TECHNICAL PAPERS ON HEALTH AND BEHAVIOR MEASUREMENT TECHNICAL PAPER 79 Concordance of chlamydia trachomatis infections within sexual partnerships S.M. Rogers, W.C. Miller, C.F. Turner, J. Ellen, J. Zenilman, R. Rothman, M. Villarroel, A. Al-Tayyib, P. Leone, C. Gaydos, L. Ganapathi, M. Hobbs, D. Kanouse Reference Citation S.M. Rogers, W.C. Miller, C.F. Turner, J. Ellen, J. Zenilman, R. Rothman, M. Villarroel, A. Al-Tayyib, P. Leone, C. Gaydos, L. Ganapathi, M. Hobbs, D. Kanouse. Technical Papers on Health and Behavior Measurement, No. 79, Washington DC: RTI Program in Health and Behavior Measurement, 2007. (Abbreviated version published in Sexually Transmitted Infections, 84: 23-28, 2008.)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TECHNICAL PAPERS ONHEALTH AND BEHAVIOR MEASUREMENT
TECHNICAL PAPER 79
Concordance of chlamydia trachomatis infections within sexual partnerships
S.M. Rogers, W.C. Miller, C.F. Turner, J. Ellen, J. Zenilman, R. Rothman, M. Villarroel,A. Al-Tayyib, P. Leone, C. Gaydos, L. Ganapathi, M. Hobbs, D. Kanouse
Reference Citation
S.M. Rogers, W.C. Miller, C.F. Turner, J. Ellen, J. Zenilman, R. Rothman, M. Villarroel, A.Al-Tayyib, P. Leone, C. Gaydos, L. Ganapathi, M. Hobbs, D. Kanouse. Technical Papers onHealth and Behavior Measurement, No. 79, Washington DC: RTI Program in Health andBehavior Measurement, 2007. (Abbreviated version published in Sexually TransmittedInfections, 84: 23-28, 2008.)

Concordance of chlamydia trachomatis infectionswithin sexual partnerships
S M Rogers,1 W C Miller,2 C F Turner,1,3 J Ellen,4 J Zenilman,5 R Rothman,6
M A Villarroel,1 A Al-Tayyib,2 P Leone,2 C Gaydos,5 L Ganapathi,7 M Hobbs,2 D Kanouse8
1 Program in Health and BehaviorMeasurement, ResearchTriangle Institute, Washington,DC, USA; 2 Division of InfectiousDiseases, Department ofMedicine and Epidemiology,University of North Carolina,Chapel Hill, NC, USA; 3 CityUniversity of New York, QueensCollege and Graduate Center,New York, NY, USA; 4 Division ofAdolescent Medicine, School ofMedicine, Johns HopkinsUniversity, Baltimore, MD, USA;5 Division of Infectious Diseases,School of Medicine, JohnsHopkins University, Baltimore,MD, USA; 6 Department ofEmergency Medicine, JohnsHopkins Medical Institution,Baltimore, MD, USA; 7 ResearchComputing Division, ResearchTriangle Institute, ResearchTriangle Park, NC, USA; 8 RAND,Santa Monica, CA, USA
Correspondence to:Dr Susan M Rogers, PhD,Program in Health and BehaviorMeasurement, ResearchTriangle Institute, 701 13th StNW, Suite 750, Washington, DC20005, USA; [email protected]
Accepted 20 September 2007
ABSTRACTObjectives: The enhanced sensitivity of nucleic acidamplification tests (NAAT) provides an opportunity forestimating the prevalence of untreated Chlamydiatrachomatis infections. The transmissibility and publichealth significance of some NAAT-identified infectionsare, however, not known.Methods: Adults attending an urban emergency depart-ment provided specimens for C trachomatis screeningusing NAAT. Participants testing positive were offeredfollow-up including re-testing for C trachomatis usingNAAT and traditional methods, eg culture and directfluorescent antibody, and were treated. Partners wereoffered identical evaluation and treatment. Overall, 90 Ctrachomatis-positive participants had one or more sexualpartners enrolled.Results: Evidence of transmission, as defined by infectionconcordance between partnerships, was observed among75% of partners of index cases testing positive by bothNAAT and traditional assay but only 45% of partners ofindex cases testing positive by NAAT only (prevalenceratio 1.7, 95% CI 1.1 to 2.5). Among index participantsreturning for follow-up, 17% had no evidence of Ctrachomatis infection by NAAT or traditional assay(median follow-up three weeks).Conclusions: A substantial proportion of positive NAATresults for chlamydial infection may be of lowertransmissibility and may not persist after a short follow-up. The long-term health effects of some positive NAATare uncertain.
Unrecognised Chlamydia trachomatis infection iscommon among US young adults.1–3 Estimates ofthe prevalence of C trachomatis have been facili-tated by the development of non-invasive nucleicacid amplification tests (NAAT). NAAT providesubstantial improvements in test sensitivity whileretaining the high specificity of traditional meth-ods.4 The use of NAAT, compared with culture,increases the yield of infections detected by 20–40%.5
Although the enhanced sensitivity of NAAT iswell recognised, the significance and transmissi-bility of the additional infections detected byNAAT are unknown. It is possible that NAAT isdetecting clinically inconsequential infectionsinvolving low levels of viable organisms, or perhapsamplifiable residual DNA from a recently con-trolled infection.
We conducted a cross-sectional study withrecruitment of sexual partners to examine thepotential transmissibility of chlamydial infectionsidentified by NAAT but not by traditional assay.We tested the hypothesis that chlamydial infections
that are detectable only by NAAT are less transmis-sible, as evidenced by infection concordance withinpartnerships, than infections that are also detectableby traditional methods. As a secondary aim, weexamined the persistence of NAAT-positive infec-tions among participants after a short follow-up.
METHODSBetween November 2002 and February 2005,trained interviewers approached adult patientsattending the Johns Hopkins Hospital EmergencyDepartment to assess eligibility for C trachomatisscreening, eg age between 18 and 35 years, Englishspeaking, and sexually active in the past 90 days.Eligible adults who consented to screening alsocompleted a brief audio computer-assisted self inter-view about recent sexual and health behaviours.6
Participants screened in the emergency departmentafter March 2003 received a US$10 food coupon.
We obtained contact information from all indexparticipants undergoing C trachomatis screening inthe emergency department to facilitate the follow-up of positive test results by trained researchdisease intervention specialists. Disease interven-tion specialists offered follow-up examination todetect clinical evidence consistent with chlamydialinfection, additional C trachomatis testing (NAATand traditional assay), and treatment at the JohnsHopkins Hospital General Clinical Research Center(GCRC). Disease intervention specialists also con-tacted up to five named sexual partners within thepast 60 days and offered evaluation and treatmentprocedures identical to those provided to indexparticipants. Index participants and partners pre-senting to the GCRC for follow-up completed adetailed behavioural audio computer-assisted selfinterview and received US$50–200 in compensa-tion for their time and travel costs. Partners notattending the GCRC were offered the option of ahome visit to complete the questionnaire and tocollect a specimen for NAAT.
The Research Triangle Institute, University ofNorth Carolina, and Western (for the Johns HopkinsUniversity School of Medicine) Institutional ReviewBoards approved all study procedures. Study partici-pants with positive test results for chlamydialinfection were reported to the Baltimore CityHealth Department.
Specimen collection and laboratory testing
NAAT for C trachomatisUS Food and Drug Administration-approved NAATwere performed according to the manufacturers’instructions at the University of North Carolina.
Chlamydia
Sex Transm Infect 2008;84:23–28. doi:10.1136/sti.2007.027029 23
on 10 May 2008 sti.bmj.comDownloaded from

Initially, urine specimens were tested using a ligase chain reaction(LCR) assay (Abbott Laboratories, North Chicago, Illinois, USA).After the LCR was withdrawn from the market in 2003, maleurine specimens and female vaginal swabs were tested using theCOBAS Amplicor PCR assay (Roche Diagnostic Systems,Indianapolis, Indiana, USA).7 8 Positive NAAT results wereconfirmed by repeating the assay. Infection with C trachomatis asdetected by NAAT (N+) was defined as a repeatedly positive teston the same specimen.
At follow-up, NAAT were performed on urine (menthroughout the study and women initially), urethral swabs(men), endocervical swabs (women), and self-administeredvaginal swabs. Each index thus received three NAAT: one uponinitial recruitment in the emergency department and two repeattests on follow-up. Sexual partners received two NAAT duringtheir GCRC visit.
Traditional assay for C trachomatisTraditional testing was performed at GCRC follow-up usingculture and direct fluorescent antibody (DFA) from urethral andendocervical specimens. Specimens were stored at 280uC untiltesting by the International STD Research Laboratory, JohnsHopkins University. Culture was performed in McCoy cells.Culture-negative specimens were tested using DFA of thesediment from the centrifuged culture transport media; a slidewas considered DFA positive if three or more elementary bodieswere present. Culture-positive specimens and DFA-positive/culture-negative specimens were considered positive for Ctrachomatis by traditional assay (T+). Specimens that testedculture and DFA negative were considered traditional assaynegative (T2).
Statistical analyses and outcomesChi-square and t-tests were used to compare characteristics ofNAAT-positive index participants who did and did not presentfor follow-up.
We assessed the concordance of infection between sexualpartners as a surrogate for the transmissibility of NAAT-identified infections, restricted to partnerships in which bothNAAT and traditional test results were available. We definedconcordance as either a positive NAAT (N+) or traditional assay(T+) result for C trachomatis among partners of C trachomatis-positive index participants. All index participants were con-sidered NAAT positive on the basis of their emergencydepartment test result.
Our primary hypothesis was that chlamydial infectionsdetectable by NAAT but not by traditional assay (N+T2) inthe index participants would be less transmissible to sexualpartners than infections that were also detectable by traditionalassay (N+T+). Non-concordance was considered as evidence oflower transmissibility. We tested this hypothesis by examiningprevalence ratios with 95% CI that compared the proportion ofpartnerships with concordant C trachomatis infections (N+ and/or T+) between index participants who tested N+T2 and thosewho tested N+T+.
We also examined characteristics of index participants andtheir partners that may be associated with infection concor-dance. For all partnership analyses, we used generalisedestimating equations with a log link and binomial errordistribution to estimate prevalence ratios for concordance.Generalised estimating equations account for within-groupcorrelation, such as that that exists between multiple partnersof the same index participant.9
As a secondary aim, we examined the persistence of NAAT-identified chlamydial infections at follow-up among individualswith positive NAAT in the emergency department. Factorspotentially influencing persistence were examined in binomialregression analyses. In addition, we examined the associationbetween the persistence and concordance of infection withinpartnerships. All statistical analyses were conducted using Stataversion 8 (Stata Corp., College Station, Texas, USA).
RESULTS
Study recruitment: C trachomatis screening and follow-upOver a 27-month period, 21 trained interviewers identified 6952eligible adults attending the emergency department (fig 1); 6094(87.7%) consented to screening. The prevalence of chlamydialinfection was 7.0% in emergency department participants. Theprevalence of C trachomatis in male urine specimens (7%) wascomparable as determined by LCR and PCR (8.4% versus 6.6%,p.0.10). Among female urine specimens tested by LCR(November 2002 to August 2003), 6.8% were C trachomatispositive; 7.3% of female swab specimens tested positive by PCR(p.0.10).
Of the 419 index participants who tested NAAT positive, 81(19.3%) received antibiotic treatment during their emergencydepartment visit. Of the remaining 338, 166 (49%) participatedin follow-up. The mean number of disease interventionspecialist contacts was two (range one to 10) and the averagenumber of days between emergency department testing andfollow-up was 21.5 (range eight to 46 days). Participants atfollow-up were slightly younger (mean age 22.5 versus 23.5 years;p = 0.04) and more were women (62% versus 50.6%, p = 0.03)compared with those who did not participate (table 1).
Most index participants (87%) named one or more recentsexual partners at follow-up; 13% refused to provide partnerinformation. Of 175 partners identified, 152 (86.9%) werecontacted successfully by disease intervention specialists and102 (58.3%) attended follow-up. Nearly half (48%) of thepartnerships presented for follow-up together.
Partner concordance of C trachomatis infectionsOur concordance analyses are limited to the 83 heterosexualcouples (72 index participants with one partner, four indexeswith two partners, and one index with three partners) forwhom both NAAT and traditional assay results were available.We excluded 17 partnerships because of missing results, inade-quate specimen collection, transcription error, or multiple enroll-ment of a positive index subject. Two exclusively male partner-ships were omitted as we did not collect anal or throat specimens.
Evidence of infection transmission, as defined by concordancewithin partnerships, was more common among index casestesting positive by both NAAT and traditional assay (N+T+)than among index cases testing positive by NAAT alone(N+T2; table 2). Evidence of transmission was observed in 39of 52 partners (75%) of N+T+ index cases, but only 14 of 31partners (45%) of N+T2 index cases (prevalence ratio 1.7, 95%CI 1.1 to 2.5).
The relationship between index test result (N+T2 or N+T+)and partner concordance did not vary by gender. Among themale partners of N+T+ female indexes, 82% were concordantfor C trachomatis, compared with 46% of male partners ofN+T2 women. Similarly, 70% of female partners of N+T+index men were concordant, in comparison with 43% of femalepartners of men testing positive by NAAT only. There was nodifference by index’s or partner’s age, the number of new
Chlamydia
24 Sex Transm Infect 2008;84:23–28. doi:10.1136/sti.2007.027029
on 10 May 2008 sti.bmj.comDownloaded from

partners in the past three months, a history of chlamydialinfection, a history of any sexually transmitted infection,antibiotic use before the follow-up visit, or time to indexfollow-up. Adjusting for the timing of the partner visit,however, reduced the prevalence ratio to 1.5 (95% CI 1.03 to2.2). Partners presenting at the same time as the indexparticipant were more likely to test concordant than partnerspresenting after the index visit.
Limiting traditional test results to culture only decreased ouroverall estimate of concordance from 64% to 54% (prevalenceratio 1.4, 95% CI 0.93 to 2.0). Differences in the type of NAAT(LCR versus PCR) or specimen type (female urine versus vaginalswab) could also influence our transmission estimates.Although all women screened in the emergency departmentprovided vaginal swabs for C trachomatis testing using PCR,initially women also provided urine specimens for LCR testing.When the LCR was withdrawn in 2003, male urine samples andfemale swabs were tested using PCR. Restricting our con-cordance analysis to include only female indexes with positiveswab results (n = 81 couples, prevalence ratio 1.7, 95% CI 1.1to 2.5) or male and female index subjects with positive PCRresults alone (n = 75 couples, prevalence ratio 1.7, 95% CI 1.2to 2.5) had no effect on our transmission estimates.
Non-persistence of NAAT-positive resultsIndex participants were screened initially in the emergencydepartment and re-evaluated at follow-up, thus it is possible toexamine the short-term persistence of NAAT-identified Ctrachomatis. Among participants who had not received antibiotictherapy during the emergency department visit and who hadboth NAAT and traditional assay results available for follow-up(n = 163; three participants had missing traditional assayresults), 27 (17%) individuals had no evidence of C trachomatisinfection by NAAT or culture/DFA. Nine (5%) individuals wereNAAT negative, but positive by culture/DFA. The remaining127 (78%) participants were NAAT positive (table 3).
In bivariable analyses, women were significantly more likelythan men to test negative for C trachomatis after a short follow-up(23% versus 6%, risk ratio 3.6, 95% CI 1.3 to 9.9) as wereindividuals who had used antibiotics in the three months beforetheir emergency department visit (32% versus 12%, risk ratio 2.6,95% CI 1.2 to 5.5). In multivariable analyses, only gender remainedsignificantly associated with the persistence of NAAT-positiveresults.
Non-persistence and partner concordanceWe also examined the association between the persistence ofNAAT-positive results and partnership concordance. Within the83 partnerships, only one partner of nine (11%) indexparticipants without evidence of C trachomatis infection atfollow-up tested positive. In contrast, 52 partners of 74 (70%)index participants with evidence of C trachomatis infection at
Figure 1 Subject participation in screening and follow-up, November2002 to February 2005. *Patients attending the emergency department(ED) were eligible for C trachomatis (CT) screening if they were between18 and 35 years of age, English-speaking, sexually active in the pastthree months, and a non-Hopkins employee or student. For the first fivemonths of data collection, respondents reporting antibiotic use within thepast three months were excluded. Patients were also ineligible if theywere critically ill or unable to participate as a result of a physicalcondition or cognitive impairment, or they had been previously enrolled inthe study and tested positive for C trachomatis. {A total of 700individuals did not consent, 82 completed the audio computer-assistedself interview only, 57 individuals were released from the emergencydepartment before completing the study, and 19 patients enrolled twice.{Subject consented and provided urine or self-administered swabspecimen for sexually transmitted infection testing using the nucleic acidamplification test (NAAT). 1As determined by repeatedly positive NAATon the same specimen. Initially male and female urine specimens weretested using ligase chain reaction (LCR) assay. After August 2003, maleurine and female self-administered vaginal swabs were tested using theCOBAS Amplicor assay. This change was necessitated by the specimenrequirements of the Roche Amplicor assay, which was used after AbbottLaboratories discontinued the LCR. "C trachomatis-positive indexsubjects who received antibiotic therapy during their emergencydepartment visit were not re-contacted for follow-up. **Forty subjectsprovided insufficient locating information, 44 received healthcareelsewhere, 40 received treatment only at the Johns Hopkins HospitalGeneral Clinical Research Center (GCRC), 16 did not show for theirscheduled GCRC appointment, and 22 either refused treatment, wereincarcerated, a non-resident of Baltimore, or in substance abuserehabilitation. {{After enrollment IDs were switched on two index
subjects’ specimens, two indexes were actually partners of twopreviously enrolled C trachomatis-positive index subjects, and onesubject did not have complete NAAT and traditional assay results.{{Seventeen partners were treated elsewhere, 20 were out of jurisdictionor not located, eight refused treatment, and five received treatment andan examination only at the GCRC. 11Two partners were enrolled at homeand provided specimens for NAAT only. An additional 14 partnershipswere missing complete NAAT and traditional assay results, one partnerwas enrolled six months after the index, and specimen IDs weremislabelled during collection for two partnerships.
Chlamydia
Sex Transm Infect 2008;84:23–28. doi:10.1136/sti.2007.027029 25
on 10 May 2008 sti.bmj.comDownloaded from
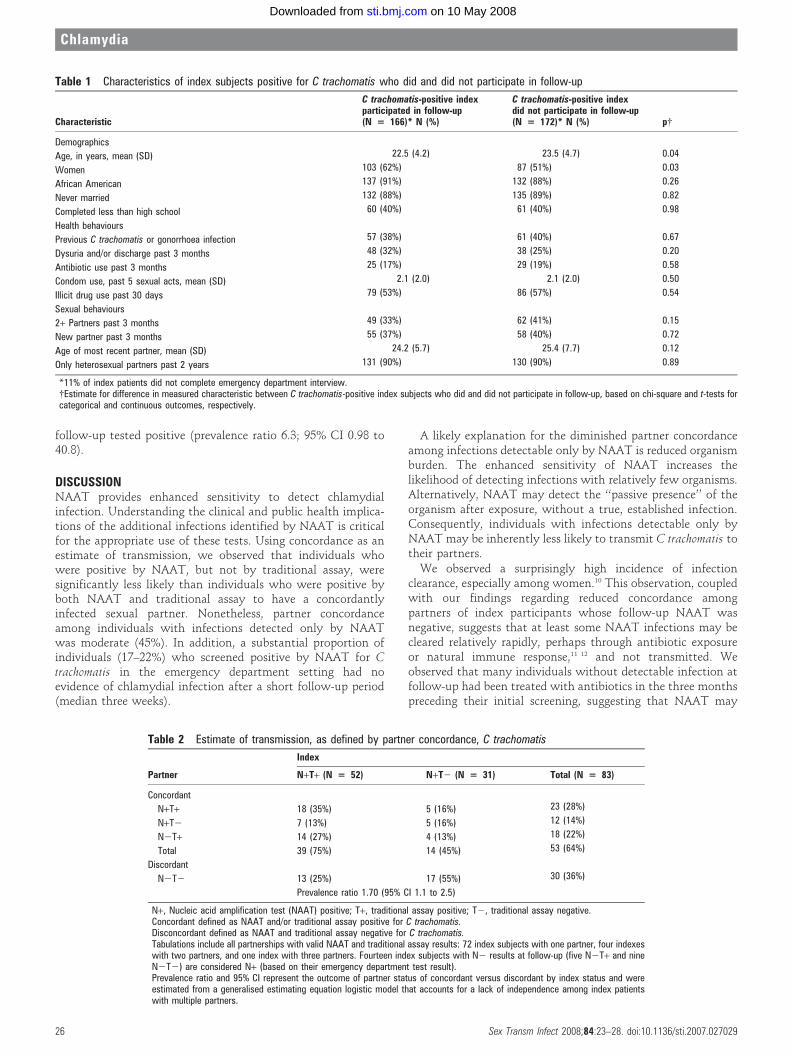
follow-up tested positive (prevalence ratio 6.3; 95% CI 0.98 to40.8).
DISCUSSIONNAAT provides enhanced sensitivity to detect chlamydialinfection. Understanding the clinical and public health implica-tions of the additional infections identified by NAAT is criticalfor the appropriate use of these tests. Using concordance as anestimate of transmission, we observed that individuals whowere positive by NAAT, but not by traditional assay, weresignificantly less likely than individuals who were positive byboth NAAT and traditional assay to have a concordantlyinfected sexual partner. Nonetheless, partner concordanceamong individuals with infections detected only by NAATwas moderate (45%). In addition, a substantial proportion ofindividuals (17–22%) who screened positive by NAAT for Ctrachomatis in the emergency department setting had noevidence of chlamydial infection after a short follow-up period(median three weeks).
A likely explanation for the diminished partner concordanceamong infections detectable only by NAAT is reduced organismburden. The enhanced sensitivity of NAAT increases thelikelihood of detecting infections with relatively few organisms.Alternatively, NAAT may detect the ‘‘passive presence’’ of theorganism after exposure, without a true, established infection.Consequently, individuals with infections detectable only byNAAT may be inherently less likely to transmit C trachomatis totheir partners.
We observed a surprisingly high incidence of infectionclearance, especially among women.10 This observation, coupledwith our findings regarding reduced concordance amongpartners of index participants whose follow-up NAAT wasnegative, suggests that at least some NAAT infections may becleared relatively rapidly, perhaps through antibiotic exposureor natural immune response,11 12 and not transmitted. Weobserved that many individuals without detectable infection atfollow-up had been treated with antibiotics in the three monthspreceding their initial screening, suggesting that NAAT may
Table 1 Characteristics of index subjects positive for C trachomatis who did and did not participate in follow-up
Characteristic
C trachomatis-positive indexparticipated in follow-up(N = 166)* N (%)
C trachomatis-positive indexdid not participate in follow-up(N = 172)* N (%) p{
Demographics
Age, in years, mean (SD) 22.5 (4.2) 23.5 (4.7) 0.04
Women 103 (62%) 87 (51%) 0.03
African American 137 (91%) 132 (88%) 0.26
Never married 132 (88%) 135 (89%) 0.82
Completed less than high school 60 (40%) 61 (40%) 0.98
Health behaviours
Previous C trachomatis or gonorrhoea infection 57 (38%) 61 (40%) 0.67
Dysuria and/or discharge past 3 months 48 (32%) 38 (25%) 0.20
Antibiotic use past 3 months 25 (17%) 29 (19%) 0.58
Condom use, past 5 sexual acts, mean (SD) 2.1 (2.0) 2.1 (2.0) 0.50
Illicit drug use past 30 days 79 (53%) 86 (57%) 0.54
Sexual behaviours
2+ Partners past 3 months 49 (33%) 62 (41%) 0.15
New partner past 3 months 55 (37%) 58 (40%) 0.72
Age of most recent partner, mean (SD) 24.2 (5.7) 25.4 (7.7) 0.12
Only heterosexual partners past 2 years 131 (90%) 130 (90%) 0.89
*11% of index patients did not complete emergency department interview.{Estimate for difference in measured characteristic between C trachomatis-positive index subjects who did and did not participate in follow-up, based on chi-square and t-tests forcategorical and continuous outcomes, respectively.
Table 2 Estimate of transmission, as defined by partner concordance, C trachomatis
Partner
Index
N+T+ (N = 52) N+T2 (N = 31) Total (N = 83)
Concordant
N+T+ 18 (35%) 5 (16%) 23 (28%)
N+T2 7 (13%) 5 (16%) 12 (14%)
N2T+ 14 (27%) 4 (13%) 18 (22%)
Total 39 (75%) 14 (45%) 53 (64%)
Discordant
N2T2 13 (25%) 17 (55%) 30 (36%)
Prevalence ratio 1.70 (95% CI 1.1 to 2.5)
N+, Nucleic acid amplification test (NAAT) positive; T+, traditional assay positive; T2, traditional assay negative.Concordant defined as NAAT and/or traditional assay positive for C trachomatis.Disconcordant defined as NAAT and traditional assay negative for C trachomatis.Tabulations include all partnerships with valid NAAT and traditional assay results: 72 index subjects with one partner, four indexeswith two partners, and one index with three partners. Fourteen index subjects with N2 results at follow-up (five N2T+ and nineN2T2) are considered N+ (based on their emergency department test result).Prevalence ratio and 95% CI represent the outcome of partner status of concordant versus discordant by index status and wereestimated from a generalised estimating equation logistic model that accounts for a lack of independence among index patientswith multiple partners.
Chlamydia
26 Sex Transm Infect 2008;84:23–28. doi:10.1136/sti.2007.027029
on 10 May 2008 sti.bmj.comDownloaded from

have detected residual DNA, rather than viable organisms, atthe initial screening evaluation.13 A proportion of the resultscould be false positives, although we re-tested all initial positiveresults to reduce this possibility. Sampling variability associatedwith the repeated testing of low-level infections is anotherpossibility, but appears less likely because of the multiplespecimens taken at follow-up.14 The likelihood of each of thesepossibilities is worthy of further clinical investigation.
The widespread application of NAAT has ‘‘resulted inconsiderable revision of our views of the clinical epidemiologyof C trachomatis’’.15 16 Only recently, however, have we begun toquestion the significance of some additional infections identifiedby NAAT.17 In this study, we examined partner concordance asa marker of the clinical significance of NAAT-identifiedinfections. Further study of the association between asympto-matic NAAT-identified chlamydial infections and other clinicalconsequences, eg the incidence of pelvic inflammatory disease,or inflammation, is needed.
Few studies have examined infection transmission withinpartnerships.18 We chose a non-sexually transmitted infectionclinic population as we were interested in understanding thetransmissibility of largely asymptomatic, unrecognised Ctrachomatis infections. Consequently, we screened over 6000individuals. In this cross-sectional sample, the timing of theprevalent infection in the index and the direction of transmis-sion between index and partner could not be established.Generalisation of our findings may be constrained by oursample selection and by incomplete recruitment, although indexparticipants had a similar risk profile to individuals who did notparticipate.
The advent of NAAT screening has expanded opportunitiesfor prevention of the serious consequences of untreated Ctrachomatis infection. Although we strongly believe thatindividuals with a positive NAAT should be informed and
treated, our study demonstrates that some NAAT-detectedinfections may not represent clinically active disease ortransmissible infections. Failure to diagnose a chlamydialinfection can negatively affect health, although incorrectlyidentifying individuals as infected can damage relationships.Patients, especially those with low-risk profiles or thosescreened from low C trachomatis prevalence populations,16
should be counselled about their test result accordingly.Guidelines for testing, patient counselling and managementshould be formulated so that users of this remarkable andpowerful tool—doctors, patients, and researchers—are aware ofthe advantages of NAAT and also its limitations.
Acknowledgements: The authors would like to thank Don Orr, Martina Morris, andHeather Miller for serving as scientific advisors to this project. They also thank SarahMobius for her managerial contribution to the study and Sheping Li at RTI forprogramming and data management; Ambreen Khalil and Chadd Krauss for theiroversight of interviews at the Johns Hopkins Adult Emergency Department; Joan Bess,Kenya S. Stewart and Nancy Willard of the Johns Hopkins Adolescent HealthResearch Group for outreach support; and Mary Ann Knott-Grasso, MS, CPNP, forproviding patient care at the Johns Hopkins General Clinical Research Center. Theauthors also wish to thank the laboratory personnel from the Department of Medicine,University of North Carolina at Chapel Hill, including Marcia Stedman, John Schmitz,and Dana Lapple; and Jeff Younger, Billie Jo Wood, and Hope L Johnson from theJohns Hopkins School of Medicine, Department of Infectious Diseases.
Funding: Primary support for this research was provided by National Institutes ofHealth (NIH) grant R01-HD039633 to SMR. RR was supported in part by a grant fromNCRR NIH 3M01RR00052-39-5(S1).
Competing interests: None.
Author contributions: SMR, WCM, CFT, PL, JE, RR and DK contributed to theconception and design of the study. SMR, WCM, CFT, JE, JZ, RR, CG and MHcontributed to the acquisition of data. SMR, WCM, MAV, AA-T and DK contributed toquestionnaire design. SMR, MAV and LG contributed to data management. SR, WCM,MAV and CFT contributed to the analysis and interpretation of data. All authorscontributed to writing the manuscript.Role of the funding source: The National Institutes of Health did not participate inthe design and conduct of the study, in the collection, analysis, and interpretation ofthe data, or in the preparation, review, or approval of the manuscript. Thecorresponding author had full access to all of the data in the study and takesresponsibility for the integrity of the data and the accuracy of the data analysis.
REFERENCES1. Miller WC, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal
infections among young adults in the United States. JAMA 2004;291:2229–36.2. Turner CF, Rogers SM, Miller HG, et al. Untreated gonococcal and chlamydial
infection in a probability sample of adults. JAMA 2002;287:726–33.3. Institute of Medicine. The hidden epidemic: confronting sexually transmitted
diseases. Washington, DC: National Academy Press, 1996.4. Schacter J. Chlamydia trachomatis: the more you look the more you find – how
much is there? Sex Transm Dis 1998;25:229–31.5. Stamm WE. Chlamydia trachomatis infections of the adult. In: Holmes KK, Sparling
PF, Mardh P, Lemon SM, Samm WE, Piot P, Wasserheit JN, editors.Sexuallytransmitted diseases. New York: McGraw Hill, 1999:407–22.
6. Cooley PC, Rogers SM, Turner CF, et al. Using touch-screen audio-CASI to obtaindata on sensitive topics. Comp Human Behav 2001;17:285–93.
Key messages
c Although the enhanced sensitivity of NAAT is well recognised,the significance and transmissibility of the additional infectionsdetected by NAAT are unknown.
c A substantial proportion of positive NAAT results forchlamydial infection may be of lower transmissibility and maynot persist after a short follow-up.
c Guidelines for testing, patient counselling and managementshould be formulated so that doctors, patients, andresearchers are aware of the advantages of NAAT as well asits limitations.
Table 3 Results of testing for C trachomatis at follow-up among NAAT-positive index participants
NAAT-positive index participants
Total Men Women
Follow-up test result
N2T2 27 (17%) 4 (6%) 23 (23%)
N2T+ 9 (5%) 3 (5%) 6 (6%)
N+T+ 83 (51%) 36 (57%) 47 (47%)
N+T2 44 (27%) 20 (32%) 24 (24%)
Total 163 63 100
Fisher’s exact p = 0.03
N+, Nucleic acid amplification test (NAAT) positive; T+, traditional assay positive; N2, NAAT negative; T2, traditional assaynegative.Fisher’s exact for test of association between gender and follow-up test result.
Chlamydia
Sex Transm Infect 2008;84:23–28. doi:10.1136/sti.2007.027029 27
on 10 May 2008 sti.bmj.comDownloaded from

7. Watson EJ, Templeton A, Russell I, et al. The accuracy and efficacy of screeningtests for Chlamydia trachomatis: a systematic review. J Med Microbiol2003;51:1021–31.
8. Schacter J, McCormack, Chernesky M, et al. Vaginal swabs are appropriatespecimens for diagnosis of genital tract infection with Chlamydia trachomatis. J ClinMicrobiol 2003;41:3784–9.
9. Hardin JW, Hilbe JM. Generalized estimating equations. Boca Raton, FL: Chapmanand Hall/CRC, 2003.
10. Brunham RC, Plummer FA. A general model of sexually transmitted diseaseepidemiology and its implication for control. Med Clin North Am 1991;74:1339–52.
11. Moore SA, Sillekens PT, Jacobs MV, et al. Monitoring of Chlamydia trachomatisinfections after antibiotic treatment using RNA detection by nucleic acid sequencebased amplification. Mol Pathol 1998;51:149–54.
12. Bianchi A, Bogard M, Cessot G, et al. Kinetics of Chlamydia trachomatis clearance inpatients with azithromycin, as assessed by first void urine testing by PCR andtranscription-mediated amplification. Sex Trans Dis 1998;25:366–7.
13. Gaydos CA, Crotchfelt C, Howell MR, et al. Molecular amplification assays to detectchlamydial infections in urine specimens from high school female students and to monitorthe persistence of chlamydial DNA after therapy. J Infect Dis 1998;177:417–24.
14. Schachter J, Chow JM, Howard H, et al. Detection of Chlamydia trachomatis by nucleicacid amplification testing: our evaluation suggests that CDC-recommended approachesfor confirmatory testing are ill-advised. J Clin Microbiol 2006;44:2512–17.
15. Stamm WE. Chlamydia trachomatis—the persistent pathogen: Thomas ParranAward Lecture. Sex Transm Dis 2001;28:684–9.
16. Zenilman JM, Miller WC, Gaydos C, et al. LCR testing for gonorrhea and chlamydiain population surveys and other screenings of low prevalence populations: copingwith decreased positive predictive value. Sex Transm Infect 2003;79:94–7.
17. Hagdu A, Dendukuri N, Hilden J. Evaluation of a nucleic acid amplification test in theabsence of a gold-standard test: a review of the statistical and epidemiologicalissues. Epidemiology 2005;16:604–12.
18. Quinn T, Gaydos C, Shepherd M, et al. Epidemiologic and microbiologic correlates ofClamydia trachomatis infection in sexual partnerships. JAMA 1996;276:1737–42.
BMJ Clinical Evidence—Call for contributors
BMJ Clinical Evidence is a continuously updated evidence-based journal available worldwide on the internetwhich publishes commissioned systematic reviews. BMJ Clinical Evidence needs to recruit newcontributors. Contributors are healthcare professionals or epidemiologists with experience in evidence-based medicine, with the ability to write in a concise and structured way and relevant clinical expertise.
Areas for which we are currently seeking contributors:c Secondary prevention of ischaemic cardiac eventsc Acute myocardial infarctionc MRSA (treatment)c Bacterial conjunctivitis
However, we are always looking for contributors, so do not let this list discourage you.
Being a contributor involves:c Selecting from a validated, screened search (performed by in-house Information Specialists) valid
studies for inclusion.c Documenting your decisions about which studies to include on an inclusion and exclusion form,
which we will publish.c Writing the text to a highly structured template (about 1500–3000 words), using evidence from the
final studies chosen, within 8–10 weeks of receiving the literature search.c Working with BMJ Clinical Evidence editors to ensure that the final text meets quality and style
standards.c Updating the text every 12 months using any new, sound evidence that becomes available. The
BMJ Clinical Evidence in-house team will conduct the searches for contributors; your task is to filterout high quality studies and incorporate them into the existing text.
c To expand the review to include a new question about once every 12 months.
In return, contributors will see their work published in a highly-rewarded peer-reviewed internationalmedical journal. They also receive a small honorarium for their efforts.If you would like to become a contributor for BMJ Clinical Evidence or require more information aboutwhat this involves please send your contact details and a copy of your CV, clearly stating the clinicalarea you are interested in, to [email protected].
Call for peer reviewersBMJ Clinical Evidence also needs to recruit new peer reviewers specifically with an interest in theclinical areas stated above, and also others related to general practice. Peer reviewers are healthcareprofessionals or epidemiologists with experience in evidence-based medicine. As a peer reviewer youwould be asked for your views on the clinical relevance, validity and accessibility of specific reviewswithin the journal, and their usefulness to the intended audience (international generalists andhealthcare professionals, possibly with limited statistical knowledge).Reviews are usually 1500–3000 words in length and we would ask you to review between 2–5systematic reviews per year. The peer review process takes place throughout the year, and ourturnaround time for each review is 10–14 days. In return peer reviewers receive free access toBMJ Clinical Evidence for 3 months for each review.
If you are interested in becoming a peer reviewer for BMJ Clinical Evidence, please complete the peerreview questionnaire at www.clinicalevidence.com/ceweb/contribute/peerreviewer.jsp
Chlamydia
28 Sex Transm Infect 2008;84:23–28. doi:10.1136/sti.2007.027029
on 10 May 2008 sti.bmj.comDownloaded from
1
Concordance of Chlamydia trachomatis Infections Within Sexual Partnerships 1
2
Susan M. Rogers, PhD 3
William C. Miller, MD, PhD, MPH 4
Charles F. Turner, PhD 5
Jonathan Ellen, MD 6
Jonathan Zenilman, MD 7
Richard Rothman, MD, PhD 8
Maria Villarroel, MA 9
Alia Al-Tayyib, MSPH 10
Peter Leone, MD 11
Charlotte Gaydos, DrPH 12
Laxminarayana Ganapathi, PhD 13
Marcia Hobbs, PhD 14
David Kanouse, PhD 15
16
Author Affiliations: Program in Health and Behavior Measurement, Research Triangle 17
Institute, Washington, DC (Drs. Rogers, Turner, Ms Villarroel); Division of Infectious 18
Diseases, Department of Medicine and Epidemiology, University of North Carolina, 19
Chapel Hill (Drs Miller, Leone, Hobbs, Ms Al-Tayyib); City University of New York, 20
Queens College and Graduate Center (Dr Turner); Division of Adolescent Medicine, 21
School of Medicine, Johns Hopkins University (Dr Ellen); Division of Infectious Diseases, 22
School of Medicine, Johns Hopkins University (Drs Zenilman and Gaydos); Department 23
of Emergency Medicine, Johns Hopkins Medical Institution (Dr Rothman); Research 24
Computing Division, Research Triangle Institute, Research Triangle Park, NC (Dr 25
Ganapathi); RAND (Dr Kanouse). 26

2
Corresponding Author: Susan M. Rogers, Program in Health and Behavior 27
Measurement, Research Triangle Institute, 701 13th St NW, Suite 750, Washington, DC 28
20005 ([email protected]) 29
Funding/support: Primary support for this research was provided by NIH grant R01-30
HD039633 to Dr Rogers. Dr. Rothman was supported in part by a grant from NCRR NIH 31
3M01RR00052-39-5(S1). 32
3
Summary 33
Background Nucleic acid amplification tests (NAATs) offer new opportunities for 34
estimating the prevalence of untreated Chlamydia trachomatis infections (Ct), providing 35
substantial improvements in test sensitivity while maintaining the high specificity of 36
traditional testing methods. However, the transmissibility and public health significance 37
of some NAAT-identified infections are not known. We conducted a cross-sectional and 38
short-duration prospective cohort study with follow-up of participants with NAAT-39
identified chlamydial infection and their sexual partners to examine the potential 40
transmissibility and short-term persistence of NAAT-identified chlamydial infections. 41
Methods 6,094 adults aged 18 to 35 years attending an urban Emergency Department 42
(ED) from November 2002 through February 2005 provided specimens for Ct screening 43
using NAATs. Unrecognized Ct infections were identified in seven percent of ED 44
participants using NAAT. Participants testing positive were offered follow-up including 45
re-testing for Ct using NAAT and traditional methods, e.g. culture and direct fluorescent 46
antibody, and treated. Partners were offered identical evaluation and treatment 47
services. Overall, 90 Ct-positive participants had one or more sexual partners enrolled. 48
Results Evidence of transmission, as defined by concordance of infection between 49
sexual partners, was observed among 75% of partners of index cases testing positive by 50
both NAAT and traditional assay (N+T+) but only 45% of partners of index cases testing 51
positive by NAAT only (N+T-) (prevalence ratio 1.7, 95% CI 1.1, 2.5). Among index 52
participants returning for follow-up who had not received antibiotic therapy during the ED 53
visit, 17% had no evidence of Ct infection by NAAT or traditional assay (median follow-54
up = 3 weeks). 55
Interpretation A substantial proportion of positive NAAT results for chlamydial infection 56
may be of lower transmissibility and may not persist after a short follow-up. The public 57
health significance and long-term health effects of some positive NAATs are uncertain. 58
4
59
Introduction 60
Unrecognized and untreated C. trachomatis infection is common among young adults in 61
the United States. Nationwide, 4.7% of women and 3.7% of men aged 18 to 26 years 62
were estimated to have an untreated chlamydial (Ct) infection in 2001-2002.1 Among 63
adults aged 18 to 35 years in Baltimore, MD, untreated chlamydial infections were 64
detected in 6.4% of African American females; the majority of infections were 65
asymptomatic. 2 Given the significant potential morbidity associated with chlamydial 66
infection, including pelvic inflammatory disease and its consequences, controlling and 67
preventing undiagnosed C. trachomatis is a major public health concern. 3 68
69
Estimates of the prevalence of C. trachomatis at the population level have been 70
facilitated by the development of non-invasive nucleic acid amplification tests (NAATs) 71
that can use urine specimens or self-collected vaginal swabs. NAAT provides 72
substantial improvements in test sensitivity while retaining the high specificity of 73
traditional methods such as culture. The enhanced sensitivity of NAAT is due to an 74
extremely low limit of detection, with the potential to detect DNA (or RNA) of 75
approximately 10 organisms per milliliter of sample. 4 In contrast to culture, NAAT does 76
not require viable organisms. Given the high sensitivity and low limit of detection, the use 77
of NAAT, as compared to culture, increases the yield of infections detected by 20 to 40 78
percent. 5 79
80
Although the enhanced sensitivity of NAAT is well-recognized, the significance and 81
transmissibility of the additional infections detected by NAAT are unknown. If the 82
additional infections detected by NAAT are as transmissible as infections detected using 83
traditional methods, such as culture or DFA of culture transport media, the findings from 84
5
population studies call for new public health strategies to reduce infection rates. On the 85
other hand, it is possible that NAAT is detecting clinically inconsequential infections 86
involving extremely low levels of viable organisms, or perhaps amplifiable residual DNA 87
from a recently treated or controlled infection. In a previous population-based study, we 88
observed that many persons with NAAT-identified infection had few behavioral risk 89
factors and most were asymptomatic. 6 This raises the possibility that certain NAAT 90
infections may be of long duration and, presumably, low organism burden. Given the 91
extensive use of NAAT for the detection and diagnosis of chlamydial infection, a better 92
understanding of the clinical and public health significance of the additional infections 93
detected by NAAT is needed. 94
95
We conducted a cross-sectional study of adults attending an urban Emergency 96
Department and offered NAAT screening for chlamydial infection. We conducted follow-97
up of participants with untreated chlamydial infection and recruitment of their sexual 98
partners to explore the potential transmissibility of NAAT-identified infections. We 99
tested the hypothesis that chlamydial infections that are detectable only by NAAT are 100
less transmissible, as evidenced by infection concordance within partnerships, than 101
infections that also are detectable by traditional methods. In addition, a short-duration 102
prospective cohort study examined persistence of chlamydial infections among the 103
NAAT-positive participants who did and did not re-test Ct-positive (by NAAT and/or 104
traditional assay) when returning for follow-up treatment. 105
106
Methods 107
Study Population 108
Between November 2002 and February 2005, trained interviewers approached adult 109
patients attending the Johns Hopkins Hospital Emergency Department (JHH-ED) in 110
6
Baltimore, MD, USA, to assess eligibility for the study. We selected an ED population, 111
rather than a sexually transmitted infection (STI) clinic population, because our focus 112
was on largely asymptomatic and untreated NAAT-identified infections. Patients were 113
eligible for Ct screening if they were between 18 and 35 years of age, English-speaking, 114
and sexually active in the past 90 days. Employees and students of Johns Hopkins, and 115
patients who were critically ill (level-1 acute trauma patients), intoxicated, or presenting 116
for acute psychiatric or STI-related care were excluded. Initially, patients were not 117
eligible if they had used antibiotics within the past 30 days, but in April 2003 this 118
exclusion criterion was discontinued to enhance enrollment. Index participants enrolled 119
after March 2003 received a $10 food coupon for their participation. 120
121
We obtained contact information from all participants undergoing C. trachomatis testing 122
to facilitate notification and follow-up of positive test results by trained research Disease 123
Intervention Specialists (DIS). The DIS informed participants who did not receive 124
antibiotics during their ED visit of their positive result and offered follow-up examination, 125
additional Ct testing (NAAT and traditional assay), and treatment at the JHH General 126
Clinical Research Center (GCRC). Positive participants also were informed that they 127
could seek care from their private physician or the local health department. 128
129
After providing written informed consent, Ct-positive participants presenting to the GCRC 130
were asked to provide names of up to 5 sexual partners in the last 90 days. DIS 131
contacted named partners and offered evaluation and treatment procedures identical to 132
those provided to index participants. Index participants and partners were offered $50-133
200 in compensation for their time and travel costs. Participants who presented to the 134
GCRC but did not wish to complete the study were provided a free medical examination 135
and treatment. 136
7
137
The Research Triangle Institute, University of North Carolina, and Western (for The 138
Johns Hopkins University School of Medicine) Institutional Review Boards approved all 139
study procedures and modifications to the original protocol. Study participants with 140
positive test results for chlamydial infection were reported to the Baltimore City Health 141
Department. 142
143
Participant Interviews and Examinations 144
Participants in the ED completed a brief, approximately 8 minute, audio computer-145
assisted self interview (ACASI) about recent sexual and health behaviors.7 146
147
At follow-up, Ct-positive index participants presenting to the GCRC underwent physical 148
examination to detect clinical evidence consistent with chlamydial infection, including 149
visible discharge, genital ulcers, and lower abdominal and testicular tenderness. 150
Detailed self-reports of current and recent sex partners, partner-specific sexual 151
behaviors and STI history, use of antibiotics, STI symptoms, drug and alcohol use were 152
collected using a touch-screen ACASI. The follow-up interview took an average of 23 153
minutes to complete. 154
155
Sexual partners located by DIS staff were offered physical examinations, testing, and 156
treatment identical to index participants and asked to complete the ACASI. Partners 157
who did not attend the GCRC (and had not sought care elsewhere) were offered the 158
option of a home visit by a study DIS to complete the questionnaire and to collect a urine 159
or vaginal swab specimen for Ct testing. 160
161
Specimen Collection and Laboratory Testing 162

8
NAAT for Ct: FDA-approved NAAT was performed according to the manufacturers’ 163
instructions at the University of North Carolina at Chapel Hill. In the first nine months of 164
the study during ED screening, male participants provided a urine specimen and females 165
provided urine and self-administered vaginal swab specimens for Ct NAAT; however, 166
after August 2003, women provided only swabs. Initially, male and female urine 167
specimens were tested using a ligase chain reaction (LCR) assay (Abbott Laboratories, 168
North Chicago, Ill). After the LCR was withdrawn from the market in 2003 and the 169
laboratory’s supply of LCR kits was depleted, male urine specimens and female self-170
collected vaginal swabs swabs were tested using the COBAS Amplicor polymerase 171
chain reaction (PCR) assay (Roche Diagnostic Systems, Indianapolis, IN). Comparisons 172
of the performance characteristics of the NAATs suggest that the assays are similar for 173
the detection of chlamydial infection in urine and vaginal swab specimens. 8 9 Positive 174
NAAT results were confirmed by repeating the assay. Infection for C. trachomatis as 175
detected by NAAT (N+) was defined as a repeatedly positive test. 176
177
At follow-up, index participants with chlamydial infection and their sexual partners 178
provided specimens for multiple NAATs. Repeat NAAT was performed on urine (men 179
throughout the study and women during the initial study period), urethral swabs (men), 180
endocervical swabs (women), and self-administered vaginal swabs. Each index 181
participant thus received three NAATs: one upon initial recruitment in the ED and two 182
repeat tests on follow-up. Sexual partners received two NAATs during their GCRC clinic 183
visit. 184
185
Traditional assay for Ct: Traditional testing for C. trachomatis was performed at follow-186
up using culture and direct fluorescent antibody (DFA) test from urethral and 187
endocervical specimens in 2-sucrose phosphate culture transport media obtained from 188
9
male and female participants, respectively. Specimens were stored at -80C until testing 189
by the International STD Research Laboratory, Johns Hopkins University. Culture was 190
performed in McCoy cells. Culture-negative specimens were tested using DFA of the 191
sediment from the centrifuged culture transport media; a slide was considered DFA-192
positive if three or more elementary bodies were present. Culture-positive specimens 193
and DFA-positive/culture-negative specimens were considered positive for Ct by 194
traditional assay (T+). Specimens that were both culture and DFA negative were 195
considered traditional assay negative (T-). 196
197
Ct Genotyping 198
To determine the C. trachomatis serovar for organisms detected by NAAT, we amplified 199
variable portions of the ompA gene encoding the major outer-membrane protein 200
(MOMP) from a subset of NAAT-positive specimens using previously described primers 201
10 11 12 and sequenced the resulting PCR products on an ABI 3730 analyzer. We 202
compared sequences from clinical samples with ompA sequences of 17 C. trachomatis 203
serovars in the Gen-Bank database 13 and assigned the serovar of the best match to 204
each specimen. 205
206 207
Statistical Analyses and Outcomes 208
We used chi-square and t-tests to compare demographic and behavioral characteristics 209
of index participants with Ct-positive NAAT test results who did and did not present for 210
follow-up. 211
212
We assessed concordance of infection between sexual partners as a surrogate for 213
transmissibility of NAAT-identified chlamydial infections. We restricted this analysis to 214

10
partnerships in which both NAAT and traditional test results were available. We defined 215
concordance as either a positive NAAT (N+) or traditional assay (T+) result for C. 216
trachomatis among partners of Ct-positive index participants. All index participants were 217
considered NAAT-positive based on their ED test result. 218
219
Our primary hypothesis was that chlamydial infections detectable by NAAT but not by 220
traditional assay (N+T-) in the index participants would be less transmissible to sexual 221
partners than infections that also were detectable by traditional assay (N+T+). Non-222
concordance was considered as evidence of lower transmissibility. We tested this 223
hypothesis by examining prevalence ratios with 95% confidence intervals (CIs) that 224
compared the proportion of partnerships with concordant Ct infections (N+ and/or T+) 225
between index participants who tested N+T- and those that tested N+T+. 226
227
We also examined characteristics of index participants and their partners that may be 228
associated with infection concordance. These variables included age, number of recent 229
sexual partners, new partners within the past 90 days, history of chlamydial infection, 230
recent antibiotic use, reporting of symptoms, time to follow-up (days between index 231
screening in the ED and follow-up, days from index follow-up to partner follow-up, and 232
days between index screening and partner follow-up), and specimen type (female urine 233
vs vaginal swab, LCR vs PCR). 234
235
For all partnership analyses, we used generalized estimating equations (GEE) with a log 236
link and binomial error distribution to estimate prevalence ratios for concordance. GEE 237
account for within-group correlation, such as that which exists between multiple partners 238
of the same index participant.14 Additional analyses of partner concordance using only 239

11
single partnerships, e.g., the index and the first enrolled partner, yielded similar results 240
and are not presented. 241
242
As a secondary aim, we examined the persistence of NAAT-identified chlamydial 243
infections at follow-up among persons with positive NAAT in the ED. We defined 244
persistent infection as a positive NAAT in one or both specimens (urine or self-245
administered vaginal swab and clinician administered endocervical/urethral swab) or a 246
positive traditional test (culture or DFA) at follow-up. Factors potentially influencing 247
persistence of infection, including the number of days from initial screening to follow-up, 248
type of NAAT, respondent's gender, age, and previous diagnosis of chlamydial infection 249
(ever and within the past year) were examined in bivariable and multivariable binomial 250
regression analyses. In addition, we examined the association between persistence and 251
concordance of infection within partnerships. All statistical analyses were conducted 252
using Stata version 8 (Stata Corp., College Station, TX). 253
254
Role of the funding source 255
The US National Institutes of Health did not participate in the design and conduct of the 256
study, in the collection, analysis, and interpretation of the data, or in the preparation, 257
review, or approval of the manuscript. The corresponding author had full access to all of 258
the data in the study and takes responsibility for the integrity of the data and the 259
accuracy of the data analysis. 260
261
Results 262
Study Recruitment: Ct Screening and Follow-up 263
Over a 27-month period, 14,188 adult patients attending the JHH-ED were screened for 264
eligibility by 21 trained interviewers. Screening identified 6,952 English-speaking 265
12
sexually active 18-35 year old adults eligible for participation (Figure 1). Of these, 6,094 266
participants (87.7%) consented to chlamydial screening. 267
268
Overall, the prevalence of chlamydial infection was 7.0% in the ED participants. The 269
prevalence of Ct in male urine specimens (7%) was comparable as determined by LCR 270
and PCR (8.4% v 6.6%, p >0.10). Among female urine specimens tested by LCR 271
between November 2002 through August 2003, 6.8% were Ct positive; 7.3% of female 272
swab specimens collected during September 2003 through February 2005 tested 273
positive by PCR (p >0.10). 274
275
Of the 419 index participants who tested NAAT positive for chlamydial infection during 276
ED screening, 81 (19.3%) received antibiotic treatment during their ED visit and were not 277
eligible for follow-up. Of the remaining 338 eligible index participants, 166 (49%) 278
returned and enrolled in follow-up. Among those enrolled, the mean number of DIS 279
contacts was 2 (range, 1 to 10) and the average number of days between ED testing 280
and follow-up was 21.5 (range, 8 to 46 days). Participants who did and did not enroll in 281
follow-up were similar based on education, race/ethnicity, marital status, previous STI, 282
and recent sexual behaviors (Table 1). In comparison to participants who did not enroll, 283
participants enrolled in follow-up were slightly younger (mean age, 22.5 vs 23.5 years; p 284
= 0.04) and more were female (62% vs 50.6%, p = 0.03). 285
286
Most index participants enrolled at follow-up (87%) named one or more recent sexual 287
partners; 22 (13%) refused to provide partner information. Of the 175 partners identified, 288
152 (86.9%) were contacted successfully by the DIS and 102 (58.3%) were enrolled. 289
One hundred partners were examined and treated; two partners refused evaluation and 290
were interviewed at home. Overall, 90 Ct-positive index participants had one or more 291
13
sexual partners enrolled; 79 index participants had one partner, 10 indexes had two 292
partners, and 1 index had three partners enrolled. Nearly one-half (48%) of the 293
partnerships enrolled in the study presented for follow-up together. 294
295
Partner Concordance of Ct Infections 296
Our analyses of Ct partnerships are limited to the 83 heterosexual couples (72 index 297
participants with one partner, four indexes with two partners, and one index with three 298
partners) for whom both NAAT and traditional assay results were available. We 299
excluded 17 partnerships because of missing NAAT or traditional assay results for the 300
index subject or their partner(s), inadequate specimen collection, transcription error, or 301
multiple enrollment of a positive index subject. In addition, two exclusively male 302
partnerships were omitted from these analyses as we did not collect anal or throat 303
specimens. 304
305
Evidence of transmission of chlamydial infection, as defined by concordance within 306
partnerships, was more common among index cases testing positive by both NAAT and 307
traditional assay (N+T+) than among index cases testing positive by NAAT only (N+T-) 308
(Table 2). Evidence of transmission was observed in 39 of 52 partners (75%) of N+T+ 309
index cases, but only 14 of 31 partners (45%) of N+T- index cases (prevalence ratio 1.7, 310
95% CI: 1.1, 2.5). 311
312
The relationship between test result of the index (N+T- or N+T+) and partner 313
concordance did not vary by gender. Among male partners of N+T+ female indexes, 314
82% were concordant for Ct, compared to 46% of male partners of N+T- females. 315
Similarly, 70% of female partners of N+T+ index males were concordant, in comparison 316
to 43% of female partners of males testing positive by NAAT only. There was no 317
14
difference by the index’s or partner’s age, number of new partners in the past 3 months, 318
history of chlamydial infection, history of any STI, or antibiotic use prior to the follow-up 319
visit. Adjusting for time from screening of the index to follow-up visit also had no 320
substantial effect. However, adjusting for the timing of the partner visit reduced the 321
prevalence ratio to 1.5 (95% CI: 1.03, 2.2). Partners presenting at the same time as the 322
index participant were the most likely to test concordant. Partners presenting after the 323
index participants were less likely to demonstrate concordance (1 – 7 days: prevalence 324
ratio 0.62; 95% CI: 0.41, 0.93; > 7 days: prevalence ratio 0.65; 95% CI: 0.39, 1.07; 325
referent = 0 days). 326
327
Limiting traditional test results to culture only decreased our overall estimate of 328
concordance from 64% to 54% (prevalence ratio = 1.4, 95% CI 0.93, 2.0). It is possible 329
that differences in NAAT results by type of NAAT (LCR vs PCR) or specimen type for 330
females (urine vs vaginal swab) could influence our transmission estimates. Although all 331
women screened in the ED provided vaginal swabs for Ct testing using PCR, initially 332
women provided urine specimens, in addition to swabs, for testing by LCR. When the 333
LCR was withdrawn in 2003, male urines and female swabs were tested using PCR. 334
Restricting our concordance analysis to include: 1) only female indexes with positive 335
swab results (n=81 couples, prevalence ratio 1.7, 95% CI 1.1, 2.5) or 2) male and female 336
index subjects with positive PCR results alone (n=75 couples, prevalence ratio 1.7, 95% 337
CI 1.2, 2.5) had no effect on our transmission estimates. 338
339
Non-persistence of NAAT Positive Results 340
Index participants were screened initially in the ED and re-evaluated at follow-up; thus it 341
is possible to examine the short-term persistence of NAAT-identified Ct. Among 342
participants who had not received antibiotic therapy during the ED visit and who had 343
15
both NAAT and traditional assay results available for follow-up (n=163; 3 participants 344
had missing traditional assay results), 27 (17%) persons had no evidence of Ct infection 345
by NAAT or culture/DFA. Nine (5%) persons were NAAT-negative, but positive by 346
culture/DFA; the remaining 127 (78%) participants were NAAT-positive (Table 3). 347
348
In bivariable analyses, women were significantly more likely than men to test negative 349
for Ct after a short follow-up (23% versus 6%, risk ratio 3.6, 95% CI: 1.3, 9.9). Persons 350
who had used antibiotics in the 3 months prior to their visit in the ED were also more 351
likely to test negative at follow-up (32% versus 12%, risk ratio 2.6, 95% CI: 1.2, 5.5). 352
Index participant’s age, previous chlamydial infection, type of NAAT, and time between 353
ED testing and the follow-up visit were not associated with infection status at follow-up. 354
In multivariable analyses, only gender remained significantly associated with persistence 355
of NAAT-positive results. 356
357
Non-persistence and Partner Concordance 358
We also examined the association between persistence of NAAT-positive results and 359
concordance of infection within partnerships. Within the 83 partnerships, only one 360
partner of 9 (11%) index participants without evidence of Ct infection at follow-up tested 361
positive. In contrast, 52 partners of 74 (70%) index participants with evidence of Ct 362
infection at follow-up tested positive for Ct (prevalence ratio 6.3; 95% CI: 0.98, 40.8). 363
364
C. trachomatis typing 365
To determine whether the nucleic acids amplified by NAAT in concordant partnerships 366
represented infection by the same chlamydial strain, we compared C. trachomatis 367
serovars established from the DNA sequences of variable portions of the ompA gene, 368
encoding the major outer-membrane protein amplified in specimens from NAAT-positive 369
16
concordant couples. In 19 of 21 couples with identifiable serovars, chlamydial 370
genotypes matched exactly. Serovar D was the most commonly identified (30%), 371
followed by Ia (25%), F (20%), and E (10%). Serovars J (5%), Ja (5%), and K (5%) 372
each were identified in one couple. 373
374
Discussion 375
NAAT technology provides enhanced sensitivity to detect chlamydial infection and 376
increased opportunities for chlamydial screening compared to traditional testing 377
methods. Understanding the clinical and public health implications of the additional 378
infections identified by NAAT is critical for appropriate use of these tests. Using 379
concordance as an estimate of transmission, we observed that persons who were 380
positive by NAAT, but not by traditional assay, were significantly less likely than persons 381
who were positive by both NAAT and traditional assay to have a concordantly infected 382
sexual partner. Nonetheless, partner concordance among persons with infections 383
detected only by NAAT was moderate (45%). In addition, a substantial proportion of 384
persons (17%-22%) who screened positive by NAAT for Ct in the ED setting had no 385
evidence of chlamydial infection by NAAT and/or traditional assay after a short follow-up 386
period (median = 3 weeks). 387
388
These results suggest that while many C. trachomatis infections detected by NAAT 389
persist and are transmissible within sexual partnerships, the significance of some 390
infections detected by these tests is unclear. This uncertainty derives from the same 391
factors that are responsible for the advantages of the assay – a low limit of detection and 392
the ability to detect DNA without viable organisms. 393
394
17
A likely explanation for the diminished partner concordance among infections detectable 395
only by NAAT is reduced organism burden. The enhanced sensitivity of NAAT increases 396
the likelihood of detecting infections with relatively few organisms. Alternatively, NAAT 397
may detect ‘passive presence’ of the organism after exposure, without a true, 398
established infection. Consequently, persons with infections detectable only by NAAT 399
may be inherently less likely to transmit Ct to their partners. 400
401
The probability of transmission is influenced by factors other than organism burden, such 402
as frequency of intercourse and previous exposure. Unfortunately, because of 403
ambiguities in partner specification for participants with multiple partners, we did not 404
have precise quantitative information on the frequency of intercourse within partnerships. 405
In our study, previous self-reported chlamydial infection did not influence the relationship 406
between test result of the index and partner concordance. 407
408
We observed a surprisingly high incidence of infection clearance, especially among 409
women. Our observed clearance rate (7.8 cases per 1000 person-days) is consistent 410
with an estimated average duration of infection of 128 days, considerably shorter than 411
the commonly cited 365 days.15 This observation, coupled with our findings regarding 412
reduced concordance among partners of index participants whose follow-up NAAT was 413
negative, suggests that at least some NAAT-identified infections may be cleared 414
relatively rapidly and not transmitted. Some of these may be infections that are close to 415
being resolved, whether through antibiotic exposure or natural immune response. 16,17 416
We observed that many persons without detectable infection at follow-up had been 417
treated with antibiotics in the 3 months preceding their initial screening, suggesting that 418
NAAT may have detected residual DNA, rather than viable organisms, at the initial 419
screening evaluation 18. A proportion of the screening results could be false positives, 420
18
although we re-tested initial positive results to reduce this possibility. Sampling variability 421
associated with repeated testing of individuals with low-level infections 19 is another 422
possibility, but appears less likely because of the multiple specimens taken at follow-up. 423
The likelikhood of each of these possibilities is not known but is worthy of further clinical 424
investigation. 425
426
Since their widespread introduction more than a decade ago, the use of NAAT has 427
“resulted in considerable revision of our views of the clinical epidemiology of C. 428
trachomatis”. 20 Not only has NAAT suggested an increased prevalence of infection in 429
nearly every population tested, but it has also allowed expansion of screening programs 430
to non-clinical settings, thereby enhancing screening services available to men and to 431
asymptomatic individuals. 21 Only recently, however, have we begun to question the 432
clinical and public health significance of some additional infections identified by NAAT. 433
11,22 In this study, we examined partner concordance as a marker of the clinical 434
significance of NAAT-identified infections. Further study of the association between 435
asymptomatic NAAT-identified chlamydial infections and other clinical consequences, 436
e.g., incidence of PID, inflammation, is needed. 437
438
Very few studies have examined infection transmission within partnerships 23. Not only 439
are such studies logistically and technically challenging, but they are expensive to 440
conduct. Our study design was intended to enhance our understanding of the likelihood 441
of transmission of NAAT-diagnosed infection in a sexual partnership – and to do so with 442
minimal risk to our study subjects. Several alternate study designs were considered by 443
our research team, but ultimately rejected. For ethical reasons, we chose not to test 444
index subjects for chlamydia using traditional assay. Only subjects who tested positive 445
for chlamydia by NAAT and their recent sexual partners had urethral or cervical samples 446
19
obtained for culture during the clinical examination. We chose an Emergency 447
Department population rather than a STI clinic setting as we were interested 448
understanding the clinical consequences of largely asymptomatic and unrecognized Ct 449
infections detectable by NAAT but not by traditional methods. As a result, it was 450
necessary to screen over 6,000 individuals. We used concordance as an estimate of 451
transmission. Because we began with a cross-sectional screening evaluation, the timing 452
of the prevalent infection in the index case was unknown. Consequently, the direction of 453
transmission between index and partner could not be established. Generalization of our 454
findings may be constrained by our sample selection – patients recruited from an urban 455
Emergency Department – and by the incomplete recruitment of index participants and 456
their partners. In general, index participants had a similar risk profile to persons who 457
were not recruited into the study. We were unable to compare characteristics of 458
partners who did and did not enroll; however, it seems unlikely that characteristics on 459
which selection might occur would bias enrollment with respect to traditional test status, 460
the basis for our primary hypothesis. 461
462
The advent of NAAT screening for chlamydial infection has vastly expanded 463
opportunities for prevention of the serious consequences of untreated infection. 464
However, questions remain regarding the clinical and public health consequences of 465
some infections detected by NAAT. The interpretation of a positive NAAT or any other 466
screening method as an ipso facto indicator of disease can have important personal 467
implications. While failure to diagnose a chlamydial infection can negatively affect 468
health, incorrectly identifying individuals as infected can damage relationships. Because 469
many Ct infections identified by NAAT screening are asymptomatic and easily treated, 470
there has been a tendency to presume that a positive result indicates the presence of 471
disease, with the responsibility to inform and provide treatment. While we strongly 472
20
believe that persons with a positive NAAT should be informed and treated, our study 473
demonstrates that some NAAT-detected infections may not represent clinically active 474
disease or transmissible infections. Patients, especially those with low risk profiles or 475
those screened from a low Ct-prevalence population, 21 should be counseled about their 476
test result accordingly. Guidelines for testing, patient counseling and management 477
should be formulated so that users of this remarkable and powerful tool -- physicians, 478
patients, and researchers -- are aware of not only NAAT’s advantages, but also its 479
limitations. 480
481 482
Contributors: S Rogers, W Miller, C Turner, P Leone, J Ellen, R Rothman, and D 483
Kanouse contributed to the conception and design of the study. S Rogers, W Miller, C 484
Turner, J Ellen, J Zenilman, R Rothman, C Gaydos, M Hobbs contributed to the 485
acquisition of data. S Rogers, W Miller, M Villarroel, A Al-Tayyib, and D Kanouse 486
contributed to questionnaire design. S Rogers, M Villarroel, and L Ganapathi 487
contributed to data management. S Rogers, W Miller, M Villarroel and C Turner 488
contributed to the analysis and interpretation of data. All authors contributed to writing 489
the manuscript. 490
Conflicts of Interest: We declare that we have no conflicts of interest. 491
Acknowledgment: We thank Don Orr, Martina Morris, and Heather Miller for serving as 492
scientific advisors to this project. We also thank Sarah Mobius for her managerial 493
contribution to the study and Sheping Li at RTI for programming and data management; 494
Ambreen Khalil and Chadd Krauss for their oversight of interviews at the Johns Hopkins 495
Adult Emergency Department; Joan Bess, Kenya S. Stewart and Nancy Willard of the 496
Johns Hopkins Adolescent Health Research Group for outreach support; and Mary Ann 497
Knott-Grasso, MS, CPNP for providing patient care at the Johns Hopkins General 498

21
Clinical Research Center. We also thank the laboratory personnel from the Department 499
of Medicine, University of North Carolina at Chapel Hill, including Marcia Stedman, John 500
Schmitz, and Dana Lapple; and Jeff Younger, Billie Jo Wood, and Hope L. Johnson from 501
the Johns Hopkins School of Medicine, Department of Infectious Diseases. 502
503
504
1 Miller WC, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA 2004; 291(18):2229-36. 2 Turner CF, Rogers SM, Miller HG, et al. Untreated gonococcal and chlamydial infection in a probability sample of adults. JAMA 2002; 287(6):726-33. 3 Institute of Medicine. The Hidden Epidemic: Confronting Sexually Transmitted Diseases. Washington, DC: National Academy Press, 1996. 4 Schacter J. Chlamydia trachomatis: the more you look the more you find – how much is there? Sex Transm Dis 1998; 25(5): 229-31. 5 Stamm WE. Chlamydia trachomatis infections of the adult. In: Holmes KK, Sparling PF, Mardh P, Lemon SM, Samm WE, Piot P, Wasserheit JN, eds. Sexually Transmitted Diseases. New York: McGraw Hill, 1999, 407-22. 6 Rogers SM, Miller HG, Miller WC, Zenilman JC, Turner CF. NAAT-identified and self-reported gonorrhea and chlamydial infections: different at-risk population subgroups? Sex Transm Dis 2002; 29(10):588-96. 7 Cooley PC, Rogers SM, Turner CF et al. Using touch-screen audio-CASI to obtain data on sensitive topics. Comp in Human Beh 2001; 17:285-93. 8 Watson EJ, Templeton A, Russell I, Paavonen J, Mardh PA, Stary A, Pederson BS. The accuracy and efficacy of screening tests for Chlamydia trachomatis: A systematic review. J Med Microbiol 2003; 51:1021-1031. 9 Schacter J, McCormack, Chernesky M, Martin DH, Van Der Pol B, Rice PA, Hook EW, Stamm WE, Quinn TC, Chow JM. Vaginal swabs are appropriate specimens for diagnosis of genital tract infection with Chlamydia trachomatis. 2003. J of Clin Microbiol 41(8): 3784-3789. 10 Bandea CI, Kubota K, Brown TM, et al. Typing of Chlamydia trachomatis strains from urine samples by amplification and sequencing the major outer membrane protein gene (omp1). Sex Transm Infect 2001; 77:419-422. 11 Lysen M, Osterlund A, Rubin CJ, et al. Characterization of ompA genotypes by sequence analysis of DNA from all detected cases of Chlamydia trachomatis infections
22
during 1 year of contact tracing in a Swedish County. J Clin Microbiol 2004; 42:1641-1647. 12 Dean D, Stephens RS. Identification of individual genotypes of Chlamydia trachomatis from experimentally mixed serovars and mixed infections among trachoma patients. J Clin Microbiol 1994; 32:1506-1510). 13 Gen-Bank Accession numbers AF118868, AY535166, DQ064279, DQ064289, DQ064291, DQ064292, DQ064293, DQ064299, M14738, M17342, M17343, M36533, U78528, X52080, X55700, X62919, X62921. 14 Hardin JW, Hilbe JM. Generalized Estimating Equations. Boca Raton, Fl: Chapman and Hall/CRC, 2003. 15 Brunham RC, Plummer FA. A general model of sexually transmitted disease epidemiology and its implication for control. Med Clin North Am 1991; 74(6):1339-52. 16 Moore SA, Sillekens PT, Jacobs MV et al. Monitoring of Chlamydia trachomatis infections after antibiotic treatment using RNA detection by nucleic acid sequence based amplification. Mol Pathol 1998; 51(3):149-54. 17 Bianchi A, Bogard M, Cessot G et al. Kinetics of Chlamydia trachomatis clearance in patients with azithromycin, as assessed by first void urine testing by PCR and transcription-mediated amplification. Sex Trans Dis 1998; 25(7):366-7. 18 Gaydos CA, Crotchfelt C, Howell MR, Kralian S, Hauptman P, Quinn TC. Molecular amplification assays to detect chlamydial infections in urine specimens from high school female students and to monitor the persistence of chlamydial DNA after therapy. Journal of Infectious Diseases 1998; 177(2):417-424. 19 Schachter J, Chow JM, Howard H, Bolan G, and Moncada J. Detection of Chlamydia trachomatis by nucleic acid amplification testing: Our evaluation suggests that CDC-recommended approaches for confirmatory testing are ill-advised. J Clin Micro 2006; 44(7):2512-17. 20 Stamm WE. Chlamydia trachomatis—The persistent pathogen: Thomas Parran Award Lecture. Sex Transm Dis 2001; 28(12):684-89. 21 Zenilman JM, Miller WC, Gaydos C, Rogers SM, Turner CF. LCR Testing for gonorrhea and chlamydia in population surveys and other screenings of low prevalence populations: Coping with decreased positive predictive value. Sex Transm Infect 2003; 79(2):94-7. 22 Hagdu A, Dendukuri N, Hilden J. Evaluation of a nucleic acid amplification test in the absence of a gold-standard test: a review of the statistical and epidemiological issues. Epidemiology 2005; 16(5):604-12. 23 Quinn T, Gaydos C, Shepherd M, Bobo L, Hook EW, Viscidi R, Rompalo A. Epidemiologic and microbiologic correlates of chlamydia trachomatis infection in sexual partnerships. Journal of the American Medical Association 1996; 276(21):1737-1742.

23
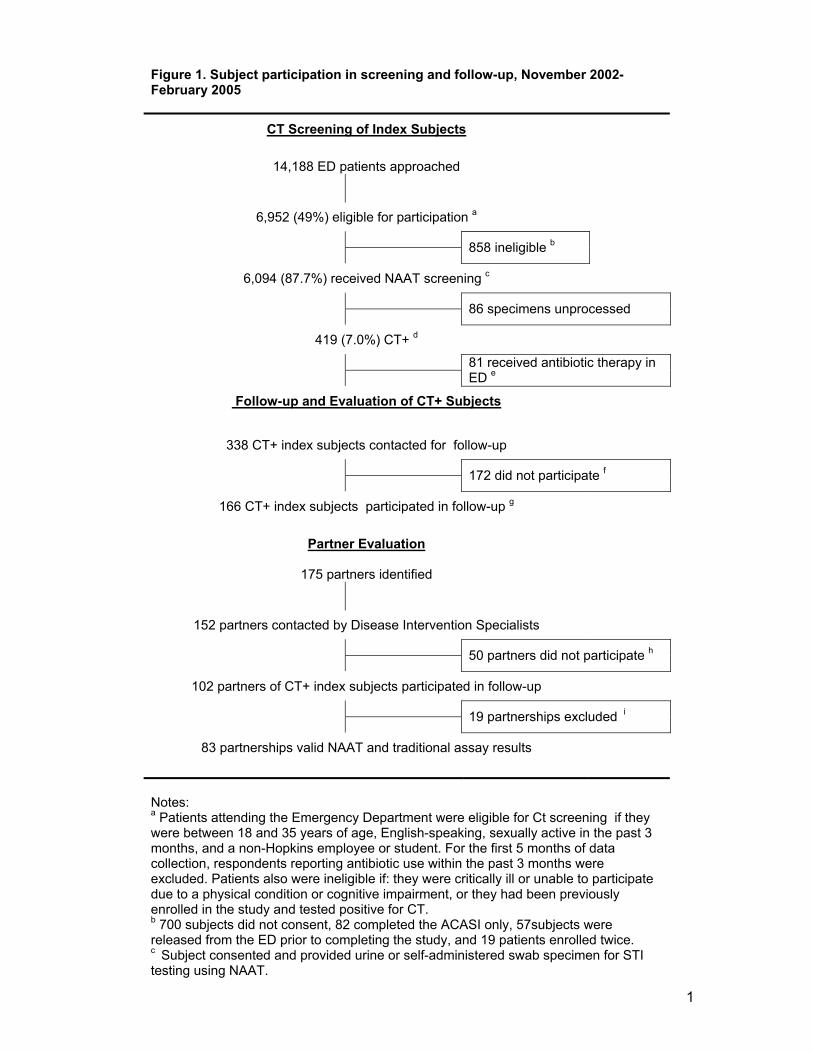
1
Figure 1. Subject participation in screening and follow-up, November 2002-February 2005
CT Screening of Index Subjects
14,188 ED patients approached
6,952 (49%) eligible for participation a
858 ineligible b
6,094 (87.7%) received NAAT screening c
86 specimens unprocessed
419 (7.0%) CT+ d
81 received antibiotic therapy in ED e
Follow-up and Evaluation of CT+ Subjects
338 CT+ index subjects contacted for follow-up
172 did not participate f
166 CT+ index subjects participated in follow-up g
Partner Evaluation
175 partners identified
152 partners contacted by Disease Intervention Specialists
50 partners did not participate h
102 partners of CT+ index subjects participated in follow-up
19 partnerships excluded i
83 partnerships valid NAAT and traditional assay results
Notes: a Patients attending the Emergency Department were eligible for Ct screening if they were between 18 and 35 years of age, English-speaking, sexually active in the past 3 months, and a non-Hopkins employee or student. For the first 5 months of data collection, respondents reporting antibiotic use within the past 3 months were excluded. Patients also were ineligible if: they were critically ill or unable to participate due to a physical condition or cognitive impairment, or they had been previously enrolled in the study and tested positive for CT. b 700 subjects did not consent, 82 completed the ACASI only, 57subjects were released from the ED prior to completing the study, and 19 patients enrolled twice. c Subject consented and provided urine or self-administered swab specimen for STI testing using NAAT.

2
d As determined by repeatedly positive NAAT on the same specimen. Initially male and female urine specimens were tested using LCR assay (Abbott Laboratories). After August 2003, male urine and female self-administered vaginal swabs were tested using the COBAS Amplicor assay (Roche Diagnostics). This change was necessitated by the specimen requirements of the Roche Amplicor assay which was used after Abbott Laboratories discontinued the LCR. e Ct+ index subjects who received antibiotic therapy during their ED visit were not re-contacted for follow-up. f 40 subjects provided insufficient locating information, 44 received healthcare elsewhere, 40 received treatment only at the GCRC, 16 did not show for their scheduled GCRC appointment, and 22 either refused treatment, were incarcerated, a non-resident of Baltimore, or in substance abuse rehabilitation. g Following enrollment, IDs were switched on 2 index subjects' specimens, 2 indexes were actually partners of 2 previously enrolled Ct-positive index subjects, and 1 subject did not have complete NAAT and traditional assay results. h 17 partners were treated elsewhere, 20 were out of jurisdiction or not located, 8 refused treatment, and 5 received treatment and an examination only at the GCRC. i Two partners were enrolled at home and provided specimens for NAAT only. An additional 14 partnerships were missing complete NAAT and traditional assay results, 1 partner was enrolled 6 months after the index, and specimen IDs were mislabeled during collection for 2 partnerships.
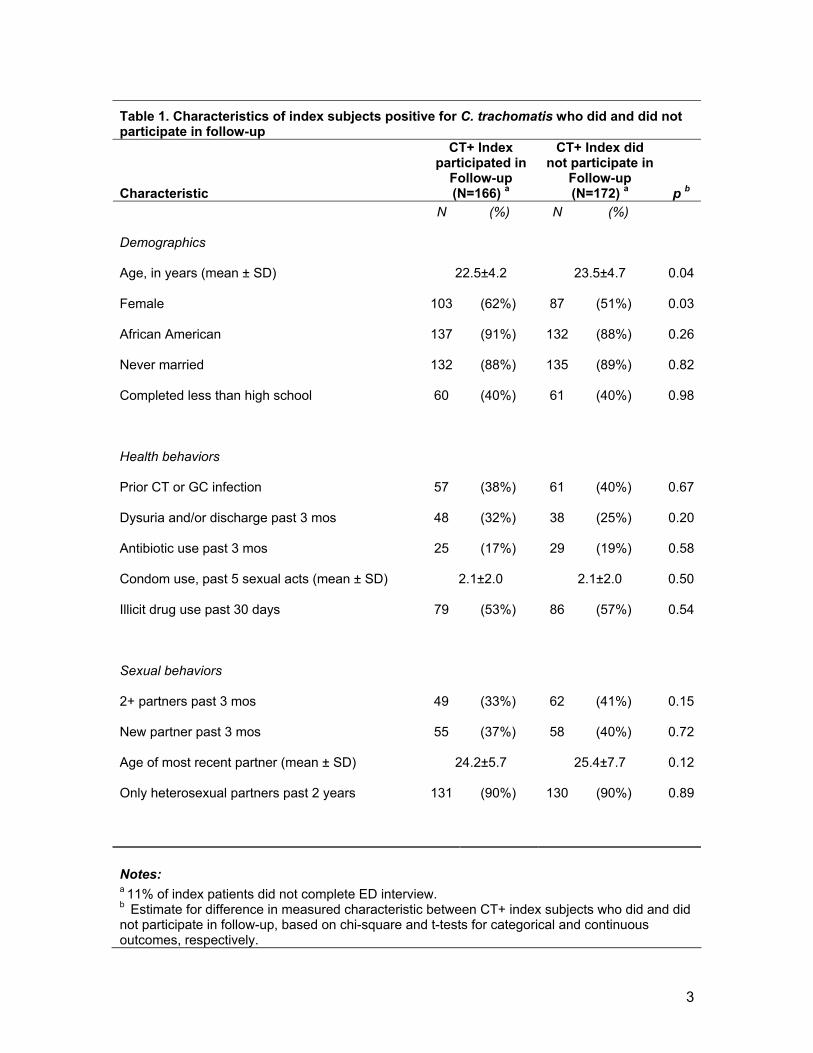
3
Table 1. Characteristics of index subjects positive for C. trachomatis who did and did not participate in follow-up
Characteristic
CT+ Index participated in
Follow-up (N=166) a
CT+ Index did not participate in
Follow-up (N=172) a p b
N (%) N (%)
Demographics
Age, in years (mean ± SD) 22.5±4.2 23.5±4.7 0.04
Female 103 (62%) 87 (51%) 0.03
African American 137 (91%) 132 (88%) 0.26
Never married 132 (88%) 135 (89%) 0.82
Completed less than high school 60 (40%) 61 (40%) 0.98
Health behaviors
Prior CT or GC infection 57 (38%) 61 (40%) 0.67
Dysuria and/or discharge past 3 mos 48 (32%) 38 (25%) 0.20
Antibiotic use past 3 mos 25 (17%) 29 (19%) 0.58
Condom use, past 5 sexual acts (mean ± SD) 2.1±2.0 2.1±2.0 0.50
Illicit drug use past 30 days 79 (53%) 86 (57%) 0.54
Sexual behaviors
2+ partners past 3 mos 49 (33%) 62 (41%) 0.15
New partner past 3 mos 55 (37%) 58 (40%) 0.72
Age of most recent partner (mean ± SD) 24.2±5.7 25.4±7.7 0.12
Only heterosexual partners past 2 years 131 (90%) 130 (90%) 0.89
Notes: a 11% of index patients did not complete ED interview. b Estimate for difference in measured characteristic between CT+ index subjects who did and did not participate in follow-up, based on chi-square and t-tests for categorical and continuous outcomes, respectively.
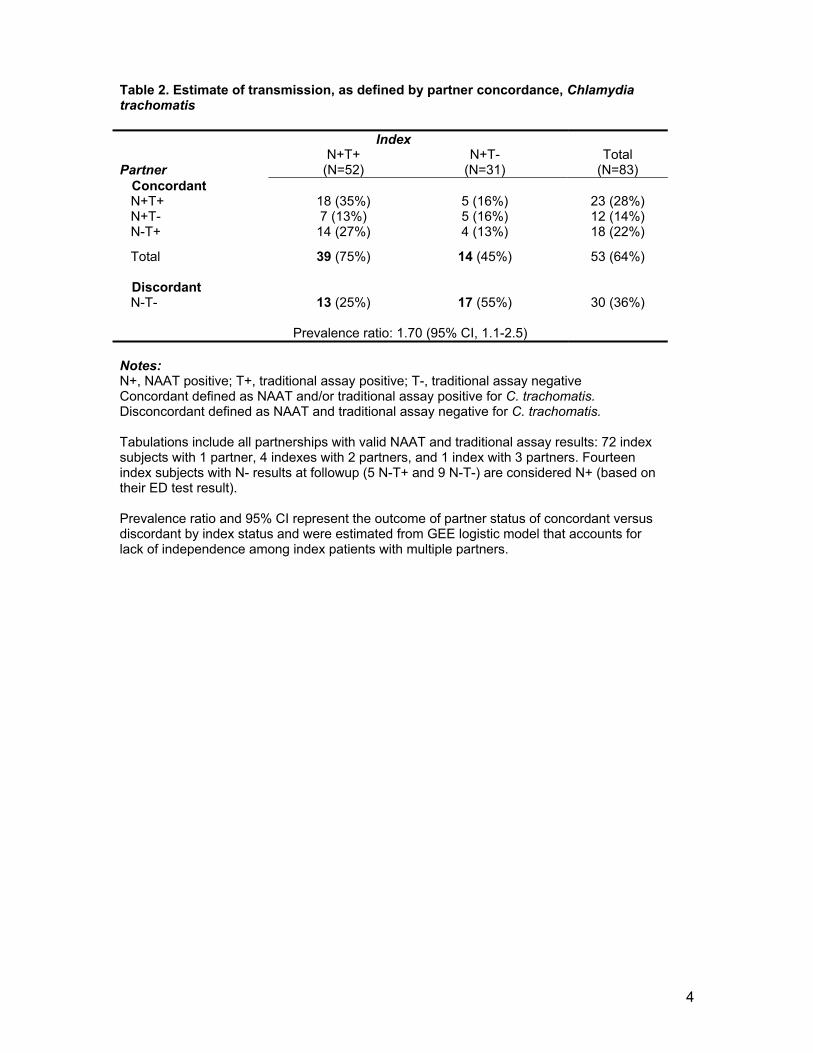
4
Table 2. Estimate of transmission, as defined by partner concordance, Chlamydia trachomatis Index N+T+ N+T- Total Partner (N=52) (N=31) (N=83)
Concordant N+T+ 18 (35%) 5 (16%) 23 (28%) N+T- 7 (13%) 5 (16%) 12 (14%) N-T+ 14 (27%) 4 (13%) 18 (22%)
Total 39 (75%) 14 (45%) 53 (64%)
Discordant N-T- 13 (25%) 17 (55%) 30 (36%)
Prevalence ratio: 1.70 (95% CI, 1.1-2.5) Notes: N+, NAAT positive; T+, traditional assay positive; T-, traditional assay negative Concordant defined as NAAT and/or traditional assay positive for C. trachomatis. Disconcordant defined as NAAT and traditional assay negative for C. trachomatis. Tabulations include all partnerships with valid NAAT and traditional assay results: 72 index subjects with 1 partner, 4 indexes with 2 partners, and 1 index with 3 partners. Fourteen index subjects with N- results at followup (5 N-T+ and 9 N-T-) are considered N+ (based on their ED test result). Prevalence ratio and 95% CI represent the outcome of partner status of concordant versus discordant by index status and were estimated from GEE logistic model that accounts for lack of independence among index patients with multiple partners.

5
Table 3. Results of testing for C. trachomatis at follow-up among NAAT positive index participants
NAAT positive index participants
Total Male Female Follow-up test result
N-T- 27 (17%) 4 ( 6%) 23 (23%) N-T+ 9 ( 5%) 3 ( 5%) 6 ( 6%) N+T+ 83 (51%) 36 (57%) 47 (47%) N+T- 44 (27%) 20 (32%) 24 (24%) Total 163 63 100
Fisher’s exact p=0.03
Notes: N+, NAAT positive; T+ traditional assay positive; N- NAAT negative; T- traditional assay negative
Related Documents











