Comparisons of methamphetamine psychotic and schizophrenic symptoms: A differential item functioning analysis Manit Srisurapanont a, ⁎, Suwanna Arunpongpaisal b , Kiyoshi Wada c , John Marsden d , Robert Ali e , Ronnachai Kongsakon f a Department of Psychiatry, Chiang Mai University, Chiang Mai, Thailand b Department of Psychiatry, Khon Kaen University, Khon Kaen, Thailand c Division of Drug Dependence Research, National Institute of Mental Health, Chiba-ken, Japan d National Addiction Centre, Institute of Psychiatry, University of London, London, UK e Department of Clinical and Experimental Pharmacology, University of Adelaide, Adelaide, Australia f Department of Psychiatry, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand abstract article info Article history: Received 15 November 2010 Received in revised form 2 January 2011 Accepted 15 January 2011 Available online 26 January 2011 Keywords: Differential item functioning Methamphetamine Psychosis Schizophrenia Symptom The concept of negative symptoms in methamphetamine (MA) psychosis (e.g., poverty of speech, flatten affect, and loss of drive) is still uncertain. This study aimed to use differential item functioning (DIF) statistical techniques to differentiate the severity of psychotic symptoms between MA psychotic and schizophrenic patients. Data of MA psychotic and schizophrenic patients were those of the participants in the WHO Multi- Site Project on Methamphetamine-Induced Psychosis (or WHO-MAIP study) and the Risperidone Long-Acting Injection in Thai Schizophrenic Patients (or RLAI-Thai study), respectively. To confirm the unidimensionality of psychotic syndromes, we applied the exploratory and confirmatory factor analyses (EFA and CFA) on the eight items of Manchester scale. We conducted the DIF analysis of psychotic symptoms observed in both groups by using nonparametric kernel-smoothing techniques of item response theory. A DIF composite index of 0.30 or greater indicated the difference of symptom severity. The analyses included the data of 168 MA psychotic participants and the baseline data of 169 schizophrenic patients. For both data sets, the EFA and CFA suggested a three-factor model of the psychotic symptoms, including negative syndrome (poverty of speech, psychomotor retardation and flatten/incongruous affect), positive syndrome (delusions, hallucinations and incoherent speech) and anxiety/depression syndrome (anxiety and depression). The DIF composite indexes comparing the severity differences of all eight psychotic symptoms were lower than 0.3. The results suggest that, at the same level of syndrome severity (i.e., negative, positive, and anxiety/depression syndromes), the severity of psychotic symptoms, including the negative ones, observed in MA psychotic and schizophrenic patients are almost the same. © 2011 Elsevier Inc. All rights reserved. 1. Introduction Methamphetamine (MA) psychosis is a state of MA intoxication with psychotic symptoms, commonly presented with delusions and hallucinations. This psychotic condition has been considered as a common and serious consequence of chronic, high dose, and/or continuous use of MA (Griffith et al., 1972). It is commonly described as closely simulating paranoid schizophrenia (Bell, 1965). The similarities in many aspects of MA psychosis and schizophre- nia have made amphetamine a primary psychotomimetic model agent in schizophrenia research. It is likely that the resemblance is caused by the altered function of mesolimbic dopamine systems and prefrontal cortical function (Robinson and Becker, 1986). Although clinical research is necessary for the development of MA psychosis services, few studies in this area have been carried out. Of many respects, symptom studies may be a priority area because these results are basic knowledge for further studies of MA psychosis, e.g., etiology, course, prognosis, and treatment. So far, most of the findings on the resemblance between MA psychosis and schizophrenia have mainly focused on positive psychotic symptoms, in particular delusions and hallucinations. The concept of negative symptoms in MA psychosis (e.g., poverty of speech, flatten affect, and loss of drive) is not new but still uncertain. Blunted affect and diminished spontaneity accompanied with paranoid-hallucinatory state were described in 1960s (Yui et al., Progress in Neuro-Psychopharmacology & Biological Psychiatry 35 (2011) 959–964 Abbreviations: CFA, confirmatory factor analysis; DIF, differential item functioning; EFA, exploratory factor analysis; IRT, item response theory; MA, methamphetamine; RLAI-Thai, Risperidone Long-Acting Injection in Thai Schizophrenic Patients; WHO- MAIP, WHO Multi-Site Project on Methamphetamine-Induced Psychosis. ⁎ Corresponding author at: Department of Psychiatry, Faculty of Medicine, Chiang Mai University, Muang, Chiang Mai 50200, Thailand. Tel.: +66 53 945422; fax: +66 53 945426. E-mail address: [email protected] (M. Srisurapanont). 0278-5846/$ – see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.pnpbp.2011.01.014 Contents lists available at ScienceDirect Progress in Neuro-Psychopharmacology & Biological Psychiatry journal homepage: www.elsevier.com/locate/pnp

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Progress in Neuro-Psychopharmacology & Biological Psychiatry 35 (2011) 959–964
Contents lists available at ScienceDirect
Progress in Neuro-Psychopharmacology & BiologicalPsychiatry
j ourna l homepage: www.e lsev ie r.com/ locate /pnp
Comparisons of methamphetamine psychotic and schizophrenicsymptoms: A differential item functioning analysis
Manit Srisurapanont a,⁎, Suwanna Arunpongpaisal b, Kiyoshi Wada c, John Marsden d,Robert Ali e, Ronnachai Kongsakon f
a Department of Psychiatry, Chiang Mai University, Chiang Mai, Thailandb Department of Psychiatry, Khon Kaen University, Khon Kaen, Thailandc Division of Drug Dependence Research, National Institute of Mental Health, Chiba-ken, Japand National Addiction Centre, Institute of Psychiatry, University of London, London, UKe Department of Clinical and Experimental Pharmacology, University of Adelaide, Adelaide, Australiaf Department of Psychiatry, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Abbreviations: CFA, confirmatory factor analysis; DIFEFA, exploratory factor analysis; IRT, item response thRLAI-Thai, Risperidone Long-Acting Injection in Thai SMAIP, WHO Multi-Site Project on Methamphetamine-In⁎ Corresponding author at: Department of Psychiatr
Mai University, Muang, Chiang Mai 50200, Thailand. Tel945426.
E-mail address: [email protected] (M. Srisurapano
0278-5846/$ – see front matter © 2011 Elsevier Inc. Aldoi:10.1016/j.pnpbp.2011.01.014
a b s t r a c t
a r t i c l e i n f oArticle history:Received 15 November 2010Received in revised form 2 January 2011Accepted 15 January 2011Available online 26 January 2011
Keywords:Differential item functioningMethamphetaminePsychosisSchizophreniaSymptom
The concept of negative symptoms in methamphetamine (MA) psychosis (e.g., poverty of speech, flattenaffect, and loss of drive) is still uncertain. This study aimed to use differential item functioning (DIF) statisticaltechniques to differentiate the severity of psychotic symptoms between MA psychotic and schizophrenicpatients. Data of MA psychotic and schizophrenic patients were those of the participants in the WHO Multi-Site Project onMethamphetamine-Induced Psychosis (orWHO-MAIP study) and the Risperidone Long-ActingInjection in Thai Schizophrenic Patients (or RLAI-Thai study), respectively. To confirm the unidimensionalityof psychotic syndromes, we applied the exploratory and confirmatory factor analyses (EFA and CFA) on theeight items of Manchester scale. We conducted the DIF analysis of psychotic symptoms observed in bothgroups by using nonparametric kernel-smoothing techniques of item response theory. A DIF composite indexof 0.30 or greater indicated the difference of symptom severity. The analyses included the data of 168 MApsychotic participants and the baseline data of 169 schizophrenic patients. For both data sets, the EFA and CFAsuggested a three-factor model of the psychotic symptoms, including negative syndrome (poverty of speech,psychomotor retardation and flatten/incongruous affect), positive syndrome (delusions, hallucinations andincoherent speech) and anxiety/depression syndrome (anxiety and depression). The DIF composite indexescomparing the severity differences of all eight psychotic symptoms were lower than 0.3. The results suggestthat, at the same level of syndrome severity (i.e., negative, positive, and anxiety/depression syndromes), theseverity of psychotic symptoms, including the negative ones, observed in MA psychotic and schizophrenicpatients are almost the same.
, differential item functioning;eory; MA, methamphetamine;chizophrenic Patients; WHO-duced Psychosis.y, Faculty of Medicine, Chiang.: +66 53 945422; fax: +66 53
nt).
l rights reserved.
© 2011 Elsevier Inc. All rights reserved.
1. Introduction
Methamphetamine (MA) psychosis is a state of MA intoxicationwith psychotic symptoms, commonly presented with delusions andhallucinations. This psychotic condition has been considered as acommon and serious consequence of chronic, high dose, and/orcontinuous use of MA (Griffith et al., 1972). It is commonly describedas closely simulating paranoid schizophrenia (Bell, 1965).
The similarities in many aspects of MA psychosis and schizophre-nia have made amphetamine a primary psychotomimetic modelagent in schizophrenia research. It is likely that the resemblance iscaused by the altered function of mesolimbic dopamine systems andprefrontal cortical function (Robinson and Becker, 1986).
Although clinical research is necessary for the development of MApsychosis services, few studies in this area have been carried out. Ofmany respects, symptom studies may be a priority area because theseresults are basic knowledge for further studies of MA psychosis, e.g.,etiology, course, prognosis, and treatment. So far, most of the findingson the resemblance between MA psychosis and schizophrenia havemainly focused on positive psychotic symptoms, in particulardelusions and hallucinations.
The concept of negative symptoms in MA psychosis (e.g., povertyof speech, flatten affect, and loss of drive) is not new but stilluncertain. Blunted affect and diminished spontaneity accompaniedwith paranoid-hallucinatory state were described in 1960s (Yui et al.,

960 M. Srisurapanont et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry 35 (2011) 959–964
2000). In a study of 11 MA psychotic inpatients assessed by using theScale for the Assessment of Negative Symptoms, Japanese investiga-tors found that most patients showed a significant impairment onavolition-apathy, anhedonia-asociality, and attentional impairment(Tomiyama, 1990). Srisurapanont et al. (2003) found negativepsychotic symptoms in 21.4% of 168 MA psychotic patients withvarious ethnicity (Srisurapanont et al., 2003) In this later study, theresults of an exploratory factor analysis (EFA) also showed anindependent syndrome of negative symptoms with a variance of26.6%. Despite the above-mentioned evidence, negative symptoms ofMA psychosis are still viewed as less severe and/or prevalent (Zoricket al., 2008).
Differential item functioning (DIF) statistical techniques are basedon the principle that if different groups of patients (e.g., males vs.females) have the same level of disease severity (e.g., depression,psychosis), they should be rated or response similarly on an individualrating item of a measure, regardless of group membership. DIFassessment proceeds by controlling for an estimate of the underlyingconstruct and then examining whether individuals in different groupshave a similar distribution of responses to a particular item. Thestatistical techniques that directly compare item severity betweengroups are inferior to DIF analyses by the fact that the difference foundby a direct comparison may not be a true phenomenologicaldifference. It may be just reflective of greater overall symptomseverity in one group versus another. In contrast, the existence of DIFbetween different groups on a symptom indicates the real differenceof symptom severity because the overall disease or syndrome severityhas been controlled.
Recently, we have finished two studies: (i) the WHO Multi-SiteProject onMethamphetamine-Induced Psychosis (WHO-MAIP study),a cross-sectional observation study aiming to evaluate MA psychosis(Ali et al., 2006, Ali et al., 2010, Srisurapanont, et al., 2003), and (ii)Risperidone Long-Acting Injection in Thai Schizophrenic Patients(RLAI-Thai study), a three-month, non-randomized, open-label,single-arm study of risperidone long-acting injection in Thai indivi-duals with schizophrenia (Arunpongpaisal et al., 2010). The psychoticsymptoms of participants in both studies were assessed using theManchester scale (Krawiecka et al., 1977). Because the symptoms ofthese two studies were comparable, we proposed to apply the DIFstatistical techniques to differentiate the severity of psychoticsymptoms between these populations.
2. Methods
Data of MA psychotic and schizophrenic patients were those of theparticipants in the WHO-MAIP and the RLAI-Thai studies, respective-ly. Both studies were carried out in accordancewith the Code of Ethicsof the World Medical Association (Declaration of Helsinki) forexperiments involving humans. The protocol of each study wasapproved by the Institution Review Board or the Ethic Committeeresponsible for the participating hospital or institution. Writteninformed consent was obtained from each participant after thestudy details had been fully explained.
2.1. Participants
The participants of WHO-MAIP study were MA psychotic patientsadmitted inmany hospitals located in Australia, Japan, the Philippines,and Thailand. In addition to the evidence of MA use during the weekprior to the admission, the diagnosis of MA psychosis was confirmedusing the Mini-International Neuropsychiatric Interview-Plus (MINI-Plus), Module M. TheMINI-Plus is a more detailed version of theMINI,a structured clinical interview for the DSM-III-R diagnosis (Sheehanet al., 1998). It includes additional questions to ascertain therelationship between a psychiatric condition and a physical illness
or drug use. These patients were assessed only once within 3–7 daysafter the admission.
The participants of RLAI-Thai study were Thai inpatients andoutpatients with DSM-IV schizophrenia, who did not fully respond orcould not tolerate their antipsychotic medications. They were willingto switch their previous antipsychotic medications to 25, 37.5, or50 mg of RLAI given by intramuscular injection. Exclusion criteriaincluded (i) serious unstable medical condition, including recent andpresent clinically relevant laboratory abnormalities; (ii) history ofalcohol dependence or drug abuse (except nicotine) within 3 monthsof entry into the trial, (iii) on clozapine during the last 3 months; (iv)history or current symptoms of tardive dyskinesia; (v) history ofneuroleptic malignant syndrome; (vi) pregnant or breast-feedingfemale; (vii) female patient of childbearing potential withoutadequate contraception; (viii) participation in an investigationaldrug trial in the 30 days prior to selection; and (ix) knownintolerance/non-responder to risperidone. Other psychiatric comor-bidity was not assessed. Therefore, the patients with comorbidity ofother psychiatric illnesses were allowed to participate in this study.Participants were assessed prior to RLAI administration (baseline) andthen again after 3 months and 6 months of monthly RLAI treatment.Because the psychotic symptoms at baseline were the most severeones, the data at this time point were applied in this study.
2.2. Measures
In WHO-MAIP study, the participants' psychotic symptoms wereassessed using the Manchester scale. This 5-point scale (0=absent,1=mild, 2=moderate, 3=marked and 4=severe) assesses eightpsychiatric symptoms commonly found in psychotic patients,including depression, anxiety, delusions, hallucinations, incoherencespeech, poverty of speech, flatten/incongruous affect, and psycho-motor retardation. For each item of the scale, its inter-rater reliability(Kandall's coefficient of concordance W) is between 0.6 and 0.9(Krawiecka, et al., 1977). Its concurrent validity has been tested withthe Schedules for the Assessment of Positive Symptoms (SAPS)(Andreasen, 1984) and the Schedules for the Assessment of NegativeSymptoms (SANS) (Andreasen, 1983). While the Manchester scaleitems of delusions, hallucinations, and incoherence are significantlycorrelated with the total SAPS score (r's=0.53–0.64), its items ofpoverty of speech, affect flattening, and psychomotor retardation arealso significantly correlated with the total SANS score (r's=0.62–0.85)(Jackson et al., 1990). Except disorganized and catatonic behavior, theManchester scale covers all DSM-IV schizophrenic symptoms andproposed remission criteria for schizophrenia (American PsychiatricAssociation, 2000, Andreasen et al., 2005).
The modified version of Manchester scale was applied in the RLAI-Thai study. As used in an antipsychotic trial (Johnstone et al., 1978),the item of flatten/incongruous affect was separated into two items offlatten and incongruous affects. To make the scores of these two itemscomparable to the single one of flatten/incongruous affect in theWHO-MAIP study, the highest score of these two items in eachparticipant was used as the representative of flatten/incongruousaffect item.
The different versions of Manchester scale used in both studieswere caused by the decision of each investigator team. Both versionswere administered by certified psychiatrists, who were well-trainedon the use of Manchester scale.
2.3. Data analyses
2.3.1. UnidimensionalityThe DIF is typically examined on the basis that the set of items is
intended to measure a single underlying construct (i.e., the uni-dimension of items). An examination of the underlying dimension ofan item set is therefore the first step in DIF detection. More

Table 1Comparisons of demographic data and severity of symptoms between 168 methamphetamine psychotic patients and 169 schizophrenic patients.a
Methamphetamine psychotic patients (n=168) Schizophrenic patients (n=169) Significant differencea
n n
Sex (male,%) 127 (75.6%) 114 (67.5%) χ2=2.74, df=1, p=0.12Mean (SD) Mean (SD) Mean (SD)
Age 27.1 (7.6) 29.8 (14.0) t=2.20, p=0.03Age at first onset of psychotic symptoms 25.0 (9.1) 23.2 (8.4) t=1.89, p=0.06Total Manchester scale score 10.7 (4.9) 8.0 (5.5) Z=−4.77, pb0.01Negative syndrome 2.7 (2.3) 2.9 (2.5) Z=−0.54, p=0.59
Poverty of speech 0.7 (0.9) 0.7 (0.9) Z=−0.18, p=0.86Psychomotor retardation 0.8 (0.8) 0.9 (1.0) Z=−0.40, p=0.69Flatten/incongruouse affect 1.2 (1.0) 1.3 (1.0) Z=−1.36, p=0.17
Positive syndrome 5.3 (2.9) 3.7 (3.0) Z=−4.86, pb0.01Delusions 2.1 (1.2) 1.4 (1.3) Z=−5.10, pb0.01Hallucinations 2.0 (1.4) 1.4 (1.3) Z=−4.03, pb0.01Incoherence speech 1.1 (1.1) 0.9 (1.0) Z=−2.11, p=0.04
Anxiety/depression syndrome 2.8 (1.7) 1.5 (1.7) Z=−6.89, pb0.01Depression 1.1 (1.0) 0.5 (0.8) Z=−6.33, pb0.01Anxiety 1.7 (1.0) 1.0 (1.1) Z=−5.70, pb0.01
a Except a Chi-square test for sex and a Student's t test for age items, Mann–Whitney U tests were used for all comparisons.
961M. Srisurapanont et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry 35 (2011) 959–964
specifically, ones should examine dimensionality separately for eachgroup (i.e., MP or schizophrenic group in the present analyses) bydetermining if the same number of factors is found in each group(Teresi and Fleishman, 2007). In addition, confirmatory factor analysis(CFA) should be applied to test the single-factor model fit of each itemset.
The EFA on the eight items of Manchester scale scores obtainedfrom the MA psychotic group was completed in our previous study(Srisurapanont et al., 2003). The same methods were applied on thescores obtained from schizophrenic patients. All eight items weresubjected to principal-component analysis for identifying the distinctfactors. Eigenvalue one test was used to keep or discard factors.Finally, varimax rotation was performed to elicit the factor compo-nents. The EFA was examined by using the SPSS 17.0. After thecombination of both data sets, each factor found on the EFA wasfurther confirmed by using the chi-square test of a single-factor modelperformed by the AMOS 18.0.
2.3.2. DIF analysesWe employed the nonparametric kernel-smoothing techniques of
item response theory (IRT) implemented in the software (TestGraf)developed by Ramsay (1991, 2001). The strengths of these techniquesare that non-parametric IRT models do not require complex
Table 2Exploratory factor analysis of eight-item Manchester scale in 168 methamphetamine psych
Methamphetamine psychotic patients (n=1
Factor 1 Factor 2
Negative syndromePoverty of speech 0.86 0.07Psychomotor retardation 0.83 0.04Flatten/incongruous affect 0.75 0.28
Positive syndromeDelusions 0.08 0.82Hallucinations 0.07 0.79Incoherent speech 0.32 0.67
Anxiety/depression syndromeDepression 0.19 -0.11Anxiety 0.05 0.27
Eigenvalue 2.13 1.92Per cent variance 26.64 23.95
a (Srisurapanont et al., 2003, reprinted with permission).
estimation procedures, can be applied to relatively small data sets,are less imposing concerning distributional form of item responsefunctions, and help to avoid misleading results obtained fromparametric IRT models. In the present analyses, we determined theitem response functions directly from the data without forcing thedata to conform to a logistic IRT model.
TestGraf analyzes the severity of symptoms observed in theparticipants of both groups. A response characteristic curve showshow the item score varies as a function of what the test is designed tomeasure, that is, its latent trait (i.e., severity of each syndrome in thepresent analyses). To examine DIF, this software calculates a weightedaverage of the squared difference between the focal group'sprobability of endorsing an item and the reference group's probabilityof endorsing an item. Thus, a composite index of DIF is obtained afterthe comparison of response characteristic curves.
For each item, there are two curves of both groups beingcompared. The curves are numbered in the order in which the filesof each group have been selected. The first group is called the focalgroup (i.e., MA psychotic patients), and the other group is called areference group (i.e., schizophrenic patients). For each focal group, asummary measure of how far the curve this group is from that of thereference group is calculated. The extent to which the curves differ iscalled differential item functioning (DIF). If this measure is
otic and 169 schizophrenic patients.
68)a Schizophrenic patients (n=169)
Factor 3 Factor 1 Factor 2 Factor 3
0.02 0.89 -0.17 0.100.25 0.88 0.23 -0.010.03 0.75 0.20 0.39
0.13 -0.01 0.56 0.730.17 0.07 0.32 0.79-0.29 0.33 -2.16 0.77
0.85 0.10 0.85 0.080.76 0.19 0.85 0.14
1.51 2.27 2.00 1.9418.81 28.35 24.93 24.24
A
B
C
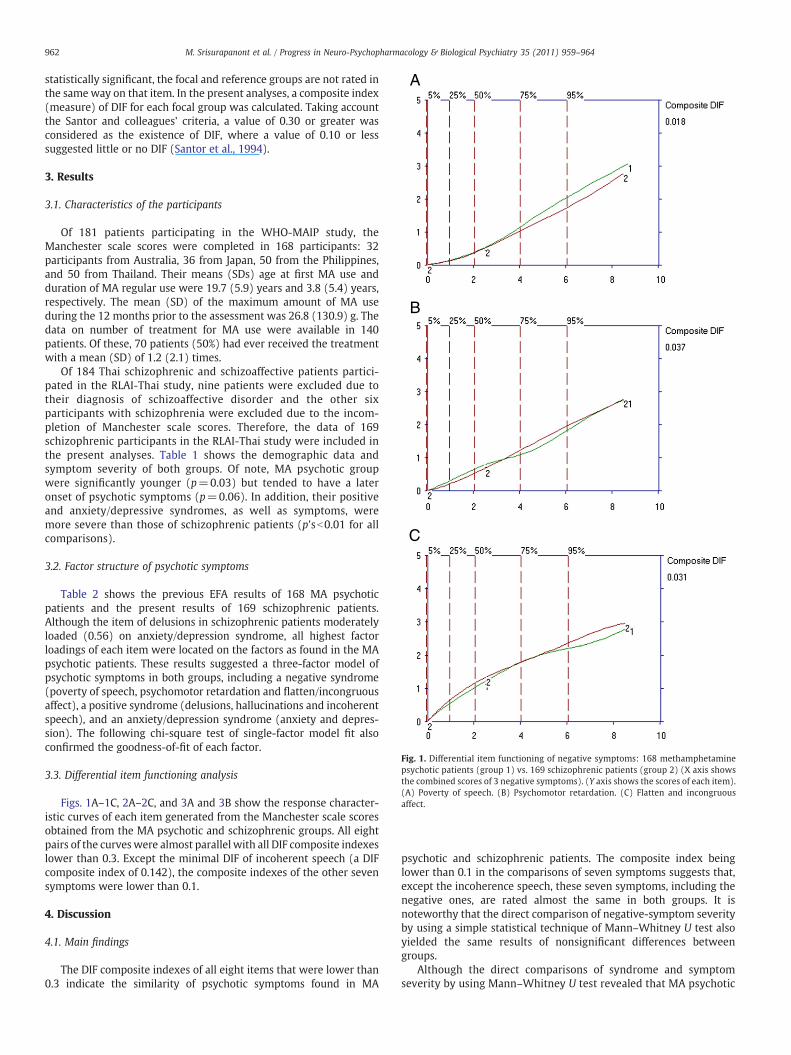
Fig. 1. Differential item functioning of negative symptoms: 168 methamphetaminepsychotic patients (group 1) vs. 169 schizophrenic patients (group 2) (X axis showsthe combined scores of 3 negative symptoms). (Y axis shows the scores of each item).(A) Poverty of speech. (B) Psychomotor retardation. (C) Flatten and incongruousaffect.
962 M. Srisurapanont et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry 35 (2011) 959–964
statistically significant, the focal and reference groups are not rated inthe same way on that item. In the present analyses, a composite index(measure) of DIF for each focal group was calculated. Taking accountthe Santor and colleagues' criteria, a value of 0.30 or greater wasconsidered as the existence of DIF, where a value of 0.10 or lesssuggested little or no DIF (Santor et al., 1994).
3. Results
3.1. Characteristics of the participants
Of 181 patients participating in the WHO-MAIP study, theManchester scale scores were completed in 168 participants: 32participants from Australia, 36 from Japan, 50 from the Philippines,and 50 from Thailand. Their means (SDs) age at first MA use andduration of MA regular use were 19.7 (5.9) years and 3.8 (5.4) years,respectively. The mean (SD) of the maximum amount of MA useduring the 12 months prior to the assessment was 26.8 (130.9) g. Thedata on number of treatment for MA use were available in 140patients. Of these, 70 patients (50%) had ever received the treatmentwith a mean (SD) of 1.2 (2.1) times.
Of 184 Thai schizophrenic and schizoaffective patients partici-pated in the RLAI-Thai study, nine patients were excluded due totheir diagnosis of schizoaffective disorder and the other sixparticipants with schizophrenia were excluded due to the incom-pletion of Manchester scale scores. Therefore, the data of 169schizophrenic participants in the RLAI-Thai study were included inthe present analyses. Table 1 shows the demographic data andsymptom severity of both groups. Of note, MA psychotic groupwere significantly younger (p=0.03) but tended to have a lateronset of psychotic symptoms (p=0.06). In addition, their positiveand anxiety/depressive syndromes, as well as symptoms, weremore severe than those of schizophrenic patients (p'sb0.01 for allcomparisons).
3.2. Factor structure of psychotic symptoms
Table 2 shows the previous EFA results of 168 MA psychoticpatients and the present results of 169 schizophrenic patients.Although the item of delusions in schizophrenic patients moderatelyloaded (0.56) on anxiety/depression syndrome, all highest factorloadings of each item were located on the factors as found in the MApsychotic patients. These results suggested a three-factor model ofpsychotic symptoms in both groups, including a negative syndrome(poverty of speech, psychomotor retardation and flatten/incongruousaffect), a positive syndrome (delusions, hallucinations and incoherentspeech), and an anxiety/depression syndrome (anxiety and depres-sion). The following chi-square test of single-factor model fit alsoconfirmed the goodness-of-fit of each factor.
3.3. Differential item functioning analysis
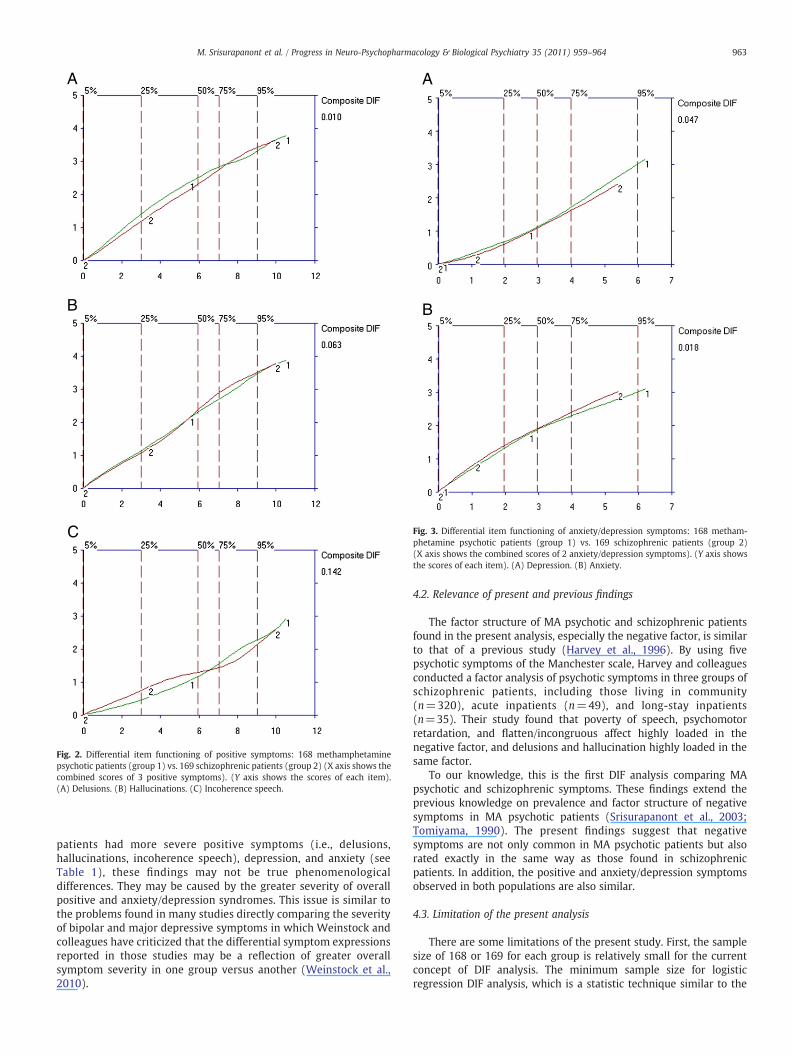
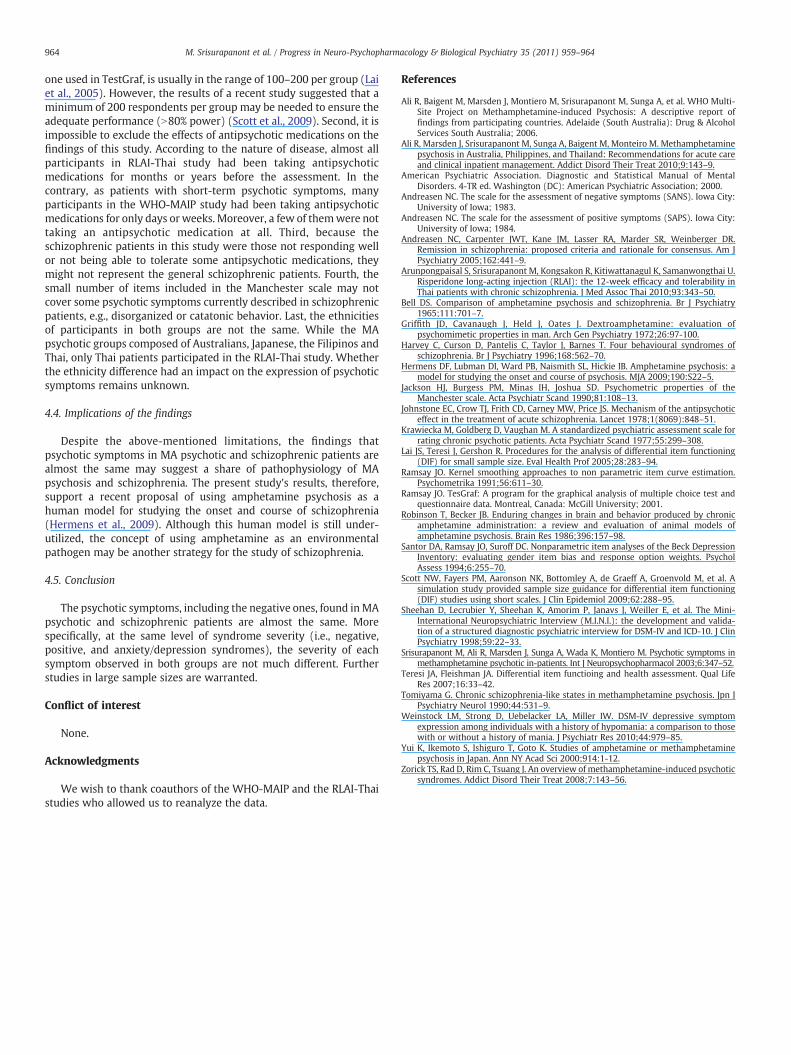
Figs. 1A–1C, 2A–2C, and 3A and 3B show the response character-istic curves of each item generated from the Manchester scale scoresobtained from the MA psychotic and schizophrenic groups. All eightpairs of the curveswere almost parallel with all DIF composite indexeslower than 0.3. Except the minimal DIF of incoherent speech (a DIFcomposite index of 0.142), the composite indexes of the other sevensymptoms were lower than 0.1.
4. Discussion
4.1. Main findings
The DIF composite indexes of all eight items that were lower than0.3 indicate the similarity of psychotic symptoms found in MA
psychotic and schizophrenic patients. The composite index beinglower than 0.1 in the comparisons of seven symptoms suggests that,except the incoherence speech, these seven symptoms, including thenegative ones, are rated almost the same in both groups. It isnoteworthy that the direct comparison of negative-symptom severityby using a simple statistical technique of Mann–Whitney U test alsoyielded the same results of nonsignificant differences betweengroups.
Although the direct comparisons of syndrome and symptomseverity by using Mann–Whitney U test revealed that MA psychotic
A
B
C
Fig. 2. Differential item functioning of positive symptoms: 168 methamphetaminepsychotic patients (group 1) vs. 169 schizophrenic patients (group 2) (X axis shows thecombined scores of 3 positive symptoms). (Y axis shows the scores of each item).(A) Delusions. (B) Hallucinations. (C) Incoherence speech.
A
B
Fig. 3. Differential item functioning of anxiety/depression symptoms: 168 metham-phetamine psychotic patients (group 1) vs. 169 schizophrenic patients (group 2)(X axis shows the combined scores of 2 anxiety/depression symptoms). (Y axis showsthe scores of each item). (A) Depression. (B) Anxiety.
963M. Srisurapanont et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry 35 (2011) 959–964
patients had more severe positive symptoms (i.e., delusions,hallucinations, incoherence speech), depression, and anxiety (seeTable 1), these findings may not be true phenomenologicaldifferences. They may be caused by the greater severity of overallpositive and anxiety/depression syndromes. This issue is similar tothe problems found in many studies directly comparing the severityof bipolar and major depressive symptoms in which Weinstock andcolleagues have criticized that the differential symptom expressionsreported in those studies may be a reflection of greater overallsymptom severity in one group versus another (Weinstock et al.,2010).
4.2. Relevance of present and previous findings
The factor structure of MA psychotic and schizophrenic patientsfound in the present analysis, especially the negative factor, is similarto that of a previous study (Harvey et al., 1996). By using fivepsychotic symptoms of the Manchester scale, Harvey and colleaguesconducted a factor analysis of psychotic symptoms in three groups ofschizophrenic patients, including those living in community(n=320), acute inpatients (n=49), and long-stay inpatients(n=35). Their study found that poverty of speech, psychomotorretardation, and flatten/incongruous affect highly loaded in thenegative factor, and delusions and hallucination highly loaded in thesame factor.
To our knowledge, this is the first DIF analysis comparing MApsychotic and schizophrenic symptoms. These findings extend theprevious knowledge on prevalence and factor structure of negativesymptoms in MA psychotic patients (Srisurapanont et al., 2003;Tomiyama, 1990). The present findings suggest that negativesymptoms are not only common in MA psychotic patients but alsorated exactly in the same way as those found in schizophrenicpatients. In addition, the positive and anxiety/depression symptomsobserved in both populations are also similar.
4.3. Limitation of the present analysis
There are some limitations of the present study. First, the samplesize of 168 or 169 for each group is relatively small for the currentconcept of DIF analysis. The minimum sample size for logisticregression DIF analysis, which is a statistic technique similar to the
964 M. Srisurapanont et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry 35 (2011) 959–964
one used in TestGraf, is usually in the range of 100–200 per group (Laiet al., 2005). However, the results of a recent study suggested that aminimum of 200 respondents per group may be needed to ensure theadequate performance (N80% power) (Scott et al., 2009). Second, it isimpossible to exclude the effects of antipsychotic medications on thefindings of this study. According to the nature of disease, almost allparticipants in RLAI-Thai study had been taking antipsychoticmedications for months or years before the assessment. In thecontrary, as patients with short-term psychotic symptoms, manyparticipants in the WHO-MAIP study had been taking antipsychoticmedications for only days or weeks. Moreover, a few of themwere nottaking an antipsychotic medication at all. Third, because theschizophrenic patients in this study were those not responding wellor not being able to tolerate some antipsychotic medications, theymight not represent the general schizophrenic patients. Fourth, thesmall number of items included in the Manchester scale may notcover some psychotic symptoms currently described in schizophrenicpatients, e.g., disorganized or catatonic behavior. Last, the ethnicitiesof participants in both groups are not the same. While the MApsychotic groups composed of Australians, Japanese, the Filipinos andThai, only Thai patients participated in the RLAI-Thai study. Whetherthe ethnicity difference had an impact on the expression of psychoticsymptoms remains unknown.
4.4. Implications of the findings
Despite the above-mentioned limitations, the findings thatpsychotic symptoms in MA psychotic and schizophrenic patients arealmost the same may suggest a share of pathophysiology of MApsychosis and schizophrenia. The present study's results, therefore,support a recent proposal of using amphetamine psychosis as ahuman model for studying the onset and course of schizophrenia(Hermens et al., 2009). Although this human model is still under-utilized, the concept of using amphetamine as an environmentalpathogen may be another strategy for the study of schizophrenia.
4.5. Conclusion
The psychotic symptoms, including the negative ones, found inMApsychotic and schizophrenic patients are almost the same. Morespecifically, at the same level of syndrome severity (i.e., negative,positive, and anxiety/depression syndromes), the severity of eachsymptom observed in both groups are not much different. Furtherstudies in large sample sizes are warranted.
Conflict of interest
None.
Acknowledgments
We wish to thank coauthors of the WHO-MAIP and the RLAI-Thaistudies who allowed us to reanalyze the data.
References
Ali R, Baigent M, Marsden J, Montiero M, Srisurapanont M, Sunga A, et al. WHO Multi-Site Project on Methamphetamine-induced Psychosis: A descriptive report offindings from participating countries. Adelaide (South Australia): Drug & AlcoholServices South Australia; 2006.
Ali R, Marsden J, Srisurapanont M, Sunga A, Baigent M, Monteiro M. Methamphetaminepsychosis in Australia, Philippines, and Thailand: Recommendations for acute careand clinical inpatient management. Addict Disord Their Treat 2010;9:143–9.
American Psychiatric Association. Diagnostic and Statistical Manual of MentalDisorders. 4-TR ed. Washington (DC): American Psychiatric Association; 2000.
Andreasen NC. The scale for the assessment of negative symptoms (SANS). Iowa City:University of Iowa; 1983.
Andreasen NC. The scale for the assessment of positive symptoms (SAPS). Iowa City:University of Iowa; 1984.
Andreasen NC, Carpenter JWT, Kane JM, Lasser RA, Marder SR, Weinberger DR.Remission in schizophrenia: proposed criteria and rationale for consensus. Am JPsychiatry 2005;162:441–9.
Arunpongpaisal S, Srisurapanont M, Kongsakon R, Kitiwattanagul K, Samanwongthai U.Risperidone long-acting injection (RLAI): the 12-week efficacy and tolerability inThai patients with chronic schizophrenia. J Med Assoc Thai 2010;93:343–50.
Bell DS. Comparison of amphetamine psychosis and schizophrenia. Br J Psychiatry1965;111:701–7.
Griffith JD, Cavanaugh J, Held J, Oates J. Dextroamphetamine: evaluation ofpsychomimetic properties in man. Arch Gen Psychiatry 1972;26:97-100.
Harvey C, Curson D, Pantelis C, Taylor J, Barnes T. Four behavioural syndromes ofschizophrenia. Br J Psychiatry 1996;168:562–70.
Hermens DF, Lubman DI, Ward PB, Naismith SL, Hickie IB. Amphetamine psychosis: amodel for studying the onset and course of psychosis. MJA 2009;190:S22–5.
Jackson HJ, Burgess PM, Minas IH, Joshua SD. Psychometric properties of theManchester scale. Acta Psychiatr Scand 1990;81:108–13.
Johnstone EC, Crow TJ, Frith CD, Carney MW, Price JS. Mechanism of the antipsychoticeffect in the treatment of acute schizophrenia. Lancet 1978;1(8069):848–51.
Krawiecka M, Goldberg D, Vaughan M. A standardized psychiatric assessment scale forrating chronic psychotic patients. Acta Psychiatr Scand 1977;55:299–308.
Lai JS, Teresi J, Gershon R. Procedures for the analysis of differential item functioning(DIF) for small sample size. Eval Health Prof 2005;28:283–94.
Ramsay JO. Kernel smoothing approaches to non parametric item curve estimation.Psychometrika 1991;56:611–30.
Ramsay JO. TesGraf: A program for the graphical analysis of multiple choice test andquestionnaire data. Montreal, Canada: McGill University; 2001.
Robinson T, Becker JB. Enduring changes in brain and behavior produced by chronicamphetamine administration: a review and evaluation of animal models ofamphetamine psychosis. Brain Res 1986;396:157–98.
Santor DA, Ramsay JO, Suroff DC. Nonparametric item analyses of the Beck DepressionInventory: evaluating gender item bias and response option weights. PsycholAssess 1994;6:255–70.
Scott NW, Fayers PM, Aaronson NK, Bottomley A, de Graeff A, Groenvold M, et al. Asimulation study provided sample size guidance for differential item functioning(DIF) studies using short scales. J Clin Epidemiol 2009;62:288–95.
Sheehan D, Lecrubier Y, Sheehan K, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and valida-tion of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J ClinPsychiatry 1998;59:22–33.
Srisurapanont M, Ali R, Marsden J, Sunga A, Wada K, Montiero M. Psychotic symptoms inmethamphetamine psychotic in-patients. Int J Neuropsychopharmacol 2003;6:347–52.
Teresi JA, Fleishman JA. Differential item functioing and health assessment. Qual LifeRes 2007;16:33–42.
Tomiyama G. Chronic schizophrenia-like states in methamphetamine psychosis. Jpn JPsychiatry Neurol 1990;44:531–9.
Weinstock LM, Strong D, Uebelacker LA, Miller IW. DSM-IV depressive symptomexpression among individuals with a history of hypomania: a comparison to thosewith or without a history of mania. J Psychiatr Res 2010;44:979–85.
Yui K, Ikemoto S, Ishiguro T, Goto K. Studies of amphetamine or methamphetaminepsychosis in Japan. Ann NY Acad Sci 2000;914:1-12.
Zorick TS, Rad D, Rim C, Tsuang J. An overview of methamphetamine-induced psychoticsyndromes. Addict Disord Their Treat 2008;7:143–56.
Related Documents











