Community- Acquired Pneumonia SAMIR EL ANSARY

Community acquired pneumonia(2)
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Community-Acquired Pneumonia
SAMIR EL ANSARY

Objectives
Diagnosis and management of CAP
Differentiate between healthcare-associated pneumonia (HCAP) and CAP
Identify risk factors for resistant organisms and less common causes of pneumonia

CAP - Epidemiology
Very common
5 million cases/year in North America
At least 1 million hospitalizations/year
9th leading cause of infectious death in US
30 day morality for hospitalized patients is up to 23%
$17 billion/year in healthcare costs in US

Which of these patients have community-acquired pneumonia (CAP)?
34 yo hospital employee, previously healthy, admitted for acute pneumonia.
56 yo man admitted with CHF, noted to have pneumonia the day after admission.
76 yo bedridden man transferred from a nursing home for acute confusion, noted to have a new infiltrate on CXR.

Alphabet Soup of Terms
• CAP: Community-acquired pneumonia– Outside of hospital or extended-care facility
• HCAP: Healthcare-associated pneumonia– Long-term or extended care facility, hemodialysis, outpatient
chemo, wound care, etc.
• HAP: Hospital-acquired pneumonia– ≥ 48 h from admission
• VAP: Ventilator-associated pneumonia– ≥ 48 h from endotracheal intubation
What differentiates acute bronchitis (or other causes of fever/cough) from pneumonia : –Clinical definition requires chest imaging – air space disease.
HCAP includes the following patients with pneumonia: hospitalized in an acute care hospital for more than 2 days within 90 days of the pneumonia; resided in a long-term care facility (e.g., nursing home); received recent parenteralantimicrobial therapy, chemotherapy, or wound care within 30 days of pneumonia; or received treatment in a hospital or hemodialysis clinic.

Pneumonia - DefinitionsSpecturm of pneumonia.

Clinical Presentation
Acute cough (>90%)
Fevers/chills (80%)
Sputum production (66%)
Dyspnea (66%)
Pleuritic chest pain (50%)
Tachypnea (RR > 24)
Egophony
Bronchial breath sounds
Percussion dullness
Diminished breath sounds

Clinical Presentation
Acute cough (>90%)
Fevers/chills (80%)
Sputum production (66%)
Dyspnea (66%)
Pleuritic chest pain (50%)
Tachypnea (RR > 24)
Egophony
Bronchial breath sounds
Percussion dullness
Diminished breath sounds
Lung physical examSensitivity 47-69% ; Specificity 58-75%

CXR

To Admit or Not?Pneumonia Severity & Deciding Site of Care
Objective criteria to risk stratify & assist in decision re outpatient vs inpatient management
Pneumonia Severity Index (PSI)
CURB-65
Caveats
Other reasons to admit apart from risk of death
Not validated for ward vs ICU
Not validated in some populations (i.e. HIV+)





Criteria for Severe CAP(Admit to ICU)
Minor criteria
Respiratory rate ≥30 breaths/minPaO2/FiO2 ratio ≥ 250Multilobar infiltratesConfusion/disorientationUremia (BUN ≥20 mg/dL)Leukopenia (WBC <4000 cells/mm3)Thrombocytopenia (platelets <100,000 cells/mm3)Hypothermia (core T <36C)Hypotension requiring aggressive fluid resuscitation
Major criteria
Invasive mechanical ventilationSeptic shock with the need for vasopressors

Microbiology
TYPICAL
– Streptococcus pneumoniae
– Haemophilus influenzae
– Moraxella catarrhalis
– Klebsiella pneumoniae
ATYPICAL
– Mycoplasma pneumoniae
– Chlamydophila pneumoniae
– Legionella pneumophila
2/3 are typical; 1/3 are atypical

Microbiology of CAP among hospitalized patients
Outpatient Streptococcus pneumoniae
Mycoplasma pneumoniae
Haemophilus influenzae
Chlamydophila pneumoniae
Respiratory viruses
Inpatient (Ward) S. pneumoniae
M. pneumoniae
H. influenzae
C. Pneumoniae
Legionella species
Respiratory viruses
Aspiration
Inpatient (ICU) S. pneumoniae
Legionella spp.
Staphylococcus aureus
Gram-negative bacilli

Age-specific Rates of Hospital
Admission by Pathogen
Marsten. Community-based pneumonia incidence study group.Arch Intern Med 1997;157:1709-18
Two-thirds of deaths due to a known CAP pathogen is due to Strep pneumoniae.
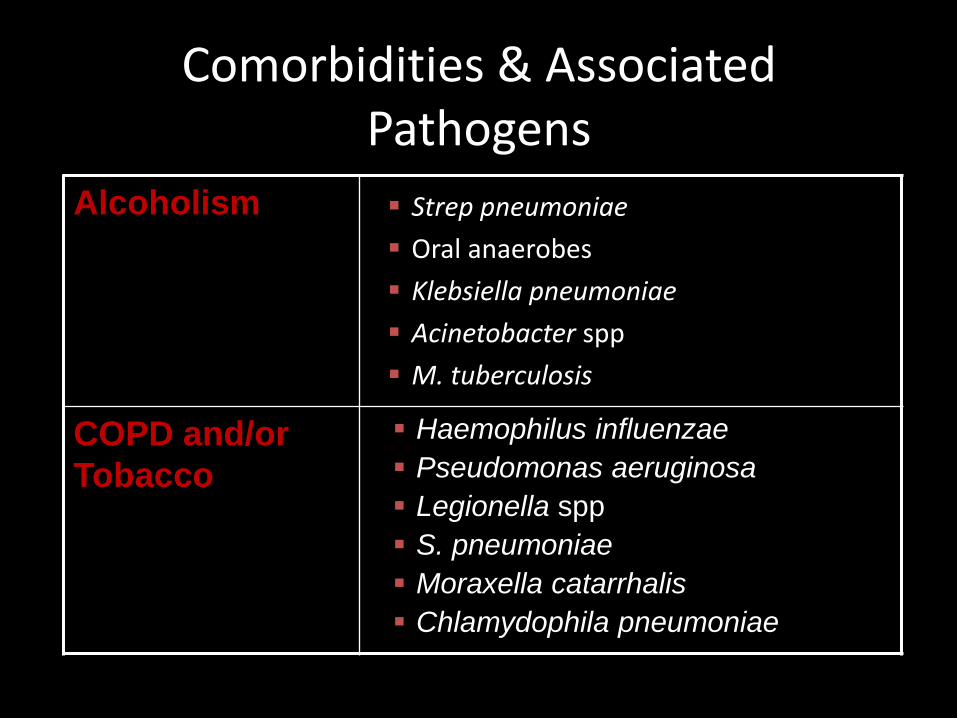
Comorbidities & Associated Pathogens
Alcoholism
COPD and/or
Tobacco
Strep pneumoniae
Oral anaerobes
Klebsiella pneumoniae
Acinetobacter spp
M. tuberculosis
Haemophilus influenzae
Pseudomonas aeruginosa
Legionella spp
S. pneumoniae
Moraxella catarrhalis
Chlamydophila pneumoniae
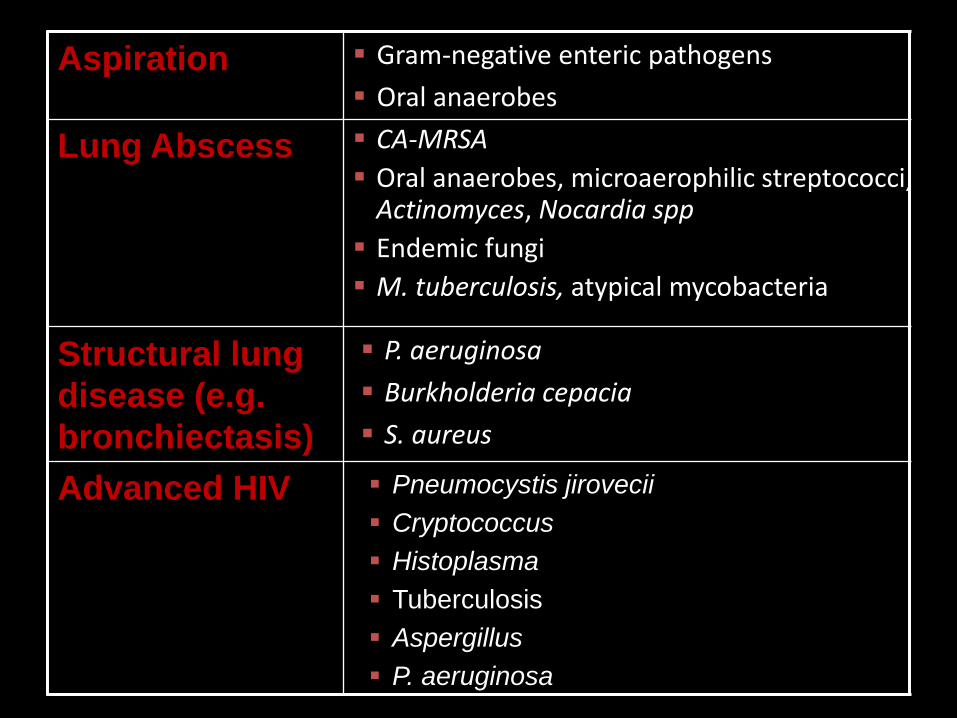
Aspiration
Lung Abscess
Structural lung
disease (e.g.
bronchiectasis)
Advanced HIV
Gram-negative enteric pathogens
Oral anaerobes
CA-MRSA
Oral anaerobes, microaerophilic streptococci, Actinomyces, Nocardia spp
Endemic fungi
M. tuberculosis, atypical mycobacteria
P. aeruginosa
Burkholderia cepacia
S. aureus
Pneumocystis jirovecii
Cryptococcus
Histoplasma
Tuberculosis
Aspergillus
P. aeruginosa

MRSAModern-day CAP pathogen
Must consider MRSA, MSSA coverage in severe CAP, esp during flu season!

MRSA CAPClinical Features
Cavitary infiltrate or necrosis
Rapidly increasing pleural effusion
Gross hemoptysis (not just blood-streaked)
Concurrent influenza
Neutropenia
Erythematous rash
Skin pustules
Young, previously healthy patient
Severe pneumonia during summer months

Is sputum culture helpful?
Sputum Gram stain and culture
Low sensitivity (25-40%)
Considered optional for outpatients
Blood culture
Positive < 10%
May help guide antibiotic therapy
Diagnosis: Cultures
Pre-abx Blood Cultures
Yield 5-15%
Stronger indication for severe CAP
Host factors: cirrhosis, asplenia, complement deficiencies, leukopenia
Only 25-30% can actually provide a decent expectorated sample.Endotracheal aspirate: Intubated patients who were too sick to be
able to produce sputum.

Diagnosis: Cultures
Pre-abx expectorated sputum Gs & Cx
Yield can be variable
Depends on multiple factors: specimen collection, transport, speed of processing, use of cytologic criteria
Adequate sample
Pre-abx endotracheal aspirate Gs & Cx
Pleural effusions > 5 cm on lateral upright CXR
Diagnosis: Other testing
Urinary antigen tests
S. pneumoniae
L. pneumophila serogroup 1
60-80% sensitive, >90% specific in adults
Pros: rapid (15 min), simple, more sensitive than Cx, can detect Pneumococcus after abxstarted
Cons: no susceptibility data, not helpful in patients with recent CAP (prior 3 months)

Diagnosis: Other testing
• Acute-phase serologies–C. pneumoniae, Mycoplasma, Legionella
spp
–Not practical given slow turnaround & single acute-phase result unreliable

Diagnosis: Other testing
• Influenza testing– Hospitalized patients: Severe respiratory illness (T> 37.8°C with
SOB, hypoxia, or radiographic evidence of pneumonia) without other explanation and suggestive of infectious etiology should get screened during season
– NP swab or nasal wash/aspirate
– Rapid flu test (15 min) - Distinguishes A vs B
• Sensitivity 50-70%; specificity >90%
– Respiratory virus DFA & culture - reflex subtyping for A
– Respiratory viral PCR panel - reflex subtyping for A
– Epidemic Influenza PCR panel – screens for A & B with reflex subtyping for A

Outpatient Empiric CAP Abx
• Healthy; no abx x past 3 months– Macrolide: azithromycin
– 2nd choice: doxycycline
• Comorbidities; abx x past 3 mon– Respiratory fluoroquinolone: Moxifloxacin, levofloxacin 750
mg, gemifloxacin
– Beta-lactam (preferred: amoxicillin 1 g3 or amox/clav 2 g2; alternative: ceftriaxone, cefuroxime 500 mg2), + macrolide
• Regions with >25% high-level macrolide-resistant S. pneumo(MIC ≥16), consider alternative agents

Inpatient Empiric CAP Abx1
• Inpatients in ward
– Respiratory fluoroquinolone
– ß-lactam (cefotaxime/ceftriaxone or ampicillin/sulbactam) + macrolide
• Inpatients in ICU
– ß-lactam + macrolide
– Respiratory fluoroquinolone for PCN-allergic pts

Inpatient Empiric CAP Abx1
• Pseudomonas (if concerns exists)
– Anti-pneumococcal & anti-pseudomonal ß-lactam + azithromycin + cipro/levofloxacin (750 mg)
– Can substitute quinolone with aminoglycoside
– PCN-allergic: can substitute aztreonam
• CA-MRSA: Add vanco or linezolid* (or ceftaroline2)
• CA-MSSA: Nafcillin or cefazolin or ceftriaxone

Risk Factors for Multidrug Resistance (MDR)
Antibiotics in the past 90 daysHigh frequency of antibiotic resistance in communityImmunosuppressive disease or medicationsHCAP Risk Factors:• Hospitalization for at least 2 days in the past 90 days• Residence in a SNF• Home infusion therapy• Dialysis within 30 days• Family member with MDR infection


Influenza pneumoniaTreatment
First-line Tx is neuroaminidase inhibitors for both
influenza A and B:
Oseltamavir 75-150* mg PO BID x 5+ days
Zanamavir 10 mg INH BID x 5+ days
NOTE: influenza A resistant to adamantanes
(amantadine, rimantadine)
* There is limited data in support of double dosing. But we do it anyway.

Antiviral Therapy for Influenza
CDC Guidelines for Influenza 2012-2013
Should be started ASAP in:
Anyone hospitalized with suspected or confirmed
influenza
Anyone with severe, complicated or progressive
respiratory illness
Anyone at higher risk of complications from influenza

Individuals at Higher Risk for Influenza Complications
CDC Guidelines for Influenza 2012-2013
• Extremes of age: children <2, adults ≥65 years
• Comorbid conditions:
– Chronic pulmonary
– Cardiovascular (except HTN alone)
– Renal, hepatic, hematologic, metabolic (DM)
– Neurologic, neuromuscular (cerebral palsy, epilepsy, CVA, SCI)
• Immunosuppression (caused by meds, HIV infection)
• Pregnant or post-partum (<2 wks) women
• Persons <19 years on long-term aspirin
• American Indians & Alaskan Natives
• Morbidly obese (BMI ≥40)
• Residents in NH or chronic-care facilities

Influenza pneumoniaWhat about the 48-hr rule?
Antiviral treatment within 48 hrs
Reduce likelihood of lower tract complications & antibacterial use in outpatients
Hospitalized patients likely benefit even if started up to 3-5 days from illness onset
Additional exceptions to <48 h rule:
Immunocompromised patients
Severe, complicated or progressive illness

Follow-up ResponseExpected improvement?
Clinical improvement w/ effective abx: 48-72 hrs
Fever can last 2-5 days with Pneumococcus, longer with other etiologies, esp Staph aureus
CXR clearing
If healthy & <50 yo, 60% have clear CXR x 4 wks
If older, COPD, bacteremic, alcoholic, etc. only 25% with clear CXR x 4 wks
Switch from IV to PO
Hemodynamically stable, improving clinically
Able to ingest meds with working GI tract

Question…
What is far & away the most common reason for non-response to antibiotics in CAP?
1. Cavitation
2. Pleural effusion
3. Multilobar involvement
4. Discordant antibiotic/etiology
5. Host factors

•
• A 58 y/o man with advanced liver disease,
construction worker in outdoor excavation
• C/O acute fever, cough, pleuritic chest pain,
WBC 23,000.
• CXR and chest CT show RML nodule. No
response to Unasyn + Levo.
• Concern for pneumococcal pneumonia.


Coccidioides immitis
- Endemic to the desert southwest
- Dissemination more common in non-Caucasians, pregnant, immunocompromised
- Acute & chronic pulmonary syndromes (“valley fever”—fever, cough, arthralgias, Erythema nodosum)
- Diagnosis based on serology, culture, or histopathology
NW Infections: Coccidioides

Exposures & Associated Pathogens
Hotel or cruise ship, built water
sources
Travel or residence in SW US
Travel or residence in SE or E
Asia
Travel or residence in Arabian
Peninsula
Influenza active in community
Cough >2 wks with whoop or
posttussive vomitting
Legionella spp
Coccidioides spp
Hantavirus pulmonary syndrome (Sin Nombre virus)
Burkolderia pseudomallei
Avian influenza A (H7N9)
MERS-CoV
Bordetella pertussis
Influenza
S. pneumoniae
Staph aureus (MSSA, MRSA)
H. influenzae
- Legionella: 1-5% CAP. L. pneumophila serogroup 1 responsible for 70-90%. U Ag(+) – contact Micro lab; specialized testing/media.
- Sin Nombre virus: activity put you in contact with rodent droppings, urine, saliva, nesting matter.
- B. pertussis rarely causes pneumonia in adults

Zoonotic Exposures & Associated Pathogens
Bat or bird
droppings
Histoplasma capsulatum
Birds Chlamydophila psittaci
Avian influenza (H7N9)
Rabbits Francisella tularensis
Farm animals or
parturient cats
Coxiella burnetti (Q fever)

Take Home Points
Ask patients about co-morbidities and travel/other potential exposures when they present with a respiratory illness
Evaluate patients for MDR risk factors when managing patients in the community with respiratory illness

Related Documents











