/ 1 / CONFRONTING PLASMODIUM VIVAX MALARIA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
/ 1 /
CONFRONTINGPLASMODIUM VIVAX MALARIA

© World Health Organization 2015
All rights reserved. Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications – whether for sale or for non-commercial distribution – should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Map production: WHO Global Malaria Programme.
Design and layout: ACW, London, UK (www.acw.uk.com)
Photo credits | Front cover (left/right), back cover and pp. 4, 5 (right), 7, 9: © The Global Fund/John Rae | p. 1: © MMV/Damien Schumann | p. 5 (left): © The Global Fund/Kuni Takahashi | p. 6: © WHO/SEARO/Nimal Garnage | p. 8: © DFID
Please consult the WHO Global Malaria Programme website for the most up-to-date version of all documents (http://www.who.int/malaria).
Printed by the WHO Document Production Services, Geneva, Switzerland.
WHO/HTM/GMP/2015.3

/ 1 /
1Plasmodium vivax is one of �ve species of Plasmodium that can cause malaria in human beings. Although P. falciparum is responsible for the majority of cases and deaths from malaria, P. vivax has a wider geographical range and is responsible for almost half the cases of malaria outside Africa.
In May 2015, the World Health Assembly endorsed the most ambitious targets for malaria control since the eradication era – namely to eliminate malaria from 35 countries and reduce case incidence and mortality rates by 90% globally.1 P. vivax presents a major challenge to achieving these targets; in 2013, it was responsible for 16 million cases globally. It predominates in countries that are prime candidates for elimination, accounting for more than 70% of cases in countries with fewer than 5000 cases of malaria each year. Not only does P. vivax present a barrier to elimination, it can also cause severe disease; severe cases and deaths due to P. vivax malaria have been reported from all endemic regions.
WHY IS ACTIONAGAINST P. VIVAX MALARIA NEEDED?
1. WHO, Global Technical Strategy for Malaria 2016–2030. Geneva, World Health Organization (WHO). 2015 (http://who.int/malaria/areas/global_technical_strategy/en/, accessed 30 June 2015).

/ 2 /
More than a third of the world’s population, mostly in Asia and Latin America, is at risk of infection with P. vivax malaria.
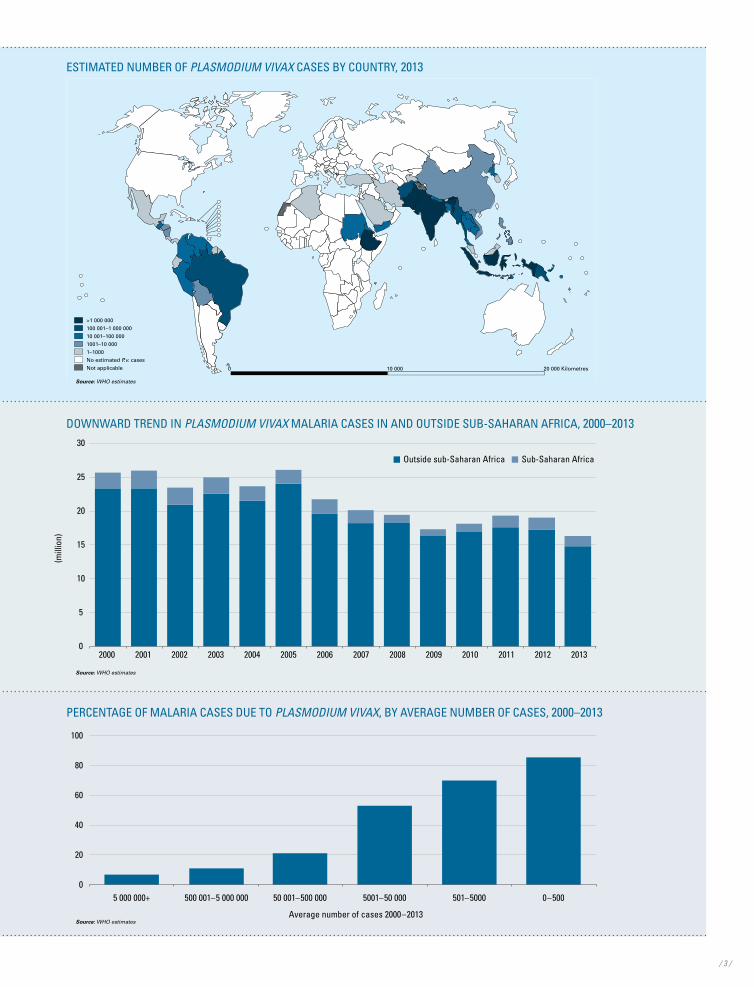
1/3P. vivax is by far the most widespread of the five malaria parasites that infect people. In 2013, it was estimated to be responsible for more than one million malaria cases in four countries (Ethiopia, India, Indonesia and Pakistan).
P. vivax malaria predominates in countries that are prime candidates for elimination. 70%
The parasite accounts for more than 70% of malaria cases in countries with fewer than 5000 cases each year.
Despite tremendous progress in reducing P. vivax malaria since 2000, there were 16 million cases globally in 2013.
16 mEven though the number of P. vivax malaria cases fell by 35% compared to 2000, P. vivax is still responsible for almost half the number of malaria cases outside Africa.
/ 3 /
PERCENTAGE OF MALARIA CASES DUE TO PLASMODIUM VIVAX, BY AVERAGE NUMBER OF CASES, 2000–2013
0
20
40
60
80
100
5 000 000+ 500 001–5 000 000 50 001–500 000 5001–50 000 501–5000 0–500
Average number of cases 2000–2013Source: WHO estimates
ESTIMATED NUMBER OF PLASMODIUM VIVAX CASES BY COUNTRY, 2013
>1 000 000
100 001–1 000 000
10 001–100 000
1001–10 000
1–1000
No estimated P.v. cases
Not applicable 0 10 000 20 000 Kilometres
Source: WHO estimates
DOWNWARD TREND IN PLASMODIUM VIVAX MALARIA CASES IN AND OUTSIDE SUB-SAHARAN AFRICA, 2000–2013
(mill
ion)
0
5
10
15
20
25
30
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Outside sub-Saharan Africa Sub-Saharan Africa
Source: WHO estimates

/ 4 // 4 /
P. VIVAX MALARIA POSES MULTIPLE CHALLENGES
2P. vivax malaria can be more dif�cult to control than P. falciparum for several reasons related to its biology or the behaviour of mosquitoes that carry it.

/ 5 /
• It can survive in cooler climates. Whereas P. falciparum is confined to tropical zones, P. vivax can develop and survive in the relatively cooler climates of more temperate countries and therefore has a wider geographical range.
• It is less responsive to conventional methods of vector control. In many of the areas where P. vivax is common, mosquitoes bite early in the evening, obtain blood meals outdoors and rest outdoors. Thus, tools such as insecticide-treated mosquito nets (ITNs), which work well against night-biting and indoor-feeding mosquitoes, can be less effective in reducing P. vivax malaria.
• It is more difficult to detect using current diagnostic techniques. Compared to P. falciparum, the number of parasites circulating in the blood of a person infected with P. vivax malaria is typically low. Therefore, P. vivax infections may be missed, even if a patient presents for treatment. The parasite also has a dormant liver stage that cannot be detected by current diagnostic tools. Hence, there may be a large reservoir of people who are infected with P. vivax but are unaware of their condition.
• A single infection can give rise to multiple episodes of malaria. Even in the absence of another mosquito bite, in those infected with P. vivax, the dormant liver stage can awaken and can trigger multiple episodes of malaria. These relapses not only cause further illness to the individual, they also provide an opportunity for the parasite to be picked up by mosquitoes and transmitted to others.
• Treatment of liver-stage parasites requires a 14-day course of primaquine. Only one drug, primaquine, is effective against dormant liver parasites. The treatment for this stage of the disease involves the patient taking tablets every day for 14 days, even though the person may no longer be experiencing symptoms of disease. In resource-poor areas where P. vivax prevails, many patients have dif�culty complying with such a lengthy treatment regimen.
• Primaquine treatment can produce serious side-effects.Patients who have a severe deficiency of the enzyme glucose-6-phosphate dehydrogenase (G6PD) are susceptible to potentially life-threatening destruction of blood cells while taking primaquine. However, current tests for G6PD de�ciency are complex and relatively expensive; thus, many clinicians are reluctant to prescribe primaquine to patients whose G6PD status is unknown. In addition, primaquine cannot be used in pregnant women and infants because of the risk of G6PD de�ciency. In the absence of treatment, these populations are prone to multiple relapses.

/ 6 // 6 /
WHAT SHOULD BE DONE AGAINST P. VIVAX ?
3Successful control and elimination of P. vivax requires action on three fronts: strengthening malaria programmes, developing new tools, and enhancing �nancing and political commitment.

/ 7 /
STRENGTHENED MALARIA PROGRAMMESMany of the strategies to control P. vivax malaria are the same as those used with P. falciparum malaria; for example, using vector control to reduce transmission by the mosquito vector (from humans to mosquitoes, and from mosquitoes to humans); using chemoprevention to prevent establishment of infections in humans; and providing accessible health services that can rapidly detect, diagnose and treat malaria infections. However, successful control of P. vivax malaria calls for additional interventions; in particular:
• targeting outdoor-biting and outdoor-resting mosquitoes, where such mosquitoes represent the main source of transmission;
• ensuring that microscopy services are able to detect low-density P. vivax infections, or that bivalent rapid diagnostic tests are used in areas where both P. falciparum and P. vivax are found;
• treating liver stages as well as blood stages; and
• testing all patients for G6PD deficiency before administering primaquine (where possible).
Consideration of P. vivax needs to be re�ected in global, regional and national plans for malaria control. These plans should be monitored at regular intervals through P. vivax-specific indicators on programme coverage and disease incidence.
DEVELOPMENT OF NEW TOOLSA more effective response to P. vivax will require new tools that will help to reduce P. vivax transmission, and increase the ability of malaria programmes to detect and treat infections. There is a particular need for tools against the dormant liver (hypnozoite) stage, such as:
• a test that is both sensitive enough to confirm the presence of hypnozoites in a patient’s liver and specific enough to confirm their absence; such a test could inform decisions about the management of a vivax malaria, and be used for epidemiological assessment of the prevalence of P. vivax infection in a given area;
• a test for G6PD deficiency that can be used where patients seek treatment, to break down a significant barrier to treatment with primaquine; and
• a drug against the liver stage that is effective, does not have significant side-effects and is suitable for use in all population groups.
ENHANCED FINANCING AND POLITICAL COMMITMENTThere is a need for international donors and domestic governments to invest in the additional measures required for control of P. vivax, and to continue investment even when malaria is reduced to low levels or eliminated. Also, those funding research will need to prioritize investments in P. vivax malaria research, to reduce the obstacles to P. vivax malaria elimination.
A MORE EFFECTIVE RESPONSE TO P. VIVAX WILL REQUIRE NEW TOOLS THAT WILL HELP TO REDUCE P. VIVAX TRANSMISSION AND INCREASE THE ABILITY TO DETECT AND TREAT INFECTIONS.
/ 8 /
WHAT CAN BE GAINED BY TAKING ACTION AGAINST P. VIVAX ?
4A comprehensive response to P. vivax malaria will relieve some of the most vulnerable populations of a signi�cant illness that disrupts schooling and work, and can be fatal. Such a response will strengthen health systems, boosting their capacity to improve the treatment of other febrile illnesses and their ability to respond to future public health threats.
Malaria interventions are highly cost effective, and provide one of the highest returns on investment in public health. They help to alleviate poverty, improve equity and contribute to overall development. If P. vivax malaria is conquered,not only will international targets to eliminate malaria from 35 countries by 2030 be achieved, but a pathway will be set for the eventual eradication of this ancient disease.
/ 8 /

/ 9 // 9 /

For further information, please refer to Control and elimination of Plasmodium vivax malaria – A technical brief published by the WHO Global Malaria Programme in July 2015 and available at http://www.who.int/malaria/publications/atoz/9789241509244/en/.
Global Malaria ProgrammeWorld Health Organization20, Avenue Appia CH-1211 Geneva 27Web: www.who.int/malariaEmail: [email protected]
Related Documents











