Roadmapping Report Community Services Research Priorities Roadmapping 22 July 2015 Workshop facilitated by the Institute for Manufacturing, Education and Consultancy Services, Cambridge Collaboration for Leadership in Applied Health Research and Care East of England Brain Injury Healthcare Technology Co-operative

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Roadmapping Report
Community Services Research Priorities Roadmapping
22 July 2015
Workshop facilitated by the Institute for Manufacturing, Education and Consultancy Services,
Cambridge
Collaboration for Leadership in Applied Health Research and Care East of England
Brain Injury Healthcare Technology Co-operative

2
Contents
1.0 Executive Summary ................................................................................... 3
2.0 Background ................................................................................................ 4
3.0 Objectives and Approach ........................................................................... 5
4.0 Landscape ................................................................................................. 7
4.1 Trends and Drivers ................................................................................. 7
4.2 Patient Impacts ....................................................................................... 7
4.3 Service Improvement ............................................................................. 8
4.4 Enabling Projects ................................................................................... 9
5.0 Selected Topic Development ................................................................... 10
5.1 Data management to support integrated care ...................................... 11
5.2 Identifying public perceptions and modifiable health psycho-social demographics ............................................................................................. 12
5.3 Personalisation and self-management ................................................. 14
5.4 Translation of research into community practice .................................. 15
6.0 Feedback and next steps ......................................................................... 17
Appendix 1- Attendees ............................................................................... 18
Appendix 2 - Populated Landscape (All) .................................................... 19
Appendix 3 - Landscape (Trends and Drivers) ........................................... 20
Appendix 4 – Landscape (Patient Impact) .................................................. 21
Appendix 5 - Landscape (Service Improvement)........................................ 22
Appendix 6 - Landscape (Enabling Projects) ............................................. 23
Appendix 7 - Prioritisation .......................................................................... 24
Appendix 8 - Topic Exploration-Template .................................................. 25
Appendix 9 - Topic Business Case (Research Proposal)-Template ........... 26
Appendix 10 - Topic Exploration: Data Management and integrated care . 27
Appendix 11 - Topic Exploration: Identifying public perceptions and modifiable health psycho-social demographics .......................................... 28
Appendix 12 - Topic Exploration: Personalisation and self-management ... 29
Appendix 13 - Topic Exploration: Translation of research into community practice ....................................................................................................... 30

3
1.0 Executive Summary The roadmapping workshop was designed to enable the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care East of England (NIHR CLAHRC EoE) and the National Institute for Health Research Brain Injury Healthcare Technology Cooperative (Brain Injury HTC) to explore regional research priorities for community providers and agree outline research proposals on key developmental areas. The workshop brought together thirteen delegates, representing community services trusts, commissioners, clinicians, research and development leads, and both academic and clinical (CLAHRC EoE) researchers. This built on a previous CLAHRC EoE event involving twenty delegates who identified broad areas of research interest for further investigation. The delegates identified a number of social, technological, economic, environmental, political and legal developments. It was also recognised that this work had to fit with the NHS England’s Five Year Forward Plan and the interest in transformation and innovation in relation to healthcare redesign to achieve more efficiency for the resources available. Following a group review of the trends and drivers, delegates reflected on possible research themes and enabling mechanisms (see appendix 1, page 18 for the full list). Delegates collectively ranked the importance of the opportunities identified and then voted on which to investigate further. Four areas were selected for further development: 1 Data management to support integrated care planning and
personalisation 2 Identifying public perceptions and modifiable health psycho-social
demographics 3 Personalisation and Self Management 4 Translation of research into the community practice Key outputs from the workshop were: • Four outline proposals developed for either submission to CLAHRC
EoE or other research funding sources • The identification of regional research priorities which will be used as a
reference point to inform CLAHRC EoE research priorities • An application to the CLAHRC EoE fellowship programme • Participants at the workshop feeding into current CLAHRC EoE funding
bids The outputs outlined in the full report will serve to drive forward future research collaborations and opportunities for community services within the Eastern Region.

4
2.0 Background The CLAHRC EoE collaboration encompasses some thirty-six NHS and social care organisations with researchers in the Universities of Cambridge, Hertfordshire and East Anglia working closely with individuals and organisations involved in the whole care pathway. CLAHRC EoE’s five year programme of health and social care research focuses on the health needs of people with complex problems (who are often vulnerable and have multiple agencies involved in their care). The roadmapping event built on a CLAHRC EoE workshop held in January 2015 which brought together community providers from across the Eastern Region. This was in recognition of CLAHRC EoE’s need to develop working relationships with community providers as a significant proportion of the region’s patients and service users are supported by these services. There was also no known history of collaboration between community providers in the region. Twenty representatives from four different community services providers, including medical directors, research development leads, Brain Injury HTC representatives and CLAHRC EoE researchers, attended this first workshop. It was an exploratory event which highlighted the potential for regional working and the need to identify the key research themes for community services to work on collaboratively. Challenges for the support and development of community based research and its dissemination and implementation across the region were also highlighted as areas which would benefit from CLAHRC EoE support. The roadmapping event was one of the action points taken forward jointly by CLAHRC EoE and the Brain Injury HTC to share and capture participant perspectives and to try and crystallise the priorities in ways which could either be supported by CLAHRC EoE or the Brain Injury HTC, or provide the infrastructure for bids to other funding sources.

5
3.0 Objectives and Approach In addition to participants from the first community services workshop held in January, other key representatives and organisations that were identified as key to the roadmapping process were also invited. This included delegates from UnitingCare Partnership, Patient and Public Involvement (PPI) and a commissioner representative. Thirteen people attended the event, representing community services and researchers from twelve different organisations (see page 18 for attendee details). The objective of the roadmapping event was to:
Collate research priorities regionally
To scope how to work together regionally
To provide a framework of research priorities for community providers
Outline research proposals and agree on key developmental areas Prior to the roadmapping workshop delegates were asked to identify short, medium and long term priority issues and actions. These were collated and transposed onto the landscape document prior to the event. The workshop was facilitated by the University of Cambridge Institute for Manufacturing (IfM) using the roadmapping methodology1. The roadmapping process is based on the following questions:
Why do we need to take action? What is needed to respond to these drivers identified? How should research and enabling projects address these?
Employing individual reflection and group discussion, the process generates information and ideas, and captures and develops these on a large wall chart (the visual format highlights the potential gaps, links, opportunities and challenges). These are then ranked via a voting process. Multiple layers are aggregated to identify linkages and clusters and therefore possible priorities for action by the group (or others). The layers within the community services research priority landscape were considered sequentially:
Why: Trends and drivers What: Patient experience and service improvement How: Research themes and enablers
1 Roadmapping is a technique – pioneered by Motorola in the 1970s – for planning an organisation’s
technological capabilities to ensure they meet its commercial or strategic goals. The graphical nature of roadmaps supports strategic alignment and dialogue between functions in the firm and between organisations. http://www.ifm.eng.cam.ac.uk/roadmapping/

6
Picture 1: Community Services Research Priority Landscape Delegates collectively ranked the importance of the opportunities identified and then voted on which to investigate further (see appendix 7, page 24). Having identified a number of priority opportunities via this method, delegates formed four groups, each tasked with taking forward one opportunity in the area of delegate expertise and interest. Each group developed a proposal for a research project using a ‘topic exploration’ template (see appendix 8, page 25) and roadmapping techniques to identify implementation issues. Roadmap charts were produced to capture the steps and timelines needed to implement change (these can be seen in appendices 10 to 13, pages 27 to 30).

7
4.0 Landscape The Landscape roadmap seen in appendix 2, page 19, covered: trends and drivers; service improvement; patient impact; and enabling projects and resources.
4.1 Trends and Drivers The first layer of the landscape (appendix 3, page 20) explored trends and drivers which were noted under the following headings:
STEEPL (social, technological, economic, environmental, political, legal developments)
Strategic healthcare context
NHS England strategy
Patient needs targets (Frail and elderly, rehabilitation, assistive technologies, wound care)
STEEPL A cluster identified by delegates was the policy imperative for real reduction in budgets; this was a current key economic driver in how research priorities should be framed. A technological driver included data that would be patient owned and more accessible across service pathways. Social and environmental drivers identified were care provision closer to home, integrated care across the service pathway, and equity of access to services both in rural and urban areas. Strategic healthcare context A key strategic need identified was the development of a research profile within community services. NHS England strategy Commissioning for outcomes was identified as key on the landscape. In addition, commissioning and the importance of NHS England’s Five Year Forward Plan was emphasised strongly. Patient needs targets Integrating mental and physical health services was highlighted as a prime driver for meeting patients’ health and social care needs.
4.2 Patient Impacts The second layer of the landscaping process (appendix 4, page 21) explored patient impacts which were noted under the following headings:
Decreased need for / demand upon services
Improved simplified access to services
Better tailored information
Reduced impact on informal carers
Other

8
Decreased need for / demand upon services Patient and public involvement was highlighted as a primary factor in understanding the use of services by patients. Improved simplified access to services The identification of modifiable health psycho-social demographics and the need to focus on the ‘at risk’ older population were documented as key to this patient impact priority. Reduce impact on family/unpaid carers Multiple localised solutions to integrated care was a driver recorded in this priority area. Cross-cutting drivers prioritised the role of personalisation and the self management of care, which by improved, simplified access to services and better tailored information could lead to a reduced impact on informal carers.
4.3 Service Improvement The third layer (appendix 5, page 22) examined service improvements which were noted under the following headings:
People (skills)
Processes (management)
Performance and modelling (KPI and metrics, data management)
Altering the allocation of community resources (District Nurses, Community Psychiatric Nurses, and Therapists etc.) was a cross-cutting driver recorded against both people skills and process management areas. Performance and modelling (KPI and metrics, data management) Using self-assessment data to show if services are / are not meeting patient needs, continuity of records / information (e.g. Out of hours), and data management to support integrated care planning and personalisation, were noted specifically under data management. The use of data could be used to monitor the translation of research into community practice through embedding this within service KPI’s and metrics.

9
4.4 Enabling Projects For the final layer (appendix 6, page 23) delegates mapped potential research and enabling projects and mechanisms against the following priority areas:
Organisation and organisation design
Processes (systematic reviews and evidence synthesis)
Technology, IT, communications (websites / databases)
Financial (care systems and models)
People and culture (information sharing) Organisation and organisation design Exploiting best practice benchmarks that were informed by evidence and the need to set up and exploit patient and public involvement were identified as important for achieving this priority area.
People and culture (information sharing) Understanding public perceptions of outcome versus experience, driving service improvement using data, and training and skills were recorded as key enablers. Cross-cutting themes identified as vital enablers for the processes, technology and financial priority areas were: data sharing and data quality; and assistive, remote, monitoring and management technologies.

10
5.0 Selected Topic Development Priority Voting Delegates voted on the priorities laid out on the landscape to select those topics for further development. The voting can be seen in appendix 7, page 24. Topic Exploration Using the topic exploration template (seen in appendix 8, page 25) groups were tasked with producing roadmap exploration plans (see appendix 10 to 13, pages 26 to 30 for completed examples). Business Case (research proposal) These were developed into a mini business case for each topic using the template in appendix 9, page 26. The primary focus of the discussion took forward the idea of integration and collaboration. Three out of the four proposals dealt with integration, whereas the fourth proposal focused on research relating to the implementation and uptake of evidence into practice. Completed Business Case (research proposals) are shown on pages 11 to 15.
Priority Voting
Topic Exploration
Business Case (research proposal)

11
5.1 Data management to support integrated care
There is a need/opportunity to maximise data collected to improve patient experience of navigating care from multiple providers because this is currently impenetrable for patients and carers. Actions to deliver include the identification of key features of a Minimum Data Set (MDS) adjusted by patient group and desired / required outcomes.
The business case for data management to support integrated care is detailed below:
Topic development proposal
In what ways does data integration improve patient outcomes (and resource use)?
Why should we do this?
To resolve issues of duplication and fragmentation and poor patient care
Required outcome and timing
Evidence of the key characteristics of a minimum data set to facilitate patient involvement and service evaluation
Current relevant projects or research
Integrated care pilots Comprehensive Geriatric Assessment (CGA) Vanguard Project Single Assessment Process (SAP) Care management / navigating Core Outcome Measures (COMET)
Staged deliverables and dates
Evidence review of how minimum data sets have been used to inform integrated care Case studies of where it has been implemented Recommendations / testable hypothesis? Development of a prototype to test – do more of this / less of that and how to evaluate it
Critical gaps How patients priorities can inform minimum data sets
Key Actions (Including Expertise to engage))
Nuffield / Health Foundation Commissioners Joint Strategic Needs Assessment (JSNA)
Other Enablers
Methodological
Other Barriers
Size and complexity

12
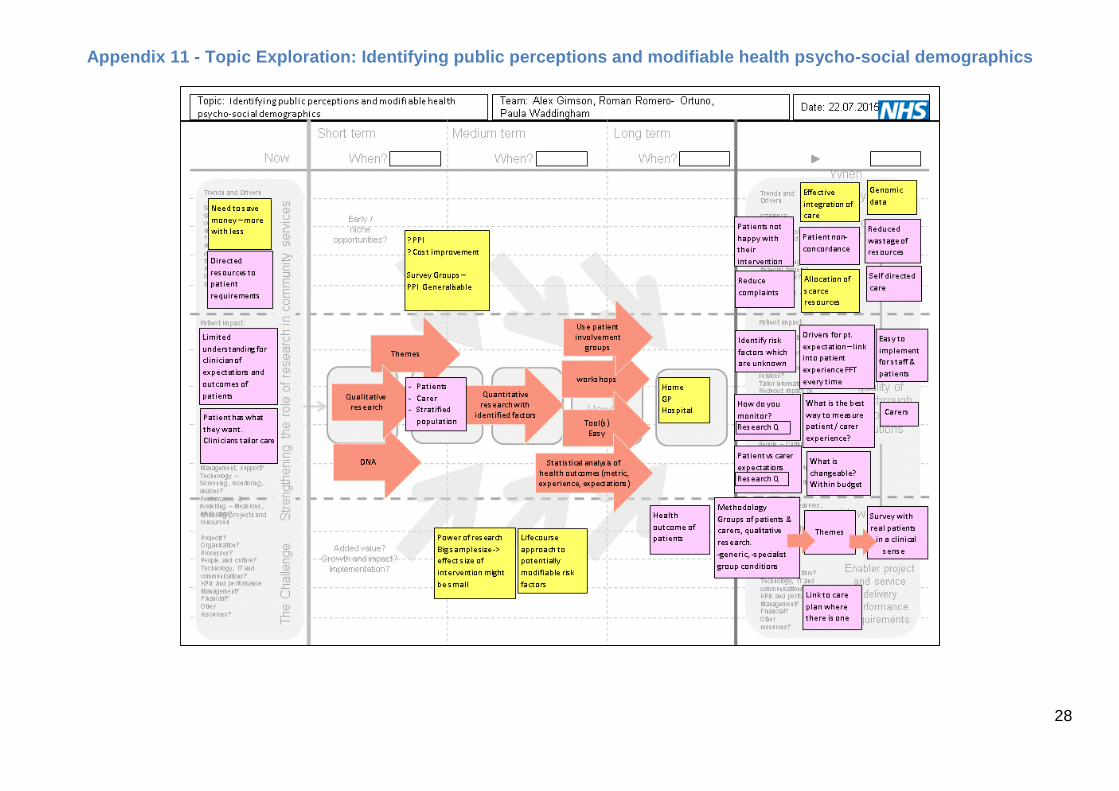
5.2 Identifying public perceptions and modifiable health psycho-social demographics
There is a need/opportunity for understanding variation in patient and carer expectations (patient experience / perceived outcomes) because we can tailor resources in a cost -effective and patient-centred way. Actions to deliver include:
Grant proposal
Research team - literature review - evidence synthesis - qualitative - quantitative / analytics
Collaborative adoption
Establishing a pilot
The business case for identifying public perceptions and modifiable health psycho-social demographics is detailed below:
Topic development proposal
What are the drivers for patient and carer expectations of future health, experiences of current health and health outcomes that might be modifiable?
Why should we do this?
To better allocate scarce resource to drivers that are potentially modifiable in order to have better health outcomes (expectation, experience, hard outcomes) from patient and carer perspective
Required outcome and timing
Survey tools applicable to various patient groups, age, ethnicities etc. with PPI validation, which are incorporated into clinical interaction / care plans / welcome pack
Current relevant projects or research
Current health literature on factors predicting outcome (A Bowling et al. Health Technology Assessment, 2012, Vol 16; 30).
Staged deliverables and dates
Stratify population by ‘triangle of care’ Qualitative resource to identify factors in patient expectation / experience Quantitative research using identified factors and other biological, psychological, social parameters Statistical analysis (multivariate / logistic regression) Longitudinal study Develop tool kit / risk score
Critical gaps Patient and carer experience unknown Impact of individual factors is known but not combinations Captured data not shared

13
Key Actions (Including Expertise to engage)
Engage with Public Health, MRC Biostatistics, experts in qualitative research methodology, ethnography, and Judge Business School.
Other Enablers Take DNA sample at first patient visit Research fellows with funding Web-based tools
Other Barriers Absence of shared data source that includes primary, secondary, mental health, community and social care

14
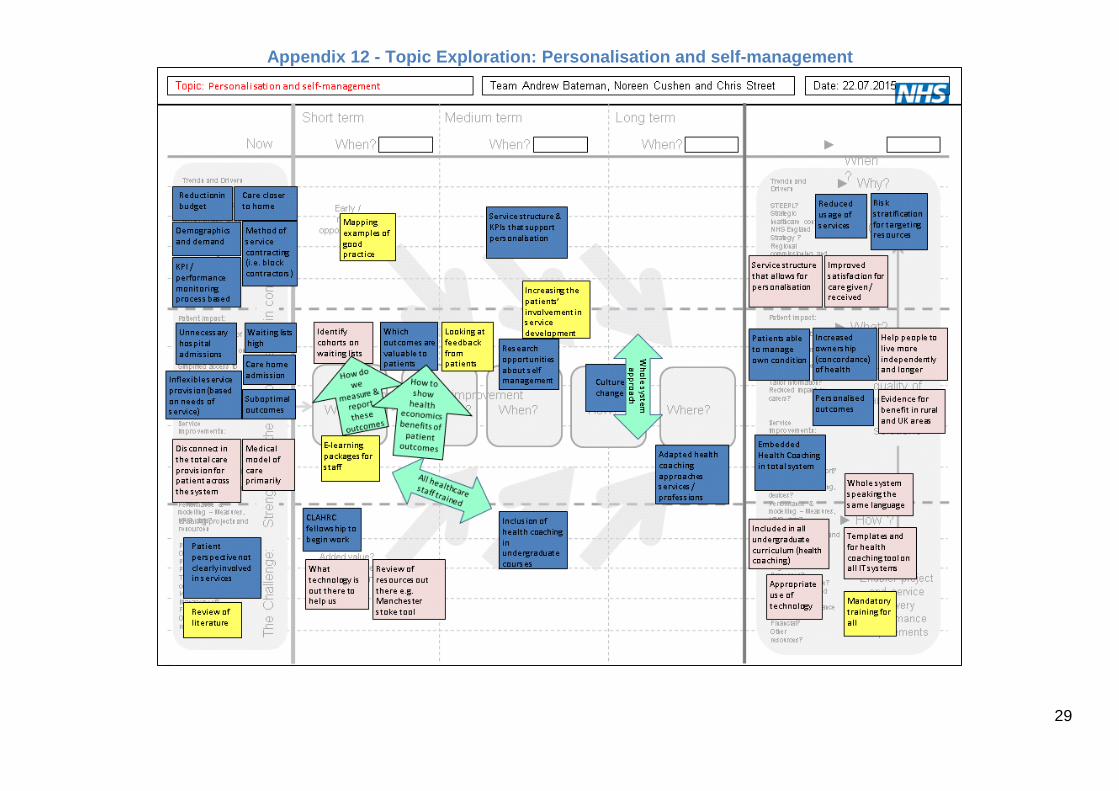
5.3 Personalisation and self-management
There is a need/opportunity for research that demonstrates benefits of personalisation / self-management in community services to support carers and families because this will improve patient experience, decrease use of resources, the demographic is passive and sustainability is challenged, and there is the potential for impact on care. Actions to deliver include studies to investigate this and resources for staff and patients (deliverables).
The business case for personalisation and self-management is detailed below:
Topic development proposal
Enabling self management through improved use of health coaching approaches
Why should we do this?
Optimise use of services and resources Improve patient experience by empowerment Manage impact of the demographic challenge
Required outcome and timing
Literature review and funding surveyed Knowing how to measure benefit Evidence of impact in variety of patient groups (e.g. physical, mental health, organisations) Availability of training and tools for patients and staff
Current relevant projects or research
Roll out of the Health Coaching evaluation Evaluation report of the East of England Existing work on computerised Cognitive Behaviour Therapy (CBT) National evaluation of health coaching
Staged deliverables and dates
Literature search and project proposal – August 2015 Mapping examples of good practice (e.g. by a CLAHRC EoE fellow) – 2016 Stakeholder network in place Benefits measure in place Availability of training
Critical gaps Absence of the 5 areas above
Key Actions (Including Expertise to engage)
Please see deliverables PPI groups
Other Enablers National projects? Research Associate / PhD students / Post Docs
Other Barriers Commissioning process and structure

15
5.4 Translation of research into community practice
There is a need/opportunity for the translation of research evidence into clinical practice in community services because we want to deliver quality, cost-efficient services to patients in the community. Actions to deliver include establishing how this happens and embody it in guidance for community services.
The business case for translation of research into community practice is detailed below.
Topic development proposal
To develop guidelines for implementing research into community practice
Why should we do this?
To reduce / eliminate wasted resources spent on un-evidenced practice To improve staff morale through better outcomes To improve patient and public experience of using services To support patient and public confidence in evidence based services
Required outcome and timing
Centralise existing information re implementation of research and create guidance that is relevant and accessible to community practitioners – by December 2018.
Current relevant projects or research
CLAHRC EoE research that has been implemented (to look at how). CLAHRC EoE literature on implementation (how to)
Staged deliverables and dates
Exploration stage by Sept 2016: identify barriers and enablers to implementation, literature review, patient experience/knowledge of using existing guidance e.g. NICE First draft of guidance by Jan 2017
Draft Implementation strategy Collect baseline data Pilot the draft guidance in local community services Analysis of pilot Final draft of guidance - by Dec 2018
Critical gaps Knowledge of current literature, Knowledge of existing implantation practice Board engagement in research implementation

16
Key Actions (Including Expertise to engage)
Form bid writing and connect with stakeholders Identify likely study co-ordinator and chief investigator Locate funding source(s) Submit bid application
Locate and cost in accommodation Identify service to involve (from April 2016) Stakeholder mapping (from April 2016)
Other Enablers
Qualitative researchers, health economist, research assistant, PPI reps/groups, budget holder and manager
Other Barriers Resource commitment from services (matched funding requirements).

17
6.0 Feedback and next steps Feedback on the workshop was very positive and delegates judged it as insightful and worthwhile. The preparation work supported the focus of the group to move quickly from ideas to proposal over a relatively short period of time. There was also acknowledgement of the importance of commissioner representation on the day and suggestion that third sector representation would be beneficial at any future events. The findings will be made available to research fellows who are currently applying for CLAHRC EoE funding. They will form a reference point both to those submitting but more importantly for the CLAHRC EoE Prioritisation Group when making decisions around which applications to fund. We also anticipate that this this will inform the future work of CLAHRC EoE, particularly when seeking to make closer working relationships with the community, commissioners and providers, as well as collaborations with other research partners.

18
Appendix 1- Attendees
Group Name Representing
Data Management to support integrated care
Claire Goodman Professor of Health Care Research CLAHRC EoE / University of Hertfordshire
Gary Barton Reader in Health Economics CLAHRC EoE / University of East Anglia
Nick Steel Clinical Reader University of East Anglia
Identifying public perceptions and modifiable health psycho-social demographics
Alexander Gimson Director, Health Analytics and Quality / Consultant Physician and Hepatologist
UnitingCare Partnership / Cambridge University Hospitals NHS Foundation Trust
Paula Waddingham Senior Research Fellow Cambridgeshire Community Services
Roman Romero-Ortuno Consultant in Care of the Elderly University Hospitals NHS Foundation Trust
Personalisation and self-management
Andrew Bateman Neuro Rehabilitation Clinical Lead, Director of Research The Oliver Zangwell Centre, Cambridgeshire Community Services NHS Trust
Chris Street Assistant Director - Medical Directorate Norfolk Community Health and Care NHS Trust
Noreen Cushen Deputy Director of Adult Services North East Coast Community Healthcare CIC
Translation of research into community practice
Elspeth Mathie Research Associate CLAHRC Patient and Public Involvement (PPI)Theme
CLAHRC EoE
Michelle Painter Psychosis Pathway Lead Cambridgeshire and Peterborough NHS Foundation Trust
Sally Anne Doyle-Caddick Research Delivery Lead Hertfordshire Community NHS Trust
Part-time attendance
Jacqui Bunce Associate Director East and North Herts CCG
Facilitation and support
Andrew Gill Facilitator Institute for Manufacturing Education and Consultancy Services
Angela Browne Business and Operations Manager CLAHRC EoE
Lorna Jacobs Senior Programme Support Officer CLAHRC EoE
Mita Brahmbhatt Programme Manager NIHR Brain Injury Healthcare Technology Cooperative
Peter Jarritt Deputy Director NIHR Brain Injury Healthcare Technology Cooperative

19
Appendix 2 - Populated Landscape (All)

20
Appendix 3 - Landscape (Trends and Drivers)

21
Appendix 4 – Landscape (Patient Impact)

22
Appendix 5 - Landscape (Service Improvement)

23
Appendix 6 - Landscape (Enabling Projects)

24
Appendix 7 - Prioritisation

25
Appendix 8 - Topic Exploration-Template

26
Appendix 9 - Topic Business Case (Research Proposal)-Template
Topic / Research Proposal Team:

27
Appendix 10 - Topic Exploration: Data Management and integrated care
28
Appendix 11 - Topic Exploration: Identifying public perceptions and modifiable health psycho-social demographics
29
Appendix 12 - Topic Exploration: Personalisation and self-management

30
Appendix 13 - Topic Exploration: Translation of research into community practice
Related Documents











