network Maximum Out-of-Pocket: $6,550 Individual/$13,100 Family In 2017, the Smith Family had total in-network medical expenses of $5,750: Mrs. Smith $5,000, Mr. Smith $500, Daughter Jamie $250
Plans with Health Savings Accounts (HSAs) ConnectiCare offers several HSA-compatible plans to choose from. An HSA is a savings account that members can fund with pre-tax dollars and use to pay for qualified health care expenses, including prescriptions. These plans are identified with HSA and (E) or (A) in their name on the plan charts in the following pages.
• (E) means that the plan has an “embedded” deductible. When any one family member has expenses equal to the single level deductible, the plan begins to pay for that one family member.
• (A) means that the plan has an “aggregate” deductible for all family members together. The plan does not begin to pay until the full family deductible is met.
With both types of plans, the maximum out-of-pocket for any one family member cannot exceed $7,150.
Mrs. Smith
Embedded Aggregate
Claims paid to date
Remaining until maximum out-of-pocket is reached Maximum
out-of-pocket expense
Claims paid to date
Remaining until maximum out-of-pocket is reached Maximum
out-of-pocket expense Deductible Copay or
Coinsurance Deductible Copay or Coinsurance
$5,000 q3 Individual
deductible met
$0 + $1,550 $6,550 $5,000 Family
deductiblenot met*
$2,150 + $0 $7,150On any single
member’s claim
*Individual deductible does not apply. Mrs. Smith’s maximum out-of-pocket spend is $600 higher with an aggregate plan. ($7,150 - $6,550 = $600)
The Smith Family
Embedded Aggregate
Claims paid to date
Remaining until maximum out-of-pocket is reached Maximum
out-of-pocket expense
Claims paid to date
Remaining until maximum out-of-pocket is reached Maximum
out-of-pocket expense Deductible Copay or
Coinsurance Deductible Copay or Coinsurance
$5,750 Family
deductiblenot met
$4,250 + $3,100 $13,100 $5,750 Family
deductiblenot met
$4,250 + $3,100 $13,100
The Smith Family’s maximum out-of-pocket spend is the same for embedded and aggregate plans.

371-800-723-29861-800-723-29866 6connecticare.com
After you review our plans, let us know if you have any questions. We’re here to help.
Call 1-800-723-2986Monday – Friday, 8 a.m. to 5 p.m.Or, call your broker
New Passage plans Improving access to quality care with ConnectiCare’s new Passage plans
Boost your employee satisfaction by offering one of our new Passage plans that provide unlimited primary care office visits for just $5 each. Passage plans remove the financial barriers to the everyday care members need and offer great benefits, including:
Specialist visits for $40 each
NO deductibles for primary care physician (PCP) and specialist visits
Care that’s right for your employees
With a Passage plan, your employees must select a PCP from over 1,000 in the Passage network during the enrollment process. ConnectiCare has contracted with three high-quality provider groups: ProHealth Physicians, Connecticut State Medical Society (CSMS IPA) and a newcomer to Connecticut, CliniSanitas Medical Centers.
Passage PCPs will help guide care, including referring members to a wide choice of specialists and hospitals in the Passage network who have been chosen for their ability to deliver high-quality care. A referral is required to see a specialist. Your employees’ PCPs know their health history and plan, so they can recommend the best care with no cost surprises.
Finding a Passage PCP is easy
Passage PCPs are available across Connecticut. Your employees may be no more than a 10-minute drive from these doctors.

391-800-723-29861-800-723-29868 *Integrated medical and prescription drug deductible.
Passage HMO plansPlan Name/Metal Level
Contract-year Contract-year Contract-year Contract-year
Passage HMO Copay $5 Platinum
Passage HMO PCP Copay $2,500/$5,000 ded.
Gold
Passage HMO PCP Copay $1,500/$3,000 ded.
Gold
Passage HMO PCP Copay $6,800/$13,600 ded.
SilverPLAN/MEDICAL DEDUCTIBLE
Deductible (Individual/Family) None $2,500/$5,000 $1,500/$3,000 $6,800/$13,600*
Maximum Out-of-Pocket Limit (Individual/Family) $3,000/$6,000 $5,000/$10,000 $4,500/$9,000 $7,150/$14,300
IN-NETWORK MEDICAL BENEFITS
Preventive Care/Screenings/Immunizations $0 $0 $0 $0
Primary Care Services $5 copay $5 copay (deductible waived)
$5 copay (deductible waived)
$5 copay (deductible waived)
Specialist Services (A referral from your PCP is required to see a specialist) $40 copay $40 copay
(deductible waived)$40 copay
(deductible waived)$40 copay
(deductible waived)
Vision $40 copay $40 copay(deductible waived)
$40 copay (deductible waived)
$40 copay (deductible waived)
Walk-In/Urgent Care Center $75 copay $75 copay (deductible waived)
$75 copay (deductible waived) $0 after deductible
Worldwide Emergency Coverage $200 copay $200 copay after deductible $200 copay after deductible $0 after deductible
Inpatient Hospital Coverage $500 copay/day$1,500 maximum per admission $0 after deductible $0 after deductible $0 after deductible
Hospital Outpatient Facilities $500 copay $0 after deductible $0 after deductible $0 after deductible
Outpatient Surgery Free Standing Locations $250 copay $0 after deductible $0 after deductible $0 after deductible
Lab Services $5 copay $5 copay (deductible waived)
$5 copay (deductible waived) $0 after deductible
X-Rays $5 copay $20 copay (deductible waived)
$40 copay (deductible waived) $0 after deductible
Advanced Imaging (CT Scans & MRI) $75 copay up to $375
$75 copayup to $375
(deductible waived)
$75 copayup to $375
after deductible$0 after deductible
OUT-OF-NETWORK MEDICAL BENEFITS
Deductible (Individual/Family) N/A N/A N/A N/A
Coinsurance N/A N/A N/A N/A
Maximum Out-of-Pocket Limit (Individual/Family) N/A N/A N/A N/A
PRESCRIPTION DRUG BENEFIT
Prescription Drug Deductible (Individual/Family) None None None Plan has integrated deductible with medical (see above)*
Tier 1 – Preferred Generic Drugs $5 copay $5 copay $5 copay $5 copay (deductible waived)
Tier 2 – Non-Preferred Generic Drugs 50% coinsurance$200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
after deductible
Tier 3 – Preferred Brand Drugs $50 copay $40 copay $50 copay $40 copay (deductible waived)
Tier 4 – Non-Preferred Brand Drugs 50% coinsurance$200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
after deductible
Tier 5 – Preferred Specialty Drugs 50% coinsurance$500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
after deductible
Tier 6 – Non-Preferred Specialty Drugs 50% coinsurance$750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
after deductible
3111-800-723-29861-800-723-298610
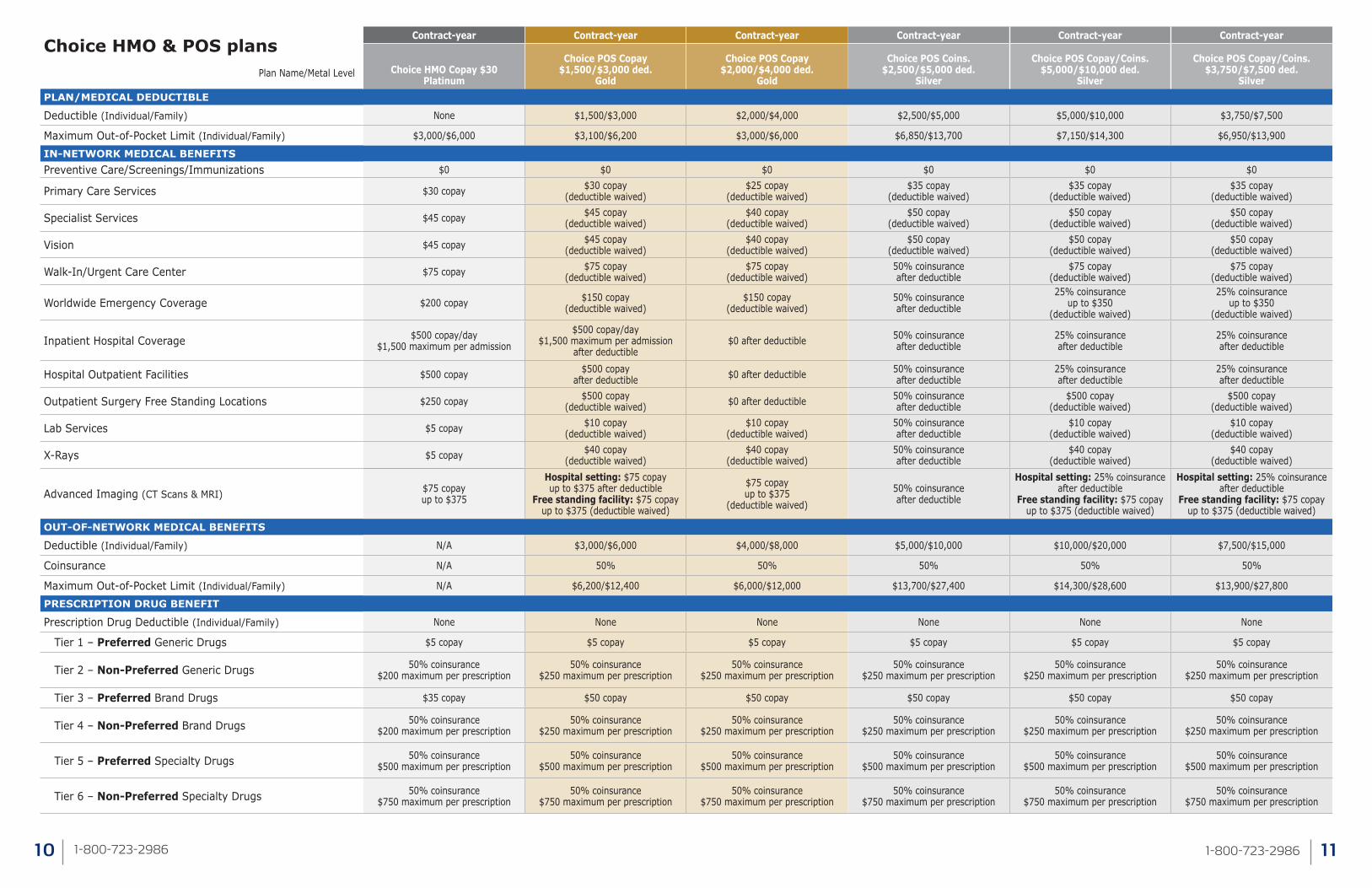
Choice HMO & POS plansPlan Name/Metal Level
Contract-year Contract-year Contract-year Contract-year Contract-year Contract-year
Choice HMO Copay $30Platinum
Choice POS Copay $1,500/$3,000 ded.
Gold
Choice POS Copay $2,000/$4,000 ded.
Gold
Choice POS Coins. $2,500/$5,000 ded.
Silver
Choice POS Copay/Coins. $5,000/$10,000 ded.
Silver
Choice POS Copay/Coins. $3,750/$7,500 ded.
SilverPLAN/MEDICAL DEDUCTIBLE
Deductible (Individual/Family) None $1,500/$3,000 $2,000/$4,000 $2,500/$5,000 $5,000/$10,000 $3,750/$7,500
Maximum Out-of-Pocket Limit (Individual/Family) $3,000/$6,000 $3,100/$6,200 $3,000/$6,000 $6,850/$13,700 $7,150/$14,300 $6,950/$13,900
IN-NETWORK MEDICAL BENEFITSPreventive Care/Screenings/Immunizations $0 $0 $0 $0 $0 $0
Primary Care Services $30 copay $30 copay (deductible waived)
$25 copay (deductible waived)
$35 copay (deductible waived)
$35 copay (deductible waived)
$35 copay (deductible waived)
Specialist Services $45 copay $45 copay (deductible waived)
$40 copay (deductible waived)
$50 copay (deductible waived)
$50 copay (deductible waived)
$50 copay (deductible waived)
Vision $45 copay $45 copay (deductible waived)
$40 copay (deductible waived)
$50 copay (deductible waived)
$50 copay (deductible waived)
$50 copay (deductible waived)
Walk-In/Urgent Care Center $75 copay $75 copay (deductible waived)
$75 copay (deductible waived)
50% coinsurance after deductible
$75 copay (deductible waived)
$75 copay (deductible waived)
Worldwide Emergency Coverage $200 copay $150 copay (deductible waived)
$150 copay (deductible waived)
50% coinsurance after deductible
25% coinsurance up to $350
(deductible waived)
25% coinsurance up to $350
(deductible waived)
Inpatient Hospital Coverage $500 copay/day$1,500 maximum per admission
$500 copay/day $1,500 maximum per admission
after deductible$0 after deductible 50% coinsurance
after deductible25% coinsurance after deductible
25% coinsurance after deductible
Hospital Outpatient Facilities $500 copay $500 copay after deductible $0 after deductible 50% coinsurance
after deductible25% coinsurance after deductible
25% coinsurance after deductible
Outpatient Surgery Free Standing Locations $250 copay $500 copay (deductible waived) $0 after deductible 50% coinsurance
after deductible$500 copay
(deductible waived)$500 copay
(deductible waived)
Lab Services $5 copay $10 copay (deductible waived)
$10 copay (deductible waived)
50% coinsurance after deductible
$10 copay (deductible waived)
$10 copay (deductible waived)
X-Rays $5 copay $40 copay (deductible waived)
$40 copay (deductible waived)
50% coinsurance after deductible
$40 copay (deductible waived)
$40 copay (deductible waived)
Advanced Imaging (CT Scans & MRI) $75 copay up to $375
Hospital setting: $75 copay up to $375 after deductible
Free standing facility: $75 copay up to $375 (deductible waived)
$75 copay up to $375
(deductible waived)
50% coinsurance after deductible
Hospital setting: 25% coinsurance after deductible
Free standing facility: $75 copay up to $375 (deductible waived)
Hospital setting: 25% coinsurance after deductible
Free standing facility: $75 copay up to $375 (deductible waived)
OUT-OF-NETWORK MEDICAL BENEFITS
Deductible (Individual/Family) N/A $3,000/$6,000 $4,000/$8,000 $5,000/$10,000 $10,000/$20,000 $7,500/$15,000
Coinsurance N/A 50% 50% 50% 50% 50%
Maximum Out-of-Pocket Limit (Individual/Family) N/A $6,200/$12,400 $6,000/$12,000 $13,700/$27,400 $14,300/$28,600 $13,900/$27,800
PRESCRIPTION DRUG BENEFIT
Prescription Drug Deductible (Individual/Family) None None None None None None
Tier 1 – Preferred Generic Drugs $5 copay $5 copay $5 copay $5 copay $5 copay $5 copay
Tier 2 – Non-Preferred Generic Drugs 50% coinsurance $200 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
Tier 3 – Preferred Brand Drugs $35 copay $50 copay $50 copay $50 copay $50 copay $50 copay
Tier 4 – Non-Preferred Brand Drugs 50% coinsurance $200 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
Tier 5 – Preferred Specialty Drugs 50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
Tier 6 – Non-Preferred Specialty Drugs 50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
3131-800-723-29861-800-723-298612
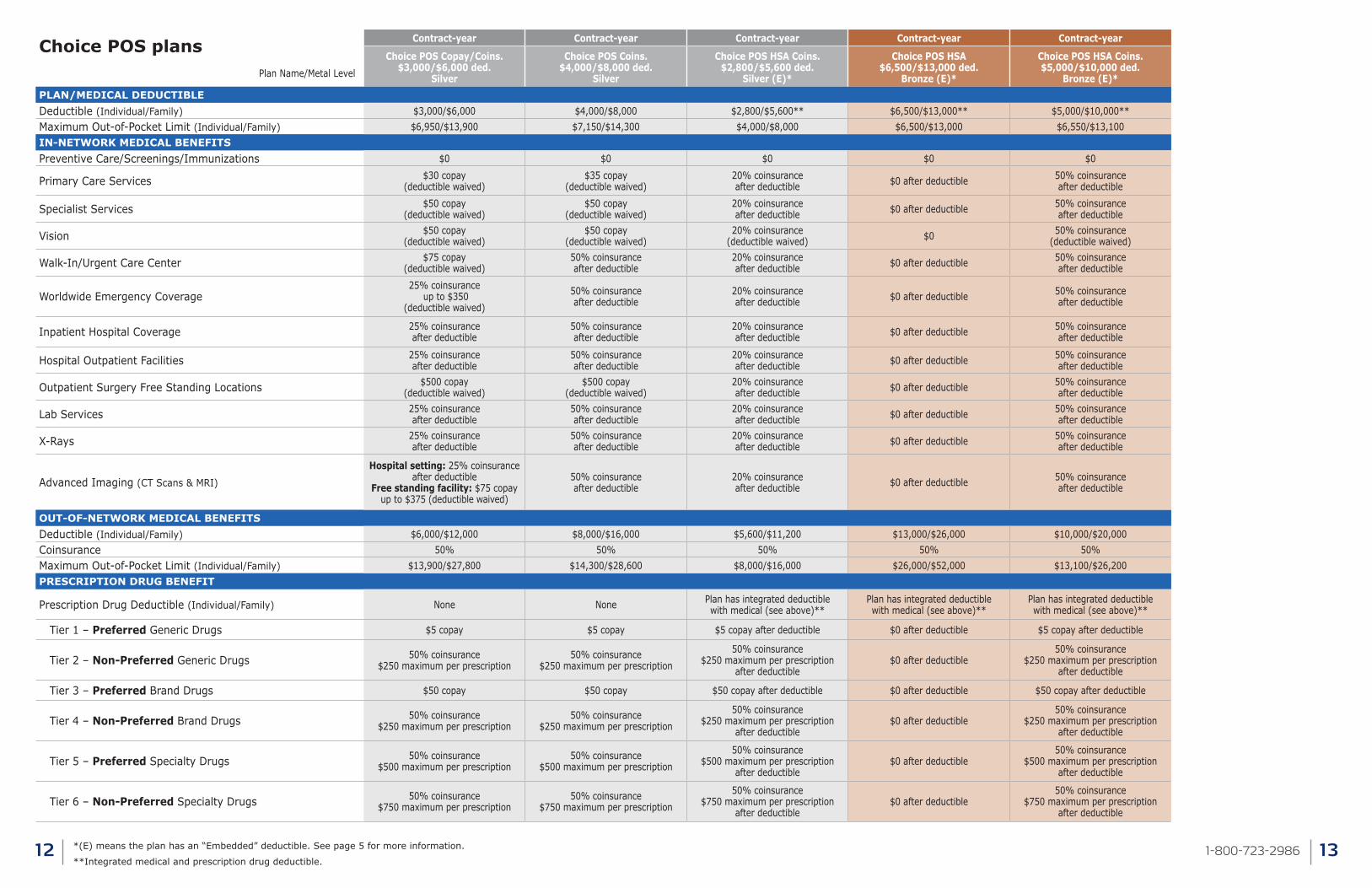
Choice POS plansPlan Name/Metal Level
Contract-year Contract-year Contract-year Contract-year Contract-year
Choice POS Copay/Coins. $3,000/$6,000 ded.
Silver
Choice POS Coins. $4,000/$8,000 ded.
Silver
Choice POS HSA Coins. $2,800/$5,600 ded.
Silver (E)*
Choice POS HSA $6,500/$13,000 ded.
Bronze (E)*
Choice POS HSA Coins. $5,000/$10,000 ded.
Bronze (E)*PLAN/MEDICAL DEDUCTIBLEDeductible (Individual/Family) $3,000/$6,000 $4,000/$8,000 $2,800/$5,600** $6,500/$13,000** $5,000/$10,000**Maximum Out-of-Pocket Limit (Individual/Family) $6,950/$13,900 $7,150/$14,300 $4,000/$8,000 $6,500/$13,000 $6,550/$13,100IN-NETWORK MEDICAL BENEFITSPreventive Care/Screenings/Immunizations $0 $0 $0 $0 $0
Primary Care Services $30 copay (deductible waived)
$35 copay (deductible waived)
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Specialist Services $50 copay (deductible waived)
$50 copay (deductible waived)
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Vision $50 copay (deductible waived)
$50 copay (deductible waived)
20% coinsurance (deductible waived) $0 50% coinsurance
(deductible waived)
Walk-In/Urgent Care Center $75 copay (deductible waived)
50% coinsurance after deductible
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Worldwide Emergency Coverage25% coinsurance
up to $350 (deductible waived)
50% coinsurance after deductible
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Inpatient Hospital Coverage 25% coinsurance after deductible
50% coinsurance after deductible
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Hospital Outpatient Facilities 25% coinsurance after deductible
50% coinsurance after deductible
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Outpatient Surgery Free Standing Locations $500 copay (deductible waived)
$500 copay (deductible waived)
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Lab Services 25% coinsurance after deductible
50% coinsurance after deductible
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
X-Rays 25% coinsurance after deductible
50% coinsurance after deductible
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
Advanced Imaging (CT Scans & MRI)
Hospital setting: 25% coinsurance after deductible
Free standing facility: $75 copay up to $375 (deductible waived)
50% coinsurance after deductible
20% coinsurance after deductible $0 after deductible 50% coinsurance
after deductible
OUT-OF-NETWORK MEDICAL BENEFITSDeductible (Individual/Family) $6,000/$12,000 $8,000/$16,000 $5,600/$11,200 $13,000/$26,000 $10,000/$20,000Coinsurance 50% 50% 50% 50% 50%Maximum Out-of-Pocket Limit (Individual/Family) $13,900/$27,800 $14,300/$28,600 $8,000/$16,000 $26,000/$52,000 $13,100/$26,200PRESCRIPTION DRUG BENEFIT
Prescription Drug Deductible (Individual/Family) None None Plan has integrated deductible with medical (see above)**
Plan has integrated deductible with medical (see above)**
Plan has integrated deductible with medical (see above)**
Tier 1 – Preferred Generic Drugs $5 copay $5 copay $5 copay after deductible $0 after deductible $5 copay after deductible
Tier 2 – Non-Preferred Generic Drugs 50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
after deductible$0 after deductible
50% coinsurance $250 maximum per prescription
after deductible
Tier 3 – Preferred Brand Drugs $50 copay $50 copay $50 copay after deductible $0 after deductible $50 copay after deductible
Tier 4 – Non-Preferred Brand Drugs 50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
50% coinsurance $250 maximum per prescription
after deductible$0 after deductible
50% coinsurance $250 maximum per prescription
after deductible
Tier 5 – Preferred Specialty Drugs 50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
after deductible$0 after deductible
50% coinsurance $500 maximum per prescription
after deductible
Tier 6 – Non-Preferred Specialty Drugs 50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
after deductible$0 after deductible
50% coinsurance $750 maximum per prescription
after deductible
*(E) means the plan has an “Embedded” deductible. See page 5 for more information.
**Integrated medical and prescription drug deductible.
3151-800-723-29861-800-723-298614
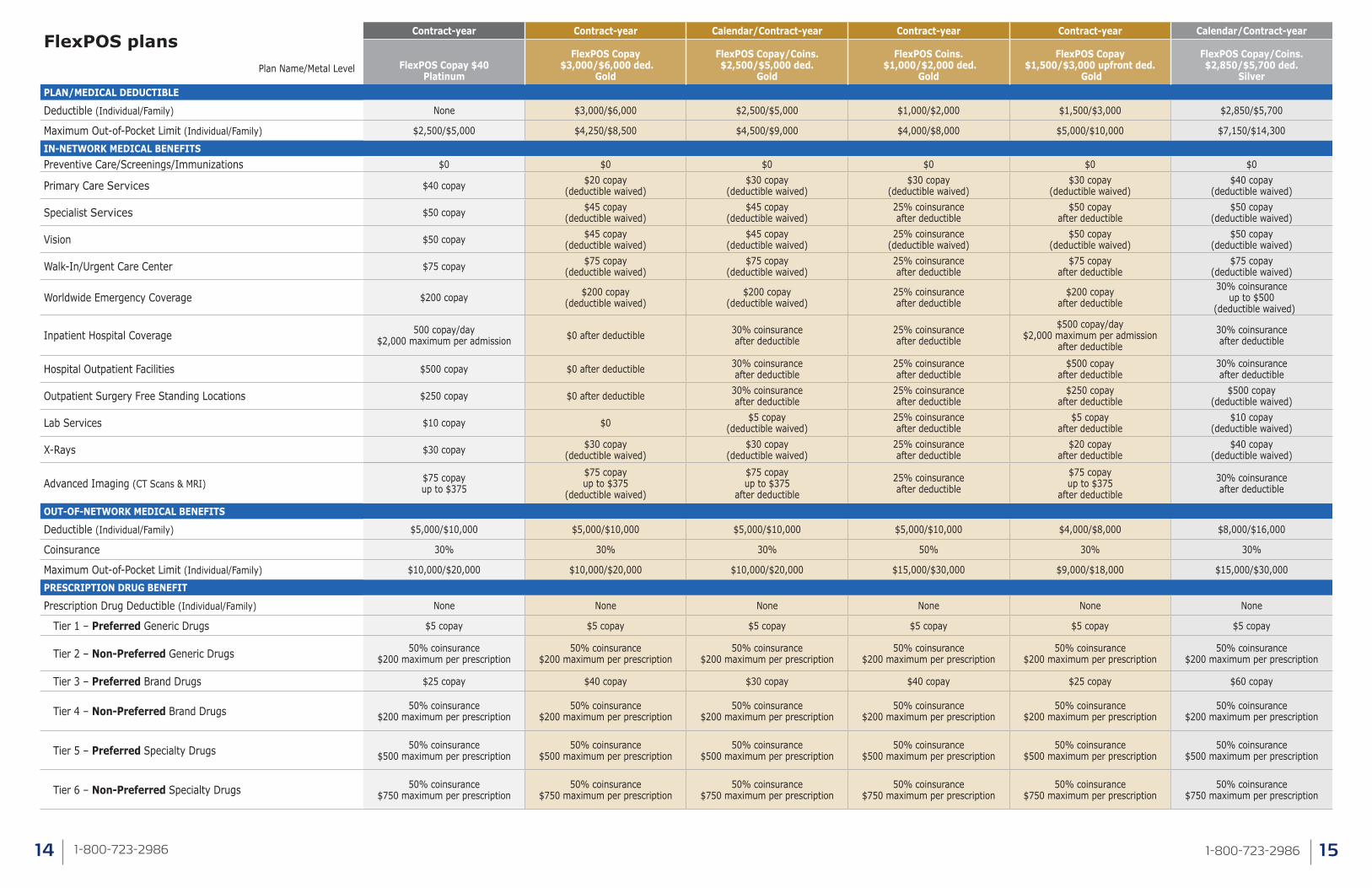
FlexPOS plansPlan Name/Metal Level
Contract-year Contract-year Calendar/Contract-year Contract-year Contract-year Calendar/Contract-year
FlexPOS Copay $40 Platinum
FlexPOS Copay $3,000/$6,000 ded.
Gold
FlexPOS Copay/Coins. $2,500/$5,000 ded.
Gold
FlexPOS Coins. $1,000/$2,000 ded.
Gold
FlexPOS Copay $1,500/$3,000 upfront ded.
Gold
FlexPOS Copay/Coins. $2,850/$5,700 ded.
SilverPLAN/MEDICAL DEDUCTIBLE
Deductible (Individual/Family) None $3,000/$6,000 $2,500/$5,000 $1,000/$2,000 $1,500/$3,000 $2,850/$5,700
Maximum Out-of-Pocket Limit (Individual/Family) $2,500/$5,000 $4,250/$8,500 $4,500/$9,000 $4,000/$8,000 $5,000/$10,000 $7,150/$14,300
IN-NETWORK MEDICAL BENEFITSPreventive Care/Screenings/Immunizations $0 $0 $0 $0 $0 $0
Primary Care Services $40 copay $20 copay (deductible waived)
$30 copay (deductible waived)
$30 copay (deductible waived)
$30 copay (deductible waived)
$40 copay (deductible waived)
Specialist Services $50 copay $45 copay (deductible waived)
$45 copay (deductible waived)
25% coinsuranceafter deductible
$50 copayafter deductible
$50 copay (deductible waived)
Vision $50 copay $45 copay (deductible waived)
$45 copay (deductible waived)
25% coinsurance(deductible waived)
$50 copay(deductible waived)
$50 copay (deductible waived)
Walk-In/Urgent Care Center $75 copay $75 copay (deductible waived)
$75 copay (deductible waived)
25% coinsuranceafter deductible
$75 copayafter deductible
$75 copay (deductible waived)
Worldwide Emergency Coverage $200 copay $200 copay(deductible waived)
$200 copay(deductible waived)
25% coinsuranceafter deductible
$200 copayafter deductible
30% coinsurance up to $500
(deductible waived)
Inpatient Hospital Coverage 500 copay/day$2,000 maximum per admission $0 after deductible 30% coinsurance
after deductible25% coinsuranceafter deductible
$500 copay/day$2,000 maximum per admission
after deductible
30% coinsuranceafter deductible
Hospital Outpatient Facilities $500 copay $0 after deductible 30% coinsuranceafter deductible
25% coinsuranceafter deductible
$500 copayafter deductible
30% coinsuranceafter deductible
Outpatient Surgery Free Standing Locations $250 copay $0 after deductible 30% coinsuranceafter deductible
25% coinsuranceafter deductible
$250 copayafter deductible
$500 copay (deductible waived)
Lab Services $10 copay $0 $5 copay (deductible waived)
25% coinsuranceafter deductible
$5 copayafter deductible
$10 copay (deductible waived)
X-Rays $30 copay $30 copay (deductible waived)
$30 copay (deductible waived)
25% coinsuranceafter deductible
$20 copayafter deductible
$40 copay (deductible waived)
Advanced Imaging (CT Scans & MRI) $75 copay up to $375
$75 copay up to $375
(deductible waived)
$75 copay up to $375
after deductible
25% coinsurance after deductible
$75 copay up to $375
after deductible
30% coinsuranceafter deductible
OUT-OF-NETWORK MEDICAL BENEFITS
Deductible (Individual/Family) $5,000/$10,000 $5,000/$10,000 $5,000/$10,000 $5,000/$10,000 $4,000/$8,000 $8,000/$16,000
Coinsurance 30% 30% 30% 50% 30% 30%
Maximum Out-of-Pocket Limit (Individual/Family) $10,000/$20,000 $10,000/$20,000 $10,000/$20,000 $15,000/$30,000 $9,000/$18,000 $15,000/$30,000
PRESCRIPTION DRUG BENEFIT
Prescription Drug Deductible (Individual/Family) None None None None None None
Tier 1 – Preferred Generic Drugs $5 copay $5 copay $5 copay $5 copay $5 copay $5 copay
Tier 2 – Non-Preferred Generic Drugs 50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance$200 maximum per prescription
Tier 3 – Preferred Brand Drugs $25 copay $40 copay $30 copay $40 copay $25 copay $60 copay
Tier 4 – Non-Preferred Brand Drugs 50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance $200 maximum per prescription
50% coinsurance$200 maximum per prescription
Tier 5 – Preferred Specialty Drugs 50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
Tier 6 – Non-Preferred Specialty Drugs 50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance $750 maximum per prescription
50% coinsurance$750 maximum per prescription
3171-800-723-29861-800-723-298616
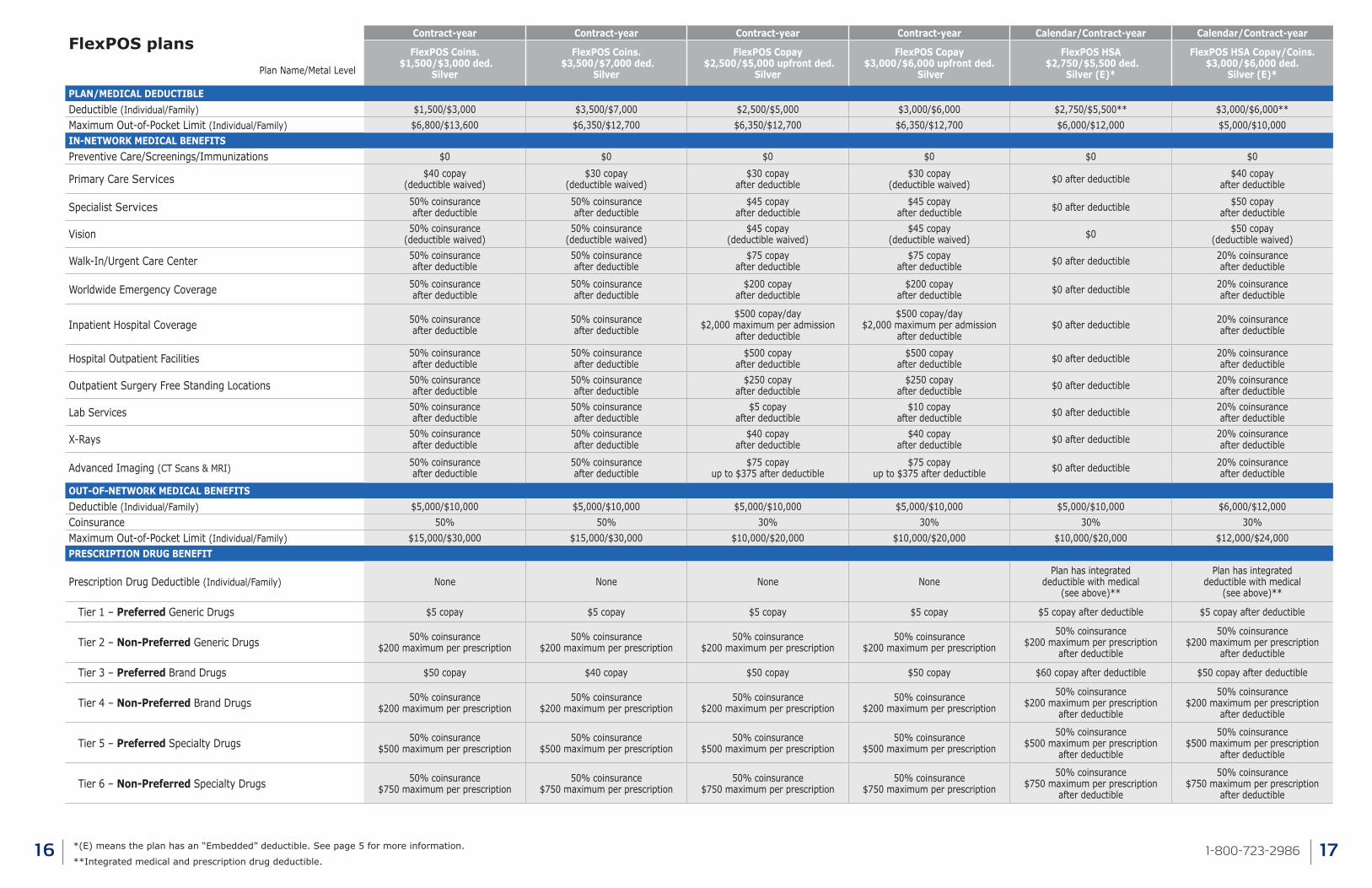
FlexPOS plansPlan Name/Metal Level
Contract-year Contract-year Contract-year Contract-year Calendar/Contract-year Calendar/Contract-year
FlexPOS Coins. $1,500/$3,000 ded.
Silver
FlexPOS Coins. $3,500/$7,000 ded.
Silver
FlexPOS Copay $2,500/$5,000 upfront ded.
Silver
FlexPOS Copay$3,000/$6,000 upfront ded.
Silver
FlexPOS HSA $2,750/$5,500 ded.
Silver (E)*
FlexPOS HSA Copay/Coins. $3,000/$6,000 ded.
Silver (E)*
PLAN/MEDICAL DEDUCTIBLEDeductible (Individual/Family) $1,500/$3,000 $3,500/$7,000 $2,500/$5,000 $3,000/$6,000 $2,750/$5,500** $3,000/$6,000**Maximum Out-of-Pocket Limit (Individual/Family) $6,800/$13,600 $6,350/$12,700 $6,350/$12,700 $6,350/$12,700 $6,000/$12,000 $5,000/$10,000IN-NETWORK MEDICAL BENEFITSPreventive Care/Screenings/Immunizations $0 $0 $0 $0 $0 $0
Primary Care Services $40 copay (deductible waived)
$30 copay (deductible waived)
$30 copay after deductible
$30 copay (deductible waived) $0 after deductible $40 copay
after deductible
Specialist Services 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$45 copay after deductible
$45 copay after deductible $0 after deductible $50 copay
after deductible
Vision 50% coinsurance (deductible waived)
50% coinsurance(deductible waived)
$45 copay (deductible waived)
$45 copay (deductible waived) $0 $50 copay
(deductible waived)
Walk-In/Urgent Care Center 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$75 copay after deductible
$75 copay after deductible $0 after deductible 20% coinsurance
after deductible
Worldwide Emergency Coverage 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$200 copay after deductible
$200 copay after deductible $0 after deductible 20% coinsurance
after deductible
Inpatient Hospital Coverage 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$500 copay/day$2,000 maximum per admission
after deductible
$500 copay/day$2,000 maximum per admission
after deductible$0 after deductible 20% coinsurance
after deductible
Hospital Outpatient Facilities 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$500 copay after deductible
$500 copay after deductible $0 after deductible 20% coinsurance
after deductible
Outpatient Surgery Free Standing Locations 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$250 copay after deductible
$250 copay after deductible $0 after deductible 20% coinsurance
after deductible
Lab Services 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$5 copay after deductible
$10 copay after deductible $0 after deductible 20% coinsurance
after deductible
X-Rays 50% coinsuranceafter deductible
50% coinsuranceafter deductible
$40 copay after deductible
$40 copay after deductible $0 after deductible 20% coinsurance
after deductible
Advanced Imaging (CT Scans & MRI) 50% coinsurance after deductible
50% coinsurance after deductible
$75 copay up to $375 after deductible
$75 copay up to $375 after deductible $0 after deductible 20% coinsurance
after deductible
OUT-OF-NETWORK MEDICAL BENEFITSDeductible (Individual/Family) $5,000/$10,000 $5,000/$10,000 $5,000/$10,000 $5,000/$10,000 $5,000/$10,000 $6,000/$12,000Coinsurance 50% 50% 30% 30% 30% 30%Maximum Out-of-Pocket Limit (Individual/Family) $15,000/$30,000 $15,000/$30,000 $10,000/$20,000 $10,000/$20,000 $10,000/$20,000 $12,000/$24,000PRESCRIPTION DRUG BENEFIT
Prescription Drug Deductible (Individual/Family) None None None NonePlan has integrated
deductible with medical (see above)**
Plan has integrated deductible with medical
(see above)**
Tier 1 – Preferred Generic Drugs $5 copay $5 copay $5 copay $5 copay $5 copay after deductible $5 copay after deductible
Tier 2 – Non-Preferred Generic Drugs 50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
Tier 3 – Preferred Brand Drugs $50 copay $40 copay $50 copay $50 copay $60 copay after deductible $50 copay after deductible
Tier 4 – Non-Preferred Brand Drugs 50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
50% coinsurance$200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
Tier 5 – Preferred Specialty Drugs 50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
50% coinsurance $500 maximum per prescription
after deductible
50% coinsurance $500 maximum per prescription
after deductible
Tier 6 – Non-Preferred Specialty Drugs 50% coinsurance$750 maximum per prescription
50% coinsurance$750 maximum per prescription
50% coinsurance$750 maximum per prescription
50% coinsurance$750 maximum per prescription
50% coinsurance$750 maximum per prescription
after deductible
50% coinsurance $750 maximum per prescription
after deductible
*(E) means the plan has an “Embedded” deductible. See page 5 for more information.
**Integrated medical and prescription drug deductible.
3191-800-723-29861-800-723-298618
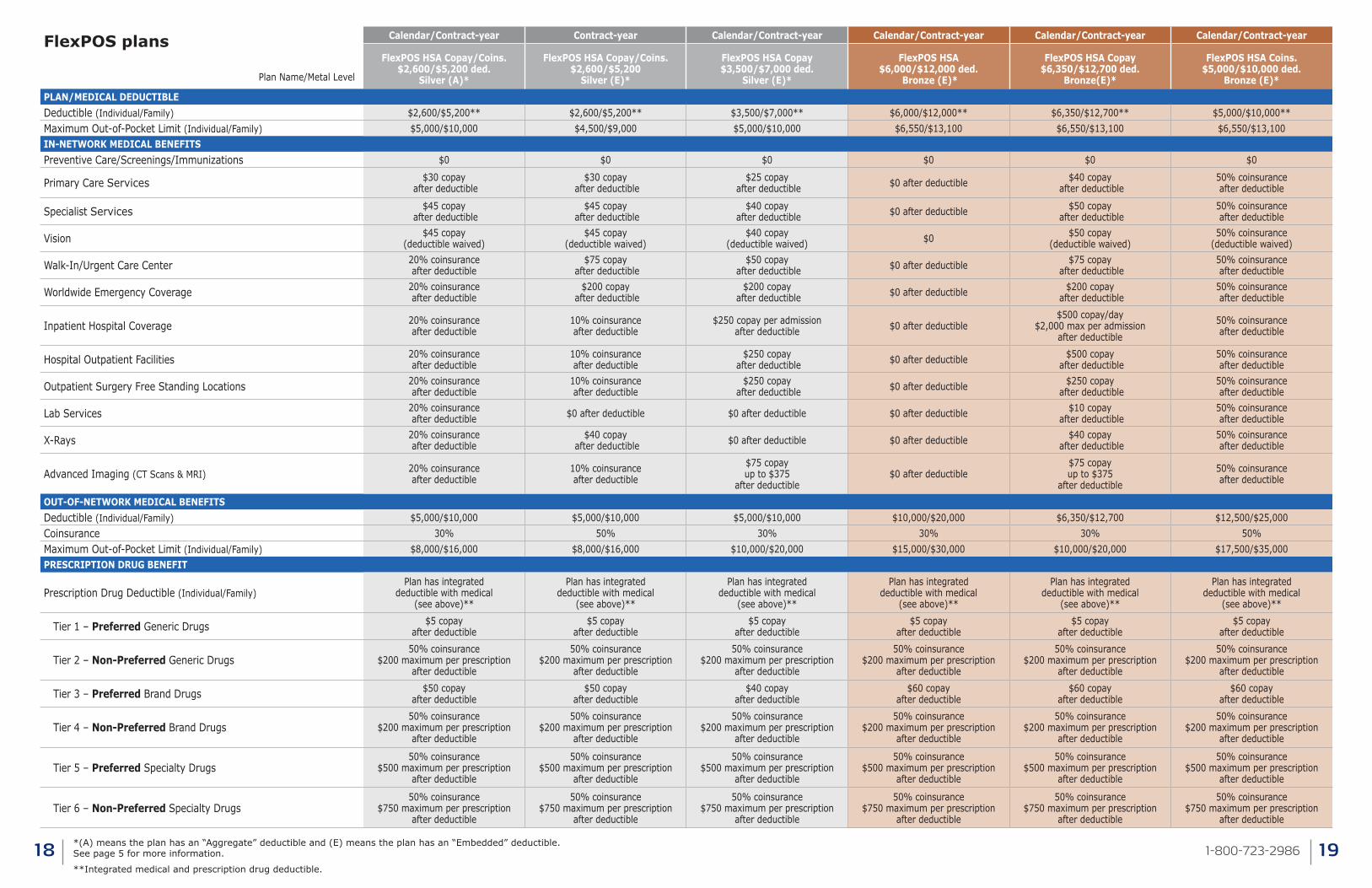
FlexPOS plans
Plan Name/Metal Level
Calendar/Contract-year Contract-year Calendar/Contract-year Calendar/Contract-year Calendar/Contract-year Calendar/Contract-year
FlexPOS HSA Copay/Coins. $2,600/$5,200 ded.
Silver (A)*
FlexPOS HSA Copay/Coins. $2,600/$5,200
Silver (E)*
FlexPOS HSA Copay $3,500/$7,000 ded.
Silver (E)*
FlexPOS HSA $6,000/$12,000 ded.
Bronze (E)*
FlexPOS HSA Copay $6,350/$12,700 ded.
Bronze(E)*
FlexPOS HSA Coins. $5,000/$10,000 ded.
Bronze (E)*
PLAN/MEDICAL DEDUCTIBLEDeductible (Individual/Family) $2,600/$5,200** $2,600/$5,200** $3,500/$7,000** $6,000/$12,000** $6,350/$12,700** $5,000/$10,000**Maximum Out-of-Pocket Limit (Individual/Family) $5,000/$10,000 $4,500/$9,000 $5,000/$10,000 $6,550/$13,100 $6,550/$13,100 $6,550/$13,100IN-NETWORK MEDICAL BENEFITSPreventive Care/Screenings/Immunizations $0 $0 $0 $0 $0 $0
Primary Care Services $30 copay after deductible
$30 copay after deductible
$25 copay after deductible $0 after deductible $40 copay
after deductible50% coinsurance after deductible
Specialist Services $45 copay after deductible
$45 copay after deductible
$40 copay after deductible $0 after deductible $50 copay
after deductible50% coinsurance after deductible
Vision $45 copay(deductible waived)
$45 copay(deductible waived)
$40 copay(deductible waived) $0 $50 copay
(deductible waived)50% coinsurance
(deductible waived)
Walk-In/Urgent Care Center 20% coinsuranceafter deductible
$75 copay after deductible
$50 copay after deductible $0 after deductible $75 copay
after deductible50% coinsurance after deductible
Worldwide Emergency Coverage 20% coinsuranceafter deductible
$200 copay after deductible
$200 copay after deductible $0 after deductible $200 copay
after deductible50% coinsurance after deductible
Inpatient Hospital Coverage 20% coinsuranceafter deductible
10% coinsurance after deductible
$250 copay per admission after deductible $0 after deductible
$500 copay/day$2,000 max per admission
after deductible
50% coinsurance after deductible
Hospital Outpatient Facilities 20% coinsuranceafter deductible
10% coinsurance after deductible
$250 copay after deductible $0 after deductible $500 copay
after deductible50% coinsurance after deductible
Outpatient Surgery Free Standing Locations 20% coinsuranceafter deductible
10% coinsurance after deductible
$250 copay after deductible $0 after deductible $250 copay
after deductible50% coinsurance after deductible
Lab Services 20% coinsuranceafter deductible $0 after deductible $0 after deductible $0 after deductible $10 copay
after deductible50% coinsurance after deductible
X-Rays 20% coinsuranceafter deductible
$40 copay after deductible $0 after deductible $0 after deductible $40 copay
after deductible50% coinsurance after deductible
Advanced Imaging (CT Scans & MRI) 20% coinsuranceafter deductible
10% coinsurance after deductible
$75 copay up to $375
after deductible$0 after deductible
$75 copay up to $375
after deductible
50% coinsurance after deductible
OUT-OF-NETWORK MEDICAL BENEFITSDeductible (Individual/Family) $5,000/$10,000 $5,000/$10,000 $5,000/$10,000 $10,000/$20,000 $6,350/$12,700 $12,500/$25,000Coinsurance 30% 50% 30% 30% 30% 50%Maximum Out-of-Pocket Limit (Individual/Family) $8,000/$16,000 $8,000/$16,000 $10,000/$20,000 $15,000/$30,000 $10,000/$20,000 $17,500/$35,000PRESCRIPTION DRUG BENEFIT
Prescription Drug Deductible (Individual/Family)Plan has integrated
deductible with medical (see above)**
Plan has integrated deductible with medical
(see above)**
Plan has integrated deductible with medical
(see above)**
Plan has integrated deductible with medical
(see above)**
Plan has integrated deductible with medical
(see above)**
Plan has integrated deductible with medical
(see above)**
Tier 1 – Preferred Generic Drugs $5 copay after deductible
$5 copay after deductible
$5 copay after deductible
$5 copay after deductible
$5 copay after deductible
$5 copay after deductible
Tier 2 – Non-Preferred Generic Drugs50% coinsurance
$200 maximum per prescription after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
Tier 3 – Preferred Brand Drugs $50 copay after deductible
$50 copay after deductible
$40 copay after deductible
$60 copay after deductible
$60 copay after deductible
$60 copay after deductible
Tier 4 – Non-Preferred Brand Drugs50% coinsurance
$200 maximum per prescription after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
50% coinsurance $200 maximum per prescription
after deductible
Tier 5 – Preferred Specialty Drugs50% coinsurance
$500 maximum per prescription after deductible
50% coinsurance $500 maximum per prescription
after deductible
50% coinsurance $500 maximum per prescription
after deductible
50% coinsurance $500 maximum per prescription
after deductible
50% coinsurance $500 maximum per prescription
after deductible
50% coinsurance $500 maximum per prescription
after deductible
Tier 6 – Non-Preferred Specialty Drugs50% coinsurance
$750 maximum per prescription after deductible
50% coinsurance $750 maximum per prescription
after deductible
50% coinsurance $750 maximum per prescription
after deductible
50% coinsurance $750 maximum per prescription
after deductible
50% coinsurance $750 maximum per prescription
after deductible
50% coinsurance $750 maximum per prescription
after deductible
*(A) means the plan has an “Aggregate” deductible and (E) means the plan has an “Embedded” deductible. See page 5 for more information.
**Integrated medical and prescription drug deductible.
3211-800-723-29861-800-723-298620
ConnectiCare complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. ConnectiCare does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
ConnectiCare:• Provides free aids and services to people with disabilities to communicate effectively
with us, including qualified interpreters and information in alternate formats.
• Provides free language services to people whose primary language is not English, including translated documents and oral interpretation.
If you need these services, contact ConnectiCare’s Committee for Civil Rights.
If you believe that ConnectiCare has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with: The Committee for Civil Rights, ConnectiCare, 175 Scott Swamp Road, Farmington, CT 06034, Phone: 1-800-251-7722, and TTY: 1-800-833-8134. You can file a grievance in person or by mail. If you need help filing a grievance, The Committee for Civil Rights is available to help you. You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of Health and Human Services, 200 Independence Avenue SW., Room 509F, HHH Building, Washington, DC 20201, 1-800-368-1019, 800-537-7697 (TDD).
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
Language & Non-Discrimination Notice

1 The Connecticut Mirror, 2015; HartfordBusiness.com, 2015; and Centers for Medicare & Medicaid Services (CMS) Monthly Summary Report (Data as of August 2016).2 2015 Net Promoter Industry Report3 NCQA Health Insurance Plan Rankings (2014-2015)4 “Free” preventive care means that you will not have a copay or have to pay money toward your deductible or coinsurance for the services. Sometimes a preventive care visit leads to other medical care or tests, even at the same appointment. You should check with your doctor or doctor’s staff during your visit to see if there are services you may be billed for.5 MDLIVE does not replace the primary care physician. MDLIVE is not an insurance product nor a prescription fulfillment warehouse. MDLIVE operates subject to state regulation and may not be available in certain states. MDLIVE does not guarantee that a prescription will be written. MDLIVE does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs, which may be harmful because of their potential for abuse. MDLIVE physicians reserve the right to deny care for potential misuse of services. MDLIVE interactive audio consultations with store and forward technology are available 24/7/365, while video consultations are available during the hours of 7 a.m. to 9 p.m. 7 days a week or by scheduled availability. MDLIVE and the MDLIVE logo are registered trademarks of MDLIVE, Inc. and may not be used without written permission. For complete terms of use visit www.mdlive.com/pages/terms.html.6 Discount programs provide access to discounted tuition and are NOT insured benefits. These discounts are offered separate from your health benefits. These arrangements do not represent an endorsement or guarantee on the part of ConnectiCare, Inc. You are responsible for the full cost of the discounted tuition. Vendors such as Sage, LLC are independent contractors and are not agents of ConnectiCare Specialty Services. Vendor participation may change without notice. Information is believed to be accurate as of the production date; however, it is subject to change. For more information about Sage, LLC, refer to www.tuitionrewards.com/cci.
©2016 ConnectiCare, Inc. & Affiliates CCISMGRPPRODGRID 1016
Questions? We’re here to help.1-800-723-2986Monday – Friday, 8 a.m. to 5 p.m.Or, call your broker
Related Documents







![GEET - Small Engine Conversion Plans[1]](https://static.cupdf.com/doc/110x72/547d27eeb4af9faa738b45fb/geet-small-engine-conversion-plans1-558461b16c9b7.jpg)


