-
7/29/2019 Common ENT Conditions PwPT2008
1/75
Common Ear Conditions
F Bhatti ST2Group B9/12/08
-
7/29/2019 Common ENT Conditions PwPT2008
2/75
Outline of the presentation
Few common presentations in general practice related toears. Examining the ears. Ear Wax and syringing. Otitis Externa
. Otitis Media( Acute and Chronic)
. Eustacian tube dysfunction
. Perforations ( Safe vs. Unsafe)
Treatment ( Evidence based)
Lots of pictures!
Few questions( AKT based)
-
7/29/2019 Common ENT Conditions PwPT2008
3/75
Sources (With hyperlinks)
GP Notebookhttp://www.gpnotebook.co.uk/homepage.cfm
CKS
http://cks.library.nhs.uk/home
ENT USA
http://www.entusa.com/index.html Passmedicine
http://www.passmedicine.com/index.php
University of Bristol, Otoscopy tutorialhttp://www.bris.ac.uk/Depts/ENT/otoscopy_tutorial.htm
You Tube
BMJ Learning
Bradford VTS website ( With thanks to Dr R Mehay)
http://www.gpnotebook.co.uk/homepage.cfmhttp://cks.library.nhs.uk/homehttp://www.entusa.com/index.htmlhttp://www.passmedicine.com/index.phphttp://www.bris.ac.uk/Depts/ENT/otoscopy_tutorial.htmhttp://www.bris.ac.uk/Depts/ENT/otoscopy_tutorial.htmhttp://www.passmedicine.com/index.phphttp://www.entusa.com/index.htmlhttp://cks.library.nhs.uk/homehttp://www.gpnotebook.co.uk/homepage.cfm -
7/29/2019 Common ENT Conditions PwPT2008
4/75
ENT Examination
You tube video of ENT examination in an OSCE situation.http://www.youtube.com/watch?v=mDbwAPr5RvU
Ear examination- You tube videohttp://uk.youtube.com/watch?v=I3sa2W83iuo&NR=1
NB:
. The canal may be partly straightened by pulling the pinna backwards
and upwards during examination.. In infants pull the pinna more horizontally backwards as the shape of
the ear canal is different.
http://www.youtube.com/watch?v=mDbwAPr5RvUhttp://uk.youtube.com/watch?v=I3sa2W83iuo&NR=1http://uk.youtube.com/watch?v=I3sa2W83iuo&NR=1http://www.youtube.com/watch?v=mDbwAPr5RvU -
7/29/2019 Common ENT Conditions PwPT2008
5/75
Normal
Anterior
direction
Inferior
Posterio
r
Anterio
r
- Consider the malleus as
an arrow; pointing inthe forward direction.
- The normal tympanicmembrane shouldappear
. pearly grey
. have a light reflex
. generally concave
. and malleus should bevisible
Abnormals:
. Retraction( bones more prominent)
. Perforations
. Bubbles (glue ear, resolving infection)
. White patches (tympanosclerosis orcholesteatoma)
. Granulations
. Red lesion at tip of malleus (glomustumour)
. Grommets/FBs
Attic
-
7/29/2019 Common ENT Conditions PwPT2008
6/75
Ear Drum-normal Landmarks
An annulus fibrosus or morecommonly referred to as
the eardrum margin. This isimportant. Note howsmooth and how ever soslightly blurry it is.
Um umbo - the end of themalleus handle and usuallymarks the centre of thedrum
Lr light reflex or Cone oflightis usually seen antero-inferioirly
At Attic also known as parsflaccida. Any perforationshere are serious and needreferral.
Lp Lateral process of themalleusHm handle of the malleusLpi long process of incus -sometimes visible through ahealthy translucent drum
-
7/29/2019 Common ENT Conditions PwPT2008
7/75
Go systematically
External:
Pinna (shape, colour, position, tenderness, haematoma) etc
Mastoid (tenderness in AOE or mastoid abscess)
Internal:
The Canal ( skin, furuncle, scales,spores,FBs,discharge, debris, wax)
The Tympanic membrane (look ant, post, superior/ attic and inferior of malleus)
. Colour( opaque, white, red, patches & translucency)
. Retraction( landmarks behind it more visible)
. Perforation ( safe/ unsafe)
. Discharge (purulent, mucopurulent)
Behind the Eardrum. Fluid behind the drum( meniscus, air fluid levels, colour, bubbles?..can ask for avalsalva if appropriate)
. Any red bits( glomus tumour, granulations or blood?, white- cholesteotoma)
-
7/29/2019 Common ENT Conditions PwPT2008
8/75
Ear Wax
Wax is produced in the outer halfof the ear canal and migratesoutwards along with the canalskin. Inappropriateinstrumentation can cause
impaction. Wax impaction can causehearing loss, pain, tinnitus,vertigo, or chronic cough butnot usually discharge.
Sudden expansion after getting
water in can cause suddendeafness or pain, but needscareful exclusion of otherpathology behind it e.g.cholesteotoma
Be mindful of other possibilities FB(crayon) in a childs ear
-
7/29/2019 Common ENT Conditions PwPT2008
9/75
Ear Wax.contd
Management:. Educate about non instrumentation of their ear canals.If Symptomatic. Syringing (with use of drops) or wax hook.. Different preparations available none superior to other.
Sodium bicarbonate drops might be better at disintegrating wax, butcan cause dryness of the canal and/ or irritation
. Instructions for use:e.g. Olive oil drops warmed on a warm spoon.Put 2-3 drops in theear and lie on the opposite side for 3-5 mins. Use BD. Get syringed in5-7 days.
. When to refer to ENT clinic:. Patients known to have a tympanic membrane perforation or
previous ear surgery (need microsuction), only hearing ear
. Syringing fails
. Causes pain or vertigo,
. Hearing loss persists after wax removal.
. Keratosis Obturans
-
7/29/2019 Common ENT Conditions PwPT2008
10/75
Otitis Externa
Infection of the external auditory canal. Mediterraneanear/Swimmers ear
Usually unilateral Gradual onset pruritis, pain, hearing loss, and ear discharge which
varies in consistency and colour. Discharge not mucoid inconsistency as no mucin glands are present in the ext aud canal.
The pt is usually well. Can result in a featureless ext aud canal Risk factors: trauma, water, Immunosuppression, eczema Can be fungal- spores might not always be visible If treatment fails or otitis externa recurs
frequently consider sending an ear swab
for bacterial and fungal microscopyand culture
-
7/29/2019 Common ENT Conditions PwPT2008
11/75
Management
Remove or treat any precipitating or aggravating factors. Analgesic A topical ear preparation for 7 days. Options include preparations containing:
a. Both a non-aminoglycoside antibiotic + a corticosteroid e.g. flumetasoneclioquinol (LocortenVioform) ear drops.b. Both an aminoglycoside antibiotic and a corticosteroid (contraindicated if
the tympanic membrane is perforated).c. Topical preparations containing only an antibiotic (gentamicin ear dropsare contraindicated if the tympanic membrane is perforated).d. Antifungal or ? something containing all three
Aural toilet: if earwax or obstruct topical medication (mayrequire referral).
If there is extensive swelling of the auditory canal, considerinserting an ear wick (may require referral). Provide appropriate self-care advice
-
7/29/2019 Common ENT Conditions PwPT2008
12/75
Current Evidence Topical corticosteroids are at least as effective as topical antibiotics
combined with corticosteroids. However, because ofmethodological weaknesses in the clinical trials and because acutediffuse otitis externa is thought to be caused by an infection, topicalcorticosteroids on their own are not generally recommended as first-line treatment
Clioquinol is antibacterial and antifungal and has lower risks of skinreactions and ototoxicity than aminoglycosides. Therefore, ontheoretical grounds, the combination flumetasoneclioquinol mightbe slightly preferred.
Oral Abx: usually where furunculosis and/or extensive spreadingcellulitis- In 1997, GPs prescribed oral antibiotics for 21% of first
episodes of otitis externa. Amoxicillin/ampicillin was the mostfrequently prescribed antibiotic (34%)
Flucloxacillin narrower spectrum but good tissue diffusion
Erythromycin wider spectrum- effective for most sensitive Gram +cocci and some Gramve cocci and anaerobes; Clarithromycin lessGI side effects but more expensive
-
7/29/2019 Common ENT Conditions PwPT2008
13/75
Malignant Otitis Externa
"Malignant" otitis externa is a severe infection due to Pseudomonasaeruginosa and anaerobes causing osteomyelitis of the skull basecharacterised by severe pain, involvement of the floor of the earcanal, sometimes with granulation tissue. If untreated, it can involvethe cranial nerves and brain. It is not a neoplastic process.
Facial nerve palsy occurs in 50% of patients, IX to XII may also beinvolved. immunocompromised patients, especially elderly diabetics.It may be life threatening.
What to look for:Elderly, DM, earotalgia, otorrhoea, hoarseness,puffiness , trismus, failure to respond to drops, granulations, CN palsiesetc
Mx:-Refer
-Intensive local and systemic antibiotics against Pseudomonas arerequired if malignant otitis externa is present, e.g. ciprofloxacin orceftazidime, plus suitable anaerobic cover e.g. metronidazole.
-
7/29/2019 Common ENT Conditions PwPT2008
14/75
Question 1
23 yr old man, 4 days Hx of itchy sore Rt ear; returned recentlyfrom holiday in Spain
O/E= Rt ext auditory canal is inflamed but no debris seen.T.membrane is visible and unremarkable. What is the mostappropriate management?
A. Topical corticosteroid + Aminoglycoside
B. Topical corticosteroid
C. Tell him serves him right for going on a holiday while you work!
D. Topical corticosteroid +Clotrimazole
E.. Oral Flucloxacillin
-
7/29/2019 Common ENT Conditions PwPT2008
15/75
Answer 1
Correct Answer is A.
Dx- Otitis externa- Topical antibiotic or
combined Antibiotic + corticosteroidpreparation
-
7/29/2019 Common ENT Conditions PwPT2008
16/75
Question 2 53 year old man, fastidiously
clean, previously normal
hearing, currently recentonset strange sensation inme ear! + slightlyreducedhearinghave been trying topop them. Perchance; youhad a brilliantpresentation
on ENT conditions from afellow registrar on the last VTShalf day release and yourecognise the cone of light isnormal, but what is this
A. Normal ear drum
B. Otitis Externa secondary toear buds use
C. Serous Otitis Media
D. Time waster/ Hidden agenda
-
7/29/2019 Common ENT Conditions PwPT2008
17/75
Answer 2
Serous Otitis media because of Eustaciantube dysfunction
Has normal cone of light, mild rednessexternally likely normal, fluid level, and mildlyretracted ear drum
-
7/29/2019 Common ENT Conditions PwPT2008
18/75
Question 3
A 28 year old woman presents witha 5 day Hx of pain in her Rt ear,reduced hearing, and yellowcoloured discharge.
A. Keeping this picture in mindwhat test on physical exam could
have given you a clue about thediagnosis.
B. What is the likely diagnosis
a. Acute Otitis Media
b. Acute Otitis Externa
c. Chronic Suppurative Otitismedia
d. Its actually a picture from acolposcopy examination!
-
7/29/2019 Common ENT Conditions PwPT2008
19/75
Answer 3
Tragal tenderness
Answer is Acute Otitis Externa( for those who thought it was a picture from a colposcopy, may be itstime for you to move on to your next job!)
-
7/29/2019 Common ENT Conditions PwPT2008
20/75
Question 4
Which of the following statements aboutotitis externa is correct?
a. You should avoid removing canal debris
b. Its common in people not wearing ear protection whileworking with loud power tools as a divine punishment.
c. It may result in a featureless tympanic membrane
d. It is usually due to a Staphylococcus aureus infection
-
7/29/2019 Common ENT Conditions PwPT2008
21/75
Answer 4
Correct answer- It may result in a featureless tympanicmembrane
Commonest causative organism for infective otitis externa is
Pseudomonas
Could be difficult to eradicate in someone wearing earprotection in certain occupations e.g. forge/factory workers
-
7/29/2019 Common ENT Conditions PwPT2008
22/75
Question 5
Which of the following statements about the use of topicaleardrops is correct?
a. Only use topical ear drops if the tympanic membrane is visible
b. Topical eardrops are contraindicated in children under the age of12years
c. Topical eardrops cannot be used in the presence of a perforatedtympanic membrane
d. Topical eardrops can worsen otitis externa
e. If its difficult putting them in your ears, they are equally effectiveputting them in your nose and standing on your head for 3.37 mins.
-
7/29/2019 Common ENT Conditions PwPT2008
23/75
Answer 5
Correct answer- Topical eardrops can worsen otitis externa if there issensitivity to them
The use of ototoxic drops in the presence of a perforated tympanicmembrane is controversial due to reports of sensorineural hearing loss
as a result of their application. Reports of this association are rare andoften the validity of such reports is questionable. Certainly the risks ofsensorineural hearing loss or of major complications of otitis mediaare of more significance. Limiting the course of treatment andensuring that they are not used in healthy ears can reduce anypotential risks from the administration of ototoxic medicines.
There is no quality evidence supporting putting ear drops in your noseand standing on your head; but there is certainly none to refute it.
-
7/29/2019 Common ENT Conditions PwPT2008
24/75
Otitis Media
Can be acute or chronic
Can be with or without serous effusion (acute orchronic)
Can be Acute or chronic suppurative
Can co-exist with Otitis externa
Otitis media with serous effusion= Glue Ear
-
7/29/2019 Common ENT Conditions PwPT2008
25/75
Acute Otitis Media
Common in children
Unwell/pyrexia, otalgia/discharge there may be tenderness over the mastoid
discharge in meatus
loss of outline of drum and landmarks
TM: red, bulging,oedematous or perforation.
Mostly viral but can be Streptococcus/Haemophilus
Risk factors: Passive smoker
Male
Family history of otitis media.
In day care
On formula feed
-
7/29/2019 Common ENT Conditions PwPT2008
26/75
Current evidence for AOM
80% of children get better by day 3 without antibiotics
It is reasonable to prescribe analgesia.-
Antibiotics should not be used routinely and prescribing them justincreases parental belief and re-attendance rates
Use delayed scripts if necessary
Adenoidectomy, as the first surgical treatment of children aged 10 to24 months with recurrent acute otitis media, is not effective in
preventing further episodes. Neither is Chemoprophylaxis.
Current Evidence for CSOM
Randomised controlled trials (RCTs) found limited evidence thattopical quinolone antibiotics versus placebo improved otoscopic
appearances. RCTs found no clear evidence of significantdifferences between topical antibiotics.
No benefits from anything else.
-
7/29/2019 Common ENT Conditions PwPT2008
27/75
-
7/29/2019 Common ENT Conditions PwPT2008
28/75
AOM (pus behind the eardrum)
-
7/29/2019 Common ENT Conditions PwPT2008
29/75
AOM continued..
Analgesia: For most children, this is the mainstay of treatment.
Antibiotics should not beroutinely prescribed for uncomplicatedAOM.
Some children may significantly benefit from antibiotics. All children aged 6 months and under
. Children aged between 6 months and 2 years where the diagnosis is reasonably
certain.. Children older than 2 years where there aresevere symptoms:. Moderate or severe ear pain (otalgia) with a fever of 39C or above, orsystemic features such as vomiting. Severe local signs, such as perforation with purulent discharge. Bilateral AOM
Choice of antibiotic:Amoxicillin is the usual first-line for 5 days. If severe symptoms present,or there has been a previous episode of AOM within the last month,use high doses (double the standard dose)..Erythromycin (use high doses) or Clarithromycin (use standarddoses) are alternative antibiotics if documented allergy to penicillin.
-
7/29/2019 Common ENT Conditions PwPT2008
30/75
AOM contd 2.
A good compromise is to use issuing a delayed prescription to beredeemed within 72 hours only if the condition has not adequately
improved. Active Follow up for:
. under 2 years of age.
. systemic symptoms such as high temps (> 39C) or vomiting.
. There is discharge from the ear. Visualisation of the tympanicmembrane can be difficult. Re-examine after 2 weeks to assess the
integrity of the membrane and to check for complications. If there is aperforation still present, monitor the situation and considerreferral if ithas not healed after 6 weeks.
Persistent AOM:Pt returning within 2 weeks with same complaints
.Analgesia
.If not had Abx-give Abx e.g. Amoxicillin double the standard dosefor 5/7
. If had Abx-check compliance-If good then try 2nd line Abx e.g. Co-Amoxiclav at double the standard dose for 5/7.
http://cks.library.nhs.uk/otitis_media_acute/management/quick_answers/scenario_first_line_treatment/should_i_refer_or_investigatehttp://cks.library.nhs.uk/otitis_media_acute/management/quick_answers/scenario_first_line_treatment/should_i_refer_or_investigate -
7/29/2019 Common ENT Conditions PwPT2008
31/75
Complications from AOM
Complications from otitis media is extremely low.
> Progression to glue ear and associated hearing impairment> Perforation. In one study 29.5 % children with AOM eardrum perfs.But spontaneously closed in 94 % of the patients within one month.
Rarely to mastoiditis, labyrinthitis, meningitis, intracranial sepsis orfacial nerve palsy.
Recurrent episodes may lead to atrophy and scarring of theeardrum, chronic perforation and otorrhoea, cholesteatoma,permanent hearing loss, chronic mastoiditis and intracranial sepsis.
-
7/29/2019 Common ENT Conditions PwPT2008
32/75
Serous Otitis Media
-
7/29/2019 Common ENT Conditions PwPT2008
33/75
Serous Otitis Media/Secretory
Glue ear, commonest cause of deafness, and the commonestindication for surgery, in children.
The condition is most frequent in early childhood,
Peaks prevalence at 2 and 5 years.
Half of 3-year-olds have at least one effusion in a year, and inthe UK, 1 in 200 children is operated on for the condition.
Ninety thousand operations are performed in England andWales annually, at an estimated cost of 30 million
-
7/29/2019 Common ENT Conditions PwPT2008
34/75
Serous otitis media with retraction
-
7/29/2019 Common ENT Conditions PwPT2008
35/75
A hearing test is not appropriate at the initial presentation if there isno evidence of significant hearing loss or developmental delay. Ifsigns and symptoms of OME continue, hearing should be assessedafter 3 months, where OME can be regarded as persistent.
Consider setting a lower threshold for referral for a hearing test in
younger children (e.g. children aged less than 3 years old) as
communication is more difficult
-
7/29/2019 Common ENT Conditions PwPT2008
36/75
Otitis media+effusion-Glue ear
Features
Dull retracted TM
May show air-fluid level
Conductive hearing loss(whisper test, Rinne/weber tests)
Notes Common in children; often after AOM and can persist for
weeks
Reduced hearing noticed by parents/teacher
Unsteadiness- child falling over
80% clear at 8 weeks
-
7/29/2019 Common ENT Conditions PwPT2008
37/75
Management
Adults presentation - the nasopharynx is examined to excludetumour. Secretory otitis media is uncommon in adults. It usually followsa cold and spontaneously resolves; this may take up to 6 weeks
In Children- 50% of cases will resolve spontaneously within 6 weeks
Persistence of bilateral Otitis media with effusion (OME) and hearingloss in a child should be confirmed over a period of 3 months beforeintervention is considered
Surgery: adenoidectomy or myringotomy and grommet insertion.however a systematic review suggests that the role of grommets inthe management of glue ear is unclear.
Hearing aids: persistent OME, not for surgery
Treatments not recommended are antihistamines,decongestants, steroids ,homeopathy,cranial osteopathy, acupuncture,dietary modification, including
probiotics,immunostimulants, massage
-
7/29/2019 Common ENT Conditions PwPT2008
38/75
About glue ear
A unilateral serous effusion in an adult is due to nasopharyngealtumour until proven otherwise.
Secretory otitis media, or `glue ear', is the most frequent cause ofhearing problems in children. May produce pain or a conductivehearing loss, or may remain symptomless. There is concern thatimpaired hearing in early childhood may interfere with educationand normal development, but the magnitude of these effects is not
clearly established. Over 50% of effusions resolve spontaneously within 8 weeks, but
bilateral hearing loss, persisting 12 months, occurs in 5% of cases
-
7/29/2019 Common ENT Conditions PwPT2008
39/75
Glue Ear vs. Otitis Media
Factors suggestive of a diagnosis of glue ear include:
. frequent attacks of otitis media
. it is unusual for children to get multiple resolving episodes ofotitis media
prolonged signs. otitis media will usually resolve within 6 weeks and certainlywithin three months
Other risk factors: cleft palate ,Down's syndrome, allergy, familyhistory
-
7/29/2019 Common ENT Conditions PwPT2008
40/75
Eustachian Tube Dysfunction
a severely retractedeardrum. Margins are
very clear as is the
malleus and it looks
very sunken.
-
7/29/2019 Common ENT Conditions PwPT2008
41/75
Eustachian Tube dysfunction
Chronic blockage of the Eustachian tube is called Eustachian tubedysfunction. The eustachian tube becomes congested and swollenso that it may temporarily close; this prevents air flow behind the eardrum and causes ear pressure, pain or popping just as youexperience with altitude change when travelling on an airplane oran elevator.
This can occur when the lining of the nose becomes irritated andinflamed, narrowing the Eustachian tube opening or its passageway.
1. Illnesses like the common cold or influenza.
2. Others: pollution, cigarette smoke, allergic rhinitis, obesity
3. Rarely nasal polyps, cleft palate, skull base tumour
-
7/29/2019 Common ENT Conditions PwPT2008
42/75
Eustachian Tube Dysfunction
. Chronic ETD may reveal retraction pockets or collapsed middle eardisease with erosion of incus/stapedius. Difficulty auto-inflating the
ear drum
. Generally the fluid clears spontaneously over a period of severalweeks
. The efficacy of treatments such as nasal decongestants, oraldecongestants, antihistamines is unclear
. Antibiotics may help prevent infection in cases of severebarotrauma
-
7/29/2019 Common ENT Conditions PwPT2008
43/75
ETD & Children
Young children (esp 1 to 6 years) at particular risk because of verynarrow Eustachian tubes. Also, they may have adenoid enlargementthat can block the opening of the Eustachian tube. Since children indaycare are highly prone to getting URTIs, they tend to get more earinfections compared to children that are cared for at home.
Eustachian tube in infants and young children runs horizontally, ratherthan sloping downward from the middle ear. Thus, bottle-feedingshould be performed with the infants head elevated, in order toreduce the risk of milk entering the middle ear space. The horizontalcourse of the Eustachian tube also permits easy transfer of bacteriafrom the nose to the middle ear space.
Most children older than 6 years have outgrown this problem andtheir frequency of ear infections should drop substantially.
-
7/29/2019 Common ENT Conditions PwPT2008
44/75
Chronic Otitis Media
Recurrent ear discharge Hearing loss, painless
Perforation of the TMcentral
Presence of cholesteatoma
Marginal, Attic perforation
Offensive discharge,bleeding, granulations
Complications:
. Vestibular symptoms
. Facial palsy
. Intracranial complications
-
7/29/2019 Common ENT Conditions PwPT2008
45/75
Ear drum Perforations
Safe vs Unsafe Perforations
Safe perforations
. may allow infection to enter the middle ear
. conductive deafness
Unsafe perforations
. in fact represent a retraction of the tympanic membrane.
. essentially a part of the drum becomes sucked inwards and maygradually enlarge.
.when the retraction becomes extensive, keratinous debris builds up
in the retraction and may become infected and an acquiredcholesteatoma develops
-
7/29/2019 Common ENT Conditions PwPT2008
46/75
UNSAFE SAFESource Cholesteatoma Mucosa
Odour Foul Inoffensive
Amount Usually scant,never profuse Can be profuse
Nature Purulent Mucopurulent
-
7/29/2019 Common ENT Conditions PwPT2008
47/75
Unsafe perforations are
a)In the attic or
b)In the posterior region. These are
often linear rather than oval
c)Or involve the eardrum margin
Anything else is generally Safe.
i.e.
a) In the anterior region orb) In the inferior region
c) And not involving the eardrum
margin
MAKE SURE YOU ALWAYS INSPECTTHE ATTIC AREA ON OTOSCOPY!
-
7/29/2019 Common ENT Conditions PwPT2008
48/75
Safe anterior perforation
Perforations in
this position is a
persistent defect
after the
extrusion of a
grommet.
-
7/29/2019 Common ENT Conditions PwPT2008
49/75
Safe inferior perforation
This is more likely to
be as a result of
chronic middle earinfection.
-
7/29/2019 Common ENT Conditions PwPT2008
50/75
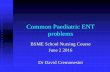
Unsafe posterior perforation
Posterior perforation.
Although posterior
perforations may
represent more
serious disease such
as cholesteatoma,
this is well described
and dry. It is possible
to make out the
posterior margin of
this
defect. Traumatic
perforations (e.g
barotrauma) are often
posterior and linear,like a tear rather than
a round hole.
Theres also some
tympanosclerosis in
this picture.
-
7/29/2019 Common ENT Conditions PwPT2008
51/75
Unsafe attic perforation
Any defect or
apparent perforation
in the attic must be
considered unsafe
and should be
referred for ENT
assessment. This
crust in the attic
represents a large
underlying
cholesteatoma sac.
Note the bulging
eardrum too.
-
7/29/2019 Common ENT Conditions PwPT2008
52/75
Marginal perforation plus cholesteatoma formation
Unsafe because it is a
perforation involving the
drum margin (the yellowy
white flakes indicating a
cholesteatoma also gives
it away!).
-
7/29/2019 Common ENT Conditions PwPT2008
53/75
Cholesteotoma
-
7/29/2019 Common ENT Conditions PwPT2008
54/75
Cholesteatoma
Cholesteatoma is "a three dimensional epidermoid structure
exhibiting independent growth, replacing middle ear mucosa,resorbing underlying bone, and tending to recur afterremoval." There is usually a persistent or recurrent scantycream coloured offensive discharge and progressive hearingloss due to ossicular destruction or toxin induced sensoryhearing loss.
Otoscopy : a pearly white mass usually in the pars tensa +/-discharge and sometimes erosion of the bone. A perforation is usuallypresent, but is not always visible due to overlying keratin. Granulationtissue or polyps may be seen due to chronic inflammation andsometimes retraction pockets are present.
A crust adherent to the tympanic membrane is indicative of acholesteatoma until proved otherwise. They can be reviewedafter a short course of steroid or ceruminolytic ear drops, but ifit is persistent or reveals an underlying abnormality then youshould refer
-
7/29/2019 Common ENT Conditions PwPT2008
55/75
Why is it important to diagnose it?
Cholesteatoma is an important diagnosis asit can cause irreversible hearing loss fromossicular destruction as well as facial nervepalsy, labyrinthitis, lateral sinus thrombosis,meningitis, intracranial abscess, and otitichydrocephalus. It is more easily treated in its
earlier stages. While waiting for their ENT appointment
patients should keep the ear dry and anyinfective discharge can be treated with atwo week course of antibiotic ear drops,with or without steroids. Aural toilet is also
advised if there is debris.
-
7/29/2019 Common ENT Conditions PwPT2008
56/75
Another cholesteotoma
http://www.entusa.com/ear_photographs_html/cholesteatoma-1.htm -
7/29/2019 Common ENT Conditions PwPT2008
57/75
Serous Otitis media
-
7/29/2019 Common ENT Conditions PwPT2008
58/75
Normal ear drum
t th h l t t
-
7/29/2019 Common ENT Conditions PwPT2008
59/75
Yet another cholesteotoma
-
7/29/2019 Common ENT Conditions PwPT2008
60/75
Question 6
A 31 year old man with a history ofrecurrent Otitis media in childhoodsees you on a Tuesday afternoonwith his wife. C/O unilateral leftsided hearing loss. Possibilities are:
a. Cholesteatoma
b. Tympanic membrane retractionpocket
c. He doesnt get along well with theMissus.
d. Tympanic membrane perforation
-
7/29/2019 Common ENT Conditions PwPT2008
61/75
Correct answer-Tympanic membrane retraction pocket
This is a pars tensa retractionpocket which is clean. It isretracted onto the longprocess of the incus. There issome incidentaltympanosclerosis.
Generalised tympanicmembrane retraction andretraction pockets are thoughtto be caused by thinning of thetympanic membrane andnegative middle ear pressure.
Thinning of the tympanicmembrane can be caused bymiddle ear fluid or infections, apoorly healed perforation, orafter extrusion of a grommet
Retraction+ serous OM
-
7/29/2019 Common ENT Conditions PwPT2008
62/75
Haemorrhagic blister on ear drum surface fromshingles
-
7/29/2019 Common ENT Conditions PwPT2008
63/75
Grommet
This grommet is in
the correct position
but is covered in
infectivegranulation and
blocked up. This
will not be doing
any good and may
be responsible for
a chronic
discharge. Notealso the extensive
tympanosclerosis
on the drum.
-
7/29/2019 Common ENT Conditions PwPT2008
64/75
Glomus tumour
. Rare vascular tumour
. Causes pulsatile tinnitus
. Needs surgical removal
. Can erode bone etc over time
-
7/29/2019 Common ENT Conditions PwPT2008
65/75
Glomus tumour
-
7/29/2019 Common ENT Conditions PwPT2008
66/75
Chronic otitis externa
-
7/29/2019 Common ENT Conditions PwPT2008
67/75
Serous Otitis Media
-
7/29/2019 Common ENT Conditions PwPT2008
68/75
Slag caused injury
Despite what conclusions mightbe drawn from the title, it wasclaimed to be sustained whilewelding and when a sparkentered Pts ear. He complainedof pain and slightly muffled
hearing. The picture to the rightshows an eardrum one weekafter the injury. The eardrum isstill red and had a crust on it. Asmall metal ball is seen at thebottom of the canal.
-
7/29/2019 Common ENT Conditions PwPT2008
69/75
Haemotympanum
-
7/29/2019 Common ENT Conditions PwPT2008
70/75
Middle ear FB
The moulding materialentered middle ear whiletaking a cast for an elderlyladys hearing aid.
-
7/29/2019 Common ENT Conditions PwPT2008
71/75
Granulations
Granulations like this are
often associated with
underlying disease,
particularly if they arise in
the attic.
-
7/29/2019 Common ENT Conditions PwPT2008
72/75
AOM (Purulent)
-
7/29/2019 Common ENT Conditions PwPT2008
73/75
Question 7
A mother brings her 4 year old son to see you. He is complaining ofpain in his ear and his mother thinks that he pushed a button batteryinto it. You try to examine him but the child is horsing around . Whatshould you do?
a. Bribe the child with sweets/ Smack him when mums not lookingb. Tell the mother to come back in a few days time when the child is
calmer
b. Refer him for immediate removal of the suspected foreign body
c. Refer him to the ENT clinic routinely
d. Prescribe waxol drops(I seem to remember something along thoselines from the ENT job.)
-
7/29/2019 Common ENT Conditions PwPT2008
74/75
Answer 7
Correct Answer- Refer him urgently for FB removal.( Mum happy, thekids out of your surgery, good clinical practice and the ENT peopleyou dislike are stuck with him- a definite win win situation).
Usually inert non organic FBs can be extracted over a number of
days .Indications for referral are pain, infection, organic FB, youngchild, yourself not having the necessary equipment etc.
Button batteries are a definite no-no for drops, because the electriccurrent can catalyse chemical reactions and release alkalis causingnasty chemical burns; hence need to be extracted ASAP.
-
7/29/2019 Common ENT Conditions PwPT2008
75/75
The End (finally..)