Congestive Heart Failure Care Management Guide Content Summary Measures: Compiled from the National Quality Forum, National Committee for Quality Assurance, Centers for Medicare and Medicaid Services, ActiveHealth Management, and more. Pathways and Guidelines: Appearing in the form of stepwise diagrams and charts, these care pathways are currently practiced as management guidelines for diabetes, and recommended by groups such as the University Health System and the Mayo Clinic. Current Tools and Encounter Forms: Refer for examples of tools used in CHF treatment contexts. Sources: 1) http://www.universityhealthsystem.com/files/03-Diuresis%20Algorithm.pdf 2) http://www.universityhealthsystem.com/files/01-Algorithm,%20Page%201.pdf 3) http://www.universityhealthsystem.com/files/02-Algorithm,%20Page%202.pdf 4) http://www.universityhealthsystem.com/files/01- Pharmacologic%20Algorithm%20for%20Acute%20Decompensated%20CHF%20%28May,%202004%29.pdf 5) http://www.lef.org/protocols/heart_circulatory/congestive_heart_failure_03.htm#treatment 6) http://www.mayoclinic.org/congestive-heart-failure/treatment.html 7) http://www.vreehealth.com/vreehealth/products/services?gclid=COGHl4LpprYCFYxaMgodY30ABw 8) http://www.rwjf.org/content/dam/farm/toolkits/toolkits/2007/rwjf27044 9) http://www.iqbalandkhansurgical.com/sitebuildercontent/sitebuilderfiles/preopencounterform.pdf 10) https://providers.amerigroup.com/ProviderDocuments/WAWA_Internal_Medicine_Encounter.pdf

Congestive Heart Failure Protocols
Mar 29, 2016
Researching the latest protocols used in medical treatment, to help clients (healthcare providers) choose their most suitable data management and servicing options.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Congestive Heart Failure Care Management Guide
Content Summary
Measures: Compiled from the National Quality Forum, National Committee for Quality Assurance, Centers for Medicare and Medicaid Services, ActiveHealth Management, and more. Pathways and Guidelines: Appearing in the form of stepwise diagrams and charts, these care pathways are currently practiced as management guidelines for diabetes, and recommended by groups such as the University Health System and the Mayo Clinic. Current Tools and Encounter Forms: Refer for examples of tools used in CHF treatment contexts. Sources: 1) http://www.universityhealthsystem.com/files/03-Diuresis%20Algorithm.pdf 2) http://www.universityhealthsystem.com/files/01-Algorithm,%20Page%201.pdf 3) http://www.universityhealthsystem.com/files/02-Algorithm,%20Page%202.pdf 4) http://www.universityhealthsystem.com/files/01-Pharmacologic%20Algorithm%20for%20Acute%20Decompensated%20CHF%20%28May,%202004%29.pdf 5) http://www.lef.org/protocols/heart_circulatory/congestive_heart_failure_03.htm#treatment 6) http://www.mayoclinic.org/congestive-heart-failure/treatment.html 7) http://www.vreehealth.com/vreehealth/products/services?gclid=COGHl4LpprYCFYxaMgodY30ABw 8) http://www.rwjf.org/content/dam/farm/toolkits/toolkits/2007/rwjf27044 9) http://www.iqbalandkhansurgical.com/sitebuildercontent/sitebuilderfiles/preopencounterform.pdf 10) https://providers.amerigroup.com/ProviderDocuments/WAWA_Internal_Medicine_Encounter.pdf

Measures Used with Congestive Heart Failure
Centers for Medicare and
Medicaid Services
NQF 229: - Hospital 30-day, all-cause, risk-standardized mortality rate (RSMR) following heart failure (HF) hospitalization for patients 18 and older
NQF 699: - 30-Day Post-Hospital HF Discharge Care Transition Composite Measure - scores a hospital on the incidence among its patients during the month following discharge from an inpatient stay having a primary diagnosis of heart failure for three types of events: readmissions, ED visits and evaluation and management (E&M) services.
NQF 505: - Hospital 30-day all-cause risk-standardized readmission rate (RSRR) following acute myocardial infarction (AMI) hospitalization.
NQF 698: - 30-Day Post-Hospital AMI Discharge Care Transition Composite Measure - scores a hospital on the incidence among its patients during the month following discharge from an inpatient stay having a primary diagnosis of heart failure for three types of events: readmissions, ED visits and evaluation and management (E&M) services.
NQF 330: - Hospital 30-day, all-cause, risk-standardized readmission rate (RSRR) following heart failure hospitalization
NQF 521: - Heart Failure Symptoms Addressed - Percent of patients exhibiting symptoms of heart failure for whom appropriate actions were taken
American Medical
Association - Physician
Consortium for Performance Improvement (AMA-PCPI)
NQF 78: - Heart Failure (HF) : Assessment of Clinical Symptoms of Volume Overload (Excess)
NQF 83: - Heart Failure : Beta-blocker therapy for Left Ventricular Systolic Dysfunction - Percentage of patients aged 18 years and older with a diagnosis of heart failure with a current or prior LVEF < 40% who were prescribed beta-blocker therapy either within a 12 month period when seen in the outpatient setting or at hospital discharge
NQF 81: - Heart Failure: Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction
NQF 1524: - Assessment of Thromboembolic Risk Factors (CHADS2) - Patients with nonvalvular atrial fibrillation or atrial flutter in whom assessment of thromboembolic risk factors using the CHADS2 risk criteria has been documented
ActiveHealth Management
NQF 610: - Heart Failure - Use of ACE Inhibitor (ACEI) or Angiotensin Receptor Blocker (ARB) Therapy - The percentage of patients aged 18 and older with Heart Failure who are on an ACEI or ARB
NQF 615: - Heart Failure - Use of Beta Blocker Therapy - The percentage of patients 18 years and older diagnosed with heart failure who are taking a beta blocker
NQF 624: - Atrial Fibrillation - Anticoagulation Therapy - Percentage of adult patients aged 25 and older with atrial fibrillation and major stroke risk factors who are on anticoagulation therapy.
Centers for Disease Control and Prevention
NQF 2020: - Adult Current Smoking Prevalence - Percentage of adult (age 18 and older) U.S. population that currently smoke.
Agency for Healthcare
Research and Quality
NQF 358: - Congestive Heart Failure (CHF) Mortality Rate (IQI 16) - Perecent of discharges with principal diagnosis code of CHF with in-hospital mortality
NQF 277: - Heart Failure Admission Rate (PQI 8) - Percent of county population with an admissions for heart failure.
Accountable Care Organization
ACO 10: - Ambulatory Sensitive Conditions Admissions: Congestive Heart Failure - age-standardized acute care hospitalization rate for conditions where appropriate ambulatory care prevents or reduces the need for admission to the hospital, per 100,000 population under age 75 years
Data gathering sources for measures like ACO 10 include claims data, ICD9 codes, and service dates.

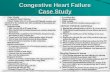
Pharmacologic Algorithm for Diuresis in CHF
Yes
No
Yes
Yes
No
No
Yes
Yes
Yes
Yes
No
No
No
No
1. Monitoring Parameters: *Weights: initially 1-2lbs weight loss per day until “ideal” weight
achieved *Volume depletion -Hypotension -Dizziness -Decreased urine output -Increased BUN (BUN/Cr > 20) *Electrolytes -Supplement K+ if <3.5 mg/dL in patient not on Digoxin and K+ <
4.0mg/dL if patient on Digoxin 2. If patient symptoms are controlled during day, but worse at night,
may need to administer diuretic regimen in evening or more frequently as needed
3. When Furosemide dose is >80-120 mg/day, use BID dosing 4. May require increase in monitoring and tighter control of K+, Mg2+
Patient volume overloaded (Sig. PND, Orthopnea, Edema)
Low Sodium diet 2 Liter Fluid Restriction Loop Diuretic (e.g.,Furosemide 40mg )
Achieve dry weight or improving symptoms,
volume status
Monitor 1,2
Lasix daily dose >
320mg?3 Double the dose
Achieve Goal?
Monitor 1,2
Add Thiazide-like Diuretic 4
CrCl >
40ml/min
HCTZ 25mg with
Furosemide
Metolazone 5mg with Furosemide 4
Achieve Dry weight or improving
symptoms, volume status
SCr <2.5 mg/dl Or
CrCL > 40 ml/min
Double HCTZ Dose
If on HCTZ switch to Metolazone 5mg. If on
Metolazone double the dose.
Achieve dry weight or improving symptoms,
volume status
Monitor 1,2
Consider admitting patient if not already in hospital for IV Furosemide
Monitor 1,2

Pharmacologic Algorithm for Congestive Heart Failure (revised 2004; page 1)
No
1. Consider Cardiology Consult, See Beta Blocker position statement
2. Target Doses: Captopril 50-100 mg TID Enalapril 10 mg BID Trandolapril 4 mg qd Fosinopril 40 mg qd 3. See Diuretic Algorithm 4. See ACE-inhibitor Position Statement 5. See ACE-inhibitor Intolerance Position Statement
Yes
Yes
Yes
No
No
Yes
Yes
Yes
No
No
No
No
Yes
No
Patients with HF symptoms: Dyspnea, Fatigue, Exercise
Intolerance
Physical Exam Assess volume Status
Determine Functional Class
Perform Echo, CXR, ECG Systolic Dysfunction
Treat HTN,CAD if present
Follow regularly to Assess response to
Treatment Q4-6 months
*Start ACE-I; Achieve Target Dose 2,4 *Diuretic if Volume Overloaded 3 *Discontinue Type I antiarrhythmics, calcium
antagonists, NSAIDs *Anticoagulate - Mobile Thrombus - Prior Thromboembolism - Atrial Fibrillation (Afib) *If Afib consider cardioversion, Amiodarone *Vtach/SCD: EPS Consult
Significant CAD
Or Valve Disease?
Refer for: Revascularization
Or Valve
Repair/Replacement Reduce CAD Risks
Consult: CT Surgery or Interventional
Cardiology Search for other causes
Nonischemic, nonvalvular CM:ETOH, drugs, HTN, low
thyroid, etc.
*Add Carvedilol1*Re-evaluate volume status and diuretic needs
*Consider Amlodipine, Felodipine Hydralazine/ISDN
*Re-evaluate volume status and diuretic needs.
ACE-I Intolerant?
SymptomsResolve
?
SymptomsResolve
?
Is patient Hypertensive
?
Follow regularly to assess response to
treatment Q-6 months
Follow regularly to assess response to
treatment Q4-6 months
Symptoms Resolve?
*Re-evaluate volume status and diuretic needs.
*Add Digoxin
Follow regularly to assess response to
treatment q 4-6 months
Hydralazine + ISDN
R/O CAD Assess Myocardial Viability
*Thallium Stress *Stress Echo
R/O Valvular disease *Cardiac Catheterization

CHF Algorithm (Con’t)
Abbreviations: HF Heart Failure CT Cardiothoracic HTN Hypertension ISDN Isosorbide dinitrate CAD Coronary artery disease NYHA New York Heart Association ACE-I Angiotensin converting enzyme inhibitors LVEF Left ventricular ejection fraction NSAID Nonsteroidal anti-inflammatory drugs CXR Chest x-ray Vtach Ventricular Tachycardia SCD Sudden cardiac death EPS Electrophysiology Service ETOH Alcohol CM Cardiomyopathy
No
Yes
Yes
Yes
Yes
No
No
Evaluate: NYHA/LVEF @ 3 months after stabilization of therapy
NYHA I?
*Consider D/C Digoxin *Continue ACE-I *Continue Carvedilol,
Metoprolol XL or Bisoprolol Follow regularly to assess response to
treatment Q 4-6 months
NYHA II or III?
NYHA IV?
*Continue Digoxin *Continue ACE-I *Adjust Diuretic *Continue Carvedilol,
Metoprolol XL or Bisoprolol1 (Carvedilol if NYHA Class IIIb) *Consider Hydralazine/ISDN *Consider Spironolactone *Research Studies *Widened QRS: Consider BiV
pacing
SymptomsResolve?
Follow regularly to assess response to
treatment Q 4-6 months
*Continue Digoxin *Continue ACE-I *Adjust Diuretic *Carvedilol (Cardiology Consult)*Consider Hydralazine /ISDN *Spironolactone *Refer for Heart Transplant *Consider Inotropes *Research Studies *Widened QRS: Consider BiV-
pacing
*Adjust Dosages *Add Remaining Drugs *Refer to CHF/Transplant Team

Page 1 of 3 Pharmacologic Algorithm for Acute Decompensated Heart Failure
Yes Yes
Yes
Yes
No
Yes
No
No Unsure No
Yes No
Yes Yes
Yes
Yes Severe AS,
HCM, restrictive CM, constrictive pericarditis, or
tamponade confirmed?
Abnormal cardiac enzymes +/-
ischemic ECG changes?
Treat as AMI or ACS • Consider cath/PCI • Consider IABP
Clinical suspicion of severe AS, HCM,
restrictive CM, constrictive pericarditis,
tamponade?
• Inotropes • Consider IABP • Cath, PCI for
suspected AMI/ACS
• Hold α HTN meds, β-blockers, ACE-I, ARB
BNP
elevated?
Cardiogenic shock or symptomatic hypotension?
• Hypoperfusion • Cool extremities • Altered mental status
Suspected acute/decompensated heart failure • History & physical, O2 sat • CXR/ECG • CBC, Chemistry, ?blood gas • Consider cardiac enzymes
Respiratory Failure
imminent?
Evidence of LV diastolic dysfunction?
• BiPAP/CPAP trial • Endotracheal intubation • If BP elevated, consider nitroglycerin, nitroprusside, nesiritide • ICU admission
Consider non-cardiac etiology
Decompensated Heart Failure
Likely?
Consider non-cardiac etiology
ECHO Refer to Diastolic
Heart Failure Pathway

Page 2 of 3
No No
No
Yes
Yes
Yes No
Yes No
No
Yes
History of LV systolic
dysfunction?ECHO
Obtain Cardiology
Consult
Evidence of LV systolic dysfunction?
Cautious hydration
Optimize SNS, RAAS antagonism
Volume depleted?
Volume overloaded?
Administer 1-2 times oral furosemide dose IV
If diuretic naïve, start with 40 mg IV furosemide
Total daily oral dose > 160 mg furosemide or
serum creatinine > 2 mg/dL?
• Diuresis and Aggressive Na+ restriction (< 2 g/day) • Consider d/c metformin, TZD’s
• D/C offending drugs Class I antiarrhythmics NSAIDS Calcium channel blockers
• Consider beta-blocker dose reduction • Supplemental oxygen • Consider anticoagulation • Consider ECHO if suspicion of
worsening pump, valve function.

Page 3 of 3
Urine output ≥ 400 mL and improved symptoms
after 2 hrs?
No
Obtain cardiology consult Initiate nesiritide 2 µg / kg loading dose followed by continuous infusion of 0.01 µg / kg / min
Urine output ≥400 mL and improved symptoms
after 2 hrs?
Yes
Yes
Optimize diuretic and ACE-I (or ARB) dose. Initiate/uptitrate beta-
blocker once euvolemic
No
Yes
Consider diuretic resistance IV bolus dose to max of 160 mg Consider continuous infusion (start at 0.1 mg/ kg/hr) after
bolus Consider addition of metolazone or hydrochlorothiazide
Re-bolus with 2 times initial IV dose at least 2 hours after first bolus
Optimize diuretic and ACE-I
(or ARB) dose Initiate / uptitrate beta-blocker once euvolemic
No
Consider diuretic resistance IV bolus dose to max of 160 mg Consider continuous infusion (start at 0.1
mg/ kg/hr) after bolus Consider metolazone or
hydrochlorothiazide Nesiritide 2 µg / kg loading dose followed by continuous infusion of 0.01 µg / kg / min
Urine output ≥ 400 mL and improved symptoms
after 2 hrs?

Home Membership Products Magazine Health News About
Print PDF Email References Suggested Products Tweet 0
Introduction
Risk Factors for CHF
Conventional Treatments For CHF
Classes Of CHF
Diagnosing CHF
Health Concerns
Page: 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9
Congestive Heart Failure
Conventional Treatments For CHF
Once CHF has been diagnosed, physicians usually rely on a constellation of pharmaceuticals to address its symptoms
and slow its progression. The exact drugs used depend on the type and severity of CHF, but some of the more common
drugs include:
Diuretics — Sometimes called “water pills”, diuretics help remove excess fluid from the body. Diuretics are
often the first line of treatment. A significant side effect is the loss of potassium in urine, which may result in
electrolyte abnormalities (Braunwald 2001).
Angiotensin-converting enzyme (ACE) inhibitors — ACE inhibitors have been shown to improve survival
among patients with CHF by lowering blood pressure. Side effects include dangerously low blood pressure,
dizziness, coughing, and birth defects (Kostis 1994).
Beta blockers — Beta blockers slow the heart rate by making it less sensitive to adrenaline (epinephrine). This
medication may be given after a patient's condition has stabilized with ACE inhibitors. Side effects may include
weight gain, tiredness, dizziness, and sensitivity to cold. Patients with a slow heart rate, elevated systolic blood
pressure, peripheral vascular disease, asthma, chronic obstructive pulmonary disease, or who have had certain
heart rhythm abnormalities should not take beta blockers (Hunt 2002).
Digoxin — Digoxin is used to control symptoms of some forms of CHF and control heart rate irregularities (Hunt
2002). Side effects include abdominal pain, nausea or vomiting, diarrhea, and rarely, dangerous heart rhythm
abnormalities.
These drugs may be prescribed in an emergency setting while the physician works to stabilize the patient's condition
and in the long-term management of CHF. While these drugs are proven to extend the lives of patients with CHF, they
also cause a wide range of side effects that often require more drug therapy. Despite such intensive drug therapy, the
condition of most patients with CHF will eventually worsen, requiring more serious measures. A physician may
recommend insertion of a pacemaker or left ventricular assist device. In extreme cases, the patient may require a heart
transplant.
Vitamins and dietary supplements have also been shown to ease the symptoms of CHF—often without the debilitating
side effects of more powerful pharmaceuticals (Witte 2005). Coenzyme Q10 (CoQ10) has been widely studied in CHF
and found to increase heart function, while L-carnitine and taurine have been shown to improve cardiac function and
lessen the heart's workload (Fugh-Berman 2000; Schaffer 2000). Other dietary supplements and nutrients, including
minerals (e.g., magnesium and potassium), antioxidants (e.g., R-lipoic acid and vitamins C and E), and herbs (e.g.,
hawthorn) may help ease symptoms of CHF. Each of these will be discussed in detail later in this chapter.
The hormonal system is also affected by CHF. In the early stages of CHF, studies have shown that the body tries to
compensate for reduced cardiac function with a series of neurohormonal adaptations that work to maintain normal
blood pressure and increase the output of the heart (Dzau 1981; Dzau 1987). As the disease progresses, however, this
hormonal response is overwhelmed, and the body's delicate hormonal balance is damaged. While there is still much to
learn about the interaction of the hormonal system and CHF, hormonal therapy may offer an option for treatment.
It is important to make lifestyle changes that will slow the progression of CHF. These changes include limiting salt
intake (sometimes severely), losing weight to reduce the workload on the heart, avoiding alcohol or drugs, and
monitoring water intake. As always, no program of dietary supplementation and lifestyle changes should be launched
without the consent of a physician.
Male Comprehensive Hormone Panel
Blood Test
Quick Buy
Female Comprehensive Hormone Panel
Blood Test
Quick Buy
VAP® Blood Test
Quick Buy
PLAC® Test (Lp-PLA2) Blood Test
Quick Buy
Thyroid Panel (TSH, T4, Free T4, Free
T3) Blood Test
Quick Buy
Show more
Super Omega-3 EPA/DHA with Sesame
Lignans & Olive Fruit Extract, 120
softgels
Quick Buy
Super Ubiquinol CoQ10 with Enhanced
Mitochondrial Support™, 100 mg 60
softgels
Quick Buy
Optimized Carnitine with Glycocarn®, 60
vegetarian capsules
Quick Buy
Taurine, 1000 mg 50 capsules
Quick Buy
Hawthorn Supreme, 60 vegetarian
liquid-filled capsules
Quick Buy
Show more
Novel Support for Chronic Heart Failure,
Arrhythmia and Coronary Artery
Blockage
Restoring Cellular Energy Metabolism
How to Circumvent 17 Independent
My Account My Cart Sale Translate Help
Like 1
Targeted Nutritional Strategies
Covering All The Bases
CHF And The Hormonal Connection
Life Extension Suggestions
Search: coq10, 00335, weight loss
Welcome, guest. Please Sign in or Sign up
Congestive Heart Failure - 3 - CHF, Heart Rate, Chronic High Blood Pre... http://www.lef.org/protocols/heart_circulatory/congestive_heart_failure_...
1 of 2 4/1/2013 5:29 AM

Contact Us Privacy Policy Terms Site Map
All Contents Copyright © 1995-2013 Life Extension® All rights reserved.
What You Have Learned So Far...
The rate of CHF is increasing, at least partly because of our ability to treat other forms of heart disease and
partly because of the aging population.
Half of all patients with CHF die within 5 years of diagnosis.
Most patients with CHF have other underlying forms of heart disease, especially CAD. This complicates both the
diagnosis and treatment of CHF.
CHF cannot be reversed, but its severity can be improved. At best, conventional medicine uses a constellation of
powerful drugs to slow it down. These drugs have side effects that range from mild to severe and may
dramatically reduce one's quality of life.
Besides drugs, CHF can be treated with surgical interventions such as implantation of a pacemaker or even with
a heart transplant.
Some nutrients and supplements—such as CoQ10, L-carnitine, and taurine—have been shown to increase the
heart's function or reduce side effects of drugs used to treat CHF.
Lifestyle changes, including dietary modifications and avoiding drugs and alcohol (which might stress the heart),
are an important part of any heart-healthy program. Patients may also be advised to limit their intake of salt and
water.
Heart Attack Risk Factors
Media Says: No Cure for Heart Disease –
Life Extension
Conventional CoQ10 Fails Severe Heart
Disease Patients
Show more
CONGESTIVE HEART FAILURE AND
CARDIOMYOPATHY
Search For This Topic
Like One person likes this. Be the first of your friends.
Vitamins & Supplements
CoQ10 (Coenzyme Q10)
Fish Oil (Omega-3)
Multivitamins
PQQ (Pyrroloquinoline Quinone)
Curcumin
Irvingia
More Supplements
Popular Health Topics
Hormone Restoration, Female
Hormone Restoration, Male
Atherosclerosis
Prostate Cancer
Diabetes
Arthritis
More Health Topics
Departments
Home
Membership
Products
Magazine
Health
News
About
Contact Us
Orders: 1-800-544-4440
Advisors: 1-800-226-2370
Help: 1-800-678-8989
E-mail: Contact & Feedback Form
Follow Us:
Receive exclusive Life Extension News weekly:
Congestive Heart Failure - 3 - CHF, Heart Rate, Chronic High Blood Pre... http://www.lef.org/protocols/heart_circulatory/congestive_heart_failure_...
2 of 2 4/1/2013 5:29 AM

Share on:
Ventricular assistdevice
EnlargeCardiacresynchronizationtherapy device
Enlarge
Congestive Heart Failure
Treatment
At Mayo Clinic, doctors trained in heart care (cardiologists) and cardiologists with advanced training in heart failure (heart failure cardiologists) treat people who have
congestive heart failure. Mayo Clinic cardiac surgeons have extensive experience in all types of surgery to treat heart failure and other heart diseases. Surgeons
perform minimally-invasive heart surgery, implant ventricular assist devices (VADs) and perform heart transplants.
Congestive heart failure treatment can significantly improve your symptoms and help your weakened heart work as efficiently as possible. Doctors treat some people by
correcting the underlying cause of the condition, such as controlling a fast heart rhythm, opening blocked arteries or repairing or replacing diseased valves. Heart failure
specialists also treat conditions that may aggravate your underlying heart problems, such as sleep apnea, thyroid problems, anemia and other blood abnormalities.
Congestive heart failure treatment at Mayo Clinic may include surgery, medical devices, medications and lifestyle changes.
Surgery
Heart valve repair or replacement. Cardiologists may recommend heart valve repair or replacement surgery to treat an underlying condition that led tocongestive heart failure. Heart valve surgery may relieve your symptoms and improve your quality of life.
Coronary bypass surgery. Cardiologists may recommend coronary bypass surgery to treat your congestive heart failure if your disease results fromseverely narrowed coronary arteries.
Heart transplant. Some people who have severe congestive heart failure may need a heart transplant.
Myectomy. In a myectomy, the surgeon removes part of the overgrown septal muscle in your heart to decrease the blockage that occurs in hypertrophiccardiomyopathy. Surgeons may perform myectomy when medication no longer relieves your symptoms.
Medical devices
Ventricular assist device (VAD). When your weakened heart needs help pumping blood, surgeons may implant a VAD into yourabdomen and attach it to your heart. These mechanical heart pumps can be used either as a "bridge" to heart transplant or aspermanent therapy for people who aren't candidates for a transplant. Mayo Clinic offers VADs to many people who may have noother options.
Cardiac resynchronization therapy (CRT) device (biventricular cardiac pacemaker). A cardiacresynchronization therapy device (biventricular cardiac heart pacemaker) sends specifically timedelectrical impulses to your heart's lower chambers. CRTs are suitable for people who have moderateto severe congestive heart failure and abnormal electrical conduction in the heart.
Internal cardiac defibrillator (ICD). Doctors implant ICDs under the skin to monitor and treat fast orabnormal heart rhythms (arrhythmias), which occur in some people who have heart failure. The ICDsends electrical signals to your heart if it detects a high or abnormal rhythm to shock your heart intobeating more slowly and pumping more effectively.
Medications. Doctors usually treat people who have congestive heart failure with medications proven torelieve symptoms and increase survival in people who have heart failure. Your doctor may also prescribemedications to lower blood pressure, improve circulation and prevent blocked arteries or blood thinners toprevent blood clots.
Several types of drugs may help treat your heart failure if you have reduced blood flow pumping out of your heart's main pumping chamber (left ventricle).
Angiotensin-converting enzyme (ACE) inhibitors. ACE inhibitors lower blood pressure, improve blood flow and decrease your heart's workload.
Angiotensin II (A-II) receptor blockers. These drugs provide several benefits of ACE inhibitors without the potential side effect of a persistent cough.
Beta blockers. Beta blockers slow the heart rate, lower blood pressure and lessen the risk of some abnormal heart rhythms.
Digoxin. Also known as digitalis, digoxin increases the strength of heart contractions and tends to slow your heartbeat.
Diuretics. Diuretics prevent fluid from collecting in your body and decrease fluid in your lungs, making breathing easier.
Nesiritide. Nesiritide, which is given through a vein (intravenously), is a synthetic version of B-type natriuretic peptide (BNP), a hormone that occurs naturallyin your body.
Congestive Heart Failure — Treatment at Mayo Clinic http://www.mayoclinic.org/congestive-heart-failure/treatment.html
1 of 2 4/1/2013 5:32 AM

Share on:
Aldosterone antagonists. These medications may help your heart work better, reverse scarring of the heart and help prolong your life if you have severecongestive heart failure.
Inotropes. These are intravenous medications used in severe heart failure patients to improve heart pumping function and maintain blood pressure.
Sometimes congestive heart failure becomes severe enough to require hospitalization and monitoring for a few days. While you're in the hospital, you may take
medications that quickly help your heart pump better and relieve your symptoms. You may also receive supplemental oxygen. People who have severe congestive
heart failure that doesn't improve with treatment may need supplemental oxygen on a long-term basis.
Lifestyle changes. Lifestyle changes often can relieve symptoms of congestive heart failure and prevent your disease from worsening. Some changes youcan make include:
Avoiding or limiting alcohol to one drink two or three times a week
Avoiding or limiting caffeine
Eating a low-fat, low-sodium diet
Exercising by yourself or in a structured cardiac rehabilitation program
Maintaining a healthy weight or losing weight if you're overweight
Quitting smoking
Reducing stress
Terms of Use and Information Applicable to this SiteCopyright ©2001-2013 Mayo Foundation for Medical Education and Research. All Rights Reserved.
Congestive Heart Failure — Treatment at Mayo Clinic http://www.mayoclinic.org/congestive-heart-failure/treatment.html
2 of 2 4/1/2013 5:32 AM

(/vreehealth
/home)
home
(/vreehealth
/home)
about
(/vreehealth
/about)
products/services
(/vreehealth
/products/services)
posts
(/vreehealth
/posts)
contact us
(/vreehealth
/contactUs)
Post-Discharge Issues Transi�onAdvantage Delivers
Incomplete hand-off of pa�ents' health
care back to their primary care
physicians
Seamless and integrated connec�vity of
pa�ents' health informa�on across their
extended care team, including primary care
physicians, family caregivers, and their
hospital care team
Lack of frequent monitoring to alert
health care providers before issues
become serious
Daily Health Checks that track pa�ents'
compliance with their physician-prescribed,
post-discharge care plan and iden�fy red
flags so health care providers can be alerted
before issues become serious
Pa�ent difficulty understanding and
complying with prescribed medica�ons
A trained Transi�on Liaison to provide
medica�on management services, including
pa�ent reminders and compliance
monitoring, and to direct pa�ents with
medica�on ques�ons to registered nurses
Difficulty coordina�ng implementa�on
of care across the extended care team
Advanced technology combined with a
Transi�on Liaison assigned to each pa�ent
to coordinate with the appropriate health
care providers and proac�vely involve
family caregivers
Enhanced post-discharge care for your pa�ents
Transi�onAdvantage is a post-discharge service that is designed to help you reduce preventable
30-day readmissions by addressing mul�ple common causes of readmissions for pa�ents with
conges�ve heart failure, pneumonia, or acute myocardial infarc�on. Our comprehensive service
is resource efficient for your hospital and works in conjunc�on with your current processes.
Benefits of implemen�ng Transi�onAdvantage in your hospital:
Reduce your Medicare reimbursement penal�es
Improve the quality of care you already provide your pa�ents
Improve overall pa�ent sa�sfac�on
Transi�onAdvantage addresses preventable 30-day readmission issues
For more informa�on on Transi�onAdvantage
When you are ready to enhance your current post-discharge service, we are ready to show you
how. Contact us (mailto:[email protected]) to see what Vree™ Health has for you and
your hospital.
Contact us to set up a free
consulta�on to see what
Transi�onAdvantage is designed to
do for you and your hospital.
(mailto:[email protected]
contact us
(mailto:[email protected])
Transi�onAdvantage™
products/services TransitionAdvantage http://www.vreehealth.com/vreehealth/products/services?gclid=COGHl...
1 of 2 4/1/2013 5:36 AM

about us (/vreehealth/about)
Vree Health is dedicated to developing technology-
enabled services that address the needs of
pa�ents, family caregivers, hospitals, and other
health care providers.
contact us (/vreehealth/contactUs)
E-mail: [email protected]
(mailto:[email protected])
site map (/vreehealth/sitemap)
home (/vreehealth/home)
about (/vreehealth/about)
products/services (/vreehealth/products/services)
posts (/vreehealth/posts)
contact us (/vreehealth/contactUs)
Copyright © 2012 Vree Health, a wholly owned subsidiary of Merck & Co., Inc. All rights reserved. vrh-07162012-web-1.0
products/services TransitionAdvantage http://www.vreehealth.com/vreehealth/products/services?gclid=COGHl...
2 of 2 4/1/2013 5:36 AM

June 2007 Pilot Version 16 – Follow-Up Form 1
The University Hospitals and Clinics
Jackson, Mississippi
CARDIOLOGY
CLINIC ENCOUNTER FORM
DATE:___________________
TIME IN:_________________
Race: ________________
Ethnicity: _____________
Language: ____________
T ____ P____ R____ BP_____ Ht_____ WT_____ BMI______ Previous Wt/date___/___
Age / gender ___________ M / F
Change in physician(s): □ yes □ no If yes, update provider list □ done Nurse’s Note: Physical Activity/Exercise:
Medications/allergies: □ updated Immunizations: : □ updated
Past Medical History: Unchanged from: ____/____/______
□ HTN □ DM □ MI □ LVSD □Dyslipidemia □ CABG □ PCI □ Implanted device
Other:
Family history:
Social History: Tobacco use: □ never □ past □ current (at present or within past 12 months)
______ Packs/day ________Duration Smoking cessation discussed: □Yes □No □ N/A
Interventions recommended: □ Yes □ No □ N/A Drug use: □ Never □ Past □ Current Type:_____________________________________________
ETOH Use: □Yes □ No Type: □ wine □ beer □ Liquor Amount:___________per day/week/month
Caffeine: □ Yes □ No ___________Cups per day/week/month? Type: ________________
CC&HPI
PLACE DEMOGRAPHIC STICKER HERE
□ HF
□ CAD □ Other
**********
Follow-Up
Visit Form

June 2007 Pilot Version 16 – Follow-Up Form 2
CARDIOVASCULAR SYMPTOMS: Medical Record#
Chest pain □ Yes □ No Dyspnea □ Yes □ No Orthopnea □ Yes □ No Number of pillows ________
Frequency: □ At rest
Quality: □ Mild exertion Y N PND
Level of activity: □ Moderate exertion Y N Palpitations
Intensity (scale 1-10): □ Strenuous exertion Y N Presyncope/syncope
Location: SOB with: Y N Orthostatic lightheadedness
Duration: Distance __________ Y N LE swelling
Precipitating/relief factors: Pace _____________ Y N Fatigue
Flat Uphill Stairs
Change from baseline □ Yes □ No Y=Yes, N= No
ROS: Unchanged from: _____/_____/______ (Date)
□ Cough □ Nocturia □ Nausea □ Headache □ Other
PHYSICAL EXAM:
VS: □ see previous page T ____ HR ____ BP ____ RR ____
General: □ well developed
□ no apparent distress
CV: Rhythm □ regular □ irregular
JVP □ normal □ elevated ____ cm H2O
Carotid bruits □ none □ present (□ left □ right)
PMI □ normal □ displaced laterally □ sustained
Murmurs □ none □ systolic location ____________
□ diastolic location ____________
Thrills □ none □ present location ____________
S3 □ no □ yes
S4 □ no □ yes
LE edema □ no □ yes level (ankle, knee, thigh, etc.) ____________
Lungs: □ symmetrical chest expansion
□ clear to auscultation bilaterally
□ Rales location ____________
□ wheezes location ____________
□ rhonchi location ____________
Abdomen: □ soft, nontender, nondistended
□ normal active bowel sounds
Hepatomegaly □ no □ yes
Ascites □ no □ yes
Rectal exam □ not indicated □ normal
Extremities: □ Edema 1+ 2+ 3+ 4+ location _______________
□ Warm □ cool □ cyanosis □ pallor □ skin changes_________________
Pulses: Radial Brachial Femoral Pop PT DP ALL
L 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
R 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 □ No cyanosis or clubbing □ Full ROM of all extremities □ Normal muscle strength and tone

June 2007 Pilot Version 16 – Follow-Up Form 3
DATA REVIEW: (Laboratory / Radiology / Additional Records)
LV Systolic Function:
Last LVEF _____% Date __________ Method ____________
High risk / Known CAD?: Yes No
If yes, diabetes screening performed? Yes No Refer to Metabolic Clinic
ICD for EF < 35% Done Planned Not indicated
HF Beta-Blocker ACE/ARB Anticoagultion (Warfarin)
Prescribed, LVEF <40% Prescribed, LVEF <40%
N/A – No Paroxysmal or Chronic Atrial FibPrescribed for Paroxysmal or Chronic Atrial Fib
Prescribed Other Reasons
Prescribed Other Reasons
Not Prescribed other reasons-why not?*
Not Prescribed -Why not?*
Not Prescribed-Why not?*
Anticoagulant prescribed for other reason:________________________
*Must document reason not prescribed
CAD
Beta-Blocker ACE/ARB Antiplatelet LDL-C
Therapy Lowering Therapy
Prescribed, Prior MI
Prescribed, LVEF <40% &/or Diabetic Prescribed
Not Indicated (LDL-c <100)
Prescribed Other Reasons
Prescribed Other Reasons
Prescribed Other Reasons Prescribed
Not Prescribed- Why not?*
Not Prescribed-Why not?*
Not Prescribed- Why not?
Not Prescribed- Why not?*
**Must document reason not prescribed
Angina (CCVS) class: I II III IV
HF (NYHA) class: I II III IV
PLACE DEMOGRAPHIC STICKER HERE
□ HF
□ CAD
□ Other
**********
Follow-Up
Visit Form

June 2007 Pilot Version 16 – Follow-Up Form 4
ASSESSMENT/PLAN:
________________________________
Physician Signature
ATTENDING SUPPLEMENT:
________________________________
Physician Signature
PLACE DEMOGRAPHIC STICKER HERE
□ HF
□ CAD
□ Other
**********
Follow-Up
Visit Form

June 2007 Pilot Version 16 – Follow-Up Form 5
PHYSICIAN ORDERS: Testing: BNP Chem 8 CBC Liver panel Glucose TSH
□ Lipid profile/panel (CAD) Other: (Specify)
Echocardiogram EKG X-Ray ____________________________
Heart Catheterization: Type___________ Date scheduled ___________________
Stress test type: _________________________________________________________________
Other: (specify) ___________________________________________________________________
Referrals: Cardiopulmonary rehab Other: ______________________________
Return appointment to clinic: _________________________________
Medication changes: ______________________________________________________________
Physician Signature: _______________________________________________ Date: ______________
Nurse/discharge note: Yes No N/A Comments Other
Treatment, test, procedure
F/U appointment
School/Work release
Prescriptions given
Patient Education (**if note follow-up, must include additional education):
□ Weight monitoring □ Symptom management □ Follow-up plans
□ Diet: sodium restriction □ Physical activity □ Medication instruction
□ Diet: fluid restriction □ Smoking cessation
□ Minimizing/avoiding use of NSAIDs
□ Other:
Comments:
Discharge Condition:_________________________________________________________________
Signature: _______________________________ Date:_________________ Time:___________
□ HF
□ CAD
□ Other
**********
Follow-Up
Visit Form
PLACE DEMOGRAPHIC STICKER HERE

BOLD Preoperative Encounter Form
Date of Visit ____________
Last Name _______________________
Weight _____________ lbs kgs Height _____________ in cm
COMORBIDITIES (You must select ONLY ONE per category for each system)
First Name _______________________ Chart Number ________________
Hypertension No history Borderline, no medication Diagnosis of hypertension, no medication Treatment with single medication Treatment with multiple medications Poorly controlled by medications, organ damage
Congestive Heart Failure No history or symptoms of congestive heart failure Class I: Symptoms with more than ordinary activity Class II: Symptoms with ordinary activity Class III: Symptoms with minimal activity Class IV: Symptoms at rest
Ischemic Heart Disease No history of ischemic heart disease Abnormal ECG, no active ischemia History of MI or antiischemic medication PCI, CABG Active ischemia
Angina Assessment No chest pain symptoms/angina Anginal chest with extreme exertion (e.g. running, swimming, etc.) Anginal chest pain occurs with moderate activity or exertion Anginal chest pain with minimal exertion (e.g. walking across a room) or 'at rest Unstable angina
Peripheral Vascular Disease No symptoms of peripheral vascular disease Asymptomatic with bruit Claudication, antiischemic medication Transient ischemic attack, rest pain Procedure for peripheral vascular disease Stroke, loss of tissue secondary to ischemia
Lower Extremity Edema No symptoms of lower extremity edema Intermittent lower extremity edema, not requiring treatment Symptoms requiring treatment, diuretics, elevation, or hose Stasis ulcers Disability, decreased function, hospitalization
DVT/PE No history of DVT/PE History of DVT resolved with anticoagulation Recurrent DVT long term anticoagulation meds Previous PE Recurrent PE, decreased function, hospitalization Vena Cava filter
CARDIOVASCULAR DISEASE
METABOLIC Glucose Metabolism No symptoms or evidence of diabetes Elevated fasting glucose Diabetes, controlled with oral medication Diabetes, controlled with insulin Diabetes, controlled with insulin and oral medication Diabetes, with severe complications (retinopathy, neuropathy, renal failure, blindness)
Gout Hyperuricemia No symptoms of gout/hyperuricemia Hyperuricemia, no symptoms Hyperuricemia, medications Arthropathy Destructive joints Disability, unable to walk
Lipids (Dyslipidemia or Hyperlipidemia) Not present Present, no treatment required Controlled with lifestyle change, including Step 1 or Step 2 diet Controlled with single medication Controlled with multiple medications Not controlled
Obstructive Sleep Apnea Syndrome No symptoms or evidence of obstructive sleep apnea syndrome Sleep apnea symptoms (negative sleep study or not done) Sleep apnea diagnosis by sleep study (no oral appliance) Sleep apnea requiring oral appliance such as CPAP Sleep apnea with significant hypoxia or oxygen dependent Sleep apnea with complications (pulmonary HTN, etc.)
Obesity Hypoventilation Syndrome No symptoms of obesity hypoventilation Hypoxemia/hypercarbia on room air Severe hypoxemia or hypercarbia Pulmonary hypertension Right heart failure Right heart failure left ventricular dysfunction
PULMONARY Pulmonary Hypertension No symptoms or indication of pulmonary hypertension Symptoms associated with PH(tiredness, SOB, dizziness, fainting) Confirmed PH diagnosis Well controlled on anticoagulants and/or calcium channel blockers Stronger medications and/or oxygen Patient needs or has had lung transplant
Asthma No symptoms of asthma Intermittent mild symptoms, no medication Symptoms controlled with oral inhaler (such as albuterol) Well controlled with ongoing daily medication Symptoms not well controlled, steroids or anticholinergics Hospitalized within last 2 years, history of intubation
GASTROINTESTINAL GERD No history of GERD Intermittent or variable symptoms, no medication Intermittent medication H2 blockers or low dose PPI High dose PPI Meet criteria for antireflux surgery, or prior surgery for GERD
Cholelithiasis No history of gallstones Gallstones with no symptoms Gallstones with intermittent symptoms Gallstones with severe symptoms or h/o cholecystectomy Gallstones with complications requiring immediate surgery prior to gastric bypass History of cholecystectomy with ongoing complications not resolved
Liver Disease No history of liver disease Hepatomegaly modest, normal LFT's, fatty change Category 1 Modest or greater hepatomegaly, LFT alteration, fatty change Category 2 Moderate to marked hepatomegaly, fatty change Category 3, mild
inflammation, mild fibrosis Definite NASH, cirrhosis, hepatic dysfunction by LFT's Hepatic failure, transplant indicated or done

Multiple Vitamin Calcium Vitamin B12 Iron Vitamin D Vitamin A, D, E Combo Calcium with Vitamin D
COMORBIDITIES (continued) (You must select ONLY ONE per category for each system)
REPRODUCTIVE Polycystic Overian Syndrome No history of polycystic ovarian syndrome Symptoms of PCOS, no treatment OCP's or antiandrogen Rx Medformin or TZD Combination therapy Infertility
Menstrual Irregularities (not PCOS) No history of menstrual irregularities Irregular periods or oligomenorrhea Menorrhagia Amenorrhea Prior total abdominal hysterectomy
MUSCULOSKELETAL
Musculoskeletal Disease No symptoms of musculoskeletal disease Pain with community ambulation Non narcotic analgesia required Pain with household ambulation Surgical intervention required (ex: arthroscopy) Awaiting or past joint replacement or other disability
Back Pain No symptoms of back pain Intermittent symptoms not requiring medical treatment Symptoms requiring nonnarcotic treatment Degenerative changes or positive objective findings, symptoms requiring narcotic treatment Surgical intervention done or recommended pending weight loss Failed previous surgical intervention with existing symptoms
Fibromyalgia No history of fibromyalgia Treatment with exercise Treatment with nonnarcotic medications Treatment with narcotics Treatment with narcotics: Surgical intervention done or recommended Disabling, treatment not effective
MEDICATIONS/VITAMINS & MINERALS
Stress Urinary Incontinence No history of stress urinary incontinence Minimal and intermittent Frequent but not severe Daily occurrence, requires sanitary pad Disabling Operation ineffective
Pseudotumor Cerebri No symptoms of pseudotumor cerebri Headaches with dizziness, nausea, and/or pain behind the eyes, no visual symptoms Headaches with visual symptoms and/or controlled with diuretics Patient has had MRI to confirm PTC, is well controlled with oral diuretics Patient is well controlled with stronger medications Patient requires narcotics or has had (or needs) surgical intervention
Abdominal Hernia No hernia Asymptomatic hernia, no prior operation Symptomatic hernia with or without incarceration Successful repair Recurrent hernia or size > 15 cm Chronic evisceration through large hernia with associated complication or multiple failed hernia repairs
GENERAL Functional Status No impairment of functional status Able to walk 200ft with assistance device (cane or crutch) Cannot walk 200ft with assistance device (cane or crutch) Requires wheelchair Bedridden
Abdominal Skin/Pannus No symptoms Intertriginous irritation Pannus so large it interferes with ambulation Recurrent cellulitis, ulceration Surgical treatment required
SIGNATURE (Name and Signature of person completing Encounter Form)
Name (print) _______________________________ Signature _____________________________________
BOLD Preoperative Encounter Form (continued)
PSYCHOSOCIAL Confirmed Mental Health Diagnosis None Bipolar disorder Anxiety/panic disorder Personality disorder Psychosis
Psychosocial Impairment No impairment Mild impairment in psychosocial functioning but able to perform all primary tasks Moderate impairment in psychosocial functioning but able to perform most primary tasks Moderate impairment in psychosocial functioning and unable to perform some primary tasks Severe impairment in psychosocial functioning and unable to perform most primary tasks Severe impairment in psychosocial functioning and unable to function
Depression No symptoms of depression Mild and episodic not requiring treatment Moderate, accompanied by some impairment, may require treatment Moderate with significant impairment, treatment indicated Severe, definitely requiring intensive treatment Severe requiring hospitalization
Alcohol Use None Rare Occasional Frequent
Tobacco Use None Rare Occasional Frequent
Substance Abuse (Prescription or Illegal) None Rare Occasional Frequent

PF-ALL-0077-12
Internal Medicine Encounter Form Mail to: Claims Department Amerigroup P.O. Box 61010 Virginia Beach, VA 23466-1010
Member Information Provider Information
Last Name: Provider Name:
First Name: Phone #: Provider ID #:
Member ID #: Date of Birth: Fax #: Date of Visit:
Address:
Level of Care: Please circle at least one CPT (Procedure) Code.
Preventive/Physical Office Visit Counseling
Age New Established New Patient
Established Patient
Code Length of Time
12–17 99384 99394 99201 99211 99401 15 minutes
18–39 99385 99395 99202 99212 99402 30 minutes
40–64 99386 99396 99203 99213 99403 45 minutes
65+ 99387 99397 99204 99214 99404 60 minutes
99205 99215
Diagnosis Codes: Please indicate primary, secondary, and tertiary codes (1, 2, 3). *If elements of well care were performed, please mark a well code as a secondary diagnosis.
Well Child/Preventive ICD-9 Codes ___ 716.90 Arthropathy, NOS ___ 244.9 Hypothyroidism
___ V70.0 Routine Physical (12+) ___ 493.9 Asthma, Unspec ___ 487.1 Influenza w/ Other Resp. Manifestations
___ V70.3 General Medical Exam ___ 724.5 Back Pain, Unspec ___ 724.2 Lower Back Pain
___ V70.5 Health Exam ___ 466.0 Bronchitis, Acute ___ 780.79 Malaise and Fatigue, Other
___ V70.6 Health Exam in Pop Survey ___ 490 Bronchitis ___ 496 Chronic Obstructed Airway (COPD)
___ V70.8 Other Specified Gen Med Exam
___ 786.50 Chest Pain ___ 729.1 Myalgia/Myositis, Unspec
___ V70.9 Gnrl Medical Exam, Unspec ___ 428.0 Congestive Heart Failure
___ 410.9 Myocardial Infarction, NOS
Counseling ICD-9 Codes ___ 372.30 Conjunctivitis, Unspec ___ 278.00 Obesity, Unspec
___ V65.3 Dietary Counseling ___ 564.0 Constipation ___ 715.90 Osteoarthrosis, Unspec
___ V65.41 Exercise ___ 780.39 Convulsions ___ 382.9 Otitis Media, Unspec
___ V65.42 Substance Use/Abuse ___ 786.2 Cough ___ 462 Pharyngitis, Acute
___ V65.43 Injury Prevention ___ 311 Depression ___ 486 Pneumonia, Organism Unspec
___ V65.44 HIV Counseling ___ 692.9 Derm. Contc/Eczema ___ 782.1 Rash

PF-ALL-0077-12
___ V65.45 STD Counseling ___ 787.91 Diarrhea ___ 477.9 Rhinitis, Allergy
Other Preventive ICD-9 Codes ___ 780.4 Dizziness/Giddiness ___ 472.0 Rhinitis, Chronic
___ V22.1 Pregnancy, Supervision Other Norm
___ 250.00 DM Type II ___ 461.9 Sinusitis, Acute
___ V22.2 Pregnant State, Incidental ___ 250.02 DM Type II, Uncontrolled
___ 473.9 Sinusitis, Chronic
___ V67.9 Follow-up Exam, Unspec ___ 786.09 Dyspnea ___ 710.0 Systemic Lupus Erythematosis
Diagnoses ___ 625.3 Dysmenorrhea ___ 305.1 Tobacco Dependence
___ 789.00 Abd Pain, Unspec ___ 558.9 Gastroenteritis ___ 463 Tonsillitis, Acute
___ 706.1 Acne ___ 530.81 Gastroesophogeal Reflux
___ 242.90 Thyrotoxicosis w/o Crisis
___ 303.91 Alcohol Dependency ___ 784.0 Headache ___ 465 URI, Acute, Mult of Unspec Site
___ 995.3 Allergy, Unspec ___ 785.2 Heart Murmur ___ 465.9 URI, Acute, Site Unspec
___ 626.0 Amenorrhea ___ 599.7 Hematuria ___ 599.0 UTI
___ 285.9 Anemia, Unspec ___ 042 HIV Disease ___ 616.10 Vaginitis & Vulvovaginitis
___ 413.9 Angina, Stable ___ 401.1 HTN, Benign Essen ___ 079.9 Other Viral Infection
___ 411.1 Angina, Unstable ___ 401.9 HTN, Essen, Unspec ___ Other
___ 300.0 Anxiety Disorder ___ 272.0 Hypercholesterolemia ___ Other
___ 714.0 Arthritis, Rheumatoid ___ 272.4 Hyperlipidemia ___ Other
Immunizations
___ 90718 DT (Adult) ___ 90658 Flu Shot (Split virus) ___ 90707 MMR
___ 90732 Pneumococcal ___ 90746 Hepatitis B (Adult) ___ Other
Laboratory Tests/Screening – For Data Collection Purposes
___ 83036 HbA1c __ 85014 Hematocrit ___ 87110 Chlamydia ___ 81000 Urinalysis
___ 85018 Hemoglobin __ 82465 Cholesterol (total)
___ 86580 Mantoux (TB) ___ 87070 Throat Culture
___ 88141 Pap Smear __ 80061 Lipid Panel ___ 82043 Microalbumin qty
___ Other
___ 85025 CBC with Diff __ 83721 LDL Cholesterol ___ 87086 Urine Culture ___ Other
Print Physician Name
Physician Signature and Date of Signature
Related Documents