Polyps – Where do they Polyps – Where do they come from and what do come from and what do you you do with them?! do with them?! Ron G. Landmann, MD Ron G. Landmann, MD Grand Rounds Grand Rounds Department of Surgery Department of Surgery St. Luke’s-Roosevelt Hospital Center St. Luke’s-Roosevelt Hospital Center March 21, 2007 March 21, 2007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Polyps – Where do they Polyps – Where do they come from and what do come from and what do youyou
do with them?!do with them?!
Ron G. Landmann, MDRon G. Landmann, MDGrand RoundsGrand Rounds
Department of SurgeryDepartment of SurgerySt. Luke’s-Roosevelt Hospital CenterSt. Luke’s-Roosevelt Hospital Center
March 21, 2007March 21, 2007

PolypsPolyps
Cancer epidemiologyCancer epidemiology Definition of the malignant polypDefinition of the malignant polyp Natural history of adenomatous polypsNatural history of adenomatous polyps Biology of polypsBiology of polyps The anatomy of the polypThe anatomy of the polyp Correlations with MalignancyCorrelations with Malignancy Endoscopic polypectomy alone???Endoscopic polypectomy alone??? Special considerationsSpecial considerations
* No discussion of technique* No discussion of technique

Colorectal Cancer – EpidemiologyColorectal Cancer – Epidemiology
Incidence: Approx. 150,000 cases/yearIncidence: Approx. 150,000 cases/year Deaths: Approx. 50,000 deaths/yearDeaths: Approx. 50,000 deaths/year
At diagnosisAt diagnosis 10% in situ disease10% in situ disease 30% local disease30% local disease 30% regional disease30% regional disease 30% distant disease30% distant disease
5 year survival, all patients: 50%5 year survival, all patients: 50% local - 90%local - 90% regional - 60%regional - 60% distant - 5%distant - 5%
U.S. Cancer Statistics Working Group. United States Cancer Statistics: 2003 Incidence and Mortality (preliminary data). Atlanta (GA): Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute; 2006.
Incidence/Prevalence of PolypsIncidence/Prevalence of Polyps
Adenomatous polypsAdenomatous polyps 30% of Western population30% of Western population
Most cancers arise from polypsMost cancers arise from polyps
*excludes syndromes*excludes syndromes

Carcinoma in situ vs. cancerCarcinoma in situ vs. cancer
ThinkThink Carcinoma Carcinoma in situ = in situ = high grade dysplasiahigh grade dysplasia Carcinoma Carcinoma in situin situ ≠ ≠ cancercancer
HistologyColorectal cancer is defined
by invasion of/through muscularis mucosa

Genetic model of colorectal tumorigenesis
Histology• Colorectal cancer is
defined by invasion of muscularis mucosa
• Lymphatics are located in submucosa

Colon Cancer StagingColon Cancer Staging
> 3 positive LNs2
1-3 positive LNs1
0 LN0
N-stage
Into other organs/perforates visceral peritoneumT4
Invades subserosa or pericolic/rectal tissuesT3
Invades muscularis propriaT2
Invades submucosaT1
Intraepithelial or invasion of lamina propriaTis
T-stage

Colon Cancer StagingColon Cancer Staging
551AnyAnyIV
404501-2AnyIII
5565003-4II
7075001-2I
00Tis0
RectumColon
MNT 5 year DSS (%)AJCC 5
Stage

Relationship Between TNM Stage and Survival in Colorectal Carcinoma
CA Cancer J Clin 2004;54;295-308
Treatment of CRCTreatment of CRC
PolypectomyPolypectomy Colonic ResectionColonic Resection
Treatment depends on the risk of lymph node metastasis.Treatment depends on the risk of lymph node metastasis.
Pathology is key!• Colorectal cancer is defined by
invasion of muscularis mucosa• Lymphatics are located in
submucosa

Incidence of malignant polypsIncidence of malignant polyps
DefinitionDefinition Malignant polyps or T1 lesions (limited to the Malignant polyps or T1 lesions (limited to the
submucosa)submucosa) Represent 5% of all adenomasRepresent 5% of all adenomas
Colonoscopy polypectomy series: 2 – 12%Colonoscopy polypectomy series: 2 – 12% Colorectal resection series: 4 – 9%Colorectal resection series: 4 – 9%

Haggitt Level (1985)Haggitt Level (1985)Classification of polyps with invasive cancerClassification of polyps with invasive cancer
Haggitt RC, Glotzbach RE, Soffer EE, Wruble LD. Prognostic factors in colorectal carcinoma arising in adenomas: Implications for lesions removed by endoscopic polypectomy. Gastroenterology 89:328-36, 1985, p 330.
Carcinoma in situ
0
Invasion of submucosa of bowel wall below polyp
Invasion of stalk
Invasion of neck
Invasion of head
Definition
4 (31%, 12-25%)
134
0 (< 1%)43
0 (< 1%)32
0 (< 1%)61
+ LN (N)Resected (N)
Level
Villuous/sessile (flat) polyps with invasive cancer are by definition Haggitt 4.

Sessile PolypsSessile PolypsKudo, 1993Kudo, 1993
Risk of lymph node metastasis in each sessile lesion is not the Risk of lymph node metastasis in each sessile lesion is not the samesame
Haggitt’s: no detail for sessile lesionsHaggitt’s: no detail for sessile lesions Classification of submucosal invasion:Classification of submucosal invasion:
Sm1—Invasion into the upper third of the submucosaSm1—Invasion into the upper third of the submucosa Sm2—Invasion into the middle third of the submucosaSm2—Invasion into the middle third of the submucosa Sm3—Invasion into the lower third of the submucosaSm3—Invasion into the lower third of the submucosa
High rate of LN metastasis: 12-25%High rate of LN metastasis: 12-25%

Sm systemSm system
Able to determine Sm1, Sm2, Sm3 in 97% of Able to determine Sm1, Sm2, Sm3 in 97% of casescases
Haggitt Level 1, 2, 3 = Sm1Haggitt Level 1, 2, 3 = Sm1 Haggitt Level 4 = Sm1, Sm2, or Sm3Haggitt Level 4 = Sm1, Sm2, or Sm3
Endoscopist must properly resect and prepare Endoscopist must properly resect and prepare specimenspecimen
Pathologist must properly section and examine Pathologist must properly section and examine all layersall layers
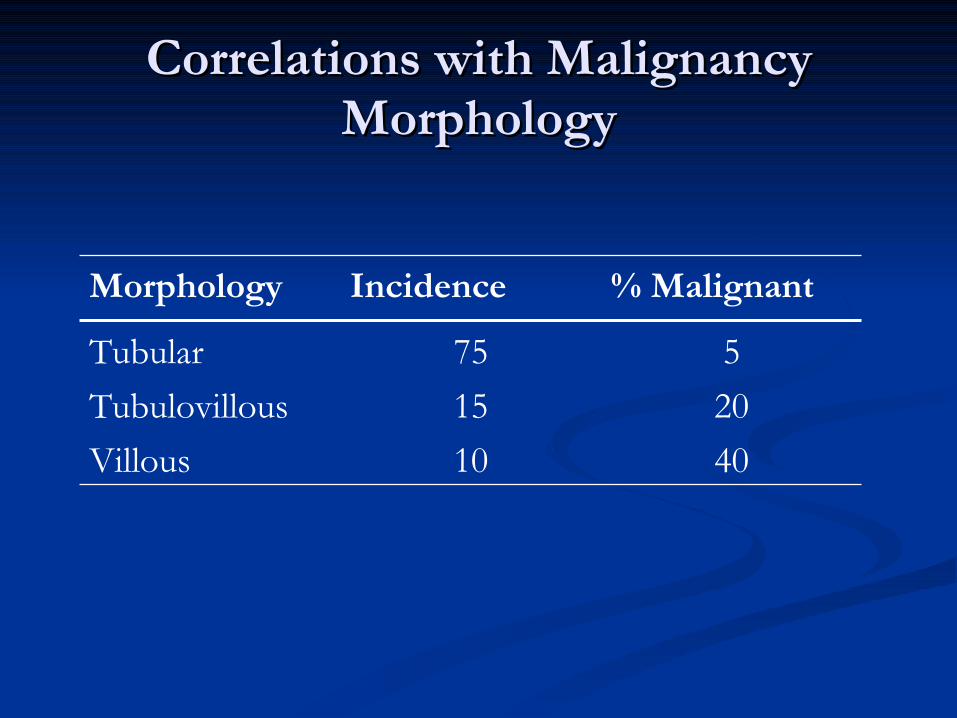
Correlations with MalignancyCorrelations with MalignancyMorphologyMorphology
4010Villous
2015Tubulovillous
575Tubular
% MalignantIncidenceMorphology

Correlations with MalignancyCorrelations with MalignancyGradeGrade
30Severe
20Moderate
5Mild
% malignantDysplasia

Correlations with MalignancyCorrelations with MalignancySizeSize
50≥ 2
101 – 2
1< 1
% malignantSize (cm)
Muto, 1975

Correlations with MalignancyCorrelations with MalignancySizeSize
Muto, 1975
76≥ 3.5
432.6-3.5
191.6 – 2.5
20.6 – 1.5
Negligible≤ 0.5
% malignantSize (cm)
Nusco, 1997
50≥ 2
101 – 2
1< 1
% malignantSize (cm)
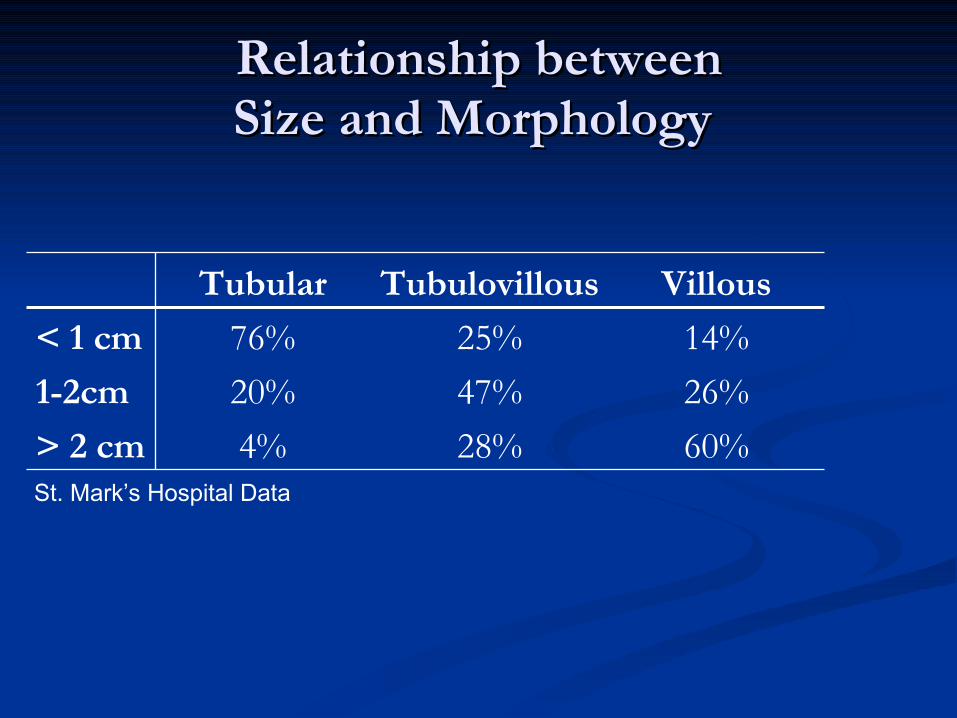
Relationship betweenRelationship betweenSize and Morphology Size and Morphology
60%28%4%> 2 cm
26%47%20%1-2cm
14%25%76%< 1 cm
VillousTubulovillousTubular
St. Mark’s Hospital Data
Increased risk of LN MetastasisIncreased risk of LN Metastasis
Unfavorable pathologic features of malignant CR Unfavorable pathologic features of malignant CR polypspolyps Poor differentiation (only on univariate)Poor differentiation (only on univariate) Lymphovascular invasion (P < 0.009)Lymphovascular invasion (P < 0.009) Invasion below submucosa (Haggitt Level 4)Invasion below submucosa (Haggitt Level 4) Depth of invasion in Sm3 (P < 0.001)Depth of invasion in Sm3 (P < 0.001) Site in lower 1/3 of the rectum (P < 0.001)Site in lower 1/3 of the rectum (P < 0.001)
Positive resection margin (< 1 mm or 1 HPF)Positive resection margin (< 1 mm or 1 HPF) Not really – this is inadequate treatment, not an adverse risk factor!Not really – this is inadequate treatment, not an adverse risk factor!
P-values from Nascimbeni et al. N = 353 T1 colorectal sessile lesions
Management of Pedunculated Management of Pedunculated Malignant PolypsMalignant Polyps
Haggitt Level 1, 2, 3Haggitt Level 1, 2, 3 Complete excision or snaringComplete excision or snaring Risk of LN metastasis < 1%Risk of LN metastasis < 1%
Haggitt Level 4Haggitt Level 4 Treat as sessile lesionsTreat as sessile lesions
Management of Sessile Malignant Management of Sessile Malignant PolypsPolyps
< 2cm in diameter< 2cm in diameter Adequate snare in one piece via colonoscopyAdequate snare in one piece via colonoscopy Requires microscopic free margin of at least 2mmRequires microscopic free margin of at least 2mm
Piecemeal removalPiecemeal removal Requires further excision/follow-up or resectionRequires further excision/follow-up or resection
High risk factors (LVI, Sm3, distal 1/3 rectum)High risk factors (LVI, Sm3, distal 1/3 rectum) Oncologic resectionOncologic resection Full thickness transanal excisionFull thickness transanal excision

Lesions amenable to colonoscopic Lesions amenable to colonoscopic polypectomypolypectomy
Pedunculated or sessile < 2cmPedunculated or sessile < 2cm Well/moderately differentiatedWell/moderately differentiated No lymphovascular invasionNo lymphovascular invasion Haggitt Level 1-3 or Sm1Haggitt Level 1-3 or Sm1 Close follow-up availableClose follow-up available
Endoscopically complete Endoscopically complete excisionexcision Negative resection margins (2mm)Negative resection margins (2mm)

Criteria for Treatment of Malignant Criteria for Treatment of Malignant CR Polyps by Polypectomy AloneCR Polyps by Polypectomy Alone
Determined by risk of metastasisDetermined by risk of metastasis
Low risk of Lymph Node MetastasisLow risk of Lymph Node Metastasis PedunculatedPedunculated
Haggitt Level 1, 2, 3Haggitt Level 1, 2, 3 Level 4 Sm1, Sm2Level 4 Sm1, Sm2
SessileSessile Sm1, Sm2Sm1, Sm2
High risk of Lymph Node MetastasisHigh risk of Lymph Node Metastasis Lower 1/3 of the submucosa (Sm3)Lower 1/3 of the submucosa (Sm3) LVILVI Distal 1/3 of rectumDistal 1/3 of rectum
Malignant Colorectal Polyps that Malignant Colorectal Polyps that Should have an Oncologic Bowel Should have an Oncologic Bowel
ResectionResection Lesions in colonLesions in colon
Pedunculated Haggitt Level 4 with invasion into distal third of Pedunculated Haggitt Level 4 with invasion into distal third of submucosa (Sm3) or LVIsubmucosa (Sm3) or LVI
Sessile lesions removed with margin < 2mmSessile lesions removed with margin < 2mm Sessile lesions removed piecemealSessile lesions removed piecemeal Sessile lesions with depth of invasion into distal third of submucosa Sessile lesions with depth of invasion into distal third of submucosa
(Sm3)(Sm3) Sessile lesions with LVISessile lesions with LVI
Lesions in middle third and upper third rectumLesions in middle third and upper third rectum Same as lesions in colonSame as lesions in colon
Lesions in distal third rectumLesions in distal third rectum Pedunculated Haggitt Level 4 with invasion into distal third of Pedunculated Haggitt Level 4 with invasion into distal third of
submucosa (Sm3) or pedunculated lesions with LVIsubmucosa (Sm3) or pedunculated lesions with LVI All sessile lesionsAll sessile lesions

Why not just resect anyway?!Why not just resect anyway?!
What if ???What if ??? What if it’s clipped in ½?What if it’s clipped in ½?
PedunculatedPedunculated Repeat endoscopy.Repeat endoscopy. Require good resection with margin (2mm)Require good resection with margin (2mm)
SessileSessile Requires operative oncologic resection (even if Sm1, Sm2)Requires operative oncologic resection (even if Sm1, Sm2)
Unable to determine exact pathologic depthUnable to determine exact pathologic depth What if it’s shredded by forceps?What if it’s shredded by forceps?
Requires operative oncologic resectionRequires operative oncologic resection What if it’s a very small lesion?What if it’s a very small lesion?
Requires marking/tattoo CIRCUMFERENTIALLYRequires marking/tattoo CIRCUMFERENTIALLY What if it’s carcinoma in situ?What if it’s carcinoma in situ?
It’s not cancer. This is high grade dysplasia. Requires close follow-up.It’s not cancer. This is high grade dysplasia. Requires close follow-up. Unless,Unless,
poor margins: repeat endoscopy with good marginspoor margins: repeat endoscopy with good margins Piecemeal resection: discussion with pathologist and patientPiecemeal resection: discussion with pathologist and patient
What if it’s a large, non-endoscopically resectable polyp?What if it’s a large, non-endoscopically resectable polyp? Repeat endoscopy (2Repeat endoscopy (2ndnd MD?) MD?) Oncologic resectionOncologic resection

Other considerations…Other considerations…
When in doubtWhen in doubt Repeat colonoscopy Repeat colonoscopy
(endoscopy)(endoscopy) Personally review pathologyPersonally review pathology Get a second opinionGet a second opinion Have a frank discussion with Have a frank discussion with
patientpatient


PolypsPolyps
Natural history of adenomatous polypsNatural history of adenomatous polyps Biology of polypsBiology of polyps Cancer epidemiologyCancer epidemiology The anatomy of the polypThe anatomy of the polyp Correlations with MalignancyCorrelations with Malignancy Endoscopic polypectomy alone???Endoscopic polypectomy alone??? Special considerationsSpecial considerations Indications for PolypectomyIndications for Polypectomy
What if it’s clipped in ½What if it’s clipped in ½ What if it’s shredded by forceps?What if it’s shredded by forceps?
Pathology…Pathology… Marking/tattooMarking/tattoo Chances of Malignancy by histopath and size/morphologyChances of Malignancy by histopath and size/morphology * NO technique *** NO technique **