Cognitive outcome of parietooccipital resection in children with epilepsy *yzxSarah Lippe ´,*y{Christine Bulteau, *y{Georg Dorfmuller, **Franc ¸ois Audren, {Olivier Delalande, and *y{yyIsabelle Jambaque ´ *Inserm, U663, Paris, France, University Paris Descartes, Faculty of Medicine, Paris, France; APHP, Necker Hospital, Paris, France; yFaculty of Medicine, Necker Hospital, University Paris Descartes, APHP, Paris, France; zCentre de Recherche CHU Ste, University of Montreal, Montreal, Quebec, Canada; xDe ´ partement de Psychologie, Centre de Recherche en Neuropsychologie et Cognition, Universite ´ de Montre ´ al, Montreal, Quebec, Canada; {Unite ´ de Neurochirurgie Pe ´ diatrique, Fondation Ophtalmologique A. de Rothschild, Paris, France; **Service d’Ophtalmologie Pe ´ diatrique Fondation Ophtalmologique A. de Rothschild, Paris, France; and yyLaboratoire de Psychologie et Neurosciences Cognitives (UMR CNRS 8189), Institut de Psychologie, Universite ´ Paris Descartes, Paris, France SUMMARY Purpose: We followed the neuropsychological develop- ment of five children who underwent unilateral neurosur- gery of the occipitoparietal lobes as a treatment for epilepsy caused by a developmental lesion (cortical dys- plasia). Methods: The follow-up period ranged from 3–7 years postsurgery. Results: Two participants had a verbal intelligence quo- tient (IQ) >100 and three had a verbal IQ between 65 and 80. All five children had abnormal nonverbal IQ and exhib- ited deficits related to visual attention, object recognition, and praxis. Nevertheless, our results suggest that brain plasticity after parietooccipital epilepsy surgery in young children allows for a schooling level of cognitive skills such as reading and arithmetic. Discussion: Although recovery for visual perceptual cog- nition was more limited than for verbal functions, long- term neuropsychological outcomes showed that early surgery for epilepsy offers the possibility of optimizing cognitive outcomes in children with posterior intractable epilepsies. KEY WORDS: Visuospatial, Plasticity, Neurosurgery. Neurosurgery is an accepted treatment for intractable partial epilepsy in pediatric and adult populations. It has been proven effective, particularly for intractable temporal lobe epilepsy (Olivier, 1992; Wiebe et al., 2001; JambaquȖ et al., 2007; Kim et al., 2008). In children, surgery for extra- temporal lobe epilepsy represents approximately 50% of procedures and has been shown successful in one-half to two-thirds of the cases (Wyllie et al., 1998; Cossu et al., 2008). The most frequent cause of surgically treated extra- temporal intractable epilepsy is cortical dysplasia, an early developmental malformation of the cortex (Wyllie et al., 1998; Janszky et al., 2000; Lortie et al., 2002; Lerner et al., 2009). A number of studies have reported that surgical treatment can improve cognitive prognosis in children with epilepsy (Bayard & Lassonde, 2001; Helmstaedter, 2004). Scores on attention and working memory, episodic memory tasks, and naming tests have been shown to improve (Gleissner et al., 2005; JambaquȖ et al., 2007), allowing for higher scholastic achievement. However, very few studies have measured the neuropsy- chological outcomes for surgery in parietal and occipital epilepsies (Smith & Billingsley, 2001). JambaquȖ et al. (1998) reported visual apperceptive agnosia with severe face recognition impairment, executive function deficits, and autistic symptoms in a 13-year-old girl who had under- gone a right occipital lobectomy for cortical dysplasia at age 7 years. Remarkably, her academic abilities in spelling, reading, and arithmetic were higher than her functional intelligence level, perhaps as a result of special abilities often encountered in patients with autism. Cohen et al. (2004) demonstrated brain reorganization of the visual word form area (VWFA) toward the right hemisphere in a young epileptic child operated at the age of 4 years for a Sturge- Weber syndrome in the left occipitotemporal lobe. Sinclair et al. (2005) reviewed the epileptic outcomes of nine children with parietal resections and six with occipital resections. Although cognitive outcome was not addressed, Accepted April 29, 2010; Early View publication June 18, 2010. Address correspondence to Sarah LippȖ, PhD, Professeure Adjointe/ Assistant Professor, DȖpartement de psychologie/Department of Psychol- ogy, UniversitȖ de MontrȖal/University of Montreal, C.P. 6128, Succursale Centre-Ville, MontrȖal, QC, H3C 3J7 Canada. E-mail: sarah.lippe@ umontreal.ca Wiley Periodicals, Inc. ª 2010 International League Against Epilepsy Epilepsia, 51(10):2047–2057, 2010 doi: 10.1111/j.1528-1167.2010.02651.x FULL-LENGTH ORIGINAL RESEARCH 2047

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cognitive outcome of parietooccipital resection in children
with epilepsy*yzxSarah Lippe, *y{Christine Bulteau, *y{Georg Dorfmuller, **Francois Audren,
{Olivier Delalande, and *y{yyIsabelle Jambaque
*Inserm, U663, Paris, France, University Paris Descartes, Faculty of Medicine, Paris, France; APHP, Necker Hospital, Paris, France;
yFaculty of Medicine, Necker Hospital, University Paris Descartes, APHP, Paris, France; zCentre de Recherche CHU Ste, University
of Montreal, Montreal, Quebec, Canada; xDepartement de Psychologie, Centre de Recherche en Neuropsychologie et Cognition,
Universite de Montreal, Montreal, Quebec, Canada;{Unite de Neurochirurgie Pediatrique, Fondation Ophtalmologique A. de
Rothschild, Paris, France; **Service d’Ophtalmologie Pediatrique Fondation Ophtalmologique A. de Rothschild, Paris, France; and
yyLaboratoire de Psychologie et Neurosciences Cognitives (UMR CNRS 8189), Institut de Psychologie,
Universite Paris Descartes, Paris, France
SUMMARY
Purpose: We followed the neuropsychological develop-
ment of five children who underwent unilateral neurosur-
gery of the occipitoparietal lobes as a treatment for
epilepsy caused by a developmental lesion (cortical dys-
plasia).
Methods: The follow-up period ranged from 3–7 years
postsurgery.
Results: Two participants had a verbal intelligence quo-
tient (IQ) >100 and three had a verbal IQ between 65 and
80. All five children had abnormal nonverbal IQ and exhib-
ited deficits related to visual attention, object recognition,
and praxis. Nevertheless, our results suggest that brain
plasticity after parietooccipital epilepsy surgery in young
children allows for a schooling level of cognitive skills such
as reading and arithmetic.
Discussion: Although recovery for visual perceptual cog-
nition was more limited than for verbal functions, long-
term neuropsychological outcomes showed that early
surgery for epilepsy offers the possibility of optimizing
cognitive outcomes in children with posterior intractable
epilepsies.
KEY WORDS: Visuospatial, Plasticity, Neurosurgery.
Neurosurgery is an accepted treatment for intractablepartial epilepsy in pediatric and adult populations. It hasbeen proven effective, particularly for intractable temporallobe epilepsy (Olivier, 1992; Wiebe et al., 2001; Jambaqu�et al., 2007; Kim et al., 2008). In children, surgery for extra-temporal lobe epilepsy represents approximately 50% ofprocedures and has been shown successful in one-half totwo-thirds of the cases (Wyllie et al., 1998; Cossu et al.,2008). The most frequent cause of surgically treated extra-temporal intractable epilepsy is cortical dysplasia, an earlydevelopmental malformation of the cortex (Wyllie et al.,1998; Janszky et al., 2000; Lortie et al., 2002; Lerner et al.,2009).
A number of studies have reported that surgical treatmentcan improve cognitive prognosis in children with epilepsy
(Bayard & Lassonde, 2001; Helmstaedter, 2004). Scores onattention and working memory, episodic memory tasks, andnaming tests have been shown to improve (Gleissner et al.,2005; Jambaqu� et al., 2007), allowing for higher scholasticachievement.
However, very few studies have measured the neuropsy-chological outcomes for surgery in parietal and occipitalepilepsies (Smith & Billingsley, 2001). Jambaqu� et al.(1998) reported visual apperceptive agnosia with severeface recognition impairment, executive function deficits,and autistic symptoms in a 13-year-old girl who had under-gone a right occipital lobectomy for cortical dysplasia at age7 years. Remarkably, her academic abilities in spelling,reading, and arithmetic were higher than her functionalintelligence level, perhaps as a result of special abilitiesoften encountered in patients with autism. Cohen et al.(2004) demonstrated brain reorganization of the visual wordform area (VWFA) toward the right hemisphere in a youngepileptic child operated at the age of 4 years for a Sturge-Weber syndrome in the left occipitotemporal lobe. Sinclairet al. (2005) reviewed the epileptic outcomes of ninechildren with parietal resections and six with occipitalresections. Although cognitive outcome was not addressed,
Accepted April 29, 2010; Early View publication June 18, 2010.Address correspondence to Sarah Lipp�, PhD, Professeure Adjointe/
Assistant Professor, D�partement de psychologie/Department of Psychol-ogy, Universit� de Montr�al/University of Montreal, C.P. 6128, SuccursaleCentre-Ville, Montr�al, QC, H3C 3J7 Canada. E-mail: [email protected]
Wiley Periodicals, Inc.ª 2010 International League Against Epilepsy
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x
FULL-LENGTH ORIGINAL RESEARCH
2047

occipital lobe patients showed visual field losses. Focusingon the possibility of generalized impairments, Gleissneret al. (2008) assessed 15 children with parietal lobe epi-lepsy. One year after surgery, these children were seizure-free with postoperative improvements in attention andbehavior, but they showed a decrease in performance intelli-gence quotient (IQ).
In the present study, we assessed the long-term cognitiveoutcome—from 3–7 years postsurgery—of occipitoparietalepilepsy in five children who showed early onset due toTaylor-type focal cortical dysplasia. Neurosurgical resec-tion involved the occipital lobe and temporal or parietal lobejunctions. Neuropsychological assessment specifically tar-geted the cognitive functions of the posterior regions of thebrain. Although the occipital lobe is mainly responsible forvisual perception and discrimination, the parietal lobe isimportant for visuospatial orientation, attention, saccades,numerical cognition, grapheme–phoneme transcoding, esti-mating time and quantities, and praxis (Leff et al., 2001;Hubbard et al., 2005; Pouthas et al., 2005; Cavanna &Trimble, 2006). Occipitotemporal areas are involved incolor, object, and face recognition; reading; and other func-tions (Dehaene et al., 2001; Casarotto et al., 2008). In bothchildren and adults, the impact of a lesion in the occipitaland parietal lobes can result in visual agnosia, neglect, vi-suospatial disorientation, alexia, sensorial extinction, andGerstmann syndrome (Laurent-Vannier et al., 2003). Giventhe early maturation of the posterior areas of the brain, wepredicted reduced recovery of visuospatial abilities as com-pared to language development. Within the posteriorregions, we also hypothesized that lesion type and location(right- or left-sided resection) would differentially impactcognitive function, given that the right and left hemispheresshow distinct preferences for Gestalt versus analytical pro-cessing (Van Kleeck & Kosslyn, 1989). We posited thatneurodevelopmental lesions, such as cortical dysplasia andearly onset epilepsy, would entail reduced recovery ofvisuoperceptual cognition compared to verbal function.Because the literature reports of long-term follow-up inchildren with postoperative occipitoparietal epilepsy arescarce, our neuropsychological case descriptions from 3–7 years postsurgery focused on visuospatial abilities andscholastic skills such as reading and arithmetic.
Methods
ParticipantsEleven children with medically refractory epilepsy
underwent surgical resection of the posterior region of thebrain at the Fondation Ophtalmologique Rothschild de Paris(France) between 1999 and 2007 (Figs S1 and S2). Childrenwere selected based on age at surgery (£7 years of age), cur-rent age (between 8 and 12 years), and postoperative status(seizure-free or greatly improved). Five children fulfilledthe inclusion criteria and agreed to participate in the study.
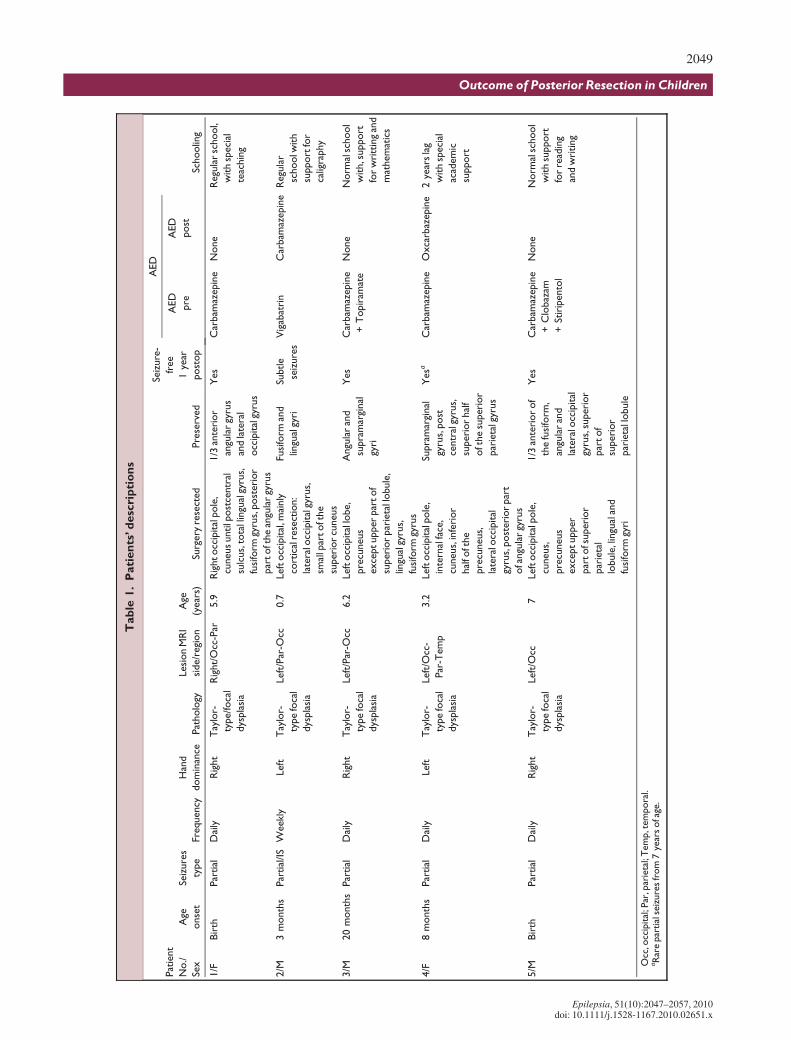
The project was approved by the Paediatric Neuro-surgery Committee of the Fondation Ophtalmologique deRothschild. Both parents and children gave informed con-sent. We reviewed preoperative and postoperative clinicalinvestigations, which included intracranial video-electroen-cephalography (video-EEG), magnetic resonance imaging(MRI), and IQ findings from Wechsler or developmentalscales. Clinical information for each patient is detailed inTable 1 and in the individual case descriptions.
ProceduresThe follow-up period ranged from 3–7 years. All children
underwent a neuroophthalmologic and comprehensive neu-ropsychological evaluation, designed to assess cognitivefunctions related to the posterior region of the brain. Verbaland nonverbal intellectual functions were evaluated preop-eratively and postoperatively on Wechsler or developmentalscales (Table 2). Postoperatively, more extensive neuropsy-chological and ophthalmologic evaluations were performed.The neuroophthalmologic evaluation included visual acuityand the Goldmann visual field examination. We used stan-dardized tests to assess the following five subdomains ofnonverbal cognition: basic visual discrimination, visualattention, visual recognition, spatial perception, and praxis.In addition, we evaluated working memory, executive func-tions, and academic skills such as reading and numericalcognition.
Screening tests from the Visual Object and Space Percep-tion (VOSP) battery (Warrington & James, 1991) were usedto assess the basic visual discrimination level of each child.We measured visual attention with cancellation tasks: theNEPSY Visual Attention Task (Korkman et al., 1998) andthe Bell test from the Batterie d’�valuation de la n�gligenceunilat�rale du Geren (BEN) (Rousseaux et al., 2001). Sub-tests for eye and head deviation, extinction, and line bisec-tion were used from the Batterie to assess symptoms ofneglect. Visual recognition was tested through naming anddesignation of objects (Jambaqu� & Dellatolas, 2000), dis-crimination of overlapping and embedded figures (Ghent,1956), and recognition of degraded figures (Gestalt closure)(Kaufman & Kaufman, 1983). For facial recognition, weused the short form of the Benton Facial Recognition Test(Benton, 1983a).
We evaluated spatial perception using the NEPSYArrows subtest (Korkman et al., 1998) and the BentonJudgement of Line Orientation Test (JLOT) (Benton,1983a; Benton et al., 1983b), with children’s norms(Lindgren & Benton, 1980). To measure visuoconstructiveabilities and praxis, we used the Rey Complex Figure Test(Rey, 1959) and NEPSY Hand Movements and VisuomotorPrecision subtests.
Reading was assessed by subtests from two batteries: theTest de l'Alouette (Lefavrais, 1967) and the Outil de D�pi-stage des Dyslexies (ODEDYS) (Neurocognition, 2002).In both cases, accuracy and speed were measured.
2048
S. Lippe et al.
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x
Tab
le1.
Pati
en
ts’d
esc
rip
tio
ns
Pat
ient
No./
Sex
Age
onse
t
Seiz
ure
s
type
Frequency
Han
d
dom
inan
cePat
holo
gy
Lesi
on
MR
I
side/r
egi
on
Age
(year
s)Su
rgery
rese
cted
Pre
serv
ed
Seiz
ure
-
free
1ye
ar
post
op
AED
Schoolin
g
AED
pre
AED
post
1/F
Bir
thPar
tial
Dai
lyR
ight
Tay
lor-
type/
foca
l
dys
pla
sia
Rig
ht/
Occ
-Par
5.9
Rig
htocc
ipital
pole
,
cuneus
untilp
ost
centr
al
sulc
us,
tota
llin
gual
gyru
s,
fusi
form
gyru
s,post
eri
or
par
toft
he
angu
lar
gyru
s
1/3
ante
rior
angu
lar
gyru
s
and
late
ral
occ
ipital
gyru
s
Yes
Car
bam
azepin
eN
one
Regu
lar
school,
with
speci
al
teac
hin
g
2/M
3m
onth
sPar
tial
/IS
Week
lyLef
tT
aylo
r-
type
foca
l
dys
pla
sia
Left
/Par
-Occ
0.7
Left
occ
ipital
,mai
nly
cort
ical
rese
ctio
n:
late
ralo
ccip
ital
gyru
s,
smal
lpar
toft
he
super
ior
cuneus
Fusi
form
and
lingu
algy
ri
Subtle
seiz
ure
s
Vig
abat
rin
Car
bam
azepin
eR
egu
lar
schoolw
ith
support
for
calig
raphy
3/M
20
month
sPar
tial
Dai
lyR
ight
Tay
lor-
type
foca
l
dys
pla
sia
Left
/Par
-Occ
6.2
Left
occ
ipital
lobe,
pre
cuneus
exce
ptupper
par
tof
super
ior
par
ieta
llobule
,
lingu
algy
rus,
fusi
form
gyru
s
Angu
lar
and
supra
mar
ginal
gyri
Yes
Car
bam
azepin
e
+T
opir
amat
e
None
Norm
alsc
hool
with,s
upport
for
wri
ttin
gan
d
mat
hem
atic
s
4/F
8m
onth
sPar
tial
Dai
lyLef
tT
aylo
r-
type
foca
l
dys
pla
sia
Left
/Occ
-
Par
-Tem
p
3.2
Left
occ
ipital
pole
,
inte
rnal
face
,
cuneus,
infe
rior
hal
foft
he
pre
cuneus,
late
ralo
ccip
ital
gyru
s,post
eri
or
par
t
ofa
ngu
lar
gyru
s
Supra
mar
ginal
gyru
s,post
centr
algy
rus,
superi
or
hal
f
oft
he
super
ior
par
ieta
lgyr
us
Yesa
Car
bam
azepin
eO
xca
rbaz
epin
e2
year
sla
g
with
speci
al
acad
em
ic
support
5/M
Bir
thPar
tial
Dai
lyR
ight
Tay
lor-
type
foca
l
dys
pla
sia
Left
/Occ
7Left
occ
ipital
pole
,
cuneus,
pre
cuneus
exce
ptupper
par
tofs
uper
ior
par
ieta
l
lobule
,lin
gual
and
fusi
form
gyri
1/3
ante
rior
of
the
fusi
form
,
angu
lar
and
late
ralo
ccip
ital
gyru
s,su
per
ior
par
tof
superi
or
par
ieta
llobule
Yes
Car
bam
azepin
e
+C
lobaz
am
+St
irip
ento
l
None
Norm
alsc
hool
with
support
for
read
ing
and
wri
ting
Occ
,occ
ipital
;Par
,par
ieta
l;T
em
p,t
em
pora
l.aR
are
par
tial
seiz
ure
sfr
om
7ye
ars
ofa
ge.
2049
Outcome of Posterior Resection in Children
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x

Numerical cognition was evaluated by the Zareki-R bat-tery of scores (2006), which includes assessment of visualcounting, mental counting, number writing, number read-ing, oral mental calculation, visual quantity estimation, andverbal contextual estimation.
Visual span and working memory were tested with theWechsler Intelligence Scale for Children – Fourth Edition(WISC-IV) Integrated Spatial Span subtest. Auditory atten-tion and working memory were tested further by compari-son to visual tasks, using the NEPSY Auditory Attentionand the WISC-IV Integrated Digit Span tests. Executivefunction was assessed through the NEPSY Tower subtest,and behavior was evaluated on the Child Behaviour CheckList (CBCL) questionnaire (Achenbach, 1991) filled out bythe parents.
Standardized neuropsychological test scores were classi-fied into two categories, according to the mean and standarddeviation (SD) of each test: 1.5 SD below the mean wasqualified as a ‘‘deficit,’’ whereas 1.0 SD above or below themean were qualified as ‘‘average.’’ With some exceptions, apathological threshold was used: for the Benton Facial Rec-ognition Test, this was more than two points from the mean(Benton), and for the embedded figures task, two omissions(Ghent, 1956). For the scoring of the BEN subtests (Belltest, Eye and Head Deviation, Extinction and Line Bisec-tion), young adult norms were used as a guideline (Rous-seaux et al., 2001). Finally, T scores above 60 on the CBCLquestionnaire (Achenbach, 1991) were rated pathological.
Results
Preoperative data and type of surgeryAll five children experienced seizure onset in the early
months of life, characterized by various types of clinicalocular manifestations. The seizures were stereotypic par-tial seizures beginning with a conjugate gaze deviation ora strabismus followed by ocular clonus; one child (Patient2) presented infantile spasms, which were well controlledby Vigabatrin. MRI lesions were visible in the occipitallobe in all children (Patients 1–5) as well as in the parietallobe in three (Patients 1–3) and in the temporoparietaljunction in one (Patient 4). Only one child, Patient 1, had
a right hemisphere lesion. In four children, between 20and more than 100 seizures were recorded during theperiod of intracranial video-EEG monitoring, whereasone patient, Patient 2, presented with only two seizures.The preoperative IQ scores revealed a range from milddeficit (Patient 1) to mental delay (Patients 3 and 5), andautistic features in one patient (Patient 4). All childrenexhibited poor visual perception and recognition in every-day life. The posterior part of the occipitotemporal gyruswas included in the occipital and posterior parietal loberesections (Figs S1 and S2) in all participants but one(Patient 2) (Tables 1 and 2) .
Cognitive outcomePostoperatively, all children improved their intellectual
abilities, but with significant differences between verbaland nonverbal components (see Table 2 and detaileddescription). Although all nonverbal IQs were abnormaland three children had a verbal IQ below 80, two had verbalIQs above 100. Parental rating of behavior (on the CBCLquestionnaire) was average for four of the five children.Nevertheless, behavioral difficulties were observed duringour evaluations and are reported in the case descriptions.
All participants displayed normal visual discrimination(VOSP). However, all performed at least 1.5 SD below themean on object naming (DEN-48), visuomotor praxis (handmovements), and regular word reading (ODEDYS-time)tasks (Table 3). Four of the five children performed at least1.5 SD below the mean on visual attention tests (Bell andNEPSY), visual perceptual integration skills (degradedforms Kaufman Assessment Battery for Children [K-ABC]),embedded figure discrimination (Ghent), face recognition(Benton), visuospatial orientation (Benton JLOT andNEPSY Arrows), visuoconstructive praxis (Rey figure),visuomotor precision (NEPSY), and irregular word readingand pseudo-word reading time (ODEDYS) (Table 1).
On the other hand, only Patient 4 did not show normalauditory attention and planning abilities (NEPSY AuditoryAttention and NEPSY Tower, SD < )1.5). The two chil-dren with normal verbal IQ (Patients 1 and 2) performedabove the mean on the planning task. Numerical abilitiessuch as number reading and writing, counting, and verbal
Table 2. Pre- and postsurgery IQ scores
Patients No./Sex
Preoperative
Age (years)
Intellectual functioning
VIQ/PIQ
Postoperative
Age (years)
Intellectual level
VIQ/PIQ
1/F 3.5 73/66 6.7 109/60
2/M ND 3.4 103/66
3/M 5.1 63/48 6.7 78/45
4/F 1.8 53a 9.2 68/54
5/M 4.8 49/57 7.8 69/55
ND, not done; VIQ, Verbal Intelligence Quotient; PIQ, Performance Intelligence Quotient.aGlobal Developmental Quotient (French Gesell scale adaptation).
2050
S. Lippe et al.
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x
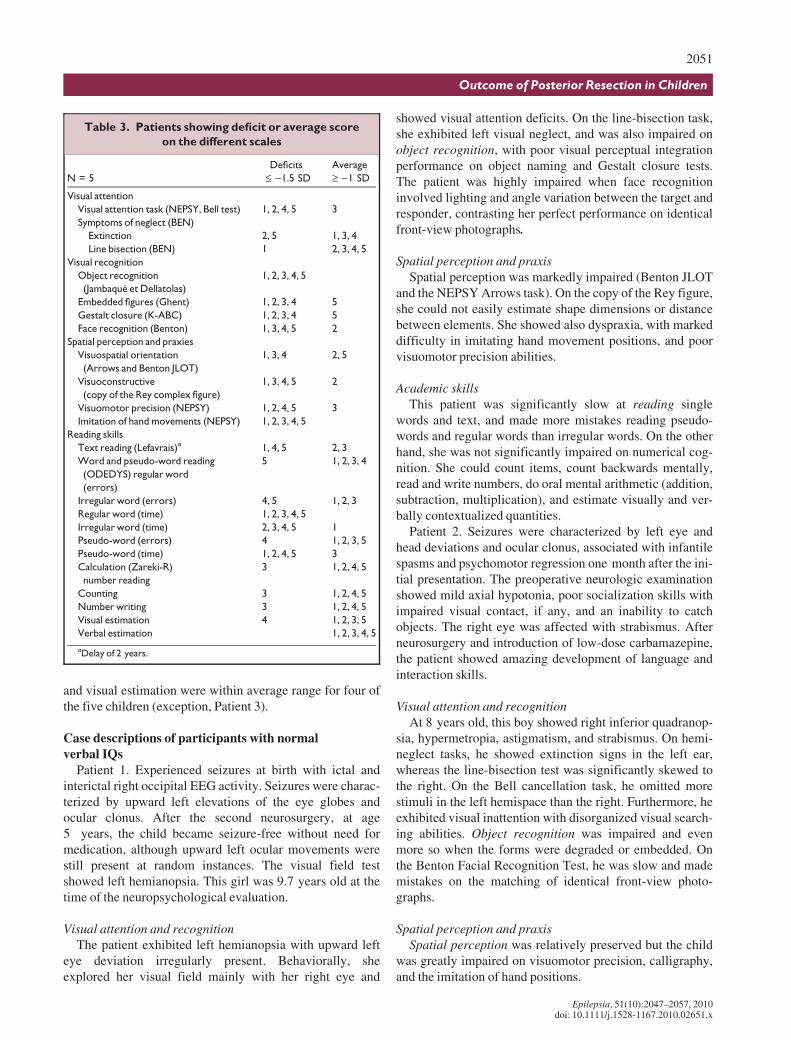
and visual estimation were within average range for four ofthe five children (exception, Patient 3).
Case descriptions of participants with normalverbal IQs
Patient 1. Experienced seizures at birth with ictal andinterictal right occipital EEG activity. Seizures were charac-terized by upward left elevations of the eye globes andocular clonus. After the second neurosurgery, at age5 years, the child became seizure-free without need formedication, although upward left ocular movements werestill present at random instances. The visual field testshowed left hemianopsia. This girl was 9.7 years old at thetime of the neuropsychological evaluation.
Visual attention and recognitionThe patient exhibited left hemianopsia with upward left
eye deviation irregularly present. Behaviorally, sheexplored her visual field mainly with her right eye and
showed visual attention deficits. On the line-bisection task,she exhibited left visual neglect, and was also impaired onobject recognition, with poor visual perceptual integrationperformance on object naming and Gestalt closure tests.The patient was highly impaired when face recognitioninvolved lighting and angle variation between the target andresponder, contrasting her perfect performance on identicalfront-view photographs.
Spatial perception and praxisSpatial perception was markedly impaired (Benton JLOT
and the NEPSY Arrows task). On the copy of the Rey figure,she could not easily estimate shape dimensions or distancebetween elements. She showed also dyspraxia, with markeddifficulty in imitating hand movement positions, and poorvisuomotor precision abilities.
Academic skillsThis patient was significantly slow at reading single
words and text, and made more mistakes reading pseudo-words and regular words than irregular words. On the otherhand, she was not significantly impaired on numerical cog-nition. She could count items, count backwards mentally,read and write numbers, do oral mental arithmetic (addition,subtraction, multiplication), and estimate visually and ver-bally contextualized quantities.
Patient 2. Seizures were characterized by left eye andhead deviations and ocular clonus, associated with infantilespasms and psychomotor regression one month after the ini-tial presentation. The preoperative neurologic examinationshowed mild axial hypotonia, poor socialization skills withimpaired visual contact, if any, and an inability to catchobjects. The right eye was affected with strabismus. Afterneurosurgery and introduction of low-dose carbamazepine,the patient showed amazing development of language andinteraction skills.
Visual attention and recognitionAt 8 years old, this boy showed right inferior quadranop-
sia, hypermetropia, astigmatism, and strabismus. On hemi-neglect tasks, he showed extinction signs in the left ear,whereas the line-bisection test was significantly skewed tothe right. On the Bell cancellation task, he omitted morestimuli in the left hemispace than the right. Furthermore, heexhibited visual inattention with disorganized visual search-ing abilities. Object recognition was impaired and evenmore so when the forms were degraded or embedded. Onthe Benton Facial Recognition Test, he was slow and mademistakes on the matching of identical front-view photo-graphs.
Spatial perception and praxisSpatial perception was relatively preserved but the child
was greatly impaired on visuomotor precision, calligraphy,and the imitation of hand positions.
Table 3. Patients showing deficit or average score
on the different scales
N = 5
Deficits
£ )1.5 SD
Average
‡ )1 SD
Visual attention
Visual attention task (NEPSY, Bell test) 1, 2, 4, 5 3
Symptoms of neglect (BEN)
Extinction 2, 5 1, 3, 4
Line bisection (BEN) 1 2, 3, 4, 5
Visual recognition
Object recognition
(Jambaque et Dellatolas)
1, 2, 3, 4, 5
Embedded figures (Ghent) 1, 2, 3, 4 5
Gestalt closure (K-ABC) 1, 2, 3, 4 5
Face recognition (Benton) 1, 3, 4, 5 2
Spatial perception and praxies
Visuospatial orientation
(Arrows and Benton JLOT)
1, 3, 4 2, 5
Visuoconstructive
(copy of the Rey complex figure)
1, 3, 4, 5 2
Visuomotor precision (NEPSY) 1, 2, 4, 5 3
Imitation of hand movements (NEPSY) 1, 2, 3, 4, 5
Reading skills
Text reading (Lefavrais)a 1, 4, 5 2, 3
Word and pseudo-word reading
(ODEDYS) regular word
(errors)
5 1, 2, 3, 4
Irregular word (errors) 4, 5 1, 2, 3
Regular word (time) 1, 2, 3, 4, 5
Irregular word (time) 2, 3, 4, 5 1
Pseudo-word (errors) 4 1, 2, 3, 5
Pseudo-word (time) 1, 2, 4, 5 3
Calculation (Zareki-R)
number reading
3 1, 2, 4, 5
Counting 3 1, 2, 4, 5
Number writing 3 1, 2, 4, 5
Visual estimation 4 1, 2, 3, 5
Verbal estimation 1, 2, 3, 4, 5
aDelay of 2 years.
2051
Outcome of Posterior Resection in Children
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x

Academic skillsReading assessment showed that word reading was
slower than expected, but error rates were normal or betterthan average. Furthermore, text reading performance waswithin normal range. The child showed normal numericalcognition.
Case descriptions of participants with abnormalverbal IQ
Patient 3. This patient was 19 months old at epilepsyonset. The EEG showed ictal and interictal left occipitopa-rietal abnormal activity. At 5 years of age, this left-handedboy had permanent deviation of the right eye and tended notto sufficiently use the right side of his body. He exhibitedlanguage delay but was characterized by evident visualagnosia and dyspraxia. At 8 years 8 months of age, thepatient still showed a lack of behavioral control.
Visual attention and recognitionOphthalmologic examination showed a right eye devia-
tion, which was irregularly present. Assessed through can-cellation tasks, he exhibited visual attention difficulties witha similar number of omissions on each side of the hemi-space. In addition, he showed significant symptoms ofapperceptive agnosia. He could recognize identical figures,but object recognition, especially for degraded and embed-ded figures, was altered. He made mistakes on both semanti-colexical (e.g., stairs for ladder) and visual (e.g., caterpillarfor snail) levels. On the Benton Facial Recognition Test, thechild’s performance was also highly impaired.
Spatial perception and praxisVisuospatial orientation abilities as well as constructive
abilities were markedly defective.
Academic skillsReading abilities were relatively preserved for text. The
boy showed only a 1-year lag in reading speed for regular,irregular, and pseudo-words. Unlike other children in oursample, he was significantly impaired on numerical cogni-tion, although, especially number reading and writing.Many mistakes were visuospatial, for example, reading 305as 135, but other errors involved a misrepresentation ofnumerical knowledge (reading 138 as one thirteen eight;reading 6,485 as 74,895). Visual and verbal contextual esti-mation abilities, however, were normal.
Patient 4. The first neurologic examination found psycho-motor delay and abnormal eye movements. Seizuresoccurred with upward right elevations of the eye globes andbody, and the EEG showed ictal and interictal left occipitalactivity. Postoperative MRI revealed blurring of the white–gray matter junction over the left posterior temporal lobe,which extended anteriorly to the resection. The patient was11 years of age at the time of the neuropsychological evalu-ation.
Visual attention and recognitionOphthalmologic examination confirmed strabismus,
hypermetropia, and right hemianopsia. On cancellationtasks, the patient omitted a large number of items on the leftand right fields but was still able to explore the entire visualfield. She showed extinction phenomena only in the tactilemodality. This girl is the only child in our sample displayingaural–verbal as well as visual attention deficits. Visuospa-tial memory and verbal working memory were bothimpaired. Object recognition was altered (naming and des-ignation), mainly for degraded forms and embedded figures.Object-naming errors were mainly semantic (e.g., grippernamed as screwdriver). On the other hand, she could per-fectly recognize front-view photographs of the face but wasvery much impaired when skew and lighting conditionschanged.
Spatial perception and praxisThe patient showed impaired visuospatial abilities on the
Benton JLOT and the NEPSY Arrows task. The copy of theRey figure was segmented and she could not estimate thedimensions of shapes or the distances between elements.The child exhibited marked impairment during hand move-ment and visuomotor precision tasks.
Academic skillsThis girl showed the greatest reading deficits of all the
participants, as she was significantly slow at reading singlewords and text. Furthermore, the number of mistakes wassimilar whether she was reading regular words, irregularwords, or pseudo-words. She made visual, phonologic, andregularization mistakes. On the other hand, she was not sig-nificantly impaired on numerical cognition. She could countitems, read and write numbers, and estimate verbally con-textualized quantities. However, the visual quantities esti-mation task was riddled with attention difficulties; in fact,this patient showed hyperactivity and lack of behavioralcontrol.
Patient 5. Preoperatively, the EEG revealed ictal and inte-rictal left parietooccipital abnormal activity. Seizuresoccurred with left upward eye movements and ocular clo-nus. At the age of 2 years, the child had mild psychomotordelay and interacted poorly with his mother. Behavioral dif-ficulties related to food, with signs of anorexia. Two neuro-surgeries were needed to obtain freedom from seizures. Theboy was 10 years and 8 months old at the time of the neuro-psychological evaluation.
Visual attention and recognitionThe ophthalmologic examination showed right hemia-
nopsia, but the patient compensated well. Although heshowed right visual extinction when stimulated bilaterally,he had a lesser level of visual attention deficit than the otherchildren in the sample. Visuospatial working memory waswithin average. However, this boy could not name objects
2052
S. Lippe et al.
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x

properly despite preserved visual perceptual integrationabilities. He could recognize front-view photographs offaces, but was impaired when lighting and skew variedbetween the target and the responder.
Spatial perception and praxisThe patient showed well-preserved visuospatial orienta-
tion abilities but poor spatial construction abilities. He alsowas affected with dyspraxia, poor imitation of hand posi-tions, and visuomotor imprecision.
Academic skillsThis patient was one of the most impaired in reading
skills, being significantly slow at single words and text.Errors were made while reading pseudo-words, regularwords, and irregular words, making visual mistakes 28% ofthe time. On the other hand, numerical cognition tasks wereeasily performed. Assessed by NEPSY tests, auditory atten-tion was within average, but digit span and verbal workingmemory were diminished.
Discussion
All children experienced seizure onset before 2 years ofage. After surgery, three children were seizure-free and offmedication, whereas the remaining two showed infrequentseizure reoccurrence and received one antiepileptic drug.Four of five children attained normal schooling level. Ver-bal IQ was improved by up to 35 points after the surgery. Asin children with Sturge-Weber syndrome with drug-resistantepilepsy, the control of epilepsy and reduction of pharmaco-therapy may have prevented severe cognitive impairments(Sujansky & Conradi, 1995). Three to seven years postoper-atively, all children showed significant discrepanciesbetween verbal and nonverbal IQs. Although two of fivechildren displayed normal verbal IQ, all were moderatelyimpaired on nonverbal IQ. Our observations are in concor-dance with the significant postsurgery difference betweenverbal and nonverbal IQ reported in adults with posteriorresections, regardless of side of surgery or visual field loss(Luerding et al., 2004).
Our neuropsychological evaluation suggests that a historyof early severe epilepsy with a focal cortical dysplasia fol-lowed by surgical resection will have an impact on the cor-responding visual, spatial, and academic cognitive abilities.All five children showed cognitive deficits related to visualattention, object recognition, praxis, and reading speed.
Visual attention and recognitionThe posterior parietal lobe is considered to have a special
role in spatial functions (Nachev & Husain, 2006). Indeed,visual spatial attention was impaired in all five children.Subregions such as the temporoparietal junctions areinvolved in the spatial attention network (Mesulam, 1981;Vallar et al., 1993). They are strongly associated with
neglect syndrome, an attention deficit disorder that causespatients to demonstrate pathologic bias for ipsilesionalitems, neglecting the contralateral ones (Mattingley et al.,1997). The one child with a right-sided lesion (Patient 1)was the most impaired on spatial attention and showed signsof neglect. Our observations are consistent with those ofrecent studies reporting that the right temporoparietal junc-tion, part of which had been resected in Patient 1, is relatedto the network involved in reorienting behaviors followingattentional capture by other stimuli (Corbetta & Shulman,2002; Mitchell, 2008). In addition, neglect has recently beendescribed in children with left and right parietal acquiredlesions (Laurent-Vannier et al., 2003). In our sample, onlyPatient 1 with a right occipitoparietal lesion showed neglectof the contralateral hemispace. With regard to developmen-tal lesions, our results do not confirm the previously prevail-ing hypothesis of more frequent spatial neglect of the righthemispace in very young children (Laurent-Vannier et al.,2003; Trauner, 2003).
Most children were impaired on degraded object recogni-tion or object naming. Object recognition is known toinvolve the lateral occipital and the fusiform cortex bilater-ally (Eger et al., 2004, 2007; Pegna et al., 2004) and to bemodulated by top-down processes by the frontoparietal net-work. Children were unable to recognize or name an objectwithout contextual cues, which suggests that recoveredbrain processes related to seizure freedom and/or brain plas-ticity failed to completely compensate for the unilateral pos-terior lesions. Interestingly, the one child who couldaccurately identify degraded objects had the lateral occipitalcortex (LOC) preserved out of his left lesion (Patient 5),whereas the analogous LOC-sparing surgery in a right hemi-sphere lesion still impaired the child on the same task(Patient 1). The right hemisphere is typically associatedwith spatial transformation of a mental Gestalt, a processlikely to be involved in degraded object recognition tasks(Warrington & James, 1991; Humphreys et al., 1992). Ourobservations, therefore, confirm the bilateral LOC role inobject recognition.
Facial recognition, tested using the Benton Facial Recog-nition Test, was impaired in four of the five children. Thetask is separated into two parts. Only the first part does notrequire visuospatial skills, as it shows front-view photo-graphs; the second part shows the angles and lighting in adifferent view. The lesions and cognitive difficulties experi-enced by the subject are reflected in corresponding deficitson the first or second part of the task. For example, the onlychild showing normal performance on orientation tasks (apatient with a small lateral resection in the left hemisphere),made mistakes on the first section but very few on the sec-ond. In contrast, the most impaired child on orientationtasks, with a median right hemisphere resection, showed aperfect performance on the first part, but a worse perfor-mance on the second part of the test. Other reports on facialperception have revealed limited postlesional plasticity in
2053
Outcome of Posterior Resection in Children
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x

the pediatric population resulting from both right and leftlesions (Mancini et al., 1994; de Schonen et al., 2005). Ourstudy supports the heterogeneity of the mechanisms relatedto developmental prosopagnosia (Duchaine & Nakayama,2006).
Spatial perception and praxisAll children showed dyspraxia, ranging from movement
imitations to constructions. Movement imitation is thoughtto involve a complex network in the frontal and parietalregions (Iacoboni et al., 1999; Shmuelof & Zohary, 2007).Authors have proposed that the anterior intraparietal area isinvolved in a kinesthetic copy of the movements to be usedduring action execution (Iacoboni et al., 1999), whereas theinferior parietal lobule is associated with body schemaknowledge (Berlucchi & Aglioti, 1997). Although the ante-rior intraparietal area was not altered in most of our chil-dren, the epilepsy and the resections, with the inferiorparietal lobe partially resected in most children, must haveproduced a disconnect in the neural network that preventedthem from performing accurate gesture imitations. Asexpected, visuomotor precision and complex figure copyingwere impaired, being associated with a number of brainareas in the frontal, parietal, and occipital lobes bilaterally,such as the cuneus (Tzagarakis et al., 2009), which had beenresected in most children in our sample.
Academic skills
Reading speedAll children were impaired with regard to reading speed.
Reading is a complex task involving an extended network.Word recognition has recently been strongly associated withthe ventral stream, where a functional specialization forrecurrent spelling patterns was found in the left occipitotem-poral sulcus, named the visual word form area (VWFA)(Cohen et al., 2003; Marinkovic et al., 2003; McCandlisset al., 2003; Binder et al., 2006; Gaillard et al., 2006). Thedorsal stream is thought to be involved in word recognition,when serial reading ensues from degraded special propertiesof words or spatial rearrangement of letters (Gitelman et al.,2005; Vinckier et al., 2006; Cohen et al., 2008). Graph-eme–phoneme conversion and semantic processing ofwords involve left temporal and frontal regions of the brain(Simos et al., 2002; Mechelli et al., 2005).
The two most impaired children had lesions spread overthe left ventral stream (Patients 3 and 5). Patient 3 had anextensive left dysplasia and Patient 5 had a resection of theleft fusiform gyrus (including the VWFA) at 7 years of age.Indeed, plasticity may have been limited in Patient 5 by vir-tue of age and the fact that he had acquired a level of readingexpertise before the surgery. The two children with the leastimpaired reading speed had very distinct lesions. Patient 4had extensive left dysplasia combined with a resected fusi-form gyrus, whereas Patient 2 had a small neurosurgery with
preserved left fusiform gyrus. Cohen et al. (2004) reportedhemispheric shift for reading but not for language in a childof preschool age at the time of left occipital resection. InPatient 4, the large left hemispheric dysplasia, the earlyresection (6 years of age), and early seizure freedom andreduction of pharmacotherapy could have resulted in brainreorganization toward the right hemisphere allowing for acertain level of reading. In all cases, it is possible that visualfield loss may have altered the saccade movements, causinga reduction in reading speed. Inefficient fixation duringreading has been described in hemianoptic patients6 months after the acquired lesion (McDonald, 2006).Although it should be considered for the two least impairedchildren, who mainly showed alteration in reading speedinstead of accuracy, this alternative explanation cannot holdtrue in the most impaired children because both accuracyand reading speed were impaired.
Although the impact of developmental lesions and neuro-surgery did not create alexia in any of the children, it didimpair all of them on word reading speed. Parietal regionsof the brain are involved in spatial attention processes, ori-enting and decoding letters and words, and consequently inearly learning of lexical functions. Epelbaum et al. (2008)showed that disconnecting the occipital cortex from theVWFA (by altering the inferior longitudinal fasciculus) wassufficient to provoke reading deficits. Therefore, it wouldseem that up to 7 years postsurgery, a right or left posteriorlesion of the extent seen in our subjects prevents the childfrom performing at normal reading capacity at school age,but does not prevent the individual from learning how toread.
Numerical cognitionNumerical cognition refers to processes such as subitiz-
ing (estimation for quantities lower than four), estimating,counting, calculating, and comparing quantities or numbers.Studies have demonstrated the role of a frontoparietal net-work for numerical cognition (Roland & Friberg, 1985;Dehaene et al., 1996). Within this network, the intraparietalsulcus regions, bilaterally, are specifically involved in mostnumerical cognition processes. In children, comparisontasks of Arabic numerals and color nonnumerical symbolsinduced bilateral intraparietal sulcus activity in normal chil-dren but not in children showing developmental dyscalculia(Mussolin et al., 2010). Only one child in our sample wasimpaired on numerical cognition, the one in whom thelargest part of the superior parietal lobule was resected(Patient 3). The child showed deficits in number reading,number writing, and dot counting. He did not show deficitson visual estimation, whereas the one child demonstratingdifficulties on the estimation tasks had an occipitotemporallesion (Patient 4). A plausible explanation is that the estima-tion task was modulated by spatial working memory(Culham & Kanwisher, 2001), which was altered in thelatter (Patient 4) but not the former (Patient 3).
2054
S. Lippe et al.
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x

Epilepsy
Side of surgeryOur sample allowed us to directly compare two chil-
dren with very early epilepsy onset and lesions of theoccipital-temporoparietal region, one in the left hemi-sphere (Patient 5) and one in the right (Patient 1). Bothchildren were impaired as to reading, but showed a doubledissociation in two aspects. First, although Patient 5 wassignificantly impaired on irregular word reading, Patient 1showed normal performance. The lexicosemantic pathnecessary for irregular word reading is thought to involvethe anterior part of the inferior frontal gyrus and of thefusiform gyrus (Mechelli et al., 2005), which had beenresected in Patient 5 but not in Patient 1. Lesioned in theleft hemisphere, Patient 5 was greatly impaired in lexicalknowledge. In contrast, Patient 1 was able to directly readwith the left hemisphere, where lexical knowledge is welldeveloped. Second, although Patient 1 showed significantpseudo-word reading errors, Patient 5 had normal perfor-mance. Words are first processed within each hemispherein the V4 area and then transferred through the corpuscallosum to the left hemisphere, in the VWFA, around thetemporooccipital sulcus (Cohen et al., 2000). Pseudo-wordreading may further involve the dorsal premotor cortex(Mechelli et al., 2005). Our results suggest that pseudo-word reading may in fact involve other networks,including the right hemisphere. Both the right and lefthemisphere fusiform gyri process newly presented words(Dehaene et al., 2001), and the posterior fusiform area hasbeen shown to correlate with the frontal region involvedin pseudo-word reading (dorsal premotor cortex) (Mechelliet al., 2005). We posit a right hemisphere contribution inthe early detection of pseudo-words that could mimicserial reading processes known to activate biparietalregions (Vinckier et al., 2006; Cohen et al., 2008).
In summary, our sample was too small to quantify cog-nitive outcome with respect to dysplastic tissue, localiza-tion, resection size, time of surgery, seizure freedom, andpharmacotherapy reduction. However, the visuospatialimpairment profile of our sample can be related to theneuroanatomic framework. We observed that the one child(Patient 2) showing the highest nonverbal IQ score wasalso the one with the smallest dysplastic tissue as visual-ized on MRI, had the least amount of resection, and wasoperated on at the youngest age. Indeed, this patientshowed a very good outcome considering the classic long-term prognosis of infantile spasms (Jambaqu� et al.,1993). Furthermore, the child showing the worst overallresults (Patient 4), including deficits in oral–verbal atten-tion, also showed the most extended dysplasia, involvingthe left temporal lobe. The other four patients may alsoshow residual nonepileptogenic dysplastic tissue not obvi-ous on MRI. In these cases, the dysplastic tissue may ormay not be cognitively functional (Janszky et al., 2000).
Patient 1, the only child with a right occipitoparietalresection, was the most impaired as concerns visual atten-tion, visuospatial orientation, simultagnosia, and visuospa-tial construction abilities. In contrast, Patient 5, with avery similar resection of the left occipitoparietal region,showed the least visual attention and visuospatial workingmemory difficulties, but was the most impaired on read-ing. Finally, the only patient in whom the resectioninvolved the left occipital-temporoparietal region (Patient3), including the superior parietal lobe, was the only oneto show numerical cognition impairments and had rela-tively preserved reading abilities.
From our small series, we can only convey that a numberof variables including dysplasia size, resection size, andlocation are important in predicting verbal and nonverbalcognitive outcomes. However, given that verbal IQimprovements occurred after surgery, we can ascertain abeneficial role for seizure freedom and antiepileptic drugreduction in verbal brain processing. The mechanismsresponsible for the visuospatial outcomes remain unclear.Whereas performance IQ did not significantly change afterthe surgery, the level of competence of each child is stillstriking when one considers the lesion sizes in some of thechildren. Possible recovery factors in visuospatial tasks mayinclude distinct cognitive strategies, brain reorganization,and normalized brain activity resulting from seizure free-dom and reduced medication.
One limitation of this study includes the fact that the moreextensive neuropsychological evaluation was conductedonly postoperatively. This limitation comes from the youngage of the patients included in this study. For future work,more comprehensive preoperative assessment could help inbetter characterizing their improvements or worsening aftersurgery.
In conclusion, early surgical intervention in children withposterior intractable epilepsies offers the possibility of opti-mizing cognitive outcome and quality of life. We believethat, in future, more attention should be paid to neuropsy-chological assessment of these patients to better understandtheir visual perceptive deficiencies and provide better clini-cal and psychological management.
Acknowledgments
This work was supported by the Canadian Institutes of HealthResearch (Lippe S) and Unit� de Neurochirurgie P�diatrique, FondationOphtalmologique A. de Rothschild, Paris, France Inserm UMR663. Epi-lepsies de l’enfant et plasticit� c�r�brale, Universit� Paris Descartes,Paris, France.
Disclosure
We confirm that we have read the journal’s position on issuesinvolved in ethical publication and affirm that this report is consistentwith those guidelines. None of the authors has any conflict of interest todisclose.
2055
Outcome of Posterior Resection in Children
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x

References
Achenbach T. (1991) Manual for the child behavior checklist/4–18and 1991 profile. Department of Psychiatry, University of Vermont,Burlington, VT.
Bayard S, Lassonde M. (2001) Cognitive, sensory and motor adjustment tohemispherectomy. In Jambaqu� I, Lassonde M, Dulac O (Eds) Neuro-psychology of childhood epilepsy. Kluwer Academic/Plenum Publish-ers, New York, pp. 229–245.
Benton A. (1983a) Facial recognition. Les Editions du Centre de Psycholo-gie Appliqu�e, Paris.
Benton A, Hamsher K, Varney NR, Spreen O. (1983b) Judgment line orien-tation form H. Contribution to neuropsychological assessment. OxfordUniversity Press, New York.
Berlucchi G, Aglioti S. (1997) The body in the brain: neural bases of corpo-real awareness. Trends Neurosci 20:560–564.
Binder JR, Medler DA, Westbury CF, Liebenthal E, Buchanan L. (2006)Tuning of the human left fusiform gyrus to sublexical orthographicstructure. Neuroimage 33:739–748.
Casarotto S, Bianchi AM, Ricciardi E, Gentili C, Vanello N, Guazzelli M,Pietrini P, Chiarenza GA, Cerutti S. (2008) Spatiotemporal dynamics ofsingle-letter reading: a combined ERP-FMRI study. Arch Ital Biol146:83–105.
Cavanna AE, Trimble MR. (2006) The precuneus: a review of its functionalanatomy and behavioural correlates. Brain 129:564–583.
Cohen L, Dehaene S, Naccache L, Lehericy S, Dehaene-Lambertz G,Henaff MA, Michel F. (2000) The visual word form area: spatial andtemporal characterization of an initial stage of reading in normalsubjects and posterior split-brain patients. Brain 123(Pt 2):291–307.
Cohen L, Martinaud O, Lemer C, Lehericy S, Samson Y, Obadia M, Sla-chevsky A, Dehaene S. (2003) Visual word recognition in the left andright hemispheres: anatomical and functional correlates of peripheralalexias. Cereb Cortex 13:1313–1333.
Cohen L, Lehericy S, Henry C, Bourgeois M, Larroque C, Sainte-Rose C,Dehaene S, Hertz-Pannier L. (2004) Learning to read without a leftoccipital lobe: right-hemispheric shift of visual word form area. AnnNeurol 56:890–894.
Cohen L, Dehaene S, Vinckier F, Jobert A, Montavont A. (2008) Readingnormal and degraded words: contribution of the dorsal and ventralvisual pathways. Neuroimage 40:353–366.
Corbetta M, Shulman GL. (2002) Control of goal-directed and stimulus-dri-ven attention in the brain. Nat Rev Neurosci 3:201–215.
Cossu M, Lo Russo G, Francione S, Mai R, Nobili L, Sartori I, Tassi L, Cit-terio A, Colombo N, Bramerio M, Galli C, Castana L, Cardinale F.(2008) Epilepsy surgery in children: results and predictors of outcomeon seizures. Epilepsia 49:65–72.
Culham JC, Kanwisher NG. (2001) Neuroimaging of cognitive functions inhuman parietal cortex. Curr Opin Neurobiol 11:157–163.
Dehaene S, Tzourio N, Frak V, Raynaud L, Cohen L, Mehler J, Mazoyer B.(1996) Cerebral activations during number multiplication and compari-son: a PET study. Neuropsychologia 34:1097–1106.
Dehaene S, Naccache L, Cohen L, Bihan DL, Mangin JF, Poline JB, RiviereD. (2001) Cerebral mechanisms of word masking and unconscious rep-etition priming. Nat Neurosci 4:752–758.
de Schonen S, Mancini J, Camps R, Maes E, Laurent A. (2005) Early brainlesions and face-processing development. Dev Psychobiol 46:184–208.
Duchaine BC, Nakayama K. (2006) Developmental prosopagnosia: a win-dow to content-specific face processing. Curr Opin Neurobiol 16:166–173.
Eger E, Henson RN, Driver J, Dolan RJ. (2004) BOLD repetition decreasesin object-responsive ventral visual areas depend on spatial attention. JNeurophysiol 92:1241–1247.
Eger E, Henson RN, Driver J, Dolan RJ. (2007) Mechanisms of top-downfacilitation in perception of visual objects studied by FMRI. Cereb Cor-tex 17:2123–2133.
Epelbaum S, Pinel P, Gaillard R, Delmaire C, Perrin M, Dupont S, DehaeneS, Cohen L. (2008) Pure alexia as a disconnection syndrome: new diffu-sion imaging evidence for an old concept. Cortex 44:962–974.
Gaillard R, Naccache L, Pinel P, Clemenceau S, Volle E, Hasboun D,Dupont S, Baulac M, Dehaene S, Adam C, Cohen L. (2006) Directintracranial, FMRI, and lesion evidence for the causal role of left infero-temporal cortex in reading. Neuron 50:191–204.
Ghent L. (1956) Perception of overlapping and embedded figures by chil-dren of different ages. Am J Psychol 69:575–587.
Gitelman DR, Nobre AC, Sonty S, Parrish TB, Mesulam MM. (2005) Lan-guage network specializations: an analysis with parallel task designsand functional magnetic resonance imaging. Neuroimage 26:975–985.
Gleissner U, Sassen R, Schramm J, Elger CE, Helmstaedter C. (2005)Greater functional recovery after temporal lobe epilepsy surgery in chil-dren. Brain 128:2822–2829.
Gleissner U, Kuczaty S, Clusmann H, Elger CE, Helmstaedter C. (2008)Neuropsychological results in pediatric patients with epilepsy surgeryin the parietal cortex. Epilepsia 49:700–704.
Helmstaedter C. (2004) Neuropsychological aspects of epilepsy surgery.Epilepsy Behav 5(suppl 1):S45–S55.
Hubbard EM, Piazza M, Pinel P, Dehaene S. (2005) Interactions betweennumber and space in parietal cortex. Nat Rev Neurosci 6:435–448.
Humphreys GW, Riddoch MJ, Quinlan PT, Price CJ, Donnelly N. (1992)Parallel pattern processing and visual agnosia. Can J Psychol 46:377–416.
Iacoboni M, Woods RP, Brass M, Bekkering H, Mazziotta JC, Rizzolatti G.(1999) Cortical mechanisms of human imitation. Science 286:2526–2528.
Jambaqu� I, Chiron C, Dulac O, Raynaud C, Syrota P. (1993) Visual inat-tention in West syndrome: a neuropsychological and neurofunctionalimaging study. Epilepsia 34:692–700.
Jambaqu� I, Mottron L, Ponsot G, Chiron C. (1998) Autism and visualagnosia in a child with right occipital lobectomy. J Neurol NeurosurgPsychiatry 65:555–560.
Jambaqu� I, Dellatolas G. (2000) Epreuves de fluence verbale et de d�nom-ination chez l’enfant d’�ge scolaire. ANAE 56:13–16.
Jambaqu� I, Dellatolas G, Fohlen M, Bulteau C, Watier L, Dorfmuller G,Chiron C, Delalande O. (2007) Memory functions following surgery fortemporal lobe epilepsy in children. Neuropsychologia 45:2850–2862.
Janszky J, Jokeit H, Schulz R, Hoppe M, Ebner A. (2000) EEG predicts sur-gical outcome in lesional frontal lobe epilepsy. Neurology 54:1470–1476.
Kaufman AS, Kaufman NL. (1983) Kaufman Assessment Battery for Chil-dren (K-ABC). American Guidance Service[Adaptation franÅaise: Bat-terie pour l’examen psychologique de l’enfant.] 1993. Editions du CPA,Paris.
Kim SK, Wang KC, Hwang YS, Kim KJ, Chae JH, Kim IO, Cho BK.(2008) Epilepsy surgery in children: outcomes and complications. JNeurosurg Pediatr 1:277–283.
Korkman M, Kirk U, Kemp S. (1998) NEPSY: a developmental neuropsy-chological assessment. The Psychological Corporation, San Antonio,TX.
Laurent-Vannier A, Pradat-Diehl P, Chevignard M, Abada G, De AgostiniM. (2003) Spatial and motor neglect in children. Neurology 60:202–207.
Lefavrais P. (1967) Test de l'Alouette. Les �ditions du Centre de Psycholo-gie Appliqu�e, Paris.
Leff AP, Scott SK, Rothwell JC, Wise RJ. (2001) The planning and guidingof reading saccades: a repetitive transcranial magnetic stimulationstudy. Cereb Cortex 11:918–923.
Lerner JT, Salamon N, Hauptman JS, Velasco TR, Hemb M, Wu JY, San-kar R, Donald Shields W, Engel J Jr, Fried I, Cepeda C, Andre VM,Levine MS, Miyata H, Yong WH, Vinters HV, Mathern GW. (2009)Assessment and surgical outcomes for mild type I and severe type IIcortical dysplasia: a critical review and the UCLA experience. Epilep-sia 50:1310–1335.
Lindgren SD, Benton AL. (1980) Developmental patterns of visuospatialjudgment. J Pediatr Psychol 5:217–225.
Lortie A, Plouin P, Chiron C, Delalande O, Dulac O. (2002) Characteristicsof epilepsy in focal cortical dysplasia in infancy. Epilepsy Res 51:133–145.
Luerding R, Boesebeck F, Ebner A. (2004) Cognitive changes after epi-lepsy surgery in the posterior cortex. J Neurol Neurosurg Psychiatry75:583–587.
Mancini J, de Schonen S, Deruelle C, Massoulier A. (1994) Face recogni-tion in children with early right or left brain damage. Dev Med ChildNeurol 36:156–166.
Marinkovic K, Dhond RP, Dale AM, Glessner M, Carr V, Halgren E.(2003) Spatiotemporal dynamics of modality-specific and supramodalword processing. Neuron 38:487–497.
2056
S. Lippe et al.
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x

Mattingley JB, Driver J, Beschin N, Robertson IH. (1997) Attentional com-petition between modalities: extinction between touch and vision afterright hemisphere damage. Neuropsychologia 35:867–880.
McCandliss BD, Cohen L, Dehaene S. (2003) The visual word form area:expertise for reading in the fusiform gyrus. Trends Cogn Sci 7:293–299.
McDonald SA. (2006) Parafoveal preview benefit in reading is onlyobtained from the saccade goal. Vision Res 46:4416–4424.
Mechelli A, Crinion JT, Long S, Friston KJ, Lambon Ralph MA,Patterson K, McClelland JL, Price CJ. (2005) Dissociating readingprocesses on the basis of neuronal interactions. J Cogn Neurosci17:1753–1765.
Mesulam MM. (1981) A cortical network for directed attention and unilat-eral neglect. Ann Neurol 10:309–325.
Mitchell JP. (2008) Activity in right temporo-parietal junction is not selec-tive for theory-of-mind. Cereb Cortex 18:262–271.
Mussolin C, De Volder A, Grandin C, Schlogel X, Nassogne MC, Noel MP.(2010) Neural correlates of symbolic number comparison in develop-mental dyscalculia. J Cogn Neurosci 22:860–874.
Nachev P, Husain M. (2006) Disorders of visual attention and the posteriorparietal cortex. Cortex 42:766–773.
Neurocognition LC-saLdPe. (2002) ODESYS Outil de D�pistage de laDyslexie. UIFM de Grenoble, Grenoble.
Olivier A. (1992) Temporal resections in the surgical treatment of epilepsy.Epilepsy Res (suppl 5):175–188.
Pegna AJ, Khateb A, Michel CM, Landis T. (2004) Visual recognition offaces, objects, and words using degraded stimuli: where and when itoccurs. Hum Brain Mapp 22:300–311.
Pouthas V, George N, Poline JB, Pfeuty M, Vandemoorteele PF, Hugue-ville L, Ferrandez AM, Lehericy S, Lebihan D, Renault B. (2005) Neu-ral network involved in time perception: an fMRI study comparing longand short interval estimation. Hum Brain Mapp 25:433–441.
Rey A. (1959) Test de copie d'une figure complexe. Les �ditions du Centrede Psychologie Appliqu�e, Paris.
Roland PE, Friberg L. (1985) Localization of cortical areas activated bythinking. J Neurophysiol 53:1219–1243.
Rousseaux M, Beis JM, Pradat-Diehl P, Martin Y, Bartolomeo P,Bernati T, Chokron SM, Leclercq M, Louis-Dreyfus A, MarchalF, Perennou DC, Prairial C, Rode G, Samuel C, Sieroff E, WiartL, Azouvi P. (2001) Pr�sentation d’une batterie de d�pistage de lan�gligence spatiale. Normes et effets de l’�ge, du niveau d’�ducation,du sexe, de la main et de la lat�ralit�. Rev Neurol (Paris) 157:1385–1400.
Shmuelof L, Zohary E. (2007) Watching others’ actions: mirror representa-tions in the parietal cortex. Neuroscientist 13:667–672.
Simos PG, Breier JI, Fletcher JM, Foorman BR, Castillo EM, PapanicolaouAC. (2002) Brain mechanisms for reading words and pseudowords: anintegrated approach. Cereb Cortex 12:297–305.
Sinclair DB, Wheatley M, Snyder T, Gross D, Ahmed N. (2005) Posteriorresection for childhood epilepsy. Pediatr Neurol 32:257–263.
Smith M, Billingsley RL. (2001) Neuropsychology of parieto-occipitalepilepsy. In Jambaqu� I, Lassonde M, Dulac O (Eds) Neuropsychologyof childhood epilepsy. Kluwer Academic/Plenum Publishers, NewYork.
Sujansky E, Conradi S. (1995) Outcome of Sturge-Weber syndrome in 52adults. Am J Med Genet 57:35–45.
Trauner DA. (2003) Hemispatial neglect in young children with early uni-lateral brain damage. Dev Med Child Neurol 45:160–166.
Tzagarakis C, Jerde TA, Lewis SM, Ugurbil K, Georgopoulos AP. (2009)Cerebral cortical mechanisms of copying geometrical shapes: a multidi-mensional scaling analysis of fMRI patterns of activation. Exp BrainRes 194:369–380.
Vallar G, Antonucci G, Guariglia C, Pizzamiglio L. (1993) Deficits of posi-tion sense, unilateral neglect and optokinetic stimulation. Neuropsycho-logia 31:1191–1200.
Van Kleeck MH, Kosslyn SM. (1989) Gestalt laws of perceptual organiza-tion in an embedded figures task: evidence for hemispheric specializa-tion. Neuropsychologia 27:1179–1186.
Vinckier F, Naccache L, Papeix C, Forget J, Hahn-Barma V, Dehaene S,Cohen L. (2006) ‘‘What’’ and ‘‘where’’ in word reading: ventral codingof written words revealed by parietal atrophy. J Cogn Neurosci18:1998–2012.
Warrington EK, James M. (1991) A new test of object decision: 2D silhou-ettes featuring a minimal view. Cortex 27:370–383.
Wiebe S, Blume WT, Girvin JP, Eliasziw M. (2001) A randomized, con-trolled trial of surgery for temporal-lobe epilepsy. N Engl J Med345:311–318.
Wyllie E, Comair YG, Kotagal P, Bulacio J, Bingaman W, Ruggieri P.(1998) Seizure outcome after epilepsy surgery in children and adoles-cents. Ann Neurol 44:740–748.
Supporting Information
Additional Supporting Information may be found in theonline version of this article:
Figure S1. Postsurgery MRI of Patient 2.Figure S2. Postsurgery MRI of Patient 5.Please note: Wiley-Blackwell is not responsible for the
content or functionality of any supporting information sup-plied by the authors. Any queries (other than missing mate-rial) should be directed to the corresponding author for thearticle.
2057
Outcome of Posterior Resection in Children
Epilepsia, 51(10):2047–2057, 2010doi: 10.1111/j.1528-1167.2010.02651.x
Related Documents