Comparison of distinctive gait variables using two different biomechanical models for knee joint kinematics in subjects with knee osteoarthritis and healthy controls Inga Krauss a, ⁎, Renate List b , Pia Janssen a , Stefan Grau a , Thomas Horstmann a, c , Alex Stacoff b a Medical Clinic, Department of Sports medicine, University of Tuebingen, Germany b Swiss Federal Institute of Technology Zurich, Institute for Biomechanics, Switzerland c Medical Park Bad Wiessee GmbH & Co., Germany abstract article info Article history: Received 26 July 2011 Accepted 28 September 2011 Keywords: Instrumented gait analysis Anatomical coordinate system Angular decomposition Knee joint kinematics Osteoarthritis Background: Gait analysis is an important instrument in clinical research and results should be objective. The purpose of this study was to quantify clinical outcomes of two biomechanical models with different anatom- ical coordinate systems and angle decomposition strategies for knee joint kinematics. Methods: The study was designed to compare a functional approach and a predictive approach with a single comprehensive marker set. 10 healthy subjects and 12 subjects with knee osteoarthritis were analysed. Distinctive gait variables were averaged across five trials. Agreement between methods was illustrated with the so-called levels of agreement. Differences between models were quantified using a paired t-test or Wilcoxon-Signed Rank test in case of non-normality (Shapiro–Wilk test). Unpaired t-tests/Wilcoxon tests were used to compare gait variables between healthy subjects and subjects with knee osteoarthritis, and to examine whether statistical analysis of this comparison would yield different data interpretations when using different models. Findings: Outcome variables differed between the functional and predictive approaches in the sagittal plane (0.1–3.1°), and transverse plane (1.0–3.7°). With respect to the range of motion in the given movement plane, variables in the sagittal plane of the knee were more consistent between methods. The functional approach was more sensitive for detecting differences between groups for sagittal plane kinematics. Statisti- cal analysis for transverse plane kinematics differed substantially between models. Interpretation: Sensitivity to detect differences of kinematic data between population groups can vary be- tween biomechanical models. Rotational gait variables are inconsistent between models and should not be used as clinical outcome variables in daily routine. © 2011 Elsevier Ltd. All rights reserved. 1. Introduction Gait analysis is an important instrument in various fields of clinical research and its protocols are intended to make kinematics interpret- able for clinicians (Ferrari et al., 2008). In subjects with knee or hip osteoarthritis, deficits with regard to strength, postural control and bodily pain can influence gait stability, which cannot be adequately described with disease specific questionnaires such as the WOMAC score alone (Lindemann et al., 2006). Clinical gait analysis is often used to describe pathologic gait patterns or to quantify the efficacy of a therapeutic intervention. In this respect, spatio-temporal vari- ables and gait parameters, such as ranges of motion, and joint excur- sions, are used (Al-Zahrani and Bakheit, 2002; Astephen et al., 2008; Brandes et al., 2008; Maly et al., 2006; Mundermann et al., 2005; Schmitt et al., 2006; Weidow et al., 2006; Yavuzer et al., 2005). Objectivity of gait analysis is a prerequisite to guarantee high quality in research and clinical practice. Attempts have been made to standardise procedures for instrumented gait analysis (Wu et al., 2002); however, there is still a variety of different approaches being used in clinical research. Protocols differ in the underlying biome- chanical model, associated marker-sets, and data recording and processing. The former defines properties of the modelled joints, the number of involved segments, the definitions of joint centres and axes, the used anatomical and technical reference frames, and the angular decomposition technique to calculate joint angles. Despite apparent differences of the outcome measures derived from different gait protocols, data of different studies are compared and interpreted (i.e. Ryu et al., 2006). Several comparisons of gait protocols have already been described in previous studies. Ferrari et al. (2008) compared five current proto- cols in gait analysis along the gait cycle. Movements in the sagittal plane showed good correlation and a small bias between protocols. Out-of-sagittal plane rotations revealed worse correlations. One sub- ject with a prosthesis restraining any movement in the coronal plane showed joint ranges of up to 35° for one protocol. Although this work Clinical Biomechanics 27 (2012) 281–286 ⁎ Corresponding author at: Medical Clinic, Department of Sports Medicine, University of Tuebingen, Silcherstr. 5, 72076 Tuebingen, Germany. E-mail address: [email protected] (I. Krauss). 0268-0033/$ – see front matter © 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.clinbiomech.2011.09.013 Contents lists available at SciVerse ScienceDirect Clinical Biomechanics journal homepage: www.elsevier.com/locate/clinbiomech

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Biomechanics 27 (2012) 281–286
Contents lists available at SciVerse ScienceDirect
Clinical Biomechanics
j ourna l homepage: www.e lsev ie r .com/ locate /c l inb iomech
Comparison of distinctive gait variables using two different biomechanical models forknee joint kinematics in subjects with knee osteoarthritis and healthy controls
Inga Krauss a,⁎, Renate List b, Pia Janssen a, Stefan Grau a, Thomas Horstmann a,c, Alex Stacoff b
a Medical Clinic, Department of Sports medicine, University of Tuebingen, Germanyb Swiss Federal Institute of Technology Zurich, Institute for Biomechanics, Switzerlandc Medical Park Bad Wiessee GmbH & Co., Germany
⁎ Corresponding author at:Medical Clinic, Departmenof Tuebingen, Silcherstr. 5, 72076 Tuebingen, Germany.
E-mail address: [email protected] (
0268-0033/$ – see front matter © 2011 Elsevier Ltd. Alldoi:10.1016/j.clinbiomech.2011.09.013
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 26 July 2011Accepted 28 September 2011Keywords:Instrumented gait analysisAnatomical coordinate systemAngular decompositionKnee joint kinematicsOsteoarthritis
Background: Gait analysis is an important instrument in clinical research and results should be objective. Thepurpose of this study was to quantify clinical outcomes of two biomechanical models with different anatom-ical coordinate systems and angle decomposition strategies for knee joint kinematics.Methods: The study was designed to compare a functional approach and a predictive approach with a singlecomprehensive marker set. 10 healthy subjects and 12 subjects with knee osteoarthritis were analysed.Distinctive gait variables were averaged across five trials. Agreement between methods was illustratedwith the so-called levels of agreement. Differences between models were quantified using a paired t-testor Wilcoxon-Signed Rank test in case of non-normality (Shapiro–Wilk test). Unpaired t-tests/Wilcoxontests were used to compare gait variables between healthy subjects and subjects with knee osteoarthritis,
and to examine whether statistical analysis of this comparison would yield different data interpretationswhen using different models.Findings: Outcome variables differed between the functional and predictive approaches in the sagittal plane(0.1–3.1°), and transverse plane (1.0–3.7°). With respect to the range of motion in the given movementplane, variables in the sagittal plane of the knee were more consistent between methods. The functionalapproach was more sensitive for detecting differences between groups for sagittal plane kinematics. Statisti-cal analysis for transverse plane kinematics differed substantially between models.Interpretation: Sensitivity to detect differences of kinematic data between population groups can vary be-tween biomechanical models. Rotational gait variables are inconsistent between models and should not beused as clinical outcome variables in daily routine.© 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Gait analysis is an important instrument in various fields of clinicalresearch and its protocols are intended to make kinematics interpret-able for clinicians (Ferrari et al., 2008). In subjects with knee or hiposteoarthritis, deficits with regard to strength, postural control andbodily pain can influence gait stability, which cannot be adequatelydescribed with disease specific questionnaires such as the WOMACscore alone (Lindemann et al., 2006). Clinical gait analysis is oftenused to describe pathologic gait patterns or to quantify the efficacyof a therapeutic intervention. In this respect, spatio-temporal vari-ables and gait parameters, such as ranges of motion, and joint excur-sions, are used (Al-Zahrani and Bakheit, 2002; Astephen et al., 2008;Brandes et al., 2008; Maly et al., 2006; Mundermann et al., 2005;Schmitt et al., 2006; Weidow et al., 2006; Yavuzer et al., 2005).
t of Sports Medicine, University
I. Krauss).
rights reserved.
Objectivity of gait analysis is a prerequisite to guarantee highquality in research and clinical practice. Attempts have been madeto standardise procedures for instrumented gait analysis (Wu et al.,2002); however, there is still a variety of different approaches beingused in clinical research. Protocols differ in the underlying biome-chanical model, associated marker-sets, and data recording andprocessing. The former defines properties of the modelled joints, thenumber of involved segments, the definitions of joint centres andaxes, the used anatomical and technical reference frames, and theangular decomposition technique to calculate joint angles. Despiteapparent differences of the outcome measures derived from differentgait protocols, data of different studies are compared and interpreted(i.e. Ryu et al., 2006).
Several comparisons of gait protocols have already been describedin previous studies. Ferrari et al. (2008) compared five current proto-cols in gait analysis along the gait cycle. Movements in the sagittalplane showed good correlation and a small bias between protocols.Out-of-sagittal plane rotations revealed worse correlations. One sub-ject with a prosthesis restraining any movement in the coronal planeshowed joint ranges of up to 35° for one protocol. Although this work

282 I. Krauss et al. / Clinical Biomechanics 27 (2012) 281–286
is outstandingwith respect to the choice and number of compared pro-tocols, comparisons are only based on three subjects (Ferrari et al.,2008). Variability of clinical gait analysis conducted in four different lab-oratories was quantified in eleven subjects with spastic cerebral palsy.However, three of the four laboratories used the same protocol andtherefore variability was mainly affected by the different investigators(Noonan et al., 2003). Cappozzo et al. (2005) compared time seriesand angle values during level walking in one subject using differentconcepts to describe relative movements between two bony segments.They reported onlyminor differences for knee flexion/extension angles,but substantial differences for knee abduction/adduction and internal/external rotation angles.
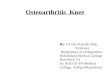
Fig. 1. Location of markers and the joint coordinate systems for the
In summary, previous studies have already focused on differencesbetween gait protocols and biomechanical models. However, conclu-sions are based on results fromvery few subjects or specific populations.Studies mainly quantify variability of angle-time-histories and do notallow a statement on discrete variables, which are important for quan-tifying efficiency of therapeutic interventions or differences betweenhealthy subjects and subjects with knee or hip osteoarthritis. Further-more, differences are not quantified in the unit of interest (degree).
Therefore, the aim of the present study was to compare distinctivegait variables of knee joint kinematics derived from two differentmodelsin subjects with knee osteoarthritis and healthy controls. Protocols varyregarding the anatomical coordinate system, the angular decomposition,
functional approach (FA) and prediction approach (PA) models.

Table 1Marker set and marker abbreviations used to determine the functional approach (FA)and prediction approach (PA) models. * Marker only used to determine hip joint centre(HJC).
Abbreviation Marker name Bilateral FA PA
Joint centresHJC Hip joint centre ● ●KJC Knee joint centre ● ● ●AJC Upper ankle joint centre ● ●
Anatomical markersRTAS Right anterior iliac spine ●*LTAS Left anterior iliac spine ●*MS Medial iliac spine ● ●*PS Posterior iliac spine ● ●*SACR Os sacrum ●*TM Trochanter major ● ●LH Thigh—lateral proximal (high) aspect ● ●LL Thigh—lateral distal (low) aspect ● ●FR Limb—frontal distal aspect ● ●ME Medial epicondyle ● ● ●LE Lateral epicondyle ● ● ●TT Tuberositas tibiae ● ● ●HF Head of the fibula ● ●LF Distal aspect of the fibula ● ●MT Anterior aspect of the bony tibia ● ●MM Medial malleolus ● ● ●ML Lateral malleolus ● ● ●
Table 2Distinctive gait variables.
Location and name Sign of motion direction
Knee joint sagittal planeInitial knee flexion maximum +Initial knee flexion +Terminal knee extension maximum −Initial knee motion (flexion movement)Midstance knee motion (extension movement)
Knee joint transverse planeMaximum knee internal rotation +Maximum knee external rotation −Total knee rotation motion
283I. Krauss et al. / Clinical Biomechanics 27 (2012) 281–286
and tracking techniques (i.e. number, placement and geometry ofmarkers). Model outcomes are compared with respect to their agree-ment, their mean differences, and their influence on results of statisticalcomparisons between population groups. We hypothesised that agree-ment is worse and differences betweenmodels are larger in out-of sagit-tal plane variables in comparison to flexion and extension movements.We further hypothesised that a more sophisticated approach can reducesources of error, therefore being more sensitive to detect differencesbetween population groups.
2. Methods
2.1. Subjects
The study was conducted on ten healthy subjects (CO: five females,BMI: 22±2.5 kg/m², age: 27±7 years) and twelve subjects sufferingfrom knee osteoarthritis (OA: seven females, BMI: 29±4 kg/m², 64±8 years). The study complied with the Helsinki Declaration and wasapproved by the ethics committees of the participating institutions,and subjects gave informed written consent. Patients were recruitedfrom a training group for patients with knee osteoarthritis and exam-ined by an orthopaedic surgeon. Healthy controls were recruited fromstaff members.
2.2. Kinematic evaluation
A single comprehensive marker set was defined including all ana-tomical markers for both approaches (Fig. 1, Table 1). Two differentapproaches were used to quantify joint angles of the lower extremity:A prediction approach (PA) and a functional approach (FA). PA usesanatomical assumptions to define the locations of joint centres/axesrelative to specific anatomical landmarks (Isman and Inman, 1969;Weidow et al., 2006). The knee joint centre for PA is defined midwaybetween medial and lateral epicondyle of the knee. The connection ofthe epicondyles represents the z-axis of the anatomical coordinatesystem of the thigh. The x-axis is perpendicular to a plane definedby the epicondyles and the trochanter major. The y-axis is perpendic-ular to z and x. The first axis of the shank segment (y) is defined as aline connecting the ankle joint centre located midway between themedial and lateral malleolus, and the tuberositas tibiae. The x-axis isperpendicular to a plane defined by the malleoli and the tuberositastibiae. The z-axis is perpendicular to x and y (see Fig. 1). Knee jointangles were calculated using Cardan angles with a ZXY order of rota-tion around the moving axis of the thigh segment.
The functional approach FA is considered functional due to the cal-culation of subject specific joint centres/axes for the knee and hipjoint by using specific movement data of adjacent segments derivedfrom basic motion tasks (Bachmann et al., 2008; List, 2009; Wolf et al.,2009). In this approach each segment is defined by a redundant numberof markers, aiming at improving orientation accuracy (Challis, 1995).Marker positions were chosen such that skin movement artefactswere small and awell distributedmarker cloudwas formed (Soderkvistand Wedin, 1993). The position and orientation of each segment weredetermined relative to the reference segments defined by the standingtrial using a least-squares fit of the corresponding marker point clouds(Gander and Hrebicek, 1997). Joint rotations were described from thedistal relative to the proximal segment using a helical axis approach(Woltring, 1994). To define clinically interpretable rotational compo-nents, the attitude vector was decomposed along the axes of a givenjoint coordinate system (Woltring, 1994). The mediolateral axis e1 ofthe knee joint coordinate system is defined by the functional estimatedknee joint axis uk (Fig. 1). The vertical axis e3 is perpendicular to e1 andlies in the plane spanned by e1 and the hip joint centre. The posteroan-terior axis e2 is perpendicular to the latter two. Amore detailed descrip-tion of the kinematic analysis of the functional approach as well as itsday-to-day consistency is given by Wolf et al. (2009).
2.3. Procedures
Markers were attached to anatomical landmarks by the samephysiotherapist. A standing trial was done in a neutral position (noflexion or extension) of the ankle, knee and hip joints. Deviationsfrom neutral were accepted in case of joint constraints. The feetwere hip-width apart. Basic motion tasks for the functional approachwere defined as flexion and extension at the knee joint and circum-duction at the hip joint (Bachmann et al., 2008; List, 2009; Wolfet al., 2009). Subjects walked at a self-selected speed along an 18 mwalkway with five integrated force plates (2000 Hz, Kistler, Winter-thur, Switzerland) to detect stance phases. At least 10 trials for eachsubject were recorded using a 12-camera system (100 Hz, MX40 Sys-tem, Oxford Metrics, UK). Vicon Workstation/IQ software packageswere used to reconstruct, label and crop the data. Further data pro-cessing, joint centres and axes definitions and angle calculationsfor the functional approach were computed using Matlab (TheMathWorks, Natick, MA, USA). For the prediction approach, jointangles were calculated with Bodybuilder (Oxford Metrics, Oxford,UK) and distinctive gait variables were then extracted using Matlab(The MathWorks, Natick, MA, USA). Joint angles were calculatedrelative to the standing trial for both approaches.
Some defaults were defined for data analysis: The same gait cyclesof each subject had to be used for both models. All subjects had tocontribute exactly five trials. The analysis of discrete gait events waslimited to the stance phase of walking. Analysis was done for the

Table 3Comparison of distinctive gait variables. MD defines mean difference between methods in degree (PA minus FA) and 95% CI. Significant differences are displayed with asterisks(*pb0.05; **pb0.01). Italic variables were tested non-parametrically. Upper and lower levels of agreement (LoA) define MD plus andminus 1.96 SD of differences between methods.95% CI and intervals ΔLoA in ° and% ROM are amended.
Variable MD (95% CI) [°] Upper LoA (95% CI) [°] Lower LoA (95% CI) [°] ΔLoA ΔLoA [%ROM]
Knee sagittal plane ROM PA: 33°Initial knee flexion maximum −2.6** (−3.3 to −1.9) 0.4 (−0.8 to 1.5) −5.6 (−6.8 to −4.4) 6.0 18Initial knee flexion −3.1** (−4.0 to −2.3) 0.5 (−0.9 to 1.9) −6.8 (−8.2 to −5.4) 7.3 22Terminal knee extension maximum 0.1 (−0.3 to 0.6) 2.0 (1.3 to 2.7) −1.7 (−2.5 to −1.0) 3.7 11Initial knee motion (flexion movement) 0.5* (0.1 to 1.0) 2.5 (1.8 to 3.3) −1.5 (−2.3 to −0.7) 4.0 12Midstance knee motion (extension movement) −2.8** (−3.4 to −2.2) −0.1 (−1.1 to 1.0) −5.4 (−6.5 to −4.4) 5.3 16Knee transversal plane ROM: 10°Maximum knee internal rotation 2.7** (1.9 to 3.6) 6.5 (5.0 to 8.0) −1.1 (−2.5 to 0.4) 7.6 76Maximum knee external rotation −1.0 (−2.3 to 0.3) 4.7 (2.5 to 6.9) −6.7 (−9.0 to −4.5) 11.4 114Total knee rotation motion 3.7** (2.8 to 4.7) 8.0 (6.3 to 9.7) −0.6 (−2.2 to 1.1) 8.6 86
Table 4Mean differences (MD) between healthy controls (CO) and subjects with osteoarthritis(OA) for PA and FA. Exclamation marks (!) designate different results of the statisticalanalysis for PA and FA. Annotation: Positive values display increased joint excursions inhealthy controls, negative values designate increased joint excursion in subjects withknee OA. Italic variables were tested non-parametrically.
Variable MD for PA(P-value)
MD for FA(P-value)
!
Knee sagittal planeInitial knee flexion maximum 6.0 (P=0.04) 6.6 (P=0.02)Initial knee flexion 3.7 (P=0.17) 5.0 (P=0.04) !Terminal knee extension maximum 1.2 (P=0.55) 1.3 (P=0.50)Initial knee motion (flexion movement) 2.4 (P=0.10) 1.6 (P=0.16)Midstance kneemotion (extensionmovement) 4.8 (P=0.02) 5.3 (P=0.02)
Knee transversal planeMaximum knee internal rotation 2.3 (P=0.11) 1.5 (P=0.26)Maximum knee external rotation −4.1 (P=0.02) −1.1 (P=0.22) !Total knee rotation motion −1.8 (P=0.04) 0.4 (P=0.72) !
284 I. Krauss et al. / Clinical Biomechanics 27 (2012) 281–286
left side, except for two subjects with OA. They only had complaintson the right side, which was then used for further analysis. Discretemeasures of knee joint movements for sagittal and transverse planewere derived from each curve and averaged across trials (Table 2).Frontal plane kinematics were not considered, as ab/adductor motionis limited to approximately 5° due to restrictions imposed by theknee's geometry and the collateral ligaments. This small value is fur-ther influenced by cross-talk from knee flexion/extension.
2.4. Statistics
Mean differences (MD) ±95% confidence intervals (CI) betweenvariables of the two methods were calculated. The correspondingupper and lower levels of agreements (LoA) of MD were defined as±1.96 standard deviation of the differences between methods. CIswere amended for the given levels of agreement (Hamilton and Sta-mey, 2007). The interval between upper and lower level of agreementwas described in absolute numbers (ΔLoA) and as percentage of thecalculated mean range of motion of the given movement plane(ΔLoA in% ROM; for sagittal knee motion, ΔLoA was related to theROM of the prediction approach for both models, as total range of mo-tion was not calculated for the functional approach). Although notpresented in the manuscript, Bland and Altman plots were used tocheck for extreme values and whether differences between modelswere dependant on the dimension of the variable (Bland and Altman,1986).
Data were tested for normality using the Shapiro–Wilk test. Pairedt-tests or Wilcoxon-Signed Rank test in case of non-normality wereconducted to test for statistically significant differences betweenmodels (alpha=0.05). Unpaired t-tests or Wilcoxon tests in case ofnon-normality were used to compare variables of healthy subjectsand subjects with knee OA, and to examine whether statistical analy-sis of this comparison would yield different data interpretations whenusing different models.
3. Results
Table 3 illustrates the comparison of distinctive gait variables be-tween models: When comparing mean differences between models,initial knee flexion, initial knee flexion maximum, and midstance kneemotionwere significantly larger using the functional approach. Termi-nal knee extension maximumwas similar between methods.Maximumknee internal rotation, total knee rotation motion and initial knee motionshowed significantly larger values for the prediction approach.
Inter-subject variation of differences was quantified using the in-terval between upper and lower levels of agreement ΔLoA in absolute(°) and relative (% ROM) values. In this regard, the knee sagittal planehad smaller values than the transverse plane (3.7–7.3° and 11–22%ROM for sagittal plane versus 7.6–11.4° and 76–114% ROM for trans-verse plane variables, respectively). Comparisons of clinical outcome
variables between population groups (Table 4) yielded larger mid-stance knee motion, initial knee flexion maximum and initial knee flexionfor healthy controls. However, the latter was only statistically signifi-cant using the functional approach (P=0.04 for FA, P=0.17 for PA).Maximum knee external rotation and total knee rotation motion weresignificantly larger in the osteoarthritis group for the prediction ap-proach only. In this respect, results of the functional approach werenot statistically different between population groups (P=0.22 andP=0.72, respectively).
4. Discussion
Different research questions, premises of movement laboratorieswith respect to hardware, software andprofessional skills and the ongo-ing process of newdevelopments in the biomechanical modelling of thehuman beingwill always result in a variety of different approaches withvarying outcome quantities. It is therefore important to investigate dif-ferent procedures of instrumented gait analyses to allowmeaningful in-terpretations of clinical results. Within the context of this study, twoconfounding variables influencing the outcome of clinical gait analysishave been used: different anatomical coordinate system definitions(functional approach [FA] versus prediction approach [PA]) anddifferent angular decomposition methods (attitude vectors and Cardanangles). The contribution of each to the total variability betweenmethods cannot be differentiated. For sagittal plane kinematics at theknee joint, the influence of the angular decomposition method alongthe stance phase seems negligible, as illustrated in the motion graphsof Capozzo et al. and Chèze (Cappozzo et al., 2005; Cheze, 2000). Vari-ability is much greater for internal/external rotations of the swingphase of the gait cycle. It is smaller for the stance phase, yet not insub-stantial. This circumstance remains a methodological drawback of thepresent study and should be kept in mind for further investigations.

285I. Krauss et al. / Clinical Biomechanics 27 (2012) 281–286
Results of this study showmean differences between the function-al and the prediction approach, which are statistically significant foralmost all distinctive gait variables. Differences relative to total jointexcursion for sagittal plane variables were smallest. This finding coin-cides with Noonan et al. (2003), who compared results from four dif-ferent laboratories. Better consistency between protocols for jointflexion and extension in comparison to out-of-sagittal plane rotationswas also reported by Ferrari et al. (2008), who compared five com-monly used protocols for lower extremity joint kinematics.
Our results revealed differences in the statistical analysis whencomparing initial knee flexion maximum between healthy controlsand subjects with knee OA. According to Mundermann et al. (2005),OA subjects made initial contact with the ground with the knee in amore extended position than that exhibited by control subjects. Thiswas true for both models. However, only the functional approachshowed significant differences between groups.
Results for internal/external rotations at the knee joint, demonstrat-ing considerable differences betweenmodels, are again consistent withFerrari et al. (2008). Although not presented in the results, maximumexternal knee rotation took place at the beginning of the stance phase,and themaximumexternal knee rotation calculatedwith the predictionapproachwas significantly larger in subjects with osteoarthritis in com-parison to healthy controls. The error due to soft tissue artefacts shouldbe more distinct in calculations of the prediction approach, since thenumber of markers to define the thigh segment was limited to three.It further seems reasonable that pre-obese osteoarthritis patients witha mean BMI of 29 kg/m² showed larger thigh rotations after the impactof heel strike due to soft tissue artefacts than normal weight controls.These sources of error may therefore be responsible for differencesbetween groups which were only demonstrated with the predictionapproach. Aside from the statistical analysis, results of the twomethodsfor group comparisons deviated substantially from each other, withopposed results for transverse range of motion.
Methods are comparable even if absolute values for variables ofinterest are different, as long as the difference is known and differencesare stable across subjects. In the current investigation, inter-subjectvariation of differences was quantified using the interval between theupper and lower level of agreement ΔLoA (Bland and Altman, 1986).There is no common agreement about what size of intervals is accept-able. Interpretations should be based on the practical relevance of thegiven values with respect to the variable and the field of application(Axmann et al., 2002). Themost stable discrete gait variables in the pre-sent data set are joint angles and motions in the sagittal plane of theknee joint. They are considered more stable than out-of-sagittal planemovements for various aspects: Aside from the lesser dependence ofthe results with respect to the underlying biomechanical model, goodreproducibility decreases the susceptibility to measurement errors(Ferber et al., 2002). In contrast, gait variables in the transverse planeare poorly reproducible (Ferber et al., 2002), and their variabilityassociated with the underlying biomechanical protocol is substantial(Ferrari et al., 2008; Noonan et al., 2003; Ryu et al., 2006). The latterappears to be even larger than the variability due to a lack of reproduc-ibility or objectivity (Ferrari et al., 2008). In the present study, individualdifferences between methods for transverse plane variables were aslarge as the total joint excursion. The results of this study do not allowa statement whether one approach is more valid than the other. It canbe hypothesised that the functional approach with various features toreduce sources of errors, such as redundant markers, well distributedmarker clouds, functionally determined joint centres etc., yields betterresults in terms of validity. However, validity has not yet been provenfor the given concept and should be investigated in future studies.
5. Conclusions
Our study reveals larger differences between models for out-of sag-ittal plane variables in comparison toflexion and extensionmovements,
as hypothesised. Variables of the knee joint transverse plane are notcomparable between different biomechanical approaches. In accor-dance with other authors we therefore recommend abstaining fromusing gait variables of the knee joint transverse plane as long as sourcesof error are not noticeably reduced (Della Croce et al., 2005; Ferrariet al., 2008).
When data from differentmodels are shared, gait protocols differingfrom standard protocols have to be described precisely and compari-sonswith other studies should be done critically. To allow a practical in-terpretation of a comparison of approaches, differences and theirvariability should be quantified in the unit of interest (i.e. degree orpercent). Furthermore, it is very important that common users of clini-cal gait analysis are sensitised to the variability of clinical outcomemea-sures derived from different biomechanical models.
Acknowledgements
This study was not funded by any sponsors or outside sources offunding. We want to thank Mr Christoph Ziegler for data acquisition,and Mrs Lisa Peterson for her linguistic assistance in the preparationof the manuscript. This work is in memory of Dr. Alex Stacoff.
References
Al-Zahrani, K.S., Bakheit, A.M., 2002. A study of the gait characteristics of patients withchronic osteoarthritis of the knee. Disabil. Rehabil. 24 (5), 275–280.
Astephen, J.L., Deluzio, K.J., Caldwell, G.E., Dunbar, M.J., 2008. Biomechanical changes atthe hip, knee, and ankle joints during gait are associated with knee osteoarthritisseverity. J. Orthop. Res. 26 (3), 332–341.
Axmann, D., Gomez, G., Groten, M., 2002. Der Bland and Altman Plot - eine einfachegraphische Methode zur Einschätzung der Verlässlichkeit von Messverfahren.Dtsch. Zahnarztl. Z. 57 (10), 613–616.
Bachmann, C., Gerber, H., Stacoff, A., 2008. Labormessmethoden und ausgewählte Beispielezur instrumentierten Ganganalyse. Schweiz. Z. Sportmed. 56 (2), 29–34.
Bland, J.M., Altman, D.G., 1986. Statistical methods for assessing agreement betweentwo methods of clinical measurement. Lancet 1 (8476), 307–310.
Brandes, M., Schomaker, R., Mollenhoff, G., Rosenbaum, D., 2008. Quantity versus qual-ity of gait and quality of life in patients with osteoarthritis. Gait Posture 28 (1),74–79.
Cappozzo, A., Della, C.U., Leardini, A., Chiari, L., 2005. Human movement analysis usingstereophotogrammetry. Part 1: theoretical background. Gait Posture 21 (2),186–196.
Challis, J.H., 1995. A procedure for determining rigid body transformation parameters.J. Biomech. 28 (6), 733–737.
Cheze, L., 2000. Comparison of different calculations of three-dimensional joint kine-matics from video-based system data. J. Biomech. 33 (12), 1695–1699.
Della Croce, U., Leardini, A., Chiari, L., Cappozzo, A., 2005. Human movement analysisusing stereophotogrammetry. Part 4: assessment of anatomical landmark mis-placement and its effects on joint kinematics. Gait Posture 21 (2), 226–237.
Ferber, R., McClay Davis, I., Williams, D.S., Laughton, C., 2002. A comparison of within-and between-day reliability of discrete 3D lower extremity variables in runners.J. Orthop. Res. 20 (6), 1139–1145.
Ferrari, A., Benedetti, M.G., Pavan, E., Frigo, C., Bettinelli, D., Rabuffetti, M., et al., 2008.Quantitative comparison of five current protocols in gait analysis. Gait Posture 28(2), 207–216.
Gander,W., Hrebicek, J., 1997. Least squaresfit of point clouds. SolvingProblems in ScientificComputing using Maple and Matlab. Springer, pp. 339–349.
Hamilton, C., Stamey, J., 2007. Using Bland–Altman to assess agreement between twomedical devices—don't forget the confidence intervals! J. Clin. Monit. Comput. 21(6), 331–333.
Isman, R.E., Inman, V.T., 1969. Anthropometric studies of the human foot and ankle.Bull. Prosthet. Res. 10 (11), 97–219.
Lindemann, U., Becker, C., Unnewehr, I., Muche, R., Aminin, K., Dejnabadi, H., et al.,2006. Gait analysis and WOMAC are complementary in assessing functional out-come in total hip replacement. Clin. Rehabil. 20 (5), 413–420.
List, R., 2009. Joint Kinematics of Unconstrained Ankle Arthroplasties., (PhD thesis). ETHZurich, Switzerland.
Maly, M.R., Costigan, P.A., Olney, S.J., 2006. Role of knee kinematics and kinetics on per-formance and disability in people with medial compartment knee osteoarthritis.Clin. Biomech. 21 (10), 1051–1059.
Mundermann, A., Dyrby, C.O., Andriacchi, T.P., 2005. Secondary gait changes in patientswith medial compartment knee osteoarthritis: increased load at the ankle, knee,and hip during walking. Arthritis Rheum. 52 (9), 2835–2844.
Noonan, K.J., Halliday, S., Browne, R., O'Brien, S., Kayes, K., Feinberg, J., 2003. Interobser-ver variability of gait analysis in patients with cerebral palsy. J. Pediatr. Orthop. 23(3), 279–287.
Ryu, T., Choi, H.S., Choi, H., Chung, M.K., 2006. A comparison of gait characteristics be-tween Korean and Western people for establishing Korean gait reference data. Int.J. Ind. Ergon. 36, 1023–1030.

286 I. Krauss et al. / Clinical Biomechanics 27 (2012) 281–286
Schmitt, H., Rohs, C., Schneider, S., Clarius, M., 2006. Führt intensiver Langstreckenlaufzur Arthrose der Hüft- oder Kniagelenke? Orthopade 35, 1087–1092.
Soderkvist, I., Wedin, P.A., 1993. Determining the movements of the skeleton usingwell-configured markers. J. Biomech. 26 (12), 1473–1477.
Weidow, J., Tranberg, R., Saari, T., Karrholm, J., 2006. Hip and knee joint rotations differbetween patients with medial and lateral knee osteoarthritis: gait analysis of 30patients and 15 controls. J. Orthop. Res. 24 (9), 1890–1899.
Wolf, P., List, R., Ukelo, T., Maiwald, C., Stacoff, A., 2009. Day-to-day consistency of lowerextremity kinematics during walking and running. J. Appl. Biomech. 25, 369–376.
Woltring, H.J., 1994. 3-D attitude representation of human joints: a standardizationproposal. J. Biomech. 27 (12), 1399–1414.
Wu, G., Siegler, S., Allard, P., Kirtley, C., Leardini, A., Rosenbaum, D., et al., 2002. ISB rec-ommendation on definitions of joint coordinate system of various joints for thereporting of human joint motion—part I: ankle, hip, and spine. International Societyof Biomechanics. J. Biomech. 35 (4), 543–548.
Yavuzer, G., Sonel, B., Suldur, N., Ergin, S., 2005. Effects of intra-articular hylan G-F 20injections on clinical and biomechanical characteristics of the knee in osteoarthri-tis. Int. J. Rehabil. Res. 28 (4), 371–374.
Related Documents