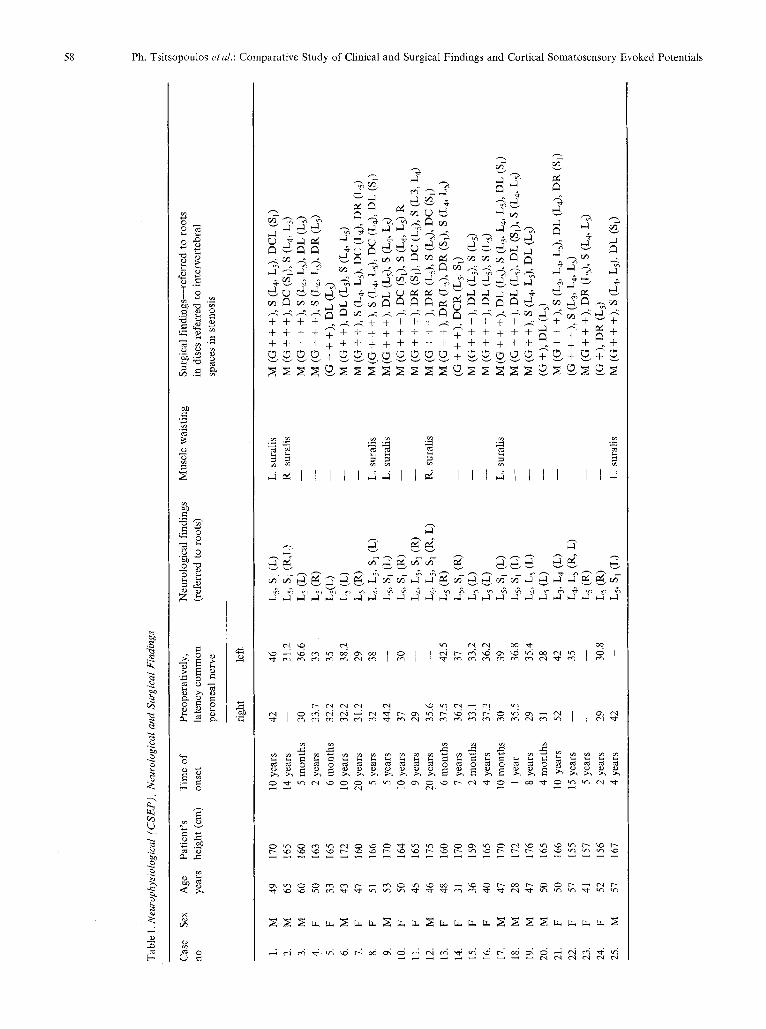
Acta Neurochir (Wien) (1987) 84:54-63 :Acta Nduro&irurgica by Springer-Verlag 1987 Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials in Patients with Lumbar Spinal Stenosis and Disc Protrusion Ph. Tsitsopoulos l, F. Fotiou 2, D. Papakostopoulos 3, C. Sitzoglou 2, and G. Tavridis t 1Department of Neurological Surgery, University Thessaloniki, Greece 2 Clinic of Neurology and Psychiatry University Thessaloniki, Greece 3 Burden Institute of Neurology, Bristol, U.K. Summary This paper is dealing with a comparative study of clinico-surgical findings and cortical somatosensory evoked potentials (CSEP's) recordings after stimulation of the right and left common peroneal nerve behind the fibula head, in twenty five patients suffering from lumbar spinal stenosis and disc prolapse. In all instances, the latencies of the first positive wave (the waveform also, when the latency was not discrete) were evaluated. The neurophysiological findings were verified by surgery. In com- bination with other roots, L 3 root was affected in 1 patient, L 4 in 6, L 5 in 13 and S 1 in 11. L 5 was affected alone in 11 and L 5 and S 1 were impaired in combination in 11 patients. Seven patients presented sural atrophy. The results of the neurophysiological study are described below: There was delayed response on both sides in six patients, while in ten patients delayed response was found on one (affected) side, inconclusive responses in seven and in two normal. Myelography and CT Scan were performed pre-operatively to ascertain disc protrusion and establish stenosis criteria. The surgical findings were: clear disc protrusion in 4 patients, stenosis in one and combined lesions in 20 (including central disc protrusion in seven). Sixteen patients out of twenty-five had a follow up neurophysi- ological evaluation in addition to the clinical follow up examination. In thirteen of the above patients, (taken with the clinical progress) the re-examination gave improved neurophysiological data both as regards latency and P1 waveform. It was obvious that high value latencies were associated with long standing clinical symptoms while at the same time root compression involved more than one level. Regarding the neurophysiological data and the surgical findings, it was found that in the majority of the cases (92%) these two parameters matched together, so that in such cases a possible prediction of the operative outcome can be given. Keywords: Disc protrusion; lumbar stenosis; CSEP; laminectomy. Abbreviations Neurologicalfindings L 5 (R): Right fifth lumbar root. L 5 (L): Left fifth lumbar root. L3, L4 (L): Left third and fourth lumbar roots. Ls, S 1 (R): Right fifth lumbar and first sacral roots. Ls, $1 (L): Left fifth lumbar and first sacral roots. L 5, S 1 (R, L): bilateral (right and left) fifth lumbar and first sacral roots. Surgicalfindings The predominant cause of the lesion, either stenosis (S) or disc protrusion (D) follows the symbol (M) in mixed lesions and the symbols (G +, G + +, G + + +) according to the severity: S (L4, L5) R: stenosis at fourth and fifth lumbar intervertebral spaces more on the right. DR: Disc protrusion to the right. DL: Disc protrusion to the left. DR or DL (Ls, $1): Disc protrusion to the right or to the left compressing both roots the fifth lumbar and the first sacral. DC: Central disc protrusion. DCR: Central disc protrusion and to the right. DCL: Central disc protrusion and to the left. Introdnetion Both central and peripheral somatosensory evoked potentials (SEPs) can be recorded by surface and implanted electrodes, stimulating peripheral nerves of the upper and lower limbs 3, 4, 8, 11, 12, 13 Positive waveform with 26-34 msec latency is invari- ably obtained in normal subjects using surface

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Acta Neurochir (Wien) (1987) 84:54-63 :Acta Nduro&irurgica �9 by Springer-Verlag 1987
Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials in Patients with Lumbar Spinal Stenosis and Disc Protrusion
Ph. Tsitsopoulos l, F. Fotiou 2, D. Papakostopoulos 3, C. Sitzoglou 2, and G. Tavridis t
1 Department of Neurological Surgery, University Thessaloniki, Greece 2 Clinic of Neurology and Psychiatry University Thessaloniki, Greece 3 Burden Institute of Neurology, Bristol, U.K.
Summary
This paper is dealing with a comparative study of clinico-surgical findings and cortical somatosensory evoked potentials (CSEP's) recordings after stimulation of the right and left common peroneal nerve behind the fibula head, in twenty five patients suffering from lumbar spinal stenosis and disc prolapse.
In all instances, the latencies of the first positive wave (the waveform also, when the latency was not discrete) were evaluated. The neurophysiological findings were verified by surgery. In com- bination with other roots, L 3 root was affected in 1 patient, L 4 in 6, L 5 in 13 and S 1 in 11. L 5 was affected alone in 11 and L 5 and S 1 were impaired in combination in 11 patients. Seven patients presented
sural atrophy. The results of the neurophysiological study are described below: There was delayed response on both sides in six patients, while in
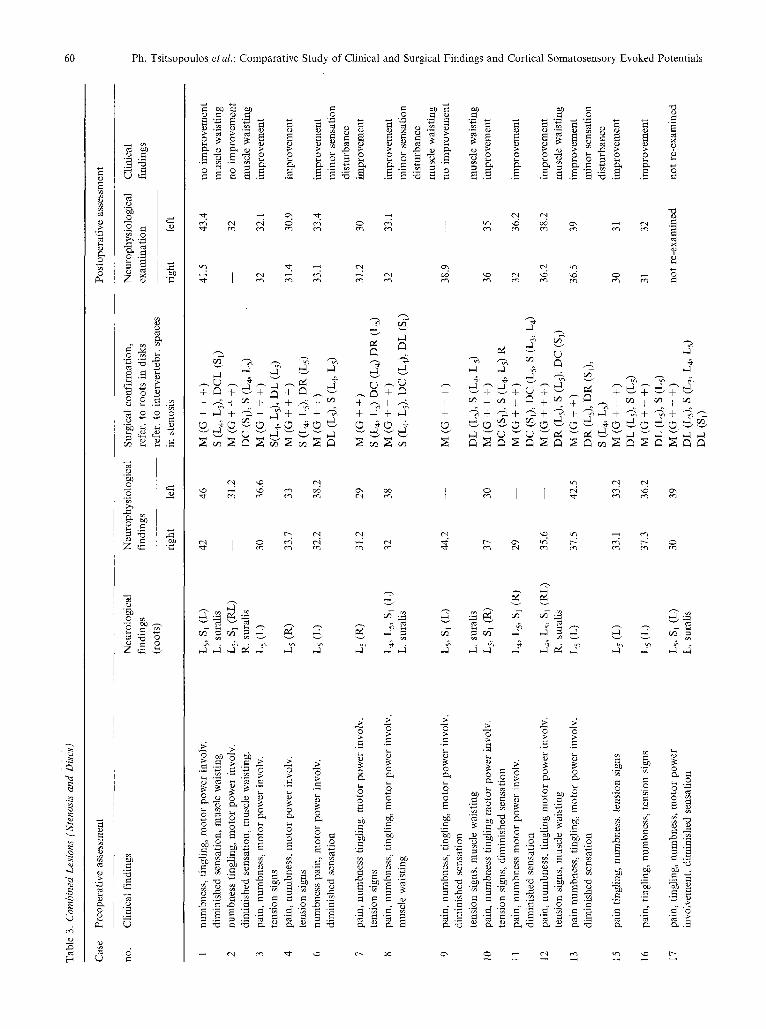
ten patients delayed response was found on one (affected) side, inconclusive responses in seven and in two normal. Myelography and CT Scan were performed pre-operatively to ascertain disc protrusion and establish stenosis criteria. The surgical findings were: clear disc protrusion in 4 patients, stenosis in one and combined lesions in 20 (including central disc protrusion in seven).
Sixteen patients out of twenty-five had a follow up neurophysi- ological evaluation in addition to the clinical follow up examination.
In thirteen of the above patients, (taken with the clinical progress) the re-examination gave improved neurophysiological data both as regards latency and P1 waveform. It was obvious that high value latencies were associated with long standing clinical symptoms while at the same time root compression involved more than one level.
Regarding the neurophysiological data and the surgical findings, it was found that in the majority of the cases (92%) these two parameters matched together, so that in such cases a possible prediction of the operative outcome can be given.
Keywords: Disc protrusion; lumbar stenosis; CSEP; laminectomy.
Abbreviations
Neurological findings
L 5 (R): Right fifth lumbar root. L 5 (L): Left fifth lumbar root. L3, L4 (L): Left third and fourth lumbar roots. Ls, S 1 (R): Right fifth lumbar and first sacral roots. Ls, $1 (L): Left fifth lumbar and first sacral roots. L 5, S 1 (R, L): bilateral (right and left) fifth lumbar and first sacral
roots.
Surgical findings
The predominant cause of the lesion, either stenosis (S) or disc protrusion (D) follows the symbol (M) in mixed lesions and the symbols (G +, G + +, G + + +) according to the severity:
S (L 4, L5) R: stenosis at fourth and fifth lumbar intervertebral spaces more on the right.
DR: Disc protrusion to the right. DL: Disc protrusion to the left. DR or DL (Ls, $1): Disc protrusion to the right or to the left
compressing both roots the fifth lumbar and the first sacral. DC: Central disc protrusion. DCR: Central disc protrusion and to the right. DCL: Central disc protrusion and to the left.
In tr o d n e t i o n
B o t h c e n t r a l a n d p e r i p h e r a l s o m a t o s e n s o r y e v o k e d
p o t e n t i a l s ( S E P s ) c a n b e r e c o r d e d b y s u r f a c e a n d
i m p l a n t e d e l ec t rodes , s t i m u l a t i n g p e r i p h e r a l n e r v e s o f
t h e u p p e r a n d l o w e r l i m b s 3, 4, 8, 11, 12, 13
P o s i t i v e w a v e f o r m w i t h 2 6 - 3 4 m s e c l a t e n c y is i n v a r i -
a b l y o b t a i n e d in n o r m a l s u b j e c t s u s i n g s u r f a c e
Ph. Tsitsopoulos etaL: Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials 55
electrodes placed on the scalp, following common peroneal nerve stimulation behind the head of the fibula.
There is a great number of studies referring to clinical applications of cortical SEPs following medial nerve stimulation mainly in patients with neurological disorders ~, e, 5, 7. On the contrary, reports concerning such applications, following lower limb nerve stimula- tion, started appearing increasingly lately 6, 9, 10, 14, 15
This paper is dealing with the recorded CSEPs, after common peroneal nerve stimulation in patients suffer- ing from lumbar spinal degenerative disease (disc protrusion--spinal canal stenosis), associated with such clinical and neuroradiological pictures indicating surgery.
The aims of this study were: 1. to detect the correlation--if any--between pre-
operative neurophysiological data (CSEPs) with the surgical findings,
2. to compare the post-operative neurophysiological status to the clinical course of the patients, and
3. to determine whether the operative outcome could be foreseen by evaluating the cortical SEPs recorded before the operation.
Clinical Material and Methods
Cortical SEPs were recorded following common peroneal nerve stimulation in twenty five patients (eleven males and fourteen females) aged 28-65 years (1.55-1.76cm height). These patients suffered from lumbar spinal canal stenosis and disc protrusion and subsequently underwent surgery. The control group consisted of sixteen age-matched healthy individuals (1.55-1.80 cm height).
All patients were examined in supine position on a comfortable bed in a quiet room with temperature 22-26 ~ The purpose of the examination was thoroughly explained to the patient. With the consent of the patient we tried to make them feel comfortable with the electrical pulse stimulation. Electrical stimuli were applied through disa type electrodes with the cathode being 3 cm proximal to anode. Stimuli were applied to common peroneal nerve at a site behind fibular head. The intensity of the stimulation was that sufficient, to produce a brisk movement of the ankle joint. The application rate of the electrical stimulus was 1 p/sec with a 0.5 msec duration.
The recording electrode was placed 2cm behind Cz with the reference electrode at Fz (10-20 international system). Cortical instead of lumbar recording was prefered because there was concomi- tant severe lumbar pain and muscle spasm in all our cases at the time of the examination. Monopolic unvarnished stainless steel needles (electrodes) of 0.2 mm diameter were used. Each common peroneal nerve was stimulated separately and the corresponding waves were recorded. Time constant was 0.8 msec and the high frequency filter of 3 .2KH ( - - 3dB). Gain was at 50 gV/1 cm. Although 256 stimuli were sufficient to produce CSEPs but in several patients it was required double number (512) of stimuli.
The parameters which were evaluated included latency and morphology of the first positive wave. The above data were compared
to those of the control group. Criteria used in the evaluation of the abnormal neurophysiological results that were obtained included: The morphology and the latency of the first positive wave of CSEPs, were in this way primarily evaluated.
A latency greater than 2 sd of the control goup, and when the difference of latencies between the most and least affected side was greater than 3 sd were addidtionally evaluated. The clinical picture and the operative findings were compared with the preoperative neurophysiological data and with those one year after surgery (of the twenty-five patients the sixteen were followed up).
In our patients, in addition to plain X-rays, lumbar CT Scan and myelography were carried out, in most of them, to confirm the clinical diagnosis.
During operation, patients were maintained in a prone position on the operative table with the spine flexed at 55-20 ~ Because of the common occurrence of severe combined lesions (disc protrusion- stenosis), the surgical technique used was the same in almost all patients (extensive laminectomy from L 3 to S 1 and exploration of the intervertebral spaces and foramina).
Results
A. Pre-operative Data
1. Neurophysiological Data
a) Control Group (16 cases)
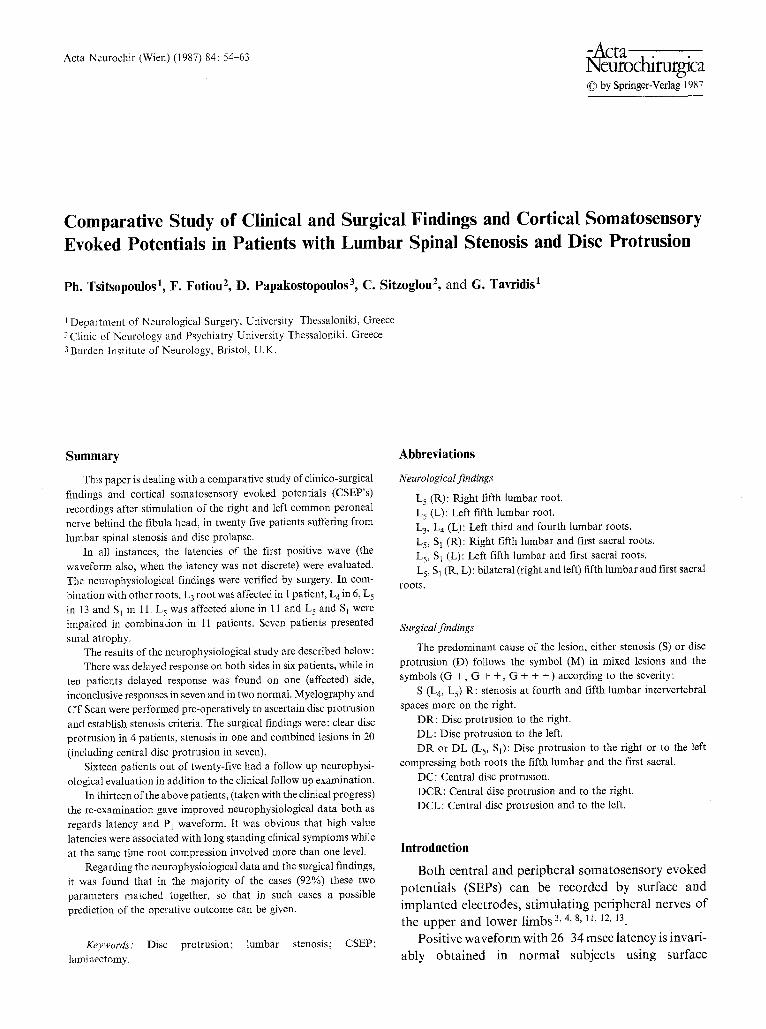
The latency of the first positive wave following the right and left common peroneal nerve stimulation was 30.9 msec with sd 2.2 msec (Fig. 1) and 30.7 msec with sd 1.9 msec respectively.
20ms
Fig. I. CSEP recording in 4 normal subjects (after right common peroneal nerve stimulation). The vertical line shows the average latency of the first positive wave in the normal subjects
56 Ph. Tsitsopoulos etal.: Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials
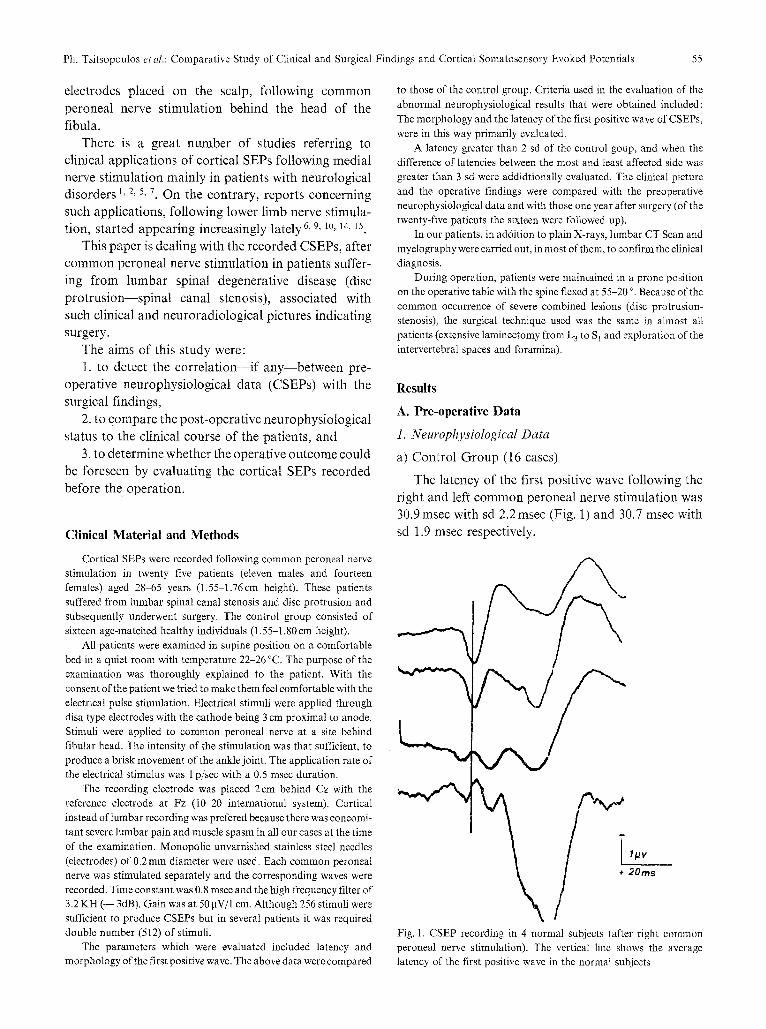
The mean difference in latency after right and left stimulation was 0.67 msec and of the sd 0.42msec (Fig. 2).
i 1/Jv + 20ms
Fig. 2. CSEP recorded after separate stimulation of the right and left
common peroneal nerve in the same individual. The similarity of the
latency as well as the morphology of the first positive wave are clearly
shown
S
i Ipv + 2 0 m s
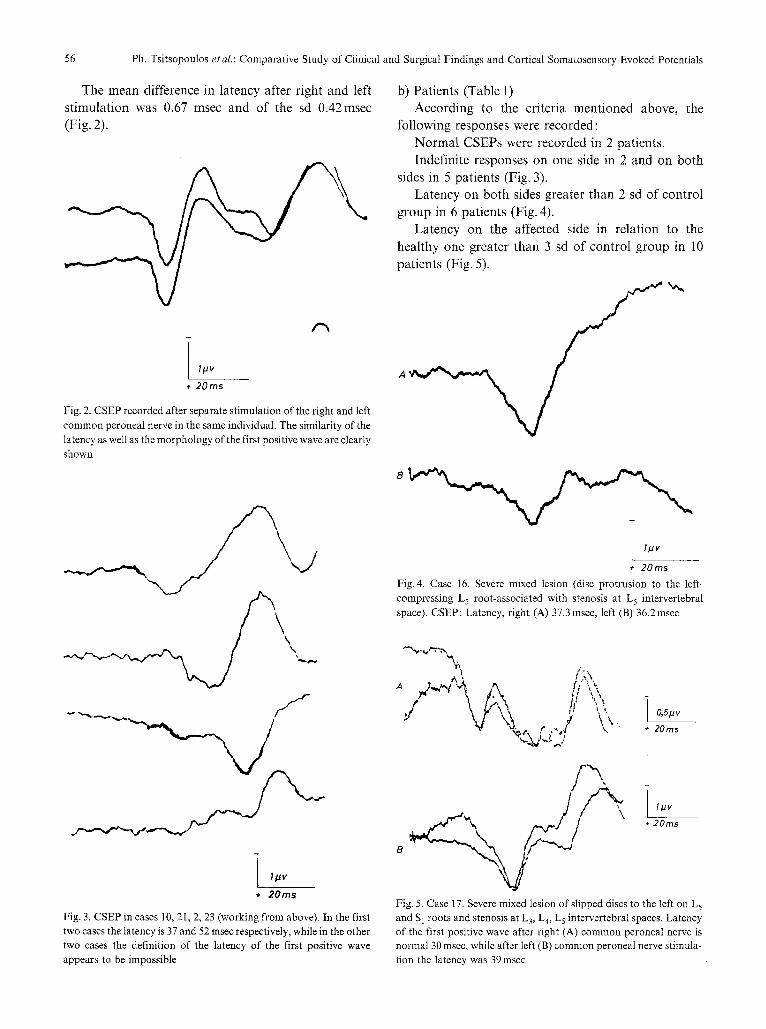
Fig. 3. CSEP in cases 10, 21, 2, 23 (working from above). In the first two cases the latency is 37 and 52 msec respectively, while in the other
two cases the definition of the latency o f the first positive wave appears to be impossible
b) Patients (Table 1) According to the criteria mentioned above, the
following responses were recorded: Normal CSEPs were recorded in 2 patients. Indefinite responses on one side in 2 and on both
sides in 5 patients (Fig. 3). Latency on both sides greater than 2 sd of control
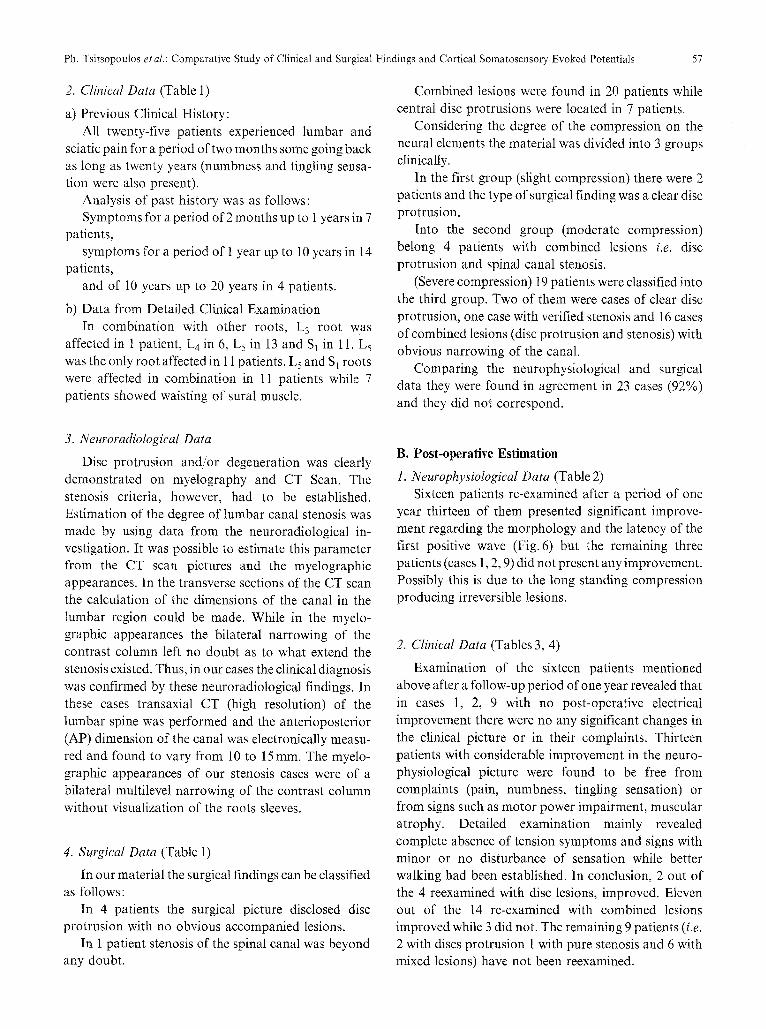
group in 6 patients (Fig. 4). Latency on the affected side in relation to the
healthy one greater than 3 sd of control group in 10 patients (Fig. 5).
A
I/Jv
+ 20ms Fig. 4. Case 16. Severe mixed lesion (disc protrusion to the left-
compressing L 5 root-associated with stenosis at L 5 intervertebral
space). CSEP: Latency, right (A) 37.3 msec, left (B) 36.2msec
'l~ / ..
A ', t ;'-,\,
" f % A r . - , - / ',. "
i O,51Jv
+ 20ms
; \ § 20ms
Fig. 5. Case 17. Severe mixed lesion of slipped discs to the left on L 5
and S 1 roots and stenosis at L3, L 4, L 5 intervertebral spaces. Latency of the first positive wave after right (A) common peroneal nerve is normal 30 msec, while after left (B) common peroneal nerve stimula-
tion the latency was 39 msec
Ph. Tsitsopoulos et al.: Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials 57
2. Clinical Data (Table 1)
a) Previous Clinical History: All twenty-five patients experienced lumbar and
sciatic pain for a period of two months some going back as long as twenty years (numbness and tingling sensa- tion were also present).
Analysis of past history was as follows: Symptoms for a period of 2 months up to 1 years in 7
patients, symptoms for a period of 1 year up to 10 years in 14
patients, and of 10 years up to 20 years in 4 patients.
b) Data from Detailed Clinical Examination In combination with other roots, L 3 root was
affected in 1 patient, L4in 6, L 5 in 13 and $1 in 11. L 5 was the only root affected in 11 patients. L5 and SI roots were affected in combination in 11 patients while 7 patients showed waisting of sural muscle.
Combined lesions were found in 20 patients while central disc protrusions were located in 7 patients.
Considering the degree of the compression on the neural elements the material was divided into 3 groups clinically.
In the first group (slight compression) there were 2 patients and the type of surgical finding was a clear disc protrusion.
Into the second group (moderate compression) belong 4 patients with combined lesions i.e. disc protrusion and spinal canal stenosis.
(Severe compression) 19 patients were classified into the third group. Two of them were cases of clear disc protrusion, one case with verified stenosis and 16 cases of combined lesions (disc protrusion and stenosis) with obvious narrowing of the canal.
Comparing the neurophysiological and surgical data they were found in agreement in 23 cases (92%) and they did not correspond.
3. Neuroradiological Data
Disc protrusion and/or degeneration was clearly demonstrated on myelography and CT Scan. The stenosis criteria, however, had to be established. Estimation of the degree of lumbar canal stenosis was made by using data from the neuroradiological in- vestigation. It was possible to estimate this parameter from the CT scan pictures and the myelographic appearances. In the transverse sections of the CT scan the calculation of the dimensions of the canal in the lumbar region could be made. While in the myelo- graphic appearances the bilateral narrowing of the contrast column left no doubt as to what extend the stenosis existed. Thus, in our cases the clinical diagnosis was confirmed by these neuroradiological findings. In these cases transaxial CT (high resolution) of the lumbar spine was performed and the anterioposterior (AP) dimension of the canal was electronically measu- red and found to vary from 10 to 15ram. The myelo- graphic appearances of our stenosis cases were of a bilateral multilevel narrowing of the contrast column without visualization of the roots sleeves.
4. Surgical Data (Table 1)
In our material the surgical findings can be classified as follows:
In 4 patients the surgical picture disclosed disc protrusion with no obvious accompanied lesions.
In 1 patient stenosis of the spinal canal was beyond any doubt.
B. Post-operative Estimation
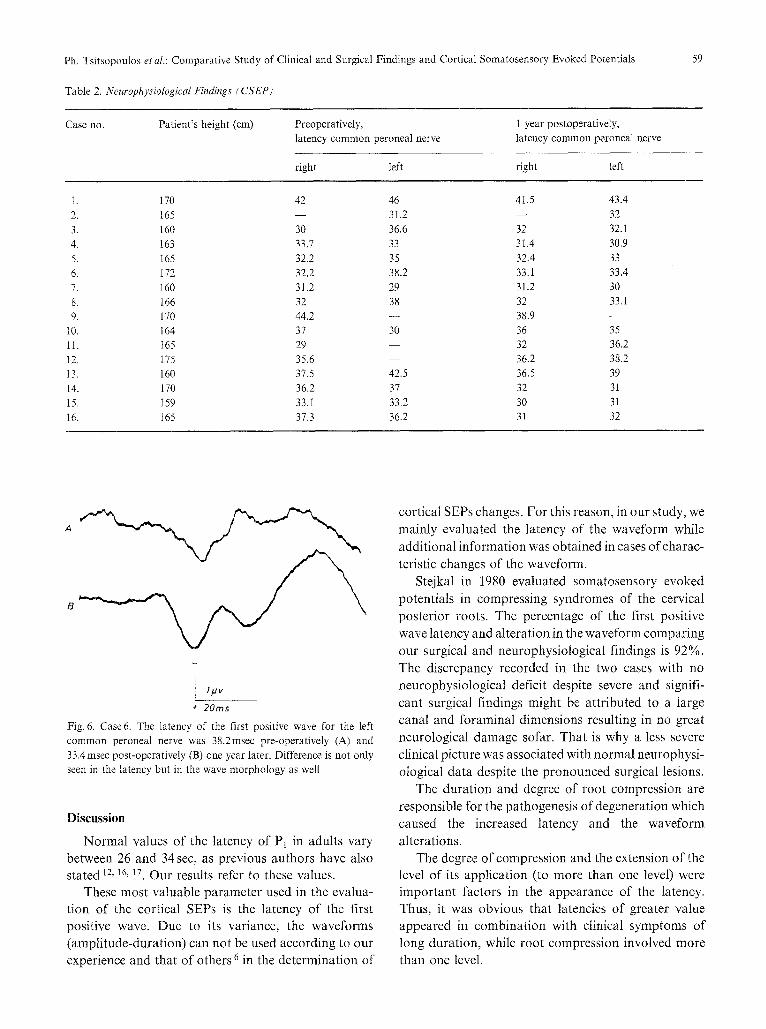
1. Neurophysiological Data (Table 2) Sixteen patients re-examined after a period of one
year thirteen of them presented significant improve- ment regarding the morphology and the latency of the first positive wave (Fig. 6) but the remaining three patients (cases 1, 2, 9) did not present any improvement. Possibly this is due to the long standing compression producing irreversible lesions.
2. Clinical Data (Tables 3, 4)
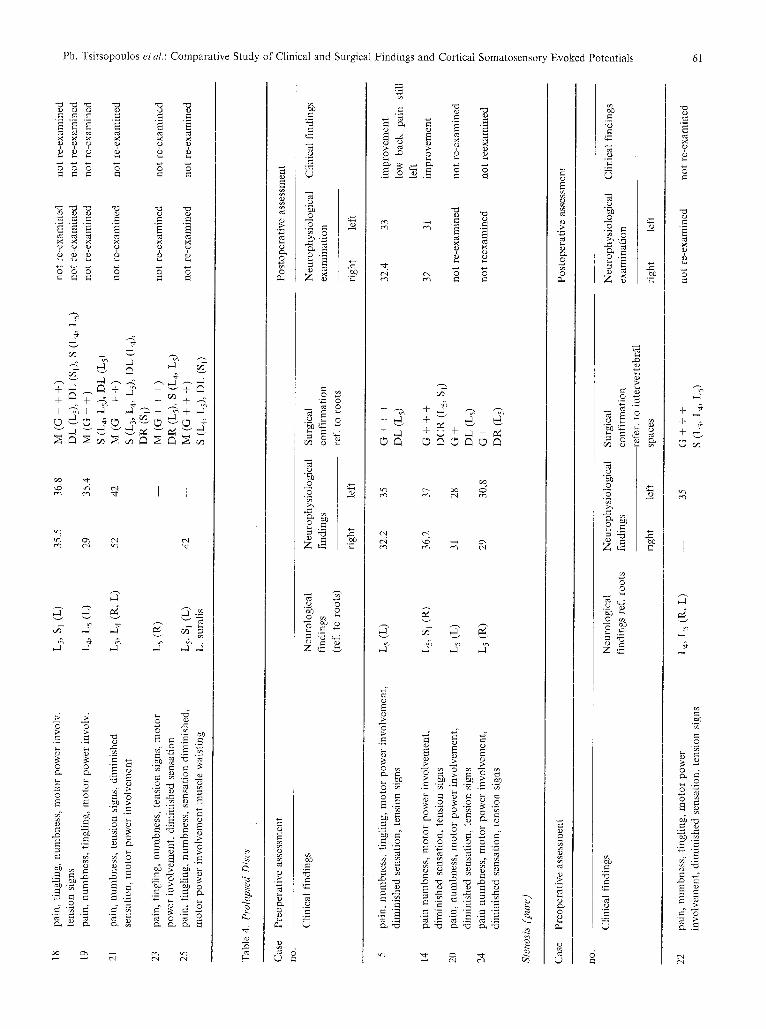
Examination of the sixteen patients mentioned above after a follow-up period of one year revealed that in cases 1, 2, 9 with no post-operative electrical improvement there were no any significant changes in the clinical picture or in their complaints. Thirteen patients with considerable improvement in the neuro- physiological picture were found to be free from complaints (pain, numbness, tingling sensation) or from signs such as motor power impairment, muscular atrophy. Detailed examination mainly revealed complete absence of tension symptoms and signs with minor or no disturbance of sensation while bet ter walking had been established. In conclusion, 2 out of the 4 reexamined with disc lesions, improved. Eleven out Of the 14 re-examined with combined lesions improved while 3 did not. The remaining 9 patients (i.e. 2 with discs protrusion 1 with pure stenosis and 6 with mixed lesions) have not been reexamined.
Tab
le 1
, Neu
roph
ysio
logi
cal (
CSE
P),
Neu
rolo
gica
l and
Sur
gica
l Fin
ding
s
Cas
e Se
x A
ge
Pat
ient
's
Tim
e of
P
reop
erat
ivel
y,
no
year
s he
ight
(cm
) on
set
late
ucy
com
mon
pe
rone
al n
erve
Neu
rolo
gica
l fi
ndin
gs
(ref
erre
d to
roo
ts)
Mus
cle
wai
stin
g S
urgi
cal
find
ings
--re
ferr
ed t
o ro
ots
in d
iscs
ref
erre
d to
int
erve
rteb
ral
spac
es i
n st
enos
is
righ
t le
ft
o �9 r �9
1.
M
49
170
10 y
ears
42
46
2.
M
65
16
5 I4
yea
rs
--
31.2
3.
M
60
16
0 5
mon
ths
30
36.6
4.
F
50
163
2 ye
ars
33.7
33
5.
F
33
165
6 m
onth
s 32
.2
35
6.
M
43
172
10 y
ears
32
.2
38.2
7.
F
47
160
20 y
ears
31
.2
29
8.
F 51
16
6 5
year
s 32
38
9.
M
53
17
0 5
year
s 44
.2
--
10.
F 50
16
4 I0
yea
rs
37
30
11.
F 45
16
5 9
year
s 29
--
12
. M
46
17
5 20
yea
rs
35.6
--
13
. F
48
160
6m
on
ths
37.5
42
.5
14.
F 31
17
0 7
year
s 36
.2
37
15.
F 36
15
9 2
mo
nth
s 33
.1
33.2
i6
. F
40
165
4 ye
ars
37.3
36
.2
17.
M
47
170
10m
onth
s 30
39
18
. M
28
17
2 I
year
35
.5
36.8
19
. M
47
17
6 8
year
s 29
35
.4
20.
M
50
165
4 m
onth
s 31
28
21
. F
50
166
10 y
ears
52
42
22
. F
57
155
15 y
ears
35
23
. F
41
157
5 ye
ars
--
--
24.
F 52
15
6 2
year
s 29
30
.8
25.
M
57
167
4 ye
ars
42
--
Ls,
S 1
(L)
L5,
S 1
(R,L
) L5
(L)
L5 (a
) Ls
(L)
L 5
(L
) L
5 (
R)
La,
L 5
, S 1
(L)
L5,
S 1
(L)
Ls,
S 1
(R)
L4,
Ls,
S 1
(R)
L4,
Ls,
S I
(R,
L)
L5 (R
) L
5, S
1 (R
) L
5 (
L)
L s
(L)
Ls,
S
1 (L
) L
s, S
t (L
) L
4, L
5 (L
) L
5 (
L)
L 3,
L 4
(L)
L4,
L 5
(R
, L
) L5
(R)
L s
(R)
Ls,
S 1
(L)
L.
sura
lis
R.
sura
lis
L.
sura
lis
L.
sura
lis
R.
sura
lis
L.
sura
lis
L.
sura
lis
M (
G +
+ +
), S
(L
4, L
5),
DC
L (
SI)
M (
G +
+ +
), D
C (
Sl)
, S
(L4,
L5)
M
(6
+ +
+),
S (
L 4,
Ls)
, D
L (
Ls)
M
(G
+ +
+),
S (
L 4,
Ls)
, D
R (
L5)
(G
+ +
+),
DL
(L
s)
M (
G +
+),
DL
(L
5),
S (L
4, L
s)
M (
G +
+),
S (
L4,
Ls)
, D
C (
L4)
, D
R (
Ls)
M
(G +
+ +
), S
(L
4, L
5) ,
DC
(L
4) ,
DL
(St
) M
(G
+ +
+ )
, D
L (
Ls)
, S
(L4,
Ls)
M
(G
+ +
+),
De
(SI)
, S
(L 4,
Ls)
R
M (
a +
+ +
), D
R (
St),
DC
(L
s),
S (L
3, L
4)
M (
G +
+ +
), D
R (
Ls)
, S
(Ls)
, D
C (
$1)
M (
G +
+),
DR
(L
s),
DR
(S1
) , S
(L
4, L
s)
(G +
+ +
), D
CR
(L
s, S
~)
M (
G +
+ +
), D
L (
Ls)
, S
(L5)
M
(G
+ +
+),
DL
(L
s),
S (L
s)
M(G
+ +
+),
DL
(L
s),
S (L
3, L
4, L
5),
DL
(S1
)
M (
G +
+ +
), D
L (
L5)
, D
L (
Sj),
S (
L 4,
Ls)
M
(a
+ +
), S
(L
4, L
s),
DL
(L
s)
(G +
), D
L (
Ls)
M
(G
+ 4
- +
), S
(L
3, L
4, L
5),
DL
(L
a),
DR
(S1
) (G
+ +
+),
S (
L 3,
L 4,
Ls)
M
(G
+ +
+),
DR
(L
s),
S (L
4, L
5)
(a +
), D
R (
Ls)
M
(G
+ +
+),
S (
L 4,
Ls)
, D
L (
Sl)
<< ('3
f~
ra,]
m C~
�9
o �9
Ph. Tsitsopoulos et al.: Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials
Table 2. Neurophysiological Findings (CSEP)
59
Case no. Patient 's height (cm) Preoperatively, latency common peroneal nerve
1 year postoperatively,
latency common peroneal nerve
right left right left
!. 170 42 46 41.5 43.4
2. 165 - - 31.2 - - 32
3. 160 30 36.6 32 32.1
4. 163 33.7 33 31.4 30.9
5. I65 32.2 35 32.4 33
6. I72 32.2 38.2 33.1 33.4
7. 160 31.2 29 31.2 30
8. 166 32 38 32 33.1
9. 170 44.2 - - 38.9 - - i0. 164 37 30 36 35
11. 165 29 32 36.2
12. 175 35.6 - - 36.2 38.2
13. 160 37.5 42.5 36.5 39
I4. 170 36.2 37 32 31
i5. 159 33.I 33.2 30 31
16. i65 37.3 36.2 3i 32
A
B
i lbzv + 20ms
Fig. 6. Case 6. The latency of the first positive wave for the left
common peroneal nerve was 38.2msec pre-operatively (A) and
33.4 msec post-operatively (B) one year later. Difference is not only seen in the latency but in the wave morphology as well
Discussion
Normal values of the latency of P1 in adults vary between 26 and 34 sec, as previous authors have also stated 12, 16, 17. Our results refer to these values.
These most valuable parameter used in the evalua- tion of the cortical SEPs is the latency of the first positive wave. Due to its variance, the waveforms (amplitude-duration) can not be used according to our experience and that of others 6 in the determination of
cortical SEPs changes. For this reason, in our study, we mainly evaluated the latency of the waveform while additional information was obtained in cases of charac- teristic changes of the waveform.
Stejkal in 1980 evaluated somatosensory evoked potentials in compressing syndromes of the cervical posterior roots. The percentage of the first positive wave latency and alteration in the waveform comparing our surgical and neurophysiological findings is 92%. The discrepancy recorded in the two cases with no neurophysiological deficit despite severe and signifi- cant surgical findings might be attributed to a large canal and foraminal dimensions resulting in no great neurological damage solar. That is why a less severe clinical picture was associated with normal neurophysi- otogical data despite the pronounced surgical lesions.
The duration and degree of root compression are responsible for the pathogenesis of degeneration which caused the increased latency and the waveform alterations.
The degree of compression and the extension of the level of its application (to more than one level) were important factors in the appearance of the latency. Thus, it was obvious that latencies of greater value appeared in combination with clinical symptoms of long duration, while root compression involved more than one level.
Tab
le 3
. C
ombi
ned
Lesi
ons
(Ste
nosi
s an
d D
iscs
)
Cas
e Pr
eope
rati
ve a
sses
smen
t
no.
Cli
nica
l fi
ndin
gs
l0
11
12
i3
15
16
i7
Neu
rolo
gica
l N
euro
phys
iolo
gica
l fi
ndin
gs
find
ings
righ
t le
ft
Surg
ical
con
firm
atio
n,
refe
r, t
o ro
ots
in d
isks
Post
oper
ativ
e as
sess
men
t
num
bnes
s, t
ingl
ing,
mot
or p
ower
inv
olv.
di
min
ishe
d se
nsat
ion,
mus
cle
wai
stin
g nu
mbn
ess
ting
ling
, m
otor
pow
er i
nvol
v.
dim
inis
hed
sens
atio
n, m
uscl
e w
aist
ing.
pa
in,
num
bnes
s, m
otor
pow
er i
nvol
v.
tens
ion
sign
s pa
in,
num
bnes
s, m
otor
pow
er i
nvol
v.
tens
ion
sign
s nu
mbn
ess
pain
, m
otor
pow
er i
nvol
v.
dim
inis
hed
sens
atio
n
pain
, nu
mbn
ess
ting
ling
, m
otor
pow
er i
nvol
v.
tens
ion
sign
s pa
in,
num
bnes
s, t
ingl
ing,
mot
or p
ower
inv
olv.
m
uscl
e w
aist
ing
(roo
ts)
L 5,
S I
(L)
42
46
L.
sura
lis
L 5,
S l
(RL
) --
31
.2
R.
sura
lis
L 5
(L)
30
36.6
L s
(R)
33.7
33
L 5
(L)
32.2
38
.2
refe
r, t
o in
terv
erte
br,
spac
es
in s
teno
sis
M(G
++
+)
S (L
4, L
s),
DC
L (
81)
M(G
++
+)
DC
(S
l) ,
S (L
4, L
S)
M(G
++
+)
S(L
4, L
s),
DL
(L
s)
M(G
++
+)
S (L
4,
Ls)
, D
R (
Ls)
M
(6+
+)
DL
(L
s),
S (L
4, L
5)
Neu
roph
ysio
logi
cal
Cli
nica
l ex
amin
atio
n fi
ndin
gs
pain
, nu
mbn
ess,
tin
glin
g, m
otor
pow
er i
nvol
v.
dim
inis
hed
sens
atio
n te
nsio
n si
gns,
mus
cle
wai
stin
g pa
in,
num
bnes
s ti
ngti
ng m
otor
pow
er i
nvol
v.
tens
ion
sign
s, d
imin
ishe
d se
nsat
ion
pain
, nu
mbn
ess
mot
or p
ower
inv
olv.
di
min
ishe
d se
nsat
ion
pain
, nu
mbn
ess,
tin
glin
g m
otor
pow
er i
nvol
v.
tens
ion
sign
s, m
uscl
e w
aist
ing
pain
num
bnes
s, t
ingl
ing,
mot
or p
ower
inv
olv.
di
min
ishe
d se
nsat
ion
pain
tin
glin
g, n
umbn
ess,
ten
sion
sig
ns
pain
, ti
ngli
ng,
num
bnes
s, t
ensi
on s
igns
pain
, ti
ngli
ng,
num
bnes
s, m
otor
pow
er
invo
lvem
ent,
dim
inis
hed
sens
atio
n
L 5
(R)
31.2
29
L4,
Ls,
S 1
(L)
32
38
L.
sura
lis
M(G
++
) S
(L 4,
L5)
DC
(L4
) D
R (
Ls)
M
(G+
++
) S
(L4,
Ls)
, D
C (
L4),
DL
(Sl
)
M(G
++
+)
Ls,
S
1 (L
) 44
.2
--
L. s
nral
is
Ls,
S 1
(R)
37
30
L4,
Ls,
S]
(R)
29
L4,
L
s, S
l (R
L)
35.6
--
R
. su
rali
s
L 5
(L)
37.5
42
.5
L 5
(L)
33.1
33
.2
L 5
(L)
37.3
36
.2
DL
(L
s),
S (L
4, L
5)
M(G
++
+)
DC
(S1
), S
(L4,
Ls)
R
M(G
++
+)
DC
(SI
), D
C (
L5,
S (L
3, L
4)
M(G
++
+)
DR
(L
s),
S (L
s) ,
DC
($1
) M
(G
++
) D
R (
Ls)
, D
R (
$1),
S
(L 4,
L5)
M
(G+
++
) D
L (
Ls)
, S
(L5)
M
(G+
++
) D
L (
Ls)
, S
(Ls)
righ
t le
ft
L5,
S l
(L)
30
39
L.
sura
lis
M(G
++
+)
DL
(L
s),
S (L
3, L
4, L
5)
DL
($1
)
41.5
43
.4
no i
mpr
ovem
ent
mus
cle
wai
stin
g --
32
no
im
prov
emen
t m
uscl
e w
aist
ing
32
32.1
im
prov
emen
t
31.4
30
.9
impr
ovem
ent
33.1
33
.4
impr
ovem
ent
min
or s
ensa
tion
di
stur
banc
e 31
.2
30
impr
ovem
ent
32
33.1
im
prov
emen
t m
inor
sen
sati
on
dist
urba
nce
mus
cle
wai
stin
g 38
.9
--
no i
mpr
ovem
ent
mus
cle
wai
stin
g 36
35
im
prov
emen
t
32
36.2
im
prov
emen
t
36.2
38
.2
impr
ovem
ent
mus
cle
wai
sfin
g
36.5
39
im
prov
emen
t m
inor
sen
sati
on
dist
urba
nce
30
31
impr
ovem
ent
31
32
impr
ovem
ent
not
re-e
xam
ined
no
t re
-exa
min
ed
.=r
c~
o �9 63
�9 P~
, t<
O'1
e~
(3
�9
~z
P~
o o
18
t9
21
23
25
pain
, ti
ngli
ng,
num
bnes
s, m
otor
pow
er i
nvol
v.
tens
ion
sign
s pa
in,
num
bnes
s, t
ingl
ing,
mot
or p
ower
inv
olv.
pain
, nu
mbn
ess,
ten
sion
sig
ns,
dim
inis
hed
sens
atio
n, m
otor
pow
er i
nvol
vem
ent
pain
, ti
ngli
ng,
num
bnes
s, t
ensi
on s
igns
, m
otor
po
wer
inv
olve
men
t, d
imin
ishe
d se
nsat
ion
pain
, ti
ngli
ng,
num
bnes
s, s
ensa
tion
dim
inis
hed,
m
otor
pow
er i
nvol
vem
ent
mus
cle
wai
stin
g
L5,
S I
(L)
35.5
36
.8
L4,
L 5
(L
) 29
35
.4
L3,
L 4
(R,
L)
52
42
Ls(
R)
L 5
, S
1 (L
) 42
L
. su
rali
s
M(G
++
+)
DL
(L
s),
DL
(Sj
), S
(L
4, L
s)
M(G
++
)
S (L
4, L
s),
DL
(L
s)
M(G
++
+)
S (L
3, L
4, L
s),
DE
(L
4) ,
DR
($1
) M
(G+
++
)
DR
(L
5),
S (L
4, L
s)
M(G
++
+)
S (L
4, L
s),
DL
(S1
)
not
re-e
xam
ined
no
t re
-exa
min
ed
not
re-e
xam
ined
not
re-e
xam
ined
not
re-e
xam
ined
not
re-e
xam
ined
not
re-e
xam
ined
no
t re
-exa
min
ed
not
re-e
xam
ined
not
re-e
xam
ined
not
re-e
xam
ined
not
re-e
xam
ined
c~
�9
�9
c~
7~
(3
�9
Tab
le 4
. P
rola
psed
Dis
cs
o
Cas
e P
reop
erat
ive
asse
ssm
ent
rl O
.
Cli
nica
l fi
ndin
gs
Pos
tope
rati
ve a
sses
smen
t
Neu
rolo
gica
l N
euro
phys
iolo
gica
l S
urgi
cal
Neu
roph
ysio
logi
cal
find
ings
fi
ndin
gs
conf
irna
atio
n ex
amin
atio
n (r
ef.
to r
oots
) re
f. t
o ro
ots
righ
t le
ft
righ
t le
ft
Cli
nica
l fi
ndin
gs
('3
g~
0~
pain
, nm
nbne
ss,
ting
ling
, m
otor
pow
er i
nvol
vem
ent,
di
min
ishe
d se
nsat
ion,
ten
sion
sig
ns
14
pain
num
bnes
s, m
otor
pow
er i
nvol
vem
ent,
di
min
ishe
d se
nsat
ion,
ten
sion
sig
ns
20
pain
, nu
mbn
ess,
mot
or p
ower
inv
olve
men
t,
dim
inis
hed
sens
atio
n, t
ensi
on s
igns
24
pa
in n
umbn
ess,
mot
or p
ower
inv
olve
men
t,
dim
inis
hed
sens
atio
n, t
ensi
on s
igns
L 5
(L)
32.2
35
G
+ +
+
32.4
33
im
prov
emen
t D
L (
Ls)
lo
w
back
pa
in
stil
l le
ft
L 5,
S 1
(R)
36.2
37
G
+ +
+
32
3t
impr
ovem
ent
DC
R (
L5,
Si)
L
5 (
L)
31
28
G +
no
t re
-exa
min
ed
DL
(L
s)
L 5
(R
) 29
30
,8
G+
no
t re
exam
ined
D
R (
Ls)
Sten
osis
(pu
re)
Cas
e P
reop
erat
ive
asse
ssm
ent
Pos
tope
rati
ve a
sses
smen
t
no
.
not
re-e
xam
ined
not
reex
amin
ed
�9
~z
t<
,<
o
Cli
nica
l fi
ndin
gs
Neu
rolo
gica
l N
euro
phys
iolo
gica
l S
urgi
cal
Neu
roph
ysio
logi
cal
Cli
nica
l fi
ndin
gs
find
ings
ref
. ro
ots
find
ings
co
nfir
mat
ion
exam
inat
ion
refe
r, t
o in
terv
erte
bffi
l ri
ght
left
sp
aces
ri
ght
left
�9
22
pain
, nu
mbn
ess,
tin
glin
g, m
otor
pow
er
L 4,
L 5
(R
, L
) --
35
G
+ +
+
not
re-e
xam
ined
no
t re
-exa
min
ed
invo
lvem
ent,
dim
inis
hed
sens
atio
n, t
ensi
on s
igns
S
(L3,
L4,
Ls)
62 Ph. Tsitsopoulos et al.: Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials
Latency of the Pl (first positive wave) was observed
in all cases o f m o t o r and sensory disturbances, while
muscle waisting correlated with a first positive wave
latency of greater value.
In cases where we were unable to record CSEPs,
severe degenerative lesions (osteophytes, thickened
l igamentum flavum and narrowing of the lumbar spinal
canal and foramina, or prot rus ion o f a large disc) were
present. Dur ing operation, severe compression of the
roots was f o u n d , which displaced and strangulated
before entering the foramina and were also adherent to
the pro t ruding disc.
An irreversible lesion (root damage) seemed possible
in a patient (case 9) who failed to give a response during
an a t tempt o f CSEP recording twelve months following surgery. Indeed, during the opera t ion a roo t lesion was
confirmed. A m o n g the eight (8) patients with central
disc protrusion, an increase in latency was recorded
bilaterally in one patient, latency on one side was found
in three patients, while an indefinite response was
obtained in another patient and latency on one side in
the last three. The above findings confi rm that central
disc protrusions have serious neurophysiological con-
sequences. More than that, in cases o f central disc
protrusion, the greater latency was recorded on the side
with the mos t severe roo t compression. Non- record ing
or recording of great latencies o f CSEPs contralateral ly
to the affected side, in four patients (cases 1, 11, 23, 25)
were mos t likely due to a combina t ion o f lesions (disc
w o t r u s i o n and stenosis) and displacement o f neural
structures (sleeve and roots). I t seems possible to us,
that the slight changes o f CSEPs recorded in two
patients, and regarded as normal according to general
criteria, cited previously, might have been regarded as
abnormal not only due to the large canal and foraminal
dimensions, as already discussed, but, additionally,
because these patients were shorter in stature than other
patients.
A definite improvement o f the latency was noticed
post-operat ively in all but three patients ment ioned
above. In one o f them the cause was a severe destructive lesion o f the root. In the rest o f the patients who showed
no improvement o f the neurophysiological picture, age (over 50) must be held responsible for this, as well as the long dura t ion o f symptoms (5-14 years) and the
presence o f muscle waisting.
Therefore, a possible prognosis regarding the out- come can be made in certain patients where neurophysi- ological informat ion is in agreement with clinical and
surgical data.
References
I. Anziska B, Cracco RQ, Cook AW, Feld EW (1978) Somato- sensory far-field potentials: studies in normal subjects and patients with multiple sclerosis. Electroencephalogr Clin Neu- rophysiol 45: 602-610.
2. Anziska B, Cracco RQ (1980) Short latency somatosensory evoked potentials: studies in patients with focal neurological disease. Electroencephalogr Clin Neurophysiol 49: 227-239.
3. Cracco RQ (1973) Spinal evoked responses: peripheral nerve stimulation in man. Electroencephalogr Clin Neurophysiol 35: 379-386.
4. Desmedt JE, Cheron G (1986a) Central somatosensory con- duction in man: neural generators and interpeak latencies of the far-field components recorded from neck and right or left scalp and earlobes. Electroencephalogr Clin Neurophysiol 50: 382- 403.
5. Dorfman LJ, Bosley TM, Cummins KL (1978) Electrophysiolog- ical localization of central somatosensory lesions in patients with multiple sclerosis. Electroencephalogr Clin Neurophysiol 44: 742-753.
6. Dorfman LJ, Perkash I, Bosley TM, Cummins K (1980) Use of cerebral evoked potentials to evaluate spinal somatosensory function in patients with traumatic and surgical myelopathies. J Neurosurg 52: 654-660.
7. Green JB, McLeod S (1979) Short latency somatosensory evoked potentials in patients with neurological lesions. Arch Neurol (Chic) 36: 846-851.
8. Jones SJ, Small DG (1978) Spinal and subcortical evoked potentials following stimulation of the posterior tibial nerve in man. Electroencephalogr Clin Neurophysiol 44: 299-306.
9. Macon JB, Poletti CE, Sweet WH, Ojemann RG, Zervas NT (1982) Conducted somatosensory evoked potentials during spinal surgery. Part2: Clinical applications. J Neurosurg 57: 354-359.
10. Mizrahi EM, Crawford ES (1984) Somatosensory evoked po- tentials during reversible spinal cord ischemia in man. Electroen- cephalogr Clin Nenrophysiol 58: 120-126.
11. Papakostopoulos D, Crow H (1980) Direct Recording of the Somatosensory Evoked Potentials from the Cerebral Cortex of Man and the Difference between Precentral and Postcentral Potentials. In: Desmedt JE (ed) Clinical uses of cerebral, brainstem and spinal somatosensory evoked potentials. Prog Clin Neurophysiol vol 7. Karger, Basel pp 15-26.
12. Rossini P, Cracco RQ, Cracco JB, House W (1981) Short latency somatosensory evoked potentials to peroneal nerve stimulation, scalp topography and the effect of different frequency filters. Electroencephalogr Clin Neurophysiol 52: 540-552.
13. Schramm J, Hashizume K, Fukushima T, Takahashi H (1979) Experimental spinal cord injury produced by slow, graded compression. Alterations of cortical and spinal evoked poten- tials. J Neurosurg 50: 48-57.
I4. Stejskal L (1980) Somatosensory evoked potentials in posterior root compression syndrome. Electoencephalogr Clin Neurophy- siol 48:56 p.
15. Tsitsopoulos Ph, Photiou Ph, Papakostopoul0s D, Athanasiadis D, Sitjoglou C, Tavridis G (1983) Cortical somatosensory evoked potential in patients with lumbar spinal stenosis and disc
Ph. Tsitsopoulos et al.: Comparative Study of Clinical and Surgical Findings and Cortical Somatosensory Evoked Potentials 63
protrusion. Proceedings ofX Panhellenic Congress of Neurology and Psychiatry, Vol II, pp 214-230, Thessaloniki.
16. Tsumoto T, Hirose N, Nonaka S, Takahashi M, (1972) Analysis of somatosensory evoked potentials to lateral popliteal nerve stimulation in man. Electroencephalogr Clin Neurophysiol 33: 379-388.
17. Vas GA, Cracco JB, Cracco RQ (1981) Scalp recorded short latency cortical and subcortical somatosensory evoked poten-
tials to peroneal nerve stimulation. Electroencephalogr Clin Neurophysiol 52: 1-8.
Authors' address: Dr. Ph. Tsitsopoulos, Department of Neuro- logical Surgery, Aristotelian University Thessaloniki Medical School, Thessaloniki, Greece. Dr. F. Fotiou, Clinic of Neurology and Psychiatry, Axepa Hospital Thessaloniki, Greece.
Related Documents


![Shape Analysis of Somatosensory Evoked Potentials to ... · factors directly into the spinal cord of immunized rats [1]. Somatosensory evoked potential (SEP) is a reliable electrophysiological](https://static.cupdf.com/doc/110x72/5f89ea2013c4ba6194512750/shape-analysis-of-somatosensory-evoked-potentials-to-factors-directly-into-the.jpg)








