Combined therapy of Sr-89 and zoledronic acid in patients with painful bone metastases Giovanni Storto a,b,d, ⁎ , Michele Klain b , Gaetano Paone b , Raffaele Liuzzi a , Leonardo Molino c , Alfredo Marinelli c , Andrea Soricelli e , Leonardo Pace b , Marco Salvatore b,d a Institute of Biostructures and Bioimages, National Council of Research, Naples, Italy b Department of Biomorphological and Functional Sciences, University Federico II of Naples, Italy c Department of Oncology, University Federico II of Naples, Italy d IRCCS, Neuromed, Pozzilli, Italy e Diagnostic Imaging, University of Naples Parthenope, Italy Received 17 June 2005; revised 22 October 2005; accepted 4 December 2005 Available online 24 January 2006 Abstract Purpose: We evaluated the pain response and daily discomfort in patients with painful bone metastases treated by merging 89 Sr-chloride and zoledronic acid. The results were compared with those of patients who received 89 Sr-chloride or zoledronic acid separately. Methods: 25 patients (12 women; mean age 65 ± 13 years) chronically treated with zoledronic acid underwent bone pain palliation with 150 MBq of 89 Sr-chloride at least 6 months later that bisphoshonate therapy started (group A). 13 patients (6 women; mean age 70 ± 12 years) received 89 Sr- chloride alone (group B) and 11 patients (5 women; mean age 69 ± 12 years) were chronically treated and continued to receive only zoledronic acid therapy (group C), both constituted the control groups. Patients kept a daily pain diary assessing both their discomfort and the pain of specific sites by using a visual analog scale (VAS), rating from 0 (no discomfort–no pain) to 10 (worst discomfort–pain). These diaries were reviewed weekly for 2 months and three different physicians rated the pain response on a scale of −2 (considerable deterioration) to +2 (considerable improvement). Results: Baseline characteristics were similar in the three groups. The reduction of total discomfort and of bone pain in the group A was significantly greater as compared to group B (P b 0.01) and group C (P b 0.01). During the monitored period, a significant improvement of clinical conditions was observed in the group A, varying the rate from −1 to 1 as compared to both groups B and C in which the rate changed from −1 to 0. Conclusion: Our findings indicate that combined therapy of 89 Sr-chloride and zoledronic acid in patients with painful bone metastases is more effective in treating pain and improving clinical conditions than 89 Sr-chloride or zoledronic acid used separately. © 2005 Elsevier Inc. All rights reserved. Keywords: Bone pain; Sr-89; Zoledronic acid; Combined therapy Introduction Most patients with advanced cancer are affected from bone metastasis [1–4]; this untreatable progression of the disease weights heavily on cancer-related mortality and morbidity. The exact molecular mechanisms of the metastatic process in cancer are widely argued. As a result, therapeutic strategies to prevent the evolution of the disease and its complications are being persistently investigated [5–7]. The pathophysiology of bone metastasis and its associated complications is composite [8–10]. Normal bone undergoes constant remodeling and systemic factors, such as the parathyroid hormone, local osteoclast- activating cytokines, and growth factors, play a role into the process [11]. When bone metastases take place, osteolytic activity increases. This leads to osteopenia and increased risk of developing fractures. The calcium released from the bone matrix in the course of this process can lead to a severe metabolic condition, the hypercalcemia of malignancy. Al- though bone metastases are often clinically quiet, both the above-mentioned conditions may sustain bone pain [12,13]. Moreover, bone pain may also represent a primitive, unrelated Bone 39 (2006) 35 – 41 www.elsevier.com/locate/bone ⁎ Corresponding author. Institute of Biostructures and Bioimages, National Council of Research, University Federico II, Via Pansini 5-80131 Napoli, Italy. Fax: +39 081 5457081. E-mail address: [email protected] (G. Storto). 8756-3282/$ - see front matter © 2005 Elsevier Inc. All rights reserved. doi:10.1016/j.bone.2005.12.004

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
) 35–41www.elsevier.com/locate/bone
Bone 39 (2006
Combined therapy of Sr-89 and zoledronic acid in patientswith painful bone metastases
Giovanni Storto a,b,d,⁎, Michele Klain b, Gaetano Paone b, Raffaele Liuzzi a, Leonardo Molino c,Alfredo Marinelli c, Andrea Soricelli e, Leonardo Pace b, Marco Salvatore b,d
a Institute of Biostructures and Bioimages, National Council of Research, Naples, Italyb Department of Biomorphological and Functional Sciences, University Federico II of Naples, Italy
c Department of Oncology, University Federico II of Naples, Italyd IRCCS, Neuromed, Pozzilli, Italy
e Diagnostic Imaging, University of Naples Parthenope, Italy
Received 17 June 2005; revised 22 October 2005; accepted 4 December 2005Available online 24 January 2006
Abstract
Purpose: We evaluated the pain response and daily discomfort in patients with painful bone metastases treated by merging 89Sr-chloride andzoledronic acid. The results were compared with those of patients who received 89Sr-chloride or zoledronic acid separately.Methods: 25 patients (12 women; mean age 65 ± 13 years) chronically treated with zoledronic acid underwent bone pain palliation with 150MBq of89Sr-chloride at least 6 months later that bisphoshonate therapy started (group A). 13 patients (6 women; mean age 70 ± 12 years) received 89Sr-chloride alone (group B) and 11 patients (5 women; mean age 69 ± 12 years) were chronically treated and continued to receive only zoledronic acidtherapy (group C), both constituted the control groups. Patients kept a daily pain diary assessing both their discomfort and the pain of specific sitesby using a visual analog scale (VAS), rating from 0 (no discomfort–no pain) to 10 (worst discomfort–pain). These diaries were reviewed weekly for2 months and three different physicians rated the pain response on a scale of −2 (considerable deterioration) to +2 (considerable improvement).Results: Baseline characteristics were similar in the three groups. The reduction of total discomfort and of bone pain in the group Awas significantlygreater as compared to group B (P b 0.01) and group C (P b 0.01). During the monitored period, a significant improvement of clinical conditionswas observed in the group A, varying the rate from −1 to 1 as compared to both groups B and C in which the rate changed from −1 to 0.Conclusion: Our findings indicate that combined therapy of 89Sr-chloride and zoledronic acid in patients with painful bone metastases is moreeffective in treating pain and improving clinical conditions than 89Sr-chloride or zoledronic acid used separately.© 2005 Elsevier Inc. All rights reserved.
Keywords: Bone pain; Sr-89; Zoledronic acid; Combined therapy
Introduction
Most patients with advanced cancer are affected from bonemetastasis [1–4]; this untreatable progression of the diseaseweights heavily on cancer-related mortality and morbidity. Theexact molecular mechanisms of the metastatic process in cancerare widely argued. As a result, therapeutic strategies to preventthe evolution of the disease and its complications are being
⁎ Corresponding author. Institute of Biostructures and Bioimages, NationalCouncil of Research, University Federico II, Via Pansini 5-80131 Napoli, Italy.Fax: +39 081 5457081.
E-mail address: [email protected] (G. Storto).
8756-3282/$ - see front matter © 2005 Elsevier Inc. All rights reserved.doi:10.1016/j.bone.2005.12.004
persistently investigated [5–7]. The pathophysiology of bonemetastasis and its associated complications is composite [8–10].Normal bone undergoes constant remodeling and systemicfactors, such as the parathyroid hormone, local osteoclast-activating cytokines, and growth factors, play a role into theprocess [11]. When bone metastases take place, osteolyticactivity increases. This leads to osteopenia and increased risk ofdeveloping fractures. The calcium released from the bonematrix in the course of this process can lead to a severemetabolic condition, the hypercalcemia of malignancy. Al-though bone metastases are often clinically quiet, both theabove-mentioned conditions may sustain bone pain [12,13].Moreover, bone pain may also represent a primitive, unrelated
36 G. Storto et al. / Bone 39 (2006) 35–41
symptom as a part of the metastatic disease, reducing theperformance status and decreasing the quality of life. Inaddition, bone pain is referred to as a particularly invalidatingcondition. Among the different, mostly palliative, therapiesused to treat bone metastases, bone-targeted approaches usingbisphosphonates, radiopharmaceuticals, or endothelin receptorantagonists currently hold great promise in terms of efficacy andtolerability. The possibility of using two or more approaches tometastatic bone pain has not been completely investigated sofar. Instead, it was speculated about the interference between thedifferent therapies [14–17]. This study investigated the effectsof a combined palliative therapy on the bone pain and theoverall performance status of patients affected by metastaticprostate or breast cancer using a bisphosphonate, the zoledronicacid, and the 89Sr-chloride.
Materials and methods
Patients
All patients had painful bone metastases from prostate or breast cancerrefractory to conventional treatment. They had definite diagnosis of metastaticbony lesions (blastic or mixed lytic/blastic) from primary cancer. Each wasrequested to have a 99mTc-MDP bone scan before receiving therapy. Pain atone or more sites presenting increased tracer uptake was required forparticipation in the study. They were required to have a performance status of40 or greater on the Karnofsky scale [18] and an estimated survival of at least6 months. Each patient repeated a 99mTc-MDP bone scan 2 months after the
Table 1Individual data from patients undergoing bone pain palliation
Combined therapy(zoledronic acid plus 89Sr)
89S
Patients 25 13Mean age ± SD (range) 65 ± 13 (46–84) 70
No. of pts. % No
SexMale 13 (52) 7Female 12 (48) 6
Performance status (Karnofsky)0–40 4 (16) 141–80 15 (60) 981–100 6 (24) 3
TumorBreast 12 (48) 6Prostate 13 (52) 7
Previous therapy b
None 7 (28) 3Chemo-hormonotherapy 16 (64) 10Radiotherapy 8 (32) 2
Sites Si
Bone involvement c (mean ± SD)Pre-therapy 6 ± 3.3 6Post-therapy 6 ± 3.1 6P d 1.0 1.0
Karnofsky index no less than 40.a Across categories.b Previous therapy at least 8 weeks before treatment started.c Number of involved body regions at bone scintigraphy.d Pre- vs. post-therapy.
radionuclide administration to compare the results with those previouslyobtained. Exclusion criteria were: leucocytes count below 2000/mm3, plateletscount below 150,000/mm3, and serum creatinine above 2.0 mg/dL. Patientswho received external radiation therapy, chemotherapy, or previous adminis-tration of radiopharmaceuticals within the past 8 weeks preceding thetreatment were excluded. The patients gave informed consent prior to undergothe treatment.
We enrolled a total of 49 consecutive patients. Twenty-five patients (12women; mean age 65 ± 13 years, 12 with previous breast cancer, and 13 withprostate cancer) chronically treated with zoledronic acid also underwent 89Sr-chloride single administration (group A). Thirteen more patients, sex-, age-, andtumor-matched (6 women; mean age 70 ± 12 years, 6 breast cancer and 7prostate cancer), who received only 89Sr-chloride (group B) as well as 11patients (5 women; mean age 69 ± 12 years, 5 breast cancer and 6 prostatecancer) who were chronically treated and continued to receive only zoledronicacid therapy (group C) constituted the control groups.
Treatment procedures
Group A patients were scheduled to receive zoledronic acid for at least 6months. It was administered intravenously (i.v.) every 3 weeks, at dose of 4 mgmixed in 100 mL of saline solution. The patients received a single dose of 150MBq of 89Sr-chloride at the end of the bisphosphonate treatment period.Radioactive treatment was administered in a room with appropriate protection.Each patient was given 250 mL of saline solution intravenously before theadministration of radioisotope and 250 mL in the subsequent 1/2 h period.Radioactive solution was administered using an i.v. catheter over 60 s thenslowly flushed with saline solution. Group B patients received only a sporadic,single dose of 89Sr-chloride. Group C patients received only zoledronic acidtherapy for 6 months and additionally through the following 2 months(assessment period).
r-chloride alone Zoledronic acid alone P a
11± 12 (38–82) 69 ± 12 (47–84)
. of pts. % No. of pts. %
(54) 6 (55)(46) 5 (45)
(8) 1 (10) 0.8(69) 8 (72) 0.6(23) 2 (18) 0.7
(46) 5 (45) 0.8(54) 6 (55) 0.6
(23) 2 (18) 0.9(76) 7 (64) 0.2(15) 2 (18) 0.5
tes Sites
± 3.2 6 ± 3.2 0.80± 3.2 6 ± 3.2 0.74
1.0
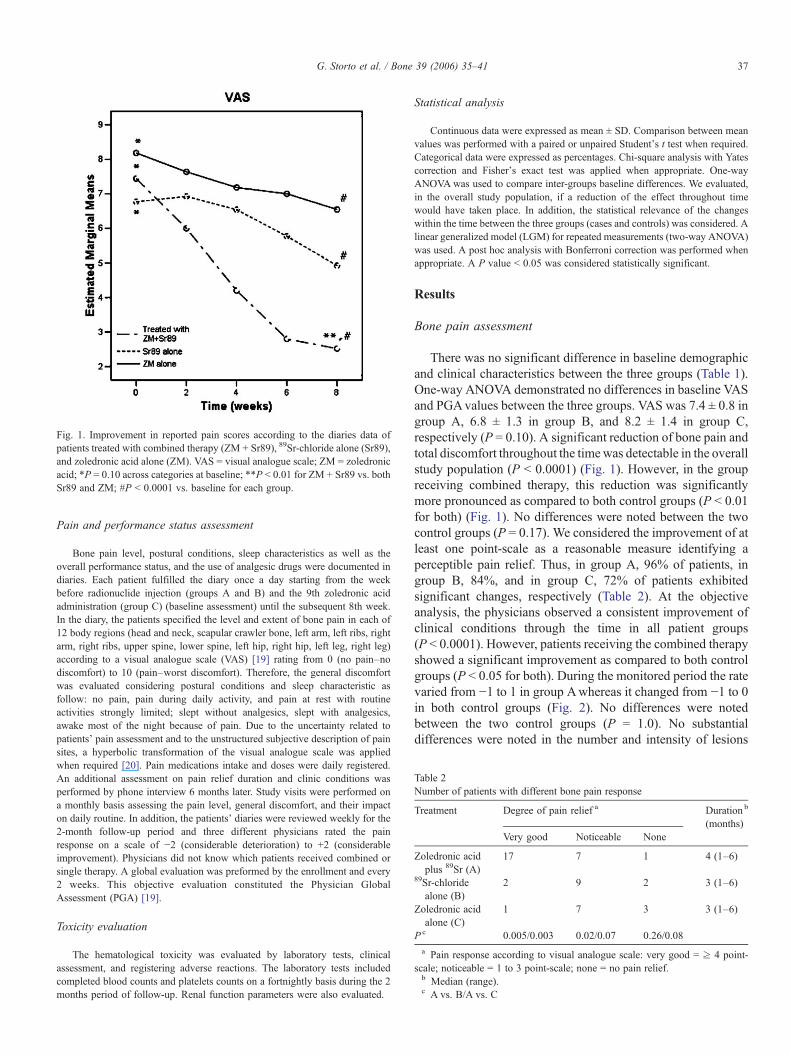
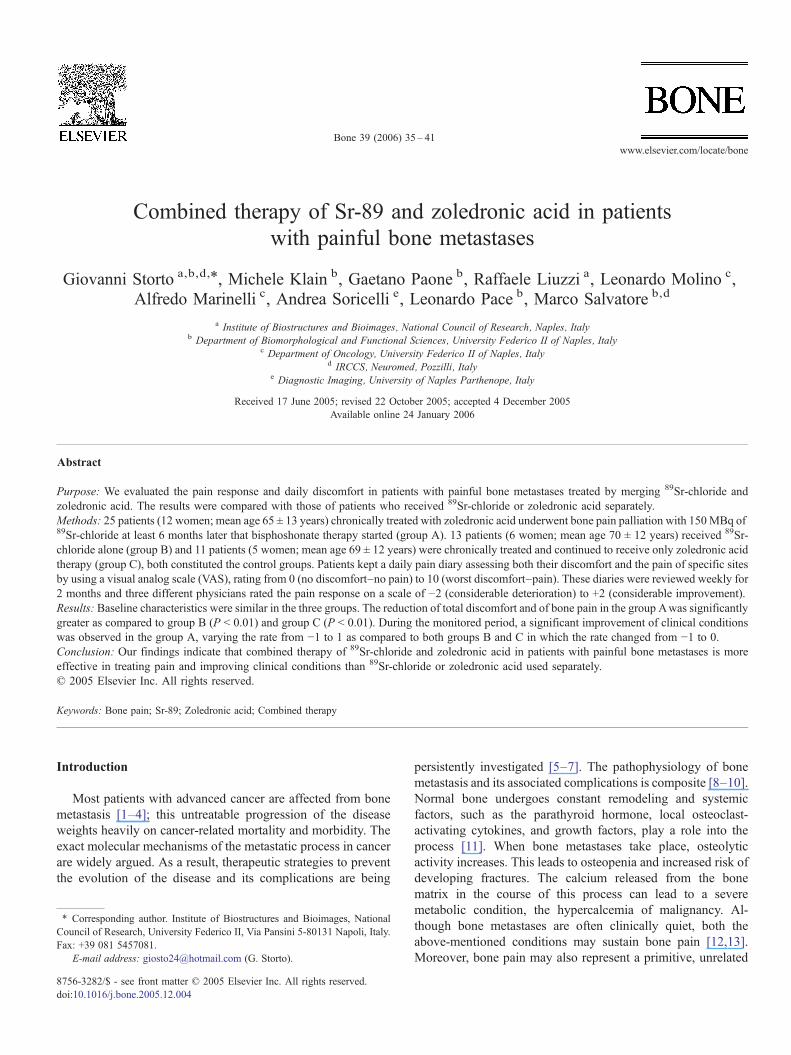
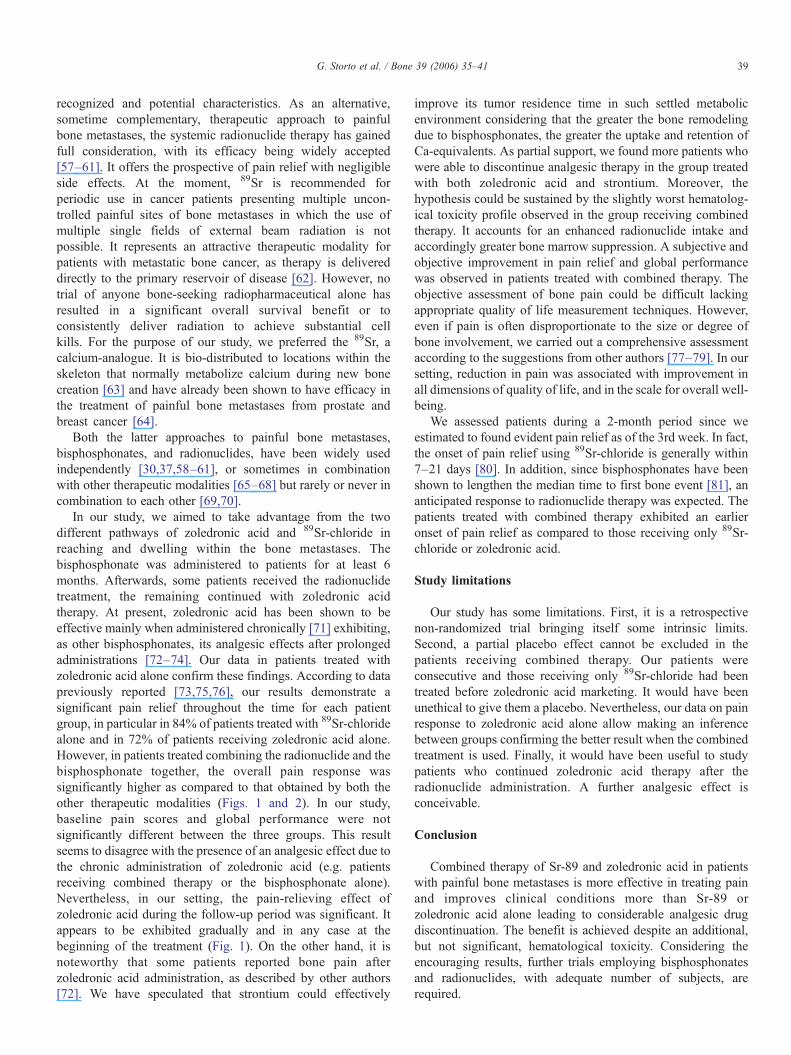
Fig. 1. Improvement in reported pain scores according to the diaries data ofpatients treated with combined therapy (ZM + Sr89), 89Sr-chloride alone (Sr89),and zoledronic acid alone (ZM). VAS = visual analogue scale; ZM = zoledronicacid; *P = 0.10 across categories at baseline; **P b 0.01 for ZM + Sr89 vs. bothSr89 and ZM; #P b 0.0001 vs. baseline for each group.
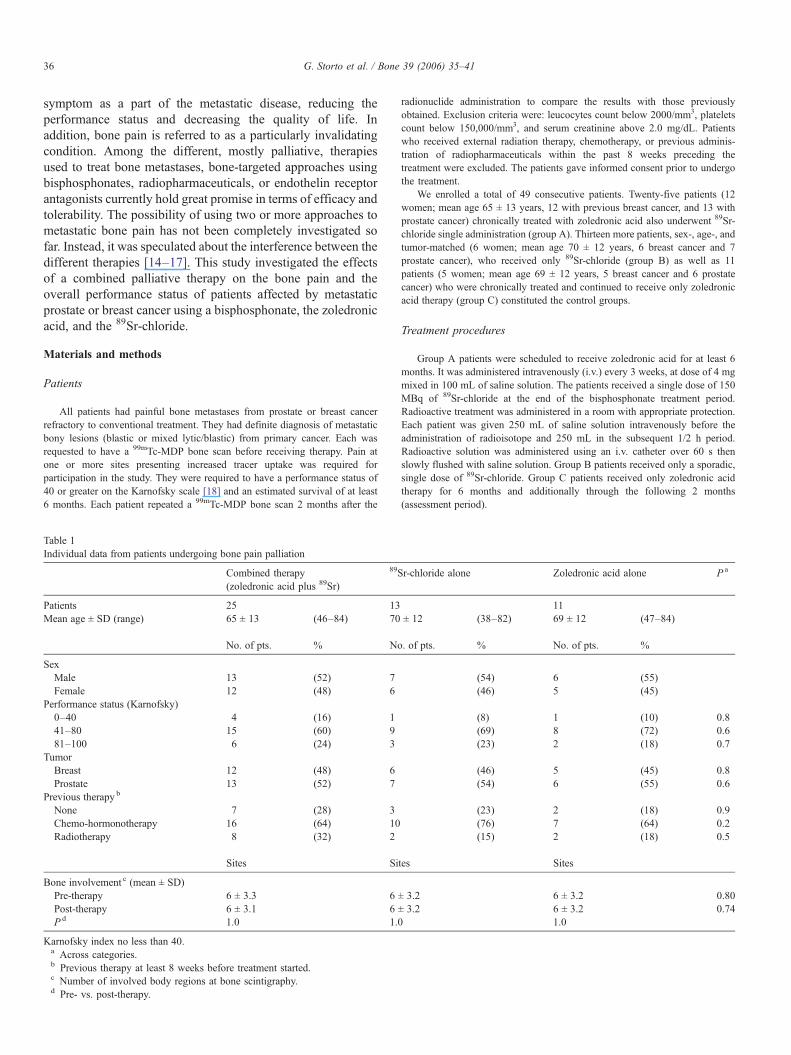
Table 2Number of patients with different bone pain response
Treatment Degree of pain relief a Duration b
(months)Very good Noticeable None
Zoledronic acidplus 89Sr (A)
17 7 1 4 (1–6)
89Sr-chloridealone (B)
2 9 2 3 (1–6)
Zoledronic acidalone (C)
1 7 3 3 (1–6)
P c 0.005/0.003 0.02/0.07 0.26/0.08
a Pain response according to visual analogue scale: very good = ≥ 4 point-scale; noticeable = 1 to 3 point-scale; none = no pain relief.b Median (range).c A vs. B/A vs. C
37G. Storto et al. / Bone 39 (2006) 35–41
Pain and performance status assessment
Bone pain level, postural conditions, sleep characteristics as well as theoverall performance status, and the use of analgesic drugs were documented indiaries. Each patient fulfilled the diary once a day starting from the weekbefore radionuclide injection (groups A and B) and the 9th zoledronic acidadministration (group C) (baseline assessment) until the subsequent 8th week.In the diary, the patients specified the level and extent of bone pain in each of12 body regions (head and neck, scapular crawler bone, left arm, left ribs, rightarm, right ribs, upper spine, lower spine, left hip, right hip, left leg, right leg)according to a visual analogue scale (VAS) [19] rating from 0 (no pain–nodiscomfort) to 10 (pain–worst discomfort). Therefore, the general discomfortwas evaluated considering postural conditions and sleep characteristic asfollow: no pain, pain during daily activity, and pain at rest with routineactivities strongly limited; slept without analgesics, slept with analgesics,awake most of the night because of pain. Due to the uncertainty related topatients' pain assessment and to the unstructured subjective description of painsites, a hyperbolic transformation of the visual analogue scale was appliedwhen required [20]. Pain medications intake and doses were daily registered.An additional assessment on pain relief duration and clinic conditions wasperformed by phone interview 6 months later. Study visits were performed ona monthly basis assessing the pain level, general discomfort, and their impacton daily routine. In addition, the patients' diaries were reviewed weekly for the2-month follow-up period and three different physicians rated the painresponse on a scale of −2 (considerable deterioration) to +2 (considerableimprovement). Physicians did not know which patients received combined orsingle therapy. A global evaluation was preformed by the enrollment and every2 weeks. This objective evaluation constituted the Physician GlobalAssessment (PGA) [19].
Toxicity evaluation
The hematological toxicity was evaluated by laboratory tests, clinicalassessment, and registering adverse reactions. The laboratory tests includedcompleted blood counts and platelets counts on a fortnightly basis during the 2months period of follow-up. Renal function parameters were also evaluated.
Statistical analysis
Continuous data were expressed as mean ± SD. Comparison between meanvalues was performed with a paired or unpaired Student's t test when required.Categorical data were expressed as percentages. Chi-square analysis with Yatescorrection and Fisher's exact test was applied when appropriate. One-wayANOVAwas used to compare inter-groups baseline differences. We evaluated,in the overall study population, if a reduction of the effect throughout timewould have taken place. In addition, the statistical relevance of the changeswithin the time between the three groups (cases and controls) was considered. Alinear generalized model (LGM) for repeated measurements (two-way ANOVA)was used. A post hoc analysis with Bonferroni correction was performed whenappropriate. A P value b 0.05 was considered statistically significant.
Results
Bone pain assessment
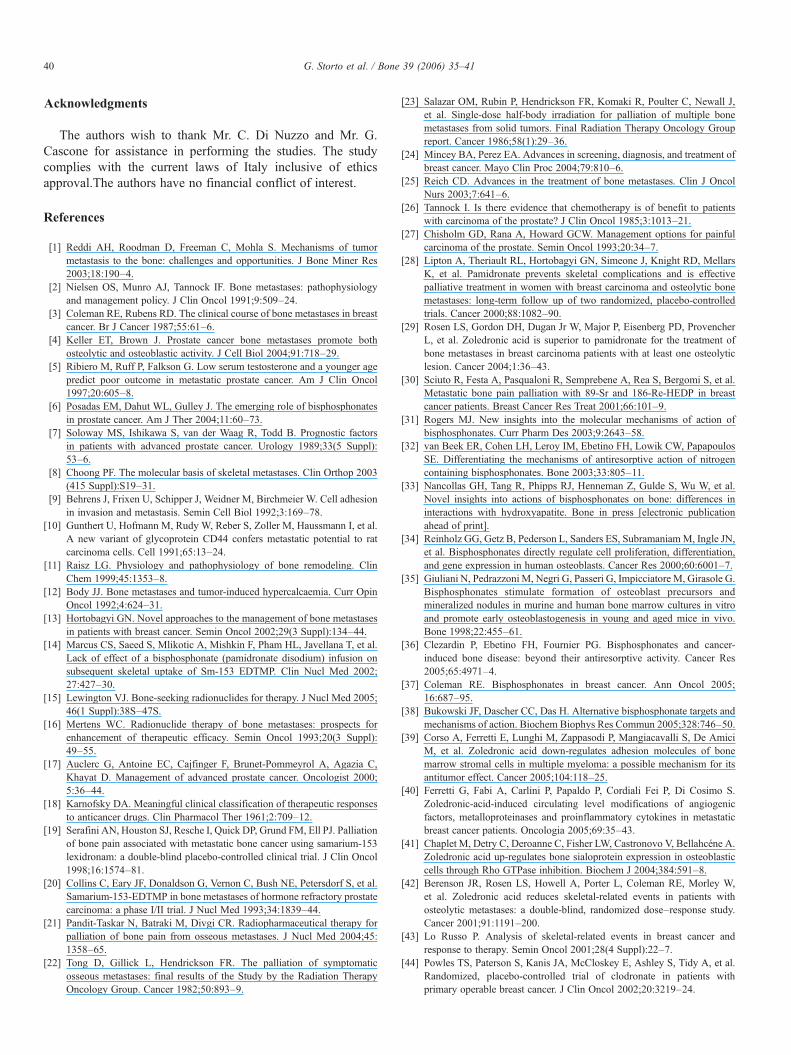
There was no significant difference in baseline demographicand clinical characteristics between the three groups (Table 1).One-way ANOVA demonstrated no differences in baseline VASand PGAvalues between the three groups. VAS was 7.4 ± 0.8 ingroup A, 6.8 ± 1.3 in group B, and 8.2 ± 1.4 in group C,respectively (P = 0.10). A significant reduction of bone pain andtotal discomfort throughout the timewas detectable in the overallstudy population (P b 0.0001) (Fig. 1). However, in the groupreceiving combined therapy, this reduction was significantlymore pronounced as compared to both control groups (P b 0.01for both) (Fig. 1). No differences were noted between the twocontrol groups (P = 0.17). We considered the improvement of atleast one point-scale as a reasonable measure identifying aperceptible pain relief. Thus, in group A, 96% of patients, ingroup B, 84%, and in group C, 72% of patients exhibitedsignificant changes, respectively (Table 2). At the objectiveanalysis, the physicians observed a consistent improvement ofclinical conditions through the time in all patient groups(P b 0.0001). However, patients receiving the combined therapyshowed a significant improvement as compared to both controlgroups (P b 0.05 for both). During the monitored period the ratevaried from −1 to 1 in group Awhereas it changed from −1 to 0in both control groups (Fig. 2). No differences were notedbetween the two control groups (P = 1.0). No substantialdifferences were noted in the number and intensity of lesions
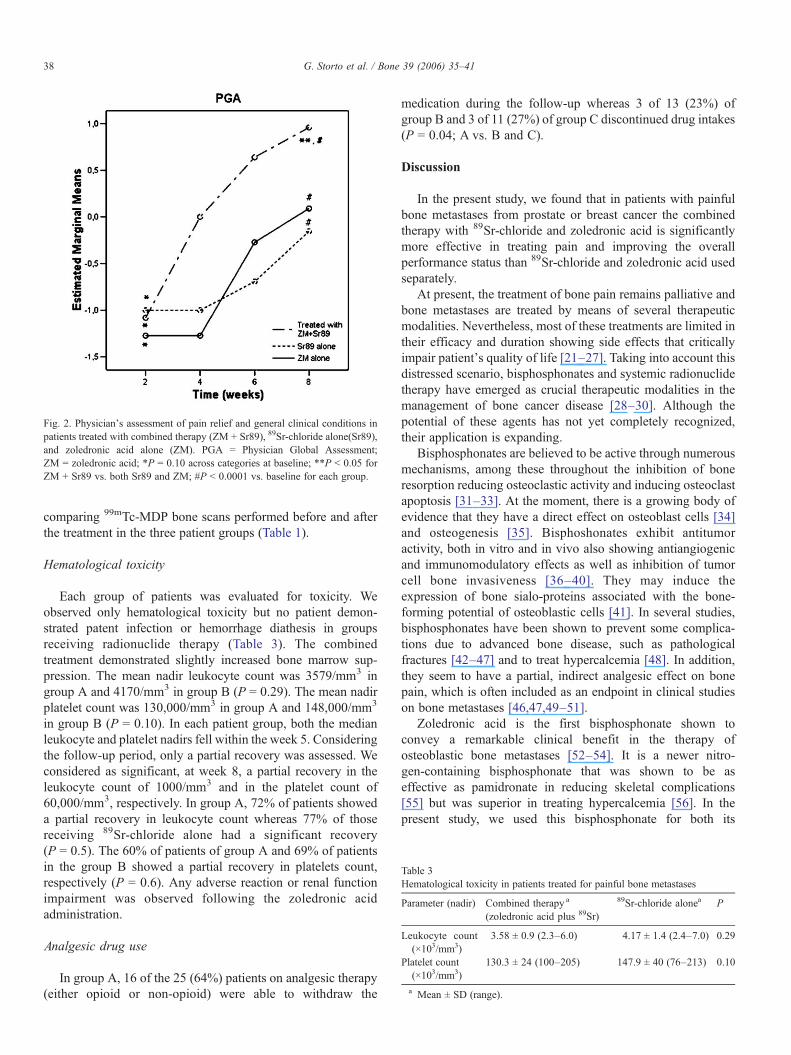
Fig. 2. Physician's assessment of pain relief and general clinical conditions inpatients treated with combined therapy (ZM + Sr89), 89Sr-chloride alone(Sr89),and zoledronic acid alone (ZM). PGA = Physician Global Assessment;ZM = zoledronic acid; *P = 0.10 across categories at baseline; **P b 0.05 forZM + Sr89 vs. both Sr89 and ZM; #P b 0.0001 vs. baseline for each group.
Table 3Hematological toxicity in patients treated for painful bone metastases
Parameter (nadir) Combined therapy a
(zoledronic acid plus 89Sr)
89Sr-chloride alonea P
Leukocyte count(×103/mm3)
3.58 ± 0.9 (2.3–6.0) 4.17 ± 1.4 (2.4–7.0) 0.29
Platelet count(×103/mm3)
130.3 ± 24 (100–205) 147.9 ± 40 (76–213) 0.10
a Mean ± SD (range).
38 G. Storto et al. / Bone 39 (2006) 35–41
comparing 99mTc-MDP bone scans performed before and afterthe treatment in the three patient groups (Table 1).
Hematological toxicity
Each group of patients was evaluated for toxicity. Weobserved only hematological toxicity but no patient demon-strated patent infection or hemorrhage diathesis in groupsreceiving radionuclide therapy (Table 3). The combinedtreatment demonstrated slightly increased bone marrow sup-pression. The mean nadir leukocyte count was 3579/mm3 ingroup A and 4170/mm3 in group B (P = 0.29). The mean nadirplatelet count was 130,000/mm3 in group A and 148,000/mm3
in group B (P = 0.10). In each patient group, both the medianleukocyte and platelet nadirs fell within the week 5. Consideringthe follow-up period, only a partial recovery was assessed. Weconsidered as significant, at week 8, a partial recovery in theleukocyte count of 1000/mm3 and in the platelet count of60,000/mm3, respectively. In group A, 72% of patients showeda partial recovery in leukocyte count whereas 77% of thosereceiving 89Sr-chloride alone had a significant recovery(P = 0.5). The 60% of patients of group A and 69% of patientsin the group B showed a partial recovery in platelets count,respectively (P = 0.6). Any adverse reaction or renal functionimpairment was observed following the zoledronic acidadministration.
Analgesic drug use
In group A, 16 of the 25 (64%) patients on analgesic therapy(either opioid or non-opioid) were able to withdraw the
medication during the follow-up whereas 3 of 13 (23%) ofgroup B and 3 of 11 (27%) of group C discontinued drug intakes(P = 0.04; A vs. B and C).
Discussion
In the present study, we found that in patients with painfulbone metastases from prostate or breast cancer the combinedtherapy with 89Sr-chloride and zoledronic acid is significantlymore effective in treating pain and improving the overallperformance status than 89Sr-chloride and zoledronic acid usedseparately.
At present, the treatment of bone pain remains palliative andbone metastases are treated by means of several therapeuticmodalities. Nevertheless, most of these treatments are limited intheir efficacy and duration showing side effects that criticallyimpair patient's quality of life [21–27]. Taking into account thisdistressed scenario, bisphosphonates and systemic radionuclidetherapy have emerged as crucial therapeutic modalities in themanagement of bone cancer disease [28–30]. Although thepotential of these agents has not yet completely recognized,their application is expanding.
Bisphosphonates are believed to be active through numerousmechanisms, among these throughout the inhibition of boneresorption reducing osteoclastic activity and inducing osteoclastapoptosis [31–33]. At the moment, there is a growing body ofevidence that they have a direct effect on osteoblast cells [34]and osteogenesis [35]. Bisphoshonates exhibit antitumoractivity, both in vitro and in vivo also showing antiangiogenicand immunomodulatory effects as well as inhibition of tumorcell bone invasiveness [36–40]. They may induce theexpression of bone sialo-proteins associated with the bone-forming potential of osteoblastic cells [41]. In several studies,bisphosphonates have been shown to prevent some complica-tions due to advanced bone disease, such as pathologicalfractures [42–47] and to treat hypercalcemia [48]. In addition,they seem to have a partial, indirect analgesic effect on bonepain, which is often included as an endpoint in clinical studieson bone metastases [46,47,49–51].
Zoledronic acid is the first bisphosphonate shown toconvey a remarkable clinical benefit in the therapy ofosteoblastic bone metastases [52–54]. It is a newer nitro-gen-containing bisphosphonate that was shown to be aseffective as pamidronate in reducing skeletal complications[55] but was superior in treating hypercalcemia [56]. In thepresent study, we used this bisphosphonate for both its
39G. Storto et al. / Bone 39 (2006) 35–41
recognized and potential characteristics. As an alternative,sometime complementary, therapeutic approach to painfulbone metastases, the systemic radionuclide therapy has gainedfull consideration, with its efficacy being widely accepted[57–61]. It offers the prospective of pain relief with negligibleside effects. At the moment, 89Sr is recommended forperiodic use in cancer patients presenting multiple uncon-trolled painful sites of bone metastases in which the use ofmultiple single fields of external beam radiation is notpossible. It represents an attractive therapeutic modality forpatients with metastatic bone cancer, as therapy is delivereddirectly to the primary reservoir of disease [62]. However, notrial of anyone bone-seeking radiopharmaceutical alone hasresulted in a significant overall survival benefit or toconsistently deliver radiation to achieve substantial cellkills. For the purpose of our study, we preferred the 89Sr, acalcium-analogue. It is bio-distributed to locations within theskeleton that normally metabolize calcium during new bonecreation [63] and have already been shown to have efficacy inthe treatment of painful bone metastases from prostate andbreast cancer [64].
Both the latter approaches to painful bone metastases,bisphosphonates, and radionuclides, have been widely usedindependently [30,37,58–61], or sometimes in combinationwith other therapeutic modalities [65–68] but rarely or never incombination to each other [69,70].
In our study, we aimed to take advantage from the twodifferent pathways of zoledronic acid and 89Sr-chloride inreaching and dwelling within the bone metastases. Thebisphosphonate was administered to patients for at least 6months. Afterwards, some patients received the radionuclidetreatment, the remaining continued with zoledronic acidtherapy. At present, zoledronic acid has been shown to beeffective mainly when administered chronically [71] exhibiting,as other bisphosphonates, its analgesic effects after prolongedadministrations [72–74]. Our data in patients treated withzoledronic acid alone confirm these findings. According to datapreviously reported [73,75,76], our results demonstrate asignificant pain relief throughout the time for each patientgroup, in particular in 84% of patients treated with 89Sr-chloridealone and in 72% of patients receiving zoledronic acid alone.However, in patients treated combining the radionuclide and thebisphosphonate together, the overall pain response wassignificantly higher as compared to that obtained by both theother therapeutic modalities (Figs. 1 and 2). In our study,baseline pain scores and global performance were notsignificantly different between the three groups. This resultseems to disagree with the presence of an analgesic effect due tothe chronic administration of zoledronic acid (e.g. patientsreceiving combined therapy or the bisphosphonate alone).Nevertheless, in our setting, the pain-relieving effect ofzoledronic acid during the follow-up period was significant. Itappears to be exhibited gradually and in any case at thebeginning of the treatment (Fig. 1). On the other hand, it isnoteworthy that some patients reported bone pain afterzoledronic acid administration, as described by other authors[72]. We have speculated that strontium could effectively
improve its tumor residence time in such settled metabolicenvironment considering that the greater the bone remodelingdue to bisphosphonates, the greater the uptake and retention ofCa-equivalents. As partial support, we found more patients whowere able to discontinue analgesic therapy in the group treatedwith both zoledronic acid and strontium. Moreover, thehypothesis could be sustained by the slightly worst hematolog-ical toxicity profile observed in the group receiving combinedtherapy. It accounts for an enhanced radionuclide intake andaccordingly greater bone marrow suppression. A subjective andobjective improvement in pain relief and global performancewas observed in patients treated with combined therapy. Theobjective assessment of bone pain could be difficult lackingappropriate quality of life measurement techniques. However,even if pain is often disproportionate to the size or degree ofbone involvement, we carried out a comprehensive assessmentaccording to the suggestions from other authors [77–79]. In oursetting, reduction in pain was associated with improvement inall dimensions of quality of life, and in the scale for overall well-being.
We assessed patients during a 2-month period since weestimated to found evident pain relief as of the 3rd week. In fact,the onset of pain relief using 89Sr-chloride is generally within7–21 days [80]. In addition, since bisphosphonates have beenshown to lengthen the median time to first bone event [81], ananticipated response to radionuclide therapy was expected. Thepatients treated with combined therapy exhibited an earlieronset of pain relief as compared to those receiving only 89Sr-chloride or zoledronic acid.
Study limitations
Our study has some limitations. First, it is a retrospectivenon-randomized trial bringing itself some intrinsic limits.Second, a partial placebo effect cannot be excluded in thepatients receiving combined therapy. Our patients wereconsecutive and those receiving only 89Sr-chloride had beentreated before zoledronic acid marketing. It would have beenunethical to give them a placebo. Nevertheless, our data on painresponse to zoledronic acid alone allow making an inferencebetween groups confirming the better result when the combinedtreatment is used. Finally, it would have been useful to studypatients who continued zoledronic acid therapy after theradionuclide administration. A further analgesic effect isconceivable.
Conclusion
Combined therapy of Sr-89 and zoledronic acid in patientswith painful bone metastases is more effective in treating painand improves clinical conditions more than Sr-89 orzoledronic acid alone leading to considerable analgesic drugdiscontinuation. The benefit is achieved despite an additional,but not significant, hematological toxicity. Considering theencouraging results, further trials employing bisphosphonatesand radionuclides, with adequate number of subjects, arerequired.
40 G. Storto et al. / Bone 39 (2006) 35–41
Acknowledgments
The authors wish to thank Mr. C. Di Nuzzo and Mr. G.Cascone for assistance in performing the studies. The studycomplies with the current laws of Italy inclusive of ethicsapproval.The authors have no financial conflict of interest.
References
[1] Reddi AH, Roodman D, Freeman C, Mohla S. Mechanisms of tumormetastasis to the bone: challenges and opportunities. J Bone Miner Res2003;18:190–4.
[2] Nielsen OS, Munro AJ, Tannock IF. Bone metastases: pathophysiologyand management policy. J Clin Oncol 1991;9:509–24.
[3] Coleman RE, Rubens RD. The clinical course of bone metastases in breastcancer. Br J Cancer 1987;55:61–6.
[4] Keller ET, Brown J. Prostate cancer bone metastases promote bothosteolytic and osteoblastic activity. J Cell Biol 2004;91:718–29.
[5] Ribiero M, Ruff P, Falkson G. Low serum testosterone and a younger agepredict poor outcome in metastatic prostate cancer. Am J Clin Oncol1997;20:605–8.
[6] Posadas EM, Dahut WL, Gulley J. The emerging role of bisphosphonatesin prostate cancer. Am J Ther 2004;11:60–73.
[7] Soloway MS, Ishikawa S, van der Waag R, Todd B. Prognostic factorsin patients with advanced prostate cancer. Urology 1989;33(5 Suppl):53–6.
[8] Choong PF. The molecular basis of skeletal metastases. Clin Orthop 2003(415 Suppl):S19–31.
[9] Behrens J, Frixen U, Schipper J, Weidner M, Birchmeier W. Cell adhesionin invasion and metastasis. Semin Cell Biol 1992;3:169–78.
[10] Gunthert U, Hofmann M, Rudy W, Reber S, Zoller M, Haussmann I, et al.A new variant of glycoprotein CD44 confers metastatic potential to ratcarcinoma cells. Cell 1991;65:13–24.
[11] Raisz LG. Physiology and pathophysiology of bone remodeling. ClinChem 1999;45:1353–8.
[12] Body JJ. Bone metastases and tumor-induced hypercalcaemia. Curr OpinOncol 1992;4:624–31.
[13] Hortobagyi GN. Novel approaches to the management of bone metastasesin patients with breast cancer. Semin Oncol 2002;29(3 Suppl):134–44.
[14] Marcus CS, Saeed S, Mlikotic A, Mishkin F, Pham HL, Javellana T, et al.Lack of effect of a bisphosphonate (pamidronate disodium) infusion onsubsequent skeletal uptake of Sm-153 EDTMP. Clin Nucl Med 2002;27:427–30.
[15] Lewington VJ. Bone-seeking radionuclides for therapy. J Nucl Med 2005;46(1 Suppl):38S–47S.
[16] Mertens WC. Radionuclide therapy of bone metastases: prospects forenhancement of therapeutic efficacy. Semin Oncol 1993;20(3 Suppl):49–55.
[17] Auclerc G, Antoine EC, Cajfinger F, Brunet-Pommeyrol A, Agazia C,Khayat D. Management of advanced prostate cancer. Oncologist 2000;5:36–44.
[18] Karnofsky DA. Meaningful clinical classification of therapeutic responsesto anticancer drugs. Clin Pharmacol Ther 1961;2:709–12.
[19] Serafini AN, Houston SJ, Resche I, Quick DP, Grund FM, Ell PJ. Palliationof bone pain associated with metastatic bone cancer using samarium-153lexidronam: a double-blind placebo-controlled clinical trial. J Clin Oncol1998;16:1574–81.
[20] Collins C, Eary JF, Donaldson G, Vernon C, Bush NE, Petersdorf S, et al.Samarium-153-EDTMP in bone metastases of hormone refractory prostatecarcinoma: a phase I/II trial. J Nucl Med 1993;34:1839–44.
[21] Pandit-Taskar N, Batraki M, Divgi CR. Radiopharmaceutical therapy forpalliation of bone pain from osseous metastases. J Nucl Med 2004;45:1358–65.
[22] Tong D, Gillick L, Hendrickson FR. The palliation of symptomaticosseous metastases: final results of the Study by the Radiation TherapyOncology Group. Cancer 1982;50:893–9.
[23] Salazar OM, Rubin P, Hendrickson FR, Komaki R, Poulter C, Newall J,et al. Single-dose half-body irradiation for palliation of multiple bonemetastases from solid tumors. Final Radiation Therapy Oncology Groupreport. Cancer 1986;58(1):29–36.
[24] Mincey BA, Perez EA. Advances in screening, diagnosis, and treatment ofbreast cancer. Mayo Clin Proc 2004;79:810–6.
[25] Reich CD. Advances in the treatment of bone metastases. Clin J OncolNurs 2003;7:641–6.
[26] Tannock I. Is there evidence that chemotherapy is of benefit to patientswith carcinoma of the prostate? J Clin Oncol 1985;3:1013–21.
[27] Chisholm GD, Rana A, Howard GCW. Management options for painfulcarcinoma of the prostate. Semin Oncol 1993;20:34–7.
[28] Lipton A, Theriault RL, Hortobagyi GN, Simeone J, Knight RD, MellarsK, et al. Pamidronate prevents skeletal complications and is effectivepalliative treatment in women with breast carcinoma and osteolytic bonemetastases: long-term follow up of two randomized, placebo-controlledtrials. Cancer 2000;88:1082–90.
[29] Rosen LS, Gordon DH, Dugan Jr W, Major P, Eisenberg PD, ProvencherL, et al. Zoledronic acid is superior to pamidronate for the treatment ofbone metastases in breast carcinoma patients with at least one osteolyticlesion. Cancer 2004;1:36–43.
[30] Sciuto R, Festa A, Pasqualoni R, Semprebene A, Rea S, Bergomi S, et al.Metastatic bone pain palliation with 89-Sr and 186-Re-HEDP in breastcancer patients. Breast Cancer Res Treat 2001;66:101–9.
[31] Rogers MJ. New insights into the molecular mechanisms of action ofbisphosphonates. Curr Pharm Des 2003;9:2643–58.
[32] van Beek ER, Cohen LH, Leroy IM, Ebetino FH, Lowik CW, PapapoulosSE. Differentiating the mechanisms of antiresorptive action of nitrogencontaining bisphosphonates. Bone 2003;33:805–11.
[33] Nancollas GH, Tang R, Phipps RJ, Henneman Z, Gulde S, Wu W, et al.Novel insights into actions of bisphosphonates on bone: differences ininteractions with hydroxyapatite. Bone in press [electronic publicationahead of print].
[34] Reinholz GG, Getz B, Pederson L, Sanders ES, SubramaniamM, Ingle JN,et al. Bisphosphonates directly regulate cell proliferation, differentiation,and gene expression in human osteoblasts. Cancer Res 2000;60:6001–7.
[35] Giuliani N, Pedrazzoni M, Negri G, Passeri G, Impicciatore M, Girasole G.Bisphosphonates stimulate formation of osteoblast precursors andmineralized nodules in murine and human bone marrow cultures in vitroand promote early osteoblastogenesis in young and aged mice in vivo.Bone 1998;22:455–61.
[36] Clezardin P, Ebetino FH, Fournier PG. Bisphosphonates and cancer-induced bone disease: beyond their antiresorptive activity. Cancer Res2005;65:4971–4.
[37] Coleman RE. Bisphosphonates in breast cancer. Ann Oncol 2005;16:687–95.
[38] Bukowski JF, Dascher CC, Das H. Alternative bisphosphonate targets andmechanisms of action. Biochem Biophys Res Commun 2005;328:746–50.
[39] Corso A, Ferretti E, Lunghi M, Zappasodi P, Mangiacavalli S, De AmiciM, et al. Zoledronic acid down-regulates adhesion molecules of bonemarrow stromal cells in multiple myeloma: a possible mechanism for itsantitumor effect. Cancer 2005;104:118–25.
[40] Ferretti G, Fabi A, Carlini P, Papaldo P, Cordiali Fei P, Di Cosimo S.Zoledronic-acid-induced circulating level modifications of angiogenicfactors, metalloproteinases and proinflammatory cytokines in metastaticbreast cancer patients. Oncologia 2005;69:35–43.
[41] Chaplet M, Detry C, Deroanne C, Fisher LW, Castronovo V, Bellahcéne A.Zoledronic acid up-regulates bone sialoprotein expression in osteoblasticcells through Rho GTPase inhibition. Biochem J 2004;384:591–8.
[42] Berenson JR, Rosen LS, Howell A, Porter L, Coleman RE, Morley W,et al. Zoledronic acid reduces skeletal-related events in patients withosteolytic metastases: a double-blind, randomized dose–response study.Cancer 2001;91:1191–200.
[43] Lo Russo P. Analysis of skeletal-related events in breast cancer andresponse to therapy. Semin Oncol 2001;28(4 Suppl):22–7.
[44] Powles TS, Paterson S, Kanis JA, McCloskey E, Ashley S, Tidy A, et al.Randomized, placebo-controlled trial of clodronate in patients withprimary operable breast cancer. J Clin Oncol 2002;20:3219–24.
41G. Storto et al. / Bone 39 (2006) 35–41
[45] Theriault RL, Lipton A, Hortobagyi GN, Leff R, Gluck S, Stewart JF, et al.Pamidronate reduces skeletal morbidity in women with advanced breastcancer and lytic bone lesions: a randomized, placebo controlled trial. J ClinOncol 1999;17:846–54.
[46] Wang RF, Zhang CL, Zhu SL, Zhu M. A comparative study of samarium-153-ethylenediaminetetramethylene phosphonic acid with pamidronatedisodium in the treatment of patients with painful metastatic bone cancer.Med Princ Pract 2003;12:97–101.
[47] Hortobagyi GN, Theriault RL, Porter L, Blayney D, Lipton A, Sinoff C,et al. Efficacy of pamidronate in reducing skeletal complications in patientswith breast cancer and lytic bone metastases. N Eng J Med 1996;335:1785–91.
[48] Wellington K, Goa KL. Zoledronic acid: a review of its use in themanagement of bone metastases and hypercalcaemia of malignancy. Drugs2003;63:417–37.
[49] Carey PO, Lippert MC. Treatment of painful prostatic bone metastaseswith oral etidronate disodium. Urology 1988;32:403–7.
[50] Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L,et al. A randomized, placebo-controlled trial of zoledronic acid in patientswith hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst2002;94:1458–68.
[51] Coleman RE. Bisphosphonates: clinical experience. Oncologist 2004;9(4 Suppl):14–27.
[52] Vogel CL, Yanagihara RH, Wood AJ, Schnell FM, Henderson C, KaplanBH, et al. Safety and pain palliation of zoledronic acid in patients withbreast cancer, prostate cancer, or multiple myeloma who previouslyreceived bisphosphonate therapy. Oncologist 2004;9:687–95.
[53] Saad F. Zoledronic acid significantly reduces pathologic fractures inpatients with advanced-stage prostate cancer metastatic to bone. ClinProstate Cancer 2002;1:145–52.
[54] Li EC, Davis LE. Zoledronic acid: a new parenteral bisphosphonate. ClinTher 2003;25:2669–708.
[55] Rosen LS, Gordon D, Antonio BS, Howell A, Belch A, Mackey J, et al.Zoledronic acid versus pamidronate in the treatment of skeletalmetastases in patients with breast cancer or osteolytic lesions of multiplemyeloma: a phase III, double-blind, comparative trial. J Cancer 2001;7:377–87.
[56] Major P, Lortholary A, Hon J, Abdi E, Mills G, Menssen HD, et al.Zoledronic acid is superior to pamidronate in the treatment ofhypercalcemia of malignancy: a pooled analysis of two randomized,controlled clinical trials. J Clin Oncol 2001;19:558–67.
[57] Serafini AN. Therapy of metastatic bone pain. J Nucl Med 2001;42:895–906.
[58] Altman GB, Lee CA. Strontium-89 for treatment of painful bonemetastases from prostate cancer. Oncol Nurs Forum 1996;23:523–7.
[59] Uchiyama M, Narita H, Makino M, Sekine H, Mori Y, Fukumitsu N, et al.Strontium-89 therapy and imaging with bremsstrahlung in bonemetastases. Clin Nucl Med 1997;22:605–9.
[60] Baziotis N, Yakoumakis E, Zissimopoulos A, Gerinicola-Tripali X,Malamitsi J, Proukakis CH. Strontium-89 in the treatment of bonemetastases from breast cancer. Oncology 1998;55:377–81.
[61] Pons F, Herranz R, Garcia A, Vidal-Sicart S, Conill C, Grau JJ, et al.Strontium-89 for palliation of pain from bone metastases in patients withprostate and breast cancer. Eur J Nucl Med 1997;24:1210–4.
[62] Morris MJ, Scher HI. Clinical approaches to osseous metastases in prostatecancer. The Oncologist 2003;2:161–73.
[63] Blake GM, Zivanovic MA, McEwan AJ, Ackery DM. Sr-89 therapy:strontium kinetics in disseminated carcinoma of the prostate. Eur J NuclMed 1986;12:447–54.
[64] Nightengale B, Brune M, Blizzard SP, Ashley-Johnson M, Slan S.Strontium chloride Sr-89 for treating pain from metastatic bone disease.Am J Health-Syst Pharm 1995;52:2189–95.
[65] Porter AT, McEwan AJB, Powe JE, Reid R, McGowan DG, Lukka H, et al.Results of a randomized phase III trial to evaluate the efficacy of strontium-89 adjuvant to local field external-beam irradiation in the management ofendocrine-resistant metastatic prostate cancer. Int J Radiat Oncol, Biol,Phys 1993;25:805–13.
[66] Quilty PM, Kirk D, Bolger JJ, Dearnaley DP, Lewington VJ, Mason MD,et al. A comparison of the palliative effects of strontium-89 and externalbeam radiotherapy in metastatic prostate cancer. Radiother Oncol 1994;31:33–40.
[67] Sciuto R, Maini CL, Tofani A, Fiumara C, Scelsa MG, Broccatelli M.Radiosensitization with low-dose carboplatin enhances pain palliation inradioisotope therapy with strontium-89. Nucl Med Commun 1996;17:799–804.
[68] Tu S, Millikan RE, Mengistu B, Delpassand ES, Amato RJ, Pagliaro LC,et al. Bone-targeted therapy for advanced androgen-independentcarcinoma of the prostate: a randomised phase II trial. Lancet 2001;357:336–41.
[69] Hamdy NA, Papapoulos SE. The palliative management of skeletalmetastases in prostate cancer: use of bone-seeking radionuclides andbisphosphonates. Semin Nucl Med 2001;31:62–8.
[70] Soerdjbalie-Maikoe V, Pelger RC, Lycklama a Nijeholt GA, Arndt JW,Zwinderman AH, Papapoulos SE, et al. Strontium-89 (Metastron) and thebisphosphonate olpadronate reduce the incidence of spinal cord compres-sion in patients with hormone-refractory prostate cancer metastatic to theskeleton. Eur J Nucl Med Mol Imaging 2002;29:494–8.
[71] Perry CM, Figgitt DP. Zoledronic acid: a review of its use in patients withadvanced cancer. Drugs 2004;64:1197–211.
[72] Rosen LS, Gordon D, Tchekmedyian NS, Yanagihara R, Hirsh V,Krzakowski M, et al. Long-term efficacy and safety of zoledronic acidin the treatment of skeletal metastases in patients with nonsmall cell lungcarcinoma and other solid tumors: a randomized, Phase III, double-blind,placebo-controlled trial. Cancer 2004;100:2613–21.
[73] Body JJ. Clinical research update: zoledronate. Cancer 1997;80(8 Suppl):1699–701.
[74] Bonabello A, Galmozzi MR, Canaparo R, Serpe L, Zara GP. Long-termanalgesic effect of clodronate in rodents. Bone 2003;33:567–74.
[75] Robinson RG, Preston DF, Schiefelbein M, Baxter KG. Strontium 89therapy for the palliation of pain due to osseous metastases. JAMA1995;274:420–4.
[76] Lewington VJ, McEwan AJ, Ackery DM, Bayly RJ, Keeling DH,Macleod PM, et al. A prospective, randomised double-blind crossoverstudy to examine the efficacy of strontium-89 in pain palliation inpatients with advanced prostate cancer metastatic to bone. Eur J Cancer1991;27:954–8.
[77] Ware Jr JE, Sherbourne CD. The MOS 36-item short-form health survey(SF-36): I. Conceptual framework and item selection. Care 1992;30:473–83.
[78] Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, et al. Thefunctional assessment of cancer therapy scale: development and validationof the general measure. J Clin Oncol 1993;11:570–9.
[79] Hwang SS, Chang VT, Kasimis B. Dynamic cancer pain managementoutcomes: the relationship between pain severity, pain relief, functionalinterference, satisfaction and global quality of life over time. J PainSymptom Manage 2002;23:190–200.
[80] Mertens WC, Stitt L, Porter AT. Strontium-89 therapy and relief of pain inpatients with prostate carcinoma metastatic to bone: a dose responserelationship? Am J Clin Oncol 1993;16:238–42.
[81] Conte PF, Latreille J, Mauriac L, Calabresi F, Santos R, Campos D, et al.Delay in progression of bone metastases in breast cancer patients treatedwith intravenous pamidronate: results from a multinational randomizedcontrolled trial. The Aredia Multinational Cooperative Group. J Clin Oncol1996;14:2552–9.
Related Documents











