JOURNAL OF PEDIATRIC NURSING: NURSING CARE OF CHILDREN & FAMILIES Journal of Pediatric Nursing (ISSN 0882-5963) is published bimonthly by W.B. Saunders Company. Months of issue are February, April, June, August, October, and December. Corporate and Editorial Offices: The Curtis Center, Independence Square West, Philadelphia, PA 19106-3399. Accounting and Circulation Offices: 6277 Sea Harbor Dr, Orlando, FL 32887-4800. Second class postage paid at Orlando, FL 32862, and additional mailing offices. POSTMASTER: Send address changes to Journal of Pediatric Nursing (ISSN 0882-5963), W.B. Saunders Company, Periodicals Dept, 6277 Sea Harbor Dr, Orlando, FL 32887-4800. Editorial correspondence should be addressed to Cecily Lynn Betz, RN, PhD, UCLA Neuropsychiatric Institute, 300 UCLA Medical Plaza, Suitc 3310, Los Angeles, CA 90024-6967. Voice mail: (310) 825-8902; fax: (213) 344-1057. Business correspondence (subscriptions, change of address) should be addressed to the Publisher, W.B. Saunders Company, Periodicals Dept, 6277 Sea Harbor Dr, Orlando, FL 32887-4800. Change of address notices, including both the old and new addresses of the subscriber, should be sent at least one month in advance. Customer Service: 1-800-654-2452. Yearly subscription rates: United States and possessions: individual, $49.00; institution, $79.00; single issue, $19.00. All other countries: individual, $93.00; institution, $110.00; single issue, $19.00. For all areas outside the United States and possessions, there is no additional charge for surface delivery. For air mail delivery, add $24.00. Students: United States and possessions, and Canada: $28.00; all other countries: $93.00. To receive student rate, orders must be accompanied by name of affiliated institution, date of term, and the signature of program coordinator on institution letterhead. Orders will be billed at individual rate until proof of status is received. Subscriptions are accepted on a calendar year basis. Current prices are in effect for back volumes and back issues. Single issues, both current and back, exist in limited quantities and are offered for sale subject to availability. Back issues sold in conjunction with a subscription are on a prorated basis. Prices are subject to change without notice. Checks should be made payable to W.B. Saunders Company and sent to Journal of Pediatric Nursing, W.B. Saunders Company, Periodicals Dept, 6277 Sea Harbor Dr, Orlando, FL 32887-4800. Agents for the United Kingdom, Ireland, and Europe: Harcourt Brace & Company, Limited, 24-28 Oval Rd, London NW1 7DX, England. Agents for Australia and New Zealand: Harcourt Brace & Company Australia, Pty. Limited, 30-52 Smidmore St (Locked Bag 16), Marrickville, NSW 2204, Australia. Agents for Japan and Korea: Harcourt Brace & Company Japan, Inc., Ichibancho Central Bldg, 22-1 Ichibancho, Chiyoda-Ku, Tokyo 102, Japan. Copyright o 1995 by W.B. Saunders Company. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publisher. Printed in the United States of America. Correspondence regarding permission to reprint all or part of any article published in this journal should be addressed to Journal Permissions Dept, W.B. Saunders Company, Orlando, FL 32887. Telephone: 1-407-345-2500. The appearance of the code at the bottom of the first page of an article in this journal indicates the copyright owner's consent that copies of the article may be made for personal or internal use, or for the personal or internal use of specific clients. This consent is given on the condition, however, that the copier pay the stated per-copy fee through the Copyright Clearance Center, Inc. (222 Rosewood Dr, Danvers, MA 01923) for copying beyond that permitted by Sections 107 or 108 of the US Copyright Law. This consent does not extend to other kinds of copying, such as copying for general distribution, for advertising or promotional purposes, for creating new collective works, or for resale. Absence of the code indicates that the material may not be processed through the Copyright Clearance Center, Inc. Advertising representative: M.J. Mrvica Associates Inc., 155 S. White Horse Pike, Berlin, NJ 08009. Telephone: (609) 768-9360. Publication of an advertisement in the Journal ofpediatric Nursing does not imply endorsement of its claims by the Editor or Publisher of the journal. Every cffort has been made to check generic and trade names and to verify drug doses. The ultimate responsibility, however, lies with the prescribing physician. Please convey any errors to the Editor. W.B. Saunders Company Philadelphia, PA A Division of Harcourt Brace €9 Company

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

JOURNAL OF PEDIATRIC NURSING: NURSING CARE OF CHILDREN & FAMILIES
Journal of Pediatric Nursing (ISSN 0882-5963) is published bimonthly by W.B. Saunders Company. Months of issue are February, April, June, August, October, and December. Corporate and Editorial Offices: The Curtis Center, Independence Square West, Philadelphia, PA 19106-3399. Accounting and Circulation Offices: 6277 Sea Harbor Dr, Orlando, FL 32887-4800. Second class postage paid at Orlando, FL 32862, and additional mailing offices.
POSTMASTER: Send address changes to Journal of Pediatric Nursing (ISSN 0882-5963), W.B. Saunders Company, Periodicals Dept, 6277 Sea Harbor Dr, Orlando, FL 32887-4800.
Editorial correspondence should be addressed to Cecily Lynn Betz, RN, PhD, UCLA Neuropsychiatric Institute, 300 UCLA Medical Plaza, Suitc 3310, Los Angeles, CA 90024-6967. Voice mail: (310) 825-8902; fax: (213) 344-1057.
Business correspondence (subscriptions, change of address) should be addressed to the Publisher, W.B. Saunders Company, Periodicals Dept, 6277 Sea Harbor Dr, Orlando, FL 32887-4800.
Change of address notices, including both the old and new addresses of the subscriber, should be sent at least one month in advance.
Customer Service: 1-800-654-2452. Yearly subscription rates: United States and possessions: individual, $49.00; institution, $79.00; single
issue, $19.00. All other countries: individual, $93.00; institution, $110.00; single issue, $19.00. For all areas outside the United States and possessions, there is no additional charge for surface delivery. For air mail delivery, add $24.00. Students: United States and possessions, and Canada: $28.00; all other countries: $93.00. To receive student rate, orders must be accompanied by name of affiliated institution, date of term, and the signature of program coordinator on institution letterhead. Orders will be billed at individual rate until proof of status is received. Subscriptions are accepted on a calendar year basis. Current prices are in effect for back volumes and back issues. Single issues, both current and back, exist in limited quantities and are offered for sale subject to availability. Back issues sold in conjunction with a subscription are on a prorated basis. Prices are subject to change without notice. Checks should be made payable to W.B. Saunders Company and sent to Journal of Pediatric Nursing, W.B. Saunders Company, Periodicals Dept, 6277 Sea Harbor Dr, Orlando, FL 32887-4800.
Agents for the United Kingdom, Ireland, and Europe: Harcourt Brace & Company, Limited, 24-28 Oval Rd, London NW1 7DX, England. Agents for Australia and New Zealand: Harcourt Brace & Company Australia, Pty. Limited, 30-52 Smidmore St (Locked Bag 16), Marrickville, NSW 2204, Australia. Agents for Japan and Korea: Harcourt Brace & Company Japan, Inc., Ichibancho Central Bldg, 22-1 Ichibancho, Chiyoda-Ku, Tokyo 102, Japan.
Copyright o 1995 by W.B. Saunders Company. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publisher. Printed in the United States of America.
Correspondence regarding permission to reprint all or part of any article published in this journal should be addressed to Journal Permissions Dept, W.B. Saunders Company, Orlando, FL 32887. Telephone: 1-407-345-2500.
The appearance of the code at the bottom of the first page of an article in this journal indicates the copyright owner's consent that copies of the article may be made for personal or internal use, or for the personal or internal use of specific clients. This consent is given on the condition, however, that the copier pay the stated per-copy fee through the Copyright Clearance Center, Inc. (222 Rosewood Dr, Danvers, MA 01923) for copying beyond that permitted by Sections 107 or 108 of the US Copyright Law. This consent does not extend to other kinds of copying, such as copying for general distribution, for advertising or promotional purposes, for creating new collective works, or for resale. Absence of the code indicates that the material may not be processed through the Copyright Clearance Center, Inc.
Advertising representative: M.J. Mrvica Associates Inc., 155 S. White Horse Pike, Berlin, NJ 08009. Telephone: (609) 768-9360.
Publication of an advertisement in the Journal ofpediatric Nursing does not imply endorsement of its claims by the Editor or Publisher of the journal.
Every cffort has been made to check generic and trade names and to verify drug doses. The ultimate responsibility, however, lies with the prescribing physician. Please convey any errors to the Editor.
W.B. Saunders Company Philadelphia, PA
A Division of Harcourt Brace €9 Company

Compensatory Parenting: How Mothers Describe Parenting Their 3-Year-Old, Prematurely Born Children
Margaret Shandor Miles, PhD, RN, FAAN Diane Holditch-Davis, PhD, RN
Premature infants and their mothers experience difficulties in establishing their relationships. The effect of these early problems on later parenting is not known. This study explored whether mothers' recollections surrounding the birth and hospitalization of a preterm infant affected their perceptions and their parenting of these children at 3 years of age. Twenty-seven primary caregivers of 30 prematurely born children completed three questionnaires on their perceptions of their children and were interviewed about parenting experiences. The core concept identified in analysis was compensatory parenting, a parenting style in which mothers provided special experiences and avoided others in an attempt to compensate the children for their neonatal experiences. Compensatory parenting was influenced by the view of these prematurely born children as both special and normal and by salient prenatal, labor, and delivery experiences; memories of the neonatal intensive care unit experience; the sequelae of emotional responses to these experiences; and subsequent health problems after discharge. Prospective research is needed to further study compensatory parenting and to develop interventions. Copyri~ht O 1995 by W.B. Saunders Company
T HE BIRTH and hospitalization of preterm infants is very stressful for mothers (Af-
fleck, Tennen, Rowe, & Higgins, 1990; Easter- brooks, 1988). They experience grief over the birth of infants who may not survive and distress over the appearance of the immature, small infants. In addition, the expected parenting relationship may be seriously altered because of the infants' immature responses, critical illness, and prolonged hospitalization.
Little is known about how these complicated experiences during the period of transition to parenting affect parenting of these children, particularly during their preschool years. This article explores whether mothers' recollections surrounding the birth and hospitalization of their preterm infants affected their perceptions of their children at 3 years of age and their parenting of the children.
REVIEW OF THE LITERATURE
Numerous studies have found that parents of preterm infants experience distress during the initial period while their infants are hospitalized in a neonatal intensive care unit (NICU) for care and treatment of various complications of prematurity. Sources of stress include the size and appearance of the infants surrounded by equipment and experiencing various invasive
treatments; changes in the expected parenting roles with newborns, including long periods of separation; and adjusting to the hospital and NICU environmetns (AfReck, Tennen, Rowe, & Higgins, 1990; Gennaro, 1988; Miles, 1989; Miles, Funk, & Kasper, 1991; Pederson, Bento, Chance, Evans, & Fox, 1987).
Mothers often are relieved and happy when the time comes for discharge from the hospital, but they also experience anxiety and depression when they assume total responsibility for their preterm infants (Bidder, Crowe, & Gray, 1974; Brooten et al., 1988; Pederson et al., 1987). Mothers of preterm infants have more concerns about their infants, especially in the areas of attachment, health, and growth, than mothers
From the Department of Health of Women and Children, School of Nursing, University of North Carolina at Chapel Hill, Chapel Hill, NC.
Supported by Grant No. I R29 NR01894from the National Center for Nursing Research, National Institutes of Health, to D. H.-D., and a 1989 University of North Carolina at Chapel Hill University Research Council Grant to M. S. M. and D. H.-D.
Address reprint requests to Diane Holditch-Davis, PhD, RN, School of Nursing, University ofNorth Carolina at Chapel Hill, CB No. 7460 Canington Hall 214H, Chapel Hill, NC 27599- 7460.
Copvnght 0 1995 by W B . Saunders Company 0882-596319511004-0006$3.00/0
Journal of Pediatric Nursing, Vol 10, No 4 (August), 1995

MILES AND HOLDITCH-DAVIS
of full-term infants (Gennaro, Zukowsky, Broo- ten, Lowell, & Visco, 1990; Goodman & Sauve, 1985). They report taking longer to assume the maternal role and to feel affection for their infants (Goodman & Sauve, 1985; Jeffcoate, Humphrey, & Lloyd, 1979). These emotional responses continue for a long time. Six months after discharge, most mothers still had distress- ing memories of their NICU experiences, and mothers with the most painful memories re- ported the least attachment to their children (Aflleck et al., 1990).
These maternal emotional responses, com- bined with the immature and disorganized be- haviors of premature infants, may interfere with parenting at least through the first year of life (Beckwith & Cohen, 1978; Brown & Bakeman, 1978; Minde, Whitelaw, Brown, & Fitzhard- inge, 1983). Interactions between mothers and premature infants have been found to be less mutually satisfying than those between mothers and full-term infants (Bakeman & Brown, 1980; Wille, 1991). Premature infants are less respon- sive, vocalize less, avert their gaze more, and show less positive affect than full-term infants (Bakeman & Brown, 1980; Crnic, Ragozin, Greenberg, Robinson, & Basham, 1983; Di- Vitto & Goldberg, 1979; Field, 1977; Laney & Sandler, 1982). Mothers leave premature in- fants alone more and look at, hold, smile, and play games with them less (Davis & Thoman, 1988; Field, 1979; Minde, Perrotta, & Marton, 1985). During brief interactions, mothers of premature infants work harder to initiate and maintain interactions than do mothers of full- term infants, but they receive fewer positive responses from their infants (Bakeman & Brown, 1980; Barnard, Bee, & Hammond, 1984; Harri- son, 1990). These differences decrease during the first year (Crawford, 1982; Goldberg, Brach- feld, & DiVitto, 1980). However, mothers of prematurely born children continue to use dif- ferent strategies to engage their children (Stevenson, Roach, Ver Hoeve, & Leavitt, 1990) and may be somewhat less involved with them (Barnard et al., 1984).
Relatively little is known about how preterm birth affects parenting after infancy. Mothers of 3-year-old prematurely born children have been reported to view their children as more vulner- able than mothers of full-term children, and this sense of vulnerability was highest for children with continuing health or developmental prob- lems (Perrin, West, & Culley, 1989). Perception
of vulnerability was associated with more prob- lems with discipline, peer relationships, and self control. O'Mara and Johnston (1989) found that mothers of 3-year-old prematurely born children were more likely to be overindulgent, but not overprotective, than mothers of children born at term. Parents of preschool, prematurely born children also have been described as highly concerned about health and developmental out- comes and the difficult personalities of their children (McCain, 1990). They rated their pre- maturely born preschooler as weaker than sib- lings born at term (Bidder et al., 1974). Some studies have found no differences in the atti- tudes of mothers toward prematurely born and normal-term preschoolers (Gross, Rocissano, & Roncoli, 1989; Scheiner, Sexton, Rockwood, Sullivan, & Davis, 1985; Trause & Kramer, 1983).
The extent to which premature birth affects mother-child interactions also is unclear. One study found no difference in interactions at age 2 years (Greenberg & Crnic, 1988). However, another study found that mothers of prema- turely born preschoolers used fewer suggestions and more directive statements, and their chil- dren showed less self-directed behavior than full-term children (Landry, Chapieski, Richard- son, Palmer, & Hall, 1990). These differences occurred primarily in the subset of prematurely born children who experienced severe medical complications.
Thus, more needs to be known about the long-term influences of prematurity and related stressors on the parenting of these children. A particularly important developmental period for the study of parenting is when the child is a preschooler. At this time, the child becomes developmentally more capable and challenges parents with growing autonomy. The purpose of this article was to explore whether mothers' recollections surrounding the births and hospi- talizations of their preterm infants affected their perceptions and parenting of these chil- dren at 3 years of age.
METHODS
Subjects
The subjects and their primary caretakers were a convenience sample recruited as part of a larger longitudinal study of the relationship between sleep-wake states during prematurity and developmental outcomes at age 3 years (Holditch-Davis, 1990; Holditch-Davis, Ed-

PARENTING PREMATURELY BORN CHILDREN
wards, & Wigger, in press; Huber, Holditch- Davis, & Brandon, 1993). Criteria for admission for the larger study were that the subjects weighed less than 1,500 g at birth or required mechanical ventilation or both and that they had no congenital neurological problems. Sub- jects with postnatal neurological insults were included. Primary caretakers of the first 30 subjects to complete the larger study were included in this study.
The subjects for this study included 27 pri- mary caretakers (24 mothers and three grand- mothers with legal custody) of 30 3-year-old, prematurely born children. (There were three sets of twins in the study.) The caretakers had a mean age of 29.9 years (SD = 4.2; 20 to 56). Educational levels varied with 3 caretakers without a high school diploma, 13 with a high school diploma, 4 with more than a high school education but no college degree, and 4 with a college education and beyond (missing data on 3). A majority (n = 20) were married.
The 18 female and 12 male subjects had a mean gestational age of 28.6 weeks (SD = 2.5) and a mean birthweight of 1,102 g (SD = 339). Twelve were white, and 18 were African- American. Their high-risk neonatal courses are indicated by the fact that they averaged 11.5 days of mechanical ventilation (SD = 12.7). Dur- ing their neonatal hospitalizations, 11 subjects had an intraventricular hemorrhage, 7 had ma- jor surgery, 6 had chronic lung disease, and 6 had sepsis. At age 3 years, two subjects had severe cerebral palsy, and two had ventricular- peritineal shunts as a result of hydrocephalus from an intraventricular hemorrhage. Six sub- jects, including 3 of the subjects with health problems, were in an early intervention pro- gram. The other subjects in the study did not have serious medical problems; however, many of them did have minor health problems and developmental delays that were not diagnosed until after the interviews (Huber et al., 1993). Sixteen of the subjects were the first-born child, 9 were the second, 4 were the third, and 1 was the fourth. Although three sets of twin subjects participated in the study, there were five addi- tional twin or triplet births in which only one subject participated in the study.
Methods
Primary caretakers of eligible infants were contacted in person or by phone regarding enrollment in the study. If they agreed to
participate, they signed an approved Internal Review Board consent form indicating agree- ment for their children and themselves to partici- pate in the study during the neonatal hospitaliza- tion. When the children reached 3 years of age, the parents and children were brought to a developmental evaluation center for develop- mental assessment. During this evaluation, the mothers were interviewed in a private office about their experiences in parenting their chil- dren. They also answered three questionnaires focusing on their perceptions of their children and completed a demographic information sheet. Most of the interviews were conducted by the first author (M.S.M.); the remainder were conducted by one of two doctoral students who were research assistants for the study.
Instruments
The Maternal Attitude Scale was adapted from a similar scale published by Bidder et al. (1974). This nine-item semantic differential scale assesses mothers' perceptions of "a child born prematurely," "an average child," and "my child." Mothers were asked first to rate their own children on the scale, the scale is repeated for average 3-year-old children, and then finally they were asked to rate children born prema- turely. Mothers completed each part of the scale before they were told about the next so that their ratings of their own children were not based on comparing their children with either average 3-year-olds or with prematurely born children in general. Each item was rated from 1 to 7 (higher scores reflect less positive ratings of the children).
The Vulnerable Child Scale (Perrin et al., 1989) measures mothers' perceptions of their children's vulnerability. The tool consists of 16 items about the child's health and physical condition. Mothers were asked to rate each characteristic as definitely true, mostly true, mostly false, or definitely false. Two items are positively worded and are reversed for scoring. Each item receives a score from 1 to 4, then the item scores are summed. The total score ranges from 16 to 64, with lower scores indicating a higher sense of vulnerability. Cronbach's alpha coefficient was reported as .75 (Perrin et al., 1989); the alpha for this sample was .52.
The Social Assets Inventory for 3-year-olds, a modification of the Social Assets Inventory by Schaefer and Edgerton (1979), assesses moth- ers' perceptions of the social strengths of their
246 MILES AND HOLDITCH-DAVIS
children. The original scale consisted of 24 items in six factors-verbal and expressive tal- ent, appearance, relationship with adults, health, athletic ability, and grooming-with factor load- ing ranging from .54 to 37. The grooming items were eliminated, and slightly different verbal talent items were selected to better reflect the capabilities of 3-year-olds. Two health items and one athletic ability item were added. Thus, the 3-year-old tool consisted of five items mea- suring athletic ability, four items measuring appearance, four items measuring relationship with adults, six items measuring health, and four items measuring verbal and expressive talents. Mothers rated their children on each item compared with average 3-year-olds on a five-point scale, that is, very low, low, average, high, and very high. Cronbach's alpha coeffi- cients for this sample were .78 for athletic abilities, .75 for appearance, .81 for relationship with adults, .73 for health, and .81 for talents.
Maternal Interviews Tape-recorded, semistructured interviews fo-
cused on memories of the births and hospitaliza- tions of the children and then on subsequent and present experiences and concerns as par- ents. Mothers were asked first to tell the stories of their children's births and subsequent hospi- talizations. Probes were used to focus on spe- cific aspects of these experiences. They also were asked to discuss their readiness for and response at the time of discharge and subse- quent health, development, or parenting prob- lems. Interviewers then focused on current experiences and issues related to parenting the children.
The interviews were transcribed verbatim. The constant comparative method was used in the analysis of the interview data (Strauss &
Corbin, 1990). Preliminary analysis was concur- rent with data collection. As themes were iden- tified from early interviews, the interview for- mat was altered to probe in areas identified as salient. The two investigators reviewed each transcript independently using a process of open coding to identify emerging concepts, including properties and dimensions. They then met and conducted an intensive review of the individual analyses to confirm or alter the find- ings. Axial coding was used to examine the relationship between concepts, and selective coding was used to further analyze the core concept and subconcepts and to establish the relationships among them.
RESULTS
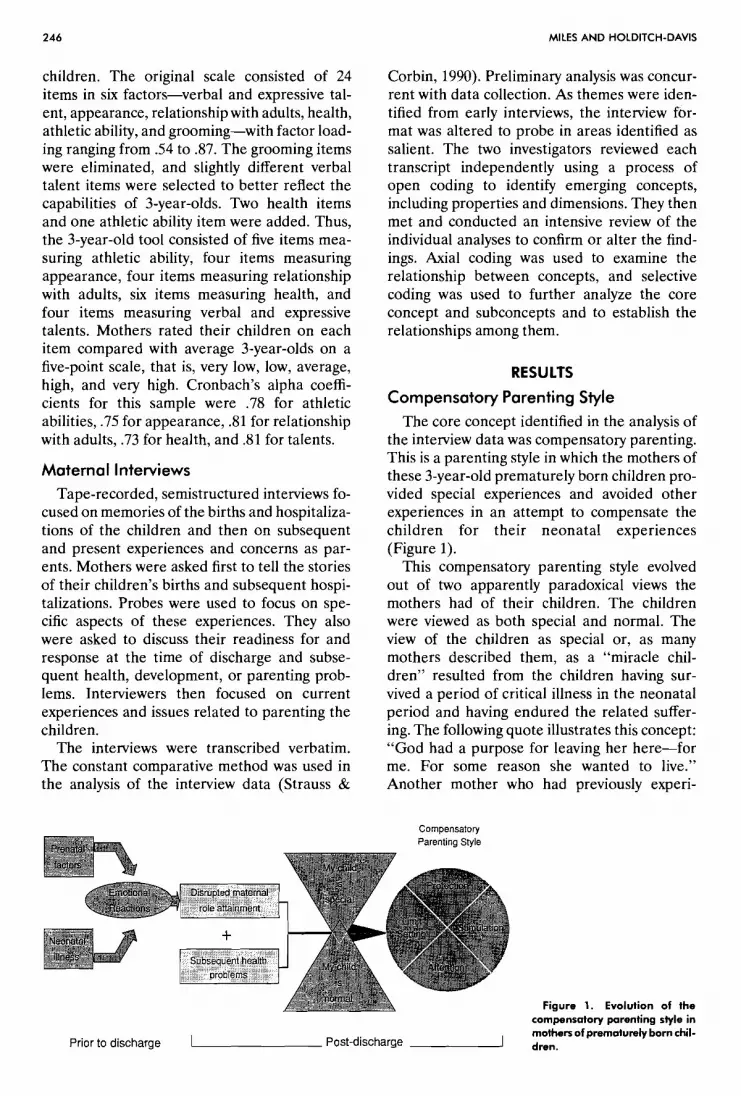
Compensatory Parenting Style The core concept identified in the analysis of
the interview data was compensatory parenting. This is a parenting style in which the mothers of these 3-year-old prematurely born children pro- vided special experiences and avoided other experiences in an attempt to compensate the children for their neonatal experiences (Figure 1).
This compensatory parenting style evolved out of two apparently paradoxical views the mothers had of their children. The children were viewed as both special and normal. The view of the children as special or, as many mothers described them, as a "miracle chil- dren" resulted from the children having sur- vived a period of critical illness in the neonatal period and having endured the related suffer- ing. The following quote illustrates this concept: "God had a purpose for leaving her here-for me. For some reason she wanted to live." Another mother who had previously experi-
. - 7 - ,
Figure 1. Evolution of the compensatory parenting style in mothers of prematurely born chil-
Prior to discharge I Post-discharge 1 dren.

PARENTING PREMATURELY BORN CHILDREN
enced the death of an infant reported that "She was a miracle to replace the child we lost." Mothers reported that this view of the children as special extended to other family members, especially grandparents.
At the same time, the mothers also worked hard at viewing the children as normal. They described their children as bright and average. "Jamey is just as bright, if not brighter, than either one of my other three children." If the children were small, comments about normality might be tempered with "except for his size." Children who had residual health problems were viewed as doing much better than ex- pected. "No one can believe they [twins] were preemies, they look so normal." For several mothers, normality extended into a denial of serious health problems. One mother, although admitting that the only thing different about her daughter was her eyes, stopped all treatment for extremely severe strabismus that eventually led to serious visual impairment.
Compensatory parenting involved alterations in the following four aspects of parenting: pro- tection, stimulation, attention, and limit setting. Not all of them were altered for all mothers. However, all mothers experienced alterations in at least one of them, and most experienced alterations in more than two.
The normal maternal protective behaviors of keeping the children safe from harm were intensified. Many mothers described not allow- ing people to get near the infants, thereby reducing the risk of infection. Some mothers also limited fathers' involvement. "I was real protective over her. I didn't let him get around her and touch her and stuff like that. 1 was like that for at least three months after she was at home." During the early months, these feelings of protection were reinforced by maternal fears that the infants might still die. Many infants went home with continued health problems, such as hernias.
Most mothers reported that feelings of protec- tion continued after infancy. One mother whose child was the only surviving triplet was still concerned about germs at the 3-year interview. "I wash her hands constantly." Feelings of protection led to difficulties in leaving the child with baby-sitters other than close family mem- bers. Mothers also described watching the chil- dren when they were sleeping and when they were playing "in case they get hurt." As one mother noted, "Deep down you feel you've got
to protect him until he can take care of himself . . . to make sure he's OK."
Maternal activities involved in fostering the children's development also were heightened. The mothers were intensely concerned about providing enough stimulation and thus reported providing more stimulation, as well as special experiences that were not ordinarily affordable, to the children than to siblings. One mother described performing finger movements, "do- d o ~ ~ , ' ' in front of her child's face twice a day "so she wouldn't be retarded." She also checked developmental milestones monthly and stimu- lated her daughter in areas in which she lagged. A low-income, single mother reported working extra hours, which necessitated leaving her daughter with her parents, to provide for the opportunity for her child to attend a private preschool.
The mothers reported that the level of atten- tion paid to the children also was increased greatly. The children became the focus of atten- tion in the family, receiving more attention than siblings. Although this was fostered by mothers, it was also encouraged by many relatives and friends. As one mother noted, "She's the star attraction." In addition, some of the children seemed to expect a high level of attention, often demanding to be cuddled, held, or stroked. One mother pondered about this attention, "I won- der if we didn't give her more than she needed. I don't know . . . these are things I ask myself a
In addition, behaviors related to limit setting and making demands to encourage develop- ment of responsibility were altered. The moth- ers believed that the children had been through too much already and thus were unable to set age-appropriate limits. They described them- selves as "lenient" and as "spoiling" the chil- dren. As one mother described her twins, "They are terribly bad but they are turning out the way I want." Mothers felt helpless to change disci- pline patterns that they knew were not good for the children. One mother articulated the prob- lem: "I have always had to make myself look back to [the NICU] when I got ready to disci- pline Katie. That she went through as much as she did and fought as hard as she did to be here. I always have to give her that little bit of leniency in discipline. And I know that it will probably ruin her in years to come."
Mothers were reluctant not to respond to the child's every want. They reported buying lots of

MILES AND HOLDITCH-DAVIS
toys and taking the child to special places. "Whatever she wants, I try to let her have it. I think I do spoil her." As another mother noted, "I want her to have everything she possibly can. I want her to live as best she can, too." The most difficult aspect of parenting for one mother was "her always wanting something and my always trying to give it to her."
As a result, the children were described as dependent, stubborn, willful, hardheaded, whiny, and determined to get their own way. Although these behaviors often are characteristics of preschool children, many mothers reported more problems with the prematurely born child than siblings. "That's one thing I do wrong. I show partiality with Mark . . . I let him get away with stuff." Another mother reported that her 3-year- old, prematurely born child was spoiled and still considered the baby despite the fact that there was a younger sibling.
Factors Influencing Compensatory Parenting
Several factors influenced the mothers' per- ceptions of their children and the development of their compensatory parenting styles. Salient prenatal and labor and delivery experiences included previous pregnancy loss, high-risk preg- nancy or acute illness of the mothers, and crises associated with prenatal diagnostic procedures. For example, one mother who experienced a rare life-threatening illness just before delivery still felt guilty about causing her child's neonatal illness. This mother reported high parenting stress primarily because she felt she had to give her child everything and could not set limits.
Memories of the NICU, particularly recall of the infants' appearances and suffering, the equipment surrounding the children, and the threat of death or serious health problems, also influenced responses to the children 3 years later. As one mother stated, "The most difficult time was all of it. I was in pure pain . . . just seeing them like that." Memories of watching acute episodes of medical deterioration or the infants in pain, such as during invasive proce- dures, were particularly salient. "It made me feel sorry for her because . . . like why did it have to happen to her." Mothers reported intense emotional responses to these experi- ences, including guilt, helplessness, fear of death, anxiety, and depression. Although most moth- ers vividly recalled their experiences, a few mothers described feeling rather detached or
stoic because of the intense distress they could not face. "There's sort of a stoicism. . . . It's just real hard to take that off and look at what's underneath." These memories directly affected later parenting. As a mother of twins noted, "I know it [lack of discipline] is because Marie was the sickest. . . . I guess I feel like I be doing her wrong . . . if I don't let her have a little bit more."
These experiences and the mothers' emo- tional responses to them affected the normal process of maternal role attainment, that is, becoming involved with the infant, assuming maternal caregiving, and developing a strong identity as mother. Several mothers reported delaying involvement and attachment until the infant could come home. This led to guilt feelings in later years: "My major regret . . . is not giving John more physical attention for two weeks . . . that is my major guilt." Other moth- ers failed to achieve the maternal role alto- gether. Two mothers who were caring for their child reported still not feeling like a mother, and the three grandmother caretakers sug- gested in their interviews that the emotional responses of the biological mothers were a factor in the relinquishment of their maternal role with the children.
Subsequent health problems, such as apnea, hernias, and infections, after discharge further influenced maternal perceptions of the chil- dren. One mother connected "spoiling her daughter badly" with her intense distress over her daughter's hernias and a subsequent bout of pneumonia.
Compensatory Parenting and Maternal Perceptions of the Child
Maternal Attitudes Scale
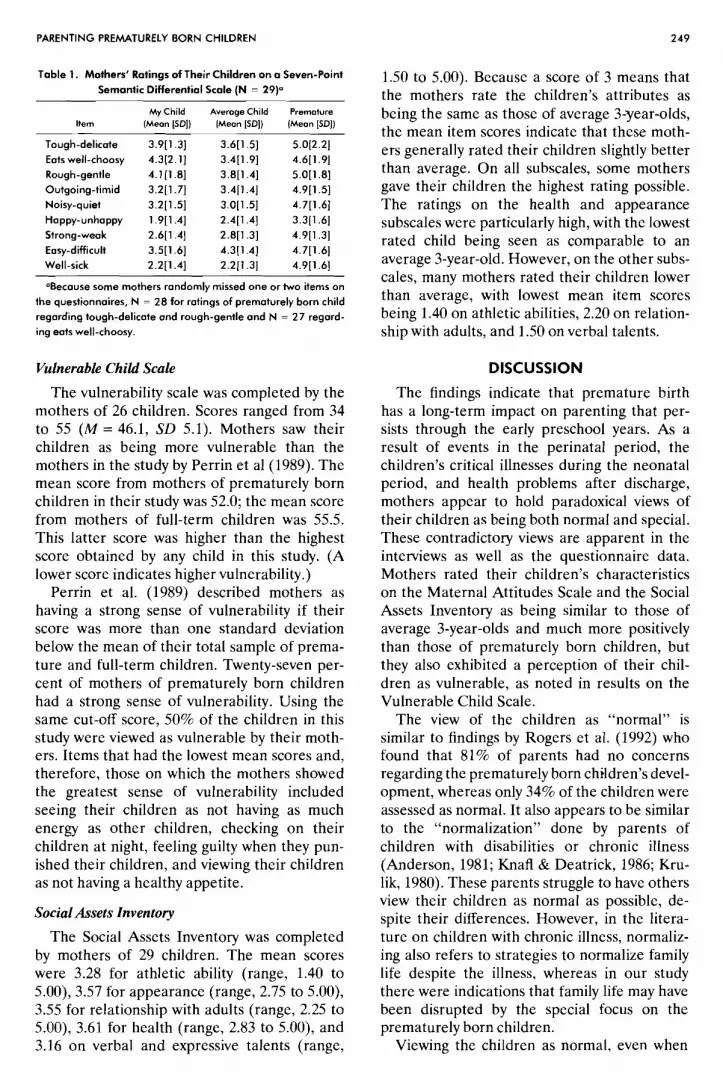
The mothers of 29 children completed the Maternal Attitudes Scale (the data for one child was missing; Table 1). The means indicated that on the average, the mothers rated their children as having more positive characteristics and be- ing stronger than typical prematurely born chil- dren and as being similar to an average 3-year- olds. In comparison with children born prematurely, 67.9% of mothers rated their chil- dren as being tougher, 44.4% as eating better, 50% as rougher, 58.6% as being more outgoing, 65.5% as being noisier, 72.4% as happier, 82.7% as stronger, 58.6% as easier, and 82.7% as more likely to be well.
PARENTING PREMATURELY BORN CHILDREN
Table 1. Mothers' Ratings of Their Children on a Seven-Point
Semantic Differential Scale (N = 2 9 ) ~
Item
Tough-delicate
Eots well-choosy
Rough-gentle
Outgoing-timid
Noisy-quiet
Happy-unhappy Strong-weak
Easy-difficult Well-sick
My Child (Mean [SO])
3.9[1.3] 4.3[2.1] 4.1 (1.81 3.2[1.7] 3.2[1.5] 1.9[1.4] 2.6[1.4] 3.5[1.6] 2.2[1.4]
Average Child (Mean [SO])
3.6[1.5] 3.411.91 3.8[1.4] 3.4[1.4] 3.0[1.5] 2.4[1.4] 2.8[1.3] 4.3r1.41 2.2[1.3]
Premature (Mean [SO])
5.0[2.2] 4.6[1.9] 5.0[1.8] 4.9[1.5] 4.7[1.6] 3.311.61 4.9[1.3] 4.7[1.6] 4.9[1.6]
OBecause some mothers randomly missed one or two items on
the questionnaires, N = 28 for ratings of prematurely born child
regarding tough-delicate and rough-gentle and N = 27 regard-
ing eats well-choosy.
Vulnerable Child Scale
The vulnerability scale was completed by the mothers of 26 children. Scores ranged from 34 to 55 (M = 46.1, SD 5.1). Mothers saw their children as being more vulnerable than the mothers in the study by Perrin et a1 (1989). The mean score from mothers of prematurely born children in their study was 52.0; the mean score from mothers of full-term children was 55.5. This latter score was higher than the highest score obtained by any child in this study. (A lower score indicates higher vulnerability.)
Perrin et al. (1989) described mothers as having a strong sense of vulnerability if their score was more than one standard deviation below the mean of their total sample of prema- ture and full-term children. Twenty-seven per- cent of mothers of prematurely born children had a strong sense of vulnerability. Using the same cut-off score, 50% of the children in this study were viewed as vulnerable by their moth- ers. Items that had the lowest mean scores and, therefore, those on which the mothers showed the greatest sense of vulnerability included seeing their children as not having as much energy as other children, checking on their children at night, feeling guilty when they pun- ished their children, and viewing their children as not having a healthy appetite.
Social Assets Inventory
The Social Assets Inventory was completed by mothers of 29 children. The mean scores were 3.28 for athletic ability (range, 1.40 to 5.00), 3.57 for appearance (range, 2.75 to 5.00), 3.55 for relationship with adults (range, 2.25 to 5.00), 3.61 for health (range, 2.83 to 5.00), and 3.16 on verbal and expressive talents (range,
1.50 to 5.00). Because a score of 3 means that the mothers rate the children's attributes as being the same as those of average 3-year-olds, the mean item scores indicate that these moth- ers generally rated their children slightly better than average. On all subscales, some mothers gave their children the highest rating possible. The ratings on the health and appearance subscales were particularly high, with the lowest rated child being seen as comparable to an average 3-year-old. However, on the other subs- cales, many mothers rated their children lower than average, with lowest mean item scores being 1.40 on athletic abilities, 2.20 on relation- ship with adults, and 1.50 on verbal talents.
DISCUSSION
The findings indicate that premature birth has a long-term impact on parenting that per- sists through the early preschool years. As a result of events in the perinatal period, the children's critical illnesses during the neonatal period, and health problems after discharge, mothers appear to hold paradoxical views of their children as being both normal and special. These contradictory views are apparent in the interviews as well as the questionnaire data. Mothers rated their children's characteristics on the Maternal Attitudes Scale and the Social Assets Inventory as being similar to those of average 3-year-olds and much more positively than those of prematurely born children, but they also exhibited a perception of their chil- dren as vulnerable, as noted in results on the Vulnerable Child Scale.
The view of the children as "normal" is similar to findings by Rogers et al. (1992) who found that 81% of parents had no concerns regarding the prematurely born children's devel- opment, whereas only 34% of the children were assessed as normal. It also appears to be similar to the "normalization" done by parents of children with disabilities or chronic illness (Anderson, 1981; Knafl & Deatrick, 1986; Kru- lik, 1980). These parents struggle to have others view their children as normal as possible, de- spite their differences. However, in the litera- ture on children with chronic illness, normaliz- ing also refers to strategies to normalize family life despite the illness, whereas in our study there were indications that family life may have been disrupted by the special focus on the prematurely born children.
Viewing the children as normal, even when

MILES AND HOLDITCH-DAVIS
they child had developmental or health prob- lems, also may be an extension of what AfBeck, Tennen, Pfeiffer, Fifield, and Rowe (1987) have described as downward comparison, in which parents make positive comparisons between their infants and other infants in the NICU. The mothers in this study viewed the characteristics of typical, prematurely born children as being much less positive than those of average chil- dren. Thus, they clearly exhibited what has been termed as prematurity stereotype (Miller & Ot- tinger, 1986; Stern & Hildebrandt, 1986; Stern & Karraker, 1988), and this stereotype persisted despite 3 years of parenting prematurely born children. However, the mothers did not appear to apply this stereotype to their own children. Instead, they viewed their own children as having characteristics that were at least as positive as those of average 3-year-olds. Prema- turity stereotyping by mothers of prematurely born children probably does not interefere with their relationship with their own children, as some researchers have suggested (Stern & Karraker), but rather serves to confirm the mothers' belief that their children are normal.
This belief that their children are normal despite everything they went through in the NICU and despite belonging to a group of at-risk children-the prematurely born-may lead the mothers' to view the children as spe- cial. This is similar to Anderson's (1981) finding that parents communicated two messages to their children with chronic illness, that is, you are normal, and you are different. Parents often idealize children with chronic illness and view them as heros who have survived despite adver- sity (Shapiro, 1983). The specialness of prema- turely born children also can be seen in the high ratings that the mothers gave their children on health and appearance on the Social Assets Inventory.
Heightened maternal protective behaviors and perceptions of the children as vulnerable might be related to this view of the children as special. A number of investigators have identified a vulnerable child syndrome in parents of chil- dren who have survived a critical illness (Green & Solnit, 1964; Levy, 1980; Perrin et al., 1989). Indeed, half of the mothers in our viewed their children as vulnerable.
The maternal views of these prematurely born children as both normal and special, coupled with the mothers' emotional responses to the neonatal experiences, led to a compensa-
tory parenting style in which the children were treated differently than other children in the family. The mothers protected these children more than usual, provided them with more stimulation and attention, demanded less, and did not set age-appropriate limits. Compensa- tory parenting is similar to the concept of overprotective parenting found in the literature on children with cancer and other serious health problems, because this concept includes diffi- culty in limit setting, increased attention, and spoiling the child as well as overprotective behaviors (Holaday, 1989; Shapiro, 1983). We choose not to label the core concept as overpro- tective parenting, however, because this con- cept connotes negative parenting.
Compensatory parenting probably has both benefits and disadvantages for prematurely born children. For example, increased maternal atten- tion and stimulation might result in better developmental outcome for the children. Mater- nal behaviors related to stimulation and atten- tion may be an extension of the behaviors taught to parents to promote infants' development both in the NICU and after discharge. In fact, the children in this sample did have a high rate of developmental problems (Huber et al., 1993). Mothers appeared to be showing that they were aware of these problems when they gave their children comparably low ratings on the athletic ability and verbal talents subscales of the Social Assets Inventory. On the other hand, the need to view the children as normal may result in some of the mothers' apparent unwillingness to participate in treatment for developmental de- lays and other health problems (Huber et al., 1993; Rogers et al., 1992).
The view of the children as special, the perceived vulnerability of these children, and the need to protect them may affect the moth- ers' ability to set limits on the children in the preschool period. Almost universally, these mothers reported discipline problems, and guilt about punishing the children was one of the most common concerns reported by them on the Vulnerable Child Scale. This difficulty ap- pears to be most directly related to residual memories of the NICU experiences, including guilt feelings, because the mothers could do nothing to spare their infants pain and suffer- ing. Other studies have reported similar feelings in mothers of prematurely born preschoolers, which have been associated with overindul- gence (O'Mara & Johnston, 1989).
PARENTING PREMATURELY BORN CHILDREN 251
RECOMMENDATIONS FOR FURTHER STUDY
Findings from this study are hypothesis gener- ating. Further research with a larger sample is needed to verify whether the findings from this study are generalizable. Prospective research is needed to determine when and how a compen- satory parenting style evolves. Research also is needed that directly measures and examines links between parental stress experiences dur- ing the NICU period and parenting over time; that examines the effects of compensatory parenting on developmental outcomes; and that examines how other factors-such as number of other children, level of family support and involvement, and marital status-might affect compensatory parenting. In addition, case stud- ies and prospective studies of differences in parenting styles of parents with multiple birth preterm infants is needed. Such studies can help to clarify the possible differential impact of maternal perceptions related to each infant's appearance, level of acuity, treatments, and suffering on the subsequent parenting of each child.
The impact of compensatory parenting on family life also needs further exploration. Data from our interviews suggests that this parenting style sometimes had the result of excluding the fathers from caregiving. In addition, the moth- ers' tendency to give the prematurely born children more attention, stimulation, and protec- tion and to set fewer limits and demands might lead to long-term problems for siblings. Nursing interventions that help mothers maximize the benefits of this parenting style while minimizing its problems must be developed.
Finally, research is needed for testing nursing interventions with these vulnerable parents both during and after the infants7 hospitalizations. The need for testing models of intervention that continue throughout the preschool period is obvious.
discharged from the hospital. One critical focus for this support is providing an opportunity for parents to discuss the impact of t.he NICU experiences on their relationship with their children and their parenting. Although it had been 3 years since their children had been hospitalized in an NICU, and the vast majority of the children did not have an obvious handi- cap, all of the mothers in our study still had issues from their NICU experiences that they eagerly shared during the interview.
This suggests the need for mothers to have an opportunity to freely share their experiences related to labor and delivery and the infants' hospitalizations in the NICU with supportive, neutral, caring people. This debriefing could be accomplished at the time of discharge by the primary nurse or the discharge nurse. During outpatient follow-up contacts, whether at high- risk infant clinics, at public health clinics, or with private health care providers, mothers may continue to need opportunities to discuss expe- riences and feelings related to their infants' births and hospitalizations. Rather than staff assuming that they know what the infants and parents experienced, intake interviews could include questions such as "Tell me about your baby's birth and hospitalization." "What was this like for you?" "How are these memories of that time affecting you now as you care for your child?" In addition, outpatient contacts and home visits by public health nurses and others need to focus on the mothers' own concerns, experiences, and needs, as well as those related to parenting their prematurely born children. Issues, such as compensation, normalization, stimulation, attention, overprotection, disci- pline, and the impact on the family, might be considered within the context of the mothers' own problems and needs. Finally, it is obvious that systems of care for these mothers need to be developed such that follow-up continues at least through their children's early preschool
IMPLICATIONS FOR PRACTICE years.
The findings from this study point to the mothers' need for ongoing support by nurses ACKNOWLEDGMENT and other health care professionals both during The authors thank Diane C. Hudson, Deborah Assad hospitalization and after premature infants are Lee, and Debra B. Miller for technical assistance.
REFERENCES Affleck, G., Tennen, H., Pfeiffer, C., Fifield, J., & Rowe, Affleck, G., Tennen, H., Rowe. J., & Higgins, P. (1990).
J. (1987). Downward comparison and coping with serious Mothers' remembrances of newborn intensive care: A medical problems. American Journal of Orthop~chiatry, 57, predictive study. Journal ofPediatric Ps)'chology, 15, 67-81 570-578. Anderson, J.M. (1981). The social construction of illness

MILES AND HOLDITCH-DAVIS
experience: Families with a chronically-ill child. Journal of Advanced Nursing, 6, 427-434.
Bakeman, R., & Brown, J.V. (1980). Early interaction: Consequences for social and mental development at three years. Child De~,elopment, 51, 437-447.
Barnard, K.E., Bee, H.L., & Hammond, M.A. (1984). Developmental changes in maternal interactions with term and preterm infants. Infant Behavior and Development, 1, 101-113.
Beckwith, L., & Cohen, S.E. (1978). Preterm birth: Hazardous obstetrical and postnatal events as related to caregiver-infant behavior. Infant Beha~ior and Development, 1, 403-411.
Bidder, R.T., Crowe, E.A., & Gray, O.P. (1974). Mothers' attitudes to preterm infants. Archives of Disease in Child- hood, 49, 766-770.
Brooten, D., Gennaro, S., Brown, L.P., Butts. P., Givons. A.L., Bakewell-Sachs, S., & Kumar, S.P. (1988). Anxiety. depression, and hostility in mothers of preterm infants. NursingResearch, 37, 213-216.
Brown. J.V., & Bakeman, R. (1978). Relationships of human mothers with their infants during the first year of life: Effect of prematurity. In R.W. Bell & W.P. Smother- man (Eds.), Maternal influences and ear& behavior (pp. 353-373). New York: Spectrum.
Crawford, J.W. (1982). Mother-infant interaction in pre- mature and fullterm infants. Child De~<elopnlent, 53, 957- 962.
Crnic, K.A., Ragozin, A.S., Greenberg, M.T., Robinson, N.M., & Basham, R.B. (1983). Social interaction and developmental competence of preterm and fullterm infants during the first year of life. Child Development, 54, 1199- 1210.
Davis, D.H., & Thoman, E.B. (1988). The early social environment of premature and fullterm infants. Earb Hu- man Developn~ent, 17, 221-232.
DiVitto, B.. & Goldberg, S. (1979). The effects of newborn medical status on early parent-infant interaction. In T.M. Field, A.M. Sostek, S. Goldberg, & H.H. Shuman (Eds.), Infants born at risk: Behavior and development (pp. 311-332). New York: SP Medical & Scientific.
Easterbrooks, M.A. (1988). Effects of infant risk status on the transition to parenthood. In G.Y. Michaels & W.A. Goldberg (Eds.), The transition toparenthood: Current theoly and research (pp. 176-208). New York: Cambridge Univer- sity Press.
Field, T. (1979). Games parents play with normal and high-risk infants. Child Psychiatly and Human Development, 10, 41-47.
Field, T.M. (1977). Effects of early separation, interactive deficits, and experimental manipulations on infant-mother face-to-face interaction. Child De~,elopment, 48, 763-777.
Gennaro, S. (1988). Postpartal anxiety and depression in mothers of premature infants. Nursing Research, 37, 82-85.
Gennaro, S., Zukowsky, K., Brooten, D., Lowell, L.. & Visco, A. (1990). Concerns of mothers of low birthweight infants. Pediatric Nursing, 16, 459-462.
Goldberg, S., Brachfeld, S., & DiVitto, B. (1980). Feed- ing, fussing, and play: Parent-infant interaction in the first year as a function of prematurity and perinatal medical problems. In T.M. Field, S. Goldberg, D. Stern, & A.M. Sostek (Eds.), High-risk infants and children: Adult andpeer inreractions (pp. 133-153). New York: Academic.
Goodman, J.R., & Sauve. R.S. (1985). High risk infant: Concerns of mother after discharge. Birth. 12, 235-242.
Green, M., & Solnit, A.J. (1964). Reactions to the threatened loss of a child: A vulnerable child syndrome. Pediatrics, 34, 58-66.
Greenberg, M.T., & Crnic, K.A. (1988). Longitudinal predictors of developmental status and social interaction in premature and fullterm infants at age two. Child Develop- ment, 59. 554-570.
Gross, D.. Rocissano, L., & Roncoli, M. (1989). Maternal confidence during toddlerhood: Comparing preterm and fullterm groups. Research in Nursing and Health, 12, 1-9.
Harrison, M.J. (1990). A comparison of parental interac: tions with term and preterm infants. Research in Nursingand Health, 13. 173-179.
Holditch-Davis, D. (1990). The development of sleeping and waking states in high-risk preterm infants. Infant Beha~ior and Development, 13, 513-53 1.
Holditch-Davis, D., Edwards, L. & Wigger, M.C. (1994). Pathologic apnea and brief respiratory pauses in preterm infants: Relation to sleep state. Nursing Research, 43, 293- 300.
Holaday, B. (1989). The family with a chronically ill child: An interactional perspective. In C. Gillis, B.L. Highley, B.M. Roberts, & I.M. Martinson. Toward a science offamily nursing. New York: Addison Wesley.
Huber, C., Holditch-Davis, D., & Brandon, D. (1993). High-risk preterms at three years of age: Parental response to the presence of developmental problems. Children's Health Care, 22, 107-124.
Jeffcoate, J.A., Humphrey, M.E., & Lloyd, J.K. (1979). Disturbance in parent-child relationship following preterm delivery. Developnlental Medicine and Child Neurology, 21, 344-352.
Knafl, K., & Deatrick, J. (1986). How families manage chronic conditions: An analysis of the concept of normaliza- tion. Research in Nursing and Health, 9, 215-222.
Krulik, T. (1980). Successful 'normalizing' tactics of parents of chronically-ill children. Journal of Advanced Nursing, 5, 573-578.
Landry, S.H., Chapieski, M.L., Richardson, M.A., Palmer, J.. & Hall, S. (1990). The social competence of children born prematurely: Effects of medical complications and parent behaviors. Child De~selopment, 61, 1605-1616.
Laney, M.D., & Sandler, H.M. (1982). Relationships among maternal stress, infant status, and mother-infant interactions. In L.P. Lipsitt & T.M. Field (Eds.), Infant behavior and development: Perinatal risk and newborn behav- ior (pp. 139-152). Nonvood, NJ: Ablex.
Levy, J.C. (1980). Vulnerable children: Parents' perspec- tives and the use of medical care. Pediatrics, 65, 956-963.
McCain, G.C. (1990). Parenting growing preterm infants. Pediatric Nursing, 16, 467-470.
Miles, M.S. (1989). Parents of critically ill premature infants: Sources of stress. Critical Care Quarterly, 12 (3), 69-74.
Miles, M.S., Funk, S.G., & Kasper, M.A. (1991). The neonatal intensive care unit environment: Sources of stress for parents. AACN Clinical Issues in Critical Care Nursing, 2, 346-354.
Miller, M.D., & Ottinger. D.R. (1986). Influence of labeling on ratings of infant behavior: A prematurity preju- dice. Journal of Pediatric Ps)'chology, 11, 561-572.
Minde, K., Perrotta, M., & Marton, P. (1985). Maternal caretaking and play with fullterm and premature infants. Journal of Child Psychology and Psychiatly, 26, 231-244.
Minde, K., Whitelaw, A., Brown, J., & Fitzhardinge, P. (1983). Effect of neonatal complications in premature infants on early parent-infant interactions. Developnlental Medicine and Child Neurology, 25, 763-777.
O'Mara. L., & Johnston, C. (1989). Mothers' attitudes and their children's behaviors in 3-year-olds born prema- turely and at term. Journal of Developmental and Behavioral Pediatrics, 10, 192-197.
Pederson, D.R., Bento, S., Chance. G.W., Evans, B., & Fox, A.M. (1987). Maternal emotional responses to preterm birth. American Journal of Orthopg~chiatly, 57 15-21.
Perrin, E.C., West, P.D.. & Culley, B.S. (1989). Is my child normal yet? Correlates of vulne;ability. pediatrics, 8j, 355-363.
Rogers, B.T., Booth, L.J., Duffy, L.C., Hassan, M.B.,

PARENTING PREMATURELY BORN CHILDREN
McCormick, P., Snitzer, J., & Zorn, W.A. (1992). Parents' developmental perceptions and expectations for their high- risk infants. De~~elopmenlal ntzd Behavioral Pediatrics, 13, 102-107.
Schaefer, E.S., & Edgerton, M. (1979). The development of llze social assels invenrory. (Available from Dr. Earl S. Schaefer, Department of Maternal and Child Health, CB No. 7400 Rosenau Hall, School of Public Health, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599- 7400.)
Scheiner, A.P., Sexton, M.E., Rockwood, J., Sullivan, D., & Davis, H. (1985). The vulnerable child syndrome: Fact and theory. Joumal of Developmental and Behavioral Pediat- rics, 6, 298-301.
Shapiro, J. (1983). Family reactions and coping strategies in response to the physically ill o r handicapped child: A review. Social Science and Medicine, 17, 913-931.
Stern, M., & Hildebrandt, K.A. (1986). Prematurity
stereotyping: Effects on mother-infant interaction. Child Development, 57, 308-3 15.
Stern, M.? & Karraker, K.H. (1988). Prematurity stereo- typing by mothers of premature infants. Journal ofPediatric P,ychology, 13, 255-263.
Stevenson, M.R. , Roach, M.A.. Ver Hoeve, J.N., & Leavitt, L.A. (1990). Rhythms in the dialogue of infant feeding: Preterm and term infants. Infant Behavior and Developnlent, 13, 51-70.
Strauss, A,, & Corbin, J. (1990). Basics of qualitative research: Grounded theory procedures and techniques. New- bury Park, CA: Sage.
Trause, M.A., & Kramer, L.I. (1983). The effects of premature birth on parents and their relationship. Develop- mental Medicine and Child Neurology, 25, 459-465.
Wille, D.E. (1991). Relation of preterm birth with quality of infant-mother attachment at one year. Infarrt Behavior arrd Development, 14, 227-240.
Related Documents











