Confusing thoughts and speech: source monitoring and psychosis Ce ´cile Henquet a, * , Lydia Krabbendam a , Jorg Dautzenberg, Jelle Jolles a , Harald Merckelbach b a Department of Psychiatry and Neuropsychology, South Limburg Mental Health Research and Teaching Network, EURON, Maastricht University, P.O. Box 616, 6200 MD Maastricht, The Netherlands b Department of Experimental Psychology, Maastricht University, P.O. Box 616, 6200 MD Maastricht, The Netherlands Received 31 July 2003; received in revised form 26 July 2004; accepted 11 August 2004 Abstract To explore the idea that deficits in source monitoring may underlie positive symptoms of schizophrenia, the current study compared schizophrenic patients’ performance (n =15) on an internal source-monitoring task with that of normal controls (n =15). On the basis of a source-monitoring task in which participants had to recall whether they had verbalized answers or merely thought about these answers, overall source monitoring performance, discrimination index, and response bias were calculated. In addition, participants completed cognitive tests and symptomatology questionnaires. Relative to controls, patients had significantly more difficulties with monitoring their own actions and showed a tendency towards misclassifying imagined thoughts as verbalized thoughts. Source-monitoring performance was related to selective attention, but not to other cognitive domains. No relationship was found between source monitoring and symptomatology. Failures in internal source monitoring are a prominent feature of schizophrenia, and our results suggest that they form a more enduring characteristic of this disorder than has previously been assumed. D 2004 Elsevier Ireland Ltd. All rights reserved. Keywords: Schizophrenia; Positive symptoms; Psychosis-related traits; Self-monitoring; Neuropsychological deficits 1. Introduction Source monitoring refers to cognitive processes involved in determining the source of memory information (Johnson et al., 1993). The following three source-monitoring situations can be distin- guished: (a) discriminating between internally gen- erated information (e.g., fantasies) and memories of externally derived information, a process that is usually termed reality monitoring (Johnson and Raye, 1981); (b) discriminating between two or more external sources (e.g., television versus a good friend); and (c) discriminating between two internal sources (e.g., fantasies versus dreams), a process that is often referred to as self-monitoring (Johnson et al., 1993). 0165-1781/$ - see front matter D 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.psychres.2004.08.009 * Corresponding author. Tel.: +31 43 3299773; fax: +31 43 3299708. E-mail address: [email protected] (C. Henquet). Psychiatry Research 133 (2005) 57 – 63 www.elsevier.com/locate/psychres

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.elsevier.com/locate/psychres
Psychiatry Research 1
Confusing thoughts and speech: source monitoring and psychosis
Cecile Henqueta,*, Lydia Krabbendama, Jorg Dautzenberg,
Jelle Jollesa, Harald Merckelbachb
aDepartment of Psychiatry and Neuropsychology, South Limburg Mental Health Research and Teaching Network, EURON,
Maastricht University, P.O. Box 616, 6200 MD Maastricht, The NetherlandsbDepartment of Experimental Psychology, Maastricht University, P.O. Box 616, 6200 MD Maastricht, The Netherlands
Received 31 July 2003; received in revised form 26 July 2004; accepted 11 August 2004
Abstract
To explore the idea that deficits in source monitoring may underlie positive symptoms of schizophrenia, the current study
compared schizophrenic patients’ performance (n=15) on an internal source-monitoring task with that of normal controls
(n=15). On the basis of a source-monitoring task in which participants had to recall whether they had verbalized answers or
merely thought about these answers, overall source monitoring performance, discrimination index, and response bias were
calculated. In addition, participants completed cognitive tests and symptomatology questionnaires. Relative to controls, patients
had significantly more difficulties with monitoring their own actions and showed a tendency towards misclassifying imagined
thoughts as verbalized thoughts. Source-monitoring performance was related to selective attention, but not to other cognitive
domains. No relationship was found between source monitoring and symptomatology. Failures in internal source monitoring are
a prominent feature of schizophrenia, and our results suggest that they form a more enduring characteristic of this disorder than
has previously been assumed.
D 2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Schizophrenia; Positive symptoms; Psychosis-related traits; Self-monitoring; Neuropsychological deficits
1. Introduction
Source monitoring refers to cognitive processes
involved in determining the source of memory
information (Johnson et al., 1993). The following
0165-1781/$ - see front matter D 2004 Elsevier Ireland Ltd. All rights re
doi:10.1016/j.psychres.2004.08.009
* Corresponding author. Tel.: +31 43 3299773; fax: +31 43
3299708.
E-mail address: [email protected] (C. Henquet).
three source-monitoring situations can be distin-
guished: (a) discriminating between internally gen-
erated information (e.g., fantasies) and memories of
externally derived information, a process that is
usually termed reality monitoring (Johnson and Raye,
1981); (b) discriminating between two or more
external sources (e.g., television versus a good friend);
and (c) discriminating between two internal sources
(e.g., fantasies versus dreams), a process that is often
referred to as self-monitoring (Johnson et al., 1993).
33 (2005) 57–63
served.
C. Henquet et al. / Psychiatry Research 133 (2005) 57–6358
Transient source-monitoring errors are common in
everyday social situations. However, psychotic
experiences have been hypothesized to originate
from a fundamentally disturbed source monitoring.
Thus, several authors have argued that a specific
source-monitoring impairment may underlie certain
positive psychotic symptoms (Heilbrun, 1980; Hoff-
man, 1986; Bentall, 1990). For example, according
to Frith’s model of psychosis (Frith and Done,
1989; Frith, 1992), symptoms of alien control and
certain hallucinations arise from difficulties with
monitoring one’s own willed intentions, actions, and
thoughts, whereas other symptoms (e.g., paranoid
delusions) are due to difficulties in monitoring the
intentions of others. A number of source-monitoring
studies have shown that during the acute phase of
schizophrenia, patients find it difficult to discrim-
inate between self-generated items and items
generated by the researcher (Keefe et al., 1999;
Brebion et al., 2000). The majority of these studies
suggest that an external attribution bias underlies
reality-monitoring failures exhibited by schizo-
phrenic patients (Harvey, 1985; Keefe et al.,
1999; see also Franck et al., 2000). In this line
of reasoning, positive symptoms (e.g., hallucinations
and certain delusions) originate from a tendency to
attribute self-generated information to an external
source (Slade and Bentall, 1988).
Many previous studies on schizophrenic patients’
source-monitoring abilities relied on tasks that were
highly artificial, in the sense of being far removed
from everyday situations. A typical approach involves
presenting the patient with examples of a certain
category and asking him/her to generate other
examples. Subsequently, the patient has to differ-
entiate between these two sources of information (e.g.,
Brebion et al., 2000). Although this type of design has
provided important insights, a potential limitation is
that its results may be difficult to generalize to real-
life source-monitoring tasks (Parks, 1997). With this
in mind, the present study relied on a source-
monitoring task involving the common situation in
which one tries to remember whether one has actually
said or only thought something (Parks, 1997). Thus,
we investigated whether schizophrenic patients make
more mistakes on such an everyday source-monitor-
ing task than matched normal controls, and if so,
whether these mistakes specifically take the form of
falsely identifying internal thoughts as verbalized
thoughts.
There is still controversy regarding the precise
relationship between source-monitoring performance
and other cognitive functions (Brebion et al., 1996;
Seal et al., 1997; Stirling et al., 1998). Seal et al.
(1997) opined that performance on self-monitoring
tasks is confounded by factors such as verbal
intelligence, whereas the study by Stirling and
colleagues indicated that self-monitoring perform-
ance is unrelated to general cognitive functioning
(Stirling et al., 1998). Interestingly, Brebion et al.
(1996) found schizophrenic patients’ source-moni-
toring performance to be related to selective
attention, but not to memory capacity. We addressed
this issue by examining the links between source-
monitoring scores and performance in other cogni-
tive domains, notably general intelligence, attention,
and memory.
2. Method
2.1. Subjects
Participants were 15 patients with schizophrenia
and 15 healthy controls. Patients were recruited
through clinical and ambulatory facilities of psychi-
atric hospital Vijverdal, Maastricht, the Netherlands.
Diagnoses were made by patients’ psychiatrists
based on DSM-IV criteria (American Psychiatric
Association, 1994). Mean age of the patient group
(14 men; 1 woman) was 26.7 years (S.D.=6.4).
Their average level of education measured on an 8-
point scale, ranging from primary school to univer-
sity degree, was 3.7 (S.D.=1.4). Average scores on
the Positive and Negative Syndrome Scale (PANSS;
Kay et al., 1986) were 9.6 (S.D.=3.1) for the
positive scale and 10.0 (S.D.=2.6) for the negative
scale, indicating low levels of acute symptoms in
the patient group. Eight patients received antipsy-
chotic medication, with four of them using conven-
tional neuroleptics and four receiving atypical
neuroleptic drugs.
Control participants were recruited from the
general population through random mailings in the
local area and through the staff in the same
psychiatric hospital. An attempt was made to match

C. Henquet et al. / Psychiatry Research 133 (2005) 57–63 59
controls with patients on age. Controls were only
included if they had an absence of a lifetime history
of any psychiatric disorder. None of them used
psychotropic medication. The mean age of the
control group (11 men; 4 women) was 26.6 years
(S.D.=8.4), while the average level of education was
5.3 (S.D.=1.0). Patient and control groups did not
differ with regard to age [t(26)b1.0, P=0.98] or
gender distribution [x2(1)=2.16, P=0.14]. However,
patients had a significantly lower level of education
than controls [t(26)=3.79, Pb0.01].
For both patients and controls, the following
exclusion criteria were used: (i) head trauma (with
loss of consciousness), (ii) alcohol abuse (more than 5
units per day), and (iii) weekly use of drugs.
Participants were paid for their participation, and
written informed consent was obtained from all
participants.
2.2. Materials and procedure
The source-monitoring task was derived from a
series of studies by Parks (1997) and addressed
participants’ ability to discriminate thoughts from
actually verbalized thoughts. More specifically, par-
ticipants had to indicate whether they had verbalized
answers to earlier presented questions or only
imagined they did. Materials consisted of 24 non-
intrusive questions concerning personal history (e.g.,
bWhen were you born?Q) and opinion (e.g., bWhat
food do you like?Q). Questions were presented on a
computer screen, using a computer program specifi-
cally developed for this purpose (Dautzenberg and
Henquet, 2000).
The source-monitoring task involved 16 trials. On
half of the trials, single questions were presented. On
the other half, questions were presented in pairs, with
one question being located at the top half of the
computer screen and the other being located at the
bottom half of the screen. Questions were presented,
after which a white screen was shown for 3 s.
Participants had to prepare an answer to the presented
questions. On single question trials, the word
banswerQ appeared shortly after presentation of the
question. On dual question trials, either the words
banswer topQ or banswer bottomQ appeared. Thus,
here participants had to prepare an answer to both
questions, but they verbalized only one answer. This
resulted in verbalizing answers to 16 questions, while
8 answers were covertly prepared but never verbal-
ized. Single questions and pairs were presented in a
quasi-random order, and two counterbalanced ver-
sions were used. Participants were randomly allo-
cated to one of the two versions. An examiner was
present to monitor whether participants actually
verbalized the answers. All participants were capable
of answering the questions, which makes clear that
the questions were simple and direct. Participants
were instructed to press a button as soon as they had
prepared an answer for the questions. Preparation
time varied between participants but never took
longer than 7 s. Given this constellation, we have
every reason to believe that participants actually did
prepare answers during the preparation phase of two-
question trials, as opposed to merely remembering
the questions. Following the presentation of the
questions and a filler task (which took about 5
min), participants were given a surprise recognition
task. In this task, participants saw original questions,
each paired with a new question of the same content
and form. For example, the old item bWhen were you
born?Q was presented along with the new item
bWhere were you born?Q Participants were asked to
identify for each of the 24 pairs of old and new items
the question they had seen before (i.e., the memory
aspect of the task). Further, they had to indicate
whether they verbalized answers to the boldQ items or
only thought about an answer (i.e., the source-
monitoring aspect of the task).
Neuropsychological assessment focused on intelli-
gence and selective attention. Overall intellectual
functioning was measured by three subtests of the
Groningen Intelligence Test (GIT; Luteijn and van der
Ploeg, 1983). The Stroop Color-Word test (Stroop,
1935) was used to tap selective attention (Houx et al.,
1991). This test involves three cards displaying color
names, colored patches, and color names printed in
inconsistent ink colors (cards I–III, respectively). The
time needed to complete card III is largely determined
by the ability to ignore irrelevant but salient verbal
color names, so as to color name the ink of the words.
To obtain a measure of selective attention, Stroop
response latencies were transformed into a Stroop
interference score. The Schizotypal Personality Scale-
A (STA; Claridge and Broks, 1984) was administered
to measure schizotypal traits. Hallucinations, delu-
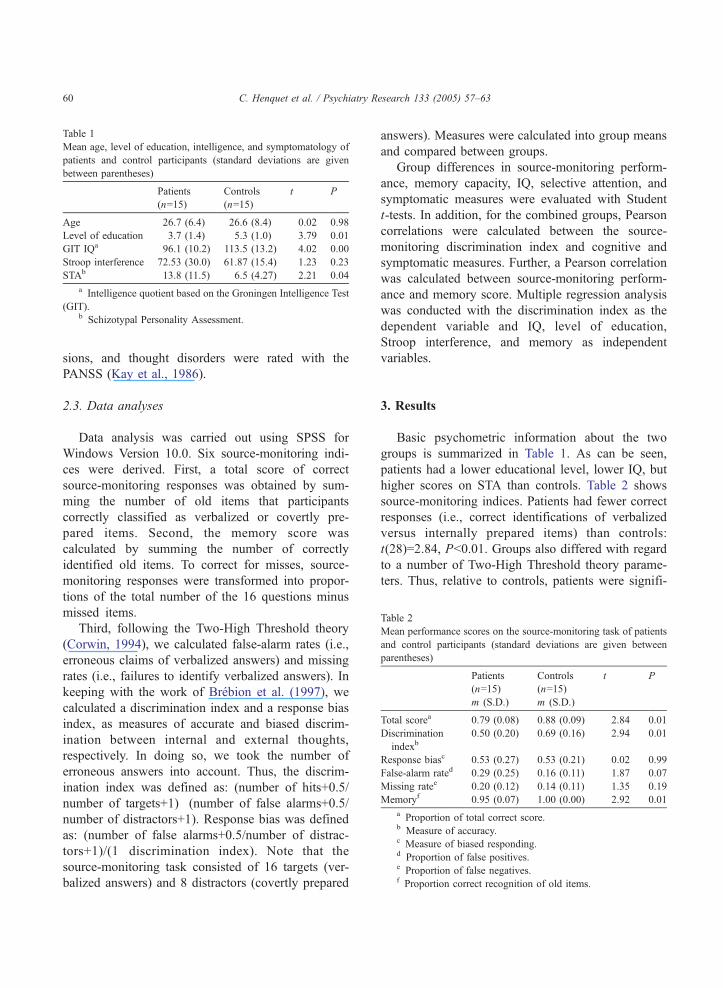
Table 1
Mean age, level of education, intelligence, and symptomatology of
patients and control participants (standard deviations are given
between parentheses)
Patients
(n=15)
Controls
(n=15)
t P
Age 26.7 (6.4) 26.6 (8.4) �0.02 0.98
Level of education 3.7 (1.4) 5.3 (1.0) 3.79 0.01
GIT IQa 96.1 (10.2) 113.5 (13.2) 4.02 0.00
Stroop interference 72.53 (30.0) 61.87 (15.4) �1.23 0.23
STAb 13.8 (11.5) 6.5 (4.27) �2.21 0.04
a Intelligence quotient based on the Groningen Intelligence Test
(GIT).b Schizotypal Personality Assessment.
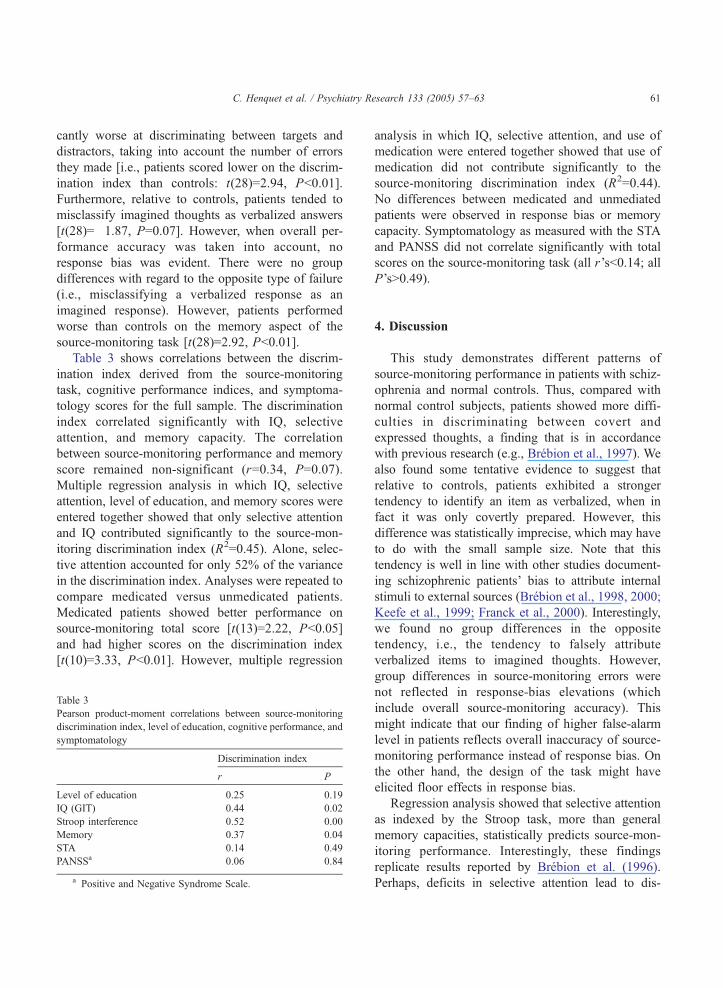
Table 2
Mean performance scores on the source-monitoring task of patients
and control participants (standard deviations are given between
parentheses)
Patients
(n=15)
m (S.D.)
Controls
(n=15)
m (S.D.)
t P
Total scorea 0.79 (0.08) 0.88 (0.09) 2.84 0.01
Discrimination
indexb0.50 (0.20) 0.69 (0.16) 2.94 0.01
Response biasc 0.53 (0.27) 0.53 (0.21) 0.02 0.99
False-alarm rated 0.29 (0.25) 0.16 (0.11) �1.87 0.07
Missing ratee 0.20 (0.12) 0.14 (0.11) �1.35 0.19
Memoryf 0.95 (0.07) 1.00 (0.00) 2.92 0.01
a Proportion of total correct score.b Measure of accuracy.c Measure of biased responding.d Proportion of false positives.e Proportion of false negatives.f Proportion correct recognition of old items.
C. Henquet et al. / Psychiatry Research 133 (2005) 57–6360
sions, and thought disorders were rated with the
PANSS (Kay et al., 1986).
2.3. Data analyses
Data analysis was carried out using SPSS for
Windows Version 10.0. Six source-monitoring indi-
ces were derived. First, a total score of correct
source-monitoring responses was obtained by sum-
ming the number of old items that participants
correctly classified as verbalized or covertly pre-
pared items. Second, the memory score was
calculated by summing the number of correctly
identified old items. To correct for misses, source-
monitoring responses were transformed into propor-
tions of the total number of the 16 questions minus
missed items.
Third, following the Two-High Threshold theory
(Corwin, 1994), we calculated false-alarm rates (i.e.,
erroneous claims of verbalized answers) and missing
rates (i.e., failures to identify verbalized answers). In
keeping with the work of Brebion et al. (1997), we
calculated a discrimination index and a response bias
index, as measures of accurate and biased discrim-
ination between internal and external thoughts,
respectively. In doing so, we took the number of
erroneous answers into account. Thus, the discrim-
ination index was defined as: (number of hits+0.5/
number of targets+1)�(number of false alarms+0.5/
number of distractors+1). Response bias was defined
as: (number of false alarms+0.5/number of distrac-
tors+1)/(1�discrimination index). Note that the
source-monitoring task consisted of 16 targets (ver-
balized answers) and 8 distractors (covertly prepared
answers). Measures were calculated into group means
and compared between groups.
Group differences in source-monitoring perform-
ance, memory capacity, IQ, selective attention, and
symptomatic measures were evaluated with Student
t-tests. In addition, for the combined groups, Pearson
correlations were calculated between the source-
monitoring discrimination index and cognitive and
symptomatic measures. Further, a Pearson correlation
was calculated between source-monitoring perform-
ance and memory score. Multiple regression analysis
was conducted with the discrimination index as the
dependent variable and IQ, level of education,
Stroop interference, and memory as independent
variables.
3. Results
Basic psychometric information about the two
groups is summarized in Table 1. As can be seen,
patients had a lower educational level, lower IQ, but
higher scores on STA than controls. Table 2 shows
source-monitoring indices. Patients had fewer correct
responses (i.e., correct identifications of verbalized
versus internally prepared items) than controls:
t(28)=2.84, Pb0.01. Groups also differed with regard
to a number of Two-High Threshold theory parame-
ters. Thus, relative to controls, patients were signifi-
C. Henquet et al. / Psychiatry Research 133 (2005) 57–63 61
cantly worse at discriminating between targets and
distractors, taking into account the number of errors
they made [i.e., patients scored lower on the discrim-
ination index than controls: t(28)=2.94, Pb0.01].
Furthermore, relative to controls, patients tended to
misclassify imagined thoughts as verbalized answers
[t(28)=�1.87, P=0.07]. However, when overall per-
formance accuracy was taken into account, no
response bias was evident. There were no group
differences with regard to the opposite type of failure
(i.e., misclassifying a verbalized response as an
imagined response). However, patients performed
worse than controls on the memory aspect of the
source-monitoring task [t(28)=2.92, Pb0.01].
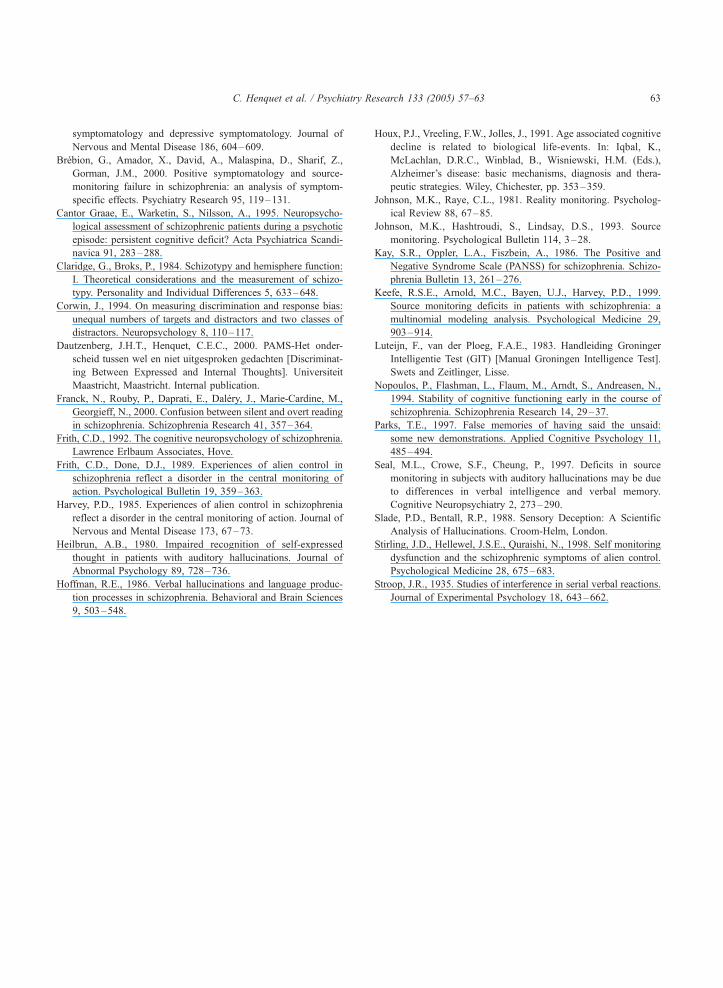
Table 3 shows correlations between the discrim-
ination index derived from the source-monitoring
task, cognitive performance indices, and symptoma-
tology scores for the full sample. The discrimination
index correlated significantly with IQ, selective
attention, and memory capacity. The correlation
between source-monitoring performance and memory
score remained non-significant (r=0.34, P=0.07).
Multiple regression analysis in which IQ, selective
attention, level of education, and memory scores were
entered together showed that only selective attention
and IQ contributed significantly to the source-mon-
itoring discrimination index (R2=0.45). Alone, selec-
tive attention accounted for only 52% of the variance
in the discrimination index. Analyses were repeated to
compare medicated versus unmedicated patients.
Medicated patients showed better performance on
source-monitoring total score [t(13)=2.22, Pb0.05]
and had higher scores on the discrimination index
[t(10)=3.33, Pb0.01]. However, multiple regression
Table 3
Pearson product-moment correlations between source-monitoring
discrimination index, level of education, cognitive performance, and
symptomatology
Discrimination index
r P
Level of education 0.25 0.19
IQ (GIT) 0.44 0.02
Stroop interference �0.52 0.00
Memory 0.37 0.04
STA �0.14 0.49
PANSSa �0.06 0.84
a Positive and Negative Syndrome Scale.
analysis in which IQ, selective attention, and use of
medication were entered together showed that use of
medication did not contribute significantly to the
source-monitoring discrimination index (R2=0.44).
No differences between medicated and unmediated
patients were observed in response bias or memory
capacity. Symptomatology as measured with the STA
and PANSS did not correlate significantly with total
scores on the source-monitoring task (all r’sb0.14; all
P’sN0.49).
4. Discussion
This study demonstrates different patterns of
source-monitoring performance in patients with schiz-
ophrenia and normal controls. Thus, compared with
normal control subjects, patients showed more diffi-
culties in discriminating between covert and
expressed thoughts, a finding that is in accordance
with previous research (e.g., Brebion et al., 1997). We
also found some tentative evidence to suggest that
relative to controls, patients exhibited a stronger
tendency to identify an item as verbalized, when in
fact it was only covertly prepared. However, this
difference was statistically imprecise, which may have
to do with the small sample size. Note that this
tendency is well in line with other studies document-
ing schizophrenic patients’ bias to attribute internal
stimuli to external sources (Brebion et al., 1998, 2000;
Keefe et al., 1999; Franck et al., 2000). Interestingly,
we found no group differences in the opposite
tendency, i.e., the tendency to falsely attribute
verbalized items to imagined thoughts. However,
group differences in source-monitoring errors were
not reflected in response-bias elevations (which
include overall source-monitoring accuracy). This
might indicate that our finding of higher false-alarm
level in patients reflects overall inaccuracy of source-
monitoring performance instead of response bias. On
the other hand, the design of the task might have
elicited floor effects in response bias.
Regression analysis showed that selective attention
as indexed by the Stroop task, more than general
memory capacities, statistically predicts source-mon-
itoring performance. Interestingly, these findings
replicate results reported by Brebion et al. (1996).
Perhaps, deficits in selective attention lead to dis-

C. Henquet et al. / Psychiatry Research 133 (2005) 57–6362
turbances in the primary encoding process of infor-
mation, which could then result in decreased quality
of source monitoring. The fact that IQ also contrib-
uted significantly to source-monitoring performance is
a finding that has been described earlier in schizo-
phrenia research (Seal et al., 1997), although other
studies did not describe such a relationship between
source-monitoring performance and overall cognitive
functioning (Stirling et al., 1998).
Although there were differences in source-mon-
itoring performance between medicated and unmedi-
cated patients, regression analyses showed that
medication was not a pure independent predictor for
source-monitoring performance, which is well in line
with the general notion that memory deficits in
schizophrenia patients have little or nothing to do
with anti-psychotic medication (Aleman et al., 1999).
There is some debate as to whether positive
symptoms are specifically linked to source-monitoring
deficits. Whereas Franck et al. (2000) and Brebion et
al. (2000) found evidence for such a specific link,
Keefe et al. (1999) found schizophrenic patients’
tendency to misclassify imagined words as externally
perceived not related to their positive symptoms. The
current study concurs with that of Keefe et al. (1999)
in that we were also unable to find a significant
correlation between psychosis-related traits or symp-
tomatology, on the one hand, and source-monitoring
performance, on the other. However, a methodological
restriction might underlie this null finding. Because of
our limited sample size, STA scores lacked sufficient
variation, with especially low rates of psychosis-
related traits in the control group. A larger sample
with more variation among trait scores might reveal a
relationship between psychosis-related traits and
source monitoring more clearly.
It has generally been assumed that failures in
source-monitoring performance reflect a state-depend-
ent deficit related to the positive symptoms of
schizophrenia (Frith and Done, 1989; Slade and
Bentall, 1988; Stirling et al., 1998; Brebion et al.,
2000), as opposed to other cognitive deficits which
seem to persist during clinical remission (Nopoulos et
al., 1994; Cantor Graae et al., 1995). Yet, the fact that
straightforward failures in source monitoring were
identified in patients with few acute positive symp-
toms contradicts the alleged state-dependent character
of these deficits.
As argued in the Section 1, many laboratory
experiments on source monitoring expose participants
to situations that rarely occur in everyday life. We feel
that the procedure used in this study has better
ecological validity because it focuses on an everyday
life situation: dDid I just answer your question, or do I
only think I did?T Our results show that patients with
schizophrenia have great difficulty with this task.
In conclusion, internal source monitoring is
impaired in patients with schizophrenia. The defec-
tive memory performance generally found in these
patients does not seem to underlie this impairment,
but selective attention and general intelligence do
contribute to variation in source-monitoring per-
formance. A relation with the severity of positive
symptoms could not be found in this study,
possibly due to limited variation in symptoms in
the current sample. Yet, failures in internal source
monitoring are present in psychotic disorders
independent of positive psychotic symptoms, indi-
cating that these deficits are at least to some extent
part of an enduring cognitive vulnerability in
schizophrenia.
Acknowledgment
The authors thank Joke Conings, MSc for her help
in collecting and analyzing the data.
References
Aleman, A., Hijman, R., de Haan, E.H., Kahn, R.S., 1999. Memory
impairment in schizophrenia: a meta-analysis. American Journal
of Psychiatry 156, 1358–1366.
American Psychiatric Association, 1994. DSM-IV: Diagnostic and
Statistical Manual of Mental Disorders. 4th ed. American
Psychiatric Association, Washington, DC.
Bentall, R.P., 1990. The illusion of reality: a review and integration
of psychological research on hallucinations. Psychological
Bulletin 107, 82–95.
Brebion, G., Smith, M.J., Gorman, J.M., Amador, X., 1996. Reality
monitoring failure in schizophrenia: the role of selective
attention. Schizophrenia Research 22, 173–180.
Brebion, G., Smith, M.J., Widlocher, D., 1997. Discrimination and
response bias in memory: effects of depression severity and
psychomotor retardation. Psychiatry Research 70, 95–103.
Brebion, G., Smith, M.J., Amador, X., Malaspina, D., Gorman,
J.M., 1998. Word recognition, discrimination accuracy, and
decision bias in schizophrenia: association with positive
C. Henquet et al. / Psychiatry Research 133 (2005) 57–63 63
symptomatology and depressive symptomatology. Journal of
Nervous and Mental Disease 186, 604–609.
Brebion, G., Amador, X., David, A., Malaspina, D., Sharif, Z.,
Gorman, J.M., 2000. Positive symptomatology and source-
monitoring failure in schizophrenia: an analysis of symptom-
specific effects. Psychiatry Research 95, 119–131.
Cantor Graae, E., Warketin, S., Nilsson, A., 1995. Neuropsycho-
logical assessment of schizophrenic patients during a psychotic
episode: persistent cognitive deficit? Acta Psychiatrica Scandi-
navica 91, 283–288.
Claridge, G., Broks, P., 1984. Schizotypy and hemisphere function:
I. Theoretical considerations and the measurement of schizo-
typy. Personality and Individual Differences 5, 633–648.
Corwin, J., 1994. On measuring discrimination and response bias:
unequal numbers of targets and distractors and two classes of
distractors. Neuropsychology 8, 110–117.
Dautzenberg, J.H.T., Henquet, C.E.C., 2000. PAMS-Het onder-
scheid tussen wel en niet uitgesproken gedachten [Discriminat-
ing Between Expressed and Internal Thoughts]. Universiteit
Maastricht, Maastricht. Internal publication.
Franck, N., Rouby, P., Daprati, E., Dalery, J., Marie-Cardine, M.,
Georgieff, N., 2000. Confusion between silent and overt reading
in schizophrenia. Schizophrenia Research 41, 357–364.
Frith, C.D., 1992. The cognitive neuropsychology of schizophrenia.
Lawrence Erlbaum Associates, Hove.
Frith, C.D., Done, D.J., 1989. Experiences of alien control in
schizophrenia reflect a disorder in the central monitoring of
action. Psychological Bulletin 19, 359–363.
Harvey, P.D., 1985. Experiences of alien control in schizophrenia
reflect a disorder in the central monitoring of action. Journal of
Nervous and Mental Disease 173, 67–73.
Heilbrun, A.B., 1980. Impaired recognition of self-expressed
thought in patients with auditory hallucinations. Journal of
Abnormal Psychology 89, 728–736.
Hoffman, R.E., 1986. Verbal hallucinations and language produc-
tion processes in schizophrenia. Behavioral and Brain Sciences
9, 503–548.
Houx, P.J., Vreeling, F.W., Jolles, J., 1991. Age associated cognitive
decline is related to biological life-events. In: Iqbal, K.,
McLachlan, D.R.C., Winblad, B., Wisniewski, H.M. (Eds.),
Alzheimer’s disease: basic mechanisms, diagnosis and thera-
peutic strategies. Wiley, Chichester, pp. 353–359.
Johnson, M.K., Raye, C.L., 1981. Reality monitoring. Psycholog-
ical Review 88, 67–85.
Johnson, M.K., Hashtroudi, S., Lindsay, D.S., 1993. Source
monitoring. Psychological Bulletin 114, 3–28.
Kay, S.R., Oppler, L.A., Fiszbein, A., 1986. The Positive and
Negative Syndrome Scale (PANSS) for schizophrenia. Schizo-
phrenia Bulletin 13, 261–276.
Keefe, R.S.E., Arnold, M.C., Bayen, U.J., Harvey, P.D., 1999.
Source monitoring deficits in patients with schizophrenia: a
multinomial modeling analysis. Psychological Medicine 29,
903–914.
Luteijn, F., van der Ploeg, F.A.E., 1983. Handleiding Groninger
Intelligentie Test (GIT) [Manual Groningen Intelligence Test].
Swets and Zeitlinger, Lisse.
Nopoulos, P., Flashman, L., Flaum, M., Arndt, S., Andreasen, N.,
1994. Stability of cognitive functioning early in the course of
schizophrenia. Schizophrenia Research 14, 29–37.
Parks, T.E., 1997. False memories of having said the unsaid:
some new demonstrations. Applied Cognitive Psychology 11,
485–494.
Seal, M.L., Crowe, S.F., Cheung, P., 1997. Deficits in source
monitoring in subjects with auditory hallucinations may be due
to differences in verbal intelligence and verbal memory.
Cognitive Neuropsychiatry 2, 273–290.
Slade, P.D., Bentall, R.P., 1988. Sensory Deception: A Scientific
Analysis of Hallucinations. Croom-Helm, London.
Stirling, J.D., Hellewel, J.S.E., Quraishi, N., 1998. Self monitoring
dysfunction and the schizophrenic symptoms of alien control.
Psychological Medicine 28, 675–683.
Stroop, J.R., 1935. Studies of interference in serial verbal reactions.
Journal of Experimental Psychology 18, 643–662.
Related Documents











