Congenital Adrenal Hyperplasia

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 1/16
Congenital Adrenal
Hyperplasia

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 2/16
defnition
• The term congenital adrenalhyperplasia (CAH) encompasses agroup o autosomal recessivedisorders, each o which involves adefciency o an enzyme involved inthe synthesis o cortisol, aldosterone,
or both

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 3/16
Epidemiology
United States
• The most common orm o congenital adrenal hyperplasia isdue to mutations or deletions o CYP21A, resulting in !"#hydro$ylase defciency This defciency accounts or morethan %&' o adrenal hyperplasia cases utations or partialdeletions that aect CYP21A are common, with estimated
re*uencies as high as " in + individuals in selectedpopulations (eg, Ashkenazi Jews) to " in individuals in-ew .or/ City The estimated prevalence is " case per 0&individuals in the general population
• Classic adrenal hyperplasia has an overall prevalence o "
case per "0,&&& population1 however, in selected populations(eg, the .upi/ o Alas/a), the prevalence is as high as " casein 2&& population Congenital adrenal hyperplasia caused by""#beta#hydro$ylase defciency accounts or 3#4' o allcongenital adrenal hyperplasia cases

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 4/16
International
• Congenital adrenal hyperplasia caused by
!"#hydro$ylase defciency is ound in allpopulations ""#beta#hydro$ylasedefciency is more common in persons o
oroccan or 5ranian#6ewish descentMortality/Morbidity
• The morbidity o the various orms oadrenal hyperplasia is best understood in
the conte$t o the steroidogenic pathway,shown below, used by the adrenal glandsand gonads

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 5/16
• The clinical phenotype can be understood byanalyzing the location o the enzyme
defciency, the accumulation o precursorhormones, the products o those precursorswhen one enzyme pathway is ineective, andthe physiologic action o those hormones (see
History)• 7evere orms o congenital adrenal
hyperplasia are potentially atal iunrecognized and untreated because o the
severe cortisol and aldosterone defcienciesthat result in salt wasting, hyponatremia,hyper/alemia, dehydration, and hypotension

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 6/16
a!e
• Congenital adrenal hyperplasia occurs among
people o all races Congenital adrenal hyperplasiasecondary to CYP21A1 mutations and deletions isparticularly common among the .upi/ 8s/imos
Se"
•
9ecause all orms o congenital adrenal hyperplasiaare autosomal recessive disorders, both se$es areaected with e*ual re*uency However, becauseaccumulated precursor hormones or associatedimpaired testosterone synthesis impacts se$ualdierentiation, the phenotypic conse*uences omutations or deletions o a particular gene dierbetween the se$es

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 7/16
Age
•Classic congenital adrenalhyperplasia is generally recognizedat birth or in early childhood because
o ambiguous genitalia, salt wasting,or early virilization -onclassicadrenal hyperplasia is generallyrecognized at or ater puberty
because o oligomenorrhea orvirilizing signs in emales

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 8/16
#athophysiology
The clinical maniestations o each orm o congenitaladrenal hyperplasia are related to the degree o cortisoldefciency and:or the degree o aldosterone defciency5n some cases, these maniestations re;ect the
accumulation o precursor adrenocortical hormones<hen present in supraphysiologic concentrations, theseprecursors lead to e$cess androgen production withresultant virilization, or because o mineralocorticoidproperties, cause sodium retention and hypertension
The phenotype depends on the degree or type o genedeletion or mutation and the resultant defciency o thesteroidogenic enzyme The enzymes and correspondinggenes are displayed in the image below

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 9/16
• Two copies o an abnormal gene are re*uired or diseaseto occur, and not all mutations and partial deletions resultin disease The phenotype can vary rom clinically
inapparent disease (occult or cryptic adrenal hyperplasia)to a mild orm o disease that is e$pressed in adolescenceor adulthood (nonclassic adrenal hyperplasia) to severedisease that results in adrenal insu=ciency in inancy withor without virilization and salt wasting (classic adrenalhyperplasia) The most common orm o adrenalhyperplasia (due to a defciency o !"#hydro$ylaseactivity) is clinically divided into + phenotypes> saltwasting, simple virilizing, and nonclassic
• CYP21A is the gene that codes or !"#hydro$ylase,
CYP11B1 codes or ""#beta#hydro$ylase, and CYP17 codesor "#alpha#hydro$ylase any o the enzymes involvedin cortisol and aldosterone syntheses are cytochrome?23& (C.?) proteins

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 10/16
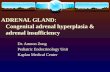
8nzymes and genes involved in adrenal steroidogenesis

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 11/16
7teroidogenic pathway or cortisol, aldosterone, and se$ steroidsynthesis A mutation or deletion o any o the genes that codeor enzymes involved in cortisol or aldosterone synthesis resultsin congenital adrenal hyperplasia The particular phenotype that
results depends on the se$ o the individual, the location o thebloc/ in synthesis, and the severity o the genetic deletion or

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 12/16

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 13/16
Treatment•
?atients with dehydration, hyponatremia, or hyper/alemia and apossible salt#wasting orm o adrenal hyperplasia should receivean intravenous (5@) bolus o isotonic sodium chloride solution(!& m:/g or 23& m:m!) over the frst hour, as needed, torestore their intravascular volume and blood pressure
" This dosage may be repeated i the blood pressure remains low
! Be$trose must be administered i the patient is hypoglycemicand must be included in the rehydration ;uid ater the bolusdose to prevent hypoglycemia
+ Ater samples are obtained to measure electrolyte, blood sugar,cortisol, aldosterone, and "#hydro$yprogesterone
concentrations, the patient should be treated withglucocorticoids based on suspected adrenal insu=ciency
Treatment should not be withheld while confrmatory results areawaited because it may be lie preserving (see edication)

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 14/16
The 8ndocrine 7ocietys !&"& clinical practice guidelines
note the ollowing >
• ?renatal treatment or CAH should be regarded ase$perimental
• Dlucocorticoid therapy should be careully titrated to avoidCushing syndrome
• ineralocorticoid replacement is encouraged 5n inants,mineralocorticoid replacement and sodiumsupplementation are encouraged
• Ese o agents to delay puberty and promote growth are
e$perimental• ?sychiatric support should be encouraged or patients with
adFustment problems
• edication should be used Fudiciously during pregnancyand in symptomatic patients with nonclassical CAH

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 15/16
S$rgi!al %are
5nants with ambiguous genitalia re*uire surgical evaluation and, i
needed, plans or corrective surgery
• The traditional approach to the emale patient with ambiguousgenitalia due to adrenal hyperplasia is clitoral recession early in lieollowed by vaginoplasty ater pubertyG"2 @ocal groups o patients
with disorders o se$ual dierentiation (eg,5nterse$ 7ociety o -orth America) have recently challenged thisapproach
• 7ome emale inants with adrenal hyperplasia have only mildvirilization and may not re*uire corrective surgery i they receiveade*uate medical therapy to prevent urther virilization
•9ilateral adrenalectomies have been suggested in the managemento virilizing orms o adrenal hyperplasia in order to prevent urthervirilization and advancement o s/eletal maturationG"3 This approachis e$perimental and should be considered only in the conte$t o acontrolled study

7/18/2019 Congenital Adrenal Hyperplasia
http://slidepdf.com/reader/full/congenital-adrenal-hyperplasia-56d47ac670214 16/16
The 8ndocrine 7ocietys !&"& clinical
practice guidelines note the ollowing>
• Adrenalectomy should be avoided
• <hile surgical reconstruction maynot be necessary during the newbornperiod in mildly virilized girls, it may
be appropriate in severely virilizedgirls 5t should be a single stagegenital repair, perormed bye$perienced surgeons
Related Documents