CONFIDENTIAL AND PROPRIETARY ©2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective Xtend Healthcare Advanced Revenue Solutions ICD-10 The Route to Readiness Linda Corley, BS, MBA, CPC Vice President – Compliance 706 577-2256 lcorley@xtendhealthcare. net

CONFIDENTIAL AND PROPRIETARY ©2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners. Xtend.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CONFIDENTIAL AND PROPRIETARY
©2015 Xtend Healthcare, LLC. All rights reserved.All registered trademarks are the property of their respective owners.
Xtend Healthcare Advanced Revenue Solutions
ICD-10 The Route to Readiness
Linda Corley, BS, MBA, CPCVice President – Compliance706 [email protected]
2 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Agenda
• Overview of current state• Review of ICD-10 basics
– Who, What, When, Why, How• Steps to take to ensure you are fully engaged and
on the right path to readiness– Governance– Project Management– Impact Assessment– Dual Coding Plan
ICD-10

3 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
ICD-10 a Call to Action
• Now is the time to prepare for ICD-10!• The differences are critical – not just another coding change.• Define facility or practice specific needs and PLAN• Assessment will provide outline for achievement of goals• Prepare tasks / activities for implementation
– Designate “owner” for completion of all required tasks– Staff members, payors, vendors, physicians
• Lead!• Manage progress, and “re-group” when necessary• Reach ICD-10 “readiness” by September 30, 2015!• Use September 1 – 30 for “contingency” planning

4 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Where Are We Now?
• ICD-9-CM and PCS required for use in transactions– Diagnoses– Inpatient Hospital Procedures
• ICD-9-CM has been in use since 1979• Required since October 2003 by HIPAA
– required by HIPAA to use a standard code set to indicate diagnoses and procedures on transactions.
• For diagnoses, we use the ICD-9-CM code set. • For inpatient hospital procedures, we use the ICD-9-CM
procedure code set. • For other types of procedures, we use CPT or HCPCS codes. • We will be discussing the soon-to-be required ICD-10-CM
codes for diagnoses, and ICD-10-PCS codes for inpatient hospital procedures.
• There are no plans to radically change the CPT or HCPCS code sets at this time.

5 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
What Is ICD-10?
• ICD-10 is the updated version of the ICD-9 codes:– Diagnoses for all providers (ICD-10-CM)– Inpatient hospital procedures (ICD-10-PCS)– In addition to coding – ICD-10 in the US will determine
reimbursement!• ICD-10-CM originated with the World Health Organization
(WHO).• Several countries have taken this code set and modified it for
use in their medical systems. • The US, through the National Center for Health Statistics, has
developed the ICD-10-CM (or clinical modification) of the code set for use in this country.
• The Centers for Medicare and Medicaid Services has created a new code set, ICD-10-PCS, for use with inpatients.
• These code sets are considered classification code sets.

6 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
So, What Is the Big Deal with ICD-10?
• Codes change every year anyway!• In our systems, we generally update code sets once a year,
sometimes more often. – We have been making these changes on a regular basis. – As new codes are added and others are retired, we have
been updating our procedures and systems to take account of the code changes.
– Furthermore, we are presently working on the implementation of updated HIPAA transactions (X12 version 5010, NCPDP version D.0).
• So, why is there so much attention being focused on implementing these new code sets?
• Why not business as usual?

7 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Difference in Organization
• ICD-10-CM has 21 chapters, compared to the 17 in ICD-9-CM• Disease of the sense organs (eyes and ears) have been
separated from the nervous system diseases and have their own ICD-10-CM Chapter
• Injuries are grouped by site (instead of type)• Postoperative complications are incorporated into the
procedure-specific body system• Addition of 6th character in some chapters• Addition of 7th character for OB, Injuries, and External Cause
of Injuries• Addition of placeholder X

8 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners8
= 13,000 Codes = 68,000 Codes
Comparison of ICD-9-CM and ICD-10-CM

9 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Comparison of ICD-9-CM and ICD-10-CM
ICD-9-CM Codes ICD-10-CM Codes
Pressure ulcer codes 9 codes
707.00 – 707.09
Pressure ulcer codes 125 codes
L89.0-L89.94
Codes:707.0 Pressure ulcer 707.00 - unspecified site 707.01 - elbow 707.02 - upper back 707.03 - lower back 707.04 - hip 707.05 - buttock 707.06 - ankle 707.07 - heel 707.09 - other site
Code Examples:L89.131 – Pressure ulcer of right lower back, stage IL89.132 – Pressure ulcer of right lower back, stage IIL89.133 – Pressure ulcer of right lower back, stage IIIL89.134 – Pressure ulcer of right lower back, stage IVL89.139 – Pressure ulcer of right lower back, unspecified stageL89.141 – Pressure ulcer of left lower back, stage I……

10 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• Combination codes for conditions and common symptoms or manifestations– I25.110 Atherosclerotic heart disease of native coronary
artery with unstable angina pectoris
10
• Added Laterality– H60.332 Swimmer's ear, left ear– M94.211 Chondromalacia, right shoulder
New Features in ICD-10-CM
11 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• Added 7th Characters for Episode of Care
– M80.051A, Age-related osteoporosis with current pathological fracture, right femur, initial encounter for fracture
• The appropriate 7th character is to be added to each code from category M80:
A - initial encounter for fractureD - subsequent encounter for fracture with routine healingG - subsequent encounter for fracture with delayed healingK - subsequent encounter for fracture with nonunionP - subsequent encounter for fracture with malunionS - sequela
11
New Features in ICD-10-CM – 7th Character

12 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• Inclusion of trimester in OB codes (and elimination of the 5th digit for episode of care)
– O91.111 Abscess of breast associated with pregnancy, first trimester
– O91.112 Abscess of breast associated with pregnancy, second trimester
– O91.113 Abscess of breast associated with pregnancy, third trimester
– O91.119 Abscess of breast associated with pregnancy, unspecified trimester
12
New Features in ICD-10-CM – 7th Character

13 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Major Changes from ICD-9 to ICD-10
• Requires changes to almost all clinical and administrative systems
• Requires changes to business processes• The updated code sets will allow, and in fact will require,
significant changes in the way services are reimbursed, and in the way that coverage (medical necessity ) is determined for services.– National Coverage Determinants (NCD’s) and Local
Coverage Determinants (LCD’s) are not slated to be published until sometime in the spring.
• Will enable significant improvements in patient care management, public health reporting, research, and quality measurement
14 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Specific Changes to Procedure Codes
• Let’s now turn our attention to the ICD-10-PCS procedure code set.
• This is a new code set developed in the United States by the Centers for Medicare and Medicaid Services (CMS). – It is not used outside of this country.– It is not related to the ICD-10-CM code set.
• This code set will only be used to report procedures on inpatient hospital claims.

15 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Structure of ICD-10 PCS
As you can see, the position designates a specific meaning.
This is consistent throughout the entire code set.
For any ICD-10-PCS code, the 4th position, for example, always refers to the body part involved in the procedure.

16 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Comparison of Procedural Coding from ICD-9 to ICD-10
16
ICD-9-PCS ICD-10 -PCS
3-4 numbers in length 7 alpha-numeric characters in length
Approximately 3,000 codes Approximately 87,000 available codes
Based on outdated technology Reflects current usage of medical terminology and devices
Limited space for adding new codes Flexible for adding new codes
Lacks detail Very specific
Lacks laterality Has laterality
Generic terms for body parts Detailed descriptions for body parts
Lacks descriptions of methodology and approach for procedures
Provides detailed descriptions of methodology and approach for procedures
Lacks precision to adequately define procedures
Precisely defines procedures with detail regarding body part, approach, any device used, and qualifying information
17 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• ICD-10-PCS has four basic characteristics:
– Allows for unique coding of procedures (easy to distinguish differences)
– Room for expansion, as new procedures and devices are used.
– Standardized terminology that reflects the current practice of medicine.
– Consistency in coding from chapter to chapter
Characteristics of ICD-10 PCS
18 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
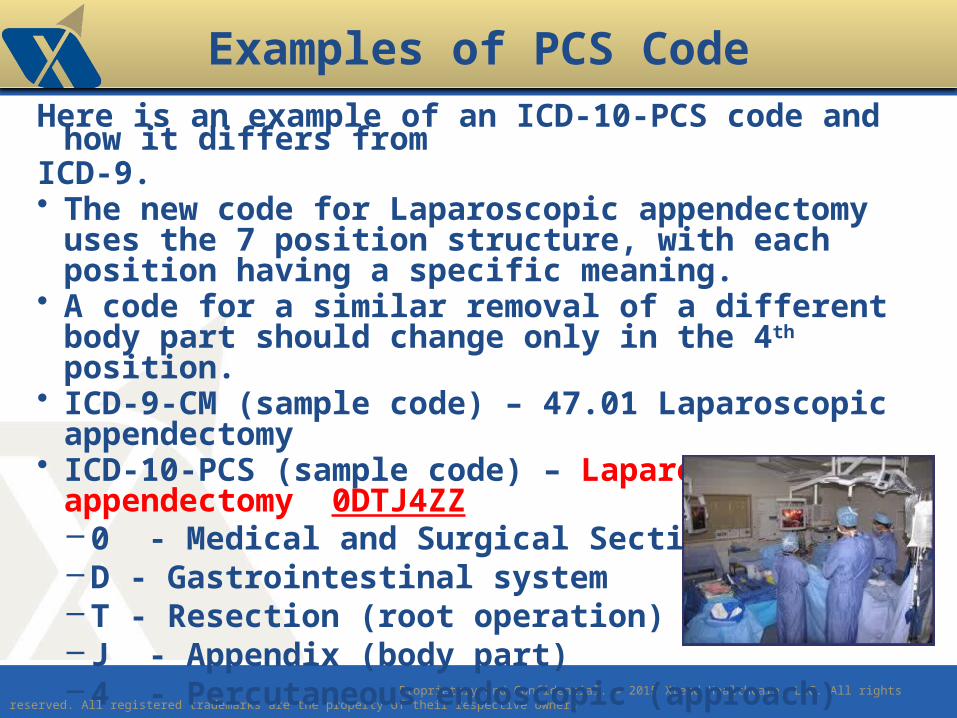
Here is an example of an ICD-10-PCS code and how it differs from ICD-9.• The new code for Laparoscopic appendectomy uses the 7
position structure, with each position having a specific meaning. • A code for a similar removal of a different body part should
change only in the 4th position.• ICD-9-CM (sample code) – 47.01 Laparoscopic appendectomy• ICD-10-PCS (sample code) – Laparoscopic appendectomy
0DTJ4ZZ– 0 - Medical and Surgical Section– D - Gastrointestinal system– T - Resection (root operation)– J - Appendix (body part)– 4 - Percutaneous endoscopic (approach)– Z - No device– Z - No qualifier
Examples of PCS Code
19 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• The practice of medicine has changed dramatically since ICD-9 was published
– Many new medical conditions discovered– Many new treatments developed– Many new types of medical devices have been placed into service– Has run out of room to allow for code expansion
• The ICD-9 code set was not designed to capture all of these changes, and has become bogged down with many types of modifications to attempt to capture information.
Why Make the Change to ICD-10?

20 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• The ICD-10 code set – Is much better at describing the current practice of
medicine – Uses today’s medical terminology– Has the flexibility to adapt as medicine changes– Allows for code set expansion to introduce new
diagnoses and procedures as medicine continues to evolve– Allows us to compare our data on an international level
(since most other developed countries are already using
ICD-10-CM)
Why Make the Change to ICD-10?

21 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• There is an increased emphasis on the use of reported medical information for a multitude of tasks. We look to manage individual care, to place patients in special targeted programs, to track population disease patterns, and identify biological threats.• We are changing the way we look at providers, attempting to measure not only cost of care, but quality of care in an attempt to manage health care expenditures. • Payors are asking providers to justify increasing health care costs by showing improved outcomes and improved health of patient populations.
– ICD-10-CM/PCS allows for greater transparency to satisfy all of our reporting requirements and scrutiny outlined above.
Why Make the Change to ICD-10?

22 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Revenue Cycle Processes Impacted
• Scheduling• Eligibility Verification • Admitting/Registration• Financial Counseling• Utilization Management• Health Information Management• Patient Financial Services (prebill edits, payments, claims
status follow ups, etc)• Coordination of Benefits
22
The list goes on and on and may be more specific based on organizational structure.
23 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Clinical Processes Impacted
• Systems used to document clinical findings will be modified or replaced to accommodate new coding language
• Any treating provider who documents in your legal medical record will impacted, required to document to the highest degree of specificity
• Any treating provider who refers to your facility will be impacted, required to document to the highest degree of specificity all orders and referrals– Failure to be specific will result in costly rework and
delays in care.

24 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Consider the “Consequences”!
• Claims for all outpatient and physician services, and hospital inpatient procedures provided on or after October 1, 2015, must use ICD-10-CM diagnosis and inpatient procedure (ICD-10-PCS) codes. Claims that do not use ICD-10 diagnosis and inpatient
procedure codes cannot be processed and paid!• It is important to note, however, that claims for services and
inpatient procedures provided before October 1, 2015, must use ICD-9 codes even if they are submitted after the compliance date.
• Consider the need to start dual coding ICD-9 and ICD-10 in June – July 2015.

25 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Establish Governance Committee
Project Management
Impact Assessments
Information Systems
Documentation Needs
Education Needs
Coding Policies
Gap Analysis and Contingency Plan(s)

26 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Project Management
• Governance = Management Plan• Develop ICD-10 implementation strategy and oversee
implementation process (this committee is responsible for overseeing all of the steps in the ICD-10 transition process, but may designate other individuals to complete specific tasks).
Interviews of clinical and financial leadersSurveys of team members who perform processesFacility walkthroughsDocumentation ReviewIT System inventory and review
• Formulate transition strategies and identify goals. • Develop organization’s ICD-10 implementation strategy and
identify actions, persons responsible, and deadlines for the various tasks required to complete the transition.
• Develop communication plan for business associates and other external entities.

27 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Project Management Budget
• How much will preparedness and implementation cost?• How do we spread out the cost?
– Departments and areas affected• IT assessment internal (hourly $?)
– IT assessment with external users, payors, BAs– IT programming– IT testing
• Education and awareness costs• Impact to productivity – Patient Access (Registration and
Scheduling), Patient Care Management, Coding, Billing and Collections
• Impact to Cash, AR and DNFB

28 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Identify all ICD‐Transition Expenses
• Software modifications (costs for in‐house as well as vendor system changes)– Education (both coding staff as well as other staff members
needing education)– Hardware/software upgrades– Testing related costs– Staff time
• Temporary or contract staffing to assist with increased work resulting from the transition, such as coding/billing backlogs, IT support, or coding accuracy review– Consulting services to assist with transition– Report redesign (and development of new reports)– Reprinting of paper forms

29 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Identify all ICD‐10 Transition Expenses
• Data conversion– Maintenance of dual code sets– Additional software or other tools/resources to facilitate the
ICD-10 transition (such as an electronic mapping tool) or improve operational processes
• Identify departmental budget(s) responsible for each transition cost, including systems changes, hardware/software upgrades, and education
• Estimate the amount of contingency and reserve funds required for the ICD-10 transition
• Allocate ICD-10 implementation costs across multiple years• Identify other projects that will be competing for resources
(financial, personnel) during the ICD-10 transition period.• Update budget estimates as needed after completing other
ICD-10 planning and impact assessment activities
30 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Project Management
Develop an Internal Communication Plan– Meetings Dates for Steering Committee– Initial Awareness Communication
• Kickoff of ICD-10 Preparation• E-mail blasts to all employees• ICD-10 Q&A dedicated e-mail box
ICD 10

31 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Project Management
Timeline– Conduct Impact Assessment– Send out initial communication to all staff members,
including physicians– Steering Committee meeting for discussion of assessment
results, and to develop action plan(s)– Bi-weekly meetings / conference calls with Steering
Committee to assess progress of action plan.– Scheduled (date specific) educational sessions with affected
staff members identified by job role / position– Conduct dual coding chart reviews July –August with
continual coder education. – Gap Analysis to be performed prior to September 1st.

32 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Impact Assessment
To get a facility or physician practice started on ICD-10 Preparation – conduct a detailed “patient flow” Impact Assessment –
• Follow a patient through an outpatient service / visit
Identify each revenue cycle process that utilizes a diagnosis
code
Admissions and Scheduling (Patient Access)• Pre-patient scheduling• Physician order receipt and review • Insurance verification, authorization, medical
necessity• Pre-registration
33 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Impact Assessment
• Identify each revenue cycle process that utilizes a diagnosis code
Providing the outpatient service while the patient is on site – – documentation, – charge capture (charge tickets)
Coding
Billing
Account follow-up to payment
Identify each system, clearinghouse, ancillary interface utilized
• Follow a patient through an inpatient stay

34 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Encoding softwareCase mix systemsMedical record abstractingBilling systemsRegistration and scheduling systemsAccounting systemsDecision support systemsClinical systemsUtilization managementQuality management
Information Systems Affected
Case managementClinical protocolsTest ordering systemsClinical reminder systemsPerformance measurement systemsMedical necessity softwareDisease management systemsProvider profiling systemsAggregate data reporting

35 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Documentation Needs
• The increased specificity of the ICD-10 codes requires more detailed clinical documentation in order to code some diagnoses to the highest level of specificity.
• There are “unspecified” codes in ICD-10-CM for those instances when medical record documentation is not available to support more specific codes.• Unspecified codes = lower payments• May not meet medical necessity for services
• The benefits of ICD-10 can not be realized if non-specific codes are used rather than taking advantage of the specificity ICD-10 offers.

36 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Improving Documentation
• Conduct medical record documentation assessments– Evaluate records to determine adequacy of
documentation to support the required level of detail in new coding systems
• Implement a documentation improvement program to address deficiencies identified during the review process– Educate providers about documentation requirements
for the new coding system through specific examples– Emphasize the value of more concise data capture for
optimal results and better data quality

37 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Assessment of Educational Needs
Identify who will require education:Coding professionalsProvidersBilling personnelClinical personnelAdministrative staff and
ManagementResearchers
Determine what type and level of education each job role will need.Assess the current level of
coder education and experience.
Assess the level of knowledge necessary per person/role based on job responsibilities.
Determine the best method of education.

38 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Coder Training and Education
• The DHHS recommends inpatient/hospital coders receive 50 hours of training and outpatient coders receive 10 hours of training.
• AHA/AHIMA anticipates that a maximum of 16 hours of training may be sufficient for experienced coding professionals on ICD-10-CM only.– 6 hours learning the fundamentals (structure, coding
conventions, guidelines and how ICD-10 is different)– 6 hours in more intensive training applying the conventions
and guidelines– 4 hours practicing applying codes to typical encounters
39 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Physician Training
• DHHS agrees that some physicians will want intensive training on ICD-10 but some will seek “awareness training.”
• One national study estimates 8 hours of intensive physician training.
• Another study predicts 12 hours of physician training in both the code set and documentation procedures.
• AHIMA believes most physicians would want no more than 4 hours of training.

40 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Implementation Gap Analysis
• A Gap Analysis will need to be performed no later than September 1, 2015, to determine any potential areas that will be negatively affected; and
• A contingency plan will need to be developed, approved and implemented.
ICD 10

41 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Sample 1st Quarter 2015
• Financial Awareness Training for relevant staff• Review readiness with vendor software;
– verify when they plan to make their ICD-10 updates available in the clinical and financial software (State Medicaid agencies;
– MAC; – Managed Care Organizations, etc.)
• Facilities order ICD-10 Manuals or electronic updates so they are available for training.
• Determine the level of training for all areas of the hospital.• Begin weekly ICD-10 Fact Sheets via e-mail blast to
appropriate staff.
42 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Payor Impacts
• Coverage determinations• Payment determinations• Medical review policies• Plan structures• Statistical reporting• Actuarial projections• Fraud and abuse monitoring• Quality measurements
ICD 10?

43 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Provider Impacts• We rely on providers to accurately code claims so that
processing decisions can be made. • First, providers must learn the new code set. • The first step to accurate coding is for the documentation to
reflect what the provider has observed or provided. • Coding must be supported by medical documentation. • Studies of the required documentation have indicated that
more documentation is required to support the increased specificity of the code set.
• We should expect providers to have to spend about 15% more time on asking questions, observing, and documenting their findings to support the ICD-10-CM code set.
• Even with increased documentation, we can expect, with better coding, an increase in denials or pending claims, and the need for providers to submit additional documentation to support the codes.

44 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Provider Impacts
• As we replace ICD-9 codes with ICD-10 codes, health plans (Medicare and Medicaid State included) will be revising coverage policies, medical review procedures, and plan design and reimbursement schedules to take advantage of the better information being collected.
• It is expected that providers will need to change their processes to adapt to the changes, and that there may even be a need to discuss treatment changes with patients.
• For example, certain conditions may not be covered to the same extent if they can be better identified in terms of specificity.
• Payments may also change.
45 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Provider Impacts
• Documentation of diagnoses and procedures– Codes must be supported by medical documentation– ICD-10-CM codes are more specific– Requires more documentation to support codes– Expect a 15% increase in documentation time (per AAPC)– Revenue Impacts of specificity
o Denialso Additional Documentation
• Coverage and Payment– New coding system will mean new coverage policies, new
medical review edits, new reimbursement schedules– Changes will be made to accommodate increased specificity– May need to discuss changes with patients

46 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Provider Impacts
• Relationship with Plans–Coding more specific and includes severity /
intensity of service–Changes will be based on new coding, coverage, and
reimbursement–Difficult to measure what the changes will mean to
overall reimbursement–Challenging to understand and plan now for cash
variances!
47 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Provider Impacts
• Billing and Eligibility Transactions– Updated transactions include support for ICD-10– New codes mean more specificity– How smooth is the transition?– Expect increased reject, denials, and pends as both
plans and providers get used to new codes• Laboratory and Pharmacy
– Will need specific ICD-10-CM codes for laboratory orders
– Expect coverage changes– Need to support the tests/drugs ordered– Transition issues for prior authorizations

48 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Provider Impacts
• There is an additional transition issue for prior authorization or prescription refills.
• If the original order or prescription was done with an ICD-9 code (prior to Oct 1, 2015), it must be updated for any service delivered on or after Oct 1, 2015.
• The lab or pharmacy must be able to submit an ICD-10 code once a service is provided on or after Oct 1, 2015.
• Quality Measures / Pay for Performance (P4P)• New measures need to be determined based on ICD-10-CM
codes– Must renegotiate with provider groups– Difficult to measure impact of change – Is it because of code set
or because of changes in the underlying practice?

49 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Provider Impacts
• Let’s talk now about the recent efforts to measure quality and adjust payments based on the performance of providers.
• Many of the performance measures are based on diagnosis codes, or at least are collected based on the diagnosis of the patient.
• With our changing code set, these measures must be revised.
• They are often contentious, and are usually discussed with provider groups.
• Efforts should be underway soon to revise these quality measures.

50 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Operational Steps
Implementation and Operational Steps• Training – not just coders
– Program staff– Administrative staff– Systems staff
• Business Process Analysis– Where do you use diagnoses/inpatient hospital procedures?– What are the interfaces that may need to be changed?– What databases need to be changed?
• This is a long-term project, which will consume considerable resources. – Planning is critical. – Initial estimates say that it will take all of the time between
now and Oct 1, 2015, to effectively implement ICD-10. – A structured Work Plan is critical.

51 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Why Does this Matter?
• More precise coding and documentation, including signs, symptoms, and risk factors, that will permit tracking of many new diagnoses and procedures and result in fewer rejected claims for reimbursement
• Opportunities for improved benchmarking to allow Mayo Clinic compare itself to other providers and health care institutions in the areas of quality, safety, value, and service
• Detailed data availability that enhances quality metrics, patient safety and compliance
• Improved disease epidemiology that will directly impact public health

52 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
• Better data mining to improve predictive accuracy • Organizational monitoring and performance that supports
determination of episodes of care and high-risk-pool patients.
• Diagnoses and procedure codes impact virtually every system and business process in plan and provider organizations, with significant impacts on reimbursements
Why Does this Matter?
53 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
Basic Education Sites
• NCHS – Basic ICD-10-CM Informationhttp://www.cdc.gov/nchs/about/otheract/icd9/abticd10.htm
• CMS – ICD-10-PCS Informationhttp://www.cms.hhs.gov/ICD10/02_ICD-10-PCS.asp
• AHIMA - ICD-10 Educationhttp://www.ahima.org/icd10/index.asp
• WEDI – ICD-10 Implementationwww.wedi.org

54 Proprietary and Confidential. © 2015 Xtend Healthcare, LLC. All rights reserved. All registered trademarks are the property of their respective owners
ICD-10 Assessment: The First Step
• Questions? . . .
Linda Corley
706 577-2256
Related Documents











