Component Therapy in Obstetrics Dr. V. L. Deshmukh M.D.(Obst.&Gyn) Associate Professor Dept. of Obstet. & Gynaec. Govt. Medical College AURANGABAD

Component therapy in obstetrics
Aug 07, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Component Therapy in Obstetrics
Dr. V. L. DeshmukhM.D.(Obst.&Gyn)
Associate Professor
Dept. of Obstet. & Gynaec.
Govt. Medical College
AURANGABAD

Introduction
• Goal of transfusion therapy is to provide the most appropriate blood product for the patient
• Variety of components can be obtained from one unit of blood hence many patients may benefit from one unit of blood.
Indications
Indications for transfusion of blood or blood products are to restore or maintain :
1. Blood volume
2. O2 carrying capacity3. Hemostasis4. Leucocyte function
(Ref. : Blood banking & transfu Med 2nd edi)
Components
- Whole blood
- PCV
- Platelets
- FFP
- Cryoprecipitate
- Others

. Animal to animal --- Richard Lower ,1665• Animal to human --- Jean Denis , 1667
. Human to human --1818, James Blundell
-- 1900 The elucidation of the ABO blood
group system by Landsteiner
-- 1914 Lewisohn - used citrate
-- 1940 Landsteiner and Wiener, in, describe Rh typing




Whole Blood
• Indication when O2 carrying capacity is low & associated with clinical symptoms of hypovolumia.
• Limited clinical settings• When blood loss is more than 20% of the
total blood volume e.g. Placenta previa, abruptio placenta.
(Reference : National Guidelines for Transfusion Therapy, Nov. 2002)
Whole blood (Contd..)
1. Identification2. Equipment : 19 Gauge needle & transf. Set.3. NO ADDITION OF ANY DRUG OR
SOLUTION.4. Infusion rate – initially slow, 2-3 hrs.5. Administration 5 ml/min for 15 min then
increase the rate.
(Ref. : Menitove JE. Transfusion : Blood and blood components
IN : Manual of Clinical Hematology, 2nd edi, 1995)

Whole Blood
• Outcome : Hb% - 1 g% Hct – 3%
Take Universal Biohazard Precautions
(Ref : High risk obstet. CE Online. Crit Care Nurse 2006, Aug 24(4):54-61)

PCV
• 250-300 ml • Expiry 35 days• CPDA – preservative• Dose• Infusion Same as whole blood• Outcome• Indication : When O2 carrying capacity is
low & no need to increase the plasma volume
PCV
• PCV in anaemic patient should be used to correct symptoms that are a direct result of anaemia only when it is determined that other treatment regimens are not effective.
e.g. pregnancy at termPatient with labour with Hb < 7 gm%Pregnant patient with Hb < 5 gm%
Ref : Menitove JE. Transfusion : Blood and blood components IN : Manual of Clinical Hematology, 2nd edi, 1995.

Platelets• Indication – thrombocytopenia• Decision to transfuse depends on :
- Clinical condition of patient- Number of platelets in patients body- Function of the platelets in patients body- Cause of thrombocytopenia
• Recommended levels :- Normal delivery – 20,000/dl- LSCS operative - > 50,000/dl

PlateletsThrombocytopenia and pregnancy :• Gestational thrombocytopenia• HELLP• Severe PIH/Eclampsia• Drug induced• Infections – bacterial/viral• TTP• ITP• Massive blood transfusion• APA syndrome• Abrptio placentaRef : Scientific foundation of ObGy, 2nd edi

Platelets• Concept of CCI• Corrected count increment • CCI – 10 min – 1 hr > 7,5000/dl
18 to 24 hrs > 4,600/dl• If CCI less at 10 min to 1 hr causes are : rapid
destruction by antiplatelet antibodies• If CCI less at 24 hrs causes are : sepsis, DIC,
fever(Ref : Menitove JE. Transfusion : Blood and blood components
IN : Manual of Clinical Hematology, 2nd edi, 1995)
FFP
• Separated from whole blood within 8 hrs. by centrifugation
• Contains all clotting factors• Volume 200-250 cc• Kept at –18°C• Dose : 15 ml/kg or 4 units in an adult• Infusion rate – 10 min – 1 hr.• ABO compatibility required• Contents no platelet

FFPIndications :• Coagulation factor deficiency• Acute DIC• Treatment of TTP• Documented coagulopathy in setting of massive
transfusion• Liver diseaseEfficacy of transfusion is assessed with PT, APTT
or special factor assay(Ref : Menitove JE. Transfusion : Blood and blood components
IN : Manual of Clinical Hematology, 2nd edi, 1995)

FFP
Indication of FFP in Obstetrics :• Abruptio placentae• Septic abortion• HELLP• IUFD• Amniotic fluid embolism• Puerperal sepsis• Massive transfusion• Severe PIH/Eclampsia• Placenta acreta• AFLP

Cryoprecipitate
• Cold insoluble portion of plasma• FFP – thawed at 1-6°C – cryo is obtained• Content : Factor VIII, fibrinogen, XIII, VIII
WF factor• Dose – 10 bags increase the fibrinogen
level by 75 mg/dl, factor VIII – by 30%• Indication – Acute DIC

Components FactorComponent Coagulation factor Volume
PCV -- 250 cc
FFP All coagulation factors + fibrinogen
200 cc
Platelets Platelets + All coagulation factors
50 cc
Cryo VIII C, Von. Will 5-20 cc
Ref : Obstet Gynecol Clin N Am 2007;34:443-58.

• China, 1000 BC The soul was contained in the blood.• Egyptians bathed in blood for their health.• Romans drinking the blood of fallen gladiators to gain strength and
vitality and to cure epilepsy.• The practice of bathing in blood as it
cascaded from a sacrificial bull, was practiced by the Romans.
Blood in History

DIC
• Multyorgan dysfunction caused by microthrombi
• Bldg is caused by consumption of platelet, fibrinogen, factor V,VIII
• Secondary fibrinolysis

DIC
• Whenever exposure of blood to tissue factor takes place, DIC occurs
• Tissue factor is a result of exposure of the endothelial cells to foreign substance e.g. malignancy, placenta, traumatized tissue
• Endotoxins liberated from sepsis act on the endothelial cells

DIC
• ENDOTHELIAL DAMAGE
• Thromboplastin released
• Microthrobi formation
• DIC
• Consumption of all coagulation factors

Test for Hemostatic Function
Test Volume Interpretation
Blood smear
1.2 – 3.8 lac/mm
Platelets
Bleeding time
3-8 min To assess platelet plug formation deranged in throbocyto. Function defect of platelets. Von Will def.
Normal in coagulation factor defect
Prothrombin time
17-16 sec. Extrinsic pathway
Common pathway
aPTT 22-37 sec Intrinsic pathway
Common pathway
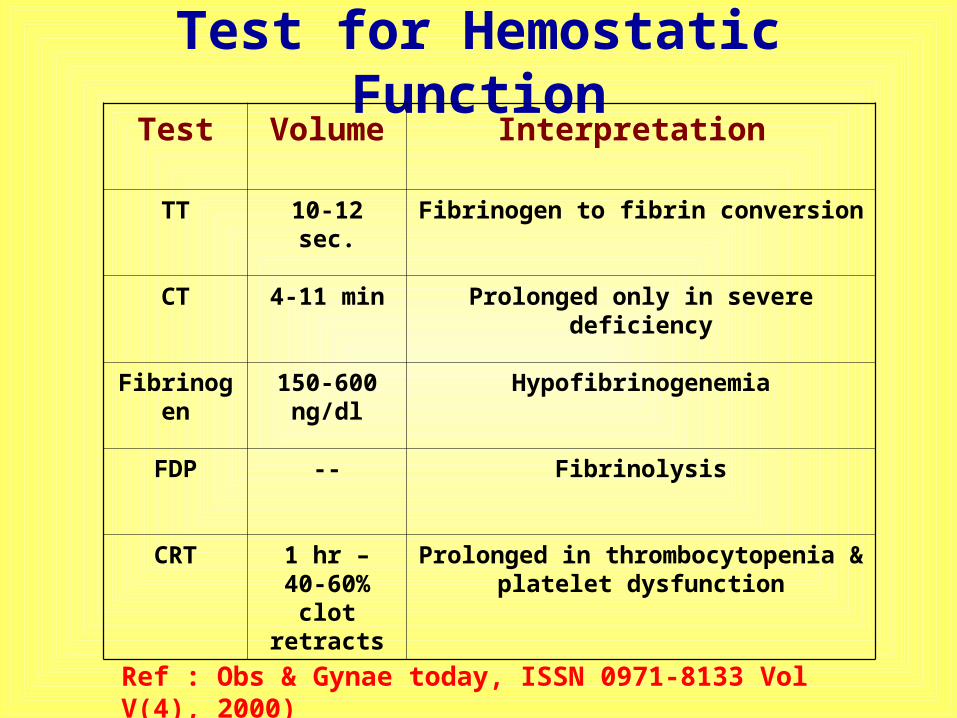
Test for Hemostatic FunctionTest Volume Interpretation
TT 10-12 sec. Fibrinogen to fibrin conversion
CT 4-11 min Prolonged only in severe deficiency
Fibrinogen 150-600 ng/dl
Hypofibrinogenemia
FDP -- Fibrinolysis
CRT 1 hr – 40-60% clot retracts
Prolonged in thrombocytopenia & platelet dysfunction
Ref : Obs & Gynae today, ISSN 0971-8133 Vol V(4), 2000)

REMEMBER…REMEMBER…THE DECISION FOR BLOOD TRANSFUSION SHOULD ALWAYS BE A BALANCE BETWEEN

Haemorrhage• Rapid & continuing blood loss is life
threatening.• Ensure tissue oxygenation is maintained at a
level consistent with avoidance of critical ischaemic organ damage or irreversible organ failure.
• Blood grouping & Rh typing• Co-ordinated effort between clinician & blood
bank• Massive haemorrhage protocol outlined in
every institute
Haemorrhage
• Management demands
- Skill
- Speed
- Knowledge
- Prompt action
- Good communication

Haemorrhage• Haem in obs may be due to acute blood
loss • Secondary to placenta previa, rupture
uterus• Or it may be due to DIC• In conditions like HELLP, severe PIH• ABRUPTIO PL -blood loss may be due to
DIC +acute blood loss• All this conditions can lead to massive
haem

Blood Volume
% Supine Sitting
B.P P B.P P
N 100 N N N N
- 500 -5 N N N N or ^
-1000 -10 : 15 N N or ^ N or ^ ^
- 1500 -20 N or v ^ v ^ or v
- 2000 - 30 v ^ or v vv ^ or v
Response Of BP and P to Hypovolemia

Massive Haemorrhage
Definition :
• Ongoing blood loss in adult > 150 ml/min• Replacement of > 50% of blood volume in
3 hrs.• In 24 hrs – 10 units of blood transfusion
required e.g. Atonic PPH, Rupture uterus(Ref : Am Soc Anaes Pract. Guidelines for Obst Anaes – An
Updated Report 2007;106(4):1-21.
Massive Haemorrhage
• Call for senior help early• Inform blood bank• Specific :
- Adequate oxygenation- Patent airway- Restore circulating blood volume- Start component therapy

Component Therapy
• Early RBC transfusion
• Anticipate coagulopathy
• Maintain or restore normothermia
• Evaluate therapeutic response
(Ref : Need for maternal critical care in Obst : A population based analysis. Int J Obstet Anaesth 2003;11(4):260-64)

Massive Haemorrhage
1. Direct contact and briefing 2. Good communication between
anaesthetist, haematologist and surgical colleauges.
3. Management of patient should be tailored according to cause of haemorrhage and disturbed hemostatic system.
4. Metabolic disturbances from gradual loss of large blood will differ from that of a acute massive loss.

Massive Haemorrhage
1. Patent airway2. 100% O23. IV access
4. Laboratory test - Full blood count- PT- APTT- Fibrinogen - KFT- Electrolytes
Massive Haemorrhage
• Send laboratory tests every 4 hourly or after replacement of 1/3rd of blood volume to access the efficacy of treatment.
• If coagulopathy detected expert advice from haematologist for interpretation and optimum correction.
Ref : A multicenter randomized control clinical trial of transfusion requirement in critical care. N Engl J Med 1999;6:409-17.

Massive Haemorrhage
Restore volume :• Perfusion pressure should be maintained • Prolonged hypoperfusion leads to
- Increase capillary permeability- Consumption of coagulation factor
in microvasculature.- Release of inflammatory mediators
• Leading to coagulopathy & secondary end organ injury

Massive Haemorrhage
• Restore volume :The volume Timing Imp. for good outcomeExtent
• Monitoring depend on ;CVPOutputHeart rate
• Increase in B.P. due to inotropes is deceptive

Massive Haemorrhage
• Restore volume : 2 lit. of fluid in adultCrystalloid ColloidCheap Expansion of BV efficiently
Easy to admin. microvascular flow
No adv. Effect Better preserv. Of oncotic pressure
No effect on coagu. Can cause allergic reaction
Short lived in circu. Adverse effect on coagulation & renal function
(Ref : Hippala S. Replacement of massive blood loss. Vox Sang 1998;74:399-407.)

Component Therapy
• Start component therapy• Decision by senior, experience staff• Supply RBCs• Request platelets• Request FFP - When blood loss I > 1.5
times of blood volume 15 mg/kg = 1 lit or 4 units till PT, APTT is < 1.5 times normal
• Request cryo if fibrinogen is < 100 mg/dl
Component Therapy
• Hemostatic defects in large transfusions is due to dilution & consumption
• Massive transfusion leads to dilution of coagulation factors
• Reduction in platelets, and clotting factors • Prolonged of PT & APTT• Sequence –
Deficiency of fibrinogen & coagulation factors, thrombocytopenia

Component Therapy
• In emergency – checking and administration of blood products should be strictly carried out.
• Most transfusion related morbidity is due to incorrect blood transfusion.
• Hemodyanamic, hemostatic and metabolic derangements occur with the clinical condition and speed and effectiveness of resuscitation.
Component Therapy
• Early use of FFP may eliminate the use of cryoprecipitate, but if fibrinogen level < 100 mg/dl – cryoprecipitate is given.
• Minimum dose in adult of cryoprecipitate is 10 packs gives 1.5 – 3.0 gm of fibrinogen.
• Platelets if < 50,000/dl - supply
DIC
Should be kept in mind :- PT- APTT Diagnosis- Dilutional thrombocyto.
Give 4-6 units FFP 5 pints of platelets10 units of cryo
Send blood sample regularly to assess the coagulation status
Ref : Guidelines National blood users group, Nov. 2002

DIC
• Send : Hb, Hct, platelets, PT, APTT, serum fibrinogen.
• Monitoring & coagulation screening should be continued
• If bleeding recurs, the monitoring should be intensified.

Normothermia
• Restore normothermia• Hypothermia is exaberated due to cold
blood infusion and low ambient temp.• Hypothermia leads to increase blood loss,
prolonged PT, APTT, platelet dysfunction, enhance fibrinolysis & increase release of potassium.
• Monitor core temperature because it is important reversible hemostatic factor

Evaluation
• Evaluate the response - Pulse- B.P.- CVP - Output- Hemoglobin- Hct
Note the details of blood component used e.g. timing and volume

Massive Haemorrhage – New invention
• Promising new alternative drug.• Identical in structure & function to
human factor VIIa• Used in uncontrolled bleeding which is
life threatening.
• rFVIIa it augments the intrinsic clotting
pathway by binding with tissue factor &
directly activating factor IX & X

Massive Haemorrhage – new invention
• Used effectively offlable to control PPH• Effective dose is 50-100 g/kg IV every 2
hrly. Until hemostasis is achieved.• Ensure adequate platelet & clotting factors
are present.• Give in early phases of shock, good in
action • Action decreased by hypothermia and
acidosis• No risk of viral transfusion

Complications of Blood
Transfusion
• Febrile reactions• Bacterial contamination• Immune reactions• Physical complications
– Circulatory overload– Air embolism– Pulmonary embolism– Thrombophlebitis– ARDS
• Metabolic complications– Hyperkalaemia– Citrate toxicity & hypocalcaemia– Release of vasoactive peptides– Release of plasticizers from PVC-
phthalates• Haemorrhagic reactions
– After massive transfusion of stored blood
– Disseminated intravascular coagulation
• Transmission of disease– Hepatitis, CMV. EBV– AIDS (Factor VIII)– Syphilis– Brucellosis– Toxoplasmosis– Malaria– Trypanosomiasis
• Haemosiderosis– After repeated transfusion in
patients with haematological diseases

Important Points
1. Errors in transfusion
2. Transfusion transmitted infections
3. Adverse effects associated with transfusion
4. Autologous transfusion
5. Intraoperative cells salvage

REMEMBER…REMEMBER…THE DECISION FOR BLOOD TRANSFUSION SHOULD ALWAYS BE A BALANCE BETWEEN

Conclusion
• Deaths are avoidable if early and effective intervention in initial golden hour is provided
• It has a major impact on eventual outcome

Related Documents











