Comorbidity of childhood balance and anxiety disorders: treatment and theory Ph.D. study by Orit Erez

Comorbidity of childhood balance and anxiety disorders: treatment and theory Ph.D. study by Orit Erez.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Comorbidity of childhood balance and anxiety disorders: treatment
and theory
Ph.D. study by Orit Erez
Comorbidity of balance and anxiety disorders
A recent special issue of the J. of Anxiety Disorders, reviewed the experimental and clinical findings related to comorbidity of balance disorders and anxiety (Sklare et al., 2001).
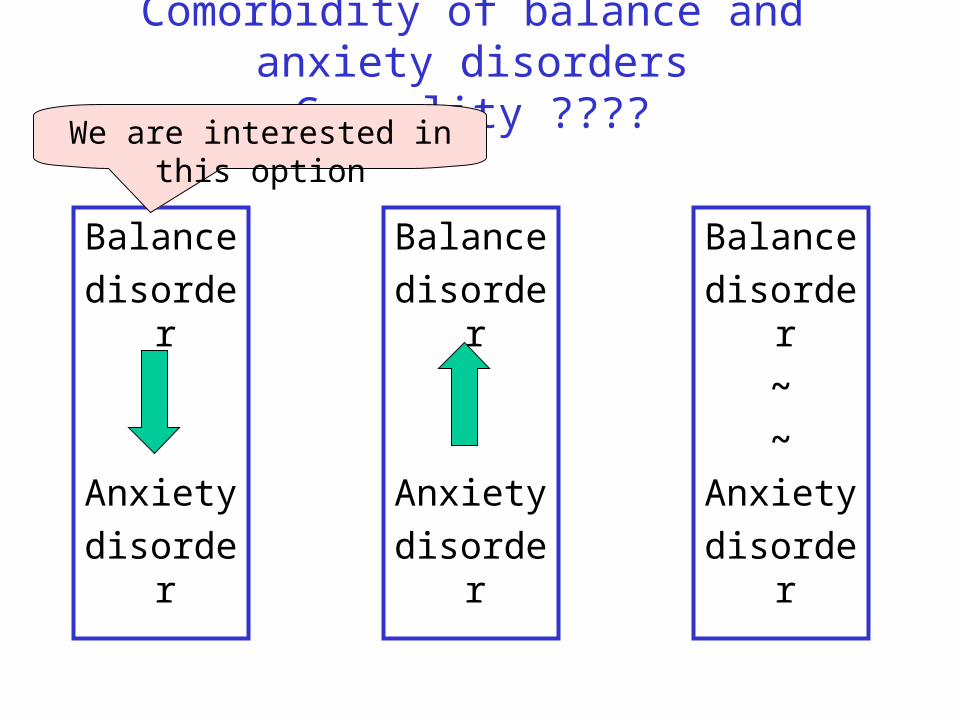
Comorbidity of balance and anxiety disorders Causality ????
Balance
disorder
Anxiety
disorder
Balance
disorder
~
~
Anxiety
disorder
Balance
disorder
Anxiety
disorder
We are interested in this option
Balance disorder as the origin of balance and anxiety comorbidity
Theoretical implication: Anxiety evolves from normal limbic system that responds excessively to interaction with deficient balance system.
Clinical implication: Successful balance treatment may ameliorate also the anxiety symptoms.
Checking for comorbidity in childhood
In children with anxiety as primary disorder.
In children with balance as primary disorder.
Comorbidity with anxiety as primary disorder
Is childhood anxiety associated with poor balance performance ?
( Erez et al., J. of Anxiety Disorders, 2003)
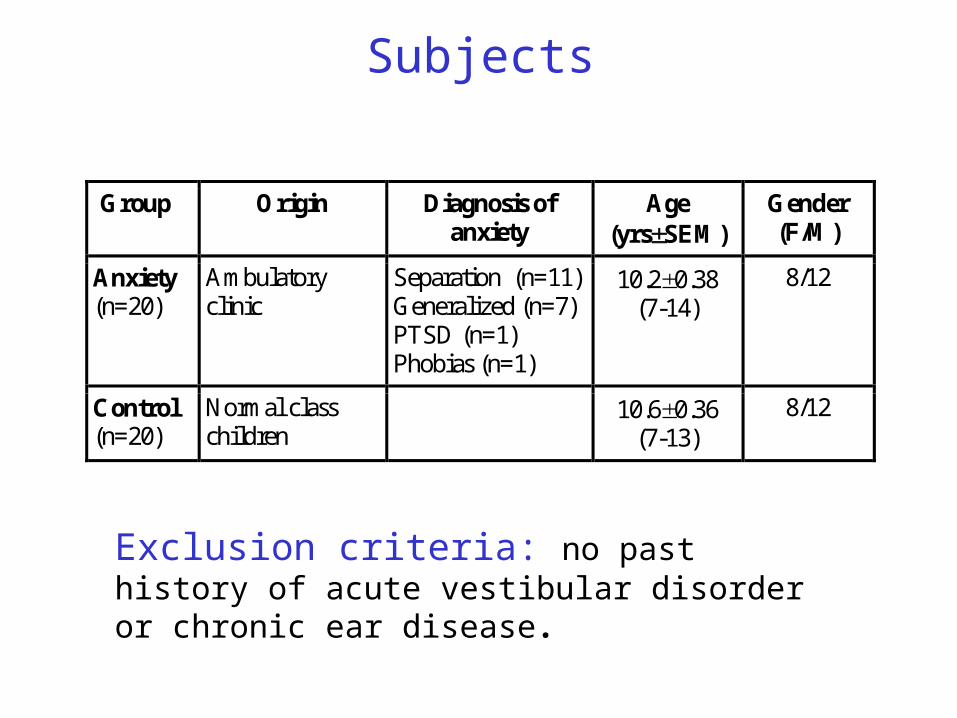
Subjects
Group Origin Diagnosis of anxiety
Age (yrsSEM)
Gender (F/M)
Anxiety (n=20)
Ambulatory clinic
Separation (n=11) Generalized (n=7) PTSD (n=1) Phobias (n=1)
10.20.38 (7-14)
8/12
Control (n=20)
Normal class children
10.60.36 (7-13)
8/12
Exclusion criteria: no past history of acute vestibular disorder or chronic ear disease.
Procedure in chronological order: DSM-IV based diagnosis of anxiety disorder by a
psychiatrist. Elevated anxiety confirmed on Fear Survey
Schedule for Children (FSSC; Ollendick, 1983). Neurological and neuro-otological examination by
a neurologist. Static and dynamic balance tests by a movement
therapist (Orit Erez). Dizziness & motion sickness questionnaires.
Results
Children with anxiety disorders vs. controls:
Reported more dizziness episodes (80 vs. 40%). Reported enhanced sensitivity to motion sickness
provoking situations. Were hypersensitive to the rotary chair test.

Children with anxiety disorders had more balance mistakes relative to controls
*p<0.05; **p<0.01; ***p<0.001
TestManipulation effectGroup effect
Interaction
G by M
Standheel-to-toe
Floor-bench ns Eyes open-closed **
nsnsns
Stand on one-foot
Floor-bench-trampoline *** Eyes open-closed ***
ns*ns
Stand on cylinder
Head still-nodding * *ns
Walk oncubicles
Eyes open-closed *** nsns
Walk onrope
Normal-heel-to-toe ***Eyes open-closed ***
*ns*
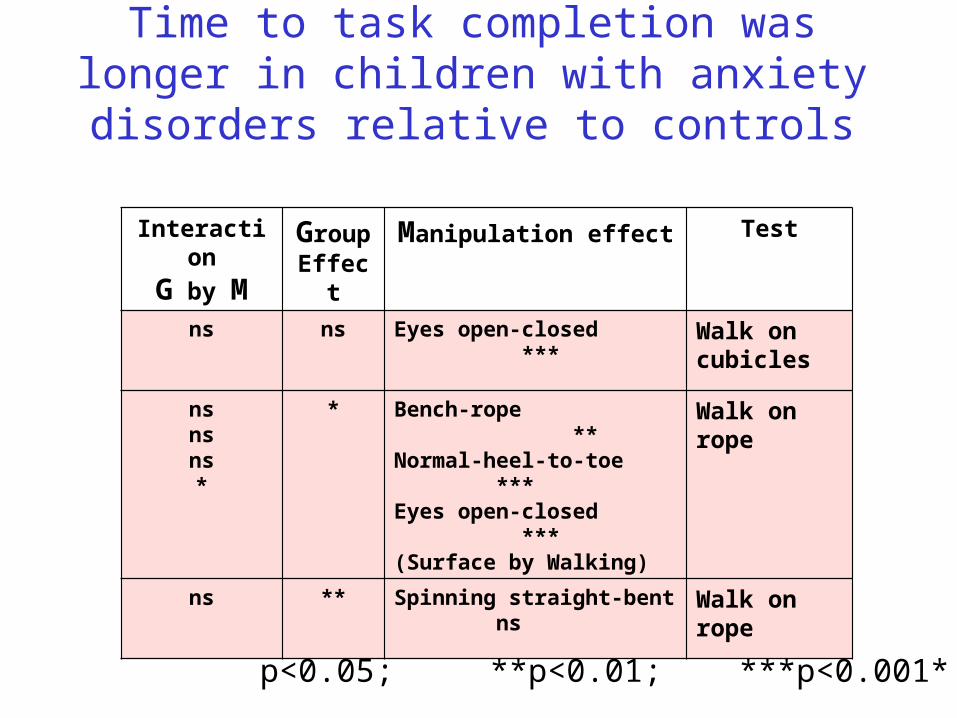
Time to task completion was longer in children with anxiety disorders relative to
controls
TestManipulation effectGroupEffect
Interaction
G by M
Walk oncubicles
Eyes open-closed ***nsns
Walk onrope
Bench-rope **Normal-heel-to-toe *** Eyes open-closed ***(Surface by Walking)
*nsnsns*
Walk onrope
Spinning straight-bent ns**ns
*p<0.05; **p<0.01; ***p<0.001
Is childhood anxiety associated with poor balance performance ?
Yes !!!
Comorbidity with balance as primary disorder
Are children with poor balance performance more anxious than normal controls?
Thesis by Moran Levin (2004)
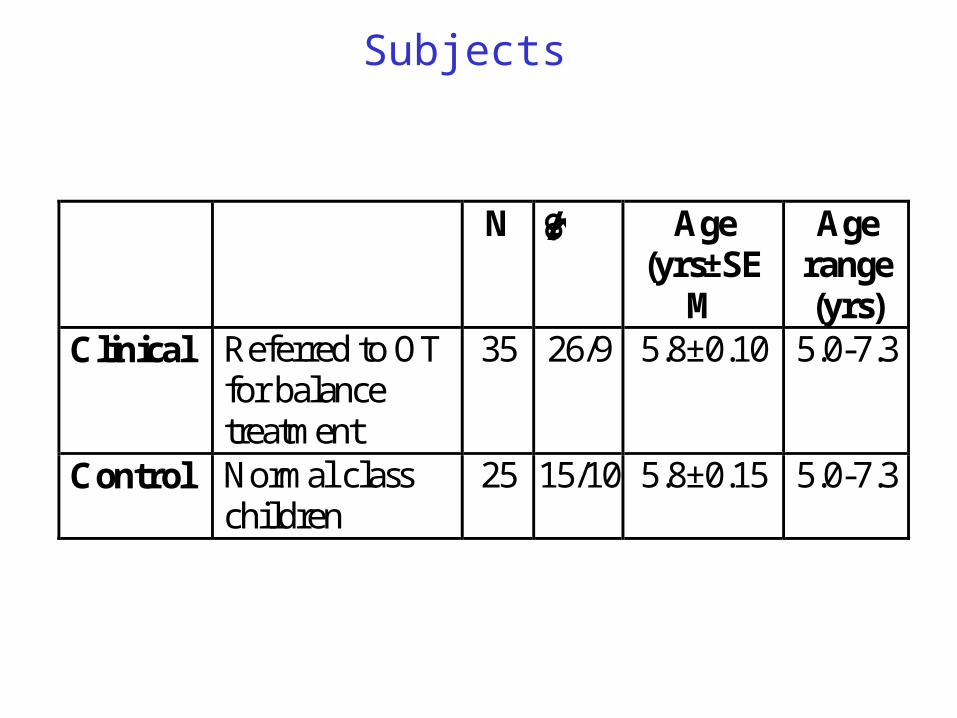
Subjects
N ♂/♀ Age (yrs±SE
M
Age range (yrs)
Clinical Referred to OT for balance treatment
35 26/9 5.8±0.10 5.0-7.3
Control Normal class children
25 15/10 5.8±0.15 5.0-7.3
Inclusion criteria in clinical group:< normal balance performance (Bruininks 1978).Normal schooling system.
Inclusion criteria in control group:No known balance difficulties.
Exclusion criteria:Tactile difficulties (Royeen & Fortune, 1990).Previous psychological or occupational therapies.No other major developmental problems.
Procedure in chronological order:Balance and anxiety were assessed upon arrival
at the clinic.Controls were tested at the school. Testing and treatment were administered by a
certified occupational therapist, experienced in
sensory integration techniques (Moran Meidan).
Balance tests: Balance sub-test of the Bruninks-Oseretsky Test of
Motor Proficiency (Bruninks, 1978).Vestibular scale of The Parental Sensory Profile
Assessment (Dunn, 1999).
Anxiety tests:Anxiety-Depression Parental Scale of the Child
Behavior Checklist (CBCL; Achenbach, 1991).Fear Survey Schedule for Children – self report
(FSSC; Ollendick, 1983).
Obvious result:
Clinical < Controls on balance tests; p<.001.
New result:
Clinical > Controls on anxiety tests; p<.001.
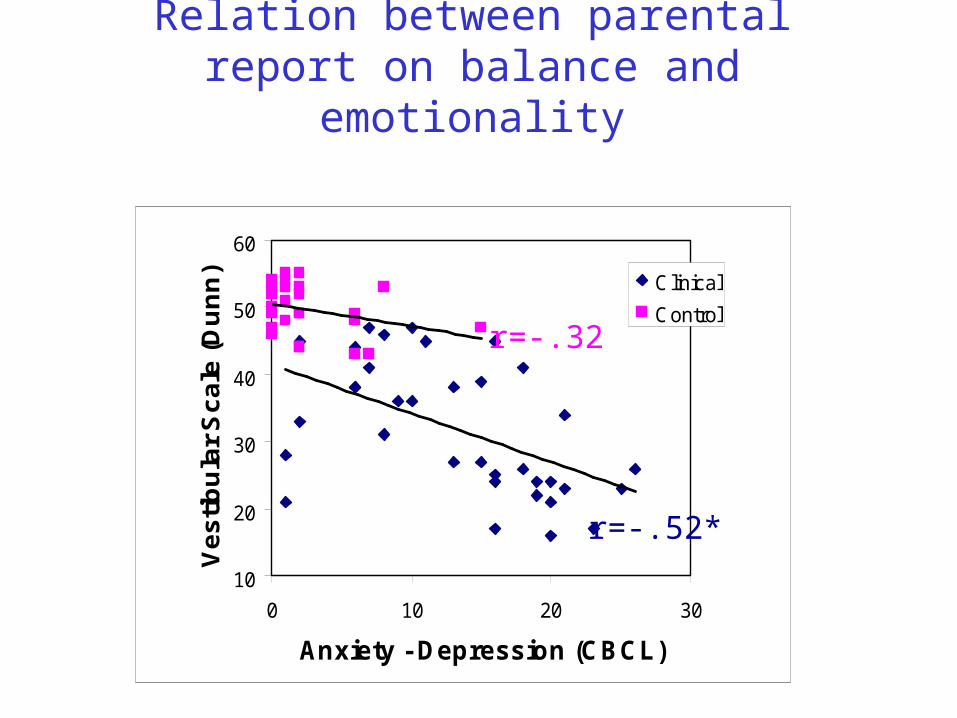
Relation between parental report on balance and emotionality
10
20
30
40
50
60
0 10 20 30
Anxiety - Depression (CBCL)
Ve
sti
bu
lar
Sc
ale
(D
un
n) Clinical
Control
r=-.32
r=-.52*
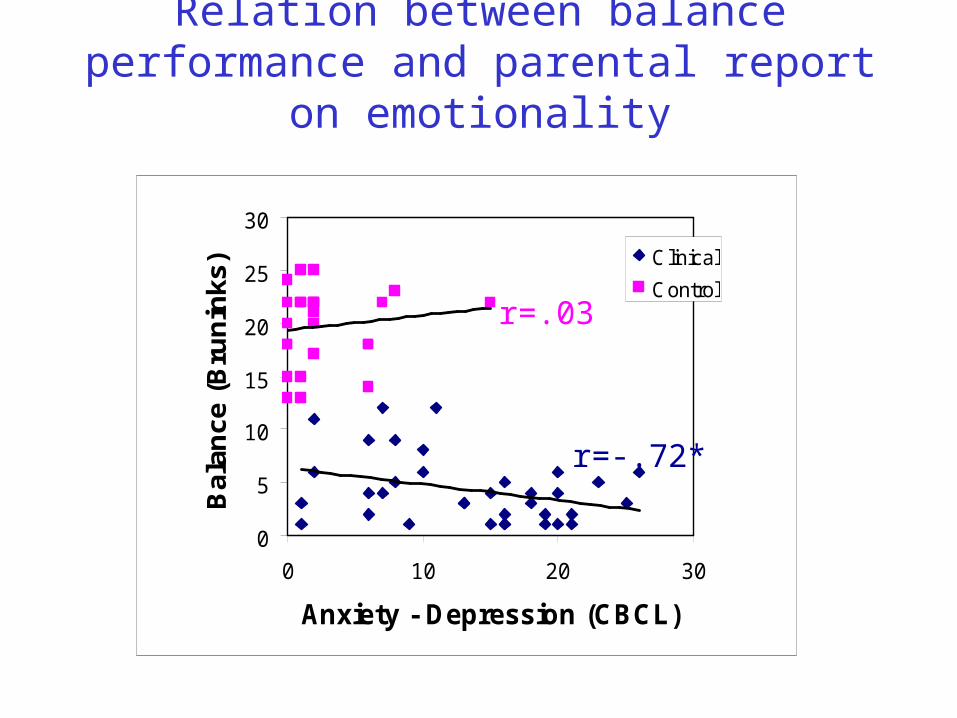
Relation between balance performance and parental report on emotionality
0
5
10
15
20
25
30
0 10 20 30
Anxiety - Depression (CBCL)
Bal
ance
(B
run
inks
) Clinical
Control
r=.03
r=-.72*
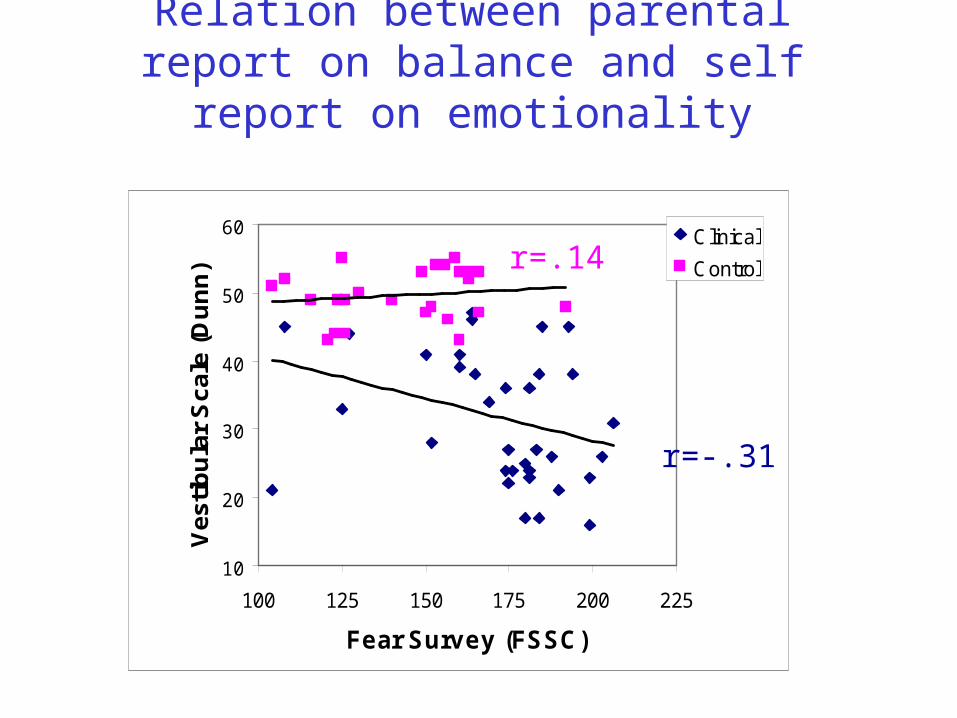
Relation between parental report on balance and self report on emotionality
10
20
30
40
50
60
100 125 150 175 200 225
Fear Survey (FSSC)
Ve
stib
ula
r S
cale
(D
un
n)
Clinical
Controlr=.14
r=-.31
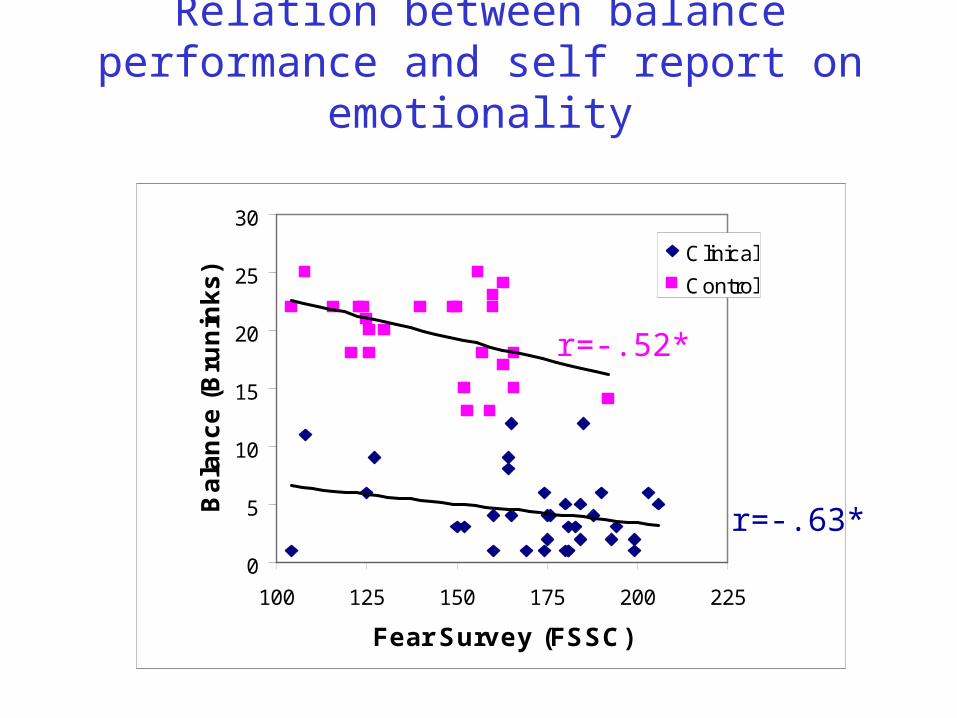
Relation between balance performance and self report on emotionality
0
5
10
15
20
25
30
100 125 150 175 200 225
Fear Survey (FSSC)
Ba
lan
ce
(B
run
ink
s)
Clinical
Control
r=-.52*
r=-.63*
Are children with poor balance performance more anxious than normal controls?
Yes !!!
Treatment of children with balance as primary disorder
and elevated anxiety
Can balance treatment alleviate the anxiety?
Thesis by Einat Karmon-Weisman (2004)
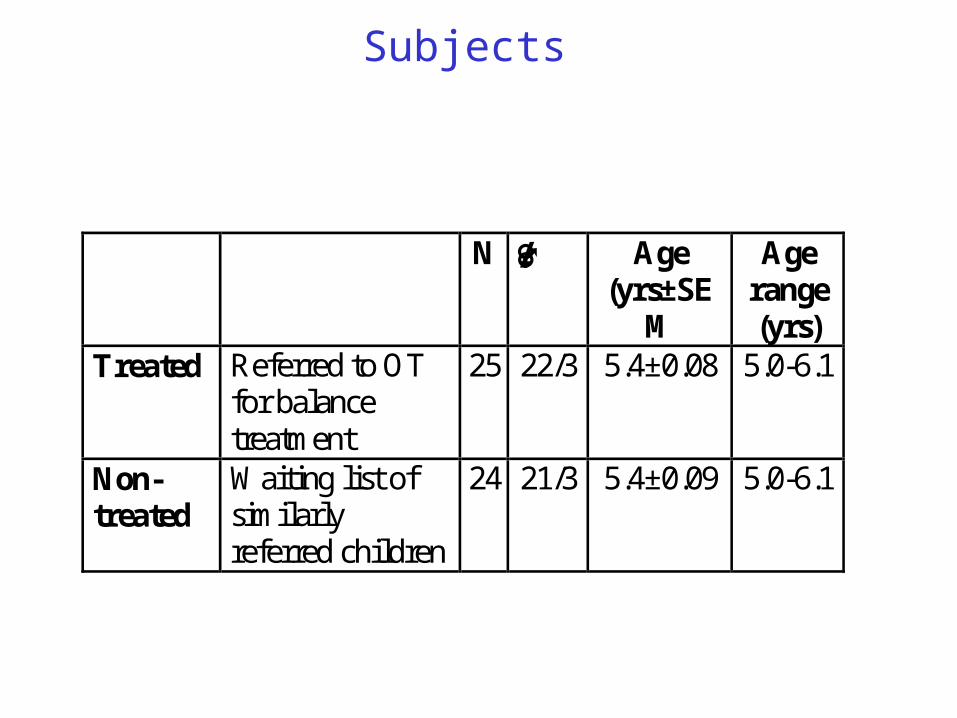
Subjects
N ♂/♀ Age (yrs±SE
M
Age range (yrs)
Treated Referred to OT for balance treatment
25 22/3 5.4±0.08 5.0-6.1
Non-treated
Waiting list of similarly referred children
24 21/3 5.4±0.09 5.0-6.1
Inclusion criteria:< normal balance performance (Bruininks 1978).> normal self report on Fear Survey (Ollendick, 1983).
Normal schooling system.
Exclusion criteria:Tactile difficulties (Royeen & Fortune, 1990).Previous psychological or occupational therapies.No other major developmental problems.
Procedure in chronological order:Balance and anxiety were assessed upon arrival at the clinic.Half of the children received 12 weekly sessions of OT with
sensory-motor orientation:
Improvement of flexor and tensor muscle tone.
Maintenance of balance in different postures.
Vestibular stim in various positions, speeds & intensities.Balance and anxiety were reassessed after the last treatment.Testing and treatment were administered by a certified
occupational therapist, experienced in sensory integration
techniques (Einat Veisman-Carmon).
Balance tests: Balance sub-test of the Bruninks-Oseretsky Test of
Motor Proficiency (Bruninks, 1978).Vestibular scale of The Parental Sensory Profile
Assessment (Dunn, 1999).
Anxiety tests:Anxiety-Depression Parental Scale of the Child
Behavior Checklist (CBCL; Achenbach, 1991).Fear Survey Schedule for Children – self report
(FSSC; Ollendick, 1983).
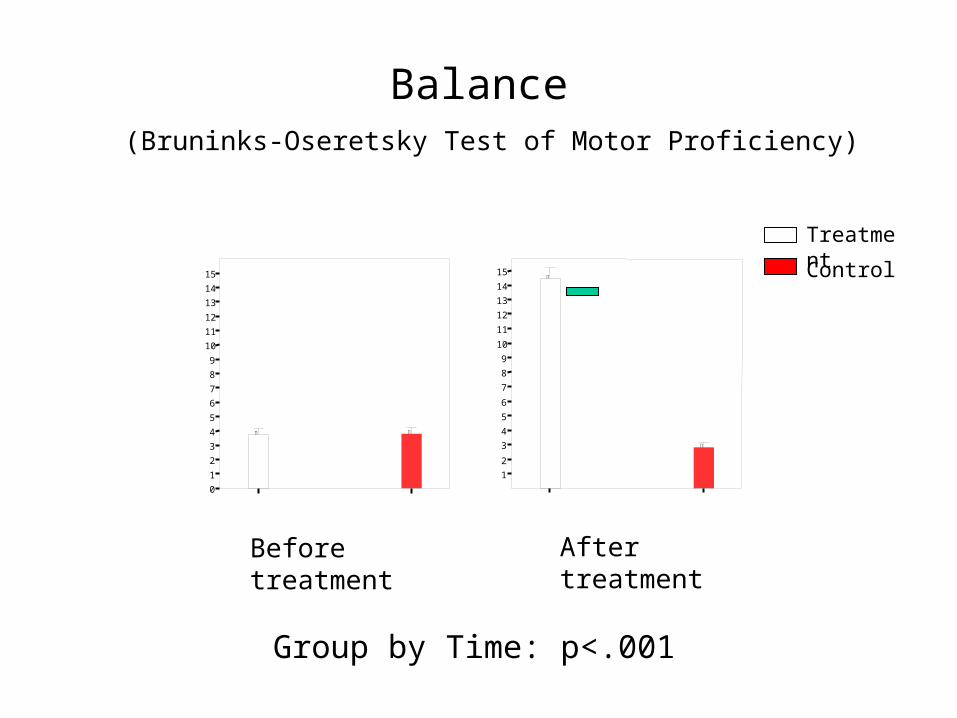
Balance(Bruninks-Oseretsky Test of Motor Proficiency)
12
3456789
101112131415
After treatment
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
Before treatment
Treatment
Control
Group by Time: p<.001
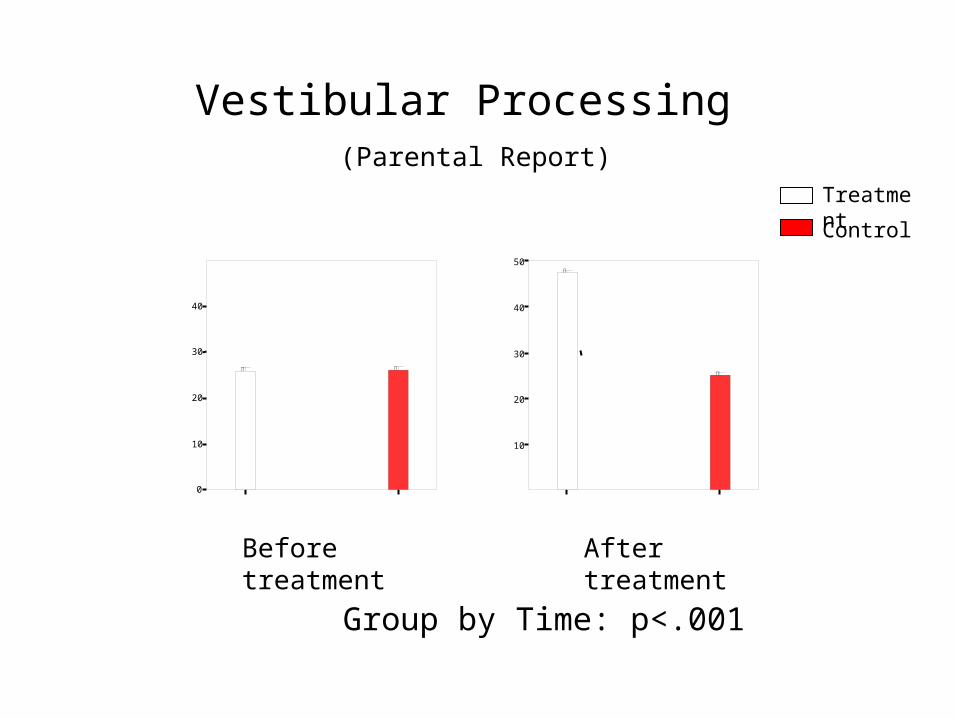
Vestibular Processing (Parental Report)
10
20
30
40
50
After treatmentBefore treatment
0
10
20
30
40
Treatment
Control
Group by Time: p<.001
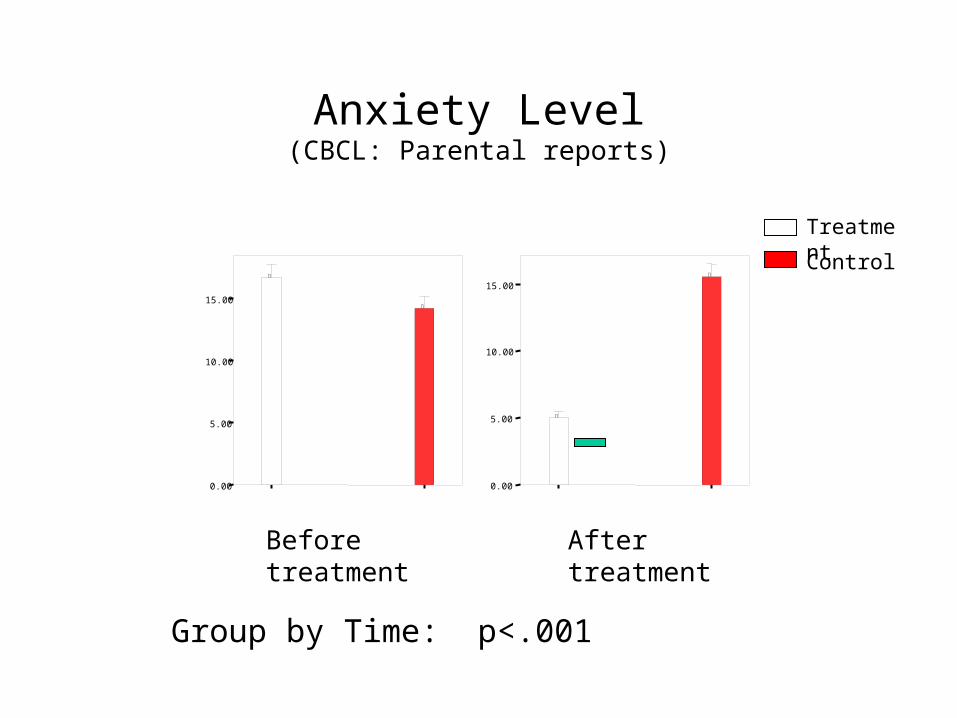
Anxiety Level(CBCL: Parental reports)
0.00
5.00
10.00
15.00
After treatment
0.00
5.00
10.00
15.00
Before treatment
Treatment
Control
Group by Time: p<.001
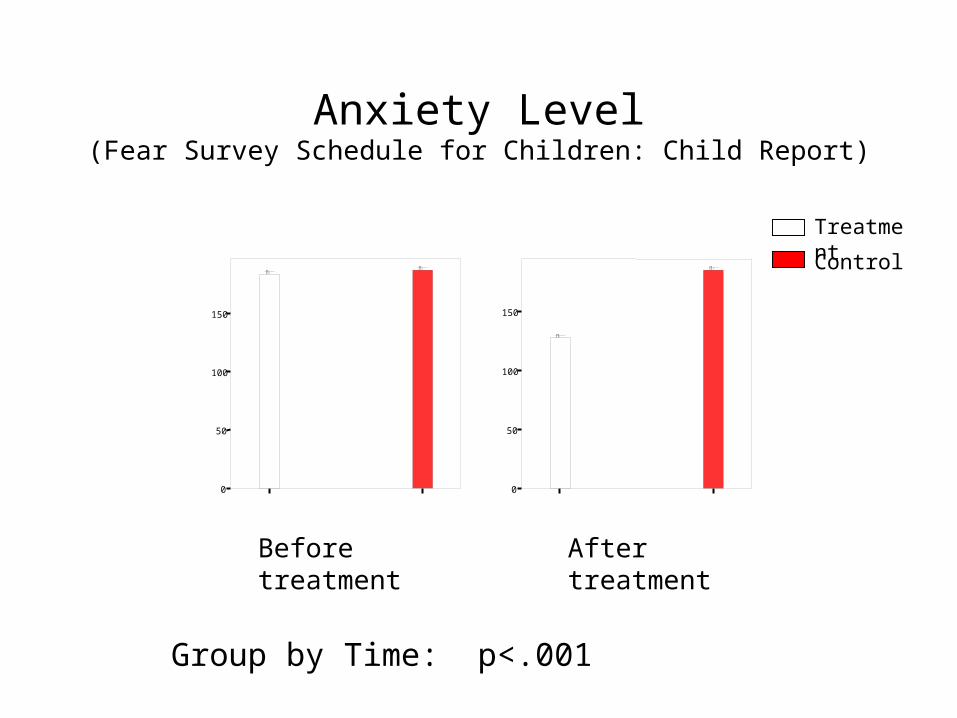
Anxiety Level(Fear Survey Schedule for Children: Child Report)
0
50
100
150
After treatment
0
50
100
150
Before treatment
Treatment
Control
Group by Time: p<.001
Can balance treatment alleviate the anxiety?
Yes !!!

Theoretical background:Normal individual facing an
aversive challenge
Two stage theory of learning predicts:
1st stage: Fast acquisition of fear response.
2nd stage: Slow acquisition of motor response.
Extension to three stage theory of learning:
3rd stage: Extinction of fear response after acquisition of motor response.
Theoretical background:Individual with balance disorder
facing balance challenging conditions
Three stage theory of learning predicts:
1st stage: Fast acquisition of fear response.
2nd stage: No acquisition of balance restoration motor response.
3rd stage: No extinction of fear response.
The next step: Treatment of children with anxiety as primary disorder and poor balance
Select a group of children with generalized or separation anxiety.
Test the group for comorbidity with balance deficiency.
Provide a 2-3 months physical balance training.
Test for improvement of balance skills.
Test for a short and long-term amelioration of anxiety symptoms.
Related Documents











