The Power of Data: Achieving Consistent Patient Outcomes Combined Sections Meeting 2015 February 4‐7, 2015 Indianapolis, IN www.aptahpa.org HPA The Catalyst is the Section on Health Policy & Administration of the American Physical Therapy Association Speaker(s): Dianne Jewell, PT, DPT, PhD Heather Smith, PT, MPH Mary Stilphen, DPT Session Type: Educational Sessions Session Level: Intermediate This information is the property of the author(s) and should not be copied or otherwise used without the express written permission of the author(s). Page 1 of 19 total pages

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Power of Data: Achieving Consistent Patient Outcomes
CombinedSectionsMeeting2015
February 4‐7, 2015
Indianapolis, IN
www.aptahpa.org HPA The Catalyst is the Section on Health Policy & Administration
of the American Physical Therapy Association
Speaker(s): Dianne Jewell, PT, DPT, PhD
Heather Smith, PT, MPH
Mary Stilphen, DPT
Session Type: Educational Sessions
Session Level: Intermediate
This information is the property of the author(s) and should not be copied or otherwise used without the
express written permission of the author(s).
Page 1 of 19 total pages

2/10/2015
1
The Power of Data: Achieving Consistent Patient Outcomes
Mary Stilphen PT, DPTCleveland Clinic Rehabilitation and Sports Therapy
Dianne V. Jewell, PT, DPT, PhDThe Rehab Intel Network
Heather Smith, PT, MPH APTA
Session Learning Objectives
After this session, you will be able to:
• Lay the groundwork for standardized outcomes data collection
• Implement a standardized outcomes tool in a consistent and accurate manner
• Analyze and share the information you collect to improve performance at the patient, clinician and/or organizational level
ACOs, Medical Homes
PTA differential payment
Pay for performance
Functional reporting
Therapy cap, MPPR
2/10/2015
2
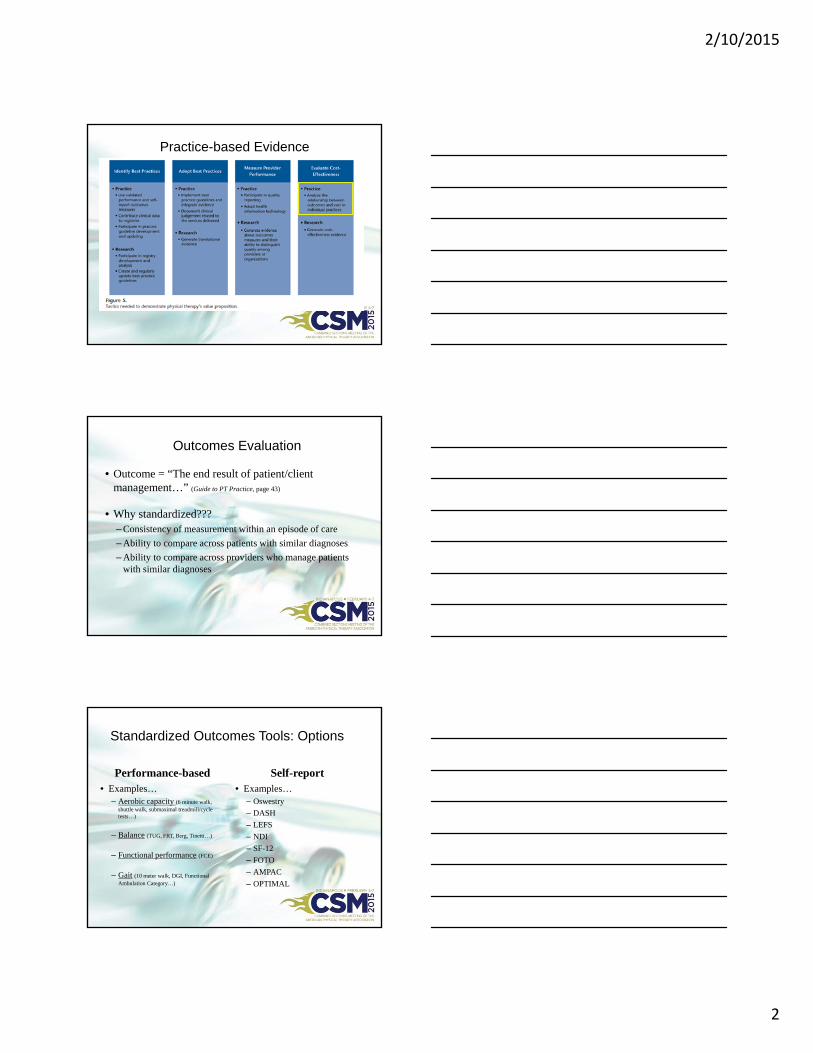
Practice-based Evidence
Outcomes Evaluation
• Outcome = “The end result of patient/client management…” (Guide to PT Practice, page 43)
• Why standardized???– Consistency of measurement within an episode of care
– Ability to compare across patients with similar diagnoses
– Ability to compare across providers who manage patients with similar diagnoses
Standardized Outcomes Tools: Options
Performance-based• Examples…
– Aerobic capacity (6 minute walk, shuttle walk, submaximal treadmill/cycle tests…)
– Balance (TUG, FRT, Berg, Tinetti…)
– Functional performance (FCE)
– Gait (10 meter walk, DGI, Functional Ambulation Category…)
Self-report• Examples…
– Oswestry
– DASH
– LEFS
– NDI
– SF-12
– FOTO
– AMPAC
– OPTIMAL

2/10/2015
3
What you need to know…
• Is the tool reliable?– Inter-tester, intra-tester, test-retest, parallel forms, split-half,
internal consistency
• Is the tool valid?– Face, content, construct (convergent/discriminant), criterion
(concurrent/predictive)
• Is the tool sensitive to change?
• Has meaningful change been determined?
The Power of Information on a Large Scale
• Internal uses–Performance improvement
–Guideline refinement
–Quality reporting
–Staff development
• External uses–Referral sources
–Payers
–Consumers
THE CLEVELAND CLINIC STORY
2/10/2015
4
• 10 Hospital nonprofit health care system (9 Ohio, 1 Florida)
*
• Unified Brand• Unified Organizational and Leadership Structure • Standard Operational and Clinical Procedures• Increased Productivity, Efficiency, and Cost Structure• Positioning for Growth
Cleveland Clinic Rehabilitation & Sports Therapy
Care Pathways
Consistency of Service
Centralized Recruiting
Outcomes Measurement
“Each time you learn something new you have to adjust the whole framework of
your knowledge”
Eleanor Roosevelt
2/10/2015
5
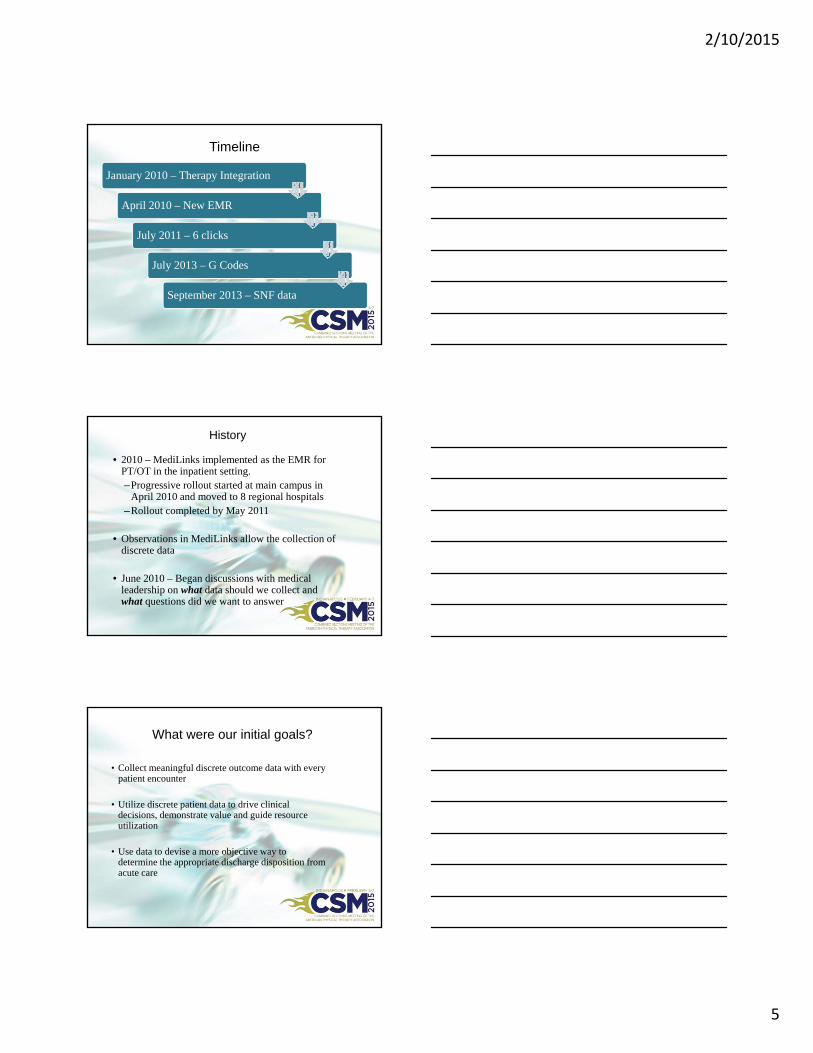
Timeline
January 2010 – Therapy Integration
April 2010 – New EMR
July 2011 – 6 clicks
July 2013 – G Codes
September 2013 – SNF data
History
• 2010 – MediLinks implemented as the EMR for PT/OT in the inpatient setting.–Progressive rollout started at main campus in
April 2010 and moved to 8 regional hospitals–Rollout completed by May 2011
• Observations in MediLinks allow the collection of discrete data
• June 2010 – Began discussions with medical leadership on what data should we collect and what questions did we want to answer
What were our initial goals?
• Collect meaningful discrete outcome data with every patient encounter
• Utilize discrete patient data to drive clinical decisions, demonstrate value and guide resource utilization
• Use data to devise a more objective way to determine the appropriate discharge disposition from acute care
2/10/2015
6
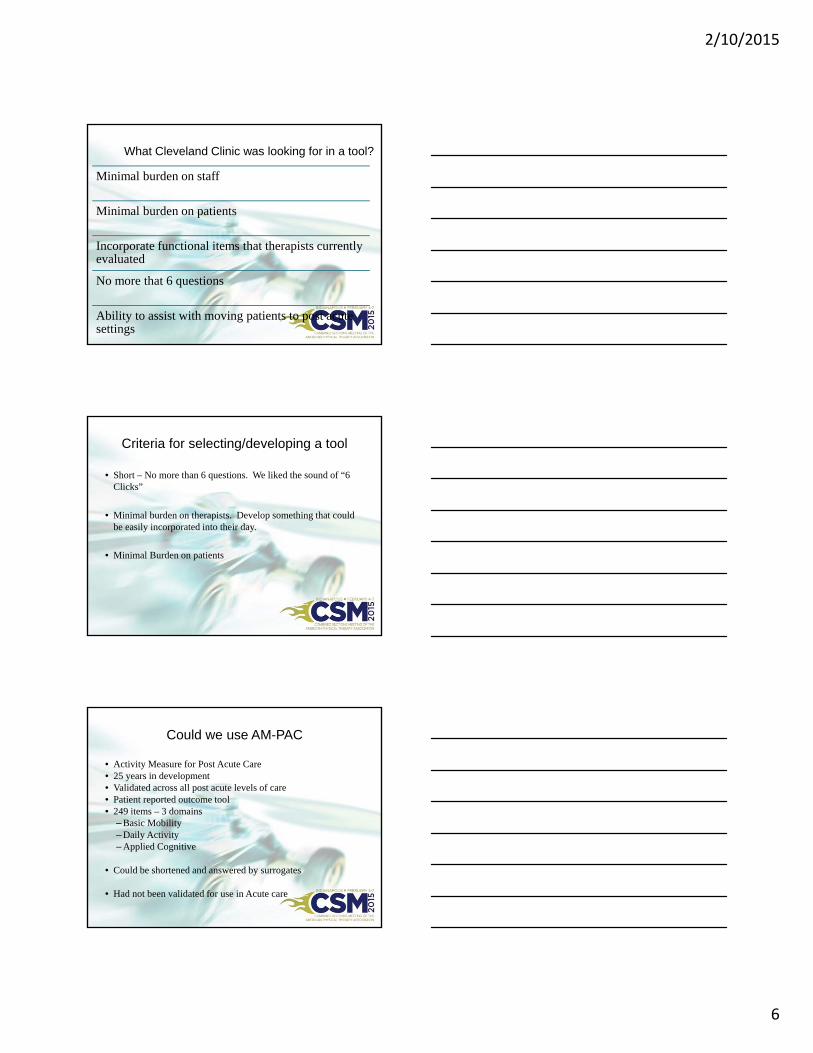
What Cleveland Clinic was looking for in a tool?
Minimal burden on staff
Minimal burden on patients
Incorporate functional items that therapists currently evaluated
No more that 6 questions
Ability to assist with moving patients to post acute settings
Criteria for selecting/developing a tool
• Short – No more than 6 questions. We liked the sound of “6 Clicks”
• Minimal burden on therapists. Develop something that could be easily incorporated into their day.
• Minimal Burden on patients
Could we use AM-PAC
• Activity Measure for Post Acute Care• 25 years in development• Validated across all post acute levels of care• Patient reported outcome tool • 249 items – 3 domains
– Basic Mobility– Daily Activity– Applied Cognitive
• Could be shortened and answered by surrogates
• Had not been validated for use in Acute care
2/10/2015
7
On Therapy evaluation, each discipline completes a functional measure assessment.
MOBILITY (PT):
1. Turning over in bed2. Supine to sit3. Bed to chair4. Sit to stand5. Walk in room6. 3-5 steps with a rail
SELF CARE (OT):
1. Feeding2. O/F hygiene3. Dressing Uppers4. Dressing Lowers5. Toilet (toilet, urinal, bedpan)6. Bathing (wash/rinse/dry)
Scale: 1= Unable (Total Assist) 2= A Lot (Mod/Max Assist)
3= A Little (Min Assist/CGA/Supervision) 4= None (Ind./Modified Independent)
Cleveland Clinic’s 6 ClicksCleveland Clinic’s 6 Clicks
Use of 6 clicks Data
Guide discharge recommendation
Guide therapist resource
utilization
Improve patient
mobility
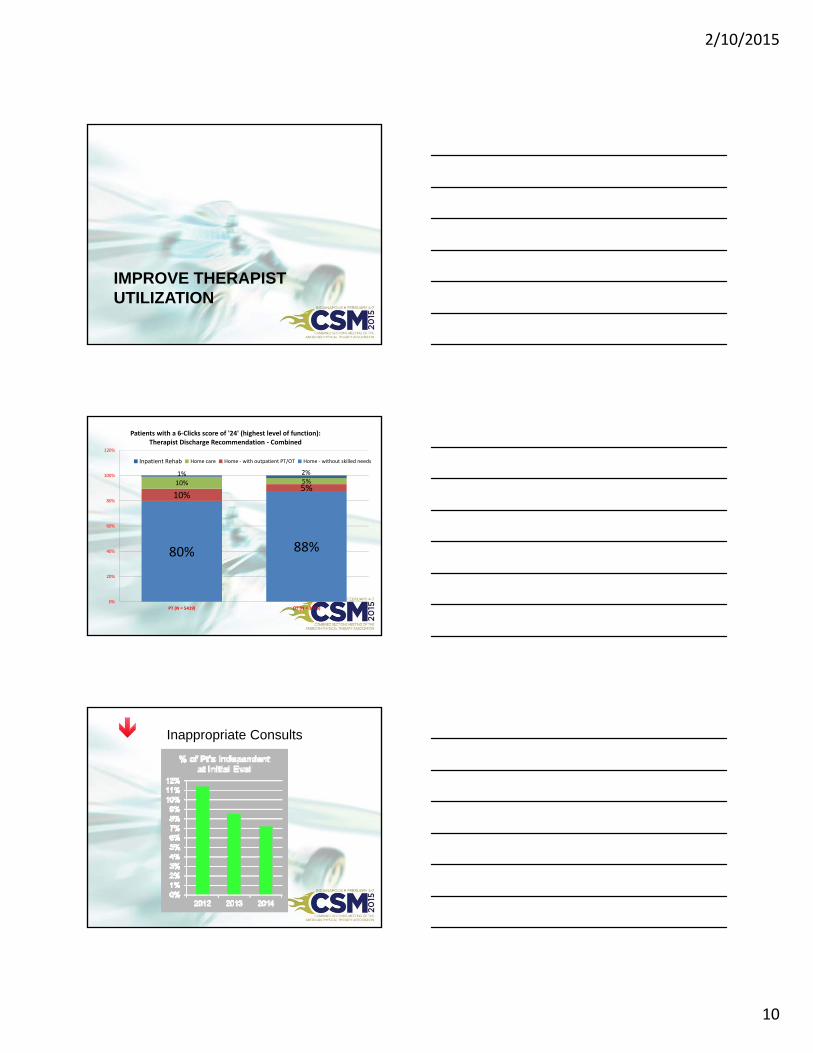
PT 6 Clicks Data Volume – CCHS Hospitals
2011 2012 2013 2014 Total
Eval 27,876 43,132 54,876 57,606 183,490
Follow up 0 67,219 86,290 93,498 247,007
Total Visits
27,876 110,351 141,166 151,104 430,497
2/10/2015
8
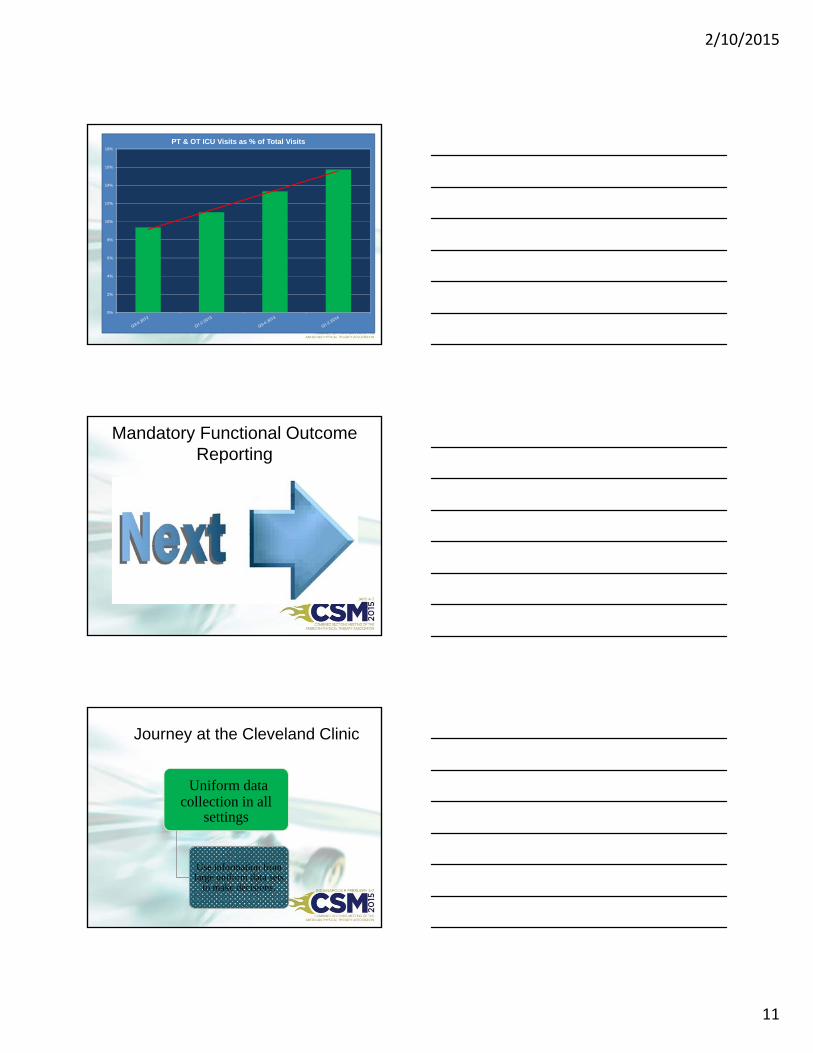
Improve Patient Mobility
Ability to collect, aggregate and display functional data in a way that is meaningful to all members of the medical team has changed behavior and contributed to a “all hands on deck”
philosophy around patient mobility
6 Clicks Distribution – All Hospitals 2014
Ideal for nursing mobility
GUIDE DISCHARGE RECOMMENDATIONS

2/10/2015
9
Using 6 Clicks to guide discharge recommendations
Data over the past three years has been consistent
Home with no services –19.48
Home with home care –17.81
SNF/IRF –
13.95 – 14.0
LTAC – 11.25
6 Clicks Predicts D/C Destination
• 83% of patients had recommendation and actual d/c placement match
• ROC analysis allowed us to define the best cutoff score for determining discharge to home on the basis of the highest sensitivity and specificity associated with the various scores.
• Cutoff scores of 42.9 for basic mobility and 39.4 for daily activity at the first visit provided fair to good accuracy for predicting discharge destination.
2/10/2015
10
IMPROVE THERAPIST UTILIZATION
80% 88%
10%5%
10% 5%1% 2%
0%
20%
40%
60%
80%
100%
120%
PT (N = 5419) OT (N = 3075)
Patients with a 6‐Clicks score of '24' (highest level of function):Therapist Discharge Recommendation ‐ Combined
Inpatient Rehab Home care Home ‐ with outpatient PT/OT Home ‐ without skilled needs
Inappropriate Consults
2/10/2015
11
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
PT & OT ICU Visits as % of Total Visits
Mandatory Functional Outcome Reporting
Journey at the Cleveland Clinic
Uniform data collection in all
settings
Use information from large uniform data sets
to make decisions.

2/10/2015
12
Opportunity at Cleveland Clinic
• Uniform Data Collection from all 47 outpatient locations into one database– Use that data to provide information back to policy makers
– Is there a benefit of using a single “generic” outcome tool.
– Useful starting point to increasing the accountability of rehabilitation professionals
– Represents a foundation for establishing a universal system of reporting
Outpatient Outcome Tools
Outpatient
• AM-PAC Short Forms both Basic and Adapted versions
• Diagnoses specific Tools• LEFS• QuickDash• Oswestry• NDI• FactB +4
Benefits of Using a Single Outcome Tool
Ability to Develop Large Data Sets
Measure function on the same scale across multiple settings
Begin to have a consistent measurement of “function”
Using a single tool to measure VALUE
2/10/2015
13
Outpatient AM-PAC Data
• Data available for patients seen between 7-1-13 to 6-30-14– Patients must have at least 2 AM-PAC to be included
• 13,000 matched patients by MRN in Database
• 6,000 additional patients with 2 AM-PACS that are not identified by MRN
What did the data tell us?
• Worked with Diane Jette to analyze data
• Manuscript submitted to PTJ– Change of severity modifier codes was heavily dependent on patients’
initial functional status
– The odds of improving at least one severity level was 4.42 (95% CI 3.38, 5.78) times greater for those with initial AM-PAC scores in the upper end of the range than for those with initial scores in lower end of the range of scores.
Aiming for Value Transformation
2/10/2015
14
Strategy for Value Transformation
• Improve outcomes without raising costs
• Lowering costs without compromising outcomes.
Goal –Improve value for patients
• Patient level • System level
What does that mean for
PT/OT/ST
“Value” of PT/OT
• Systematic utilization of PRO’s for every patient in every setting.
Outcome
• Resources consumed during service deliveryCost
Should we start measuring patient reported functional outcomes longitudinally across an episode of care
Acute Hospital
Skilled Nursing • Hospital Based
SNF’s• Connected Care
Units
Home Care Outpatient
2/10/2015
15
Outcome Tools
Acute Hospital
• 6 Clicks Basic Mobility• 6 Clicks Daily Activity• Mini Cog
Outcome Tools
SNF’s / Connected Care Units
• AM-PAC Basic Mobility Adapted• AM-PAC Basic Mobility Adapted with
w/c• AM-PAC Daily Activity• Completed on all patients at admission
and discharge from therapy
Use of AM-PAC in SNF
• SNF – Connected Care
• Compare LOS
• # visits
• Patient’s functional change between facilities
Can we establish a therapy efficiency measure??

2/10/2015
16
Next Steps
• We will adjust our thinking based on what we have learned.– Continue to collect “6 clicks” on EVERY patient at EVERY
visit
– Continue to collect functional outcome data as patients move to other post acute settings (SNF, IRF, Home Care)
– Standardize outcome tools that are used
– Move to diagnosis specific tools for non-Medicare patients.
Where do I start?
Lay the Groundwork
• Get the conversation started with key members of your organization– Who will be interested/impacted
• Identify your goals for outcomes collection– Questions you want/can answer
– Benchmarks for performance
• Identify criteria for selecting your outcomes tools– Focus, feasibility, meaningfulness

2/10/2015
17
Lay the Groundwork
• Select your tool(s) and train your team– Accuracy, consistency
• Prepare a database– Internal v. commercial
– “Minimum data set” of information to collect
Measure…Analyze…Share
• Ground rules for measurement– Frequency (intake + …)
• Ground rules for data analysis– Frequency of data review
– Reviews that address the questions posed
– What to do about problem cases
• Ground rules for reporting– What information will be shared
– What format will be used
– Who will receive the information
Effective Messaging
• Know your audience and their value priorities
• Ingredients of an effective message– Direct
– Concise
– Easy to remember
2/10/2015
18
APTA Tools and Resources
Evidence-Based Practice & Research
• PT Now – www.ptnow.org
• Clinical practice guidelines– http://www.apta.org/EvidenceResearch/ImplementingEBP/
• Physical Therapy Outcomes Registry– www.ptoutcomes.com
Additional Resources
• Validity of the AM-PAC ''6-Clicks'' Inpatient Daily Activity and Basic Mobility Short Forms. Diane U. Jette, Mary Stilphen, VinothK. Ranganathan, Sandra D. Passek, Frederick S. Frost and Alan M. Jette. PHYS THER. Published online November 14, 2013
• AM-PAC “6-Clicks” Functional Assessment Scores Predict Acute Hospital Discharge Destination. Diane U. Jette, Mary Stilphen, Vinoth K. Ranganathan, Sandra D. Passek, Frederick S. Frost and Alan M. Jette. PHYS THER. published ahead of print April 24, 2014
• A Sample of Private-Sector Hospital Discharge Tools: Case studies of hospital discharge planning tools that strive to improve transitions to post-acute care and reduce readmissions. American Hospital Association. 2015.
Related Documents











