Colorectal Cancer by prof/ gouda ellabban

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Colorectal Cancer
by
prof/ gouda ellabban
One of the most common cancers in the world
US: 4th most common cancer (after lung, prostate, and breast
cancers) 2nd most common cause of cancer death (after lung cancer)
2001: 130,000 new cases of CRC 56,500 deaths
caused by CRC

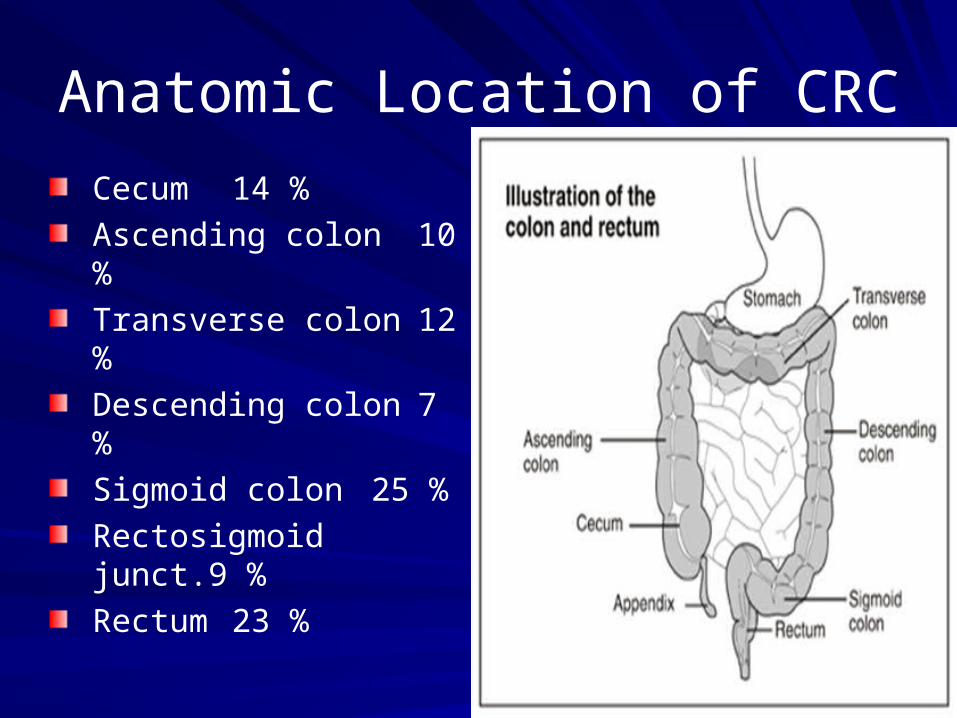
Anatomic Location of CRC
Cecum 14 %Ascending colon 10 %Transverse colon 12 %Descending colon 7 %Sigmoid colon 25 %Rectosigmoid junct.9 %Rectum 23 %
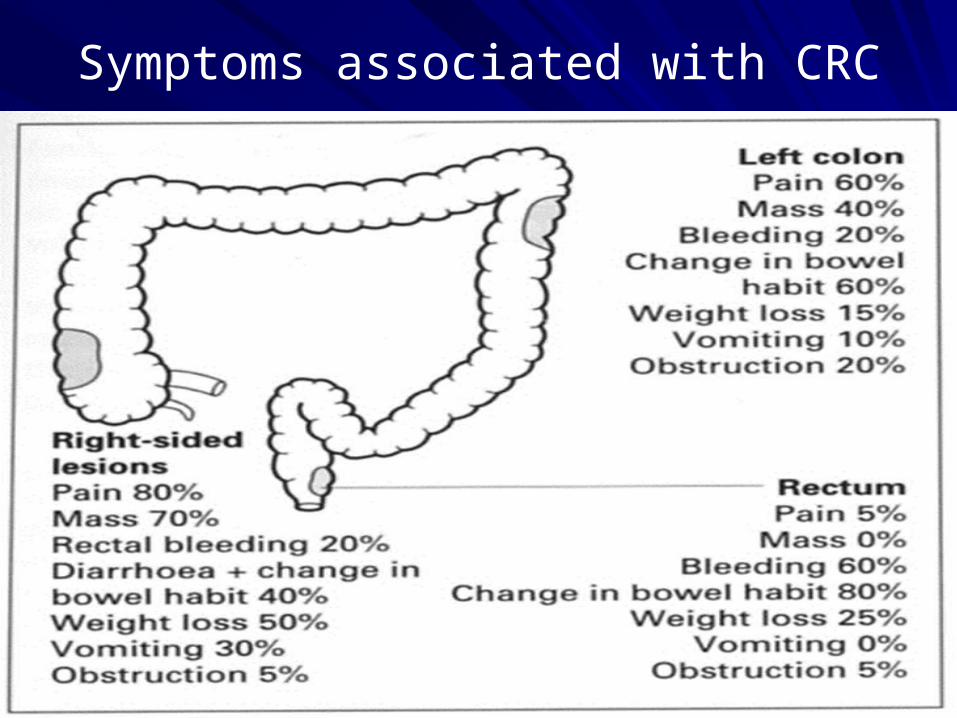
Symptoms associated with CRC
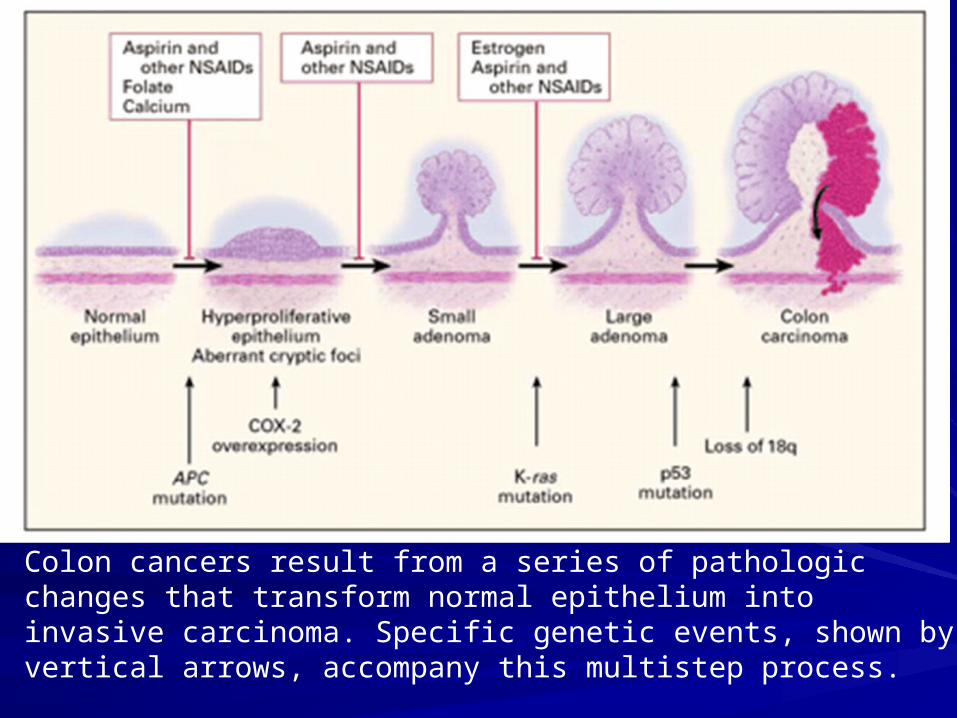
Colon cancers result from a series of pathologic changes that transform normal epithelium into invasive carcinoma. Specific genetic events, shown by vertical arrows, accompany this multistep process.
WHO Classification of CRC
Adenocarcinoma in situ / severe dysplasiaAdenocarcinomaMucinous (colloid) adenocarcinoma (>50% mucinous)Signet ring cell carcinoma (>50% signet ring cells)Squamous cell (epidermoid) carcinomaAdenosquamous carcinomaSmall-cell (oat cell) carcinomaMedullary carcinomaUndifferentiated Carcinoma
Risk factors for CRC
AgeAdenomas, PolypsSedentary lifestyle, Diet, ObesityFamily History of CRCInflammatory Bowel Disease (IBD)Hereditary Syndromes (familial adenomatous polyposis (FAP))
Development of CRC
Result of interplay between environmental and genetic factors
Central environmental factors:
Diet and lifestyle
35% of all cancers are attributable to diet
50%-75% of CRC in the US may be preventable through dietary modifications
Dietary factors implicated in colorectal carcinogenesis
Increased risk
consumption of red meat
animal and saturated fat
refined carbohydrates
alcohol

Dietary factors implicated in colorectal carcinogenesis
Decreased risk
dietary fiber
vegetables
fruits
antioxidant vitamins
calcium
folate (B Vitamin)
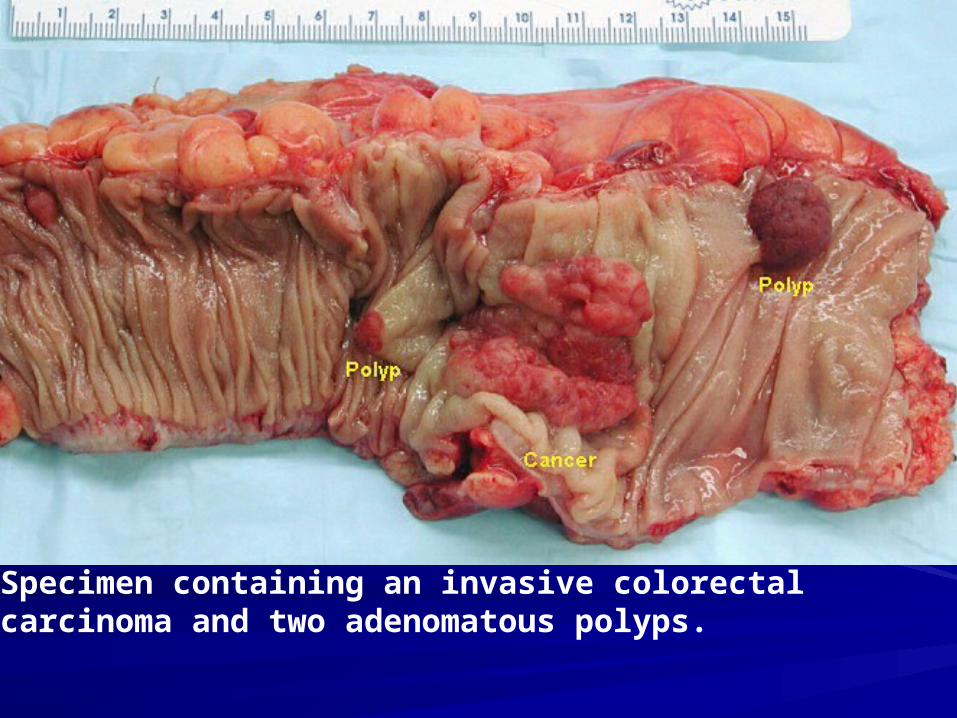
Specimen containing an invasive colorectal carcinoma and two adenomatous polyps.

Multiple adenomatous polyps of the cecum are seen here in a case of familial polyposis.

Familial polyposis in which mucosal surface of the colon is a carpet of small adenomatous polyps. Even though they are small , there is a 100% risk over time for development of adenocarcinoma, for which total colectomy is recommended
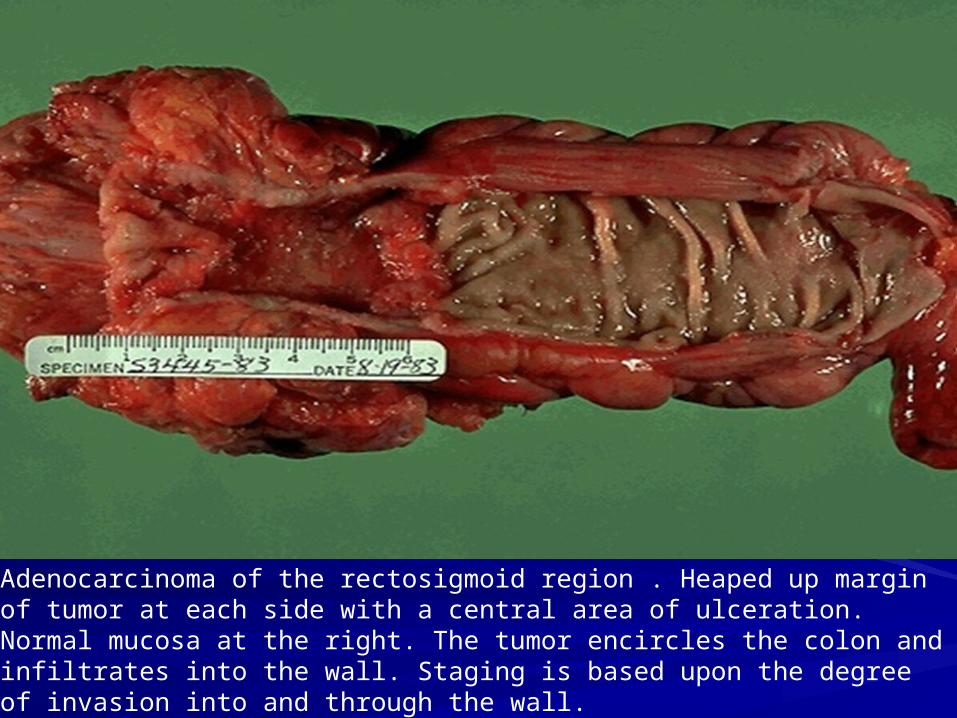
Adenocarcinoma of the rectosigmoid region . Heaped up margin of tumor at each side with a central area of ulceration. Normal mucosa at the right. The tumor encircles the colon and infiltrates into the wall. Staging is based upon the degree of invasion into and through the wall.
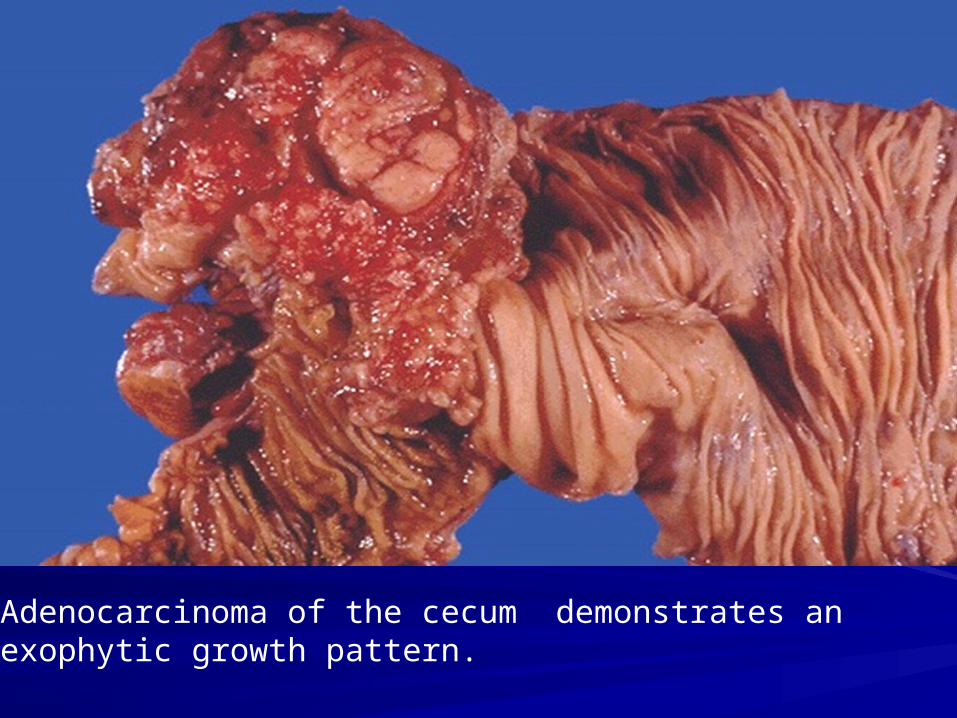
Adenocarcinoma of the cecum demonstrates an exophytic growth pattern.
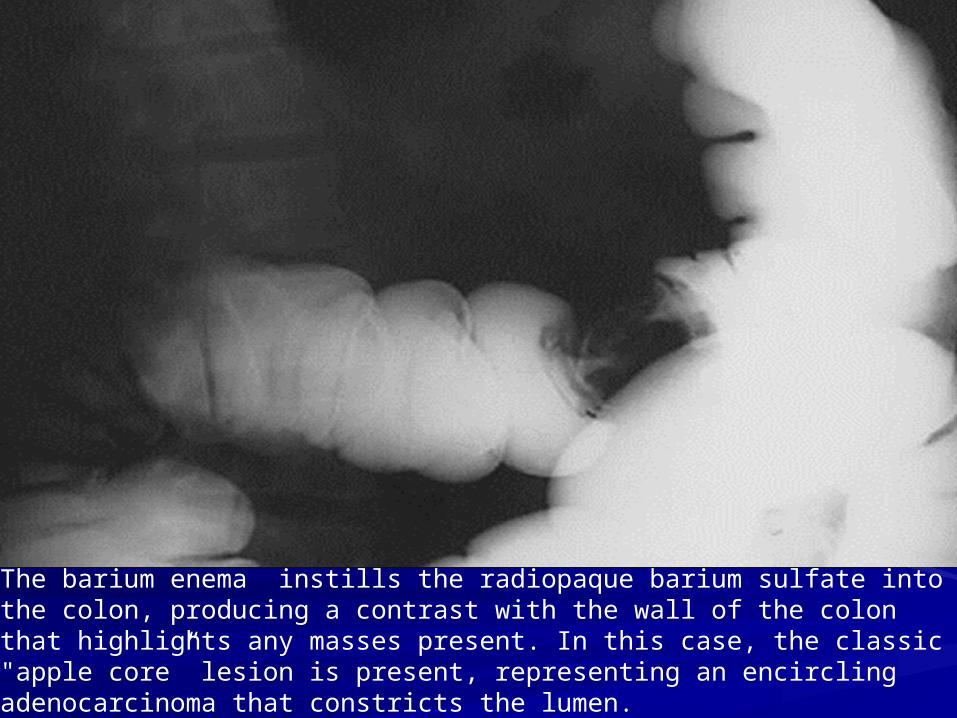
The barium enema instills the radiopaque barium sulfate into the colon, producing a contrast with the wall of the colon that highlights any masses present. In this case, the classic "apple core” lesion is present, representing an encircling adenocarcinoma that constricts the lumen.
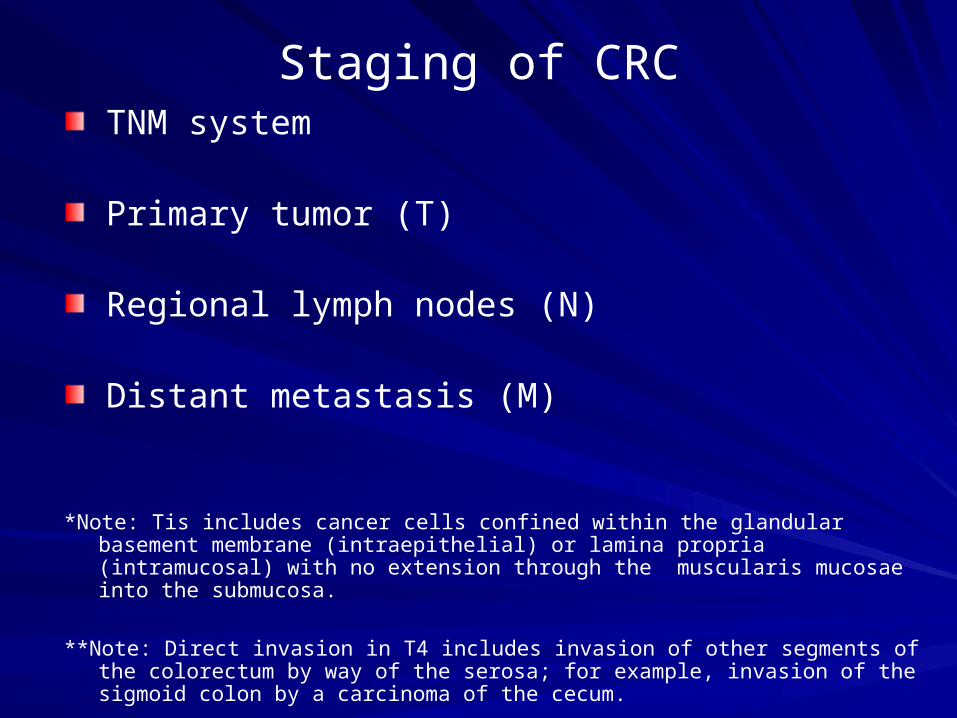
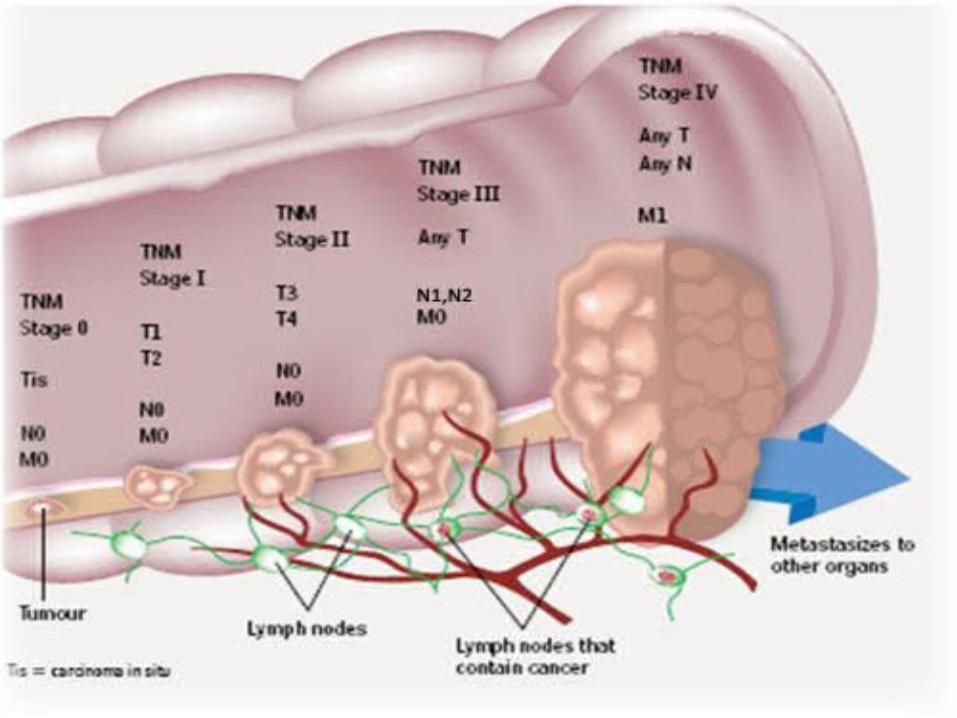
Staging of CRCTNM system
Primary tumor (T)
Regional lymph nodes (N)
Distant metastasis (M)
*Note: Tis includes cancer cells confined within the glandular basement membrane (intraepithelial) or lamina propria (intramucosal) with no extension through the muscularis mucosae into the submucosa.
**Note: Direct invasion in T4 includes invasion of other segments of the colorectum by way of the serosa; for example, invasion of the sigmoid colon by a carcinoma of the cecum.
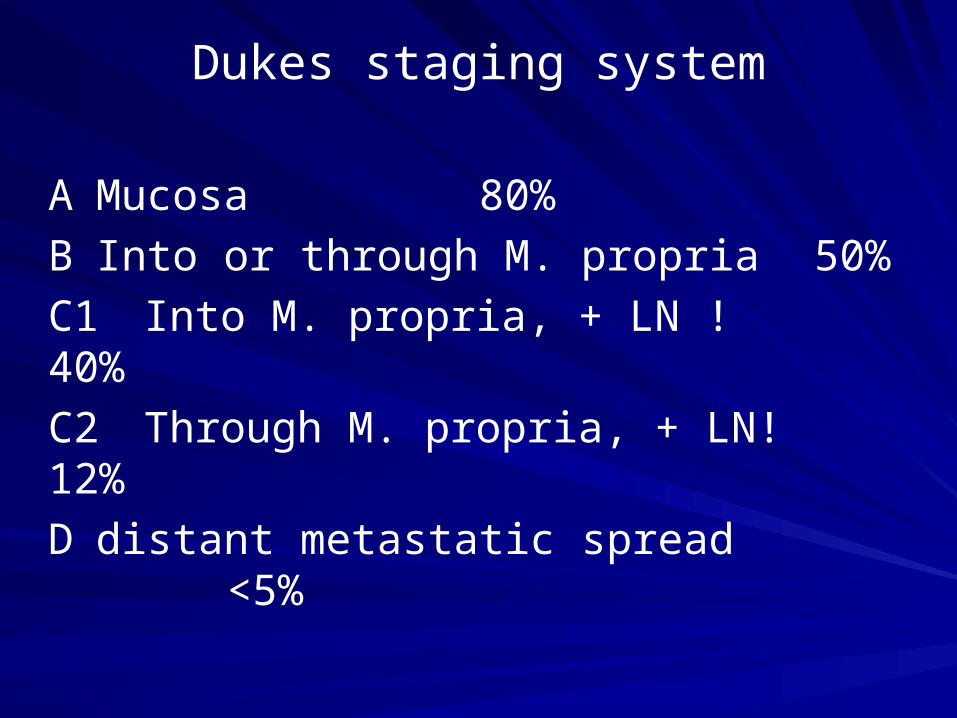
Dukes staging system
A Mucosa 80%
B Into or through M. propria 50%
C1 Into M. propria, + LN ! 40%
C2 Through M. propria, + LN! 12%
D distant metastatic spread <5%

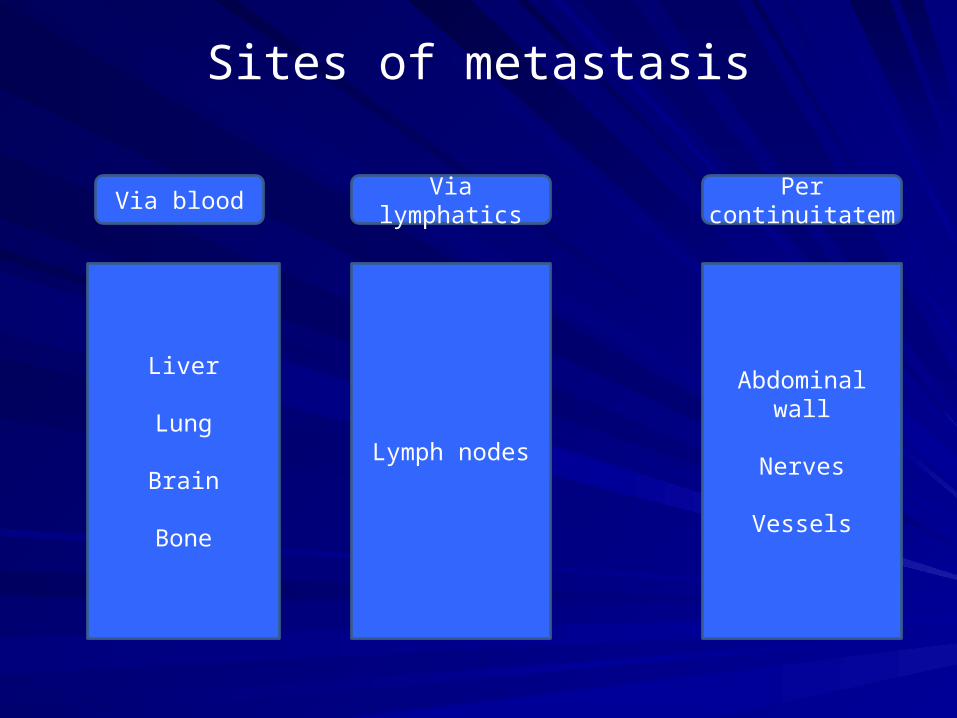
Sites of metastasis
Liver
Lung
Brain
Bone
Via blood
Lymph nodes
Abdominal wall
Nerves
Vessels
Via lymphatics Per continuitatem

Therapy
Surgical resection the only curative treatment
Likelihood of cure is greater when disease is detected at an early stage
Early detection and screening is of pivotal
importance

Surgery is the mainstay of treatment of RC
After surgical resection, local failure is common
Local recurrence after conventional surgery:
15%-45% (average of 28%)
Radiotherapy significantly reduces the number of local recurrences in rectal cancers, its use in colon cancer is not routine due to the sensitivity of the bowels to radiation.
Radiotherapy in the management of Rectal Cancer
In at least 28 randomised trials the value of either preoperative or postoperative RT has been tested
Preoperative RT (30+Gy): 57% relative reduction of local failurePostoperative RT (35+Gy): 33% relative reduction
Colorectal Cancer Collaborative Group. Lancet 2001;358:1291
Gamma C. JAMA 2000;284:1008
Adjuvant Therapy of Rectal Cancer
1990 US NIH Consensus Conference
Postoperative chemoradiotherapy = standard of care for RC Stage II,III
The consensus statement was based upon the results of three randomised trials
ESMO Recommendations
Resectable cases
Surgical procedure: TME
Preoperative RT: recommended
Postoperative chemoradiotherapy: T3,4 or N+
Non-resectable cases: local recurrences
Preoperative RT with or without CT
Predicting risk of recurrence in Rectal Carcinoma
Surgery-related-Low anterior resection-Excision of the mesorectum-Extend of lymphadenectomy-postoperative anastomotic
leakage-Tumor perforation
Tumor-related-Anatomic location-Histologic type-Tumor grade-Pathologic stage-radial resection margin-neural, venous, lymphatic invasion
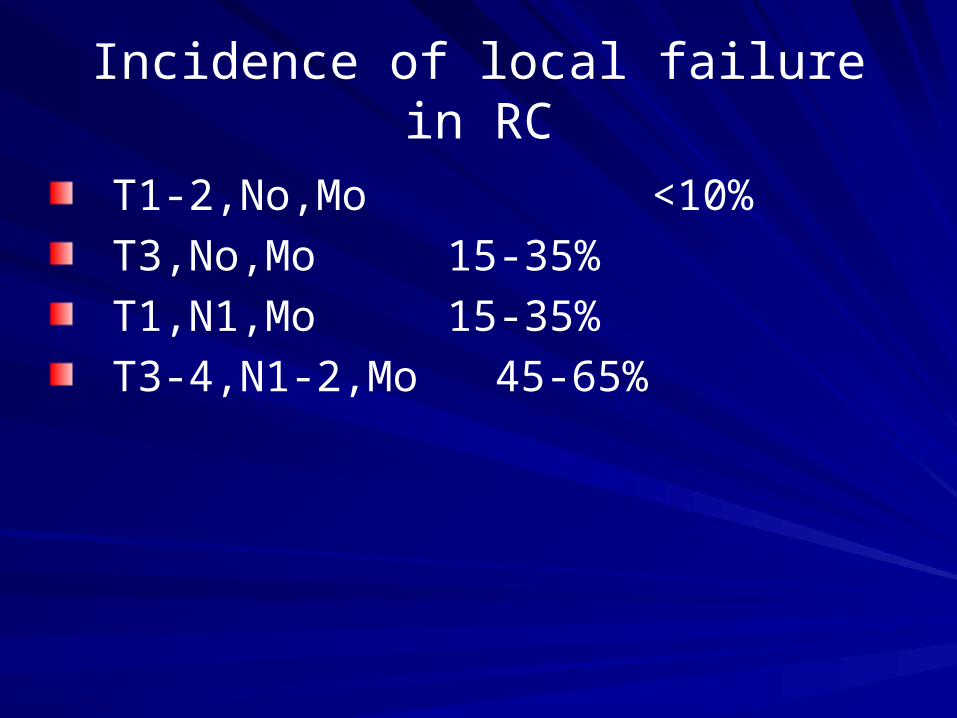
Incidence of local failure in RC
T1-2,No,Mo <10%
T3,No,Mo 15-35%
T1,N1,Mo 15-35%
T3-4,N1-2,Mo 45-65%
Total Mesorectal Excision (TME)
Local recurrence rates after surgical resection of RC have decreased from about 30% to < 10%
1. Radio(chemo)therapy
2. Importance of circumferential margin (TME)
Screening
What is screening?
A public health service in which members of a defined population are examined to identify those individuals who would benefit from treatment
To benefit: to reduce the risk of a disease or its complications
Types of Screening
Fecal occult blood test (FOBT)Chemical test for blood in a stool sample. Annual screening by FOBT reduces colorectal cancer deaths by 33%
Flexible sigmoidoscopy can detect about 65%–75% of polyps and 40%–65% of colorectal cancers. Rectum and sigmoid colon are visually inspected

Current Screening Guidelines
Regular screening for all adults aged 50 years or older is recommended
FOBT every year
Flexible sigmoidoscopy every 5 years
Total colon examination by colonoscopy every 10 years or by barium enema every 5–10 years
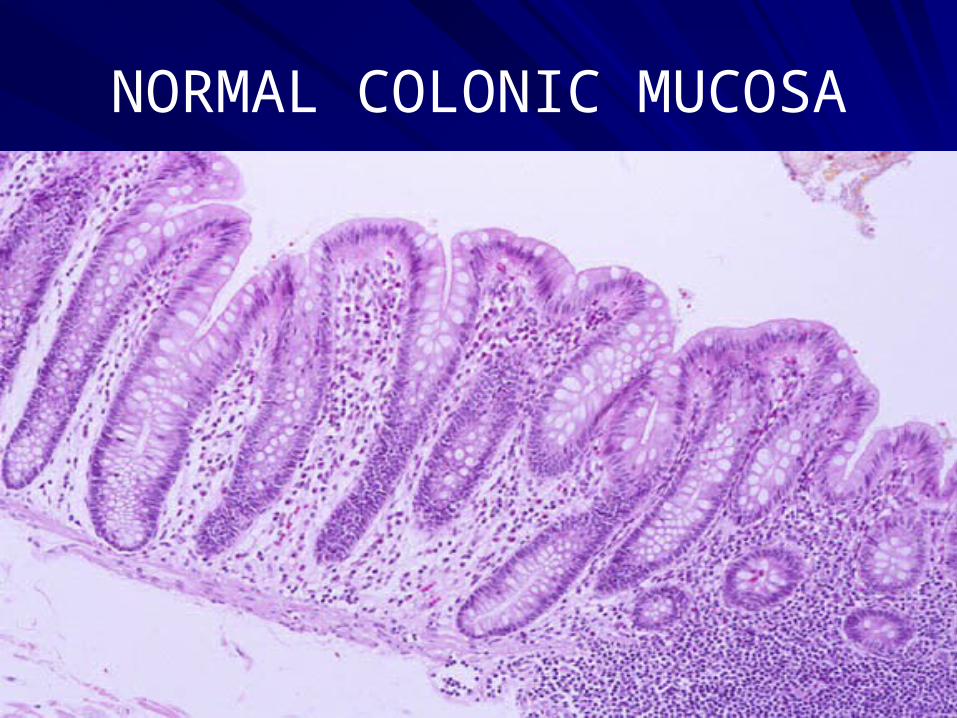
NORMAL COLONIC MUCOSA
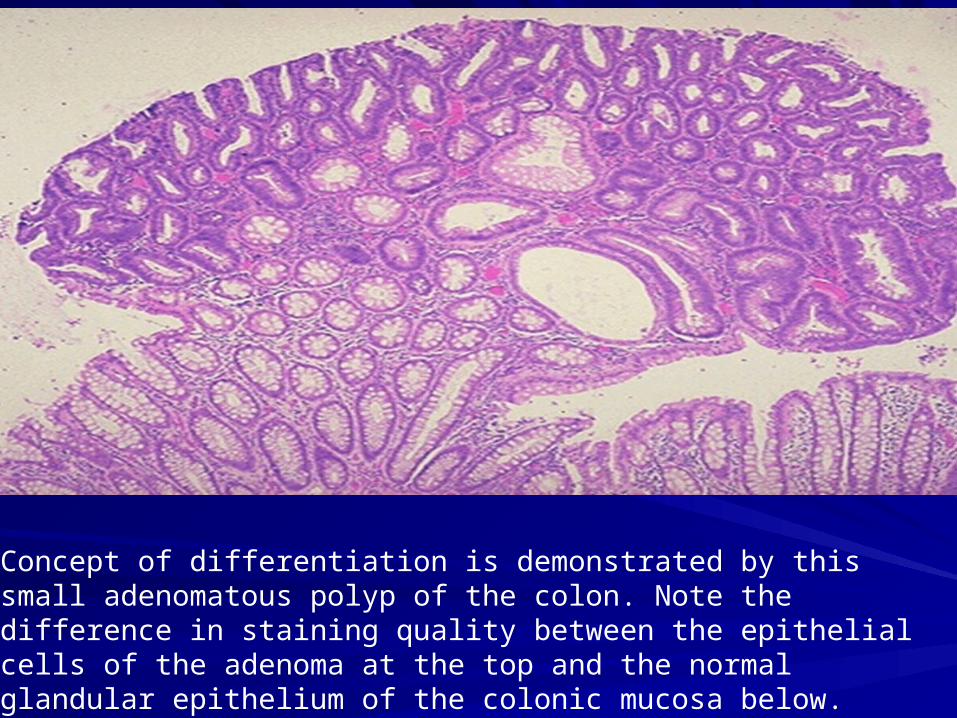
Concept of differentiation is demonstrated by this small adenomatous polyp of the colon. Note the difference in staining quality between the epithelial cells of the adenoma at the top and the normal glandular epithelium of the colonic mucosa below.
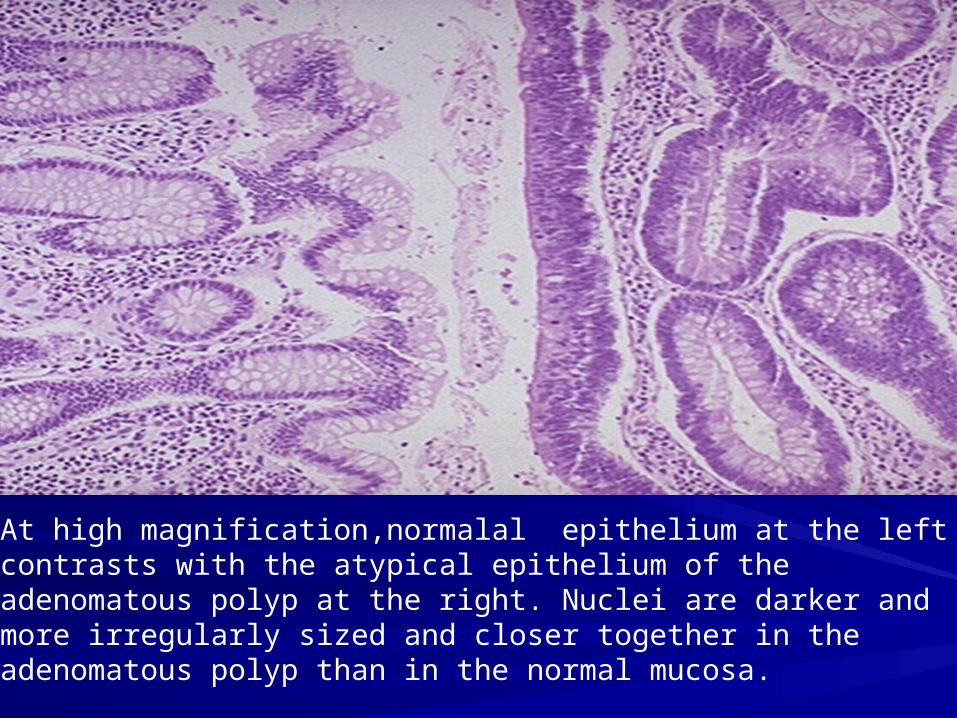
At high magnification,normalal epithelium at the left contrasts with the atypical epithelium of the adenomatous polyp at the right. Nuclei are darker and more irregularly sized and closer together in the adenomatous polyp than in the normal mucosa.
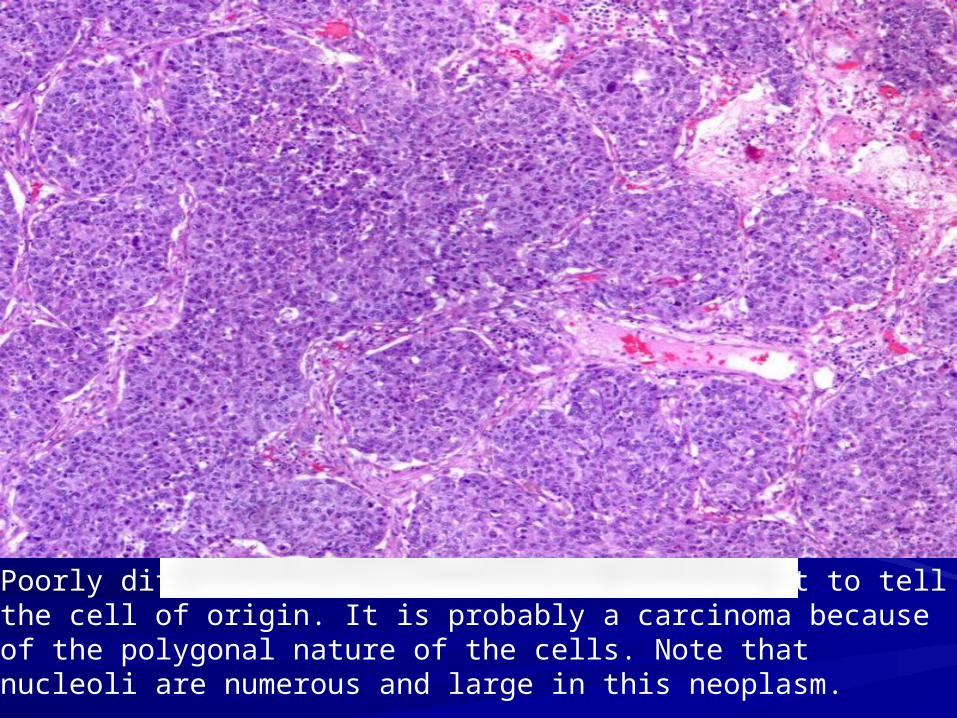
Poorly differentiated neoplasm, it is difficult to tell the cell of origin. It is probably a carcinoma because of the polygonal nature of the cells. Note that nucleoli are numerous and large in this neoplasm.

CK staining reaction for carcinomas helps to distinguish carcinoma from sarcomas and lymphomas. Immunoperoxidase staining is helpful to determine the cell type of a neoplasm when the degree of differentiation, or morphology alone, does not allow an exact classification.
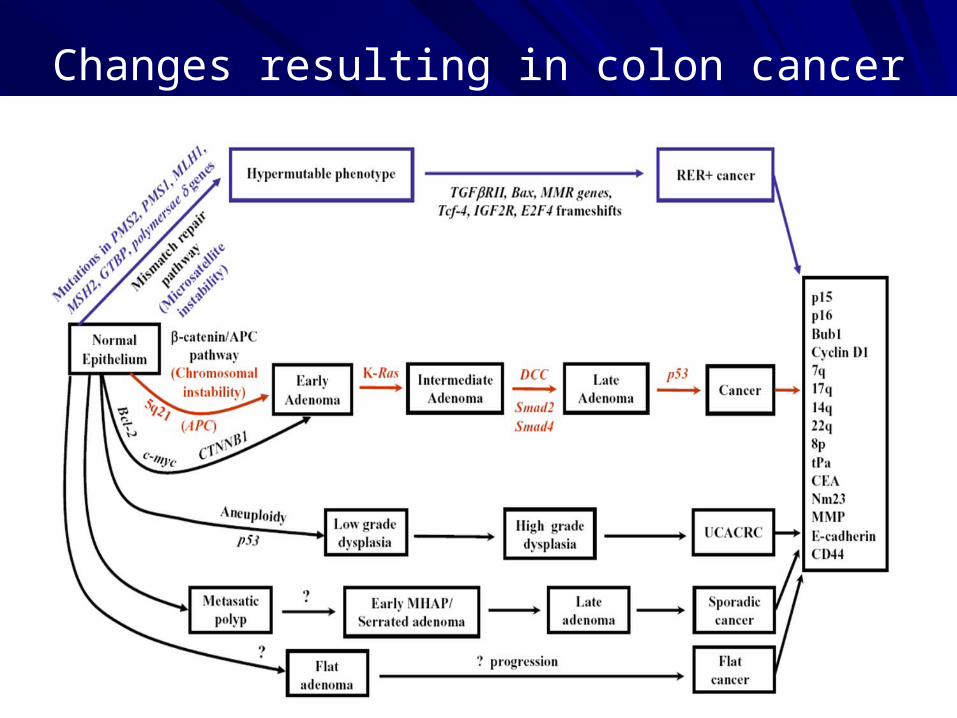
Changes resulting in colon cancer

Molecular Biology & Pathology
CRCs arise from a series of histopathological and molecular changes that transform normal epithelial cells
Intermediate step is the adenomatous polyp
Adenoma-Carcinoma-Sequence (Vogelstein & Kinzler)
Polyps occur universally in FAP, but FAP accounts for only 1% of CRCs
Adenomatous Polyps in general population:33% at age 5070% at age 70

Summary
CRC is a leading cause of death
Early stages are detectable
Screening can prevent CRC
thanks
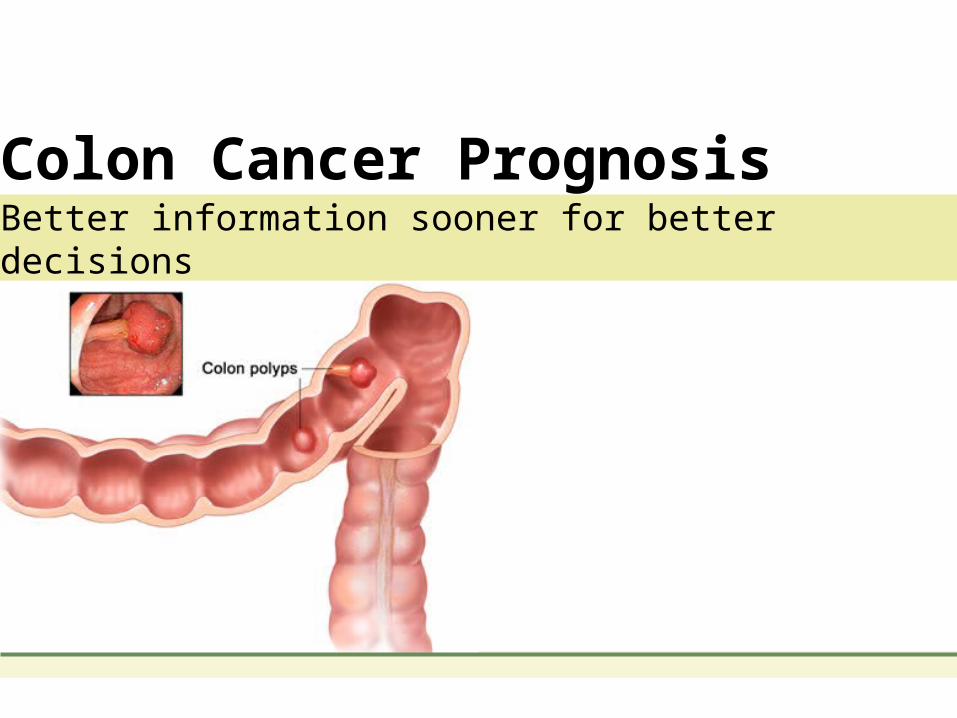
Colon Cancer PrognosisBetter information sooner for better decisions
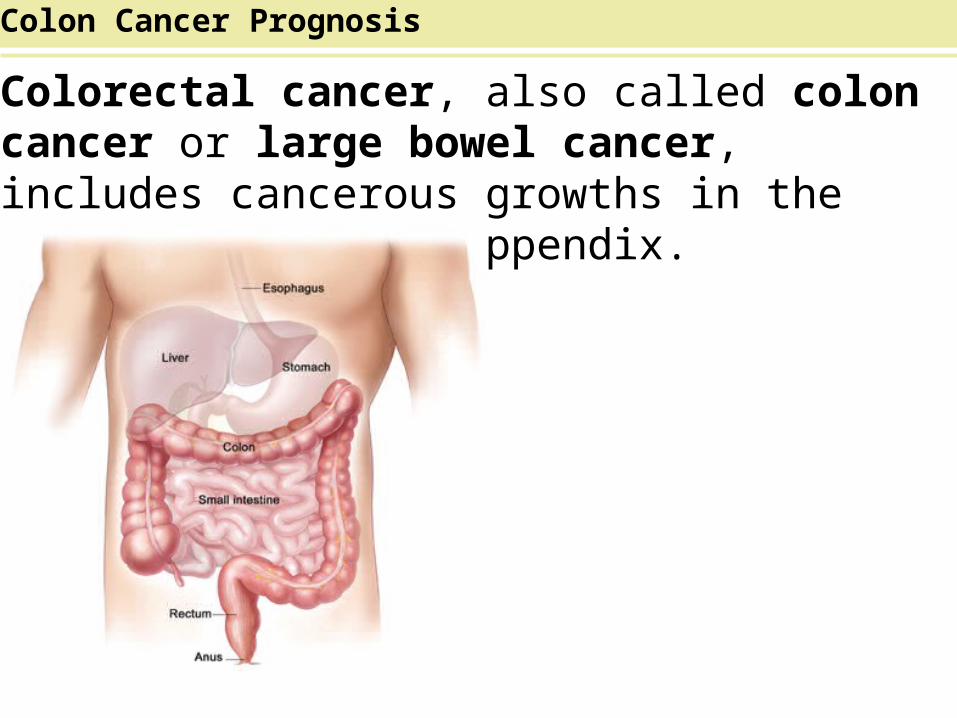
Colorectal cancer, also called colon cancer or large bowel cancer, includes cancerous growths in the colon, rectum and appendix.
Colon Cancer Prognosis
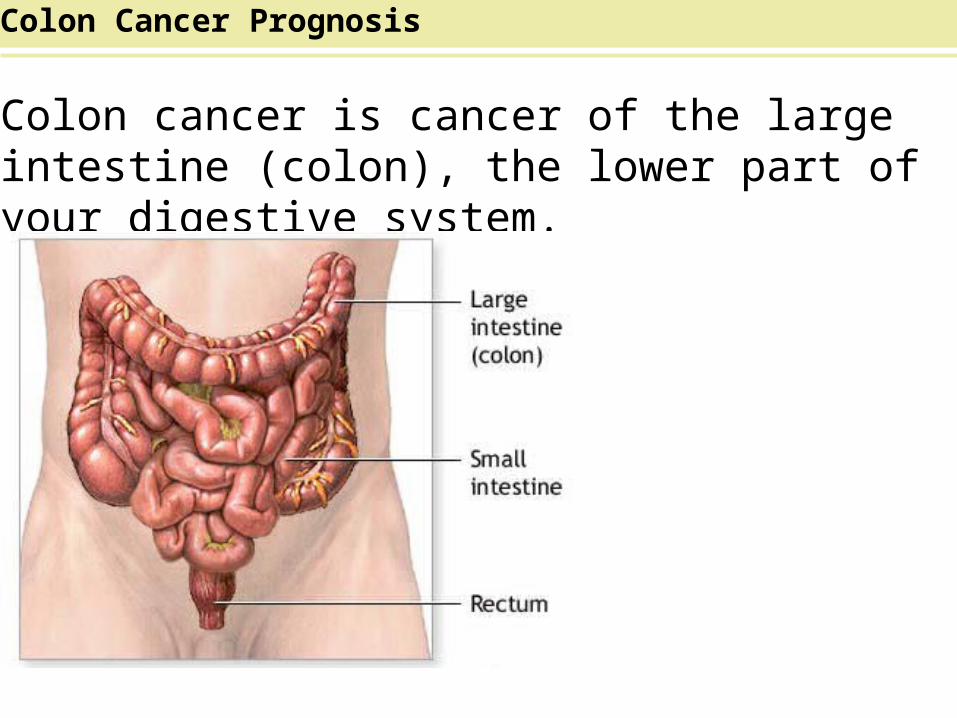
Colon cancer is cancer of the large intestine (colon), the lower part of your digestive system.
Colon Cancer Prognosis

The symptoms of colorectal cancer depend on the location of tumor in bowel and whether it has spread to elsewhere in the body (metastasis).
Colon Cancer Prognosis

There are five colon cancer stages (0-4).Stage 0 Colon Cancer is the earliest form of cancer where it is in its original place.In stage 1,cancer has extended beyond the innermost layer of the colon into the middle layers of the colon.Colon cancer is considered stage 2 after it moves beyond the middle layers of the colon.If colon cancer is found in at least three lymph nodes, it has reached stage 3.Stage 4 is the most advanced colon cancer stage where the cancer has spread to nearby lymph nodes and other parts of the body.
Colon Cancer Prognosis

Most cases of colon cancer begin as small, noncancerous (benign) clumps of cells called adenomatous polyps(adenomatous polyposis).
Colon Cancer Prognosis
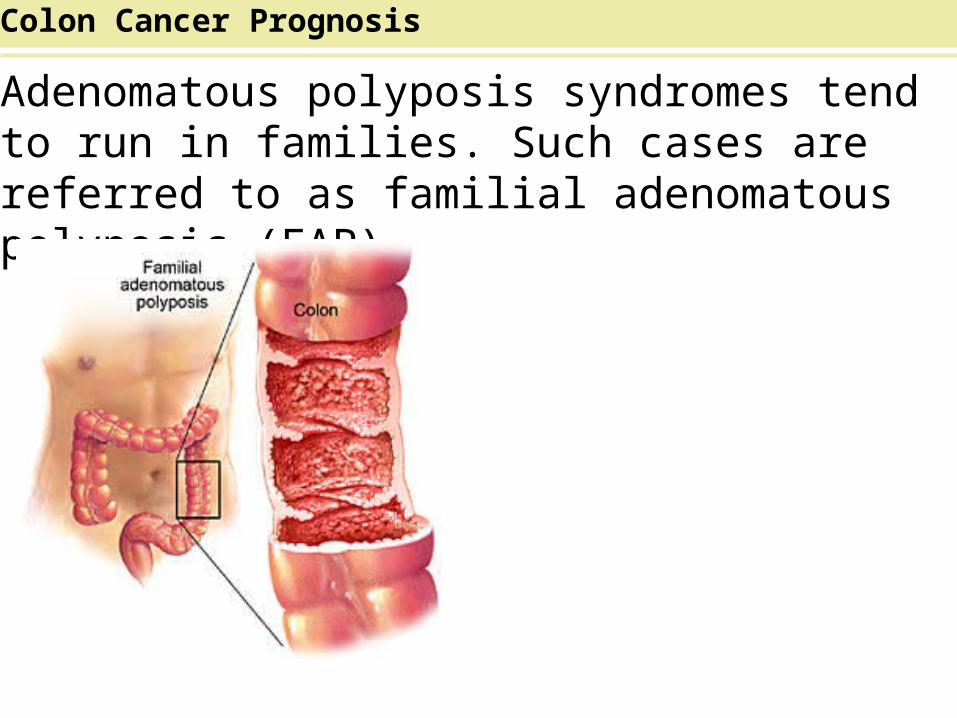
Adenomatous polyposis syndromes tend to run in families. Such cases are referred to as familial adenomatous polyposis (FAP).
Colon Cancer Prognosis
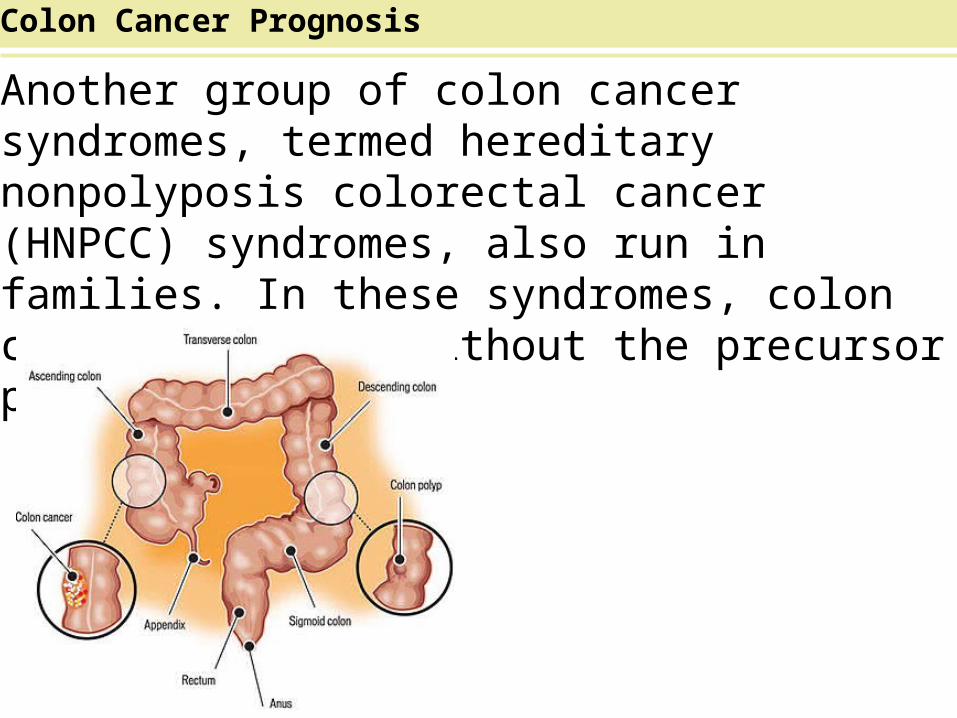
Another group of colon cancer syndromes, termed hereditary nonpolyposis colorectal cancer (HNPCC) syndromes, also run in families. In these syndromes, colon cancer develops without the precursor polyps.
Colon Cancer Prognosis

Polyps may be small and due to this reason, doctors recommend regular screening tests to help prevent colon cancer by identifying polyps before they become colon cancer.
Colon Cancer Prognosis
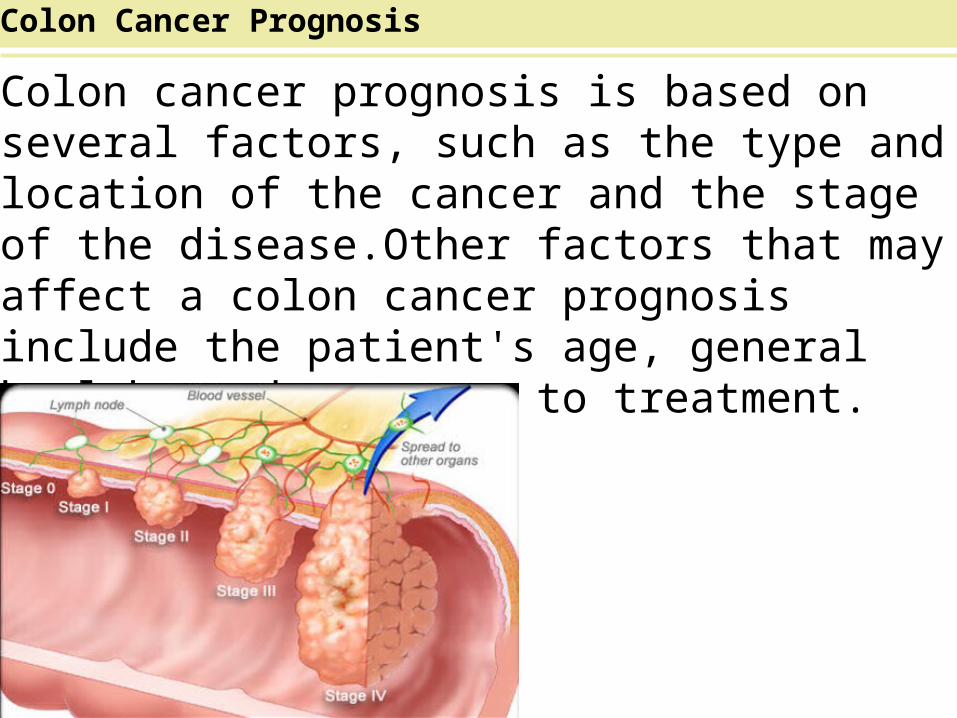
Colon cancer prognosis is based on several factors, such as the type and location of the cancer and the stage of the disease.Other factors that may affect a colon cancer prognosis include the patient's age, general health, and response to treatment.
Colon Cancer Prognosis
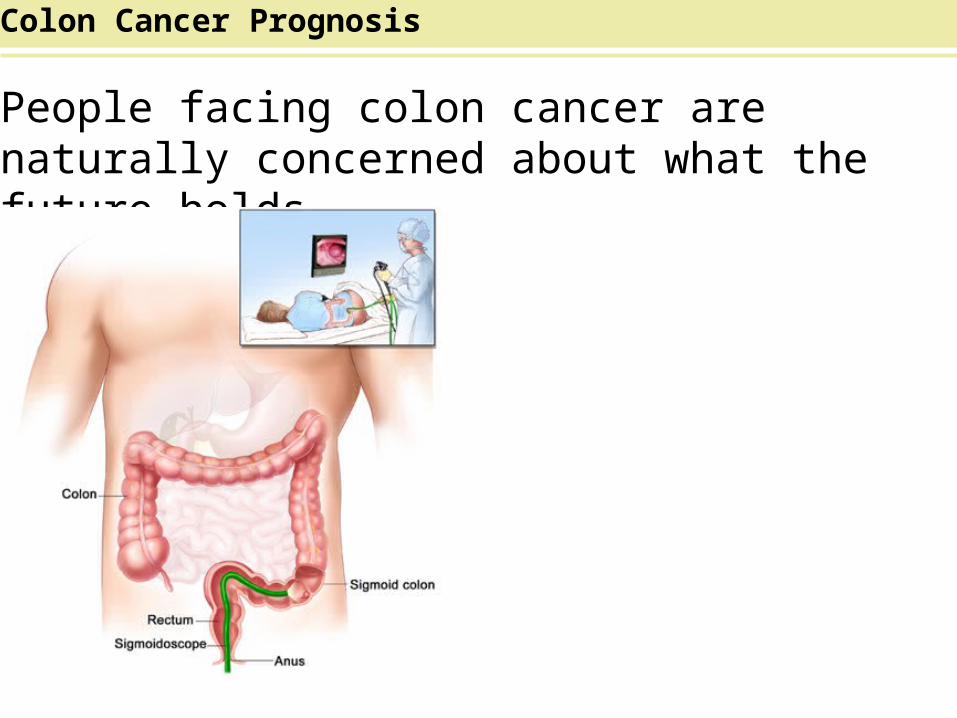
People facing colon cancer are naturally concerned about what the future holds.
Colon Cancer Prognosis

Understanding colon cancer and what to expect can help patients and their loved ones:
Colon Cancer Prognosis
Related Documents











