Common Neonatal Presentations Handbook Neonatal guidelines and protocols http://www.dvh.nhs.uk/adagio/directorates-and-departments/women- children/neonatal/ Compiled by Dr Abdul Hasib. Consultant Paediatrician Dr Shahinul Khan. Consultant Paediatrician Date: November 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Common Neonatal Presentations Handbook
Neonatal guidelines and protocols http://www.dvh.nhs.uk/adagio/directorates-and-departments/women-
children/neonatal/
Compiled by Dr Abdul Hasib. Consultant Paediatrician Dr Shahinul Khan. Consultant Paediatrician Date: November 2013
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 2 of 60
Contents Page
1. Neonatal resuscitation 4 2. Management of extremely premature babies 10 3. Neonatal hypoglycaemia 11 4. Management of IUGR 16 5. Neonatal hypernatraemic dehydration 17 6. Jaundice 18 7. Sepsis/ Antibiotics guidelines 24 8. Respiratory distress 30 9. Infants born to HIV +ve mothers 31 10. Infants born to HBsAg +ve mothers 33 11. Infants born to HCV +ve mothers 34 12. Neonatal blood transfusion 35 13. Polycythaemia 37 14. Maternal thyroid disease 38 15. Care of the baby whose mother is drug dependant 40 16. Feeding guideline 42
17. Baby checks 46 17.1 Skin 46 17.2 Appearance 46 17.3 Eyes 48 17.4 Ears 48 17.5 Scalp 48 17.6 Face 48 17.7 Heart 48 17.8 Fingers 49 17.9 Genitalia 49 17.10 Hips 49 17.11 Feet 49 17.12 Sacral dimple 49 17.13 Renal pelvic dilatation 50 17.14 Delayed passage of meconium 50 18. Brachial plexus injuries 52 19. Cleft palate 54
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 3 of 60
20. Cord gas 56 21. Hypoxic ischaemic encephalopathy 57 22. Bilious vomiting 60
Please note this handbook is only a guide, it does not replace standard textbooks or Consultant decisions made on the ward rounds. If unsure discuss with the Consultant and please refer to the full guideline or policy wherever relevant. The aim is to guide you to deal with common problems efficiently and effectively. Acknowledgements Adapted from Medway NCIU Guidelines; Evelina Neonatal Guidelines; St George’s Guidelines; Dr Diana Iskander, Paediatric ST trainee. Agreed by Paediatric Consultants: Dr. Selwyn D’Costa, Clinical Lead for Paediatrics Dr. Alok Gupta Dr. Abdul Hasib Dr. Ali Bokhari Dr. Gautam Kulkarni Dr. Suresh Kumar Dr. Shahinul Khan Dr. Sanjay Wazir Pandita Dr. Lazarus Anguvaa
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 4 of 60
1.0 RESUSCITATION (see also guideline WAC 065 Neonatal Resuscitation on Adagio) 1.1 Initial Attendance at delivery – SHO but escalate to Registrar if any concerns
• Forceps and ventouse deliveries for fetal distress, • Delivery is instrumental and is not low instrumental delivery (i.e. not a “lift-out”). • Trial of instrumental delivery in obstetric theatre • Breech deliveries • Delivery is by caesarean section under general anaesthesia. • Premature deliveries ( < 36 weeks) and severe IUGR • Thin Meconium stained liquor • Severe APH and cord prolapse • Shoulder dystocia • Obstetric /midwifery concerns • Rhesus positive antibodies with rising titre present. • There is any concern about the baby, e.g. suspected abnormality.
1.2 Attendance at delivery – Registrar • Deliveries of babies <34 weeks gestation and severe IUGR • Deliveries where problems with resuscitation are anticipated (Please think if Consultant presence
is required) • Thick Meconium stained liquor • Severe APH • Cord prolapse • Shoulder dystocia • Fetal Bradycardia • Multiple births • SHO’s who have not had experience in neonatal resuscitation will be accompanied by the
Registrar initially until confidence and competence is achieved. • All babies <31 weeks or any delivery with anticipated problems – discuss with Consultant. 1.3 Attendance at delivery – full team Where admission to the unit is anticipated (e.g. very premature babies) the registrar, SHO, Designated Nurse, equipment box and transport incubator should be present prior to delivery. 1.4 On arrival On arrival the paediatrician must check equipment and take a brief history, where time permits, noting: Gestation, pregnancy problems e.g. PET, APH, fetal distress, PROM, maternal pyrexia, meconium. a) Resuscitaire
• Oxygen/air flow – set to 4-6 l/min if T piece, 8-10 l/min if self inflation bag (450-500 ml) • Blow off pressure 30 cm in > 34 wks, 25 cm in <33+6 wks, 20 cm in <27+6 wks • Bag and mask • Suction and catheters -‐ for meconium deliveries, check suction tubing fits ET tube adapter or that
attached suction catheter fits down ETT
b) Intubation equipment Laryngoscope - 3 blades sizes (0, 1, 00) spare handle
ET tubes - size 2.5, 3.0 and 3.5 Introducers for Vygon ETTs Stethoscope

Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 5 of 60
c) Suction adapter for ETT d) Drugs (on unit resus trolley)
Adrenaline – 1:10 000 solution only Sodium bicarbonate 4.2% solution 10% glucose; 0.9%NaCl
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 6 of 60
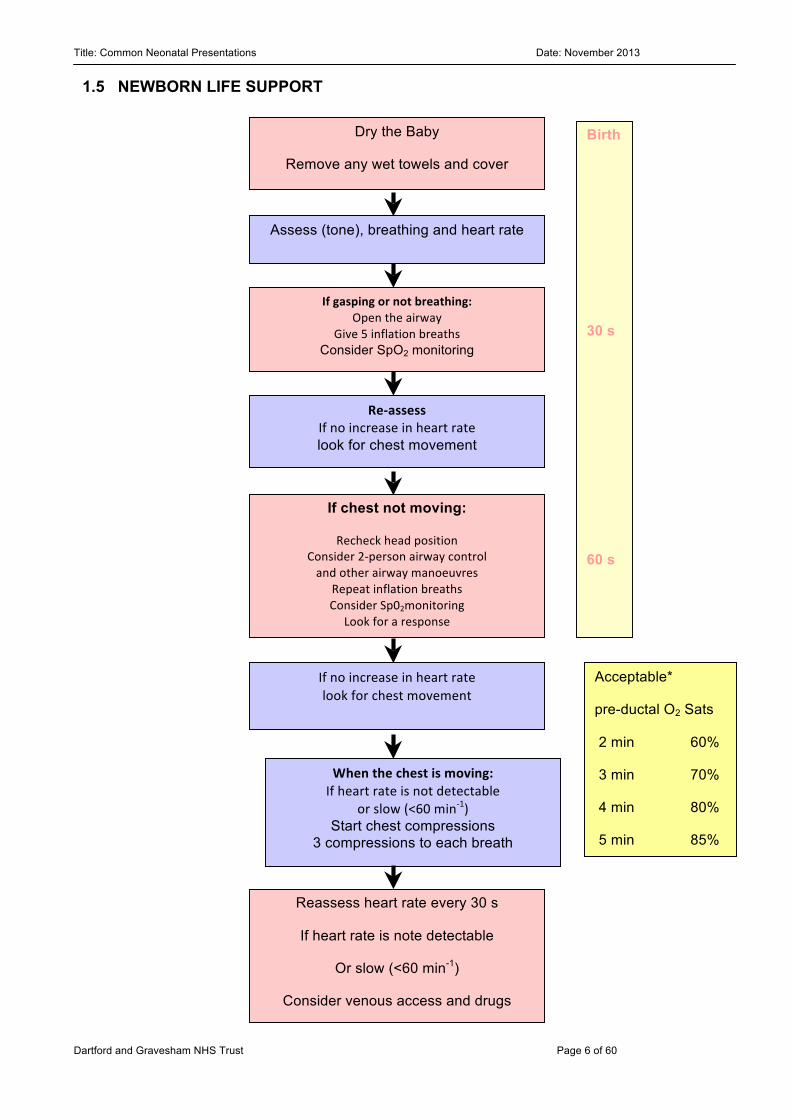
Assess (tone), breathing and heart rate
If gasping or not breathing: Open the airway
Give 5 inflation breaths Consider SpO2 monitoring
Re-‐assess If no increase in heart rate look for chest movement
Acceptable*
pre-ductal O2 Sats
2 min 60%
3 min 70%
4 min 80%
5 min 85%
10 min 90%
If no increase in heart rate look for chest movement
When the chest is moving: If heart rate is not detectable
or slow (<60 min-‐1) Start chest compressions
3 compressions to each breath
Dry the Baby
Remove any wet towels and cover
Start the clock or note the time
If chest not moving:
Recheck head position Consider 2-‐person airway control and other airway manoeuvres
Repeat inflation breaths Consider Sp02monitoring
Look for a response
Reassess heart rate every 30 s
If heart rate is note detectable
Or slow (<60 min-1)
Consider venous access and drugs
Birth
30 s
60 s
1.5 NEWBORN LIFE SUPPORT
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 7 of 60
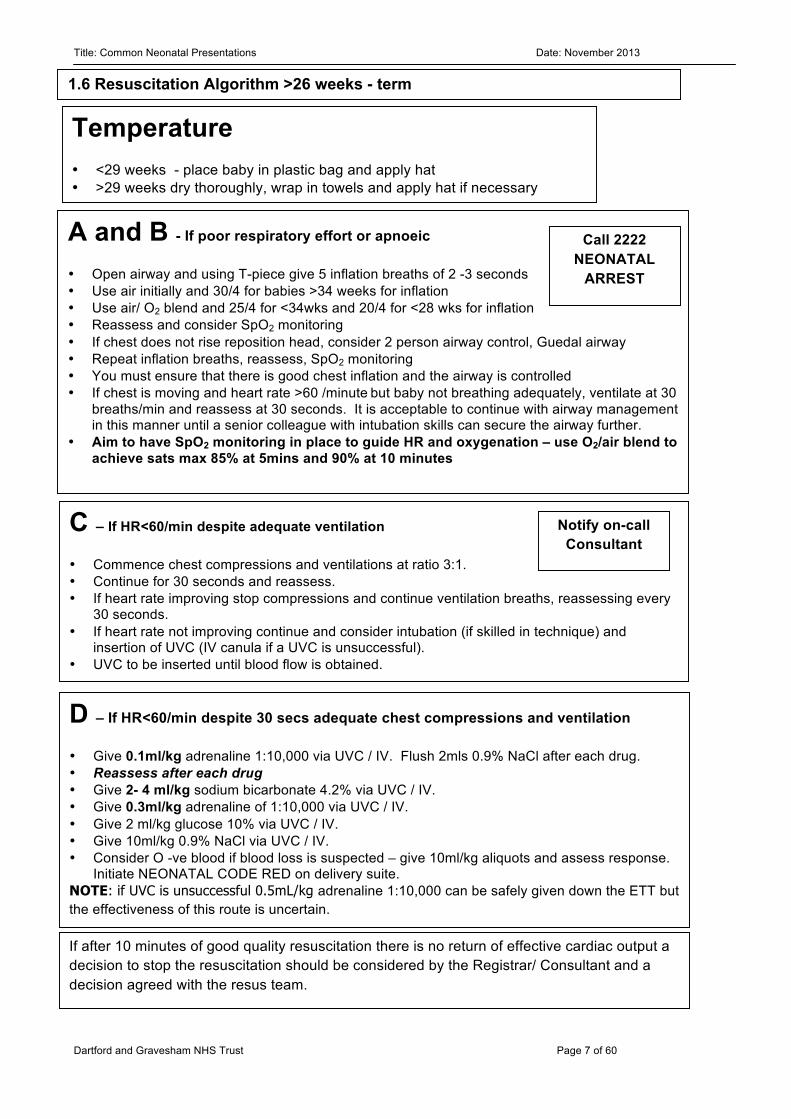
C – If HR<60/min despite adequate ventilation
• Commence chest compressions and ventilations at ratio 3:1. • Continue for 30 seconds and reassess. • If heart rate improving stop compressions and continue ventilation breaths, reassessing every
30 seconds. • If heart rate not improving continue and consider intubation (if skilled in technique) and
insertion of UVC (IV canula if a UVC is unsuccessful). • UVC to be inserted until blood flow is obtained. •
A and B - If poor respiratory effort or apnoeic
• Open airway and using T-piece give 5 inflation breaths of 2 -3 seconds • Use air initially and 30/4 for babies >34 weeks for inflation • Use air/ O2 blend and 25/4 for <34wks and 20/4 for <28 wks for inflation • Reassess and consider SpO2 monitoring • If chest does not rise reposition head, consider 2 person airway control, Guedal airway • Repeat inflation breaths, reassess, SpO2 monitoring • You must ensure that there is good chest inflation and the airway is controlled • If chest is moving and heart rate >60 /minute but baby not breathing adequately, ventilate at 30
breaths/min and reassess at 30 seconds. It is acceptable to continue with airway management in this manner until a senior colleague with intubation skills can secure the airway further.
• Aim to have SpO2 monitoring in place to guide HR and oxygenation – use O2/air blend to achieve sats max 85% at 5mins and 90% at 10 minutes
D – If HR<60/min despite 30 secs adequate chest compressions and ventilation
• Give 0.1ml/kg adrenaline 1:10,000 via UVC / IV. Flush 2mls 0.9% NaCl after each drug. • Reassess after each drug • Give 2- 4 ml/kg sodium bicarbonate 4.2% via UVC / IV. • Give 0.3ml/kg adrenaline of 1:10,000 via UVC / IV. • Give 2 ml/kg glucose 10% via UVC / IV. • Give 10ml/kg 0.9% NaCl via UVC / IV. • Consider O -ve blood if blood loss is suspected – give 10ml/kg aliquots and assess response.
Initiate NEONATAL CODE RED on delivery suite. NOTE: if UVC is unsuccessful 0.5mL/kg adrenaline 1:10,000 can be safely given down the ETT but the effectiveness of this route is uncertain.
Temperature
• <29 weeks - place baby in plastic bag and apply hat • >29 weeks dry thoroughly, wrap in towels and apply hat if necessary
1.6 Resuscitation Algorithm >26 weeks - term
Call 2222 NEONATAL
ARREST
If after 10 minutes of good quality resuscitation there is no return of effective cardiac output a decision to stop the resuscitation should be considered by the Registrar/ Consultant and a decision agreed with the resus team.
Notify on-call Consultant
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 8 of 60
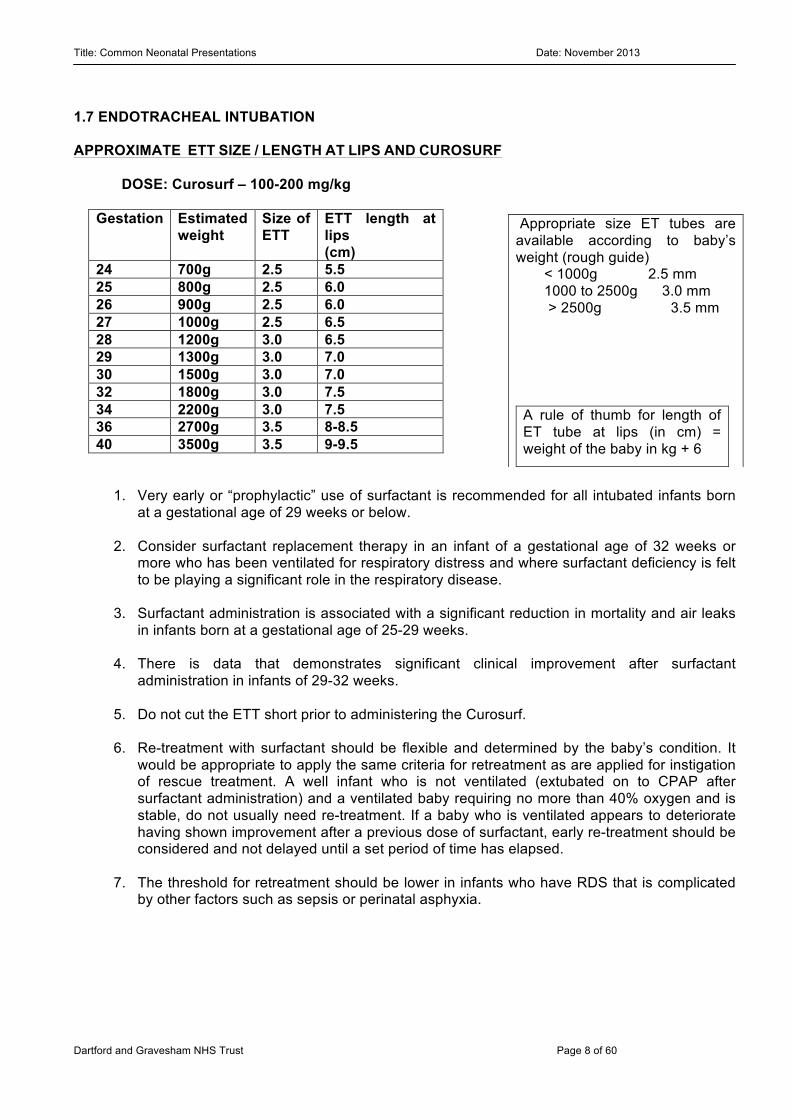
1.7 ENDOTRACHEAL INTUBATION APPROXIMATE ETT SIZE / LENGTH AT LIPS AND CUROSURF
DOSE: Curosurf – 100-200 mg/kg
Gestation Estimated weight
Size of ETT
ETT length at lips (cm)
24 700g 2.5 5.5 25 800g 2.5 6.0 26 900g 2.5 6.0 27 1000g 2.5 6.5 28 1200g 3.0 6.5 29 1300g 3.0 7.0 30 1500g 3.0 7.0 32 1800g 3.0 7.5 34 2200g 3.0 7.5 36 2700g 3.5 8-8.5 40 3500g 3.5 9-9.5
1. Very early or “prophylactic” use of surfactant is recommended for all intubated infants born at a gestational age of 29 weeks or below.
2. Consider surfactant replacement therapy in an infant of a gestational age of 32 weeks or
more who has been ventilated for respiratory distress and where surfactant deficiency is felt to be playing a significant role in the respiratory disease.
3. Surfactant administration is associated with a significant reduction in mortality and air leaks
in infants born at a gestational age of 25-29 weeks. 4. There is data that demonstrates significant clinical improvement after surfactant
administration in infants of 29-32 weeks. 5. Do not cut the ETT short prior to administering the Curosurf. 6. Re-treatment with surfactant should be flexible and determined by the baby’s condition. It
would be appropriate to apply the same criteria for retreatment as are applied for instigation of rescue treatment. A well infant who is not ventilated (extubated on to CPAP after surfactant administration) and a ventilated baby requiring no more than 40% oxygen and is stable, do not usually need re-treatment. If a baby who is ventilated appears to deteriorate having shown improvement after a previous dose of surfactant, early re-treatment should be considered and not delayed until a set period of time has elapsed.
7. The threshold for retreatment should be lower in infants who have RDS that is complicated
by other factors such as sepsis or perinatal asphyxia.
A rule of thumb for length of ET tube at lips (in cm) = weight of the baby in kg + 6
Appropriate size ET tubes are available according to baby’s weight (rough guide)
< 1000g 2.5 mm 1000 to 2500g 3.0 mm
> 2500g 3.5 mm
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 9 of 60
1.8 Suggested drugs and doses for intubation premedication • 1ST MORPHINE 50 -100 micrograms/ kg slow i.v. injection
• 2ND SUXAMETHONIUM 2 mg/kg slow i.v. injection (paralysis lasts 5-10 min) after discussion
with Consultant
• 3RD ATROPINE 20 microgram/kg (+/ - with 2nd dose of suxamethonium or bradycardia)
1.9 Umbilical Lines
UAC cm : (wt in kg x 3) + 9+ stump – T6-9 UVC cm : ½ UAC +1 At the level of diaphragm Check X ray for position before use.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 10 of 60
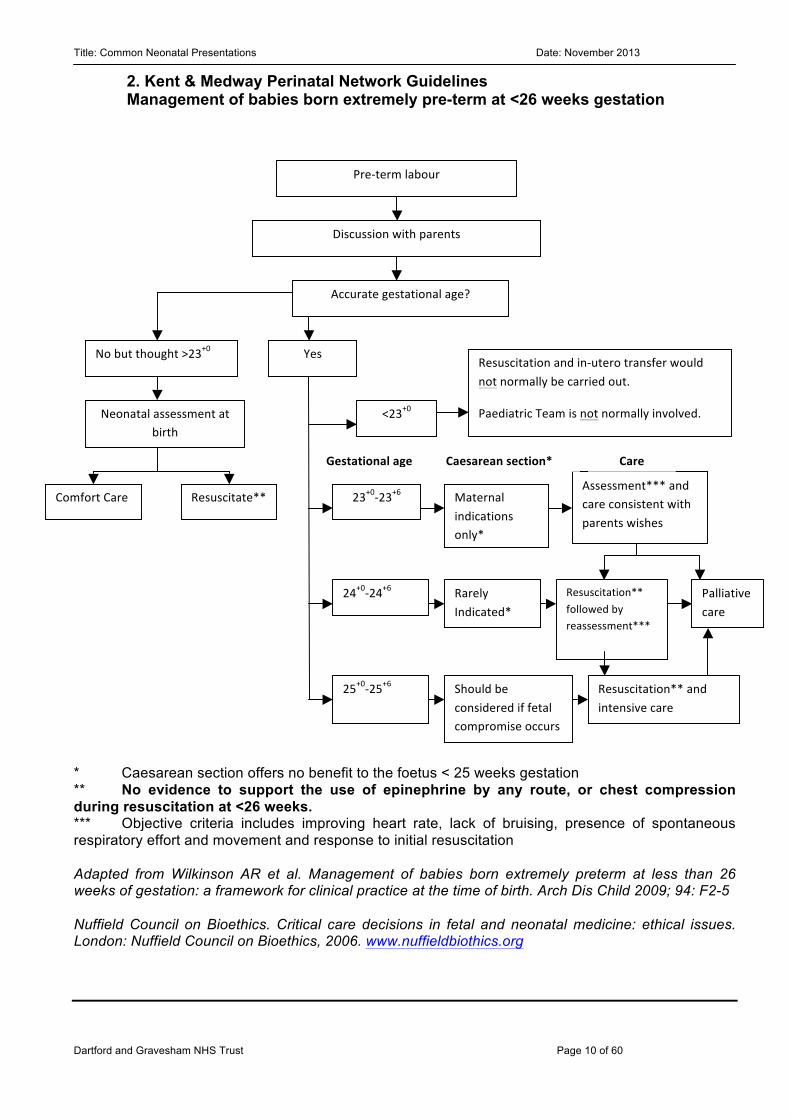
* Caesarean section offers no benefit to the foetus < 25 weeks gestation ** No evidence to support the use of epinephrine by any route, or chest compression during resuscitation at <26 weeks. *** Objective criteria includes improving heart rate, lack of bruising, presence of spontaneous respiratory effort and movement and response to initial resuscitation Adapted from Wilkinson AR et al. Management of babies born extremely preterm at less than 26 weeks of gestation: a framework for clinical practice at the time of birth. Arch Dis Child 2009; 94: F2-5 Nuffield Council on Bioethics. Critical care decisions in fetal and neonatal medicine: ethical issues. London: Nuffield Council on Bioethics, 2006. www.nuffieldbiothics.org
Pre-‐term labour
Discussion with parents
Accurate gestational age?
No but thought >23+0
Neonatal assessment at birth
Comfort Care Resuscitate**
Yes
<23+0
Resuscitation and in-‐utero transfer would not normally be carried out.
Paediatric Team is not normally involved.
23+0-‐23+6
24+0-‐24+6
25+0-‐25+6
Maternal indications only*
Rarely Indicated*
Should be considered if fetal compromise occurs
Assessment*** and care consistent with parents wishes
Resuscitation** followed by reassessment***
Palliative care
Resuscitation** and intensive care
Gestational age Caesarean section* section
Care
2. Kent & Medway Perinatal Network Guidelines Management of babies born extremely pre-term at <26 weeks gestation
Management of babies born extremely pre-‐term at <26 weeks gestation
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 11 of 60
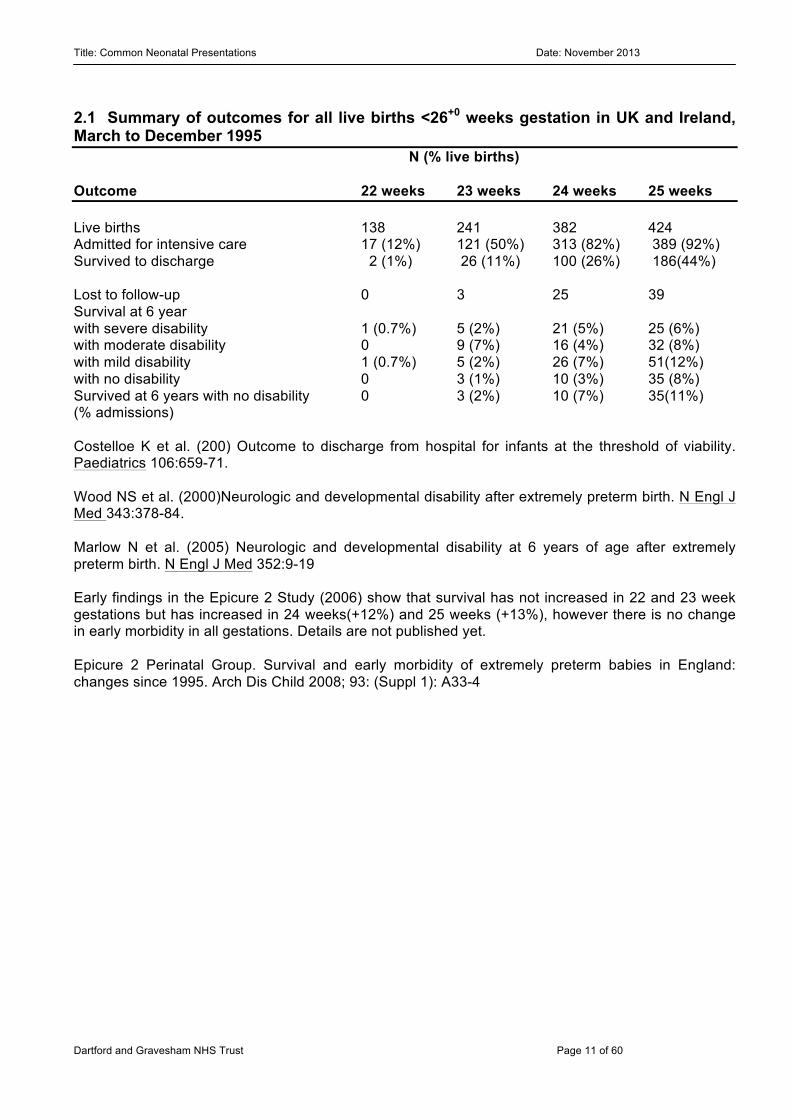
2.1 Summary of outcomes for all live births <26+0 weeks gestation in UK and Ireland, March to December 1995 N (% live births) Outcome 22 weeks 23 weeks 24 weeks 25 weeks Live births 138 241 382 424 Admitted for intensive care 17 (12%) 121 (50%) 313 (82%) 389 (92%) Survived to discharge 2 (1%) 26 (11%) 100 (26%) 186(44%) Lost to follow-up 0 3 25 39 Survival at 6 year with severe disability 1 (0.7%) 5 (2%) 21 (5%) 25 (6%) with moderate disability 0 9 (7%) 16 (4%) 32 (8%) with mild disability 1 (0.7%) 5 (2%) 26 (7%) 51(12%) with no disability 0 3 (1%) 10 (3%) 35 (8%) Survived at 6 years with no disability 0 3 (2%) 10 (7%) 35(11%) (% admissions) Costelloe K et al. (200) Outcome to discharge from hospital for infants at the threshold of viability. Paediatrics 106:659-71. Wood NS et al. (2000)Neurologic and developmental disability after extremely preterm birth. N Engl J Med 343:378-84. Marlow N et al. (2005) Neurologic and developmental disability at 6 years of age after extremely preterm birth. N Engl J Med 352:9-19 Early findings in the Epicure 2 Study (2006) show that survival has not increased in 22 and 23 week gestations but has increased in 24 weeks(+12%) and 25 weeks (+13%), however there is no change in early morbidity in all gestations. Details are not published yet. Epicure 2 Perinatal Group. Survival and early morbidity of extremely preterm babies in England: changes since 1995. Arch Dis Child 2008; 93: (Suppl 1): A33-4
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 12 of 60
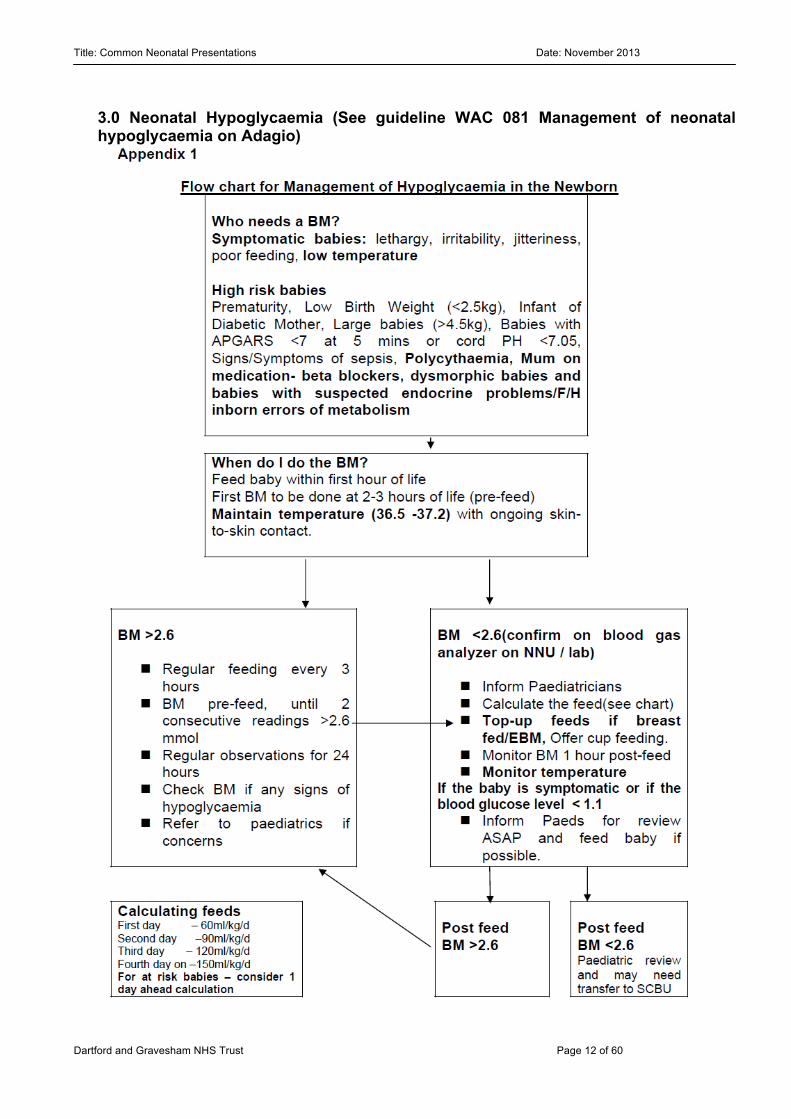
3.0 Neonatal Hypoglycaemia (See guideline WAC 081 Management of neonatal hypoglycaemia on Adagio)
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 13 of 60
3.1 Progress in SCBU
• If the blood glucose is > 2.6mmols
Interval between feeds can be increased gradually until baby is on demand feeds. If bottle fed the volume of milk can also be increased by 20 – 30 ml/kg/day.
• If the blood glucose is 2.0 - 2.6mmols No clinical signs, increase the milk volume to 90ml/kg/day, two hourly feeds. Breast feeds must be topped up with the full amount of milk by bottle or NG tube. The blood glucose should be measured prior to feeds 2.6mmols or above. Gradually discontinue supplemental feeds when the blood glucose is consistently 3mmols or above. Nutriprem is not appropriate for the treatment of hypoglycaemia unless indicated by prematurity/ weight.
• If the glucose is < 2.0mmols The baby is otherwise well, give an hourly amount of 90 ml/kg/day on D1 by NG or start on IV 10% dextrose
• If the baby is symptomatic or if the blood glucose level remains < 1.1mmols The paediatrician must review immediately. Consider blood tests / sepsis Bolus 10% dextrose 2mls/kg and consider increasing IV Dextrose concentrations – 12.5 -15%. Concentrations >12.5% must be given via central access.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 14 of 60
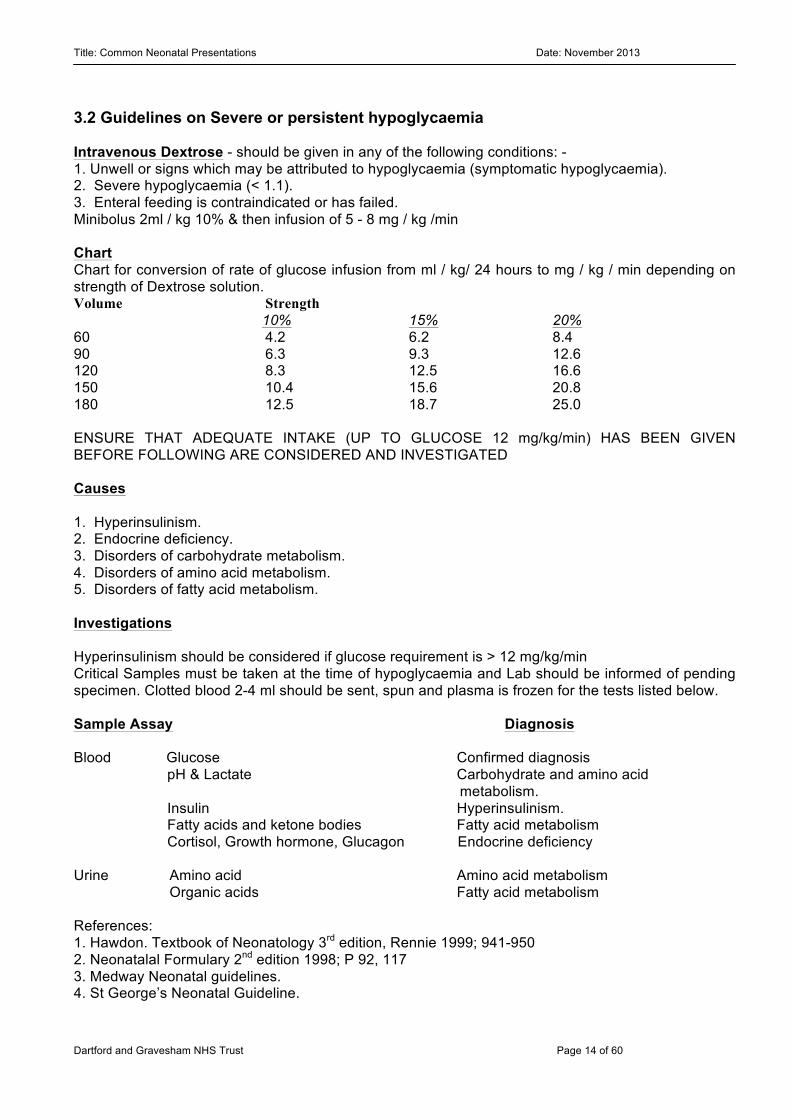
3.2 Guidelines on Severe or persistent hypoglycaemia Intravenous Dextrose - should be given in any of the following conditions: - 1. Unwell or signs which may be attributed to hypoglycaemia (symptomatic hypoglycaemia). 2. Severe hypoglycaemia (< 1.1). 3. Enteral feeding is contraindicated or has failed. Minibolus 2ml / kg 10% & then infusion of 5 - 8 mg / kg /min Chart Chart for conversion of rate of glucose infusion from ml / kg/ 24 hours to mg / kg / min depending on strength of Dextrose solution. Volume Strength 10% 15% 20% 60 4.2 6.2 8.4 90 6.3 9.3 12.6 120 8.3 12.5 16.6 150 10.4 15.6 20.8 180 12.5 18.7 25.0 ENSURE THAT ADEQUATE INTAKE (UP TO GLUCOSE 12 mg/kg/min) HAS BEEN GIVEN BEFORE FOLLOWING ARE CONSIDERED AND INVESTIGATED Causes 1. Hyperinsulinism. 2. Endocrine deficiency. 3. Disorders of carbohydrate metabolism. 4. Disorders of amino acid metabolism. 5. Disorders of fatty acid metabolism. Investigations Hyperinsulinism should be considered if glucose requirement is > 12 mg/kg/min Critical Samples must be taken at the time of hypoglycaemia and Lab should be informed of pending specimen. Clotted blood 2-4 ml should be sent, spun and plasma is frozen for the tests listed below. Sample Assay Diagnosis Blood Glucose Confirmed diagnosis pH & Lactate Carbohydrate and amino acid metabolism. Insulin Hyperinsulinism. Fatty acids and ketone bodies Fatty acid metabolism Cortisol, Growth hormone, Glucagon Endocrine deficiency Urine Amino acid Amino acid metabolism Organic acids Fatty acid metabolism References: 1. Hawdon. Textbook of Neonatology 3rd edition, Rennie 1999; 941-950 2. Neonatalal Formulary 2nd edition 1998; P 92, 117 3. Medway Neonatal guidelines. 4. St George’s Neonatal Guideline.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 15 of 60
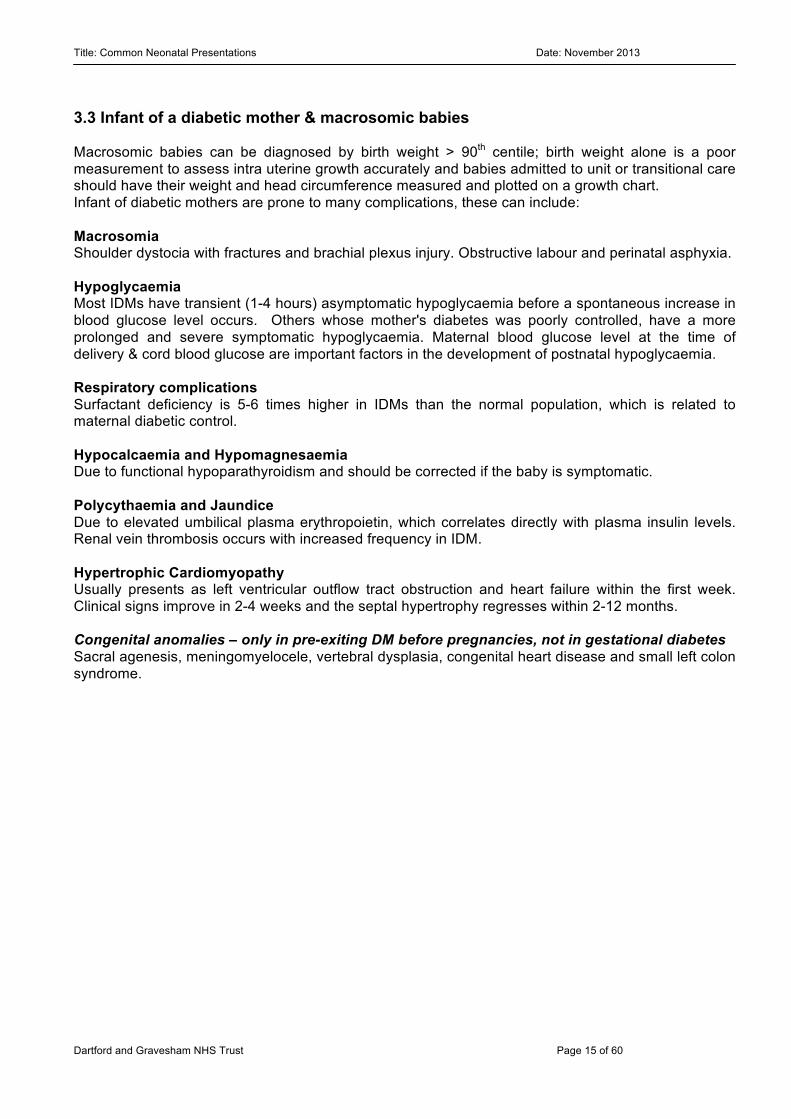
3.3 Infant of a diabetic mother & macrosomic babies Macrosomic babies can be diagnosed by birth weight > 90th centile; birth weight alone is a poor measurement to assess intra uterine growth accurately and babies admitted to unit or transitional care should have their weight and head circumference measured and plotted on a growth chart. Infant of diabetic mothers are prone to many complications, these can include:
Macrosomia Shoulder dystocia with fractures and brachial plexus injury. Obstructive labour and perinatal asphyxia. Hypoglycaemia Most IDMs have transient (1-4 hours) asymptomatic hypoglycaemia before a spontaneous increase in blood glucose level occurs. Others whose mother's diabetes was poorly controlled, have a more prolonged and severe symptomatic hypoglycaemia. Maternal blood glucose level at the time of delivery & cord blood glucose are important factors in the development of postnatal hypoglycaemia. Respiratory complications Surfactant deficiency is 5-6 times higher in IDMs than the normal population, which is related to maternal diabetic control. Hypocalcaemia and Hypomagnesaemia Due to functional hypoparathyroidism and should be corrected if the baby is symptomatic. Polycythaemia and Jaundice Due to elevated umbilical plasma erythropoietin, which correlates directly with plasma insulin levels. Renal vein thrombosis occurs with increased frequency in IDM. Hypertrophic Cardiomyopathy Usually presents as left ventricular outflow tract obstruction and heart failure within the first week. Clinical signs improve in 2-4 weeks and the septal hypertrophy regresses within 2-12 months. Congenital anomalies – only in pre-exiting DM before pregnancies, not in gestational diabetes Sacral agenesis, meningomyelocele, vertebral dysplasia, congenital heart disease and small left colon syndrome.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 16 of 60
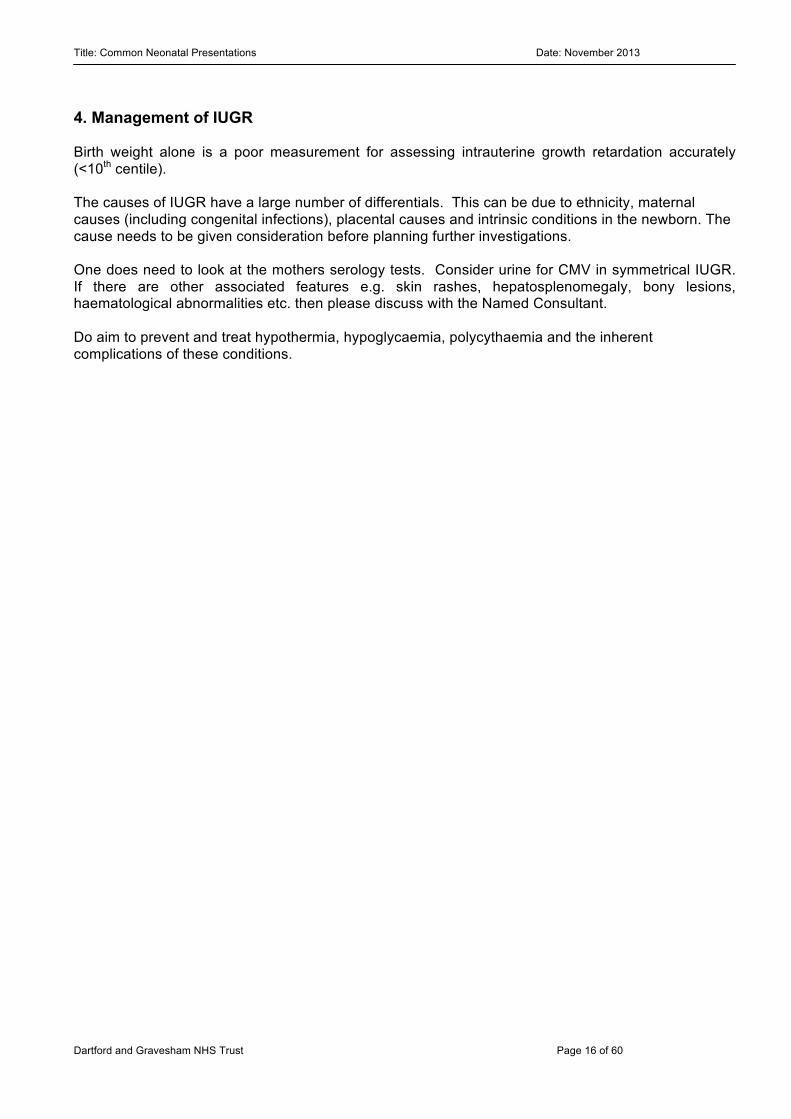
4. Management of IUGR Birth weight alone is a poor measurement for assessing intrauterine growth retardation accurately (<10th centile). The causes of IUGR have a large number of differentials. This can be due to ethnicity, maternal causes (including congenital infections), placental causes and intrinsic conditions in the newborn. The cause needs to be given consideration before planning further investigations. One does need to look at the mothers serology tests. Consider urine for CMV in symmetrical IUGR. If there are other associated features e.g. skin rashes, hepatosplenomegaly, bony lesions, haematological abnormalities etc. then please discuss with the Named Consultant. Do aim to prevent and treat hypothermia, hypoglycaemia, polycythaemia and the inherent complications of these conditions.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 17 of 60
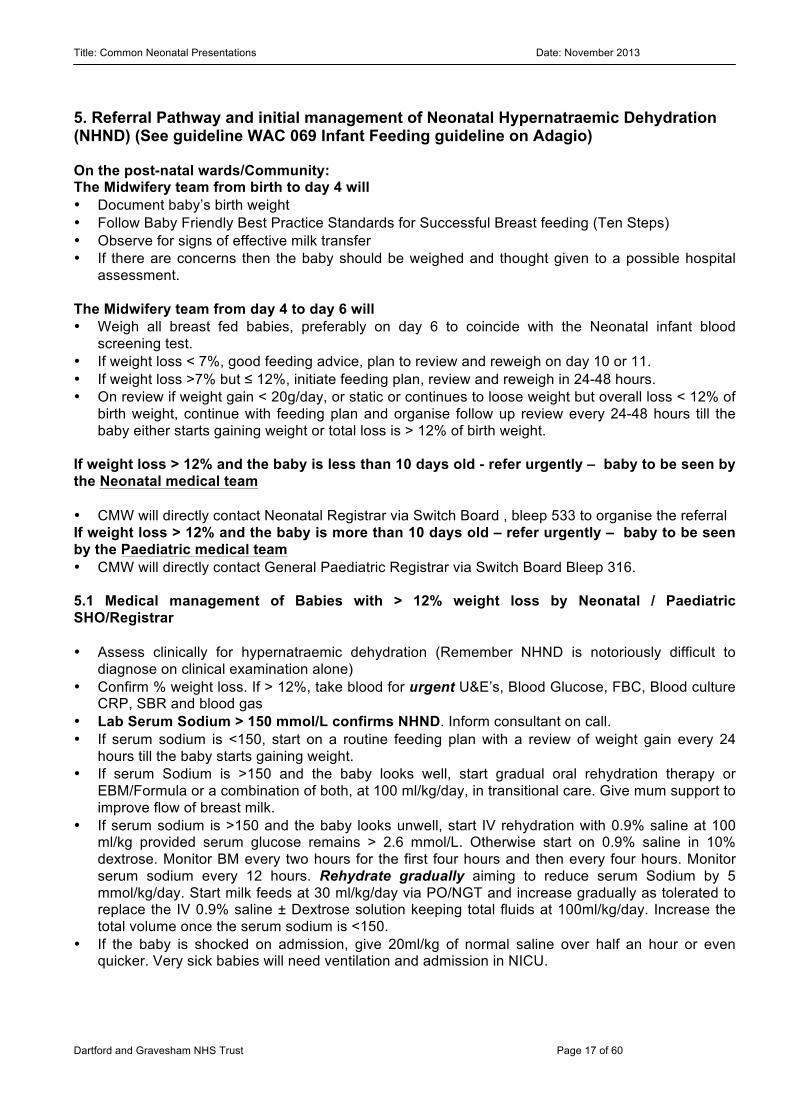
5. Referral Pathway and initial management of Neonatal Hypernatraemic Dehydration (NHND) (See guideline WAC 069 Infant Feeding guideline on Adagio) On the post-natal wards/Community: The Midwifery team from birth to day 4 will • Document baby’s birth weight • Follow Baby Friendly Best Practice Standards for Successful Breast feeding (Ten Steps) • Observe for signs of effective milk transfer • If there are concerns then the baby should be weighed and thought given to a possible hospital
assessment. The Midwifery team from day 4 to day 6 will • Weigh all breast fed babies, preferably on day 6 to coincide with the Neonatal infant blood
screening test. • If weight loss < 7%, good feeding advice, plan to review and reweigh on day 10 or 11. • If weight loss >7% but ≤ 12%, initiate feeding plan, review and reweigh in 24-48 hours. • On review if weight gain < 20g/day, or static or continues to loose weight but overall loss < 12% of
birth weight, continue with feeding plan and organise follow up review every 24-48 hours till the baby either starts gaining weight or total loss is > 12% of birth weight.
If weight loss > 12% and the baby is less than 10 days old - refer urgently – baby to be seen by the Neonatal medical team • CMW will directly contact Neonatal Registrar via Switch Board , bleep 533 to organise the referral If weight loss > 12% and the baby is more than 10 days old – refer urgently – baby to be seen by the Paediatric medical team • CMW will directly contact General Paediatric Registrar via Switch Board Bleep 316. 5.1 Medical management of Babies with > 12% weight loss by Neonatal / Paediatric SHO/Registrar • Assess clinically for hypernatraemic dehydration (Remember NHND is notoriously difficult to
diagnose on clinical examination alone) • Confirm % weight loss. If > 12%, take blood for urgent U&E’s, Blood Glucose, FBC, Blood culture
CRP, SBR and blood gas • Lab Serum Sodium > 150 mmol/L confirms NHND. Inform consultant on call. • If serum sodium is <150, start on a routine feeding plan with a review of weight gain every 24
hours till the baby starts gaining weight. • If serum Sodium is >150 and the baby looks well, start gradual oral rehydration therapy or
EBM/Formula or a combination of both, at 100 ml/kg/day, in transitional care. Give mum support to improve flow of breast milk.
• If serum sodium is >150 and the baby looks unwell, start IV rehydration with 0.9% saline at 100 ml/kg provided serum glucose remains > 2.6 mmol/L. Otherwise start on 0.9% saline in 10% dextrose. Monitor BM every two hours for the first four hours and then every four hours. Monitor serum sodium every 12 hours. Rehydrate gradually aiming to reduce serum Sodium by 5 mmol/kg/day. Start milk feeds at 30 ml/kg/day via PO/NGT and increase gradually as tolerated to replace the IV 0.9% saline ± Dextrose solution keeping total fluids at 100ml/kg/day. Increase the total volume once the serum sodium is <150.
• If the baby is shocked on admission, give 20ml/kg of normal saline over half an hour or even quicker. Very sick babies will need ventilation and admission in NICU.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 18 of 60
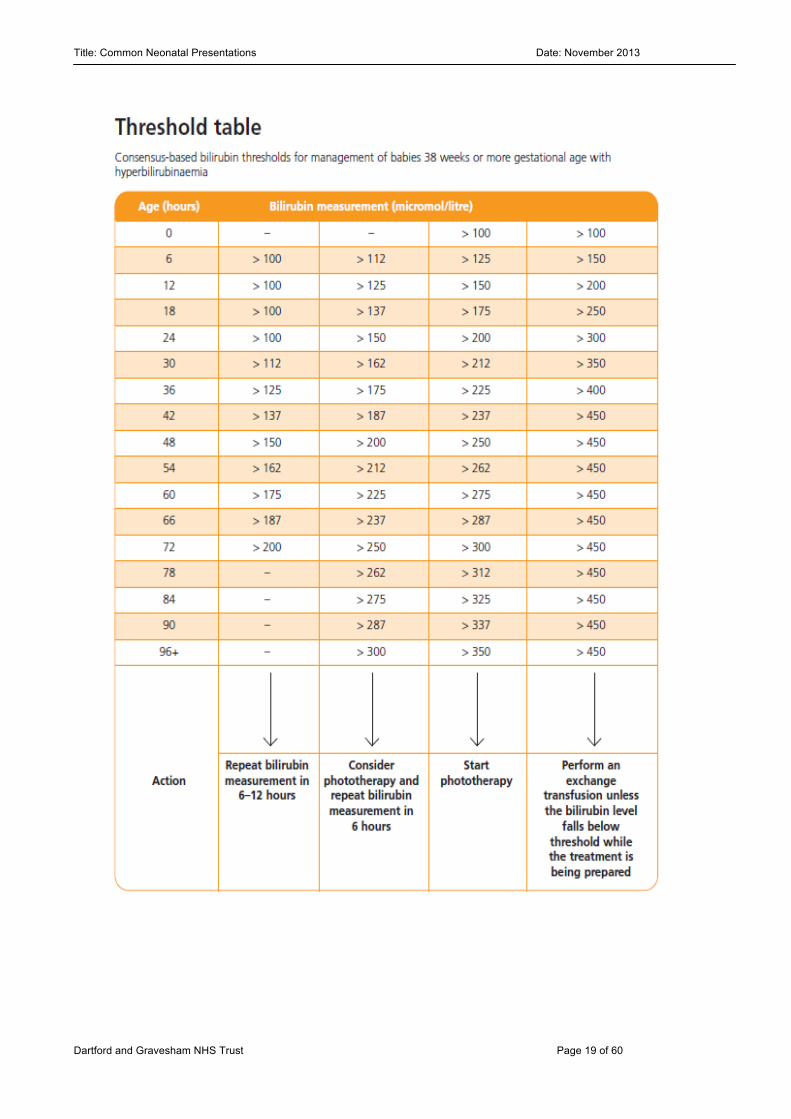
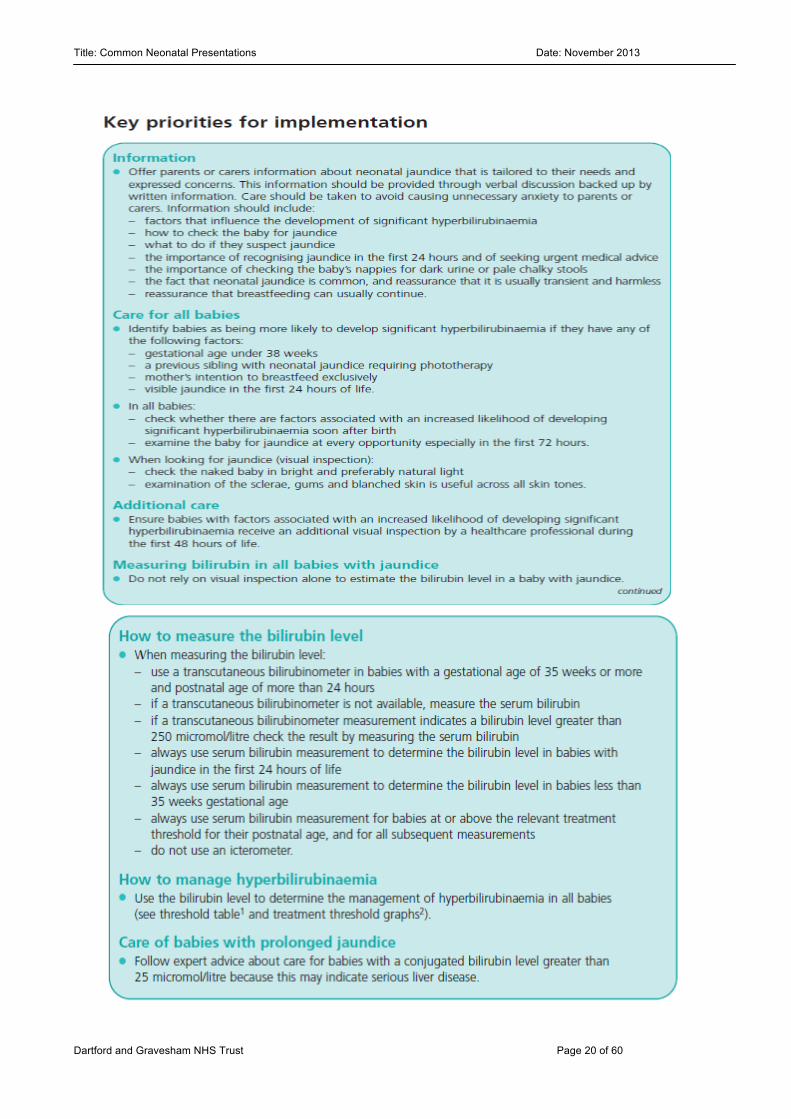
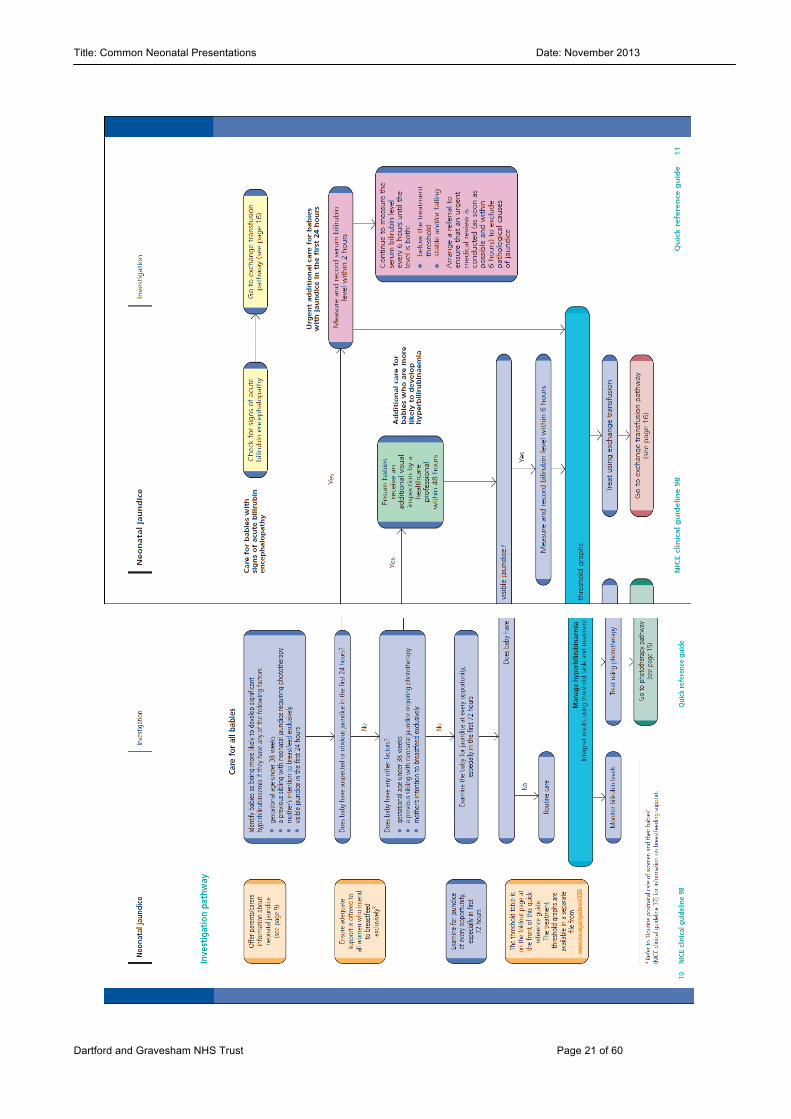
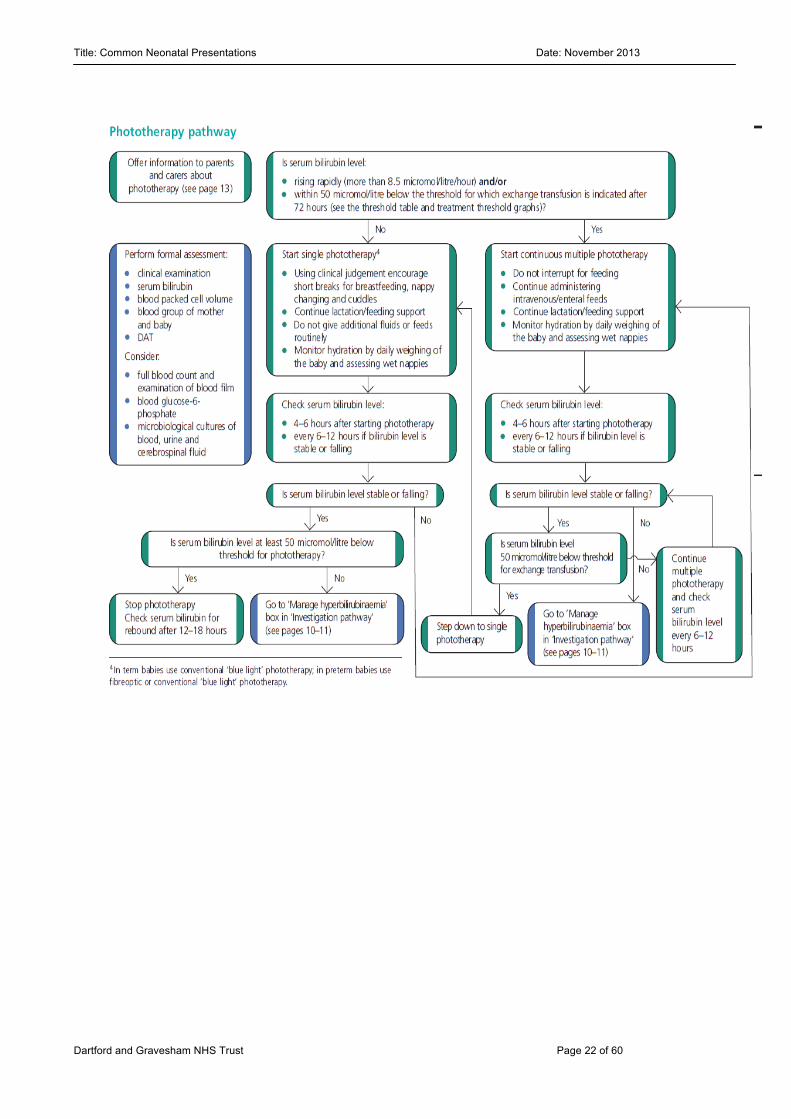
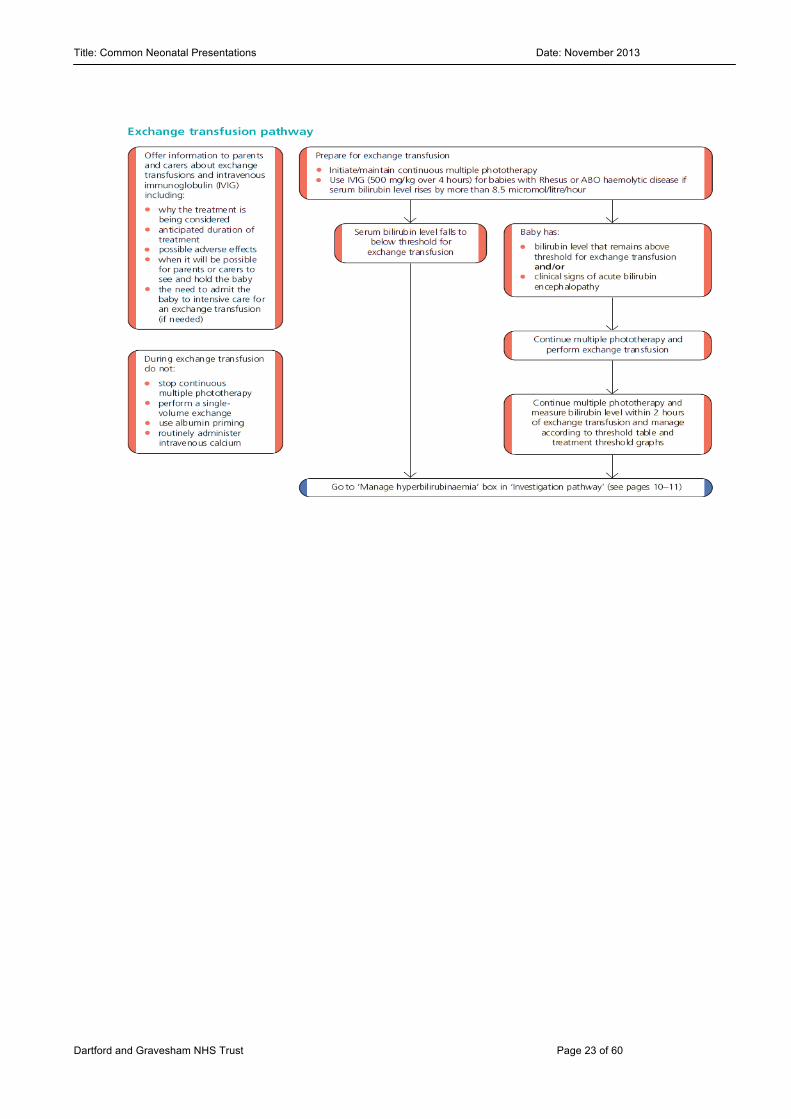
6. Neonatal Jaundice The majority of babies will become jaundiced. This occurs more commonly in preterm and unwell infants. The causes and clinical situation will need to be thought about on an individualised basis. It is no longer acceptable to visually estimate the level of jaundice, this must be quantified. NICE has set out the guidance below on how this should be done. We do not currently utilise transcutaneous bilirubinometers in our hospital and as a result a blood test is required. Please refer to the NICE guidelines on www.nice.org.uk
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 19 of 60
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 20 of 60
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 21 of 60
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 22 of 60
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 23 of 60
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 24 of 60
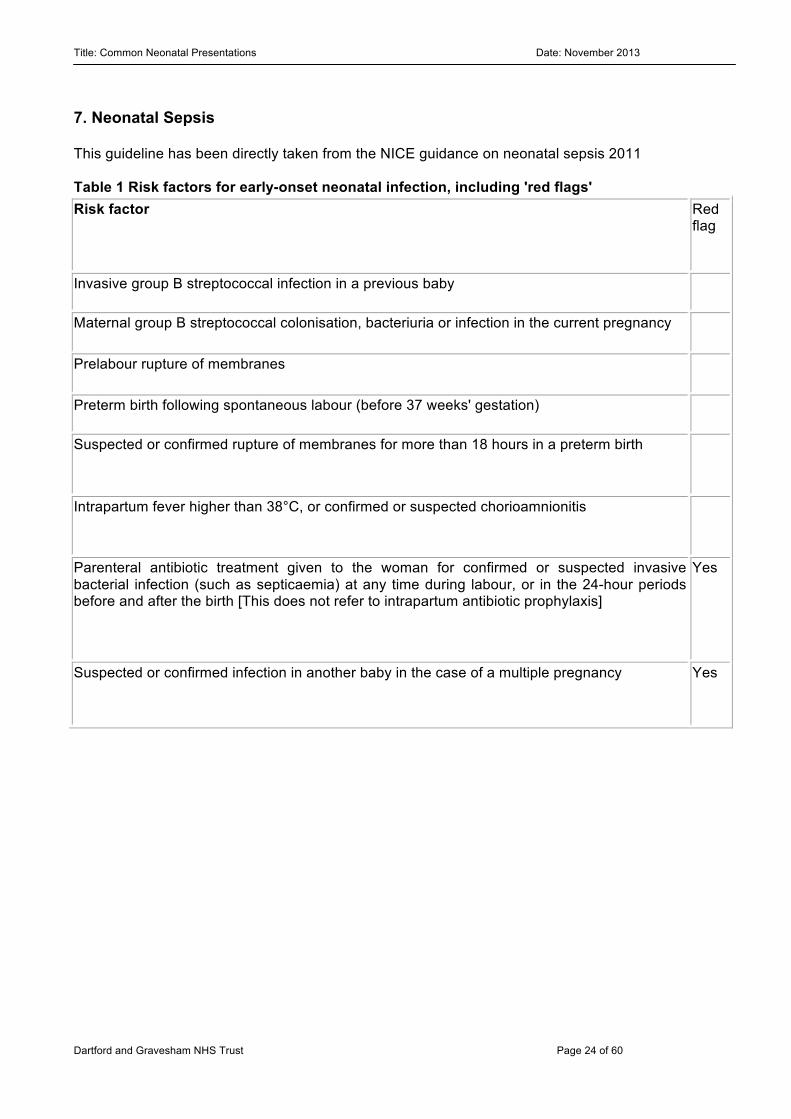
7. Neonatal Sepsis This guideline has been directly taken from the NICE guidance on neonatal sepsis 2011 Table 1 Risk factors for early-onset neonatal infection, including 'red flags' Risk factor Red
flag
Invasive group B streptococcal infection in a previous baby
Maternal group B streptococcal colonisation, bacteriuria or infection in the current pregnancy
Prelabour rupture of membranes
Preterm birth following spontaneous labour (before 37 weeks' gestation)
Suspected or confirmed rupture of membranes for more than 18 hours in a preterm birth
Intrapartum fever higher than 38°C, or confirmed or suspected chorioamnionitis
Parenteral antibiotic treatment given to the woman for confirmed or suspected invasive bacterial infection (such as septicaemia) at any time during labour, or in the 24-hour periods before and after the birth [This does not refer to intrapartum antibiotic prophylaxis]
Yes
Suspected or confirmed infection in another baby in the case of a multiple pregnancy Yes
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 25 of 60
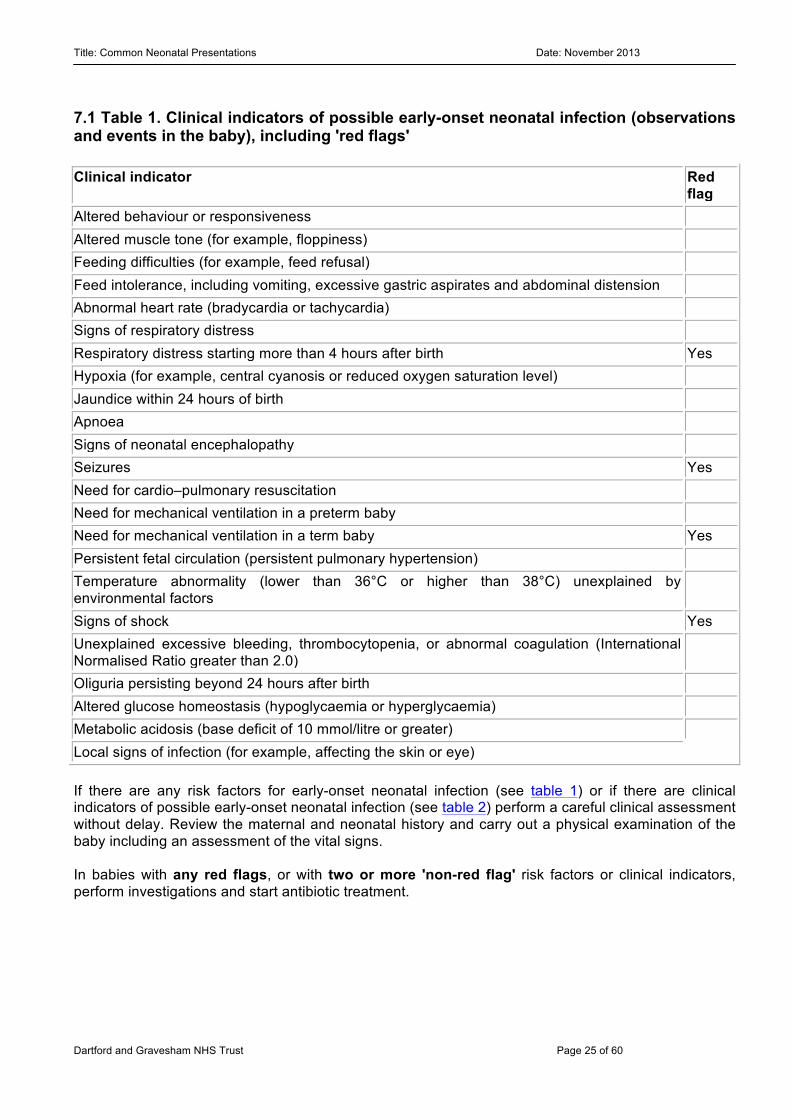
7.1 Table 1. Clinical indicators of possible early-onset neonatal infection (observations and events in the baby), including 'red flags' Clinical indicator Red
flag Altered behaviour or responsiveness Altered muscle tone (for example, floppiness) Feeding difficulties (for example, feed refusal) Feed intolerance, including vomiting, excessive gastric aspirates and abdominal distension Abnormal heart rate (bradycardia or tachycardia) Signs of respiratory distress Respiratory distress starting more than 4 hours after birth Yes Hypoxia (for example, central cyanosis or reduced oxygen saturation level) Jaundice within 24 hours of birth Apnoea Signs of neonatal encephalopathy Seizures Yes Need for cardio–pulmonary resuscitation Need for mechanical ventilation in a preterm baby Need for mechanical ventilation in a term baby Yes Persistent fetal circulation (persistent pulmonary hypertension) Temperature abnormality (lower than 36°C or higher than 38°C) unexplained by environmental factors
Signs of shock Yes Unexplained excessive bleeding, thrombocytopenia, or abnormal coagulation (International Normalised Ratio greater than 2.0)
Oliguria persisting beyond 24 hours after birth Altered glucose homeostasis (hypoglycaemia or hyperglycaemia) Metabolic acidosis (base deficit of 10 mmol/litre or greater) Local signs of infection (for example, affecting the skin or eye) If there are any risk factors for early-onset neonatal infection (see table 1) or if there are clinical indicators of possible early-onset neonatal infection (see table 2) perform a careful clinical assessment without delay. Review the maternal and neonatal history and carry out a physical examination of the baby including an assessment of the vital signs. In babies with any red flags, or with two or more 'non-red flag' risk factors or clinical indicators, perform investigations and start antibiotic treatment.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 26 of 60
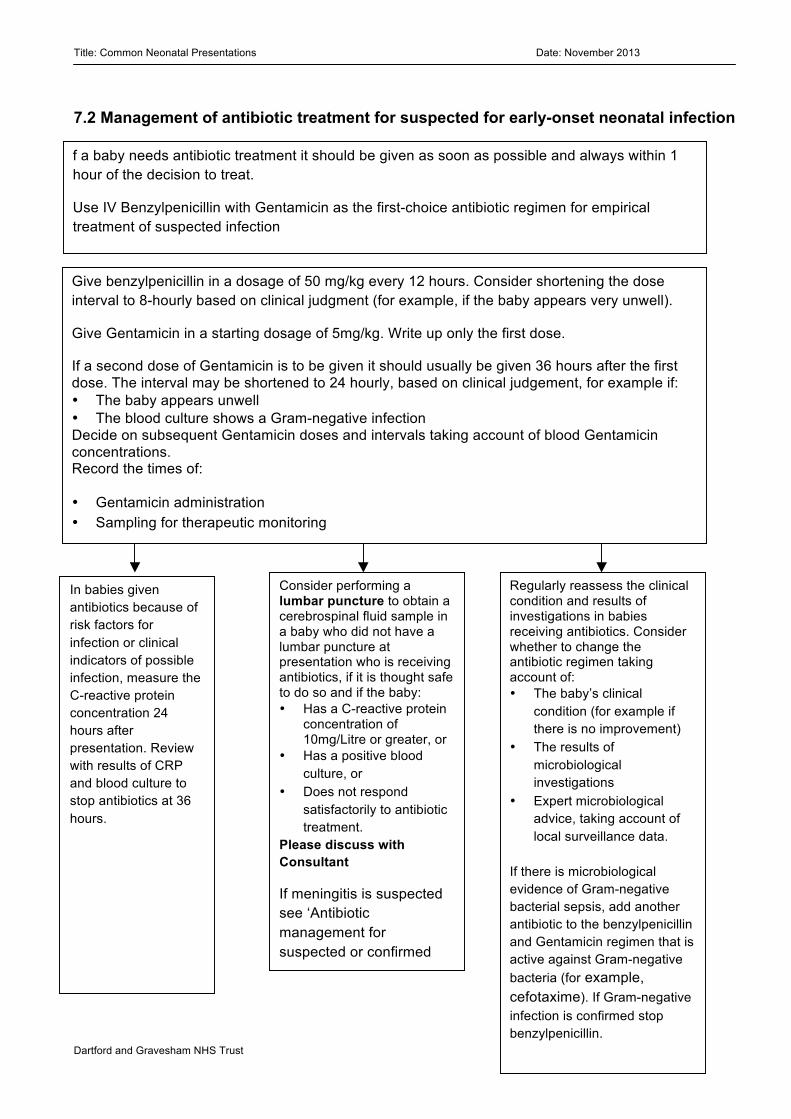
7.2 Management of antibiotic treatment for suspected for early-onset neonatal infection f a baby needs antibiotic treatment it should be given as soon as possible and always within 1 hour of the decision to treat.
Use IV Benzylpenicillin with Gentamicin as the first-choice antibiotic regimen for empirical treatment of suspected infection
Give benzylpenicillin in a dosage of 50 mg/kg every 12 hours. Consider shortening the dose interval to 8-hourly based on clinical judgment (for example, if the baby appears very unwell).
Give Gentamicin in a starting dosage of 5mg/kg. Write up only the first dose.
If a second dose of Gentamicin is to be given it should usually be given 36 hours after the first dose. The interval may be shortened to 24 hourly, based on clinical judgement, for example if: • The baby appears unwell • The blood culture shows a Gram-negative infection Decide on subsequent Gentamicin doses and intervals taking account of blood Gentamicin concentrations. Record the times of:
• Gentamicin administration • Sampling for therapeutic monitoring
In babies given antibiotics because of risk factors for infection or clinical indicators of possible infection, measure the C-reactive protein concentration 24 hours after presentation. Review with results of CRP and blood culture to stop antibiotics at 36 hours.
Consider performing a lumbar puncture to obtain a cerebrospinal fluid sample in a baby who did not have a lumbar puncture at presentation who is receiving antibiotics, if it is thought safe to do so and if the baby: • Has a C-reactive protein
concentration of 10mg/Litre or greater, or
• Has a positive blood culture, or
• Does not respond satisfactorily to antibiotic treatment.
Please discuss with Consultant
If meningitis is suspected see ‘Antibiotic management for suspected or confirmed meningitis’ pathway.
Regularly reassess the clinical condition and results of investigations in babies receiving antibiotics. Consider whether to change the antibiotic regimen taking account of: • The baby’s clinical
condition (for example if there is no improvement)
• The results of microbiological investigations
• Expert microbiological advice, taking account of local surveillance data.
If there is microbiological evidence of Gram-negative bacterial sepsis, add another antibiotic to the benzylpenicillin and Gentamicin regimen that is active against Gram-negative bacteria (for example, cefotaxime). If Gram-negative infection is confirmed stop benzylpenicillin.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 27 of 60
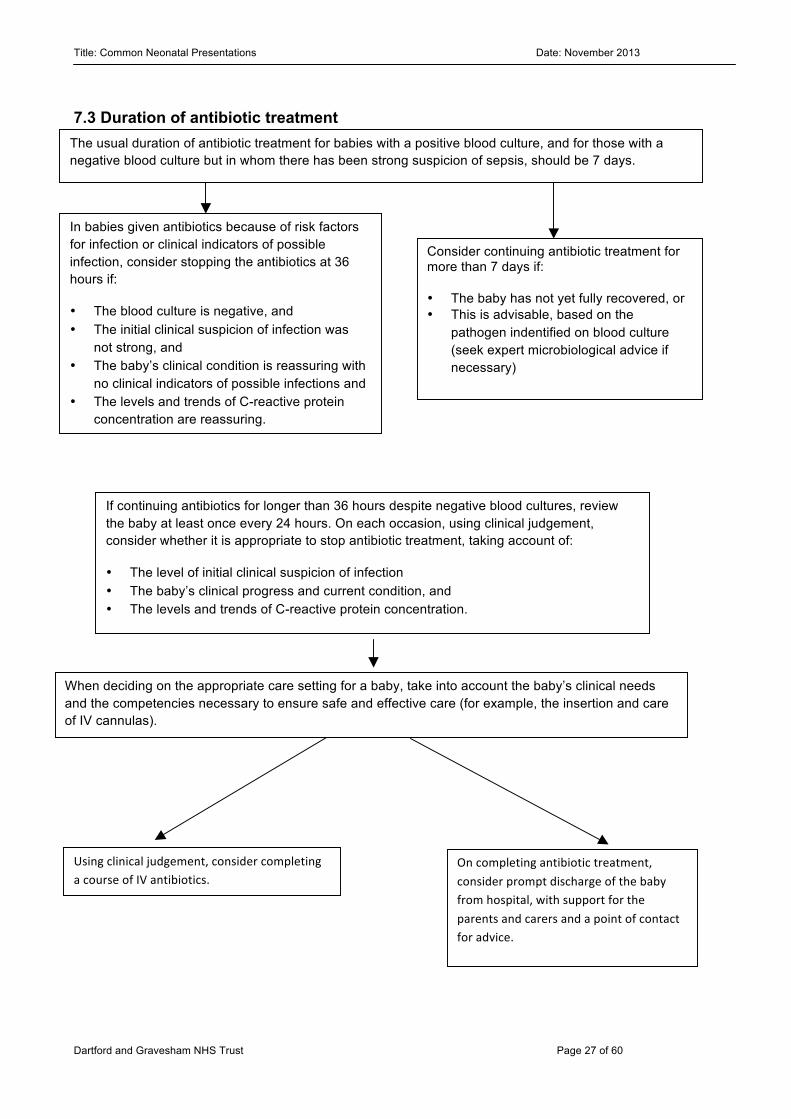
7.3 Duration of antibiotic treatment 6.4 Care setting for antibiotic treatment
The usual duration of antibiotic treatment for babies with a positive blood culture, and for those with a negative blood culture but in whom there has been strong suspicion of sepsis, should be 7 days.
In babies given antibiotics because of risk factors for infection or clinical indicators of possible infection, consider stopping the antibiotics at 36 hours if:
• The blood culture is negative, and • The initial clinical suspicion of infection was
not strong, and • The baby’s clinical condition is reassuring with
no clinical indicators of possible infections and • The levels and trends of C-reactive protein
concentration are reassuring.
Consider continuing antibiotic treatment for more than 7 days if: • The baby has not yet fully recovered, or • This is advisable, based on the
pathogen indentified on blood culture (seek expert microbiological advice if necessary)
If continuing antibiotics for longer than 36 hours despite negative blood cultures, review the baby at least once every 24 hours. On each occasion, using clinical judgement, consider whether it is appropriate to stop antibiotic treatment, taking account of:
• The level of initial clinical suspicion of infection • The baby’s clinical progress and current condition, and • The levels and trends of C-reactive protein concentration.
When deciding on the appropriate care setting for a baby, take into account the baby’s clinical needs and the competencies necessary to ensure safe and effective care (for example, the insertion and care of IV cannulas).
Using clinical judgement, consider completing a course of IV antibiotics.
On completing antibiotic treatment, consider prompt discharge of the baby from hospital, with support for the parents and carers and a point of contact for advice.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 28 of 60
7.5 Duration of treatment: NICE guideline 2010 & 2012 The Guidelines Development Group (GDG) agreed that in babies in whom the CSF culture confirms GBS meningitis, treatment should be continued with benzylpenicillin for at least 14 days and Gentamicin for 5 days. The GDG noted that combining benzylpenicillin and Gentamicin has a synergistic bactericidal effect. This is most beneficial in the early stages of treatment (the first 5 days) and lessens afterwards because Gentamicin does not penetrate the CSF as effectively as benzylpenicillin and it is, therefore, less active against bacteria in the central nervous system. After 5 days the beneficial effect of combining Gentamicin with benzylpenicillin becomes less relevant because of the toxic effects reduced by prolonged exposure to Gentamicin. Toxicity associated with Gentamicin use is similar to the long-term sequelae of meningitis itself (for example hearing loss) and so the GDG sought to limit he duration of Gentamicin use to 5 days to reduce the risk of such effects. The GDG recommended that antibiotic treatment be continued beyond 14 days if the baby remains unwell. The GDG also noted that it is not routine practice to repeat lumbar puncture, but this may be helpful if the baby’s condition is not improving. Treat bacterial meningitis due to Listeria with intravenous amoxicillin or ampicillin for 21 days in total, plus Gentamicin for at least the first 7 days. Treat bacterial meningitis due to Gram-negative bacilli with intravenous cefotaxime for at least 21 days unless directed otherwise by the results of antibiotic susceptibilities. If the clinical course is complicated consider extending the duration of treatment and consulting an expert in paediatric infectious diseases. Recommendations relating to duration of antibiotic treatment for unconfirmed bacterial meningitis In unconfirmed but clinically suspected bacterial meningitis, treat with cefotaxime plus either ampicillin or amoxicillin for at least 14 days. If the clinical course is complicated, consider extending the duration of treatment and consulting an expert in paediatric infectious diseases. Early-onset neonatal infection without meningitis In babies with a strong initial clinical suspicion of infection the NICE GDG recommended a default course length of 7 days. Such babies may be clinically well but have risk factors for early-onset neonatal infection, or they may have clinical indicators of possible infection. The NICE GDG considered that for babies in whom there is still clinical concern of infection at 7 days, consideration should be given to continuing antibiotic treatment. The GDG also agreed that laboratory evidence (a positive blood culture) of a pathogen requiring a longer duration of treatment might trigger extension of antibiotic treatment beyond 7 days, Different antibiotics:
• First line: Start Benzylpenicillin and Gentamicin • Cefotaxime for - confirmed meningitis with gram negative bacilli • Amoxicillin and Gentamicin if Listeria is suspected • If the baby has recently been treated and antibiotics were stopped within 48 hours start
Flucloxacillin and Gentamicin, otherwise start Benzylpenicillin and Gentamicin • Add Metronidazole if NEC is suspected. • Start Teicoplanin and Gentamicin if long line infection is suspected • Vancomycin is used for Coagulase negative sepsis.

Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 29 of 60
• Others antibiotics (e.g. Augmentin, Flucloxacillin, Ceftazidime, Meropenem) to be used after discussion with Consultant on call or Consultant Microbiologist.
• If staph infection is suspected – start Flucloxacillin and Gentamicin.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 30 of 60
8. Respiratory distress 8.1 Presentation One or more signs of increased work of breathing: tachypnoea, grunting, nasal flaring and chest wall retractions. There are many causes of respiratory distress, this can include: • RDS • Pnuemothorax • Pneumonia • Meconium Aspiration syndrome • Transient tachypnoea of the newborn • Persistent pulmonary hypertension of the newborn • Chronic lung disease • Pulmonary haemorrhage • Upper airway obstruction:
o Pierre-Robin sequence o Subglottic stenosis o Choanal atresia o Laryngomalacia
• Congenital chest/lung anomalies: o Congenital diaphragmatic hernia o Trachea-oesophageal fistula o Congenital cystic adenomatoid malformation o Congenital lobar emphysema o Small chest syndromes o Pulmonary hypoplasia o Congenital abnormalities of surfactant
• Non-respiratory causes: o Metabolic acidosis, Perinatal asphyxia, Congenital heart disease, Severe anaemia
8.2 Initial Management: if unsure involve senior input • ABC resuscitation, temperature stability. • Review history: gestation, type of delivery, time of rupture of membranes, risk factors for infection,
maternal diabetes, and meconium stained amniotic fluids etc. • Examine baby • SATS monitoring • Admit to Special care unit if indicated • Check BP and Temperature • IV access • Bloods: Glucose, FBC, CRP, Culture, Gas. • Start IV fluids (60ml/kg/day 10% dextrose) • Start IV antibiotics (broad spectrum Benzylpenicillin and Gentamicin) • CXR Respiratory support: (guided by clinical state, oxygen requirements and blood gases) • Ambient/nasal cannula oxygen • Nasal CPAP • Positive pressure ventilation
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 31 of 60
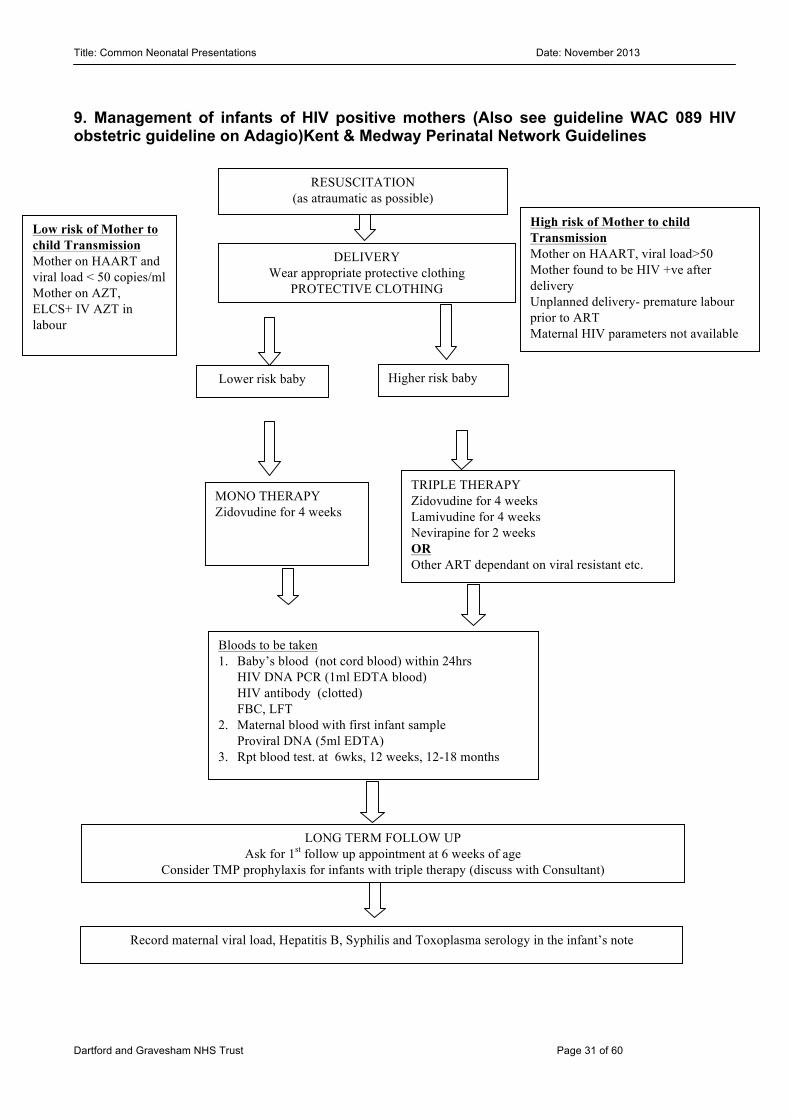
9. Management of infants of HIV positive mothers (Also see guideline WAC 089 HIV obstetric guideline on Adagio)Kent & Medway Perinatal Network Guidelines
DELIVERY Wear appropriate protective clothing
PROTECTIVE CLOTHING
RESUSCITATION (as atraumatic as possible)
Higher risk baby Lower risk baby
TRIPLE THERAPY Zidovudine for 4 weeks Lamivudine for 4 weeks Nevirapine for 2 weeks OR Other ART dependant on viral resistant etc.
MONO THERAPY Zidovudine for 4 weeks
Low risk of Mother to child Transmission Mother on HAART and viral load < 50 copies/ml Mother on AZT, ELCS+ IV AZT in labour
High risk of Mother to child Transmission Mother on HAART, viral load>50 Mother found to be HIV +ve after delivery Unplanned delivery- premature labour prior to ART Maternal HIV parameters not available
Bloods to be taken 1. Baby’s blood (not cord blood) within 24hrs
HIV DNA PCR (1ml EDTA blood) HIV antibody (clotted) FBC, LFT
2. Maternal blood with first infant sample Proviral DNA (5ml EDTA)
3. Rpt blood test. at 6wks, 12 weeks, 12-18 months
LONG TERM FOLLOW UP Ask for 1st follow up appointment at 6 weeks of age
Consider TMP prophylaxis for infants with triple therapy (discuss with Consultant)
Record maternal viral load, Hepatitis B, Syphilis and Toxoplasma serology in the infant’s note
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 32 of 60
9.1 Advice to be given to avoid Breast feeding and BCG vaccination. Maintain Confidentiality and ask mother about information sharing with GP/partner etc. Zidovudine Oral >34 weeks: 4 mg/kg twice daily for 4 weeks 30–34 weeks: 2 mg/kg twice daily for 2 weeks then 2 mg/kg three times a day for 2 weeks <30 weeks: 2 mg/kg twice daily for 4 weeks Lamivudine Oral 2 mg/kg twice daily for 4 weeks. Nevirapine 2mg/kg PO OD for week 1 followed by an increase up to 4mg/kg PO OD for week 2, then stop. (Duration of treatment 2 weeks).
Intravenous Term: 1.5 mg/kg four times a day Prem: 1.5 mg/kg twice daily
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 33 of 60
no
yes no
yes
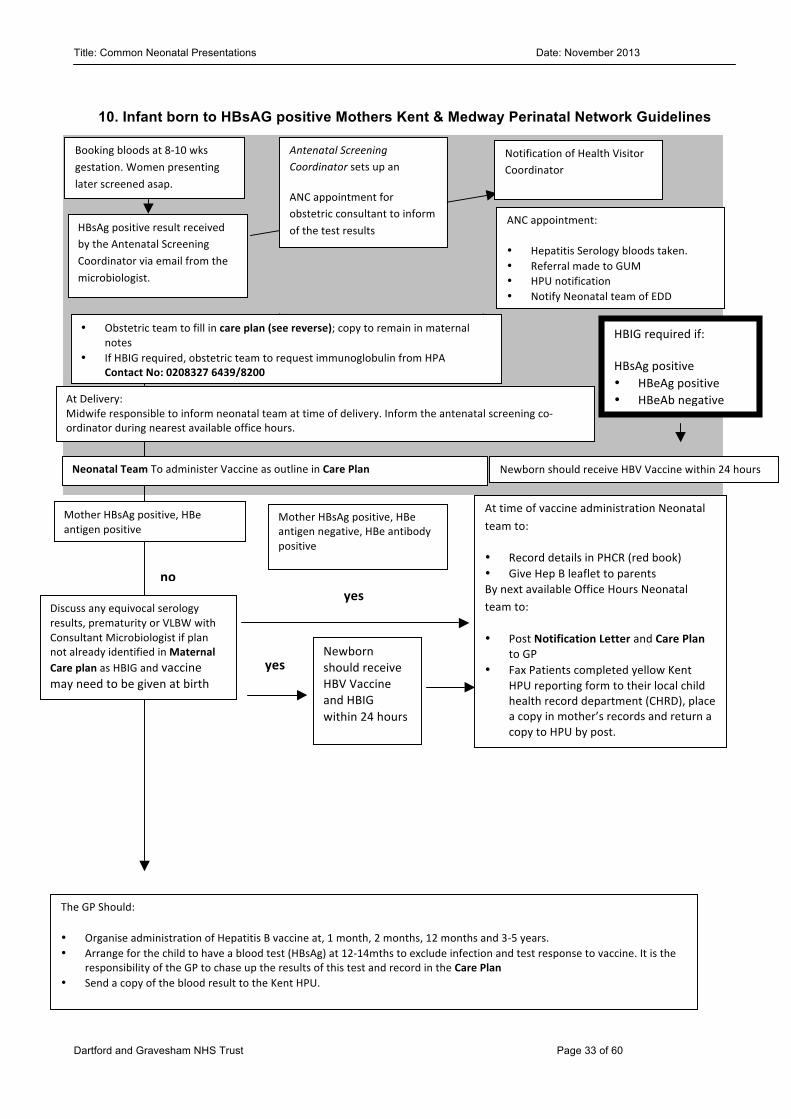
10. Infant born to HBsAG positive Mothers Kent & Medway Perinatal Network Guidelines
HBsAg positive result received by the Antenatal Screening Coordinator via email from the microbiologist.
Antenatal Screening Coordinator sets up an
ANC appointment for obstetric consultant to inform of the test results
ANC appointment:
• Hepatitis Serology bloods taken. • Referral made to GUM • HPU notification • Notify Neonatal team of EDD
Notification of Health Visitor Coordinator
Mother HBsAg positive, HBe antigen negative, HBe antibody positive
Newborn should receive HBV Vaccine within 24 hours
At Delivery: Midwife responsible to inform neonatal team at time of delivery. Inform the antenatal screening co-‐ordinator during nearest available office hours.
At time of vaccine administration Neonatal team to:
• Record details in PHCR (red book) • Give Hep B leaflet to parents By next available Office Hours Neonatal team to:
• Post Notification Letter and Care Plan to GP
• Fax Patients completed yellow Kent HPU reporting form to their local child health record department (CHRD), place a copy in mother’s records and return a copy to HPU by post.
Discuss any equivocal serology results, prematurity or VLBW with Consultant Microbiologist if plan not already identified in Maternal Care plan as HBIG and vaccine may need to be given at birth
The GP Should:
• Organise administration of Hepatitis B vaccine at, 1 month, 2 months, 12 months and 3-‐5 years. • Arrange for the child to have a blood test (HBsAg) at 12-‐14mths to exclude infection and test response to vaccine. It is the
responsibility of the GP to chase up the results of this test and record in the Care Plan • Send a copy of the blood result to the Kent HPU.
• Obstetric team to fill in care plan (see reverse); copy to remain in maternal notes
• If HBIG required, obstetric team to request immunoglobulin from HPA Contact No: 0208327 6439/8200
Mother HBsAg positive, HBe antigen positive
Newborn should receive HBV Vaccine and HBIG within 24 hours
Booking bloods at 8-‐10 wks gestation. Women presenting later screened asap.
HBIG required if:
HBsAg positive • HBeAg positive • HBeAb negative
Neonatal Team To administer Vaccine as outline in Care Plan
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 34 of 60
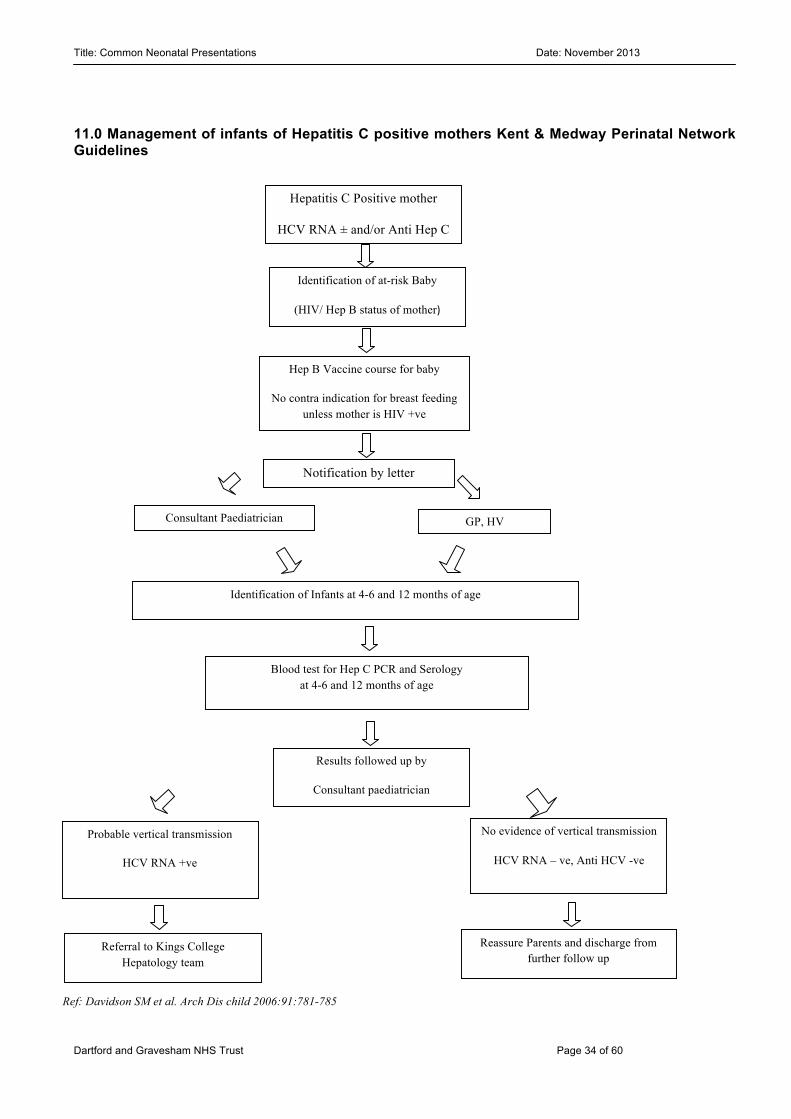
11.0 Management of infants of Hepatitis C positive mothers Kent & Medway Perinatal Network Guidelines
Hepatitis C Positive mother
HCV RNA ± and/or Anti Hep C Ab ±
No evidence of vertical transmission
HCV RNA – ve, Anti HCV -ve
GP, HV
Results followed up by
Consultant paediatrician
Probable vertical transmission
HCV RNA +ve
Identification of Infants at 4-6 and 12 months of age
Consultant Paediatrician
Referral to Kings College Hepatology team
Notification by letter
Hep B Vaccine course for baby
No contra indication for breast feeding unless mother is HIV +ve
Identification of at-risk Baby
(HIV/ Hep B status of mother)
Blood test for Hep C PCR and Serology at 4-6 and 12 months of age
Reassure Parents and discharge from further follow up
Ref: Davidson SM et al. Arch Dis child 2006:91:781-785
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 35 of 60
12. Neonatal Blood Transfusion Introduction
Neonatal transfusion is used when the following scenario is encountered: • Anaemia • Babies with cardio-respiratory disease. • Shock due to blood loss - APH in delivery suite • Prematurity
Guideline of suggested thresholds for children under 4 months of age
• Anaemia in 1st 24 hours Hb <120 g/L Hct <0.36 • Cumulative blood loss in 1 week
of neonate requiring intensive care 10% blood volume. • Neonate receiving intensive care Hb 120g/L • Acute blood loss 10% • Chronic oxygen dependency Hb 100g/L • Late anaemia – stable patient Hb 70g/L
In addition, consider transfusion in stable babies with Hb 7-10 g/dl if • Weight gain <10g/kg/day or reduction in linear growth velocity despite optimal nutrition or • Retic count <100,000, lactate >2.5mmol/l • Clinical indication after discussion with Consultant. There is an arrangement in place which ensures a Consultant request for red cells during the first 24hrs of a child’s life will not be challenged by Blood Bank staff, regardless of the patients Hb status. There is a NEONATAL CODE RED policy for urgent request for blood in the delivery suite. 12.1 Transfusion History Remember, if the patient has been transferred from another hospital it is extremely important to include/source any transfusion history and state this on the request form. Also, a child who has a history of intrauterine/exchange transfusion will require irradiated blood products in the first year. 12.2 Maternal sample and history Neonates do not produce their own blood group antibodies in the first few month of life. Their blood may however contain circulating maternal antibody. If the laboratory does not have a recent result of the maternal antibody screen they will ask for a (one off) maternal sample for group and screen. If the mother is known to have antibodies, a maternal sample will be required for cross-matching blood intended for her baby. If you have any queries, please contact the blood bank. 12.3 Sample from baby less than 4 months of age Sample required is a minimum of 0.5ml EDTA blood. Sample from baby more than 4 months of age Minimum volume 2 mls EDTA sent in a 4 ml EDTA bottle as this must be tested for antibody production 12.4 Small volume transfusion “top ups” (10-20ml/kg) Blood for this will be supplied as paedipacks, - where one blood donation is divided into 6 aliquots. This enables repeated transfusions to be given from one donation. It is important when ordering the first unit to indicate to blood bank staff whether further units may be required so they can reserve the stock.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 36 of 60
12.5 Exchange transfusion This is a specialist procedure which should be undertaken by experienced staff to manage severe anaemia and/or severe hyperbilirubinaemia. Darent Valley patients are usually transferred to Medway or elsewhere via EBS. Please remember that if the patient returns to Walnut ward the transfusion history should be relayed to the blood bank staff when requesting blood products. 12.6 Intrauterine transfusions
This procedure is not performed at D.V.H. However consider the patient may have been transfused at a specialist centre before returning to Walnut ward. This information must be relayed to Transfusion staff when requesting blood products.
12.7 Platelets Consider transfusion if:-
• Preterm or term neonate, with bleeding count 50 x 109/l . • Sick preterm or term infant, not bleeding count 30 x 109/l . • Stable preterm or term infant, not bleeding count 20 x 109/l . • If there is petechaie, bruising, bleeding or co-existent coagulopathy / DIC or concurrent use of
anticoagulants count <50 x 109/l When unexpected thrombocytopenia occurs in a neonate Neonatal alloimmune thrombocytopenia (NAIT) must be considered. NAIT is where the neonate’s platelets are destroyed / impaired by maternal platelet antibodies which have crossed the placenta. Specially selected platelets are issued from NHSBT once testing of maternal and paternal samples has been performed to select compatible units.
If it appears that the neonate has Thrombasthenia, advice must be sought from the consultant haematologist. 12.8 Fresh Frozen Plasma (FFP) (virally inactivated) Be aware that FFP is often supplied as group AB. It is used for:
• Disseminated Intravascular Coagulation (DIC) with Clinical bleeding. • Severe liver disease • Bleeding due to sepsis • Congenital thrombotic thrombocytopenia (TTP) syndromes. • PT or APTT ratio >2 in well, stable babies <28 wks gestation in 1st week of life • PT or APTT ratio >1.5 in any baby and
o active bleeding o in 1st week of life with IVH o sick (discuss with consultant) o about to undergo LP, central line or chest drain
• Vitamin K deficiency is suspected in bleeding baby ( Haemorrhagic disease of the newborn) - give with IV vitamin K
12.9 Cryoprecipitate (virally inactivated) Cryoprecipitate is a fibrinogen rich product prepared from plasma. It is used for Hypofibrinogenaemia where the fibrinogen level is < 1g/l, <0.8 -1.0g/l in context of DIC or in ttreatment of patients with fibrin stabilising factor (FactorXIII deficiency). Please refer to the BCSH website for guidelines and further information on: Transfusion guidelines for neonates and older children http://www.bcshguidelines.com/4_HAEMATOLOGY_GUIDELINES.html?dpage=1&dtype=Transfusion&dstatus=All&dsdorder=&dstorder=&dmax=10&dsearch=&sspage=0&ipage=0#gl
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 37 of 60
13. Polycythaemia Definition Central Venous Haematocrit >70% or >65% with symptoms especially in high risk groups. (Haematocrit (Hct) has linear relationship with viscosity up to 60%, but over 65-70%, the viscosity increases exponentially and 25% of babies with Hct of 65% will have increased red cell viscosity) 13.1 Sample Peripheral venous (free flow sample) or arterial haematocrit. (Capillary, well perfused, sample is only useful for screening and always followed by peripheral venous sample if >65%) 13.2 High risk groups Small for gestational age Downs Syndrome Post-maturity Twin to twin transfusion Infants of diabetic mothers Maternal pregnancy induced hypertension 13.3 Symptoms Hypoglycaemia, jaundice CNS - lethargy, irritability, feeding problems, jitteriness, convulsions Tachypnoea, cyanosis, CCF, PPHN Poor circulation, CRT > 4 sec Thrombosis - cerebral infarction, NEC, renal 13.4 Management • Peripheral venous/arterial haematocrit (Hct) > 65% with symptoms or >70% - perform partial
exchange transfusion (see below) • Dehydration (>8 % wt loss) – give normal saline 20 ml/kg over 1 hour and recheck Hct at 4 hr • If haematocrit 65-69% without symptoms – recheck at 4 hr. If in doubt about partial exchange
discuss with consultant 13.5 Partial exchange transfusion Volume of saline for exchange (ml) = weight (kg) x 80ml x [(measured Hct - desired Hct)
measured Hct (Where desired Hct approx 50) 13.6 Procedure: (under ECG monitor) • Place peripheral venous cannula and start infusion of replacement normal saline (usually over one
hour); give 10ml/kg saline before starting to remove blood • Place either UAC / peripheral arterial cannula or high position UVC for removal of blood • Recheck Hct immediately after exchange and after 6 hours
Cautious feeding for 24 hours after partial exchange References 1. Letsky. Textbook of Neonatology 3rd edition, Rennie 1999; 834-838 2. Doyle. Effective care of the Newborn Infants 1992; 833-834
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 38 of 60
14.0 Maternal and neonatal thyroid disease. Under the influence of TRH, TSH stimulates the thyroid to synthesize and release thyroxine (T4) and triiodothyronine (T3). T4 is deiodinated peripherally to the active compound T3. Most T3 is produced in this way. Fetal and neonatal thyroid function • The hypothalamic-pituitary axis is functional by 20 weeks gestation. • Initially T4 is deiodinated to reverse T3 (rT3) which is inactive. • During gestation TSH, T4 and T3 gradually increase and rT3 gradually falls. • At birth there are:
- Sudden surges in TSH, T4 and T3 which return to near normal by 3 days of age - This is less in preterms and T4 may take some weeks to rise to normal levels.
• Maternal thyroid hormones - Maternal T4 crosses the placenta well in the first trimester, but this decreases with increasing
gestional age - TSH and T3 do not cross the placenta (due to poor permeability and placental deiodinases).
14.1 Maternal thyrotoxicosis 95% is due to Grave’s disease due to TSH receptor stimulating immunoglobulins (TSI) which cross the placenta. TSI are sometimes balanced by TSH inhibiting immunoglobulins (TII) which also cross the placenta. TSI may be produced whether thyroid gland treated, active, inactive or after surgery. Neonatal thyrotoxicosis occurs in only 1% of cases. 14.2 Maternal antithyroid drugs • Propylthiouracil (PTU) and carbimazole (CB) are not teratogenic. • PTU and CB do cross the placenta - therefore need to monitor fetus for goitre (1-2%), bradycardia, +/- cordocentesis for TFTs. • Can Rx fetal hypothyroidism with intra-amniotic thyroxine. • 10-20% neonates have asymptomatic hypothyroidism for +/-5 days (no Rx needed). 14.3 Neonatal thyrotoxicosis • Rare. Most cases are transient and due to maternal Grave’s disease. (rarely permanent due to a TSH receptor mutation) • May cause intra-uterine or neonatal death • Presents at 1-6 weeks, resolves by 4-6 months Signs and symptoms
- IUGR, goitre, proptosis, oedema, sweating - Irritable, appetite↑, weight↓, diarrhoea - Tachycardia, arrhythmia, heart failure, acrocyanosis - Hepatosplenomegaly, enlargement of thymus, lymphadenopathy - Thrombocytopenia, PCV↑ - Advanced skeletal maturation
Diagnosis - T4↑ (and TSH↓) after 3 days of age
- Isotope scan not usually necessary • Management – ( Discuss with on call consultant; Paediatric Endocrinologist as necessary
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 39 of 60
- Measure TFTs at 7-10 days in all babies of mothers who have had/have Grave’s disease. - If thyrotoxic, discuss with paediatric Endocrinologist use same antithyroid medication as mother (usually propylthiouracil or carbimazole) - May need to use high doses and add thyroxine to achieve normal T4 levels. - Can add propranolol and aqueous iodine - Breast feeding: if maternal daily dose =/>15mg carbimazole or =/>150mg propylthiouracil, split
the dose and monitor baby’s thyroid function. If lower maternal dose than above - no risk. 14.4 Maternal hypothyroidism • Usually due to Hashimoto’s thyroiditis (antibodies do not usually cross the placenta). • Can be due to iodine deficiency. • If mother hypothyroid in pregnancy, particularly in first trimester, increased incidence of subsequent
neurodevelopmental delay. (50% if hypothyroidism due to iodine deficiency) 14.5 Neonatal hypothyroidism • 1: 3500 live births Causes
- Aplastic, hypoplastic or ectopic thyroid (sporadic) (TSH↑,T4↓,T3+/-↓) 85-90% - Biochemical defect (usually autosomal recessive) (TSH↑,T4↓,T3+/-↓) 10-15% - Hypothalamic (T4 and T3↓, TSH +/- ↑) - Pituitary (TSH, T4, T3 all↓) 2% - Transient hypothyroidism - particularly preterm babies 2% - (?due to iodine↓; iodine↑ from antiseptic use; TSH receptor antibodies)
Signs and symptoms - At birth – LGA, postmature, delayed bone age, umbilical hernia, +/- goiter, +/- RDS - First 4/52 – sleepy, poor feeding, constipation, abdominal distension, hypothermia, poor
perfusion, oedema, prolonged jaundice - Late – cretinous appearance, growth failure, delayed development, hearing loss
Diagnosis - TSH↑ on Guthrie Card taken at 1 week – TSH>10mU/L. (after 1 week >5mU/L) Confirm with full
TFTs. N.B. This test will not pick up the rare cases of hypothalamic/pituitary hypothyroidism - Full TFTs – TSH>10mU/L (usually much >10mU/L) (unless pituitary/hyopothalamic cause), T4↓,
T3 may be normal initially but ↓ later - Clinical suspicion (often late). Confirm with full TFTs. - TRH stimulation and radioisotope scanning rarely indicated in newborn but if so must be done before or immediately after starting treatment - If there is any evidence of maternal thyroid disease, check baby’s TFT’s at 4-7 days.
Treatment Discuss with Consultant on call and Dr Hulse and refer to Paediatric Endocrine Clinic on discharge from the Neonatal Unit
- Delay in starting Rx beyond the first few weeks of life compromises neurodevelopment particularly if initial T4 levels are very low.
- As soon as the diagnosis made and blood for confirmatory TFTs taken (do not wait for results) – start thyroxine 10-15µg/kg once daily (Discuss with Endocrinologist)
- Monitor TFTs weekly initially to maintain T4 at upper limits of normal - TSH may remain ↑ but only increase thyroxine if TSH remains raised beyond the first few weeks. - At 6-8weeks, monitor TFTs, growth, and development and thereafter 2-3 monthly
-
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 40 of 60
15.0 Care of the baby whose mother is drug dependant. (Also see WAC007 Substance and Alcohol Misuse Guidelines on Adagio) This includes mothers on such drugs as heroin, morphine, Pethidine, methadone and cocaine and also babies whose mothers have had prolonged analgesia, e.g. in sickle cell disease, and mothers who are alcoholic. Withdrawal symptoms in the baby may occur from day 1 up to day 7 and in mothers dependent on methadone seizures may occur even later. Monitoring is necessary to detect and treat withdrawal symptoms and to assess the mother’s ability to adequately care for her baby. 15.1 Delivery
• The neonatal team should be informed of the baby’s delivery and the baby should be reviewed soon after birth, when it should be ascertained what drugs the mother has been taking, by what route and how recently.
• Check mother’s HIV, Hepatitis B and C status and act accordingly. • Naloxone should not be used as it may provoke a serious or even fatal withdrawal reaction. • Inform the Social Worker of the birth as soon as possible.
15.2 Postnatal care
• Look in mother’s notes and ‘Antenatal File’ for information about pre-birth planning. • The baby is kept with mother on the postnatal wards and monitored for withdrawal symptoms. • Drug withdrawal symptoms should be scored 4 hourly from birth and recorded on a drug
withdrawal chart. The midwife should call the SHO/Reg if the score is >4. • TPR 4 hourly • Minimal handling • If there are signs of withdrawal, monitor for signs of dehydration • Send urine for toxicology to the Poisons Unit at New Cross Hospital as soon as possible after
birth. Inform mother and obtain consent wherever possible. • If the mother has been on cocaine, a cranial u/s scan should be done. • Breast feeding should be encouraged unless the mother is a poly-user or she known to be HIV
positive or if HIV status is unknown and she is known or suspected to be an intravenous drug user. If in doubt discuss with registrar or consultant.
• A feed chart must be kept by the mother but supervised by the midwife. • Weigh on alternate days • All babies must be kept in hospital for at least a week or until symptoms have been controlled
and the baby is gaining weight. 15.3 Medication Indications:
• Withdrawal score persistently >4 • Seizures • Inability to feed, sleep or gain weight.
15.4 Dose and drug: Refer to pharmacy guidelines for new morphine preparation.
• Oral morphine: Initial - 0.04mg/kg 4 hourly • Increase by 0.02mg/kg/dose until control achieved
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 41 of 60
Continue this dose for at least a week. If the baby is then stable, feeding well and gaining weight, attempts may be made to reduce the dose. However the controlling dose may sometimes need to be maintained for up to 6 weeks Regime for reducing dose – reduce frequency of dose to 6, 8,12, 24 hourly on a 2-7 day basis; discontinue at a dose of 0.04mg/kg daily
15.5 Discharge
• No baby should be discharged without prior consultation with the Social Worker. A discharge planning meeting needs to be organized. There should be a written discharge plan from the Social Worker in the baby’s notes prior to the sanctioning of the baby’s discharge.
• Inform GP / Health Visitor of discharge (i.e. discharge letter at time of discharge) • All babies need an outpatient appointment in the follow-up clinic after discharge.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 42 of 60
16. Summary of feeding guidelines (Also WAC 069 see Infant Feeding guideline on Adagio) Breast milk is strongly preferred for all babies. Maternal breast milk is the first choice if it is available. Even the tiniest amount of colostrum should be used. Term formula can be used on appropriately grown babies of > 34weeks gestation and > 1.8 kgs if the mother does not wish to breast feed. Preterm formula <34 weeks, <1800g consider risk factors but breast milk would be preferable. The risk of NEC is low in stable babies. A preterm Stage1 ( < 1800 gm) formula can be used in the absence of any risk factors. Change to Pre term stage 2 formula if wt > 1.8 kgs or at discharge. Post discharge formula suitable for infants from discharge to 6 months corrected age. Change to normal term formula when weight gain adequate or crosses 2 centile upwards. Standard risk Start feeds at 30 mls/kg/day and increase 30 mls/kg/day as tolerated. High risk babies High risk cases of any gestation should be discussed with the attending consultant.
• Gestation < 27 +6 weeks or > 28+0 wks and ‘sick’ [unstable baby with problems such as hypoxaemia, hypotension etc.]
• IUGR <34+0 weeks +/- antenatal doppler absent or reversed EDF • Severe SGA infant (0.4th centile and >34 weeks gestations) • Twins ( mono and di-chorionic) <32+0weeks • Perinatal hypoxic- ischaemia with significant organ dysfunction; HIE – Sarnat stages 2 & 3 • Polycythaemia ( arterial PCV>65 – who require partial dilutional exchange) • Congenital gut malformations - gastroschisis
High risk babies
• Trophic feeding is commenced with EBM or peptijunior soon after birth at 20mls/kg/day 2 hourly for duration of 1-2 days. Then increase by 20/mls/kg/day to achieve full feeds. Some babies in this group may be increased by 30 mls/kg/day if tolerating well and after risk assessment by Consultant.
If on peptijunior - pre-term formula may be introduced by slow regrade over 3-6 days (cautious approach). • Do not have combination of 3 milks – EBM +fortifier and pre term formula + peptijunior. • If preterm formula is started in addition to EBM and BMF, the fortifier should be stopped once 50% of requirements are given as formula.
16.1 Necrotising Enterocolitis When initiating or starting feeds A. Post proven NEC (all gestational ages)
- mother’s breast milk if available - Pepti-Junior
B. Post laparotomy and resection for NEC : as above re: choice of milk. Babies who have had significant bowel resection are likely to remain on hydrolysate/amino acid formula for the first year of life. These individual cases will be discussed with tertiary units and Paediatric surgeons.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 43 of 60
C. If conservatively managed NEC – continue breast feeds. If on Peptijunior - > tolerated full feeds for 1 week, baby can be gradually regraded over a minimum of 3-6 days to Pre term (< 1.8 kg) or term formula.
There is no evidence to support the use of term elemental/semi elemental formulas –Neocate / Nutramigen AA in the early stages of feeding unless there is a compelling clinical reason to do so. Grading on to formula – use the quarters rule If mother’s milk is in decreasing supply/ unavailable
• Start with ¼ formula for 24 hr (i.e. 3 EBM to 1 formula feed, 3:1) • Increase by ¼ every 24 hr as tolerated i.e. regrading should take minimum 3 days or upto 6
days in high risk cases (2:1→ 1-1 →all formula feeds). A Cochrane review from 2001 recommends careful restriction of fluid intake so that physiological needs are met without allowing significant dehydration. This practice may minimise the risks of patent ductus arteriosus and necrotising enterocolitis – and perhaps the overall risk of death – without significantly increased risk of adverse consequences. Guidelines for milk intake for healthy term babies Day 1 - 60 mL/kg/day Day 2 - 90 mL/kg/day Day 3 - 120 mL/kg/day Day 4 - 150 mL/kg/day Day 5 - 150 ml/kg/day Desired milk intake: Aim for 150 -180mls/kg/day of breast milk. Sick babies and those that are IUGR, hypoglycaemic, HIE - will have their fluid intakes prescribed individually. Fluid requirements: No additives are required in intravenous fluids for the first 24 - 48 hours of life. Sick term babies may not improve GFR until the 3rd day, and preterm babies’ respiratory outcome is likely to be worse if sodium is added before natriuresis and weight loss has started. Do not automatically increase fluids or add electrolytes on day 2 particularly if baby has respiratory distress or low sodium or decreased urine output. Discuss with Senior. Above fluid regimen may alter depending on: 1. Gestation – very premature babies, <28 weeks, have high insensible losses and may require more
fluid than this. Incubator humidification is very important in these babies. 2. Clinical state e.g. oedema (reduce fluids or increase more slowly) or dehydration (may need more
fluids). 3. Perinatal asphyxia – fluid restriction. 4. Serum sodium – the best guide to hydration in the first few days of life, especially in preterm;
hypernatraemia indicates dehydration. 5. Weight – daily weights are required in all HDU/ unwell babies. Beware of increasing the fluids and
consider fluid restriction in any unwell baby that has gained weight from birth during the first week of life.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 44 of 60
Weight loss from birth will usually indicate that the baby has started to have an obligatory sodium requirement.
6. Urine output – should be at least 1 mL/kg/hour Vitamins: (see separate guidelines on ADAGIO) Dalavit 0.3ml orally once daily is started D7 when the infant is on full feeds of breast milk EBM +/- fortifier, or term formula. Sytron .On D28 the baby will normally receive iron as Sytron 1 mls daily. Babies on full feeds with preterm or pre term follow on formulas – no need for vitamin or iron supplements. Breast milk fortifier (BMF) Breast milk fortifier can be considered if:
• Weight gain is not satisfactory and the infant is on a maximum tolerable volume 165 - 180/mls/kg/day. Baby has been on full feeds for > 1 week
• The blood urea is less than 2mmol/l Breast milk fortifier needs to be started at ½ strength and then slowly increased, if needed, to full strength. Infants on fortified expressed breast milk will still need iron supplementation as breast milk fortifier contain no iron. Fortified feeds should be kept in the fridge for not more than 4 hours. ♦ Never mix fortifier with formula milk (studies have shown an increase risk of gastrointestinal
calcium bolus obstruction)
Gaviscon Infant Sachets Can be used in a dietary management of infants who are
• vomiting and possetting more than usual • have recurrent vomiting as in gastro oesophageal reflux
Phosphate supplements The plasma calcium and phosphorus concentrations in babies <1500 gms or on diuretics should be monitored. Aim for a Phosphate level of 1.8 - 2.2 mmol/L and a Calcium level of 2.15-2.65 mmol/L, with Ca>P and Alk Phos < 500. Add buffered phosphate if Phosphate <1.8 and rising ALP >500 and continue to monitor. If the serum phosphate level is normal, but the alkaline phosphatase remains high (>900IU), calcium supplements should be considered. If plasma calcium falls below 2.2 mmol/L, phosphorus supplements should be reduced, or calcium supplements commenced. Do not add further phosphate if the urine phosphate is high; secondary hyperparathyroidism can occur which can cause iatrogenic hypocalcaemia. If no increase in phosphate levels and ALP continues to rise, consider ergo/alphacalcidol. Check urine calcium and phosphate:
• Urinary Calcium/Phosphorous ratio <1 implies Calcium depletion, with more Calcium supplementation needed
• Urinary Calcium/Phosphorous ratio >1 implies depletion of Phosphate stores.

Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 45 of 60
If phosphorus and calcium are both added to feeds, the phosphorus should be added first. Another way of avoiding co-precipitation is to give the calcium separately. Usually babies on phosphate supplements are reviewed at discharge to consider stopping the supplements if phosphate and calcium levels are normal and ALP is <500.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 46 of 60
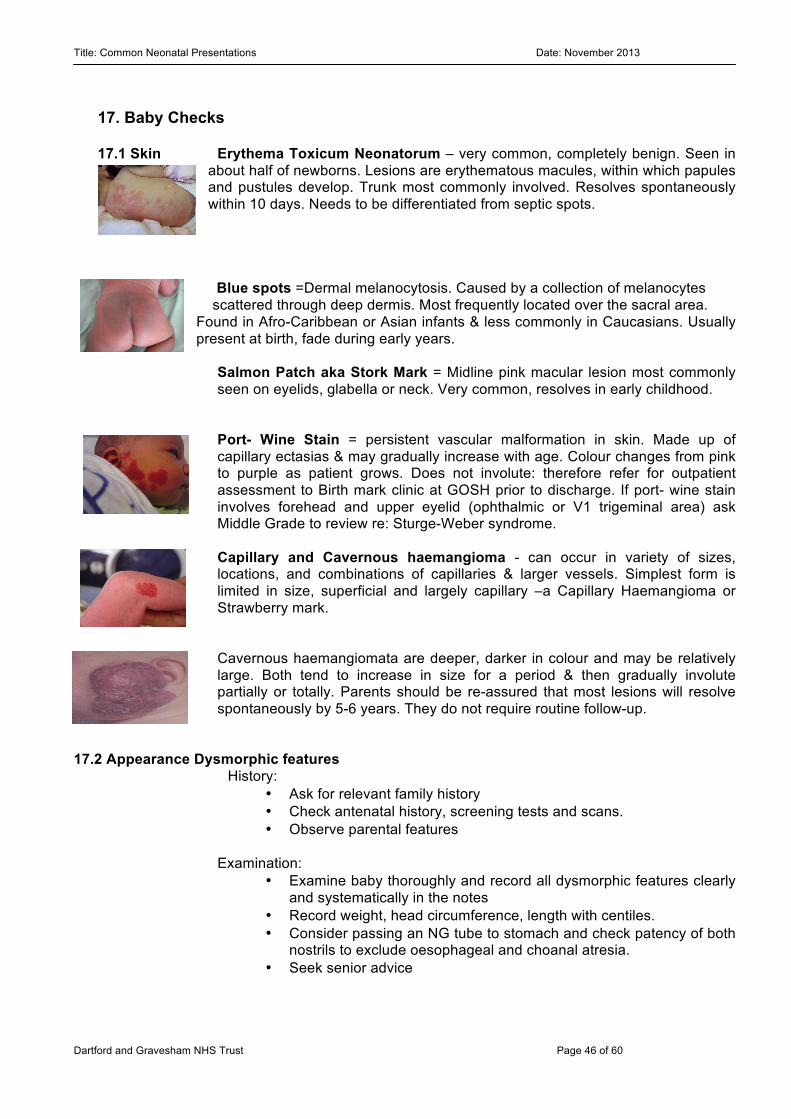
17. Baby Checks 17.1 Skin Erythema Toxicum Neonatorum – very common, completely benign. Seen in
about half of newborns. Lesions are erythematous macules, within which papules and pustules develop. Trunk most commonly involved. Resolves spontaneously within 10 days. Needs to be differentiated from septic spots.
Blue spots =Dermal melanocytosis. Caused by a collection of melanocytes scattered through deep dermis. Most frequently located over the sacral area. Found in Afro-Caribbean or Asian infants & less commonly in Caucasians. Usually present at birth, fade during early years.
Salmon Patch aka Stork Mark = Midline pink macular lesion most commonly seen on eyelids, glabella or neck. Very common, resolves in early childhood. Port- Wine Stain = persistent vascular malformation in skin. Made up of capillary ectasias & may gradually increase with age. Colour changes from pink to purple as patient grows. Does not involute: therefore refer for outpatient assessment to Birth mark clinic at GOSH prior to discharge. If port- wine stain involves forehead and upper eyelid (ophthalmic or V1 trigeminal area) ask Middle Grade to review re: Sturge-Weber syndrome. Capillary and Cavernous haemangioma - can occur in variety of sizes, locations, and combinations of capillaries & larger vessels. Simplest form is limited in size, superficial and largely capillary –a Capillary Haemangioma or Strawberry mark. Cavernous haemangiomata are deeper, darker in colour and may be relatively large. Both tend to increase in size for a period & then gradually involute partially or totally. Parents should be re-assured that most lesions will resolve spontaneously by 5-6 years. They do not require routine follow-up.
17.2 Appearance Dysmorphic features
History: • Ask for relevant family history • Check antenatal history, screening tests and scans. • Observe parental features
Examination: • Examine baby thoroughly and record all dysmorphic features clearly
and systematically in the notes • Record weight, head circumference, length with centiles. • Consider passing an NG tube to stomach and check patency of both
nostrils to exclude oesophageal and choanal atresia. • Seek senior advice
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 47 of 60
Possible further investigations: • Array CGH • Rapid PCR test for specific disorders (Trisomy 13, 18 and 21). • DNA analysis (seek prior genetics opinion if necessary, so that
specific test can be arranged) • Chest, Abdomen, spine X ray • Cranial, renal and abdomen US • ECHO • Eye examination by paediatric ophthalmologist • Hearing screen • Keep nil by mouth and give IV fluids if any doubt about gut
malformation
Down’s syndrome: Diagnosis made antenatally:
• Check fetal ECHO findings for evidence of congenital heart disease • Full clinical examination, particularly CVS • Check result of antenatal karyotype • Seek senior review
Diagnosis suspected postnatally:
• See early and perform full examination, particularly of Cardiovascular system
• Seek immediate senior review • Be sensitive to parents’ anxiety and , if necessary, say you are
asking a more senior doctor to see the baby • Take blood for e and request urgent PCR for Trisomy 21 • Consider checking FBC for polycythaemia, transient
myeloproliferative disorder and thrombocytopenia
Once confirmed or if diagnosis likely on clinical grounds: • Refer for echocardiogram and discuss with paediatric cardiologist • Consider the presence of associated problems e.g. duodenal atresia,
hirschsprung’s. • Ensure appropriate feeding assessment and support • Ensure parents receive appropriate counselling.
Consultant or registrar should have covered the following issues:
• Confirmation of the diagnosis, with discussion of the genetics (94% full Trisomy 21, 2.4% mosaic, 3.3% translocation ) and arranged follow-up with a geneticist
• Developmental delay and learning difficulties • High incidence of congenital heart disease (~45%) • Potential for feeding problems, hypotonia, visual impairment (e.g.
squint and cataracts), hearing impairment, duodenal atresia, hypothyroidism (1%), leukaemia (< 1%) and recurrent UTI’s & otitis media, short stature
• Reassure about close community follow-up with many healthcare professionals
• Give written information about Down's Syndrome and refer to Early Support groups
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 48 of 60
Follow up: • Paediatrician (within a few weeks of discharge) • Geneticist • SALT (if necessary) • Hearing screening • Early support group • Ophthalmologist (3-6 months) • Inform GP and health visitor • Early referral to community paediatrician
17.3 Eyes: Mild discharge or sticky eye: advice regular cleaning, lacrimal duct massage
Discuss with Registrar/Cons if moderate or severe periorbital cellulitis Moderate: If discharge is heavy, muco purulent , the eye is red or swollen:
• Eye swab MC+S (chase and change antibiotics according to sensitivities). Remember gonococcus and chlamydia
• Topical chloramphenicol eye drops every 4 hours for 5 days.
• Consider starting IV antibiotics – discuss with Consultant.
Severe periorbital cellulitis: • IV antibiotics
17.4 Ears: Look at shape of ear helical pattern, oits transverse ear lobe crease
Hearing assessment as OPD if on Gentamicin > 5 days /Gent overdose/diagnosed meningitis
17.5 Scalp: Caput seccadaneum (measure and advice to observe closely)
Cephalhaematoma: If severe may develop jaundice and anaemia Differentiate from subgaleal haemorrhage
17.6 Face: Shape or dyspmorphism,
In Forceps delivery: (Look for bruising mark) SBR
Take a photograph Examine for facial palsy (D/W senior re: follow up) Shoulder dystocia: Examine clavicle for fractures (X ray if necessary) Examine for Erb’s palsy (D/W senior re: follow up) Physio referral on PNW ALL instrumental deliveries – monitor closely for signs of scalp bleed/ unwell baby. Consider suspected subgaleal bleed /intracranial bleed if seizures, changes in tone or looking pale ( Will need urgent neuro imaging). Discuss with Registrar or Consultant.
17.7 Heart: Murmurs: -Check femorals
-ECG, CXR, Preductal and postductal SATS (Rt upper limb and Rt lower limb) and 4 limb BP -Ask Middle Grade to review- child cannot be discharged without senior review and NOT BEFORE 24 HOURS - Follow heart murmur guidelines of Dr Ali Bokhari
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 49 of 60
If unwell, abnormal investigations, loud or diastolic murmur or significant murmur present beyond 24 hours D/W Consultant re: ECHO -If discharging after > 24 hours and baby well - arrange week review with Consultant. -Ask parents to return if symptoms suggestive of cardiac disease- e.g. breathlessness, sweatiness, not completing feeds, failure to gain weight, cyanosis etc.
17.8 Fingers: Polydactyly: OPD referral to Plastic surgeons at East Grinstead 17.9 Male genitilia Hypospadias: -Ensure baby has normal urinary flow and is well.
-Arrange follow up appointment in Consultant clinic. Then at a later stage referral will be made to Consultant Paediatric Surgeon for outpatient assessment. -If very severe hypospadia or ambiguous genitalia ask for Middle Grade review ASAP.-Tell parents NOT to circumcise baby Consider renal USS
Testes: Undescended testes, for r/v by GP and refer by 8/12 - 1 year of age if still concerns. Babies with bilateral undescended testis and hypoplastic scrotum consider USS.
Any testicular swelling – Consider differential diagnosis of testicular torsion and discuss with Consultant for urgent investigations and transfer.
17.10Hips: Clicky Hips:
i) with obvious dislocation – arrange inpatient USS of hips & refer to orthopaedics (Mr Addison) as inpatient. Use double nappies. ii) without obvious dislocation- review prior to discharge, arrange outpatient USS if still clicky. If breech delivery or first degree family history of Developmental dysplasia of hips (DDH), any positional deformities, arrange OPD USS.
17.11 Feet: Talipes Equino-varus:
Positional: Foot can be passively moved through full range but tends to adopt equino-varus position when baby is relaxed.
- Arrange Physio to r/v on ward and make a plan. Positional talipes usually self corrects within first few days after birth. If foot is still turning in when baby is actively kicking after a week, parents should take baby to GP.
Sturctural (Fixed): Foot cannot be moved passively through full range of movement or feels stiff.
-Refer immediately to physio within 12 - 24 hours of birth. -Refer baby to Orthopaedic surgeon to be seen in outpatient clinic-(may need to Refer to Maidstone Ponsetti clinic) -F/U with Paediatric consultant to exclude neuromuscular disease.
If in doubt whether a talipes is fixed or positional, ask paediatric physiotherapist to review. Talipes Calcaneo-valgus
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 50 of 60
Foot is held in extreme dorsiflexion up against shin. Usually due to position in utero and self corrects. If the baby’s foot cannot be passively stretched to 900 or feels stiff then refer to Physio. Refer to Orthopaedic surgeons for review before 3 months of age.
17.12 Sacral dimple: Ensure that you see a skin base. The following skin markers over or near spine be regarded as suspicious:
• Birth marks – vascular, pigmented (except blue spots). • Discrete hairy patches (not merely slightly increased hairiness over the
lower back). • Swellings/ lumps/ appendages/ skin tags. • Possible sinuses – where intact skin cannot be demonstrated. • Pits and dimples above natal cleft. Asymmetric natal cleft
These should be referred to a Middle Grade for review and investigations. Remember that most babies with these markers will be normal & parents should be told this.
17.13 Renal Pelvis Dilatation All babies with antenatal finding of RPD ≥ 5.0 mm at second trimester even resolved in third trimester Or RPD≥ 7.0 mm at third trimester needs postnatal ultrasound and follow up. On postnatal ward: Start trimethoprim 2mg/kg nocte Check BP *RPD <10 mm - Arrange Postnatal Renal USS at 6 week *If AN scan showed / suggested - Hydroureter - Calyceal dilation - RPD > 10.0 mm (uni or bilateral) Inform Reg on call.
Arrange Postnatal USS within 24-48 hrs if bilateral or else within 1 week. Renal functions on D2. Do not discharge the baby without discussion with Consultant on call for further management.
*If male baby has bilateral renal pelvic dilatation – posterior urethral valves may be the cause. – Ensure renal USS performed BEFORE discharge (i.e. 24-48 hrs of age) Advise parents explaining need for follow up, vigilance for UTI’s & continued prophylaxis. Arrange follow up with consultant at 6-8 weeks. 17.14 Delayed passage of meconium Most healthy babies pass meconium within 24 h of birth. Delay beyond 24 h is unusual and underlying pathology should be considered. Possible aetiologies are: Meconium ileus Meconium plug Intestinal dysmotility, particularly in growth restricted baby Hirschprung’s disease Imperforate anus Prematurity
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 51 of 60
Management: Review full history with mother and midwives; ensure that no meconium was passed prior to delivery.
Examine maternal notes for polyhydramnios or other abnormalities of AN scans Take feeding history ? bilious vomiting, abdominal distension Fully examine baby, clinical state, perfusion, abdo distension, tenderness and check anus If <24 h old, baby is well with no vomiting and normal examination then -> Observe closely
If >24 h old or <24 h but with concerning features in history or examination, consider bowel obstruction, Hirschprung’s disease, enterocolitis and sepsis:
Admit to Neonatal unit Seek senior review AXR and discuss with consultant
If meconium plug is passed, IRT (spot blood on Guthrie card) for Cystic fibrosis should be checked. Hirschsprung’s disease should also be considered.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 52 of 60
18. BRACHIAL PLEXUS INJURIES It is important to record the details of delivery and management in the notes as this frequently results in complaint / litigation in later years. • Risk factors - The usual mechanism is traction of the upper extremity away from the head and
neck and stretching the nerve roots as they exit from the cervical spine. The delivery is often prolonged or traumatic or with shoulder dystocia and the infant is large.
18.1 Erb’s palsy • C5-C6 nerve roots • "waiter's tip" position - decreased or absent shoulder abduction with elbow extension, forearm
internal rotation and wrist flexion 18.2 Klumpke's palsy (rare) • C8-T1 nerve roots • “claw hand” - intrinsic muscles of the hand involved, along with wrist and finger flexors,
sympathetic nerves leading to Horner’s syndrome and also hyperabduction of shoulder 18.3 Erb-Duchenne-Klumpke palsy • C4-T1 nerve roots • entire arm paralysed • raised hemidiaphragm may occur if extensive enough lesion to involve C4 Management:
1. Chest and arm x-ray to exclude clavicle and humerus fracture. 2. Assess and record full neurological examination of affected limb − Position including flexion / extension of elbow / wrist − Extent of spontaneous movement of shoulder, elbow and wrist and degree of reduction of
movement (e.g. reduced or absent Moro reflex on affected side) − Muscle tone and tendon reflexes − Presence or absence of grasp reflex. − Assess for signs of respiratory distress (implying diaphragm involvement) or unequal pupils
(Horner’s syndrome) which may indicate a worse prognosis. 4. Inform the Registrar/consultant. They will give appropriate information to the parents re. Likely course / prognosis. This information should be clearly recorded in the patient’s notes 5. Physiotherapy before discharge (the primary goal is to avoid contractures of the involved joints by preserving a full range of passive movements). 6. Neonatal clinic 4-6 weeks. 7. Prognosis
• 80-90% chance of full recovery in all but most extensive lesions • For extensive lesions or if weakness persists >3 months, refer to Mr Birch at the
Peripheral Nerve Injury Unit at the Royal National Orthopaedic Hospital, Stanmore for nerve conduction studies, MRI and possible surgical exploration.
References 1. Hensinger – Textbook of Neonatology, Rennie 1999; 1085-86 2. Aston – Orthopaedic 1999; 2: 594-601

Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 53 of 60
3. Guy’ Neonatal guidelines 4. Medway NNU guidelines
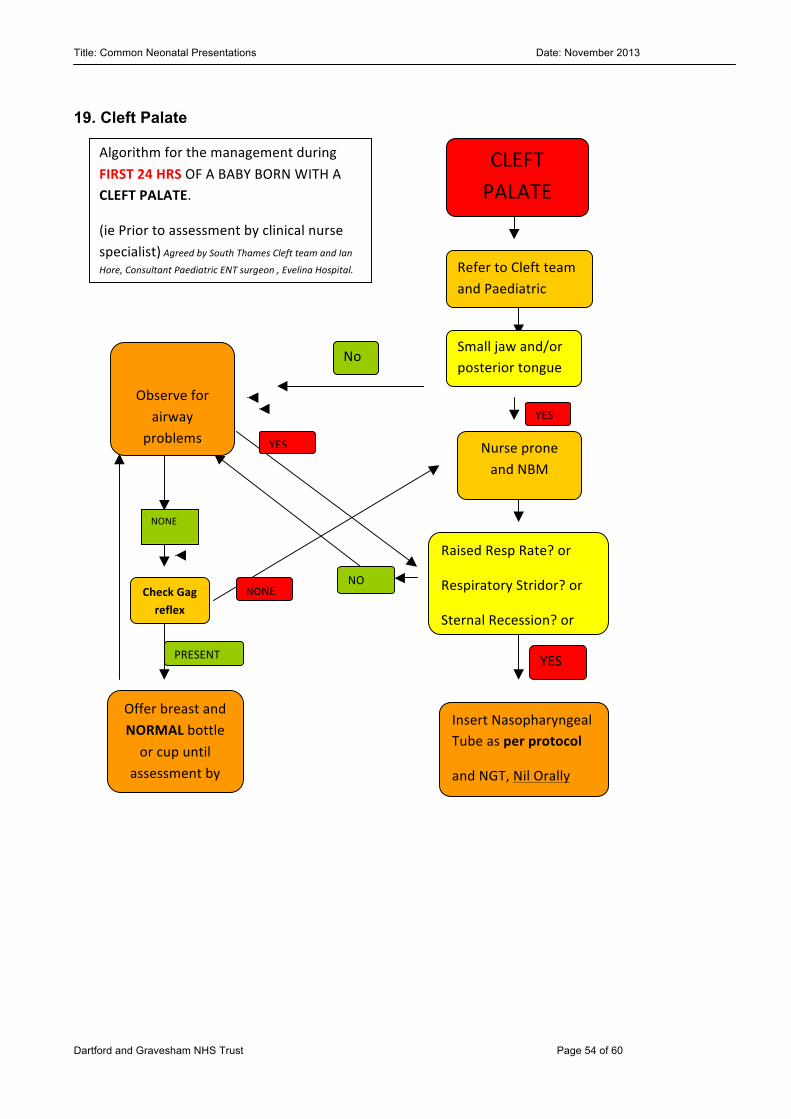
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 54 of 60
19. Cleft Palate
CLEFT PALATE
Refer to Cleft team and Paediatric team
Small jaw and/or posterior tongue
Nurse prone and NBM
Monitor o2 sats NONE
NO
YES
YES
PRESENT
No
YES
Check Gag reflex
NONE
Raised Resp Rate? or
Respiratory Stridor? or
Sternal Recession? or
Tracheal Tug? or
Low Oxygen Saturation?
Algorithm for the management during FIRST 24 HRS OF A BABY BORN WITH A CLEFT PALATE.
(ie Prior to assessment by clinical nurse specialist) Agreed by South Thames Cleft team and Ian
Hore, Consultant Paediatric ENT surgeon , Evelina Hospital.
Reviewed March 2012
Insert Nasopharyngeal Tube as per protocol
and NGT, Nil Orally
Offer breast and NORMAL bottle or cup until
assessment by CSN
Observe for airway
problems
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 55 of 60
19.1 Management of babies with oro-facial clefts In cases of antenatally suspected cases, the parents may have already seen the Cleft Lip and Palate Team. They should be offered details of the CLAPA Association and appropriate literature given. The baby does not need admission to NICU unless there are other factors e.g. cleft palate with significant micrognathia, prematurity, hypoglycaemia etc. Transitional care is the preferred option. Examination To exclude other abnormalities / associations. If these are present, the on-call consultant should be informed. Investigations Echocardiography Cranial USS Renal tract USS (as OPD) A Karyotype [including 22q Fish] should be requested in all babies with cleft palate. Inform Giselle Murphy on 07810 483923 / Wendy Tuohy on 07768 474876 Cleft Nurse Specialist South Thames Cleft Service On-call Consultant in cases of cleft palate with significant micrognathia. These babies with Pierre-Robin sequence may have significant difficulties in maintaining an airway and will often require a Guedal oral airway and prone position or a naso-pharyngeal airway. The Neonatal Outreach Nursing Team will need to be involved closely with the care of these babies at home and will require specific monitoring of pulse-oximetry, feeding and growth. Ask Ophthalmologist to exclude Marshall-Stickler syndrome only in cases with Pierre-Robin sequence. Before discharge from hospital It should be confirmed that the baby can feed adequately and there is access to a supply of special teats or Haberman bottles. All relevant agencies have been contacted, including speech therapy, whose help may be needed if significant feeding difficulties are encountered. A discharge summary with plans for follow-up should be sent to GP at the time of discharge. Follow up - Named Consultant
Cleft Lip and Palate team
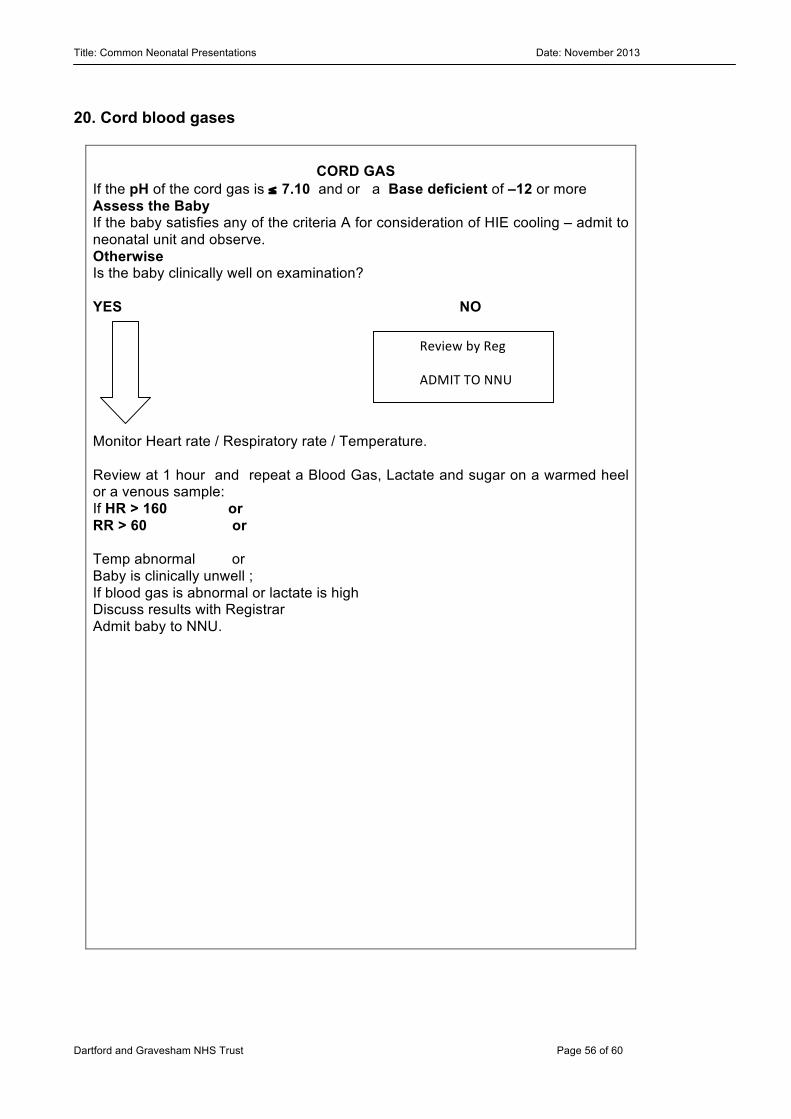
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 56 of 60
20. Cord blood gases
CORD GAS If the pH of the cord gas is ≤ 7.10 and or a Base deficient of –12 or more Assess the Baby If the baby satisfies any of the criteria A for consideration of HIE cooling – admit to neonatal unit and observe. Otherwise Is the baby clinically well on examination? YES NO Monitor Heart rate / Respiratory rate / Temperature. Review at 1 hour and repeat a Blood Gas, Lactate and sugar on a warmed heel or a venous sample: If HR > 160 or RR > 60 or Temp abnormal or Baby is clinically unwell ; If blood gas is abnormal or lactate is high Discuss results with Registrar Admit baby to NNU.
Review by Reg
ADMIT TO NNU
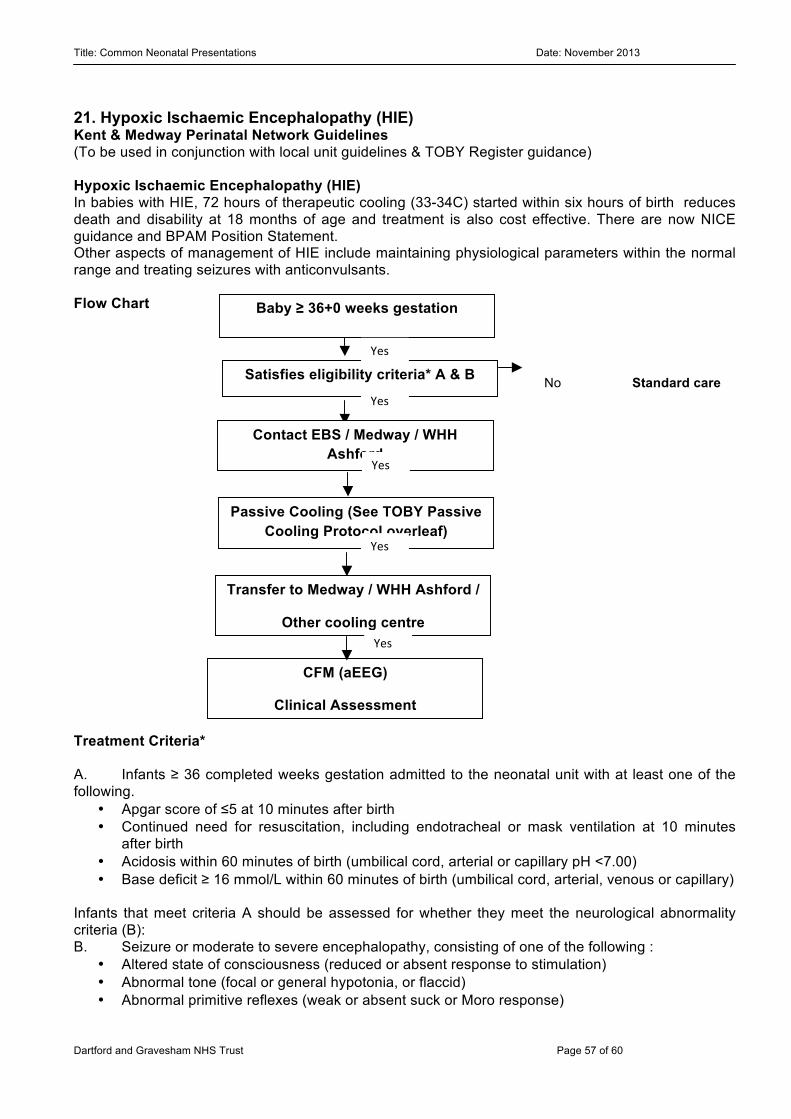
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 57 of 60
No
21. Hypoxic Ischaemic Encephalopathy (HIE) Kent & Medway Perinatal Network Guidelines (To be used in conjunction with local unit guidelines & TOBY Register guidance) Hypoxic Ischaemic Encephalopathy (HIE) In babies with HIE, 72 hours of therapeutic cooling (33-34C) started within six hours of birth reduces death and disability at 18 months of age and treatment is also cost effective. There are now NICE guidance and BPAM Position Statement. Other aspects of management of HIE include maintaining physiological parameters within the normal range and treating seizures with anticonvulsants. Flow Chart Treatment Criteria* A. Infants ≥ 36 completed weeks gestation admitted to the neonatal unit with at least one of the following.
• Apgar score of ≤5 at 10 minutes after birth • Continued need for resuscitation, including endotracheal or mask ventilation at 10 minutes
after birth • Acidosis within 60 minutes of birth (umbilical cord, arterial or capillary pH <7.00) • Base deficit ≥ 16 mmol/L within 60 minutes of birth (umbilical cord, arterial, venous or capillary)
Infants that meet criteria A should be assessed for whether they meet the neurological abnormality criteria (B): B. Seizure or moderate to severe encephalopathy, consisting of one of the following :
• Altered state of consciousness (reduced or absent response to stimulation) • Abnormal tone (focal or general hypotonia, or flaccid) • Abnormal primitive reflexes (weak or absent suck or Moro response)
Baby ≥ 36+0 weeks gestation
born with signs of perinatal asphyxia
Satisfies eligibility criteria* A & B Standard care Yes
Contact EBS / Medway / WHH Ashford
(Cot & Transport available)
Yes
Yes
Passive Cooling (See TOBY Passive Cooling Protocol overleaf)
Yes
Transfer to Medway / WHH Ashford /
Other cooling centre
CFM (aEEG)
Clinical Assessment
Cooling
Yes
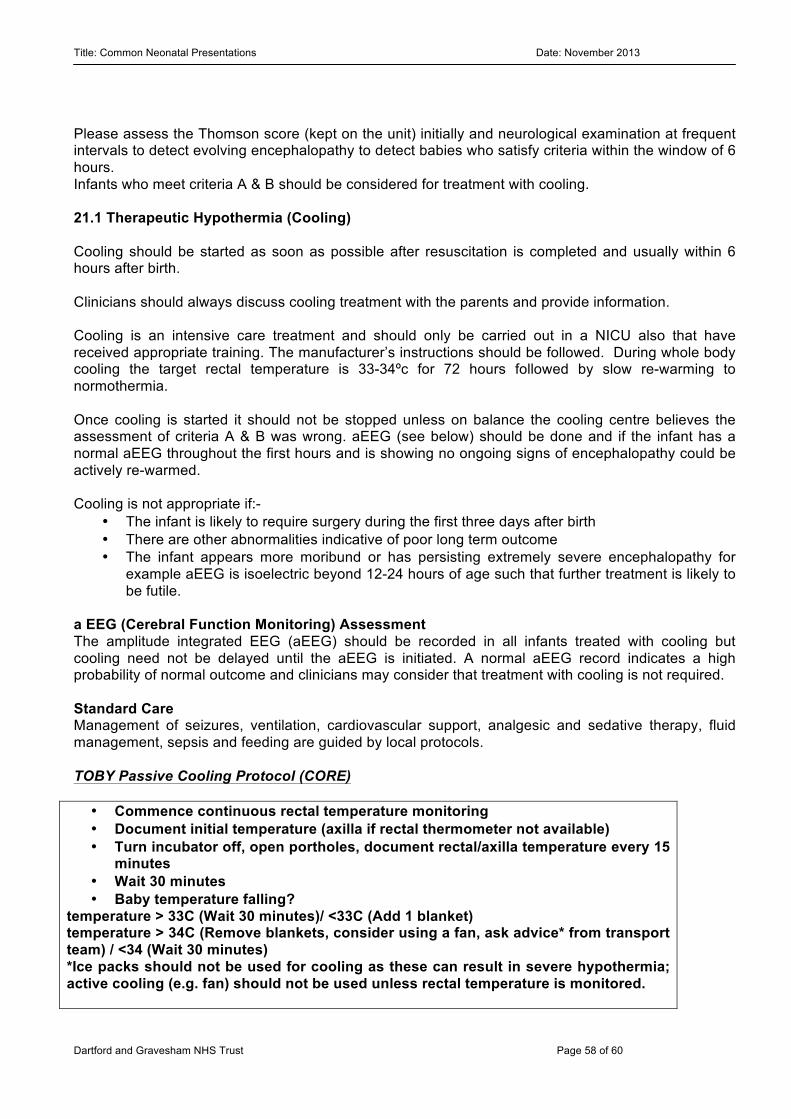
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 58 of 60
Please assess the Thomson score (kept on the unit) initially and neurological examination at frequent intervals to detect evolving encephalopathy to detect babies who satisfy criteria within the window of 6 hours. Infants who meet criteria A & B should be considered for treatment with cooling. 21.1 Therapeutic Hypothermia (Cooling) Cooling should be started as soon as possible after resuscitation is completed and usually within 6 hours after birth. Clinicians should always discuss cooling treatment with the parents and provide information. Cooling is an intensive care treatment and should only be carried out in a NICU also that have received appropriate training. The manufacturer’s instructions should be followed. During whole body cooling the target rectal temperature is 33-34ºc for 72 hours followed by slow re-warming to normothermia. Once cooling is started it should not be stopped unless on balance the cooling centre believes the assessment of criteria A & B was wrong. aEEG (see below) should be done and if the infant has a normal aEEG throughout the first hours and is showing no ongoing signs of encephalopathy could be actively re-warmed. Cooling is not appropriate if:-
• The infant is likely to require surgery during the first three days after birth • There are other abnormalities indicative of poor long term outcome • The infant appears more moribund or has persisting extremely severe encephalopathy for
example aEEG is isoelectric beyond 12-24 hours of age such that further treatment is likely to be futile.
a EEG (Cerebral Function Monitoring) Assessment The amplitude integrated EEG (aEEG) should be recorded in all infants treated with cooling but cooling need not be delayed until the aEEG is initiated. A normal aEEG record indicates a high probability of normal outcome and clinicians may consider that treatment with cooling is not required. Standard Care Management of seizures, ventilation, cardiovascular support, analgesic and sedative therapy, fluid management, sepsis and feeding are guided by local protocols. TOBY Passive Cooling Protocol (CORE) • Commence continuous rectal temperature monitoring • Document initial temperature (axilla if rectal thermometer not available) • Turn incubator off, open portholes, document rectal/axilla temperature every 15
minutes • Wait 30 minutes • Baby temperature falling?
temperature > 33C (Wait 30 minutes)/ <33C (Add 1 blanket) temperature > 34C (Remove blankets, consider using a fan, ask advice* from transport team) / <34 (Wait 30 minutes) *Ice packs should not be used for cooling as these can result in severe hypothermia; active cooling (e.g. fan) should not be used unless rectal temperature is monitored.
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 59 of 60
References
1. UK TOBY Cooling Register Clinician’s Handbook version 3 June 2007 www.npeu.ox.ac.uk/tobyregister.
2. Azzopardi D. et al. For the TOBY Study Group. Moderate Hypothermia to Treat Perinatal
Asphyxial Encephalopathy. NEJM 2009 361:1349-1358 3. NICE IPG374: http://www.nice.org.uk/nicemedia/live/11315/48809/48809.pdf 4. BAPM Position Statement on Therapeutic Cooling for Neonatal Encephalopathy 2010
www.bapm.org/publications/
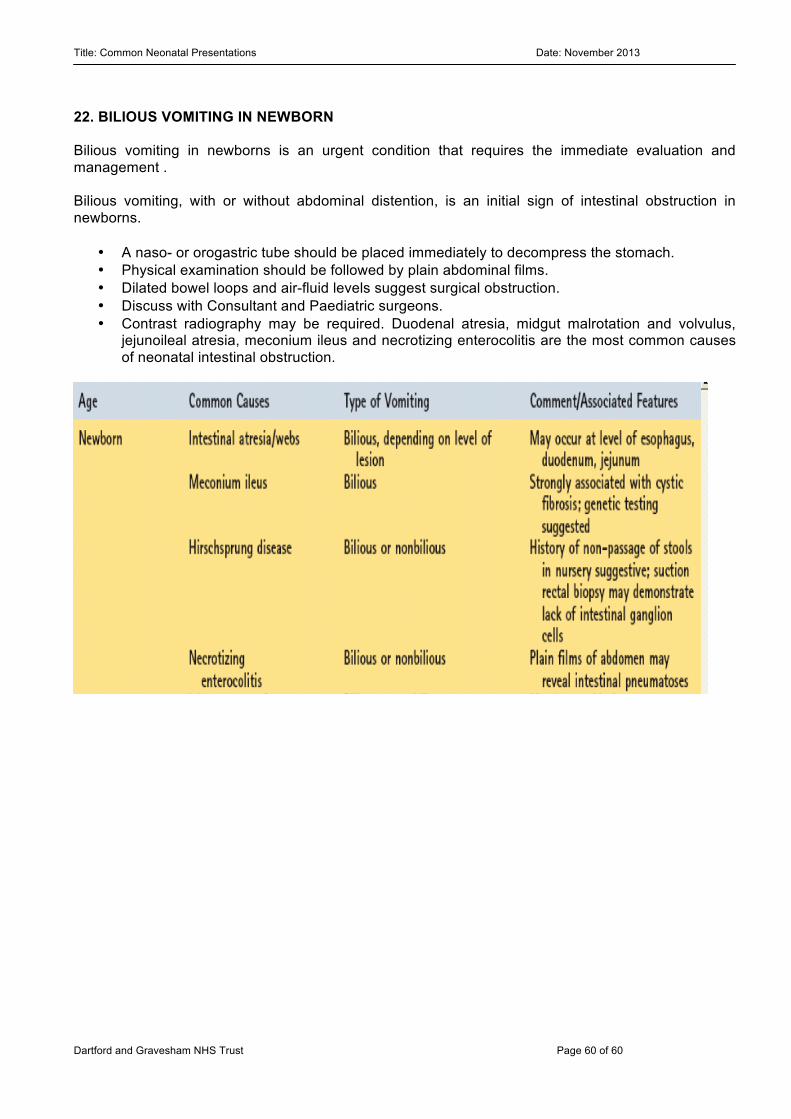
Title: Common Neonatal Presentations Date: November 2013
Dartford and Gravesham NHS Trust Page 60 of 60
22. BILIOUS VOMITING IN NEWBORN Bilious vomiting in newborns is an urgent condition that requires the immediate evaluation and management . Bilious vomiting, with or without abdominal distention, is an initial sign of intestinal obstruction in newborns.
• A naso- or orogastric tube should be placed immediately to decompress the stomach. • Physical examination should be followed by plain abdominal films. • Dilated bowel loops and air-fluid levels suggest surgical obstruction. • Discuss with Consultant and Paediatric surgeons. • Contrast radiography may be required. Duodenal atresia, midgut malrotation and volvulus,
jejunoileal atresia, meconium ileus and necrotizing enterocolitis are the most common causes of neonatal intestinal obstruction.
Related Documents











