Complications of diabetes mellitus Ceri Jones Cwm Taf University LHB 2014 Ceri Jones Cwm Taf University LHB 2014

Complications of diabetes mellitus Ceri Jones Cwm Taf University LHB 2014.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Complications of diabetes mellitus
Ceri Jones Cwm Taf University LHB 2014Ceri Jones Cwm Taf University LHB 2014

Complications of diabetes mellitus
Chronic complications: Microvascular
NeuropathiesNephropathiesRetinopathies
Macrovascular complications Myocardial infarctions
Cerebrovascular accidents
Peripheral vascular disease
Aim & Objectives Understand the micro & macrovascular complications
of diabetes
Understand the factors, interventions and therapies which can prevent or delay the onset of complications
Be able to advise people with diabetes on self-care strategies to prevent and manage macrovascular complications

Facing Facts: The burden of diabetes complications
Diabetes is a progressive disease; many present with complications on diagnosis
Complications can have devastating effects on individuals lives:
human costs shortened life expectancy
Healthcare costs for diabetes, account for 9% of total healthcare expenditure

NSF for Diabetes Standard 10
Regular surveillance for the long term complications of diabetes
Standard 11
Agreed protocols and systems of care
Standard 12
All people with diabetes requiring multi agency support will receive integrated health and social care
Why do Problems Occur?Long term exposure to hyperglycaemia leads to:
Vessel closure (full or partial) – supply of oxygen and nutrients are decreased
Vessel permeability – damaged vessels dilate and leak unwanted substances
Diabetes risk factors for complications: Hyperglycaemia
Hypertension
Dyslipidaemia
Smoking
Macrovascular Complications - Risk Factors Type 2 diabetes is a strong risk factor for CV disease in both
men and women
Risk of atherosclerotic cardiovascular disease is 2-4 times higher for those with Type 2 diabetes compared to non diabetic population
CHD is the principle cause of death in people with diabetes
Normal protection afforded to pre-menopausal women is negated by diabetes
People with diabetes have the same risk as those without diabetes but who have had an MI

Acute Myocardial Infarction People with type 2 diabetes have the same risk of an
MI as people without diabetes who have already had an MI
Immediate and later mortality rates following MI are high in people with Type 2 diabetes
MIs may be silent in people with diabetes or symptoms may be atypical
Cerebrovascular Events No long term studies on stroke management to date
General consensus is to treat all vascular risk factors aggressively
ACEi
Statins
Aspirin
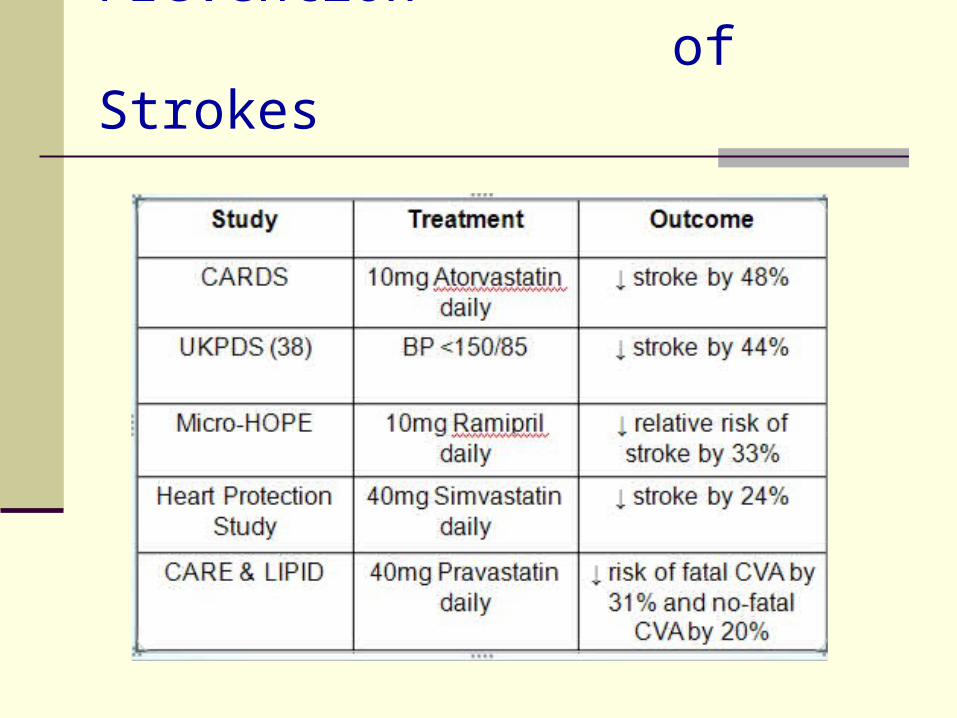
Evidence for Primary Prevention of Strokes

Peripheral Vascular Disease
Approx 20% of people with PVD will die within 2 yrs of symptoms
Generally PVD is asymptomatic until arterial stenosis occurs
Symptoms include: Intermittent claudication Rest pain Buttock pain
Management: Aspirin Vasodilating agents Reconstructive surgery Angioplasty Amputation & rehabilitation & foot care

Aspirin
For Secondary Prevention
People with cardiovascular disease 75 mg once daily
For Primary Prevention
British Hypertension Society recommends aspirin 75 mg once daily for those aged 50 and over, with Type 2 diabetes, with a blood pressure controlled to <150/90 mmHg (NICE suggest <145 systolic).
All people with a 10 year risk >15% to be prescribed aspirin - according to precautions and contra- indications in British National Formulary.
Microvascular Microvascular ComplicationsComplications
Nephropathy
Neuropathy
Retinopathy

Diabetic retinopathy
A silent complication with no initial symptoms
When symptoms occur, treatment is more complicated and often impossible
Screening for retinopathy is of the utmost importance

When to screen for retinopathy
Type 1 diabetes: within 5 years of diagnosis
Type 2 diabetes: at time of diagnosis
Thereafter, every 1 to 2 years, depending on the status of the retina
Diabetic eye disease
Blurred vision: common symptom of hyperglycaemia
Epidemiology: any retinopathy: 21-36% vision-threatening retinopathy:
6-13%
Risk factors
Poor glycaemic control Long duration Hypertension
Dyslipidemia Nephropathy Pregnancy

Intensive therapy
DCCT – type 1 diabetes: Primary prevention cohort:
reduced risk of developing retinopathy by 76%
Secondary intervention cohort: reduced risk of progression of retinopathy by 54%
DCCT 1993

Treatment
Blood pressure: reduces macular oedema
Blood glucose control: slows progression
Control lipids
Use of aspirin

Treatment
Laser therapy:Pan-retinal for proliferative
retinopathyFocal or grid for macular
oedema
Laser therapy
Side effects
Loss of peripheral vision, tunnel vision, night blindness
Colour blindness
Vision can get worse but “laser saves sight” in long term
Summary
100% of people with diabetes will develop some retinopathy
The higher the blood glucose level the greater the risk
Different grades of retinopathy Laser therapy saves sight Timely treatment is most effective Regular screening is a must

Diabetic nephropathy
About 20% to 30% of people with diabetes
In type 2 diabetes, a smaller fraction of these progress to CKD
People with type 2 diabetes – over half of those with diabetes starting on dialysis

Risk factors
Poor glycaemic control Hyperlipidaemia Hypertension Genetic predisposition Glomerular hyper-filtration during early
period Ethnicity Long disease duration Smoking
Type 1 diabetes
Decreasing incidence over past 35 years
Overall incidence
2.2% at 20 years duration
7.8% at 30 years duration
Finne 2005
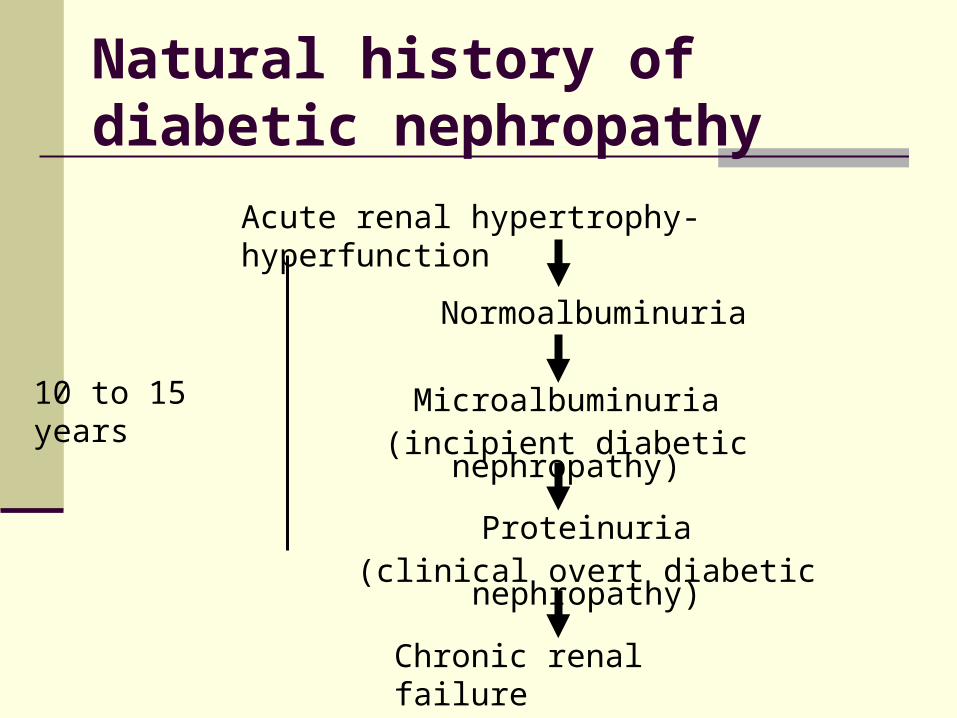
Microalbuminuria(incipient diabetic nephropathy)
Acute renal hypertrophy-hyperfunction
Normoalbuminuria
Proteinuria(clinical overt diabetic nephropathy)
Chronic renal failure
10 to 15 years
Natural history of diabetic nephropathy

Diabetic renal assessment Urinalysis for proteinuria Spot urine for microalbuminuria
morning and resting or preferably with albumin/creatinine ratio
(normal <2.5 mg/mmol in men and <3.5 mg/mmol in women)
Serum creatinine; preferably with adjustment of body size
Estimated glomerular filtration rate Repeat the tests at about yearly intervals if
normal If GFR <60 ml/min test 3-6 monthly

Microalbuminuria
Type 1 diabetes indicates incipient nephropathy
Type 2 diabetes marker of increased cardiovascular morbidity
and mortality
Presence of microalbuminuria is an indication for screening of vascular disease and intensive intervention

Interventions: glycaemic control
Diabetes Control and Complications Trial (DCCT) occurrence of microalbuminuria by 40% occurrence of macroalbuminuria by 50%
United Kingdom Prospective Diabetes Study (UKPDS)
overall microvascular complication rate by 25%
Diabetic nephropathy
Treatment intensive treatment of blood
pressure
target <130/80 mmHg
reduce salt in diet
reduce alcohol
Sacks, 2001
Management of people with elevated creatinine
Caution should be taken when using the following:
metformin
non-steroidal anti-inflammatory drugs
glibenclamide
radiographic contrast
Management of people with elevated creatinine Insulin dosage may need adjustment
due to change in insulin half life and dialysis
Anaemia is common and may need treatment – measure haemoglobin every 6 months if eGFR is <60 ml/min/1.73 m2
Refer to nephrologist when eGFR <30 ml/min/1.73m2
Estimated Glomerular Filtration Rate (eGFR) May underestimate actual renal
function especially in women, the young and the obese
More accurate in lower ranges <60 ml/min
If eGFR is <60 ml/min, 30% risk of CVD
Most common cause of death in CKD is cardiac arrest (22%)
Summary
Diabetes is a common cause of CKD
Various grades of nephropathy
The higher the A1c the higher the risk
Control matters
Blood pressure

Diabetic foot disease –the high-risk foot
Peripheral vasculardisease
Peripheral neuropathy
Peripheral neuropathy andperipheral vascular disease
Some statistics
• Half of all limb amputations are caused by diabetes
• Risk is 40 times increased in diabetes
• 70% of people die five years following an amputation
• Foot problems account for 40% of healthcare resources in developing countries; 15% in developed countries
Some statistics• 85% of all amputations begin with an ulcer
• 49-85% of amputations can be prevented
Peripheral neuropathy – sensory motor
Most common form of neuropathy Affects approximately 50% after 15 years Affects long nerves (feet and legs) first
glove and stocking distribution
Bilateral Equal symptoms in both limbs

Diabetic peripheral neuropathy – risk factors
Poor glycaemic control
Long duration
Age
Height
Excessive alcohol

Nerve damage – neuropathy
Symptoms:burningpins and needlespain
No symptoms
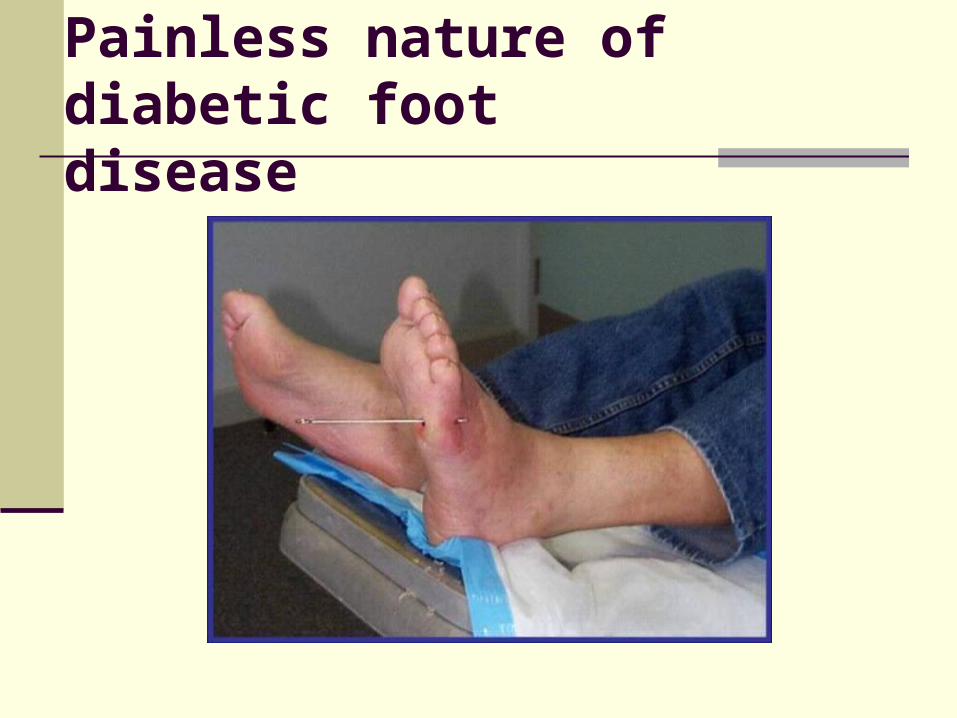
Painless nature of diabetic foot disease

Sensory nerve damage

Motor nerve damage

Autonomic nerve damage

Take off the shoes!Take off the shoes!
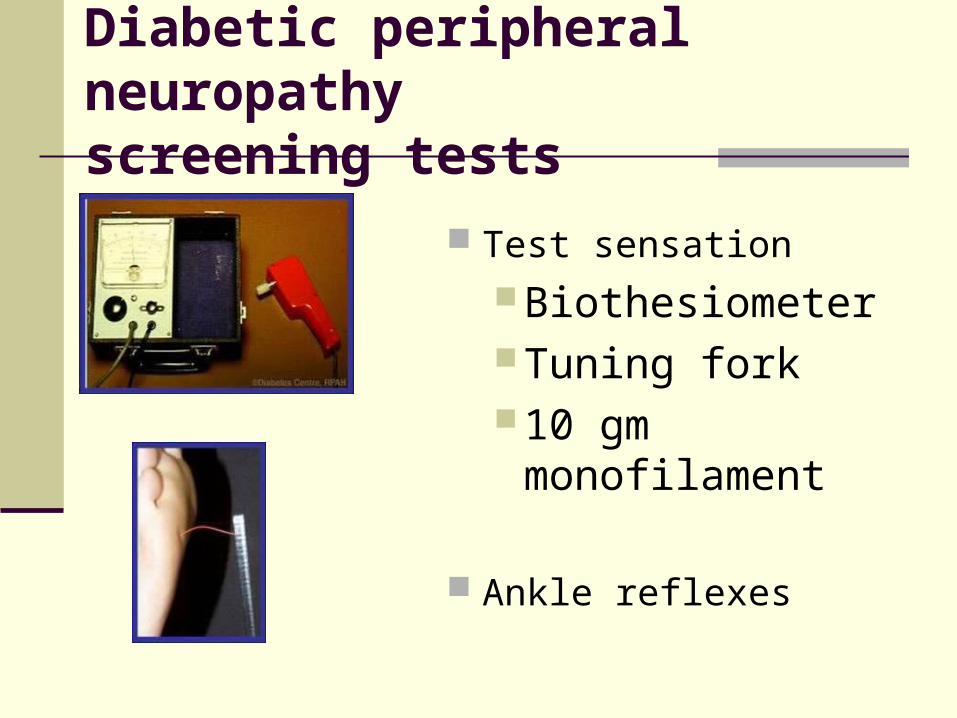
Diabetic peripheral neuropathyscreening tests
Test sensation BiothesiometerTuning fork10 gm
monofilament
Ankle reflexes

Assessment of high risk characteristics
Peripheral vascular disease
Symptoms Intermittent claudicationRest pain
No symptoms
InactivityNeuropathy
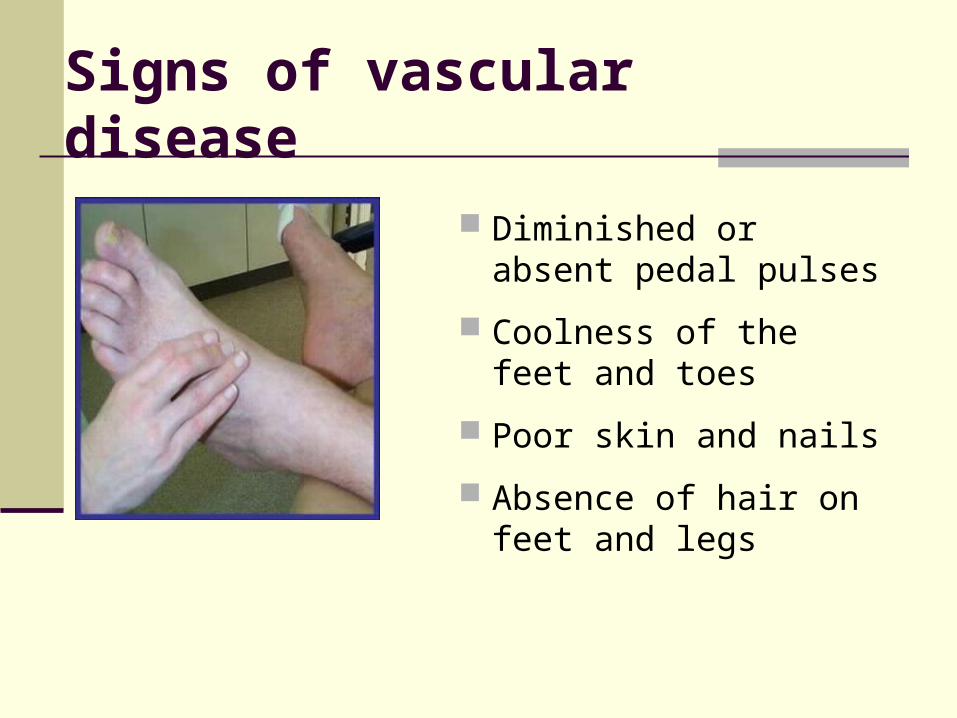
Signs of vascular disease
Diminished or absent pedal pulses
Coolness of the feet and toes
Poor skin and nails
Absence of hair on feet and legs

Vascular assessment
Palpation of foot pulses
Dorsalis pedis (10% absent due to anatomical reasons)
Tibialis posterior
Peripheral vascular diseasenon-invasive evaluation
Methods Doppler pressure studies (ABI) Duplex arterial imaging
Rationale Identify and confirm presence of
disease Predict healing of ulcers or determine
need for early surgical intervention
Peripheral vascular disease
Treatment
• Quit smoking
• Walk through pain
• Surgical intervention
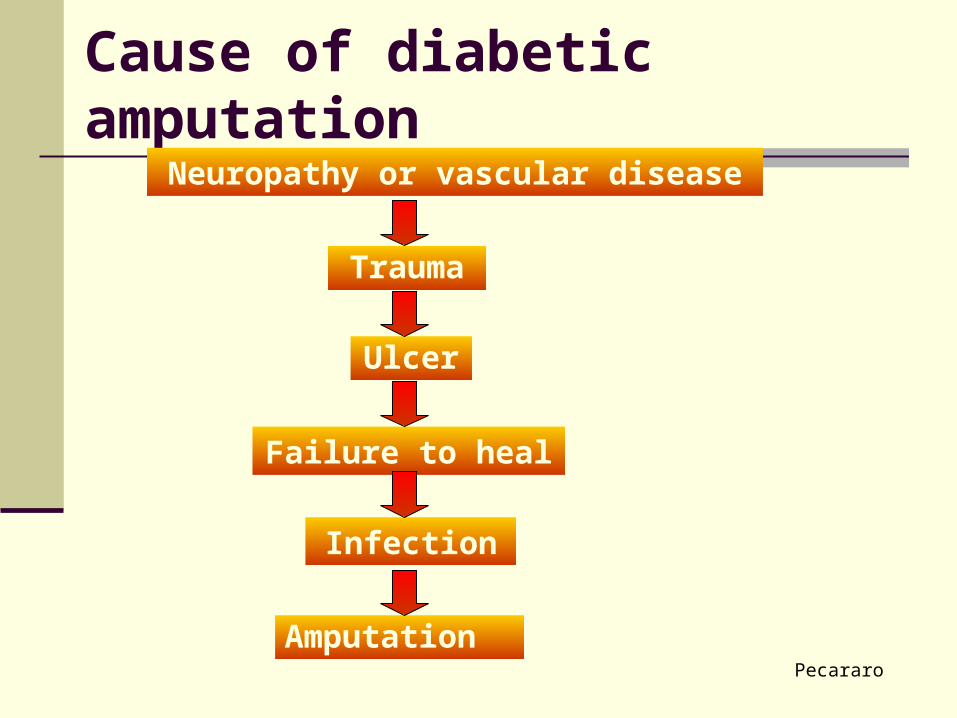
Cause of diabetic amputation
Pecararo
Trauma
Ulcer
Failure to heal
Infection
Amputation
Neuropathy or vascular disease

An amputation every 30 secondsdue to diabetes

Modifiable Risk FactorsHyperglycaemia
Hypertension
Dyslipidaemia
Smoking
Excess visceral adiposity
Lifestyle

Why Treat to Target?
Many people with Type 2 diabetes have both microvascular and
macrovascular complications (1)
UKPDS showed that treating to target levels helped reduce the
complications of Type 2 diabetes (2,3)
HbA1c and blood pressure are modifiable cardiovascular risk factors in
Type 2 diabetes (2,3)
Treating to target levels reduces complications and reduces the burden
of Type 2 diabetes (2,3)
Each 1% reduction in HbA1c for 10 years was associated with 37%
reduction in microvascular problems.1.UKPDS 6. Diabetes Research 1990;13:1–11
2. UKPDS 33. Lancet1998;352:837–835 .
3, UKPDS 38. BMJ 1998;317:703–713

UKPDSUKPDS
The risk of each of the macrovascular and microvascular complications in type 2 diabetes was strongly associated with hyperglycaemia, as measured by HbA1c.
Good glycaemic control reduces the risk of complications.
DCCTDCCT This landmark diabetes study established that good
control prevents and delays the progression of chronic complications in people with type 1 diabetes.
Retinopathy and nephropathy (urine albumin excretion) were reduced by 35-75% in the group with tight control.
In those with initial early retinopathy, risk of progression reduced by about 50%.
The tight control group experienced 3x more severe hypos than the control group.
Conclusion
Macrovascular complications of diabetes can have a profound and devastating affect on the quality of life and life expectancy of people with diabetes.
Many factors, interventions and therapies which can prevent or delay the onset of complications are available.
Ongoing and new research strive to reach more positive outcomes for people with diabetes.
As healthcare professionals our roles are to advise people with diabetes on self-care strategies to prevent and manage macrovascular complications.
Related Documents











