Clinical study Complications related to positioning in posterior fossa craniectomy G.P. Rath, P.K. Bithal * , A. Chaturvedi, H.H. Dash Department of Neuroanaesthesiology, Neurosciences Centre, Room 709-A, All India Institute of Medical Sciences, New Delhi 110 029, India Received 3 December 2005; accepted 21 February 2006 Abstract To compare complications associated with surgical position, a retrospective study was conducted on 260 patients who underwent pos- terior fossa craniectomy. Data collected from the records included demographic profile, American Society of Anesthesiologists’ physical status score, neurological status, cranial nerve involvement, associated medical illnesses, anaesthetic technique, patient position, haemo- dynamic changes, duration of surgery, venous air embolism (VAE), blood loss/transfusion, postoperative complications, duration of ICU stay, and postoperative neurological status. Statistical analysis was done using the Chi-square test and independent t-tests. The demo- graphic profile and preoperative associated medical illnesses of patients were comparable between groups. The incidence of end-tidal car- bon dioxide (EtCO2) detected VAE was more (p = 0.00) in the sitting position than the horizontal positions (15.2% vs. 1.4%). Blood loss/ transfusion and the duration of surgery were significantly higher in the horizontal position (p < 0.05). Brainstem handling was the most common cause of prolonged postoperative mechanical ventilation and was seen more in the sitting position. Lower cranial nerve functions were preserved better in the sitting position (p < 0.05). Most postoperative complications (surgical or otherwise) were comparable between the groups (p > 0.05). Most patients in both groups developed mild-to-moderate disability with independent lifestyle at the seventh post- operative day. To conclude, both sitting and horizontal positions can be used safely in posterior fossa surgeries. Ó 2006 Elsevier Ltd. All rights reserved. Keywords: Posterior fossa craniectomy; Surgical positions; Complications 1. Introduction Posterior fossa craniectomy can be performed either in the sitting or horizontal position. The use of the sitting po- sition is controversial because of the significant potential for complications such as the venous air embolism (VAE), intraoperative haemodynamic instability, tension pneumocephalus, lingual and laryngeal oedema, nerve inju- ries and quadriparesis. 1–8 The specific advantages which made this position popular include improved surgical expo- sure and anatomical orientation, improved venous drain- age, haemostasis, gravitational drainage of the cerebrospinal fluid (CSF) and blood from the operative field, improved access to the endotracheal tube, chest wall and upper extremities by the anaesthesiologist, free dia- phragmatic movements, and the ability to observe the face for signs of surgical stimulation of cranial nerves. 1–8 De- spite these advantages the use of the sitting position ap- pears to be diminishing because of its potential for serious complications and malpractice claims. The decline has been observed worldwide. In India there is also pro- nounced reduction of use of the sitting position in various neurosurgical centres (personal communication) for the reasons cited above. In our institution, the sitting position is still used, although the frequency is reduced as compared to previous years. It is used depending on the surgeon’s preference over other horizontal positions used for poster- ior fossa craniectomies. Presently at our centre, it is mainly used for excision of brain stem gliomas and posterior third ventricular tumours. This study was undertaken to assess the perioperative complications in patients who underwent posterior fossa craniectomy in the sitting and horizontal positions. 0967-5868/$ - see front matter Ó 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.jocn.2006.02.010 * Corresponding author. Tel.: +91 11 26588700 4347; fax: +91 11 26588663. E-mail address: [email protected] (P.K. Bithal). www.elsevier.com/locate/jocn Journal of Clinical Neuroscience 14 (2007) 520–525

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
www.elsevier.com/locate/jocn
Journal of Clinical Neuroscience 14 (2007) 520–525
Clinical study
Complications related to positioning in posterior fossa craniectomy
G.P. Rath, P.K. Bithal *, A. Chaturvedi, H.H. Dash
Department of Neuroanaesthesiology, Neurosciences Centre, Room 709-A, All India Institute of Medical Sciences, New Delhi 110 029, India
Received 3 December 2005; accepted 21 February 2006
Abstract
To compare complications associated with surgical position, a retrospective study was conducted on 260 patients who underwent pos-terior fossa craniectomy. Data collected from the records included demographic profile, American Society of Anesthesiologists’ physicalstatus score, neurological status, cranial nerve involvement, associated medical illnesses, anaesthetic technique, patient position, haemo-dynamic changes, duration of surgery, venous air embolism (VAE), blood loss/transfusion, postoperative complications, duration of ICUstay, and postoperative neurological status. Statistical analysis was done using the Chi-square test and independent t-tests. The demo-graphic profile and preoperative associated medical illnesses of patients were comparable between groups. The incidence of end-tidal car-bon dioxide (EtCO2) detected VAE was more (p = 0.00) in the sitting position than the horizontal positions (15.2% vs. 1.4%). Blood loss/transfusion and the duration of surgery were significantly higher in the horizontal position (p < 0.05). Brainstem handling was the mostcommon cause of prolonged postoperative mechanical ventilation and was seen more in the sitting position. Lower cranial nerve functionswere preserved better in the sitting position (p < 0.05). Most postoperative complications (surgical or otherwise) were comparable betweenthe groups (p > 0.05). Most patients in both groups developed mild-to-moderate disability with independent lifestyle at the seventh post-operative day. To conclude, both sitting and horizontal positions can be used safely in posterior fossa surgeries.� 2006 Elsevier Ltd. All rights reserved.
Keywords: Posterior fossa craniectomy; Surgical positions; Complications
1. Introduction
Posterior fossa craniectomy can be performed either inthe sitting or horizontal position. The use of the sitting po-sition is controversial because of the significant potentialfor complications such as the venous air embolism(VAE), intraoperative haemodynamic instability, tensionpneumocephalus, lingual and laryngeal oedema, nerve inju-ries and quadriparesis.1–8 The specific advantages whichmade this position popular include improved surgical expo-sure and anatomical orientation, improved venous drain-age, haemostasis, gravitational drainage of thecerebrospinal fluid (CSF) and blood from the operativefield, improved access to the endotracheal tube, chest wall
0967-5868/$ - see front matter � 2006 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jocn.2006.02.010
* Corresponding author. Tel.: +91 11 26588700 4347; fax: +91 1126588663.
E-mail address: [email protected] (P.K. Bithal).
and upper extremities by the anaesthesiologist, free dia-phragmatic movements, and the ability to observe the facefor signs of surgical stimulation of cranial nerves.1–8 De-spite these advantages the use of the sitting position ap-pears to be diminishing because of its potential forserious complications and malpractice claims. The declinehas been observed worldwide. In India there is also pro-nounced reduction of use of the sitting position in variousneurosurgical centres (personal communication) for thereasons cited above. In our institution, the sitting positionis still used, although the frequency is reduced as comparedto previous years. It is used depending on the surgeon’spreference over other horizontal positions used for poster-ior fossa craniectomies. Presently at our centre, it is mainlyused for excision of brain stem gliomas and posterior thirdventricular tumours. This study was undertaken to assessthe perioperative complications in patients who underwentposterior fossa craniectomy in the sitting and horizontalpositions.
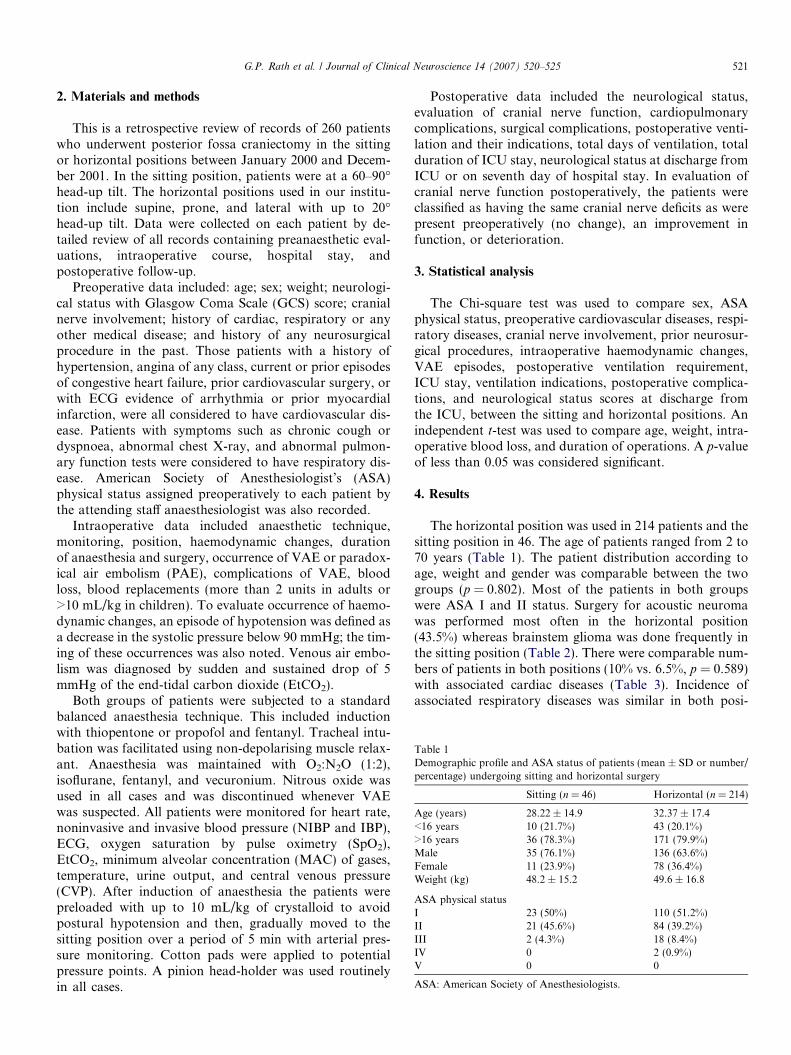
Table 1Demographic profile and ASA status of patients (mean ± SD or number/percentage) undergoing sitting and horizontal surgery
Sitting (n = 46) Horizontal (n = 214)
Age (years) 28.22 ± 14.9 32.37 ± 17.4<16 years 10 (21.7%) 43 (20.1%)>16 years 36 (78.3%) 171 (79.9%)Male 35 (76.1%) 136 (63.6%)Female 11 (23.9%) 78 (36.4%)Weight (kg) 48.2 ± 15.2 49.6 ± 16.8
ASA physical statusI 23 (50%) 110 (51.2%)II 21 (45.6%) 84 (39.2%)III 2 (4.3%) 18 (8.4%)IV 0 2 (0.9%)V 0 0
ASA: American Society of Anesthesiologists.
G.P. Rath et al. / Journal of Clinical Neuroscience 14 (2007) 520–525 521
2. Materials and methods
This is a retrospective review of records of 260 patientswho underwent posterior fossa craniectomy in the sittingor horizontal positions between January 2000 and Decem-ber 2001. In the sitting position, patients were at a 60–90�head-up tilt. The horizontal positions used in our institu-tion include supine, prone, and lateral with up to 20�head-up tilt. Data were collected on each patient by de-tailed review of all records containing preanaesthetic eval-uations, intraoperative course, hospital stay, andpostoperative follow-up.
Preoperative data included: age; sex; weight; neurologi-cal status with Glasgow Coma Scale (GCS) score; cranialnerve involvement; history of cardiac, respiratory or anyother medical disease; and history of any neurosurgicalprocedure in the past. Those patients with a history ofhypertension, angina of any class, current or prior episodesof congestive heart failure, prior cardiovascular surgery, orwith ECG evidence of arrhythmia or prior myocardialinfarction, were all considered to have cardiovascular dis-ease. Patients with symptoms such as chronic cough ordyspnoea, abnormal chest X-ray, and abnormal pulmon-ary function tests were considered to have respiratory dis-ease. American Society of Anesthesiologist’s (ASA)physical status assigned preoperatively to each patient bythe attending staff anaesthesiologist was also recorded.
Intraoperative data included anaesthetic technique,monitoring, position, haemodynamic changes, durationof anaesthesia and surgery, occurrence of VAE or paradox-ical air embolism (PAE), complications of VAE, bloodloss, blood replacements (more than 2 units in adults or>10 mL/kg in children). To evaluate occurrence of haemo-dynamic changes, an episode of hypotension was defined asa decrease in the systolic pressure below 90 mmHg; the tim-ing of these occurrences was also noted. Venous air embo-lism was diagnosed by sudden and sustained drop of 5mmHg of the end-tidal carbon dioxide (EtCO2).
Both groups of patients were subjected to a standardbalanced anaesthesia technique. This included inductionwith thiopentone or propofol and fentanyl. Tracheal intu-bation was facilitated using non-depolarising muscle relax-ant. Anaesthesia was maintained with O2:N2O (1:2),isoflurane, fentanyl, and vecuronium. Nitrous oxide wasused in all cases and was discontinued whenever VAEwas suspected. All patients were monitored for heart rate,noninvasive and invasive blood pressure (NIBP and IBP),ECG, oxygen saturation by pulse oximetry (SpO2),EtCO2, minimum alveolar concentration (MAC) of gases,temperature, urine output, and central venous pressure(CVP). After induction of anaesthesia the patients werepreloaded with up to 10 mL/kg of crystalloid to avoidpostural hypotension and then, gradually moved to thesitting position over a period of 5 min with arterial pres-sure monitoring. Cotton pads were applied to potentialpressure points. A pinion head-holder was used routinelyin all cases.
Postoperative data included the neurological status,evaluation of cranial nerve function, cardiopulmonarycomplications, surgical complications, postoperative venti-lation and their indications, total days of ventilation, totalduration of ICU stay, neurological status at discharge fromICU or on seventh day of hospital stay. In evaluation ofcranial nerve function postoperatively, the patients wereclassified as having the same cranial nerve deficits as werepresent preoperatively (no change), an improvement infunction, or deterioration.
3. Statistical analysis
The Chi-square test was used to compare sex, ASAphysical status, preoperative cardiovascular diseases, respi-ratory diseases, cranial nerve involvement, prior neurosur-gical procedures, intraoperative haemodynamic changes,VAE episodes, postoperative ventilation requirement,ICU stay, ventilation indications, postoperative complica-tions, and neurological status scores at discharge fromthe ICU, between the sitting and horizontal positions. Anindependent t-test was used to compare age, weight, intra-operative blood loss, and duration of operations. A p-valueof less than 0.05 was considered significant.
4. Results
The horizontal position was used in 214 patients and thesitting position in 46. The age of patients ranged from 2 to70 years (Table 1). The patient distribution according toage, weight and gender was comparable between the twogroups (p = 0.802). Most of the patients in both groupswere ASA I and II status. Surgery for acoustic neuromawas performed most often in the horizontal position(43.5%) whereas brainstem glioma was done frequently inthe sitting position (Table 2). There were comparable num-bers of patients in both positions (10% vs. 6.5%, p = 0.589)with associated cardiac diseases (Table 3). Incidence ofassociated respiratory diseases was similar in both posi-
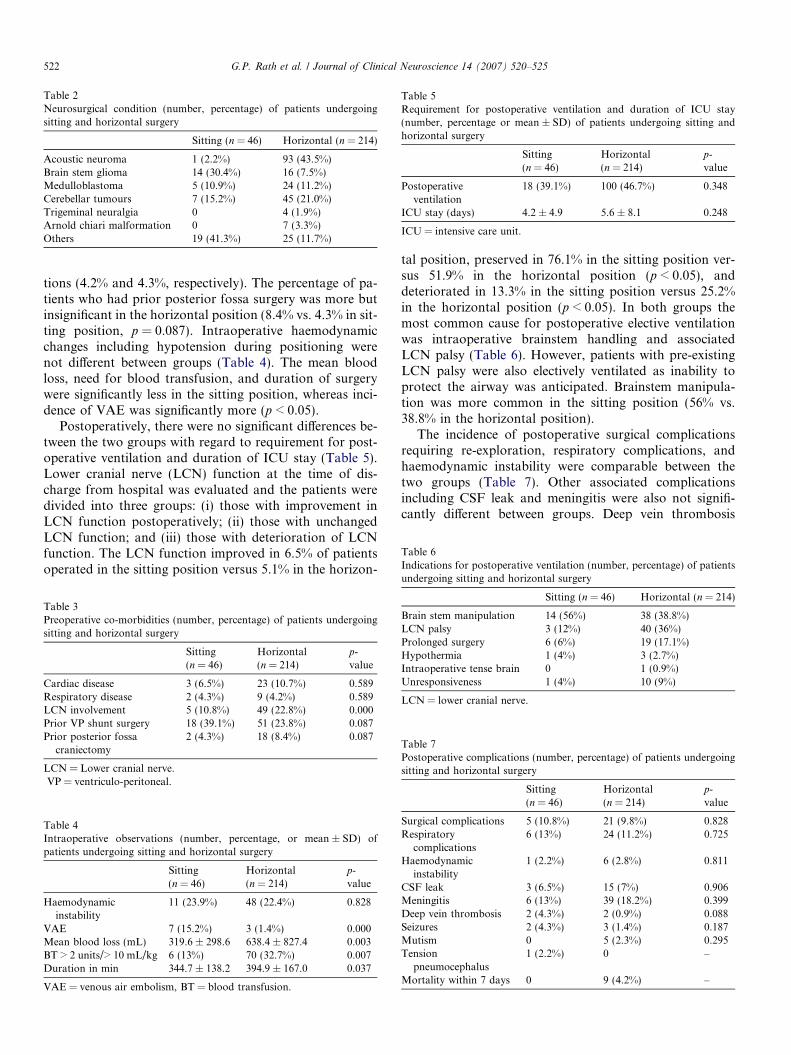
Table 2Neurosurgical condition (number, percentage) of patients undergoingsitting and horizontal surgery
Sitting (n = 46) Horizontal (n = 214)
Acoustic neuroma 1 (2.2%) 93 (43.5%)Brain stem glioma 14 (30.4%) 16 (7.5%)Medulloblastoma 5 (10.9%) 24 (11.2%)Cerebellar tumours 7 (15.2%) 45 (21.0%)Trigeminal neuralgia 0 4 (1.9%)Arnold chiari malformation 0 7 (3.3%)Others 19 (41.3%) 25 (11.7%)
Table 5Requirement for postoperative ventilation and duration of ICU stay(number, percentage or mean ± SD) of patients undergoing sitting andhorizontal surgery
Sitting(n = 46)
Horizontal(n = 214)
p-value
Postoperativeventilation
18 (39.1%) 100 (46.7%) 0.348
ICU stay (days) 4.2 ± 4.9 5.6 ± 8.1 0.248
ICU = intensive care unit.
Table 6Indications for postoperative ventilation (number, percentage) of patients
522 G.P. Rath et al. / Journal of Clinical Neuroscience 14 (2007) 520–525
tions (4.2% and 4.3%, respectively). The percentage of pa-tients who had prior posterior fossa surgery was more butinsignificant in the horizontal position (8.4% vs. 4.3% in sit-ting position, p = 0.087). Intraoperative haemodynamicchanges including hypotension during positioning werenot different between groups (Table 4). The mean bloodloss, need for blood transfusion, and duration of surgerywere significantly less in the sitting position, whereas inci-dence of VAE was significantly more (p < 0.05).
Postoperatively, there were no significant differences be-tween the two groups with regard to requirement for post-operative ventilation and duration of ICU stay (Table 5).Lower cranial nerve (LCN) function at the time of dis-charge from hospital was evaluated and the patients weredivided into three groups: (i) those with improvement inLCN function postoperatively; (ii) those with unchangedLCN function; and (iii) those with deterioration of LCNfunction. The LCN function improved in 6.5% of patientsoperated in the sitting position versus 5.1% in the horizon-
Table 3Preoperative co-morbidities (number, percentage) of patients undergoingsitting and horizontal surgery
Sitting(n = 46)
Horizontal(n = 214)
p-value
Cardiac disease 3 (6.5%) 23 (10.7%) 0.589Respiratory disease 2 (4.3%) 9 (4.2%) 0.589LCN involvement 5 (10.8%) 49 (22.8%) 0.000Prior VP shunt surgery 18 (39.1%) 51 (23.8%) 0.087Prior posterior fossa
craniectomy2 (4.3%) 18 (8.4%) 0.087
LCN = Lower cranial nerve.VP = ventriculo-peritoneal.
Table 4Intraoperative observations (number, percentage, or mean ± SD) ofpatients undergoing sitting and horizontal surgery
Sitting(n = 46)
Horizontal(n = 214)
p-value
Haemodynamicinstability
11 (23.9%) 48 (22.4%) 0.828
VAE 7 (15.2%) 3 (1.4%) 0.000Mean blood loss (mL) 319.6 ± 298.6 638.4 ± 827.4 0.003BT > 2 units/> 10 mL/kg 6 (13%) 70 (32.7%) 0.007Duration in min 344.7 ± 138.2 394.9 ± 167.0 0.037
VAE = venous air embolism, BT = blood transfusion.
tal position, preserved in 76.1% in the sitting position ver-sus 51.9% in the horizontal position (p < 0.05), anddeteriorated in 13.3% in the sitting position versus 25.2%in the horizontal position (p < 0.05). In both groups themost common cause for postoperative elective ventilationwas intraoperative brainstem handling and associatedLCN palsy (Table 6). However, patients with pre-existingLCN palsy were also electively ventilated as inability toprotect the airway was anticipated. Brainstem manipula-tion was more common in the sitting position (56% vs.38.8% in the horizontal position).
The incidence of postoperative surgical complicationsrequiring re-exploration, respiratory complications, andhaemodynamic instability were comparable between thetwo groups (Table 7). Other associated complicationsincluding CSF leak and meningitis were also not signifi-cantly different between groups. Deep vein thrombosis
Table 7Postoperative complications (number, percentage) of patients undergoingsitting and horizontal surgery
Sitting(n = 46)
Horizontal(n = 214)
p-value
Surgical complications 5 (10.8%) 21 (9.8%) 0.828Respiratory
complications6 (13%) 24 (11.2%) 0.725
Haemodynamicinstability
1 (2.2%) 6 (2.8%) 0.811
CSF leak 3 (6.5%) 15 (7%) 0.906Meningitis 6 (13%) 39 (18.2%) 0.399Deep vein thrombosis 2 (4.3%) 2 (0.9%) 0.088Seizures 2 (4.3%) 3 (1.4%) 0.187Mutism 0 5 (2.3%) 0.295Tension
pneumocephalus1 (2.2%) 0 –
Mortality within 7 days 0 9 (4.2%) –
undergoing sitting and horizontal surgery
Sitting (n = 46) Horizontal (n = 214)
Brain stem manipulation 14 (56%) 38 (38.8%)LCN palsy 3 (12%) 40 (36%)Prolonged surgery 6 (6%) 19 (17.1%)Hypothermia 1 (4%) 3 (2.7%)Intraoperative tense brain 0 1 (0.9%)Unresponsiveness 1 (4%) 10 (9%)
LCN = lower cranial nerve.

Table 8Status at discharge from the intensive care unit (number, percentage) ofpatients undergoing sitting and horizontal surgery
Outcome Sitting(n = 46)
Horizontal(n = 214)
1. Neurologically normal or with milddisability
35 (74.8%) 160 (76.1%)
2. Moderately disabled, butindependent
7 (15.2%) 31 (14.5%)
3. Severely disabled and dependent 2 (4.3%) 11 (5.1%)4. Vegetative 2 (4.3%) 3 (1.4%)5. Dead 0 9 (4.2%)
G.P. Rath et al. / Journal of Clinical Neuroscience 14 (2007) 520–525 523
(DVT) was seen more in patients operated in the sitting po-sition (4.3% vs. 0.9% in the horizontal position, p = 0.088).Postoperative seizures were similar in both groups (4.3%vs. 1.4%). Postoperative mutism was observed in five cases(2.3%), all operated for medulloblastomas in the horizontalposition. One patient with tension pneumocephalus wasseen after surgery in the sitting position (2.2%). The inci-dence of acute mortality within 7 days was 4.2% (9 pa-tients), all operated in the horizontal position.
Ninety percent of patients operated in the sitting posi-tion and 90.6% patients operated in the horizontal positionwere discharged with mild to moderate disability with anindependent life style, whereas, 8.6% of sitting patientsand 6.5% of horizontal patients became dependent eitherdue to severe disability or were in a vegetative state(p = 0.679) (Table 8). Mortality was 4.2%, all in the hori-zontal position group.
5. Discussion
Controversy surrounds the use of the sitting position inneurosurgery. It was often used for patients undergoingposterior fossa surgery in the past but has become less fa-voured because of the potential for complications. Of allthese, the main concern is VAE and its sequelae. However,the sitting position is still practiced in some centres, thoughinfrequently.1–3 Alternative positions for surgical access tothe posterior fossa include the prone, lateral and park-bench positions (horizontal positions). Several studies havebeen published examining the sitting position.4–6 However,only a few of these studies compared sitting to alternativehorizontal positions.7,8 Therefore, to make recommenda-tions, it is appropriate to compare the various positions.This series of 260 patients who underwent posterior fossacraniectomy performed over a period of 2 years providesan opportunity to compare patients operated in the sittingand horizontal positions.
Venous air embolism is a potentially fatal complicationof neurosurgical procedures performed in the sitting posi-tion. Early detection and prompt management by continu-ous monitoring is vital to reduce morbidity and mortality.The incidence of VAE varies widely depending on methodof detection. These include trans-oesophageal echocardiog-raphy (TEE); precordial Doppler ultrasound; end-tidal
nitrogen (EtN2); EtCO2; transcutaneous O2; right heartcatheter; and oesophageal stethoscope, in decreasing orderof sensitivity.9 In the present study, EtCO2 monitoring de-tected VAE in 15.2% of cases in the sitting position. This iscomparable to reports by other authors.4,5,10–12 However,it is much less than reported by Black et al. (45%),Michenfelder et al. (32%), Voorhies et al. (50%), andPapadopoulos et al. (76%).7,13–15 However, in all thesestudies, precordial Doppler ultrasound and TEE were usedfor detection of VAE, which are highly sensitive; whereasthe mainstay of monitoring in our study was EtCO2. Thecomparable incidence of VAE found in the studies by Mu-ley (17.2%) and Bithal (22%) are due to monitored EtCO2
to detect VAE.10,11 Nevertheless, there are reports support-ing capnography as a satisfactory method for the detectionof VAE in these clinical situations.16 Though horizontalpositioning in the current study did not eliminate VAE(1.4%), it was significantly less than in the sitting position(p = 0.00). However, the incidence of VAE in this studyis much less when compared to Black et al.7 and Albinet al.4 who reported incidences of 11% and 12%, respec-tively, in patients undergoing posterior fossa craniotomyin the horizontal position, using precordial Doppler ultra-sound.4,7 In the current study, the low incidence of VAEwas probably due to use of less sensitive monitors.
The sitting position may reduce blood loss by facilitat-ing drainage of venous blood away from the operative site.9
In this study, the mean blood loss and blood transfusionwere significantly less in the sitting position (Table 4). Thisis comparable to the study by Black et al. where bloodtransfusion of more than 2 units was significantly morecommon in the horizontal position. In the current studytoo, it was found that more than 2 units blood transfusionwas required in a significant number of cases in the hori-zontal position (p = 0.007).
The usual causes of intraoperative haemodynamic insta-bility during posterior fossa surgery are anaesthesia induc-tion, positioning, sudden severe bleeding, VAE, and brainstem or cranial nerve handling. These changes manifest inthe form of hypotension or hypertension, and bradycardiaor tachycardia. The incidence of haemodynamic instabilitywas comparable (p = 0.828) in both the groups with anoverall incidence of 22.7%.
It was found that significantly less time was taken forsurgery in the sitting position as compared to that in thehorizontal position (p = 0.037). Better anatomical orienta-tion and improved visualization of the surgical field due togravitational drainage of CSF and venous blood may ac-count for this. However, these findings are in variance withthe study by Black et al. where they found comparable timewas required in the two positions.7 The possible reasons forthis difference may be the surgeon’s experience or tumoursize, and location.
Postoperative mechanical ventilation was required in acomparable number of patients in both groups (Table 7).The main indications for ventilation were brainstem han-dling, LCN palsy with absence of gag and cough reflex,

524 G.P. Rath et al. / Journal of Clinical Neuroscience 14 (2007) 520–525
prolonged surgery (> 8 h), hypothermia (core temperature< 34 �C), intraoperative tense brain and unresponsive pa-tients. Brainstem handling was the most common causeresponsible for 56% of patients requiring postoperativeventilation in the sitting and 38.8% in the horizontal posi-tions (p < 0.05).
Cranial nerve function was more likely to be preservedin patients operated in the sitting position (76.1% vs.51.9% in horizontal, p < 0.05), whereas deterioration wasmore common in patients operated in the horizontal posi-tion (25.2% vs. 13.3% in sitting, p < 0.05). However,improvement of postoperative cranial nerve function wascomparable in both groups (6.5% in sitting vs. 5.1% in hor-izontal). The deterioration of cranial nerve function in thehorizontal position may be due to inadequate surgicalexposure in this position. Black et al. in contrast, reportedsignificant improvement of cranial nerve function in pa-tients within the horizontal group (20% vs. 12%).7 How-ever, 26% of patients in the horizontal group, in thatstudy, underwent microvascular decompression for ticdoloureux, which requires little tissue dissection. In theirstudy, preservation of nerve function was found to be sig-nificantly higher in the sitting position, which is compara-ble to our study. Deterioration of cranial nerve functionin our study is comparable to that reported by Black et al.
Prolonged surgery (> 8 h) was the main cause of postop-erative ventilation in 17.1% of patients in the horizontalposition as compared to 6% of patients in the sitting posi-tion. This is probably because of improved surgicalexposure.
Postoperative tension pneumocephalus is a potentiallyfatal neurological complication often associated with sur-gery in the sitting position.17,18 The symptoms may occur2–4 h after surgery with delayed recovery, severe restless-ness, deterioration of conciousness and seizures.17 In thisstudy symptomatic pneumocephalus occurred only in onepatient in the sitting position (2.2%). This is comparableto the studies by Black et al.7 and Bithal et al.19 This inci-dence is much less as compared to the reports of Dashet al.17 despite the presence of predisposing factors such asprior insertion of VP shunt (39.1%), mannitol administra-tion and continuation of N2O till the end of surgery in thesitting position. No patient in our study operated in the hor-izontal position deteriorated because of tension pneumo-cephalus, though there are rare case reports of it.20–22
Seizures after supratentorial surgery are common,23 butthey are rare after posterior fossa surgery, as the cortex isnot involved. In the present study, the incidence of seizuresin the immediate postoperative period was relatively higherin the sitting position (4.3% vs. 1.4%) though statisticallynot significant (p = 0.187). Black et al. also, reported acomparable incidences of postoperative seizures betweenboth groups with higher preponderance (2%) in the sittingposition.7 A higher incidence of seizures (5.9%) in the sit-ting position has also been reported by Suri et al.24 Thus,the sitting position may predispose to early postoperativeseizures after posterior fossa surgery. The overall incidence
of seizures in our analysis was 1.9%, which is comparableto the incidence (1.8%) reported Lee et al.25
The incidence of postoperative DVT has been reportedto be 24–50% in patients with brain tumours and it isnow standard that all patients should wear thromboembo-lic deterrent (TED) stockings perioperatively as a mechan-ical prophylaxis.26,27 There is also significant support in theliterature for the use of low molecular weight heparin peri-operatively to provide better prophylaxis.27 No prophylac-tic measure was followed routinely in the current study andDVT was observed in two patients (4.3%) in the sitting po-sition and two patients (0.9%) in the horizontal position(p = 0.088). The overall incidence of DVT in the currentstudy was 1.5%, much less than that reported by Kumaret al. (4.7%) following neurosurgical procedures.28
CSF leak following posterior fossa craniectomy may oc-cur at the suture line due to failure of dural closure or infec-tion; this leads to wound dehiscence. It may present as CSFotorrhoea after surgery for acoustic neuromas due to com-munication between the CSF spaces with the middle earcavity. The incidence of CSF leak varies from 4–27%.29
In the current study, the overall incidence of CSF leakwas 6.9%. This is comparable to the incidence (7.1%) re-ported by Santamarta et al.30 in an analysis of CSF-relatedcomplications, following posterior fossa surgery.
In our analysis, the overall incidence of meningitis is17.3%. The cause of meningitis in all cases was hospital-ac-quired bacterial infection. There was no aseptic meningitis,which is commonly associated with posterior fossa surgeryin children.31 The high incidence of meningitis in this studymay be due to CSF leak which doubles the incidence ofpostoperative meningitis.32
Gnanalingham et al. found that craniectomy was associ-ated with more postoperative CSF leaks.33 They also foundthat CSF leak is less likely if the bone flap is replaced. Thismay be the cause of the high incidence of bacterial menin-gitis in our study, because all our patients underwentcraniectomy.
Transient mutism is a recognized complication of pos-terior fossa surgery, particularly in children.34,35 It is asso-ciated with surgery for midline posterior fossa lesionsincluding medulloblastoma and other cerebellar tumours.It has been postulated that interruption of the dentatothal-amocortical pathway, which connects the dentate nucleusof the cerebellum to the supplementary motor area viathe ventrolateral nucleus of thalamus, is important in thedevelopment of mutism, especially if the disconnection isbilateral. In the present study, postoperative transient mut-ism occurred in 5/53 paediatric patients (9.4%), with anoverall incidence of 1.9%. All the patients were operatedfor medulloblastoma, which is similar to the reports inthe literature.35
6. Conclusion
To conclude, no position can be considered superior tothe other in posterior fossa surgery as each has its own

G.P. Rath et al. / Journal of Clinical Neuroscience 14 (2007) 520–525 525
advantages and risks. Consideration of the advantages anddisadvantages of both positions is required to select the po-sition for a specific patient, keeping in mind the abilities ofclinicians providing the care. However, our analysis sug-gests that both sitting and horizontal positions can be usedsafely in a wide variety of posterior fossa surgeries.
References
1. Drummond JC, Patel PM. Neurosurgical anesthesia. In: Miller RD,editor. Anesthesia. 5th ed. Philadelphia: Churchill Livingstone; 2000.p. 1895–933.
2. Elton RJ, Howell SC. The sitting position in neurosurgical anaesthe-sia: a survey of British practice in 1991. Br J Anaesth 1994;73:257–8.
3. Kida H, Nishikawa N, Matsunami K, et al. Sitting position in theneurosurgery: the result of a questionnaire sent to neurosurgeons ofmedical colleges. Masui 2000;49:566–9.
4. Albin MS, Babinski M, Maroon JC, et al. Anesthetic management ofposterior fossa surgery in the sitting position. Acta Anaesthesiol Scand
1976;20:117–28.5. Matjasko J, Petrozza P, Cohen M, et al. Anesthesia and surgery in
seated position: Analysis of 554 cases. Neurosurgery 1985;17:695–702.6. Standefer M, Bay JW, Trusso R. The sitting position in neurosurgery:
A retrospective analysis of 488 cases. Neurosurgery 1984;14:649–87.7. Black S, Ockert DB, Oliver WC, et al. Outcome following posterior
fossa craniectomy in patients in the sitting or horizontal positions.Anesthesiology 1988;69:49–56.
8. Duke DA, Lynch JJ, Harner SG, et al. Venous air embolism in sittingand supine patients undergoing vestibular schwannoma resection.Neurosurgery 1998;42:1282–6.
9. Black S, Cucchiara RF. Tumor surgery. In: Cucchiara RF, Black S,Michenfelder JD, editors. Clinical Neuroanaesthesia. 2nd ed. NewYork: Churchill-Livingstone; 1998. p. 340–65.
10. Muley SS, Saini SS, Dash HH, et al. End tidal carbon dioxidemonitoring for detection of venous air embolism. Indian J Med Res
[B] 1990;92:362–6.11. Bithal P, Dash HH, Vishnoi N, et al. Venous air embolism: Does the
site of embolism influence the hemodynamic changes? Neurol India
2003;51:370–2.12. Bithal PK, Pandia MP, Dash HH, et al. Comparative incidence of
venous air embolism and associated hypotension in adults andchildren operated for neurosurgery in the sitting position. Eur J
Anaesthesiol 2004;21:517–22.13. Michenfelder JD, Terry HR, Daw EF, et al. Air embolism during
neurosurgery: A new method of treatment. Anesth Analg
1966;45:390–5.14. Voorhies RM, Fraser RAR, Van Poznak A. Prevention of air
embolism in positive end expiratory pressure. Neurosurgery
1983;12:503–6.15. Popadopoulos G, Kulhy P, Brock M, et al. Venous and paradoxical
air embolism in the sitting position. A prospective study. Acta
Neurochir 1994;126:140–3.
16. Mammato T, Hayashi Y, Ohnishi Y, et al. Incidence of venous andparadoxical air embolism in neurosurgical patients in the sittingposition: Detection by transesophageal echocardiography. Acta Ana-
esthesiol Scand 1998;42:643–7.17. Dash HH, Bithal PK, Muley S, et al. Tension pneumocephalus
following posterior fossa surgery in sitting position. J Anaesth Clin
Pharmacol 1990;6:207–12.18. Kitahata LM, Katz JD. Tension pneumocephalus after posterior
fossa craniotomy: a complication of sitting position. Anesthesiology
1976;44:448–50.19. Bithal P, Pawar DK, Dash HH, et al. Anaesthetic management in
posterior fossa surgery- An experience of 203 cases. Ind J Anaesth
1991;39:90–7.20. Suri A, Mahapatra AK, Singh VP. Posterior fossa tension pneumo-
cephalus. Childs Nerv Syst 2000;16:196–9.21. Satapathy GC, Dash HH. Tension pneumocephalus after neurosur-
gery in supine position. Br J Anaesth 2000;84:115–7.22. Prabhakar H, Bithal PK, Garg A. Tension pneumocephalus after
craniotomy in supine position. J Neurosurg Anesthesiol
2003;15:278–81.23. De Giorgio CM, Robinowicz AL. Seizures. In: Apuzzo MLJ, editor.
Brain Surgery: Complication Avoidance and Management, Vol. 1. NewYork: Churchill Livingstone; 1993. p. 155–62.
24. Suri A, Mahapatra AK, Bithal P. Seizures following posterior fossasurgery. Br J Neurosurg 1998;12:41–4.
25. Lee S, Lui T, Chang C, et al. Early postoperative seizures afterposterior fossa surgery. J Neurosurg 1990;73:541–4.
26. Hamilton MG, Hull RD, Pineo GF. Venous thromboembolism inneurosurgery and neurology patients: a review. Neurosurgery
1994;34:280–96.27. Powers SK, Edwards MS. Prophylaxis of thromboembolism in
neurosurgical patients: a review. Neurosurgery 1982;10:509–13.28. Kumar N, Tang KK, Thomas J, et al. Is postoperative deep vein
thrombosis a problem in neurosurgical patients with brain tumors inSingapore? Singapore Med J 2002;43:345–9.
29. Nautik SL, Korol HW. Cerebrospinal fluid leak after acousticneuroma sugery. Surg Neurol 1995;43:553–7.
30. Santamarta D, Blazquez JA, Maillo A, et al. Analysis of cerebrospi-nal fluid related complications (hydrocephalus, fistula, pseudomen-ingocele and infection) following surgery for posterior fossa tumors.Neurochirurgia (Astur) 2003;14:117–26.
31. Carmel PW, Fraser RA, Stein BM. Aseptic meningitis followingposterior fossa surgery in children. J Neurosurg 1974;41:44–8.
32. Buckwold FJ, Hand R, Hansebout RR. Hospital acquired bacterialmeningitis in neurosurgical patients. J Neurosurg 1977;46:494–500.
33. Gnanalingham KK, Lafunte J, Thompson D. Surgical procedures forposterior fossa tumors in children: does craniotomy lead to fewercomplications than craniectomy? J Neurosurg 2002;97:821–6.
34. Jones S, Kirllos RW, Van Hille PT. Cerebellar mutism followingposterior fossa tumor surgery. Br J Neurosurg 1996;10:221–4.
35. Gelabert-Gonzalez M, Fernandez-Villa J. Mutism after posteriorfossa surgery. Review of literature. Clin Neurol Neurosurg
2001;103:111–4.
Related Documents











