Congenital Heart Disease Dr. Md.Toufiqur Rahman Dr. Md.Toufiqur Rahman MBBS, MBBS, FCPS FCPS , MD, , MD, FACC FACC , FESC, , FESC, FRCPE FRCPE , FSCAI, , FSCAI, FAPSC, FAPSC, FAPSIC FAPSIC , FAHA, , FAHA, FCCP, FCCP, FRCPG FRCPG Associate Professor of Cardiology Associate Professor of Cardiology National Institute of Cardiovascular Diseases(NICVD), National Institute of Cardiovascular Diseases(NICVD), Sher-e-Bangla Nagar, Dhaka-1207 Sher-e-Bangla Nagar, Dhaka-1207 Consultant, Medinova, Malibagh branch Consultant, Medinova, Malibagh branch Honorary Consultant, Apollo Hospitals, Dhaka and Honorary Consultant, Apollo Hospitals, Dhaka and STS Life Care Centre, Dhanmondi STS Life Care Centre, Dhanmondi drtoufi[email protected] drtoufi[email protected] CRT 2014 Washin gton DC, USA

Congenital heart disease toufiqur rahman NICVD
Aug 12, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Congenital Heart Disease
Dr. Md.Toufiqur Dr. Md.Toufiqur Rahman Rahman
MBBS, MBBS, FCPSFCPS, MD, , MD, FACCFACC, FESC, , FESC, FRCPEFRCPE, FSCAI, , FSCAI,
FAPSC, FAPSC, FAPSICFAPSIC, FAHA, , FAHA, FCCP,FCCP, FRCPG FRCPG
Associate Professor of CardiologyAssociate Professor of CardiologyNational Institute of Cardiovascular Diseases(NICVD),National Institute of Cardiovascular Diseases(NICVD),
Sher-e-Bangla Nagar, Dhaka-1207Sher-e-Bangla Nagar, Dhaka-1207
Consultant, Medinova, Malibagh branchConsultant, Medinova, Malibagh branch
Honorary Consultant, Apollo Hospitals, Dhaka and Honorary Consultant, Apollo Hospitals, Dhaka and
STS Life Care Centre, Dhanmondi STS Life Care Centre, Dhanmondi [email protected]@yahoo.com
CRT 2014Washington DC, USA

Introduction
Congenital Heart Disease (CHD) are Congenital Heart Disease (CHD) are diseases a child is born with, that is CHD diseases a child is born with, that is CHD are due to defects a child has since birth.are due to defects a child has since birth.
A congenital abnormality of the heart is A congenital abnormality of the heart is present in nearly 1% live birth.present in nearly 1% live birth.
Most form of CHD are amenable to Most form of CHD are amenable to surgery, in most cases this lead to cure.surgery, in most cases this lead to cure.

General Comments
The appropriate management of the CHD The appropriate management of the CHD is depends on the precise identification of is depends on the precise identification of the anatomy & pathophysiology of the the anatomy & pathophysiology of the patients abnormality. This is achieved bypatients abnormality. This is achieved by
1.1. Clinical AssessmentClinical Assessment2.2. CXRCXR3.3. ECGECG4.4. Echocardiography + Color DopplerEchocardiography + Color Doppler5.5. Cardiac Catheterization in some cases Cardiac Catheterization in some cases

No epidemiological data .No epidemiological data . Prevalence of CHD is 1%. As such Prevalence of CHD is 1%. As such
total CHD patient in Bangladesh is total CHD patient in Bangladesh is nearly 1400000.nearly 1400000.
NICVD is the only centre that has NICVD is the only centre that has infrastructure for treating such infrastructure for treating such patientspatients..
CHD in Bangladesh

Spectrum of Problem
Huge number of untreated casesHuge number of untreated cases Late presentationLate presentation Limited resourcesLimited resources IlliteracyIlliteracy Poor socio-economic conditionPoor socio-economic condition Social and cultural tabooSocial and cultural taboo

Before going on to the details of CHD, let Before going on to the details of CHD, let us recapitulate some of the basic anatomy us recapitulate some of the basic anatomy of the heart and the cardiovascular system of the heart and the cardiovascular system as a whole.as a whole.
Then we shall discuss the classification, in a Then we shall discuss the classification, in a simplified form.simplified form.
Then Some of the common CHD is some Then Some of the common CHD is some details. details.

Normal Anatomy of the Heart



Classification of CHD
Classification of CHD can be done in four Classification of CHD can be done in four groups, as follows:groups, as follows:
1.1. Pure Obstructive lesionsPure Obstructive lesions
2.2. Simple Left-Right shunt (acyanotic)Simple Left-Right shunt (acyanotic)
3.3. Right –Left shunts (cyanotic)Right –Left shunts (cyanotic)
4.4. Complex congenital defects (mixing Complex congenital defects (mixing defect)defect)

Pulmonary stenosisPulmonary stenosis Mitral stenosis Mitral stenosis Aortic stenosisAortic stenosis Coarctation of aortaCoarctation of aorta Interrupted Aortic archInterrupted Aortic arch
Pure Obstructive lesions (congenital)

Simple L-R Shunts
Patient Ductus Arteriosus (PDA)Patient Ductus Arteriosus (PDA) Atrial Septal Defect (ASD)Atrial Septal Defect (ASD) Ventricular Septal Defect (VSD)Ventricular Septal Defect (VSD) Endocardial cushion defect (AV canal)Endocardial cushion defect (AV canal) Aortopulmonary windowAortopulmonary window

R-L Shunts Cyanotic Heart disease
Tetralogy of Fallot (TOF)Tetralogy of Fallot (TOF) Pulmonary atresia with VSDPulmonary atresia with VSD Pulmonary atresia with out VSDPulmonary atresia with out VSD Tricuspid atresiaTricuspid atresia Ebstein’s anomalyEbstein’s anomaly

Complex CHD (Mixing defect)
Double outlet right ventricle (DORV)Double outlet right ventricle (DORV) Univentricular heartUniventricular heart Transposition of Great Arteries (TGA)Transposition of Great Arteries (TGA) Total Anomalous Pulmonary Venous Total Anomalous Pulmonary Venous
Drainage (TAPVD)Drainage (TAPVD) Truncus Arteriosus Truncus Arteriosus Hypoplastic Left Heart Syndrome Hypoplastic Left Heart Syndrome

Spectrum of CHD
AcyanoticAcyanotic
L>R shuntL>R shunt ASD .VSD. ASD .VSD. PDA. AVSDPDA. AVSD
Obstructive lesionObstructive lesion CoA. AS. PSCoA. AS. PS
CyanoticCyanotic
With increased With increased PBFPBF TGATGA. . TAPVC.TAPVC. TRUNCUSTRUNCUS ARTERIOSUSARTERIOSUS
With decreased With decreased PBFPBF: : TOF. PA. TOF. PA. DORVDORV

Some myths about CHD
Complex CHD is not worth treatingComplex CHD is not worth treating Most VSD’s close spontaneously and Most VSD’s close spontaneously and
so can be ignored in early childhoodso can be ignored in early childhood Child below 10 kg does not with stand Child below 10 kg does not with stand
surgerysurgery Cyanosis is harmless till the child Cyanosis is harmless till the child
grows upgrows up Child with CHD cannot digest rich Child with CHD cannot digest rich
foodfood
CHD - REALITIESCHD - REALITIES
Simple CHD can become inoperable if not Simple CHD can become inoperable if not tackled on timetackled on time
Late presentation has high morbidity and long Late presentation has high morbidity and long term survival is sub optimal.term survival is sub optimal.
Timing of surgery is crucial to optimal Timing of surgery is crucial to optimal survival.survival.
Child with CHD needs extra calories and is Child with CHD needs extra calories and is
capable of digestingcapable of digesting it. it.

Common & Usually symptomaticCommon & Usually symptomatic Diagnosis is made by Clinical + Diagnosis is made by Clinical +
EchoEcho Surgery totally cures by “ Surgery totally cures by “ Division Division
& Suturing & Suturing ””
PDA

PDA…indications
Surgery whenever diagnosedSurgery whenever diagnosed All detectable PDA’s should be All detectable PDA’s should be
closedclosed In pre-term PDA-institutional In pre-term PDA-institutional
approachapproach

ASD…1
Usually symptomless in childrenUsually symptomless in children Diagnosis is by clinical and echo Diagnosis is by clinical and echo Exceptional cases -catheter & Exceptional cases -catheter &
angiographyangiography Cures totally by open heart Cures totally by open heart
surgerysurgery


ASD…2
Infancy ( relatively uncommon)Infancy ( relatively uncommon) Symptoms of CHF unresponsive to therapySymptoms of CHF unresponsive to therapy §§ Failure to thrive Failure to thrive §§ Documented Pulmonary hypertension, Documented Pulmonary hypertension,
Obstructed TAPVCObstructed TAPVC
Beyond infancyBeyond infancy Evidence of RV volume over loadEvidence of RV volume over load §§ Increased Pulmonary Shunt (Qp/Qs >1.8)Increased Pulmonary Shunt (Qp/Qs >1.8) §§ Presence of PAPVC as Load Increases Presence of PAPVC as Load Increases
with agewith age

ASD…3
Contentious issue isContentious issue is
§§ Shunt <1.5Shunt <1.5
§§ Large DefectLarge Defect
§§ Paradoxical Embolism Paradoxical Embolism ContraindicationsContraindications
§§ Established PVDEstablished PVD
§§ RV Failure RV Failure

VSD’s - FEW MYTHSVSD’s - FEW MYTHS
MostMost VSDs close sontaneously VSDs close sontaneously
Large VSDs also Closes Large VSDs also Closes
SpontaneouslySpontaneously
Time of surgery: 10 years/10 KgsTime of surgery: 10 years/10 Kgs
Clinical improvement as ClosureClinical improvement as Closure

VSD - FEW FACTSVSD - FEW FACTS
Highest incidence among CHD Highest incidence among CHD Timely surgery: mortality < 1%Timely surgery: mortality < 1% Commonest Cause of Eisenmenger Commonest Cause of Eisenmenger
Complex Complex

VSD’s - CURRENT FACTSVSD’s - CURRENT FACTS
Large VSDs & subarterial VSDs do Large VSDs & subarterial VSDs do not close spontaneouslynot close spontaneously
Onset of Eisenmenger complex is Onset of Eisenmenger complex is also coincident with clinical also coincident with clinical
improvementimprovement..

Large VSD
Beyond 3 months of age at presentationBeyond 3 months of age at presentation
§§ CHF control a formidable taskCHF control a formidable task
§§ Poorly tolerate inter current illnesses Poorly tolerate inter current illnesses
§§ Development of PVD particularly Development of PVD particularly
rapidrapid
Prior to 3 monthsPrior to 3 months
§§ Chance at medical stabilization , if Chance at medical stabilization , if
fails fails Surgery Surgery

Large vsd : How to proceed ?Large vsd : How to proceed ?
Optimize CHF managementOptimize CHF management
Hyper Caloric feeds? NG Tube feedsHyper Caloric feeds? NG Tube feeds
Surgical Intervention :Surgical Intervention : §§ Poor weight gain despite best efforts Poor weight gain despite best efforts §§ Evidence of increased PAH Evidence of increased PAH

THRUST TOWARDS EARLY SURGERY- Why ?
Restores Normal physiologyRestores Normal physiology
Better preservation of Myocardial functionBetter preservation of Myocardial function
Hyperplasia and angiogenesis Vs. Hyperplasia and angiogenesis Vs. HypertrophyHypertrophy
Better remodeling Better remodeling
Reduces potential for electrical instabilityReduces potential for electrical instability How early is early ? Realistically 3 months How early is early ? Realistically 3 months
and beyondand beyond

MODERATE SIZED VSD
Operate Electively at 6 monthsOperate Electively at 6 months Risk of surgery MinimalRisk of surgery Minimal Chances of spontaneous closure Chances of spontaneous closure
remoteremote Increased possibility of PVDIncreased possibility of PVD Earlier if:Earlier if:
- Poor control of CHF- Poor control of CHF
- Failure to thrive- Failure to thrive

Small VSD- approach
Medical follow up.Medical follow up. Nutritional counselingNutritional counseling IE prophylaxisIE prophylaxis SurgerySurgery :(restrictive indications):(restrictive indications)
§§ Sub- arterial VSD with aortic incompetence Sub- arterial VSD with aortic incompetence (Grade-III/IV; calcification / fibrosis)(Grade-III/IV; calcification / fibrosis)
§§ IE or LV dilatation IE or LV dilatation

TETROLOGY OF FALLOT, DORV,P.S
Asymptomatic - Total Correction >6 MonthsAsymptomatic - Total Correction >6 Months
wt>7 Kgwt>7 Kg Symptomatic - SpellsSymptomatic - Spells
- Desaturation (Spo2 <70% )- Desaturation (Spo2 <70% )
- Failure To thrive- Failure To thrive 3 Months - B.T Shunt3 Months - B.T Shunt 3-6 Months - Good Anatomy - Total Correction3-6 Months - Good Anatomy - Total Correction
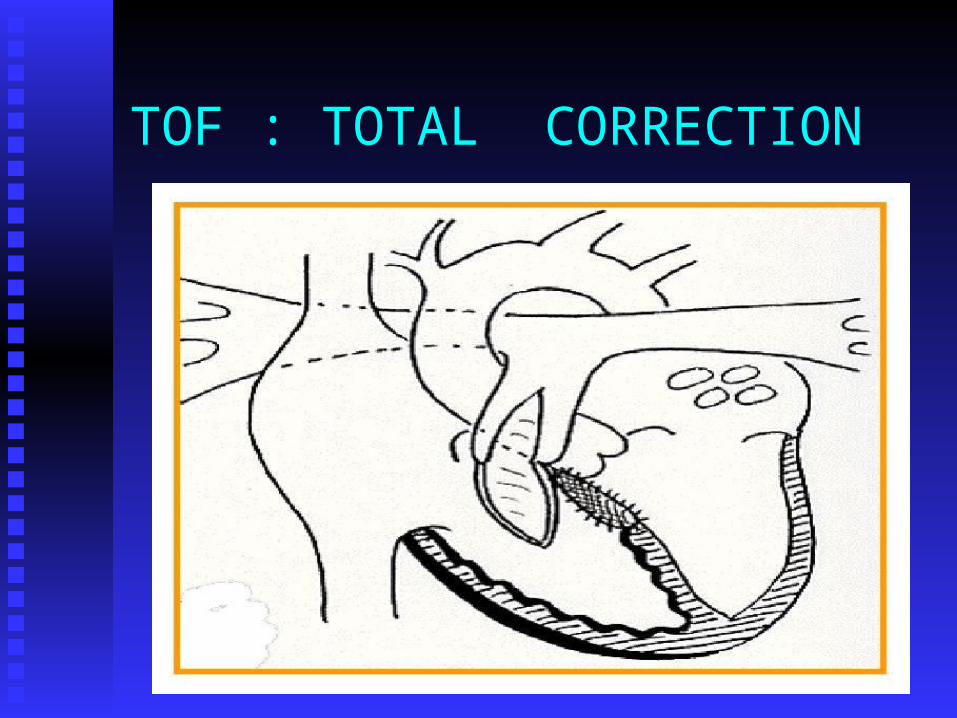
TOF : TOTAL CORRECTION

IS LOW WEIGHT FOR AGE DETRIMENTAL
release of inflammatory markersrelease of inflammatory markers
- IL-6, IL-2, TNF, ICAM- IL-6, IL-2, TNF, ICAM Poor immunologic profilePoor immunologic profile Poor ventilatory mechanics - CPAP Post Poor ventilatory mechanics - CPAP Post
extubation more a rule than exception extubation more a rule than exception Re-institution of post-op. feeding poor Re-institution of post-op. feeding poor Inodilator requirements (PGE- inhibitors) Inodilator requirements (PGE- inhibitors) ICU + Hospital stayICU + Hospital stay

OPERATIVE RISK FOR VARIOUS CHD PDA, ASDPDA, ASD VSD without PHTVSD without PHT Unobstructed TAPVC Unobstructed TAPVC 0-2 %0-2 %
Coarctation Repair Coarctation Repair
VSD/P SVSD/P S Senning RepairSenning Repair AV Canal Repair AV Canal Repair 3-5 %3-5 % Conduit Repair Conduit Repair

OPERATIVE RISK CONTD...
Arterial switch operationArterial switch operation Fontan OperationFontan Operation Obstructed TAPVCObstructed TAPVC
TGA / VSD With hypertension TGA / VSD With hypertension 10-15%10-15% VSD With Pulmonary VSD With Pulmonary
hypertensionhypertension

RECENT ADVANCES
In preoperative diagnosis & In preoperative diagnosis & stabilization.stabilization.
In Operative Management.In Operative Management. In Post operative careIn Post operative care

PREOPERATIVE ADVANCES
Early accurate noninvasive diagnosisEarly accurate noninvasive diagnosis - 2 D Echocardiography with Color Doppler- 2 D Echocardiography with Color Doppler
- Fetal echocardiography- Fetal echocardiography StabilizationStabilization - Prostaglandin ( PGE1 )- Prostaglandin ( PGE1 ) - Elective Ventilation- Elective Ventilation - Ionotrope- Ionotrope Monitor TransportMonitor Transport

INTRAOPERATIVE ADVANCES
Improved Cardiopulmonary bypass Improved Cardiopulmonary bypass
CircuitsCircuits Improved understanding of Deep Improved understanding of Deep
Hypothermia and circulatory arrest.Hypothermia and circulatory arrest.
Better myocardial protection.Better myocardial protection.

ADVANCES IN POST- ADVANCES IN POST- OPERATIVE CAREOPERATIVE CARE
Sophisticated haemodynamic Sophisticated haemodynamic monitoringmonitoring Pharmacological manipulationPharmacological manipulation Better ventilatorsBetter ventilators Mechanical support : ECMO / Mechanical support : ECMO / LVAD/IABPLVAD/IABPNitric Oxide therapy.Nitric Oxide therapy.

Thank [email protected]
Asia Pacific Congress of Hypertension, 2014, February
Cebu city, Phillipines
Seminar on Management of Hypertension, Gulshan, Dhaka
Related Documents











