31 C ongenital heart disease (CHD) is one of the most common birth defects, with ≈1% incidence in live births. The heri- table nature of CHD is indicated by the increased recurrence risk for CHD and the observation that syndromic forms of CHD are often associated with chromosomal anomalies, such as 22q11 deletion in DiGeorge syndrome. However, investi- gations into the genetic basis of CHD have been challenging given that CHD is often sporadic. Even when there is strong evidence of heritability, there may be variable penetrance and variable expressivity. This could reflect the confounding effects of genetic heterogeneity in the human population. In addition, evidence suggests that environmental factors can contribute to CHD, indicating a multifactorial pathogenesis to CHD. Clinical Perspective on p 42 Studies in mice have expanded our knowledge of genes that can cause CHD. Mice are well suited for modeling CHD because they have the same cardiac anatomy as humans, with 4-chamber hearts and distinct left–right asymmetries that provide separate pulmonary systemic circulation required for oxygenation of blood. These structures are the major targets of CHD. Although knockout mice have yielded new insights into the genetic pathogenesis of CHD, the analysis is limited to one gene at a time. In comparison, forward genetic screens using ethylnitrosourea (ENU) mutagenesis can greatly accel- erate novel gene discovery. With ENU mutagenesis, every animal by design harbors many mutations. Thus, with focused phenotyping, gene discovery can proceed rapidly and without a priori gene bias. By conducting such screens in an inbred mouse strain background, the confounding effects of genetic heterogeneity could be minimized. 1 We previously conducted a small-scale mouse forward genetic screen to recover CHD mutants using the Acuson clinical ultrasound system for noninvasive fetal echocardiog- raphy. 2,3 Although echocardiography is the imaging modality of choice for diagnosing CHD, the poor imaging resolution of Background—Congenital heart disease (CHD) has a multifactorial pathogenesis, but a genetic contribution is indicated by heritability studies. To investigate the spectrum of CHD with a genetic pathogenesis, we conducted a forward genetic screen in inbred mice using fetal echocardiography to recover mutants with CHD. Mice are ideally suited for these studies given that they have the same four-chamber cardiac anatomy that is the substrate for CHD. Methods and Results—Ethylnitrosourea mutagenized mice were ultrasound-interrogated by fetal echocardiography using a clinical ultrasound system, and fetuses suspected to have cardiac abnormalities were further interrogated with an ultrahigh-frequency ultrasound biomicroscopy. Scanning of 46 270 fetuses revealed 1722 with cardiac anomalies, with 27.9% dying prenatally. Most of the structural heart defects can be diagnosed using ultrasound biomicroscopy but not with the clinical ultrasound system. Confirmation with analysis by necropsy and histopathology showed excellent diagnostic capability of ultrasound biomicroscopy for most CHDs. Ventricular septal defect was the most common CHD observed, whereas outflow tract and atrioventricular septal defects were the most prevalent complex CHD. Cardiac/visceral organ situs defects were observed at surprisingly high incidence. The rarest CHD found was hypoplastic left heart syndrome, a phenotype never seen in mice previously. Conclusions—We developed a high-throughput, 2-tier ultrasound phenotyping strategy for efficient recovery of even rare CHD phenotypes, including the first mouse models of hypoplastic left heart syndrome. Our findings support a genetic pathogenesis for a wide spectrum of CHDs and suggest that the disruption of left–right patterning may play an important role in CHD. (Circ Cardiovasc Imaging. 2014;7:31-42.) Key Words: heart defects, congenital ◼ microscopy, acoustic © 2013 American Heart Association, Inc. Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.113.000451 Received March 14, 2013; accepted November 27, 2013. From Department of Developmental Biology, University of Pittsburgh, Pittsburgh, PA (X.L., R.F., A.J.K., R.R., G.C., R.S., S.A., Y.K., L.W., K.T., C.W.L.); Genetic Resource Science, The Jackson Laboratory, Bar Harbor, ME (J.M., H.C.P., L.R.); Department of Pediatric Pathology, Children’s Hospital of Pittsburgh, Pittsburgh, PA (W.D.); and Children’s National Medical Center, Washington, DC (L.L.). The Data Supplement is available at http://circimaging.ahajournals.org/lookup/suppl/doi:10.1161/CIRCIMAGING.113.000451/-/DC1. Correspondence to Cecilia W. Lo, 530 45th St, Pittsburgh, PA 15201. E-mail [email protected] Interrogating Congenital Heart Defects With Noninvasive Fetal Echocardiography in a Mouse Forward Genetic Screen Xiaoqin Liu, MD, PhD; Richard Francis, PhD; Andrew J. Kim, BS; Ricardo Ramirez, BS; Guozhen Chen, MD; Ramiah Subramanian, MD, PhD; Shane Anderton, BS; Youngsil Kim, BS; Liyin Wong, BS; Judy Morgan, PhD; Herbert C. Pratt, PhD; Laura Reinholdt, PhD; William Devine, BS; Linda Leatherbury, MD; Kimimasa Tobita, MD; Cecilia W. Lo, PhD Congenital Heart Disease by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from by guest on July 14, 2018 http://circimaging.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
31
Congenital heart disease (CHD) is one of the most common birth defects, with ≈1% incidence in live births. The heri-
table nature of CHD is indicated by the increased recurrence risk for CHD and the observation that syndromic forms of CHD are often associated with chromosomal anomalies, such as 22q11 deletion in DiGeorge syndrome. However, investi-gations into the genetic basis of CHD have been challenging given that CHD is often sporadic. Even when there is strong evidence of heritability, there may be variable penetrance and variable expressivity. This could reflect the confounding effects of genetic heterogeneity in the human population. In addition, evidence suggests that environmental factors can contribute to CHD, indicating a multifactorial pathogenesis to CHD.
Clinical Perspective on p 42
Studies in mice have expanded our knowledge of genes that can cause CHD. Mice are well suited for modeling CHD because they have the same cardiac anatomy as humans, with
4-chamber hearts and distinct left–right asymmetries that provide separate pulmonary systemic circulation required for oxygenation of blood. These structures are the major targets of CHD. Although knockout mice have yielded new insights into the genetic pathogenesis of CHD, the analysis is limited to one gene at a time. In comparison, forward genetic screens using ethylnitrosourea (ENU) mutagenesis can greatly accel-erate novel gene discovery. With ENU mutagenesis, every animal by design harbors many mutations. Thus, with focused phenotyping, gene discovery can proceed rapidly and without a priori gene bias. By conducting such screens in an inbred mouse strain background, the confounding effects of genetic heterogeneity could be minimized.1
We previously conducted a small-scale mouse forward genetic screen to recover CHD mutants using the Acuson clinical ultrasound system for noninvasive fetal echocardiog-raphy.2,3 Although echocardiography is the imaging modality of choice for diagnosing CHD, the poor imaging resolution of
Background—Congenital heart disease (CHD) has a multifactorial pathogenesis, but a genetic contribution is indicated by heritability studies. To investigate the spectrum of CHD with a genetic pathogenesis, we conducted a forward genetic screen in inbred mice using fetal echocardiography to recover mutants with CHD. Mice are ideally suited for these studies given that they have the same four-chamber cardiac anatomy that is the substrate for CHD.
Methods and Results—Ethylnitrosourea mutagenized mice were ultrasound-interrogated by fetal echocardiography using a clinical ultrasound system, and fetuses suspected to have cardiac abnormalities were further interrogated with an ultrahigh-frequency ultrasound biomicroscopy. Scanning of 46 270 fetuses revealed 1722 with cardiac anomalies, with 27.9% dying prenatally. Most of the structural heart defects can be diagnosed using ultrasound biomicroscopy but not with the clinical ultrasound system. Confirmation with analysis by necropsy and histopathology showed excellent diagnostic capability of ultrasound biomicroscopy for most CHDs. Ventricular septal defect was the most common CHD observed, whereas outflow tract and atrioventricular septal defects were the most prevalent complex CHD. Cardiac/visceral organ situs defects were observed at surprisingly high incidence. The rarest CHD found was hypoplastic left heart syndrome, a phenotype never seen in mice previously.
Conclusions—We developed a high-throughput, 2-tier ultrasound phenotyping strategy for efficient recovery of even rare CHD phenotypes, including the first mouse models of hypoplastic left heart syndrome. Our findings support a genetic pathogenesis for a wide spectrum of CHDs and suggest that the disruption of left–right patterning may play an important role in CHD. (Circ Cardiovasc Imaging. 2014;7:31-42.)
Key Words: heart defects, congenital ◼ microscopy, acoustic
© 2013 American Heart Association, Inc.
Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.113.000451
Received March 14, 2013; accepted November 27, 2013.From Department of Developmental Biology, University of Pittsburgh, Pittsburgh, PA (X.L., R.F., A.J.K., R.R., G.C., R.S., S.A., Y.K., L.W., K.T.,
C.W.L.); Genetic Resource Science, The Jackson Laboratory, Bar Harbor, ME (J.M., H.C.P., L.R.); Department of Pediatric Pathology, Children’s Hospital of Pittsburgh, Pittsburgh, PA (W.D.); and Children’s National Medical Center, Washington, DC (L.L.).
The Data Supplement is available at http://circimaging.ahajournals.org/lookup/suppl/doi:10.1161/CIRCIMAGING.113.000451/-/DC1.Correspondence to Cecilia W. Lo, 530 45th St, Pittsburgh, PA 15201. E-mail [email protected]
Interrogating Congenital Heart Defects With Noninvasive Fetal Echocardiography in a Mouse Forward Genetic Screen
Xiaoqin Liu, MD, PhD; Richard Francis, PhD; Andrew J. Kim, BS; Ricardo Ramirez, BS; Guozhen Chen, MD; Ramiah Subramanian, MD, PhD; Shane Anderton, BS; Youngsil Kim, BS;
Liyin Wong, BS; Judy Morgan, PhD; Herbert C. Pratt, PhD; Laura Reinholdt, PhD; William Devine, BS; Linda Leatherbury, MD; Kimimasa Tobita, MD; Cecilia W. Lo, PhD
Congenital Heart Disease
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
by guest on July 14, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
by guest on July 14, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
by guest on July 14, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
by guest on July 14, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
by guest on July 14, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
by guest on July 14, 2018
http://circimaging.ahajournals.org/
Dow
nloaded from
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
32 Circ Cardiovasc Imaging January 2014
the Acuson restricted the ultrasound assessments to analysis of hemodynamic function. As a result, specific CHD diagnosis could only be made after necropsy and histopathology exami-nation. Although CHD mutants were successfully recovered, these limitations compromised the efficacy of the screen, and some CHD phenotypes may be missed.
In this study, we incorporated the dual use of the Acuson and the Vevo2100 ultrahigh-frequency ultrasound biomicros-copy (UBM) for cardiovascular phenotyping to recover CHD mutants in a large-scale mouse mutagenesis screen. In con-trast to our previous study, the Vevo2100 with its much higher resolution allowed direct diagnosis of structural heart defects. We diagnosed a wide spectrum of CHDs and recovered the first mouse model of hypoplastic left heart syndrome (HLHS), a rare phenotype never seen in mice previously.
MethodsENU Mutagenesis and Mouse BreedingAll studies were conducted under an approved Institute Animal Care and Use Committee protocol of the University of Pittsburgh. C57BL/6J male mice were ENU-mutagenized as previously de-scribed with first generation(G)1 male mice backcrossed to 4 to 6 G2 daughters, and the resulting G3 fetuses were ultrasound-scanned in utero.2,3 All offsprings from one G1 male mouse were tracked as a distinct pedigree.
Ultrasound Imaging and Doppler EchocardiographyPregnant G2 dams were sedated with isoflurane and ultrasound-scanned using the Acuson Sequoia C512 with a 15-MHz transducer. Litters with abnormal fetuses were further scanned using the Vevo2100 UBM with a 40-MHz transducer for specific CHD diagnosis. The protocol used for ultrasound scanning, including the method for mapping the fetus position in utero, is described in the Methods section in the Data Supplement.
Necropsy, Microcomputed Tomography (Micro-CT)/Micromagnetic Resonance Imaging, and Histopathology ExaminationsFetuses or neonates were collected, fixed in 10% formalin, and then examined by necropsy, micro-CT or micromagnetic resonance im-aging, and episcopic fluorescence image capture (EFIC),4 a histo-pathology examination. EFIC served as the gold standard for CHD
diagnosis. All CHD diagnoses were reviewed by a panel of pediatric cardiologists and a pathologist (see the Data Supplement).
Efficacy of Ultrasound CHD DiagnosisThe efficacy of cardiovascular phenotyping with Acuson ver-sus Vevo2100 was assessed by χ2 analysis, with significance set at P<0.05. The positive and negative predictive values of Vevo2100 ul-trasound for CHD diagnosis were calculated as described in the Data Supplement. Statistical analysis was performed using SPSS 11.5 (SPSS Inc, Chicago, IL).
ResultsPregnant dams from ENU-mutagenized C57BL6/J mouse colony were ultrasound-scanned using the Acuson ultra-sound system equipped with a 15-MHz transducer. The large 2-dimensional imaging window (25×20 mm) provided direct visualization of multiple fetuses, whereas the small footprint of the transducer facilitated rapid scanning. This allowed quick determination of the total number of embryos in a litter and their relative orientation in the uterine horn. Together with the spectral Doppler/color flow imaging capa-bility, abnormal fetuses can be readily identified based on the finding of hemodynamic perturbation, hydrops, or growth restriction. The fewer litters with abnormal fetuses identi-fied were further interrogated in a second-tier analysis using the higher-resolution Vevo2100 (30 um axial×75 um lateral resolution versus Acuson’s 300–500 um resolution).5,6 The Vevo2100 has a much smaller imaging window (15×14 mm) that allows visualization of only one fetus at a time, but its ultrahigh 2-dimensional resolution equipped with the same color flow imaging capability as the Acuson5 allows direct diagnosis of structural heart defects.
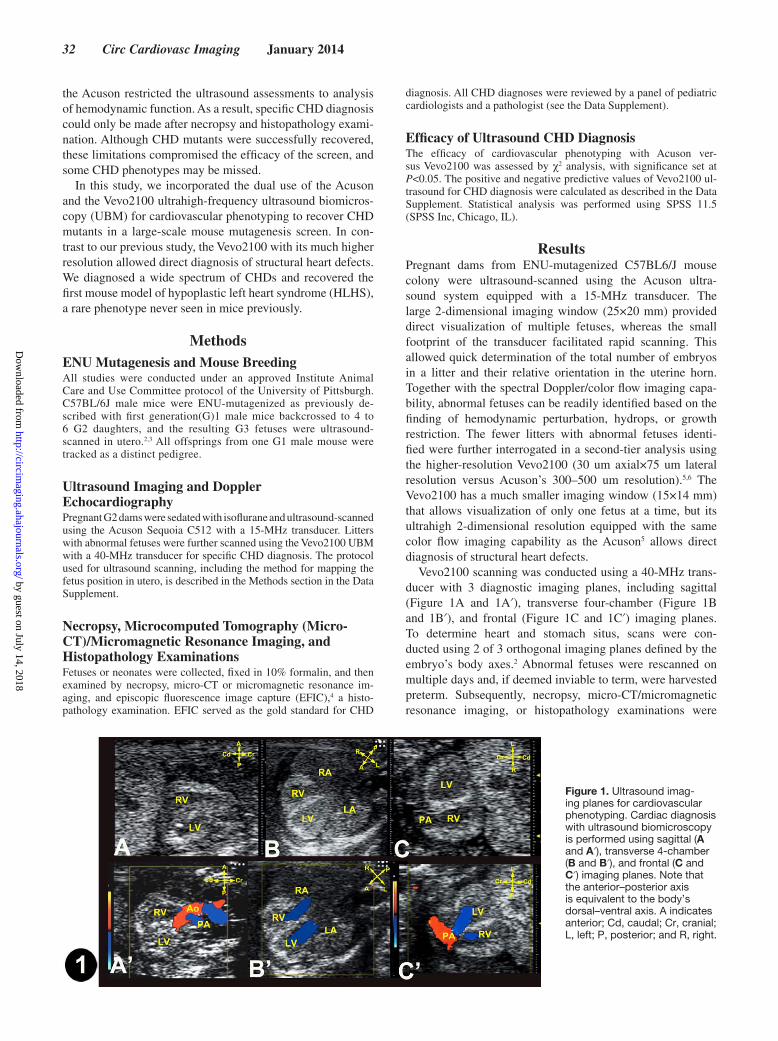
Vevo2100 scanning was conducted using a 40-MHz trans-ducer with 3 diagnostic imaging planes, including sagittal (Figure 1A and 1A′), transverse four-chamber (Figure 1B and 1B′), and frontal (Figure 1C and 1C′) imaging planes. To determine heart and stomach situs, scans were con-ducted using 2 of 3 orthogonal imaging planes defined by the embryo’s body axes.2 Abnormal fetuses were rescanned on multiple days and, if deemed inviable to term, were harvested preterm. Subsequently, necropsy, micro-CT/micromagnetic resonance imaging, or histopathology examinations were
Figure 1. Ultrasound imag-ing planes for cardiovascular phenotyping. Cardiac diagnosis with ultrasound biomicroscopy is performed using sagittal (A and A′), transverse 4-chamber (B and B′), and frontal (C and C′) imaging planes. Note that the anterior–posterior axis is equivalent to the body’s dorsal–ventral axis. A indicates anterior; Cd, caudal; Cr, cranial; L, left; P, posterior; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from

Liu et al Modeling Complex Congenital Heart Disease in Mice 33
used to confirm CHD diagnosis. Typically, scans with the Acuson had ultrasound examination time of 55±16 (standard deviation) seconds per fetus for normal fetuses (median, 52 seconds; range, 34–100 seconds, based on 68 litters with 434 normal fetuses) and 64±15 (standard deviation) seconds per fetus for abnormal fetuses (median, 61 seconds; range, 32–105 seconds, based on 57 litters with 107 abnormal fetuses). The second-tier interrogation of abnormal fetuses using the Vevo2100 had a much longer examination time of 1049±297 (standard deviation) seconds per fetus (median, 1035 seconds; range, 600–1500 seconds, based on 27 abnormal fetuses in 20 litters). Overall, 20 litters were ultrasound-scanned per day, with ≤15 minutes required for a litter of 6 to 8 fetuses and longer scan times for litters with abnormal fetuses.
Fetuses were scanned from embryonic day (E) 13.5 to E18.5, with a mean of E15.2±1.4 (standard deviation) and median of E15.5. Because ventricular chamber and outflow tract (OFT) septation are not completed until E13.5 to 14.5, scanning at E13.5 to 15.5 should minimize false-positive CHD diagnosis that might reflect developmental delay. Also problematic with earlier scans is echogenicity of blood in younger embryos (due to nucleated erythrocytes), making it difficult to visualize the endocardial lumen, detracting from the otherwise high UBM 2-dimensional spatial resolution. Given these considerations, our fetal ultrasound screening was predominantly conducted at E14.5 to E15.5, with earlier scans conducted if dead embryos were observed at E14.5 to E15.5 (Figure 2A–2D).
Prevalence of Developmental Anomalies Identified by Ultrasound PhenotypingUsing the 2-tier ultrasound phenotyping strategy, we screened 46 270 G3 fetuses from 1381 G1 pedigrees (August 2010 to March 2012). We identified 2590 abnor-mal fetuses exhibiting a spectrum of cardiac and noncar-diac defects (Table I and Figure I in the Data Supplement). Cardiac anomalies were found in 1722 fetuses (3.7%), which accounted for 66.5% of all developmental anomalies detected. In contrast, the incidences of extracardiac defects were much lower, ranging from 2% to 8% (Table I in the Data Supplement). These included craniofacial defects, limb anomalies, body wall closure defects, and laterality defects, including heterotaxy with discordant left–right heart and stomach positioning and situs inversus totalis (dextrocardia/dextrogastria; Table I in the Data Supplement).
Association of Prenatal Lethality and Growth Restriction With Cardiac DefectsThe majority of fetuses with severe cardiovascular defects were observed to expire between E15.5 and term, whereas <20% of deaths at E14.5 were associated with CHD (Fig-ure 2E). Cardiac anomalies were overall enriched in mutants with noncardiac defects (Table I in the Data Supplement). Thus, cardiac defects were found in 80.3% of mutants with body wall closure defects and 92.3% of mutants with het-erotaxy. Growth retardation was also highly associated with cardiac defects, with 88.7% of growth-restricted fetuses exhibiting cardiac defects. More than 25% of fetuses (481 of
Figure 2. Ultrasound detec-tion of prenatal lethality. A to D, Acuson (A) and Vevo2100 (B) imaging of an E13.5 fetus showed hydrops (arrowheads). Vevo2100 also showed atrio-ventricular septal defect (AVSD; arrowhead in C) with common valve regurgitation (C′, arrow-head). This fetus was found dead the next day (D). E, Pre-natal death with and without congenital heart disease (CHD) was detected by ultrasound screening. Scale bar, 1 mm. A indicates anterior; Cd, caudal; Cr, cranial; L, left; P, posterior; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from

34 Circ Cardiovasc Imaging January 2014
1722; 27.9%) with cardiac defects died prenatally, showing
the importance of prenatal screening. This included 15.1%
(260 of 1722) fetuses found dead with follow-up ultrasound
scans and 12.8% (221 of 1722) fetuses that were harvested
prenatally given pending death was indicated with ultrasound
presentations such as hydrops, pericardial effusion, dilated
heart with bradycardia/arrhythmia, or severe inflow or outflow
regurgitation (Figure 2A–2D; also see Movie IA–ID in the Data Supplement).
Recovery of a Wide Spectrum of Structural Heart DefectsA wide spectrum of CHDs was recovered from the ultra-sound screen (Table 1). This included cardiac septation defects, OFT defects, left or right heart obstructive lesions,
Table 1. Efficiency of Cardiovascular Phenotyping With Acuson Versus Vevo2100
Ultrasound Diagnosis Acuson* Vevo2100* P Value†
Abnormal echocardiography findings (n=1457)‡
Cardiac structural defects (n=352; 24%)
Septal defects 17 (4.8%) 241 (68.5%) <0.01
VSD 15 (4.3%) 176 (50%) <0.01
AVSD 2 (0.6%) 65 (18.5%) <0.01
Outflow tract defects 12 (3.4%) 127 (36.1%) <0.01
DORV/overriding aorta 9 (2.6%) 75 (21.3%) <0.01
With VSD 9 (2.6%) 57 (16.2%) <0.01
With AVSD 0 (0%) 18 (5.1%) <0.01
With pulmonary stenosis 0 (0%) 17 (4.8%) <0.01
PTA/PA 3 (0.9%) 38 (10.8%) <0.01
With VSD 3 (0.9%) 25 (7.1%) <0.01
With AVSD 0 (0%) 13 (3.7%) <0.01
TGA 0 (0%) 14 (4.0%) <0.01
With VSD 0 (0%) 13 (3.7%) <0.01
With AVSD 0 (0%) 1 (0.3%) 1.000
With pulmonary stenosis 0 (0%) 1 (0.3%) 1.000
Left heart obstruction lesions 7 (2.0%) 23 (6.5%) <0.01
Mitral atresia/stenosis 0 (0%) 8 (2.3%) <0.05
Aortic atresia/stenosis/coarctation 7 (2.0%) 15 (4.3%) 0.083
Hypoplastic left heart syndrome 0 (0%) 4 (1.1%) 0.133
Right heart obstruction lesions 10 (2.8%) 50 (12.2%) <0.01
Tricuspid atresia/hypoplasia 0 (0%) 15 (4.3%) <0.01
Pulmonary stenosis 10 (2.8%) 35 (9.9%) <0.01
Hypoplastic right heart syndrome 0 (0%) 11 (3.1%) <0.01
Coronary artery fistula 4 (1.1%) 8 (2.3%) 0.244
Cardiac situs anomalies 0 (0%) 40 (11.4%) <0.01
Dextrocardia 0 (0%) 34 (9.7%) <0.01
Mesocardia 0 (0%) 6 (1.7%) <0.05
Nonspecific abnormal findings (n=1105)
Total arrhythmia 262 262 1.000
Without structural defects 103 103 1.000
Total hydrops/pericardial effusion 598 635 0.113
Without structural defects 344 364 0.362
Total hemodynamic perturbations§ 1010 1030 0.110
Mild without structural defects 670 690 0.382
AVSD indicates atrioventricular septal defect; DORV, double outlet right ventricle; PTA, persistent truncus arteriosus; PA, pulmonary atresia; TGA, transposition of the great arteries; and VSD, ventricular septal defect.
*Values in parentheses represent percentage of affected fetuses among 352 fetuses identified as having congenital heart disease based on 2-tier ultrasound scanning.
†P values from χ2 analysis.‡1457 fetuses identified with cardiac defects by 2-tier ultrasound screening.§Hemodynamic pertubations including inflow tract and outflow tract increased velocity and regurgitation.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
Liu et al Modeling Complex Congenital Heart Disease in Mice 35
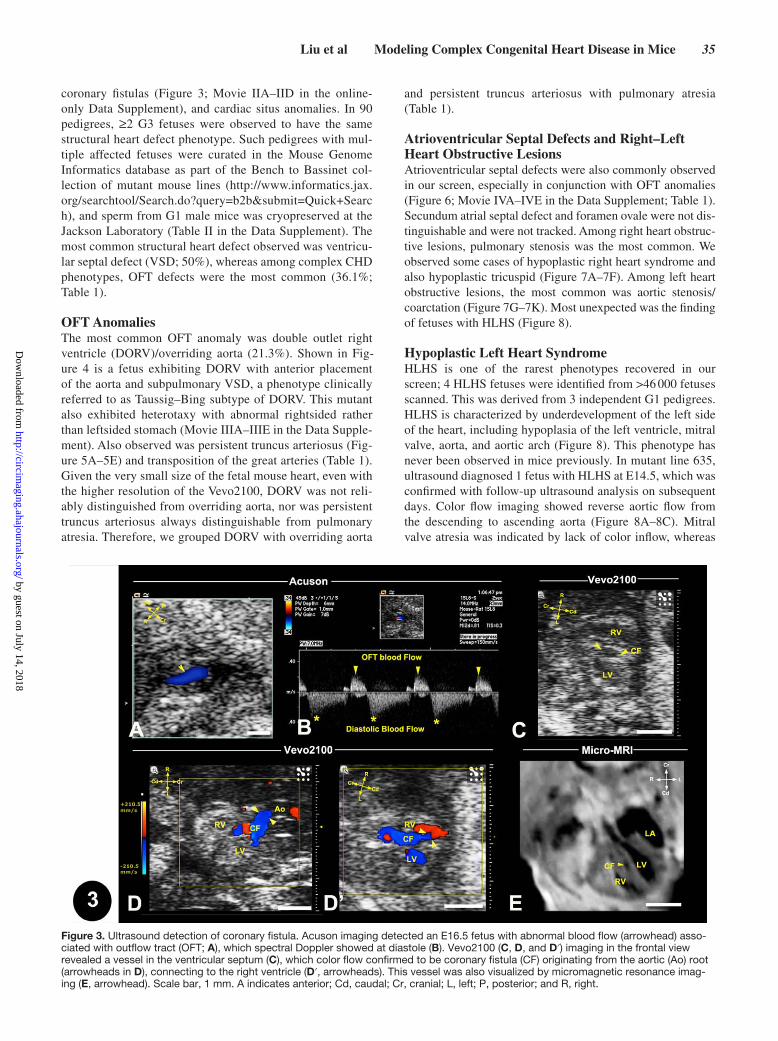
coronary fistulas (Figure 3; Movie IIA–IID in the online-only Data Supplement), and cardiac situs anomalies. In 90 pedigrees, ≥2 G3 fetuses were observed to have the same structural heart defect phenotype. Such pedigrees with mul-tiple affected fetuses were curated in the Mouse Genome Informatics database as part of the Bench to Bassinet col-lection of mutant mouse lines (http://www.informatics.jax.org/searchtool/Search.do?query=b2b&submit=Quick+Search), and sperm from G1 male mice was cryopreserved at the Jackson Laboratory (Table II in the Data Supplement). The most common structural heart defect observed was ventricu-lar septal defect (VSD; 50%), whereas among complex CHD phenotypes, OFT defects were the most common (36.1%; Table 1).
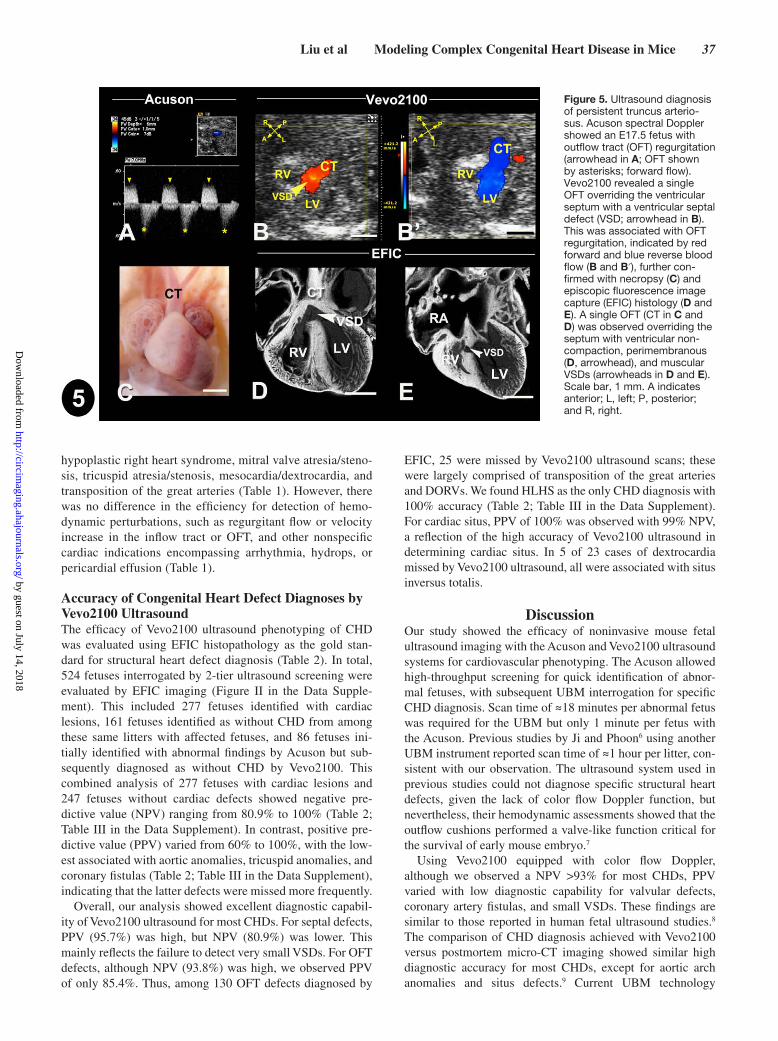
OFT AnomaliesThe most common OFT anomaly was double outlet right ventricle (DORV)/overriding aorta (21.3%). Shown in Fig-ure 4 is a fetus exhibiting DORV with anterior placement of the aorta and subpulmonary VSD, a phenotype clinically referred to as Taussig–Bing subtype of DORV. This mutant also exhibited heterotaxy with abnormal rightsided rather than leftsided stomach (Movie IIIA–IIIE in the Data Supple-ment). Also observed was persistent truncus arteriosus (Fig-ure 5A–5E) and transposition of the great arteries (Table 1). Given the very small size of the fetal mouse heart, even with the higher resolution of the Vevo2100, DORV was not reli-ably distinguished from overriding aorta, nor was persistent truncus arteriosus always distinguishable from pulmonary atresia. Therefore, we grouped DORV with overriding aorta
and persistent truncus arteriosus with pulmonary atresia (Table 1).
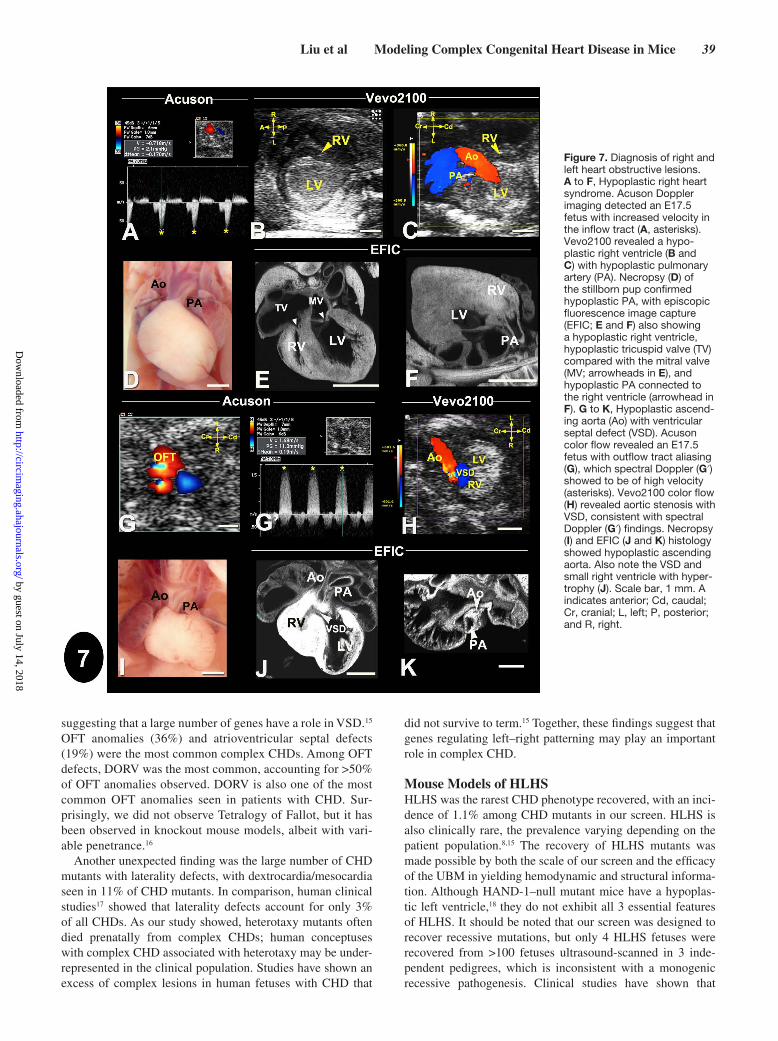
Atrioventricular Septal Defects and Right–Left Heart Obstructive LesionsAtrioventricular septal defects were also commonly observed in our screen, especially in conjunction with OFT anomalies (Figure 6; Movie IVA–IVE in the Data Supplement; Table 1). Secundum atrial septal defect and foramen ovale were not dis-tinguishable and were not tracked. Among right heart obstruc-tive lesions, pulmonary stenosis was the most common. We observed some cases of hypoplastic right heart syndrome and also hypoplastic tricuspid (Figure 7A–7F). Among left heart obstructive lesions, the most common was aortic stenosis/coarctation (Figure 7G–7K). Most unexpected was the finding of fetuses with HLHS (Figure 8).
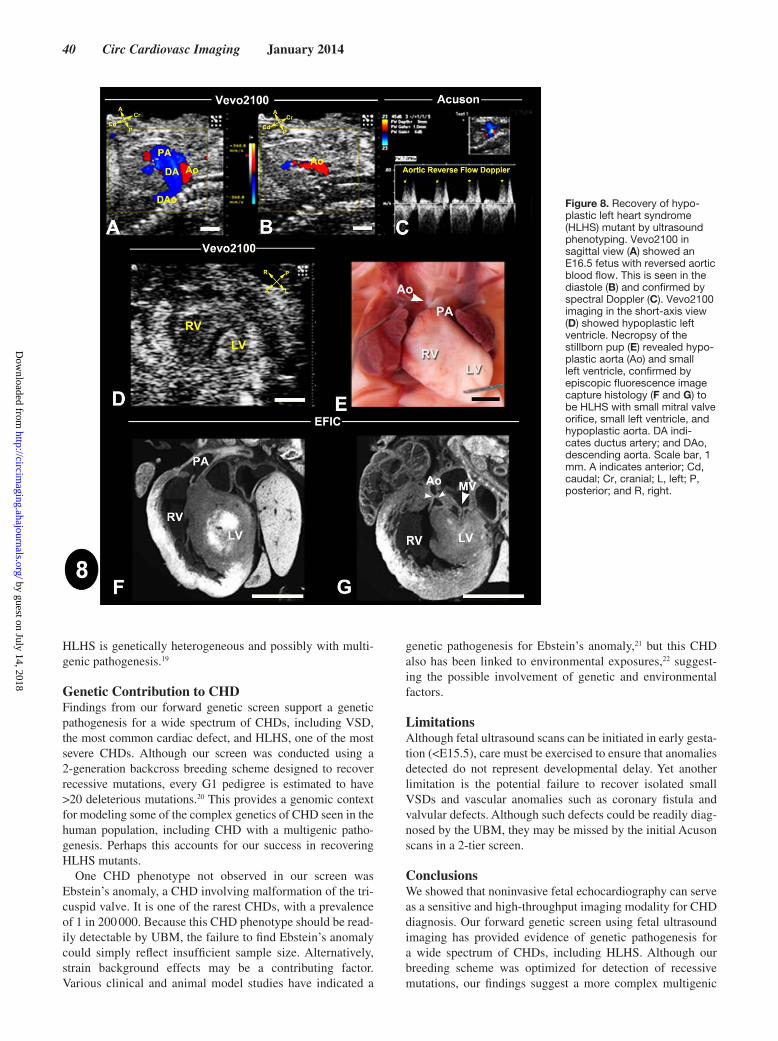
Hypoplastic Left Heart SyndromeHLHS is one of the rarest phenotypes recovered in our screen; 4 HLHS fetuses were identified from >46 000 fetuses scanned. This was derived from 3 independent G1 pedigrees. HLHS is characterized by underdevelopment of the left side of the heart, including hypoplasia of the left ventricle, mitral valve, aorta, and aortic arch (Figure 8). This phenotype has never been observed in mice previously. In mutant line 635, ultrasound diagnosed 1 fetus with HLHS at E14.5, which was confirmed with follow-up ultrasound analysis on subsequent days. Color flow imaging showed reverse aortic flow from the descending to ascending aorta (Figure 8A–8C). Mitral valve atresia was indicated by lack of color inflow, whereas
Figure 3. Ultrasound detection of coronary fistula. Acuson imaging detected an E16.5 fetus with abnormal blood flow (arrowhead) asso-ciated with outflow tract (OFT; A), which spectral Doppler showed at diastole (B). Vevo2100 (C, D, and D′) imaging in the frontal view revealed a vessel in the ventricular septum (C), which color flow confirmed to be coronary fistula (CF) originating from the aortic (Ao) root (arrowheads in D), connecting to the right ventricle (D′, arrowheads). This vessel was also visualized by micromagnetic resonance imag-ing (E, arrowhead). Scale bar, 1 mm. A indicates anterior; Cd, caudal; Cr, cranial; L, left; P, posterior; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from

36 Circ Cardiovasc Imaging January 2014
2-dimensional imaging showed a very small left ventricle with little or no lumen (Figure 8D). This mutant was still-born, and necropsy revealed hypoplastic ascending aorta (Figure 8E), with subsequent EFIC histopathology show-ing small left ventricle with almost no lumen, hypoplastic ascending aorta, and hypoplastic mitral valve. These findings together confirmed the ultrasound diagnosis of HLHS (Fig-ure 8F and 8G; Movie IVA–IVC in the Data Supplement). Heritability of the HLHS phenotype was demonstrated in this mutant line with the recovery of 2 HLHS mutants from 62 offsprings screened. In the other 2 mutant lines, only a single HLHS fetus was found among 18 and 29 offsprings inter-rogated, respectively. Given the rarity of HLHS, all 3 HLHS mutant lines were curated in Mouse Genome Informatics and sperm was cryopreserved at the Jackson Laboratory.
Congenital Heart Defects Associated With Laterality DefectsBecause visceral organ situs can be determined by ultra-sound phenotyping with the Vevo2100, we assessed situs anomalies as part of the routine CHD phenotyping workflow.
Surprisingly, more than half (49 of 90) of the mutant lines with CHD exhibited laterality defects (Table II in the online-only Data Supplement). This included fetuses with situs inver-sus totalis with mirror symmetrical visceral organ situs, and heterotaxy with randomized visceral organ situs. Nearly all heterotaxy mutants had complex CHD, which was readily detected by echocardiography (see example in Figure 4). In contrast, mutants exhibiting situs inversus totalis generally did not have CHD, although some had VSDs.
Efficacy of Congenital Heart Defect Diagnosis With UBM Versus AcusonWe compared the efficacy of the Acuson versus the UBM in CHD diagnosis by examining the ultrasound findings obtained in 1457 abnormal fetuses using both ultrasound systems (Table 1). UBM was significantly better in detecting structural heart anomalies, such as septal defects (P<0.01), OFT defects (P<0.01), left heart obstructive lesions (P<0.01), right heart obstructive lesions (P<0.01), and cardiac situs anomaly (P<0.01). We noted that some structural heart defects were only detected with the UBM, including HLHS,
Figure 4. Ultrasound diagnosis of heterotaxy with Taussig–Bing double outlet right ventricle. Acuson imaging (A, B, and B′) showed an E15.5 fetus with hydrops (arrowheads) and outflow tract regurgitation (OFT R). Vevo2100 imaging (C and C′) showed heterotaxy with heart apex on left (C, arrowhead) and stomach to right (S in C′), which was confirmed by necropsy (F). Vevo2100 (D and E) and episcopic fluorescence image capture (EFIC; G and H) showed aorta (Ao) anterior and pulmonary artery (PA) posterior with both outflows connected to the right ven-tricle (D, G, and E), with large ventricular septal defect (VSD; E and H). Scale bar, 1 mm. InnA indicates innominate artery; L, left; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
Liu et al Modeling Complex Congenital Heart Disease in Mice 37
hypoplastic right heart syndrome, mitral valve atresia/steno-sis, tricuspid atresia/stenosis, mesocardia/dextrocardia, and transposition of the great arteries (Table 1). However, there was no difference in the efficiency for detection of hemo-dynamic perturbations, such as regurgitant flow or velocity increase in the inflow tract or OFT, and other nonspecific cardiac indications encompassing arrhythmia, hydrops, or pericardial effusion (Table 1).
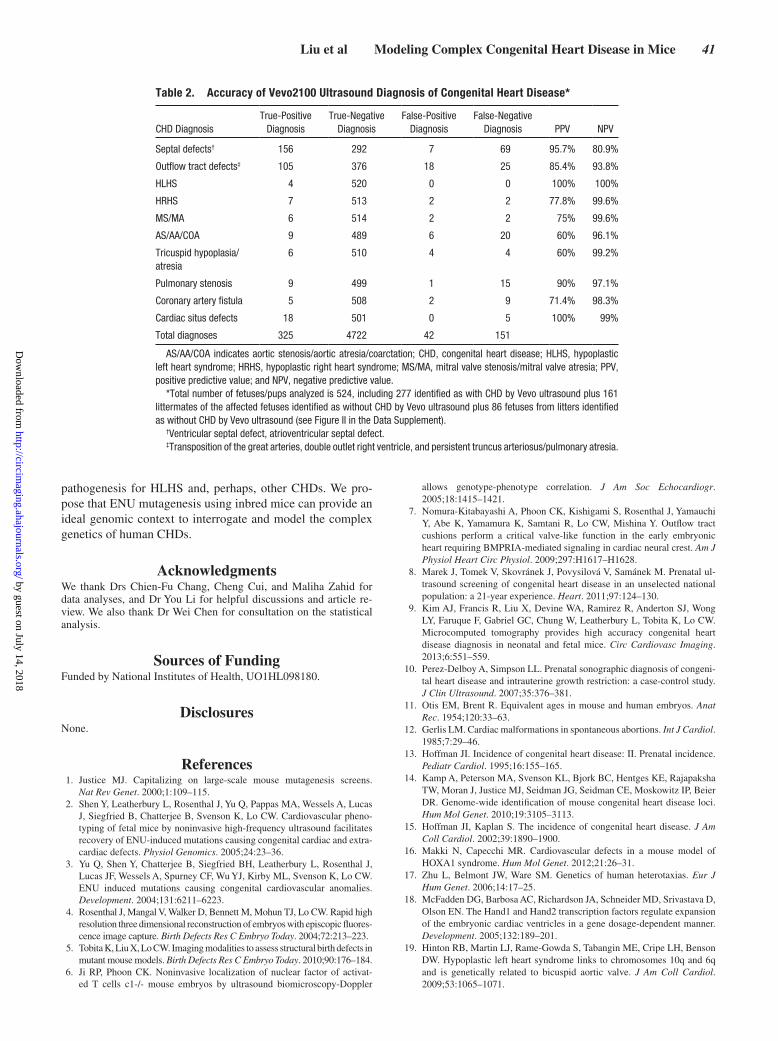
Accuracy of Congenital Heart Defect Diagnoses by Vevo2100 UltrasoundThe efficacy of Vevo2100 ultrasound phenotyping of CHD was evaluated using EFIC histopathology as the gold stan-dard for structural heart defect diagnosis (Table 2). In total, 524 fetuses interrogated by 2-tier ultrasound screening were evaluated by EFIC imaging (Figure II in the Data Supple-ment). This included 277 fetuses identified with cardiac lesions, 161 fetuses identified as without CHD from among these same litters with affected fetuses, and 86 fetuses ini-tially identified with abnormal findings by Acuson but sub-sequently diagnosed as without CHD by Vevo2100. This combined analysis of 277 fetuses with cardiac lesions and 247 fetuses without cardiac defects showed negative pre-dictive value (NPV) ranging from 80.9% to 100% (Table 2; Table III in the Data Supplement). In contrast, positive pre-dictive value (PPV) varied from 60% to 100%, with the low-est associated with aortic anomalies, tricuspid anomalies, and coronary fistulas (Table 2; Table III in the Data Supplement), indicating that the latter defects were missed more frequently.
Overall, our analysis showed excellent diagnostic capabil-ity of Vevo2100 ultrasound for most CHDs. For septal defects, PPV (95.7%) was high, but NPV (80.9%) was lower. This mainly reflects the failure to detect very small VSDs. For OFT defects, although NPV (93.8%) was high, we observed PPV of only 85.4%. Thus, among 130 OFT defects diagnosed by
EFIC, 25 were missed by Vevo2100 ultrasound scans; these were largely comprised of transposition of the great arteries and DORVs. We found HLHS as the only CHD diagnosis with 100% accuracy (Table 2; Table III in the Data Supplement). For cardiac situs, PPV of 100% was observed with 99% NPV, a reflection of the high accuracy of Vevo2100 ultrasound in determining cardiac situs. In 5 of 23 cases of dextrocardia missed by Vevo2100 ultrasound, all were associated with situs inversus totalis.
DiscussionOur study showed the efficacy of noninvasive mouse fetal ultrasound imaging with the Acuson and Vevo2100 ultrasound systems for cardiovascular phenotyping. The Acuson allowed high-throughput screening for quick identification of abnor-mal fetuses, with subsequent UBM interrogation for specific CHD diagnosis. Scan time of ≈18 minutes per abnormal fetus was required for the UBM but only 1 minute per fetus with the Acuson. Previous studies by Ji and Phoon6 using another UBM instrument reported scan time of ≈1 hour per litter, con-sistent with our observation. The ultrasound system used in previous studies could not diagnose specific structural heart defects, given the lack of color flow Doppler function, but nevertheless, their hemodynamic assessments showed that the outflow cushions performed a valve-like function critical for the survival of early mouse embryo.7
Using Vevo2100 equipped with color flow Doppler, although we observed a NPV >93% for most CHDs, PPV varied with low diagnostic capability for valvular defects, coronary artery fistulas, and small VSDs. These findings are similar to those reported in human fetal ultrasound studies.8 The comparison of CHD diagnosis achieved with Vevo2100 versus postmortem micro-CT imaging showed similar high diagnostic accuracy for most CHDs, except for aortic arch anomalies and situs defects.9 Current UBM technology
Figure 5. Ultrasound diagnosis of persistent truncus arterio-sus. Acuson spectral Doppler showed an E17.5 fetus with outflow tract (OFT) regurgitation (arrowhead in A; OFT shown by asterisks; forward flow). Vevo2100 revealed a single OFT overriding the ventricular septum with a ventricular septal defect (VSD; arrowhead in B). This was associated with OFT regurgitation, indicated by red forward and blue reverse blood flow (B and B′), further con-firmed with necropsy (C) and episcopic fluorescence image capture (EFIC) histology (D and E). A single OFT (CT in C and D) was observed overriding the septum with ventricular non-compaction, perimembranous (D, arrowhead), and muscular VSDs (arrowheads in D and E). Scale bar, 1 mm. A indicates anterior; L, left; P, posterior; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from

38 Circ Cardiovasc Imaging January 2014
cannot visualize the small aortic arch vessels, but these can be detected by contrast-enhanced micro-CT.9 Micro-CT also gave high accuracy in the detection of situs anomalies because the animal’s left–right axis can be predictably fixed during CT scanning.9 In contrast, fetus orientation in utero during ultra-sound scanning may be highly variable.
Recovery of CHD Mutants by Fetal Ultrasound PhenotypingOur screen encompassing >46 000 fetuses is one of the larg-est CHD screens to date. We observed a 3.7% incidence of cardiac defects and curated and cryopreserved >90 mutant mouse lines with CHD. We observed that CHD is highly associated with growth retardation and extracardiac anoma-lies. This is consistent with clinical studies showing intra-uterine growth restriction as a significant risk factor for CHD10 and the report that CHD is linked with chromosomal abnormalities, suboptimal growth, and extracardiac mal-formations.10 We found that >25% of fetuses with cardiac defects died prenatally, with many expiring between E15.5 and E16.5, equivalent to 8- to 12-week gestation in human embryos.11 Interestingly, clinical studies have shown higher
fetal death associated with CHD in human fetuses <15 weeks and an overall increase in CHD incidence in fetuses dying before term.8,12,13
With fetal ultrasound imaging, we recovered at-risk fetuses that would otherwise be missed in a postnatal screen. Moreover, with the identification of fetuses with CHD by ultrasound, we could exercise more caution in recovering stillborn pups, which might otherwise be cannibalized by the mother. We note another study, in which CHD mutants were screened with postnatal collection of stillborn pups, followed by phenotyping using histopathology in a mouse mutagen-esis screen.14 Although CHD mutants can be recovered in this manner, such screen is not high throughput, and a significant fraction of CHD mutants would be missed. Our analysis of stillborn pups showed that only 13% had CHD, most of which were isolated VSDs (unpublished observations).
Wide Spectrum of CHD Recovered From the Mutagenesis ScreenThe most prevalent cardiac defect found was VSD, observed in 50% of CHD mutants, half of which were isolated VSDs. VSD is also the most common CHD observed clinically,
Figure 6. Diagnosis of double outlet right ventricle with hypoplastic pulmonary artery (PA) and atrioventricular septal defect. Acuson imaging detected an E16.5 fetus with outflow tract regurgitation (OFT R in A). Vevo2100 imaging (B and B′) revealed a RV–LV shunt, indi-cating a ventricular septal defect (VSD; arrowheads in B). Vevo2100 imaging in the transverse view (C and C′) showed inflow tract forward (C, arrow) and regurgitant (C′, arrow) flow, whereas the sagittal view (D) showed that the majority of the aorta (Ao) connects to the right ventricle with an adjacent small vessel (arrowhead, PA) and a VSD. Necropsy (E) and episcopic fluorescence image capture (EFIC) histol-ogy (F and G) revealed a hypoplastic PA (E–G) and large VSD (G, arrowhead). A common atrioventricular valve (CV in F) was observed in the transverse view (F). CVF indicates common atrioventricular valve forward flow; and CVR, common atrioventricular valve reverse flow. Scale bar, 1 mm. A indicates anterior; Cd, caudal; Cr, cranial; L, left; P, posterior; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
Liu et al Modeling Complex Congenital Heart Disease in Mice 39
suggesting that a large number of genes have a role in VSD.15 OFT anomalies (36%) and atrioventricular septal defects (19%) were the most common complex CHDs. Among OFT defects, DORV was the most common, accounting for >50% of OFT anomalies observed. DORV is also one of the most common OFT anomalies seen in patients with CHD. Sur-prisingly, we did not observe Tetralogy of Fallot, but it has been observed in knockout mouse models, albeit with vari-able penetrance.16
Another unexpected finding was the large number of CHD mutants with laterality defects, with dextrocardia/mesocardia seen in 11% of CHD mutants. In comparison, human clinical studies17 showed that laterality defects account for only 3% of all CHDs. As our study showed, heterotaxy mutants often died prenatally from complex CHDs; human conceptuses with complex CHD associated with heterotaxy may be under-represented in the clinical population. Studies have shown an excess of complex lesions in human fetuses with CHD that
did not survive to term.15 Together, these findings suggest that genes regulating left–right patterning may play an important role in complex CHD.
Mouse Models of HLHSHLHS was the rarest CHD phenotype recovered, with an inci-dence of 1.1% among CHD mutants in our screen. HLHS is also clinically rare, the prevalence varying depending on the patient population.8,15 The recovery of HLHS mutants was made possible by both the scale of our screen and the efficacy of the UBM in yielding hemodynamic and structural informa-tion. Although HAND-1–null mutant mice have a hypoplas-tic left ventricle,18 they do not exhibit all 3 essential features of HLHS. It should be noted that our screen was designed to recover recessive mutations, but only 4 HLHS fetuses were recovered from >100 fetuses ultrasound-scanned in 3 inde-pendent pedigrees, which is inconsistent with a monogenic recessive pathogenesis. Clinical studies have shown that
Figure 7. Diagnosis of right and left heart obstructive lesions. A to F, Hypoplastic right heart syndrome. Acuson Doppler imaging detected an E17.5 fetus with increased velocity in the inflow tract (A, asterisks). Vevo2100 revealed a hypo-plastic right ventricle (B and C) with hypoplastic pulmonary artery (PA). Necropsy (D) of the stillborn pup confirmed hypoplastic PA, with episcopic fluorescence image capture (EFIC; E and F) also showing a hypoplastic right ventricle, hypoplastic tricuspid valve (TV) compared with the mitral valve (MV; arrowheads in E), and hypoplastic PA connected to the right ventricle (arrowhead in F). G to K, Hypoplastic ascend-ing aorta (Ao) with ventricular septal defect (VSD). Acuson color flow revealed an E17.5 fetus with outflow tract aliasing (G), which spectral Doppler (G′) showed to be of high velocity (asterisks). Vevo2100 color flow (H) revealed aortic stenosis with VSD, consistent with spectral Doppler (G′) findings. Necropsy (I) and EFIC (J and K) histology showed hypoplastic ascending aorta. Also note the VSD and small right ventricle with hyper-trophy (J). Scale bar, 1 mm. A indicates anterior; Cd, caudal; Cr, cranial; L, left; P, posterior; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
40 Circ Cardiovasc Imaging January 2014
HLHS is genetically heterogeneous and possibly with multi-genic pathogenesis.19
Genetic Contribution to CHDFindings from our forward genetic screen support a genetic pathogenesis for a wide spectrum of CHDs, including VSD, the most common cardiac defect, and HLHS, one of the most severe CHDs. Although our screen was conducted using a 2-generation backcross breeding scheme designed to recover recessive mutations, every G1 pedigree is estimated to have >20 deleterious mutations.20 This provides a genomic context for modeling some of the complex genetics of CHD seen in the human population, including CHD with a multigenic patho-genesis. Perhaps this accounts for our success in recovering HLHS mutants.
One CHD phenotype not observed in our screen was Ebstein’s anomaly, a CHD involving malformation of the tri-cuspid valve. It is one of the rarest CHDs, with a prevalence of 1 in 200 000. Because this CHD phenotype should be read-ily detectable by UBM, the failure to find Ebstein’s anomaly could simply reflect insufficient sample size. Alternatively, strain background effects may be a contributing factor. Various clinical and animal model studies have indicated a
genetic pathogenesis for Ebstein’s anomaly,21 but this CHD also has been linked to environmental exposures,22 suggest-ing the possible involvement of genetic and environmental factors.
LimitationsAlthough fetal ultrasound scans can be initiated in early gesta-tion (<E15.5), care must be exercised to ensure that anomalies detected do not represent developmental delay. Yet another limitation is the potential failure to recover isolated small VSDs and vascular anomalies such as coronary fistula and valvular defects. Although such defects could be readily diag-nosed by the UBM, they may be missed by the initial Acuson scans in a 2-tier screen.
ConclusionsWe showed that noninvasive fetal echocardiography can serve as a sensitive and high-throughput imaging modality for CHD diagnosis. Our forward genetic screen using fetal ultrasound imaging has provided evidence of genetic pathogenesis for a wide spectrum of CHDs, including HLHS. Although our breeding scheme was optimized for detection of recessive mutations, our findings suggest a more complex multigenic
Figure 8. Recovery of hypo-plastic left heart syndrome (HLHS) mutant by ultrasound phenotyping. Vevo2100 in sagittal view (A) showed an E16.5 fetus with reversed aortic blood flow. This is seen in the diastole (B) and confirmed by spectral Doppler (C). Vevo2100 imaging in the short-axis view (D) showed hypoplastic left ventricle. Necropsy of the stillborn pup (E) revealed hypo-plastic aorta (Ao) and small left ventricle, confirmed by episcopic fluorescence image capture histology (F and G) to be HLHS with small mitral valve orifice, small left ventricle, and hypoplastic aorta. DA indi-cates ductus artery; and DAo, descending aorta. Scale bar, 1 mm. A indicates anterior; Cd, caudal; Cr, cranial; L, left; P, posterior; and R, right.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
Liu et al Modeling Complex Congenital Heart Disease in Mice 41
pathogenesis for HLHS and, perhaps, other CHDs. We pro-pose that ENU mutagenesis using inbred mice can provide an ideal genomic context to interrogate and model the complex genetics of human CHDs.
AcknowledgmentsWe thank Drs Chien-Fu Chang, Cheng Cui, and Maliha Zahid for data analyses, and Dr You Li for helpful discussions and article re-view. We also thank Dr Wei Chen for consultation on the statistical analysis.
Sources of FundingFunded by National Institutes of Health, UO1HL098180.
DisclosuresNone.
References 1. Justice MJ. Capitalizing on large-scale mouse mutagenesis screens.
Nat Rev Genet. 2000;1:109–115. 2. Shen Y, Leatherbury L, Rosenthal J, Yu Q, Pappas MA, Wessels A, Lucas
J, Siegfried B, Chatterjee B, Svenson K, Lo CW. Cardiovascular pheno-typing of fetal mice by noninvasive high-frequency ultrasound facilitates recovery of ENU-induced mutations causing congenital cardiac and extra-cardiac defects. Physiol Genomics. 2005;24:23–36.
3. Yu Q, Shen Y, Chatterjee B, Siegfried BH, Leatherbury L, Rosenthal J, Lucas JF, Wessels A, Spurney CF, Wu YJ, Kirby ML, Svenson K, Lo CW. ENU induced mutations causing congenital cardiovascular anomalies. Development. 2004;131:6211–6223.
4. Rosenthal J, Mangal V, Walker D, Bennett M, Mohun TJ, Lo CW. Rapid high resolution three dimensional reconstruction of embryos with episcopic fluores-cence image capture. Birth Defects Res C Embryo Today. 2004;72:213–223.
5. Tobita K, Liu X, Lo CW. Imaging modalities to assess structural birth defects in mutant mouse models. Birth Defects Res C Embryo Today. 2010;90:176–184.
6. Ji RP, Phoon CK. Noninvasive localization of nuclear factor of activat-ed T cells c1-/- mouse embryos by ultrasound biomicroscopy-Doppler
allows genotype-phenotype correlation. J Am Soc Echocardiogr. 2005;18:1415–1421.
7. Nomura-Kitabayashi A, Phoon CK, Kishigami S, Rosenthal J, Yamauchi Y, Abe K, Yamamura K, Samtani R, Lo CW, Mishina Y. Outflow tract cushions perform a critical valve-like function in the early embryonic heart requiring BMPRIA-mediated signaling in cardiac neural crest. Am J Physiol Heart Circ Physiol. 2009;297:H1617–H1628.
8. Marek J, Tomek V, Skovránek J, Povysilová V, Samánek M. Prenatal ul-trasound screening of congenital heart disease in an unselected national population: a 21-year experience. Heart. 2011;97:124–130.
9. Kim AJ, Francis R, Liu X, Devine WA, Ramirez R, Anderton SJ, Wong LY, Faruque F, Gabriel GC, Chung W, Leatherbury L, Tobita K, Lo CW. Microcomputed tomography provides high accuracy congenital heart disease diagnosis in neonatal and fetal mice. Circ Cardiovasc Imaging. 2013;6:551–559.
10. Perez-Delboy A, Simpson LL. Prenatal sonographic diagnosis of congeni-tal heart disease and intrauterine growth restriction: a case-control study. J Clin Ultrasound. 2007;35:376–381.
11. Otis EM, Brent R. Equivalent ages in mouse and human embryos. Anat Rec. 1954;120:33–63.
12. Gerlis LM. Cardiac malformations in spontaneous abortions. Int J Cardiol. 1985;7:29–46.
13. Hoffman JI. Incidence of congenital heart disease: II. Prenatal incidence. Pediatr Cardiol. 1995;16:155–165.
14. Kamp A, Peterson MA, Svenson KL, Bjork BC, Hentges KE, Rajapaksha TW, Moran J, Justice MJ, Seidman JG, Seidman CE, Moskowitz IP, Beier DR. Genome-wide identification of mouse congenital heart disease loci. Hum Mol Genet. 2010;19:3105–3113.
15. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–1900.
16. Makki N, Capecchi MR. Cardiovascular defects in a mouse model of HOXA1 syndrome. Hum Mol Genet. 2012;21:26–31.
17. Zhu L, Belmont JW, Ware SM. Genetics of human heterotaxias. Eur J Hum Genet. 2006;14:17–25.
18. McFadden DG, Barbosa AC, Richardson JA, Schneider MD, Srivastava D, Olson EN. The Hand1 and Hand2 transcription factors regulate expansion of the embryonic cardiac ventricles in a gene dosage-dependent manner. Development. 2005;132:189–201.
19. Hinton RB, Martin LJ, Rame-Gowda S, Tabangin ME, Cripe LH, Benson DW. Hypoplastic left heart syndrome links to chromosomes 10q and 6q and is genetically related to bicuspid aortic valve. J Am Coll Cardiol. 2009;53:1065–1071.
Table 2. Accuracy of Vevo2100 Ultrasound Diagnosis of Congenital Heart Disease*
CHD DiagnosisTrue-Positive
DiagnosisTrue-Negative
DiagnosisFalse-Positive
DiagnosisFalse-Negative
Diagnosis PPV NPV
Septal defects† 156 292 7 69 95.7% 80.9%
Outflow tract defects‡ 105 376 18 25 85.4% 93.8%
HLHS 4 520 0 0 100% 100%
HRHS 7 513 2 2 77.8% 99.6%
MS/MA 6 514 2 2 75% 99.6%
AS/AA/COA 9 489 6 20 60% 96.1%
Tricuspid hypoplasia/ atresia
6 510 4 4 60% 99.2%
Pulmonary stenosis 9 499 1 15 90% 97.1%
Coronary artery fistula 5 508 2 9 71.4% 98.3%
Cardiac situs defects 18 501 0 5 100% 99%
Total diagnoses 325 4722 42 151
AS/AA/COA indicates aortic stenosis/aortic atresia/coarctation; CHD, congenital heart disease; HLHS, hypoplastic left heart syndrome; HRHS, hypoplastic right heart syndrome; MS/MA, mitral valve stenosis/mitral valve atresia; PPV, positive predictive value; and NPV, negative predictive value.
*Total number of fetuses/pups analyzed is 524, including 277 identified as with CHD by Vevo ultrasound plus 161 littermates of the affected fetuses identified as without CHD by Vevo ultrasound plus 86 fetuses from litters identified as without CHD by Vevo ultrasound (see Figure II in the Data Supplement).
†Ventricular septal defect, atrioventricular septal defect. ‡Transposition of the great arteries, double outlet right ventricle, and persistent truncus arteriosus/pulmonary atresia.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from

42 Circ Cardiovasc Imaging January 2014
20. Balling R. ENU mutagenesis: analyzing gene function in mice. Annu Rev Genomics Hum Genet. 2001;2:463–492.
21. Digilio MC, Bernardini L, Lepri F, Giuffrida MG, Guida V, Baban A, Versacci P, Capolino R, Torres B, De Luca A, Novelli A, Marino B, Dallapiccola B. Ebstein anomaly: genetic heterogeneity and
association with microdeletions 1p36 and 8p23.1. Am J Med Genet A. 2011;155A:2196–2202.
22. Lupo PJ, Langlois PH, Mitchell LE. Epidemiology of Ebstein anom-aly: prevalence and patterns in Texas, 1999-2005. Am J Med Genet A. 2011;155A:1007–1014.
CLINICAL PERSPECTIVECongenital heart disease (CHD) is one of the most common birth defects. Investigations into the genetic pathogenesis of CHD have been challenging given the sporadic nature and variable penetrance and expressivity of CHD. Further compli-cations come from indications that environmental factors also contribute to CHD. To interrogate the genetic pathogen-esis of CHD, we undertook a forward genetic screen in chemically mutagenized C57BL6 inbred mice to recover CHD mutants. A 2-tier ultrasound screening protocol was developed involving initial scans using the Acuson clinical ultrasound system to identify fetuses with cardiac defects, followed by detailed scans of abnormal fetuses for CHD diagnosis using the ultrahigh-frequency Vevo2100 ultrasound biomicroscopy. We scanned 46 270 fetuses and identified 1722 with cardiac defects, >25% of which died prenatally. A wide spectrum of CHDs was observed, most of which could be diagnosed using Vevo2100 but not with Acuson. The confirmation of CHD diagnosis by necropsy and histopathology showed excellent diagnostic capability of ultrasound biomicroscopy for most CHDs. Ventricular septal defect was the most common CHD observed, whereas outflow tract and atrioventricular septal defects were the most prevalent complex CHD. Laterality defects including heterotaxy were observed at surprisingly high incidence. The rarest CHD found was hypoplastic left heart syn-drome, a phenotype never seen in mice previously. Our findings support a genetic pathogenesis for a wide spectrum of CHDs and suggest that mouse fetal echocardiography together with forward genetic screens can be used to interrogate and model the complex genetics of human CHD.
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
Laura Reinholdt, William Devine, Linda Leatherbury, Kimimasa Tobita and Cecilia W. LoSubramanian, Shane Anderton, Youngsil Kim, Liyin Wong, Judy Morgan, Herbert C. Pratt, Xiaoqin Liu, Richard Francis, Andrew J. Kim, Ricardo Ramirez, Guozhen Chen, Ramiah
Mouse Forward Genetic ScreenInterrogating Congenital Heart Defects With Noninvasive Fetal Echocardiography in a
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.113.0004512014;7:31-42; originally published online December 6, 2013;Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/7/1/31World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org/content/suppl/2013/12/06/CIRCIMAGING.113.000451.DC1Data Supplement (unedited) at:
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 14, 2018http://circim
aging.ahajournals.org/D
ownloaded from
1
SUPPLEMENTAL MATERIAL
SUPPLEMENTAL METHODS
SUPPLEMENTAL TABLES Supplemental Table S1 Supplemental Table S2 Supplemental Table S3
SUPPLEMENTAL FIGURES Supplemental Figure S1 Supplemental Figure S2
SUPPLEMENTAL REFERENCES
SUPPLEMENTAL VIDEO LEGENDS Video Legend 1A-D. Video Legend 2A-D. Video Legend 3A-E. Video Legend 4A-E. Video Legend 5A-C.

2
SUPPLEMENTAL METHODS Ultrasound Imaging and Doppler Echocardiography
When fetal ultrasound was performed, the mother’s bladder was used as an anatomic
landmark to locate fetuses proximally from the cervix to more distally in the uterine horn on
the left as L1,2,3, etc., and on the right as R1,2,3, etc. The imaging modalities used included
B-mode imaging, and color flow and spectral Doppler, and M-mode imaging as previously
described1,2. The initial Acuson scan was used to determinate litter size, orientation of fetuses
and developmental staging of the fetuses with crown to rump length and fetus area
measurements. Crown-to-rump length of fetus > two standard deviations below the mean
compared to age-matched normal fetuses were considered growth restricted3.
Analysis of Positive and Negative Predictive Value with Vevo2100 Ultrasound Imaging
Fetuses examined by the Acuson-Vevo2100 two-tier ultrasound screen were subsequently
analyzed by EFIC histology as the gold standard for CHD diagnosis. This included fetuses
that were Vevo ultrasound diagnosed with CHD, fetuses Vevo ultrasound diagnosed as
without CHD from the same litters with fetuses Vevo diagnosed with CHD, and fetuses from
entire litters that were Vevo ultrasound diagnosed as without CHD. Provisional CHD
diagnoses were made based on the ultrasound findings. Then after the EFIC imaging data was
obtained, a panel of pediatric cardiologists and a pediatric pathologist reviewed the data and
made consensus CHD diagnoses. The CHD diagnosis determined by EFIC imaging was
compared to the diagnosis made by Vevo ultrasound imaging to determine the number of true
positives, false positives, true negatives and false negatives. Using these numbers, the
positive predictive value (PPV) and negative predictive value (NPV) were calculated. The
3
PPV = (number of true positives)/ (number of true positives+ number of false positives); the
NPV =(number of true negatives)/ (number of true negatives+ number of false negatives).

4
SUPPLEMENTAL TABLES
Table S1. Developmental anomalies detected by fetal ultrasound
Defects Pedigrees* G2 Females†
Total Fetuses‡
Abnormal Fetuses§
Cardiac Defects║
%Abnormal Fetus/Litter#
Total Screened 1,381 5,745 46,270 2,590
Cardiac Anomalies 664
(48.1%) 1,095
(19.1%) 1,722 (3.7%)
66.5% 20.9%
Prenatal Lethality 523
(37.9%) 871
(15.2%) 1,189
(2.6%) 45.9% 481
(40.5%) 20.0%
Growth Retarded 130
(9.4%) 168
(2.9%) 204
(0.4%) 7.9% 181
(88.7%) 17.7%
Hydrops 303
(21.9%) 425
(7.4%) 635
(1.4%) 24.5% 271
(42.7%) 20.8%
Craniofacial/Limb Defects
109 (7.9%)
143(2.5%)
221(0.5%)
8.5% 143 (64.7%)
20.6%
Body Wall Defects 34 (2.5%)
41(0.7%)
61(0.1%)
2.4% 49 (80.3%)
22.1%
Heterotaxy/ Situs Defects
30 (2.2%)
41(0.7%)
52(0.1%) 2.0%
48 (92.3%)
19.5%
*Number G1 pedigrees screened. Number in parentheses represents percent pedigrees with indicated defects in total pedigrees screened. †Number G2 females scanned with fetuses exhibiting the indicated defects. Number in parentheses represents percent G2 females with indicated defects in total G2 females screened. ‡ Number in parentheses represents percent of fetuses with indicated defects in total fetuses screened. §Percent of abnormal fetuses with the indicated defects. ║Fetuses with indicated developmental anomaly in conjunction with cardiac defects. Percent = fetuses with indicated anomaly with cardiac defects/total fetuses with indicated anomaly. #Percent of fetuses with indicated defects amongst all fetuses in the affected litters.

5
Table S2. Congenital Heart Disease Mutant Lines Archived*
*All mutant lines curated in the Mouse Genome Informatics Database (www.informatics.jax.org) and with sperm cryopreserved at the Jackson Laboratory. †Mutant lines may be represented in multiple CHD categories.
Congenital Heart Defect Phenotype No. Lines† Lines with CHD 90 Laterality Defects 49 Septal Defects
Ventricluar Septal Defect 64 Atrial Septal Defect 30 Atrioventricular Septal Defect 35
Outflow Tract Malalignments Double Outlet Right Ventricle 41 Persistent Truncus Arteriosus/Pulmonary atresia 16 Transposition of Great Arteries 10
Aortic Stenosis/Coarctation 10 Pulmonary Stenosis 16 Tricuspid Atresia 6 Hypoplastic Left Heart Syndrome 3 Hypoplastic Right Heart Syndrome 4 Arch Anomaly
Right aortic arch 22 Interrupted Aortic Arch 8 Vascular Ring 3
Coronary Fistula 5

6
Table S3. Accuracy of Vevo2100 Ultrasound Diagnosis of Congenital Heart Disease*
Values Obtained
Without the Additional 86 Normal Fetuses
Values Obtained With the Additional 86 Normal
Fetuses CHD diagnosis PPV NPV PPV NPV
Septal Defects† 95.7% 75.6% 95.7% 80.9% Outflow Tract Defects‡ 85.4% 92.1% 85.4% 93.8% HLHS 100% 100% 100% 100% HRHS 77.8% 99.5% 77.8% 99.6% MS/MA 75% 99.5% 75% 99.6% AS/AA/COA 60% 95.3% 60% 96.1% Tricuspid Hypoplasia/Atresia 60% 99.1% 60% 99.2% Pulmonary Stenosis 90% 96.5% 90% 97.1% Coronary Artery Fistula 71.4% 97.9% 71.4% 98.3% Cardiac Situs Defects 100% 99% 100% 99% *Greycolumns:Totalnumberfetuses/pupsanalyzed=438.Itincluded277identifiedwithCHD+161littermatesofaffectedfetusesbutultrasoundidentifiedaswithoutCHD.Clearcolumns:Totalnumberfetuses/pupsanalyzed=524.Itincluded277identifiedwithCHD+161littermatesofaffectedfetusesbutultrasoundidentifiedaswithoutCHD+86fetusesfromlittersthatwereultrasoundidentifiedaswithoutCHD.

7
SUPPLEMENTAL FIGURES Figure S1 Summary of Ultrasound Screen

8
Figure S2. EFIC Imaging Analysis to Assess Accuracy of Vevo2100 Diagnosis of CHD
Note fetuses analyzed by EFIC imaging for CHD confirmation are denoted in the blue boxes.

9
SUPPLEMENTAL REFERENCES 1. Shen Y, Leatherbury L, Rosenthal J, Yu Q, Pappas MA, Wessels A, Lucas J, Siegfried B,
Chatterjee B, Svenson K, Lo CW. Cardiovascular phenotyping of fetal mice by noninvasive high-frequency ultrasound facilitates recovery of ENU-induced mutations causing congenital cardiac and extracardiac defects. Physiol Genomics. 2005;24:23-36.
2. Yu Q, Shen Y, Chatterjee B, Siegfried BH, Leatherbury L, Rosenthal J, Lucas JF, Wessels A, Spurney CF, Wu YJ, Kirby ML, Svenson K, Lo CW. ENU induced mutations causing congenital cardiovascular anomalies. Development. 2004;131:6211-6223.
3. Yu Q, Leatherbury L, Tian X, Lo CW. Cardiovascular assessment of fetal mice by in utero echocardiography. Ultrasound Med Biol. 2008;34:741-752.

10
VIDEO LEGENDS
VIDEO 1
Video 1A: A fetus was found with hydrops at E13.5 by the Acuson
Video 1B: Hydrops (Arrow) and pericardial effusion (labeled PE with arrow) were detected
by further UBM scanning. (PE=pericardial effusion)
Video 1C: The UBM color flow mapping in transverse view showed bidirectional shunt and
regurgitation of AVSD.
Video 1D: Acuson scan of the same fetus one day later (E14.5) showed the affected fetus had
died, as it exhibited no heart beating.
VIDEO 2
Video 2A: The Acuson imaging in sagittal view detected abnormal blood flow (blue color
flow) during diastole.
Video 2B: The UBM 2D imaging in frontal view revealed a gap or hole (labeled CF with
arrow) in the ventricular septum. (CF=coronary artery fistula).
Video 2C: UBM color flow mapping in frontal view detected an abnormal vessel (blue flow
stream) during diastole (arrow), which originated from the root of the aorta and exited into the
RV, suggesting it is a coronary artery fistula.
Video 2D: Micro-MRI confirmed UBM diagnosis of coronary artery fistula.
VIDEO 3
Video 3A: Levocardia as seen in the transverses view by 2D imaging with the Vevo2100.
Video 3B: Right-sided stomach seen in the transverse view by 2D imaging with the
Vevo2100.
Video 3C: Vevo2100 color flow mapping in the sagittal view revealed anterior positioning of
the aorta, posterior pulmonary artery, and outflow regurgitation, which together indicated
transposition of the great arteries.
Video 3D: Vevo2100 color flow mapping in the sagittal view showed two overlapping red
flow streams representing anterior aorta with aortic regurgitation, posterior pulmonary artery
emerging from the RV, and a subpulmonary VSD. Together these presentations would
suggest DORV of the Taussig-Bing type.
Video 3E: EFIC 2D serial image stack of the same fetus confirmed DORV of the Taussig-
Bing type.

11
VIDEO 4
Video 4A: 2D imaging in the transverse view with the Vevo2100 showed atrioventricular
septal defect. (CV= common atrioventricluar valve)
Video 4B: Color flow mapping using the Vevo2100 showed atrioventricular septal defect
with regurgitation in the transverse view.
Video 4C: Pulmonary artery and majority of aorta emerge from the RV with hypoplastic PA
seen by UBM 2D imaging in sagittal view.
Video 4D: The UBM color flow mapping in the sagittal view was diagnosed as pulmonary
artery and majority of aorta connected with the RV, but no obvious flow from the PA and a
possible subaortic VSD, which together indicated DORV with severe pulmonary stenosis.
Video 4E: EFIC movie displayed DORV with severe pulmonary stenosis and AVSD. There
was also a hypoplastic branch pulmonary artery with PDA.
VIDEO 5
Video 5A: Vevo2100 color flow imaging in the sagittal view revealed hypoplastic aorta with
reversal of aortic blood flow, indicating severe aortic stenosis. Note blood flow from the
descending aorta into the ascending aorta, with only very small flow through the aortic valve.
Video 5B: Hypoplastic LV as seen by Vevo2100 2D imaging in the transverse view.
Video 5C: Quicktime movie of EFIC serial 2D image stack showed hypoplastic aorta with
severe aortic stenosis, and hypoplastic left ventricle with hypoplastic mitral valve, which
together comprises HLHS.
Related Documents