Cognitive Impairment in Schizophrenia Richard S.E. Keefe and Philip D. Harvey Contents 1 Cognitive Impairment in Schizophrenia and Its Clinical Relevance ....................... 12 1.1 Cognition in the Diagnosis of Schizophrenia ......................................... 12 1.2 Cognitive Deficits Are Found in Almost All Patients with Schizophrenia .......... 12 1.3 Cognitive Impairment Is Not Caused by Psychotic Symptoms ...................... 13 1.4 Cognitive Impairment Is an Important Cause of Functional Disability and Related Outcomes in Schizophrenia .............................................. 14 1.5 The Profile of Cognitive Impairment in Schizophrenia .............................. 15 1.6 Cognitive Impairment Precedes the Onset of Psychosis ............................. 18 1.7 Assessment of Cognition in Schizophrenia Treatment Studies ...................... 20 1.8 Early Phase Trials ...................................................................... 21 1.9 Functional Capacity .................................................................... 24 2 Treatments for Cognitive Impairment in Schizophrenia ................................... 25 2.1 Antipsychotic Effects on Cognition ................................................... 26 2.2 Pharmacological Augmentation as a Cognitive Enhancement Strategy ............. 27 2.3 Results of Cognitive Enhancement Efforts to Date .................................. 29 2.4 Cognitive Remediation as a Platform for Pharmacologic Studies ................... 29 3 Conclusions .................................................................................. 30 References ........................................................................................ 31 Abstract Cognitive functioning is moderately to severely impaired in patients with schizophrenia. This impairment is the prime driver of the significant disabilities in occupational, social, and economic functioning in patients with schizophrenia and an important treatment target. The profile of deficits in schizophrenia includes many of the most important aspects of human cognition: attention, memory, reasoning, R.S.E. Keefe (*) Duke University Medical Center, Durham, NC 27710, USA e-mail: [email protected] P.D. Harvey University of Miami Miller School of Medicine, Miami, FL 33136, USA e-mail: [email protected] M.A. Geyer and G. Gross (eds.), Novel Antischizophrenia Treatments, Handbook of Experimental Pharmacology 213, DOI 10.1007/978-3-642-25758-2_2, # Springer-Verlag Berlin Heidelberg 2012 11

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cognitive Impairment in Schizophrenia
Richard S.E. Keefe and Philip D. Harvey
Contents
1 Cognitive Impairment in Schizophrenia and Its Clinical Relevance . . . . . . . . . . . . . . . . . . . . . . . 12
1.1 Cognition in the Diagnosis of Schizophrenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
1.2 Cognitive Deficits Are Found in Almost All Patients with Schizophrenia . . . . . . . . . . 12
1.3 Cognitive Impairment Is Not Caused by Psychotic Symptoms . . . . . . . . . . . . . . . . . . . . . . 13
1.4 Cognitive Impairment Is an Important Cause of Functional Disability
and Related Outcomes in Schizophrenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
1.5 The Profile of Cognitive Impairment in Schizophrenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
1.6 Cognitive Impairment Precedes the Onset of Psychosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
1.7 Assessment of Cognition in Schizophrenia Treatment Studies . . . . . . . . . . . . . . . . . . . . . . 20
1.8 Early Phase Trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
1.9 Functional Capacity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
2 Treatments for Cognitive Impairment in Schizophrenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
2.1 Antipsychotic Effects on Cognition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
2.2 Pharmacological Augmentation as a Cognitive Enhancement Strategy . . . . . . . . . . . . . 27
2.3 Results of Cognitive Enhancement Efforts to Date . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
2.4 Cognitive Remediation as a Platform for Pharmacologic Studies . . . . . . . . . . . . . . . . . . . 29
3 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Abstract Cognitive functioning is moderately to severely impaired in patients with
schizophrenia. This impairment is the prime driver of the significant disabilities in
occupational, social, and economic functioning in patients with schizophrenia and
an important treatment target. The profile of deficits in schizophrenia includes many
of the most important aspects of human cognition: attention, memory, reasoning,
R.S.E. Keefe (*)
Duke University Medical Center, Durham, NC 27710, USA
e-mail: [email protected]
P.D. Harvey
University of Miami Miller School of Medicine, Miami, FL 33136, USA
e-mail: [email protected]
M.A. Geyer and G. Gross (eds.), Novel Antischizophrenia Treatments,Handbook of Experimental Pharmacology 213,
DOI 10.1007/978-3-642-25758-2_2, # Springer-Verlag Berlin Heidelberg 2012
11
and processing speed. While various efforts are under way to identify specific
aspects of neurocognition that may lie closest to the neurobiological etiology and
pathophysiology of the illness, and may provide relevant convergence with animal
models of cognition, standard neuropsychological measures continue to demon-
strate the greatest sensitivity to functionally relevant cognitive impairment.
The effects of antipsychotic medications on cognition in schizophrenia and
first-episode psychosis appear to be minimal. Important work on the effects of
add-on pharmacologic treatments is ongoing. Very few of the studies completed to
date have had sufficient statistical power to generate firm conclusions; recent
studies examining novel add-on treatments have produced some encouraging
findings. Cognitive remediation programs have generated considerable interest
as these methods are far less costly than pharmacologic treatment and are likely
to be safer. A growing consensus suggests that these interventions produce modest
gains for patients with schizophrenia, but the efficacy of the various methods used
has not been empirically investigated.
Keywords Cognition • Neurocognition • Neuropsychology • Cognitive
neuroscience • Memory • Attention • Processing speed • Executive functioning •
Social cognition • Cognitive remediation • Enhancement
1 Cognitive Impairment in Schizophrenia and Its Clinical
Relevance
1.1 Cognition in the Diagnosis of Schizophrenia
Cognitive impairment associated with schizophrenia is now viewed as a potential
psychopharmacological target for treatment (Hyman and Fenton 2003). Although
cognition is not a formal part of the current diagnostic criteria for schizophrenia,
the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders
DSM-IV-TR (American Psychiatric Association 2000) includes seven references to
cognitive dysfunction in the description of the disorder. Diagnostic and scientific
experts increasingly have expressed the idea that neurocognitive impairment
is a core feature of the illness and not simply the result of the symptoms or the
current treatments of schizophrenia. It is likely that the fifth edition of DSM will
include cognition as a domain that will need to be evaluated by clinicians in the
course of a diagnostic assessment (Keefe and Fenton 2007; Barch and Keefe 2010).
1.2 Cognitive Deficits Are Found in Almost All Patientswith Schizophrenia
Severely impaired performance on cognitive tests is the strongest evidence for
the importance of cognitive deficits in schizophrenia. In several cognitive domains,
12 R.S.E. Keefe and P.D. Harvey

the average cognitive impairment in schizophrenia can reach two standard
deviations below the healthy control mean (Harvey and Keefe 1997; Heinrichs
and Zakzanis 1998; Saykin et al. 1991; Keefe et al. 2011a). Although approxi-
mately 27% of patients with schizophrenia (and 85% of the general population) are
not rated as “impaired” by clinical neuropsychological assessment (Palmer et al.
1997), these patients tend to have the highest levels of premorbid functioning
(Kremen et al. 2000) and demonstrate cognitive functioning that is considerably
below what would be expected of them based on their premorbid levels and the
education level of their parents. Up to 98% of patients with schizophrenia perform
more poorly on cognitive tests than would be predicted by their parents’ education
level (Keefe et al. 2005). In addition, comparisons of monozygotic twins discordant
for schizophrenia suggest that almost all affected twins perform worse than their
unaffected twin on cognitive tests (Goldberg et al. 1990). Therefore, it is likely
that almost all patients with schizophrenia are functioning below the level that
would be expected in the absence of the illness.
1.3 Cognitive Impairment Is Not Caused by Psychotic Symptoms
Neurocognitive ability is not strongly correlated with severity of psychotic
symptoms in patients with schizophrenia (Addington et al. 1991; Keefe and Harvey
2008; Bilder et al. 1985). Although some exceptions exist, such as isolated reports of
significant correlations of positive symptoms with working memory (Strauss 1993;
Bressi et al. 1996; Carter et al. 1996), source monitoring (Keefe et al. 2002), and
auditory distractibility (Walker and Lewine 1988), the overall trend is for general
neurocognitive impairment not to be correlated with positive symptoms. This low
correlation across various patient samples, including first-episode (Mohamed et al.
1999), chronic (Addington et al. 1991), and elderly (Tamlyn et al. 1992; Davidson
et al. 1995) patients, and confirmed in 1,331 patients assessed at entrance into the
CATIE schizophrenia trial (Keefe et al. 2006a), suggests that positive symptoms are
clearly not the sole cause of the cognitive impairment found in patients
with schizophrenia. However, there are some reasonable caveats to these data.
First, patients who are too psychotic to be tested are of course never included in
empirical studies assessing the relationship between cognition and psychosis sever-
ity. Second, it is possible that patients with more preserved cognitive performance
may be more articulate about their psychotic symptoms, causing higher scores on
symptom rating scales, and thus reducing the detection of any true relationship
between cognitive impairment and psychosis. Finally, most of the studies that have
assessed cognition have focused on standardized measures of neuropsychological
function. As described later, the identification of the true relation between cognitive
impairment and psychosis may require more specific assessments of the processes
that lead to these symptoms (Keefe et al. 2011b; Kraus et al. 2009; Krishnan et al.
2011a, 2011b).
Cognitive Impairment in Schizophrenia 13
1.4 Cognitive Impairment Is an Important Cause of FunctionalDisability and Related Outcomes in Schizophrenia
Cognition has been firmly established as a predictor of real-world community
functioning (Green 1996) as well as the ability to perform everyday living skills
in assessment settings (Evans et al. 2003; Patterson et al. 2001). All of the key
neurocognitive constructs have demonstrated significant relationships to elements
of functional outcome and to manifest effect sizes in the medium range in cross-
sectional (Green et al. 2000; Nuechterlein et al. 2004) and longitudinal follow-up
studies (Malla et al. 2002).
1.4.1 Employment
Ratings of work behavior/performance are related to baseline scores on cognitive
tests in schizophrenia. For example, improvement in patient work performance in a
6-month work rehabilitation program was predicted by baseline performance on
various cognitive tests (Bell and Bryson 2001). Patients enrolled in school full-time
or holding competitive employment show superior performance across measures of
working memory, sustained attention, problem solving, and episodic memory when
compared with unemployed patients (Lysaker and Bell 1995; McGurk and Meltzer
2000); neurocognitive performance plays a more important role than clinical
symptoms in the ability of patients with schizophrenia to work (McGurk et al.
2003).
1.4.2 Independence in Residential Functioning
Cognitive impairments and associated deficits in the ability to perform everyday
living skills (referred to as functional capacity) are highly related to the ability to
live independently. Residential independence can be predicted with considerable
accuracy by performance-based measures (Mausbach et al. 2008). The aspect of
functioning that differed most substantially between samples of schizophrenia
patients that performed near the mean of healthy controls and those who were
more impaired was independent residential status (Leung et al. 2008). These data
suggest that perhaps the most significant impact of neurocognitive impairment is a
patient’s ability to find and maintain adequate independent living.
1.4.3 Quality of Life
Reductions in quality of life are strongly associated with cognitive impairment. The
relationship between subjective experience and social functioning has been shown
to be mediated by executive functioning (Brekke et al. 2001). The long-term effects
14 R.S.E. Keefe and P.D. Harvey
of impaired neurocognition on quality of life in patients with schizophrenia are
quite substantial. While cognitive impairment is a key component of reduced
quality of life in schizophrenia, it is not the entire story as the severity of positive
and negative symptoms is also a significant contributor (Mohamed et al. 2008).
1.4.4 Relapse Prevention
Cognitive functions have been shown to be associated with medication adherence
and are the strongest predictors of patients’ ability to manage medications (Jeste
et al. 2003; Fenton et al. 1997). Cognitive deficits contribute to patterns of medica-
tion mismanagement that are associated with poor adherence and risk of relapse
(Jarboe and Schwartz 1999). In one study, memory impairment was the best
predictor of partial compliance (Donohoe et al. 2001). Patients performing poorly
in medication management tests also had poor global scores on a dementia inven-
tory (Patterson et al. 2002).
1.4.5 Medical Comorbidity
Neurocognitive impairment is also related to medical comorbidities in schizophre-
nia. Deficits in executive functions such as planning directly affect patients’ ability
to seek treatment for medical problems. In elderly patients with schizophrenia,
cognitive and functional impairments predicted the later incidence of new-onset
medical problems, whereas medical problems did not predict the subsequent wors-
ening of cognitive and self-care deficits (Friedman 2002). Inability of patients with
schizophrenia to reduce damaging habits such as smoking has been correlated with
deficits in memory and attention (Buchanan et al. 1994; George et al. 2000) and is a
likely determinant of the substantial increase in cardiac morbidity and mortality in
this population. Cognitive impairments may thus directly effect new-onset medical
problems in people with schizophrenia.
1.4.6 Costs
Cognitive impairment is also a major factor in the costs (direct and indirect)
associated with schizophrenia (Sevy and Davidson 1995). Factors leading to the
increased cost include loss of ability for self-care, level of inpatient and outpatient
care needed, and loss of productivity for patients as well as caregivers.
1.5 The Profile of Cognitive Impairment in Schizophrenia
Neurocognitive tests often assess more than one domain of functioning, and many
tests do not fit neatly into a single domain. Thus, descriptions of the profile of
cognitive deficits in schizophrenia have varied across literature reviews. The opinion
Cognitive Impairment in Schizophrenia 15

of a group of experts who served on the Neurocognition Subcommittee for the
Measurement and Treatment Research to Improve Cognition in Schizophrenia
(MATRICS) project (http://www.matrics.ucla.edu) is that the most important
domains of cognitive deficit in schizophrenia are working memory, attention/vigi-
lance, verbal learning and memory, visual learning and memory, reasoning and
problem solving, speed of processing, and social cognition (Green et al. 2004). As
described later, the outcomemeasure derived by this group has been approved by the
Psychiatry Division of the Food and Drug Administration as the gold standard for
registration trials targeting cognition in schizophrenia (Buchanan et al. 2005;
Buchanan et al. 2011a). Since this organization of the domains of cognition is
particularly relevant for treatment studies emphasized in this volume, these domains
are described later. Alternative views have also been considered (Reichenberg et al.
2009). In addition, recent data have supported the hypothesis that perception may
not only be impaired in schizophrenia, but may mediate some of the higher level
cognitive deficits, such as working memory performance. However, any serious
review of this literature suggests that the profile of cognitive deficits and level of
performance in patients with schizophrenia include almost no aspect of cognition
that is similar to those in healthy control subjects (Dias et al. 2011). This profile
contrasts with the cognitive performance of patients with other psychotic disorders
such as bipolar disorder, which suggests near-normal performance in the reasoning
and problem solving or social cognition domains of the MATRICS battery (Burdick
et al. 2011).
1.5.1 Vigilance and Attention
Vigilance refers to the ability to maintain attention over time. Impairments in vigi-
lance can result in difficulty following social conversations and an inability to follow
important instructions; simple activities such as reading or watching television
become labored or impossible. Vigilance deficits in patients with schizophrenia are
related to various aspects of outcome, including social deficits, community function-
ing, and skills acquisition (Green 1996; Green et al. 2000).
1.5.2 Verbal Learning and Memory
The abilities involved in memory functioning include learning new information,
retaining newly learned information over time, and recognizing previously
presented material. In general, patients show larger deficits in learning than in
retention. The tests used to measure learning typically involve the ability to learn
lists of words or written passages. Much empirical evidence points to severe
verbal memory impairments in schizophrenia (Aleman et al. 1999). There is
a clear connection between verbal memory impairments and social deficits in
patients with schizophrenia, including both real-world functioning (Green 1996)
and performance on social competence tests (McClure et al. 2007).
16 R.S.E. Keefe and P.D. Harvey
1.5.3 Visual Learning and Memory
Because visual information is not as easily expressed as verbal information, fewer
tests sensitive to the deficits of schizophrenia have been developed, and this area of
cognitive function has generally been found not to be as impaired as verbal memory
(Heinrichs and Zakzanis 1998). Visual memory has been found to correlate mod-
estly with employment status (Gold et al. 2003), job tenure (Gold et al. 2002),
psychosocial rehabilitation success (Mueser et al. 1991), social functioning
(Dickerson et al. 1999), quality of life ratings (Buchanan et al. 1994), and strongly
with functional capacity (Twamley et al. 2003). Other studies have reported no
significant correlations (Addington and Addington 1998, 2000; Ertugrul and Ulug
2002; Velligan et al. 2000).
1.5.4 Reasoning and Problem Solving
Although there are many tests of reasoning and problem solving, the most well
known and most frequently used in schizophrenia research is the Wisconsin Card
Sorting Test (WCST). The very poor performance of patients with schizophrenia on
the WCST and the reduced activity of the dorsolateral prefrontal cortex during
performance of this test (Goldberg et al. 1987; Weinberger 1987) led to widespread
pursuit of the hypothesis of frontal hypoactivation in schizophrenia. It is important to
note, however, that performance on the WCST reflects a variety of cognitive
functions and is not a pure measure of executive functions (Keefe 1995). The rules
of society and the workplace change regularly, and success in these arenas is often
measured by one’s ability to adapt to changes. Patients with schizophrenia who are
impaired on measures of executive functions have difficulty adapting to the rapidly
changing world around them.
1.5.5 Speed of Processing
Many neurocognitive tests require subjects to process information rapidly and can
be compromised by impairments in processing speed. Standard examples of this
type of task are the coding tasks, which have been found to demonstrate the most
severe deficits in schizophrenia (Dickinson et al. 2007). This aspect of cognitive
impairment is relatively nonspecific and has been found to correlate with a variety
of clinically important features of schizophrenia, such as daily life activities (Evans
et al. 2003), job tenure (Gold et al. 2002), and independent living status (Brekke
et al. 1997). Reduced processing speed can impair the ability to keep in step with
the task-oriented jobs that are frequently held by patients with schizophrenia.
Increased response latency in social settings may hamper social relationships.
Cognitive Impairment in Schizophrenia 17

1.5.6 Working Memory
Working memory has been described by various authors as a core component of the
cognitive impairment in schizophrenia (Brekke et al. 1997; Goldman-Rakic 1994;
Keefe 2000) and is related to functional outcomes such as employment status
(Lysaker and Bell 1995) and job tenure (Gold et al. 2003). Much of the clinical
relevance of working memory deficits in schizophrenia comes from strong
correlations that working memory measures have with a variety of other cognitive
domains impaired in schizophrenia, such as attention, planning, memory (Silver
et al. 2003), and intelligence (Keefe 2000), as well as the advanced understanding
of the neuroanatomy of working memory functions in human and nonhuman
primates. This neuroanatomical work has suggested that neural circuitry that
includes prefrontal cortical regions mediates aspects of working memory functions
(Baddeley 1992; Callicott et al. 1999) and that this circuitry may be impaired in
schizophrenia (Baddeley 1992; Goldman-Rakic 1987).
1.5.7 Social Cognition
Theory-of-mind skills and social and emotion perception and recognition have been
the general focus of the literature on social cognition in schizophrenia. Theory of
mind is the ability to infer another’s intentions and/or to represent the mental states of
others. Individuals with schizophrenia perform poorly onmeasures of theory-of-mind
abilities (Tan et al. 2005; Corcoran et al. 1995; Drury et al. 1998). Facial affect
recognition and social cue perception are the two general areas into which studies of
social perception in schizophrenia can be broken down. Reviews of the literature on
facial affect recognition (Sarfati et al. 1997; Morrison et al. 1988; Penn et al. 1997)
suggest that individuals with schizophrenia have stable deficits on tests of facial
affect perception and that perception of negative emotions and fear may be particu-
larly impaired (Addington and Addington 2000; Penn et al. 1997; Pinkham et al.
2011; Edwards et al. 2001). Tests of social cue perception use more dynamic stimuli
that require multiple sensory modalities, such as watching people interacting. Patients
with schizophrenia show consistent impairments on these tasks (Gaebel and W€olwer1992; Bell et al. 1997). Social cognition is related to social impairments in schizo-
phrenia, even after controlling for performance on neurocognitive tasks (Corrigan
et al. 1990; Trumbetta and Mueser 2001). Path models have suggested that the
relations between social cognition and functional outcomes are complex, but that
social cognition may explain more of the direct variance in social functioning than
other aspect of cognitive performance (Penn et al. 1996).
1.6 Cognitive Impairment Precedes the Onset of Psychosis
Various methods for assessing the relationship between premorbid cognitive
impairment and later psychotic disorders have suggested that young people destined
18 R.S.E. Keefe and P.D. Harvey
to develop schizophrenia are modestly impaired on cognitive measures. However,
these deficits tend to be quite mild (Brekke et al. 2007) and their ability to help
predict psychotic disorders is under question. In a special circumstance, the longitu-
dinal follow-up of individuals who manifest prodromal symptoms (Reichenberg
et al. 2010), deficits on standard neuropsychological tests that are present at the time
of the development of the prodrome discriminate cases who go on to develop
psychosis from those who do not. However, impairment on these measures was
not able to contribute to the prediction of psychosis beyond clinical measures
implemented in the study.
Early work completed in the U.K. (Seidman et al. 2010) and Sweden (Jones et al.
1994) suggested that children who went on to develop schizophrenia as adults
differed significantly from the general population in a wide range of cognitive and
behavioral domains. Similar findings were generated from a population-based study
that investigated the risk of schizophrenia in the United States. Scores from grades
4, 8, and 11 on the Iowa Tests for 70 children who later developed schizophrenia
suggested that those children who later developed schizophrenia, test scores
dropped significantly between grades 8 and 11, corresponding with the onset of
puberty (David et al. 1997).
In Israel, a study of all adolescents between the ages of 16 and 17 years
suggested that cognitive functions are significantly impaired in those adolescents
who are later hospitalized for schizophrenia. These deficits thus precede the onset
of psychosis in young people destined to develop schizophrenia, and, along with
social isolation and organizational ability, cognitive deficits are a significant pre-
dictor of which young people will eventually develop a psychotic disorder (Fuller
et al. 2002). However, the mean level of performance of this group, at about the
35th percentile of the overall population, does not allow for a very strong predictive
signal on a case-by-case basis. In the young people who later experienced a first
episode of schizophrenia, their cognitive results in the prodrome suggested that
most of the cognitive impairment of schizophrenia occurs prior to the first psychotic
episode (Davidson et al. 1999).
Recent work from the Dunedin study in New Zealand, which tracked the
cognitive and mental health of a large group of individuals in a single geographical
location, suggests that a subtle pattern of cognitive changes over early childhood
may predict schizophrenia compared to depression and no illness (Brekke et al.
2007). In this study, children aged 7–13 who developed adult schizophrenia
exhibited cognitive impairments that emerged early and remain stable on tests of
verbal and visual knowledge acquisition, reasoning, and conceptualization. They
also demonstrated developmental cognitive growth that was slower relative to
healthy comparison subjects on tests indexing processing speed, attention,
visual–spatial problem solving ability, and working memory. These two premorbid
cognitive patterns were not observed in children who later developed recurrent
depression. The authors concluded that the origins of schizophrenia include two
interrelated developmental processes evident from childhood to early adolescence.
Children who will grow up to develop adult schizophrenia enter primary school
Cognitive Impairment in Schizophrenia 19

struggling with verbal reasoning and lag further behind their peers in working
memory, attention, and processing speed as they get older.
Prospective studies have suggested that cognitive impairment is manifest in
individuals who are identified as being at “ultra-high” risk (Caspi et al. 2003) for
schizophrenia by virtue of their family history of schizophrenia and/or the manifes-
tation of mild signs and symptoms consistent with the prodromal symptoms of
schizophrenia (Yung and McGorry 1996; Brewer et al. 2003). Some aspects of
cognitive and perceptual performance in ultra-high risk individuals have been
found to predict which individuals will develop psychotic symptoms such as
olfactory impairment (Yung and McGorry 1996), verbal memory impairment
(Hawkins et al. 2004), and attentional impairment (Brewer et al. 2005). Data
combined from the seven sites of the North American Prodromal Longitudinal
Study (NAPLS) consortium indicate that poorer scores on an overall composite
score of several tests provided the most sensitive measure that differentiated those
high-risk children who would develop psychosis from those who would not, and
worse verbal memory scores predicted a briefer time to psychosis in those who
developed schizophrenia (Reichenberg et al. 2010). However, when regression
models were used, a clinical cluster of genetic risk for schizophrenia with recent
deterioration in functioning, higher levels of unusual thought content, higher levels
of suspicion/paranoia, greater social impairment, and a history of substance abuse
predicted psychosis best (Keefe et al. 2006b) and cognitive measures did not
contribute additionally beyond the clinical measures.
One of the important limitations of the work completed to date has been a
reliance upon the assessment of cognition in schizophrenia and at-risk states with
measures designed to measure intelligence or brain damage that may not be
sensitive to the specific neural circuitry impairments underlying schizophrenia.
Methodologies investigating the specific cognitive and neurobiological processes
that may underlie and possibly precede the conversion to psychosis are likely to
yield greater risk prediction specificity. Human perception, thought, and action—
the basic elements of maintaining reality—are based upon a hierarchical process
that conjoins memory and external stimuli, which has been referred to as learning-
dependent predictive perception (Cannon et al. 2008; Keefe et al. 2011b). It has
been hypothesized that perturbations of the circuitry underlying learning-dependent
predictive perception may contribute to risk for developing schizophrenia and thus
early detection of risk may be more successful with tasks specifically designed to
test memory-prediction function (Krishnan et al. 2011a; Keefe et al. 2011c; Kraus
et al. 2009).
1.7 Assessment of Cognition in Schizophrenia Treatment Studies
As listed in Table 3, multisite trials present a large number of challenges that need
to be met for cognitive data to be collected reliably and efficiently (Keefe and Kraus
2009). Sites and testers must be trained and certified on the test battery and related
20 R.S.E. Keefe and P.D. Harvey
procedures. Data review processes must be established, followed, and maintained
throughout the course of the study. Plans must be in place for adding replacement
testers or new sites during the study. Test selection must address the scientific
hypotheses of the investigators yet be efficient to implement without excessive
missing data. Finally, the data analytic plan should focus on a single or small number
of outcome measures to reduce statistical errors and avoid reduced statistical power.
1.7.1 Registration (Phase III) Trials
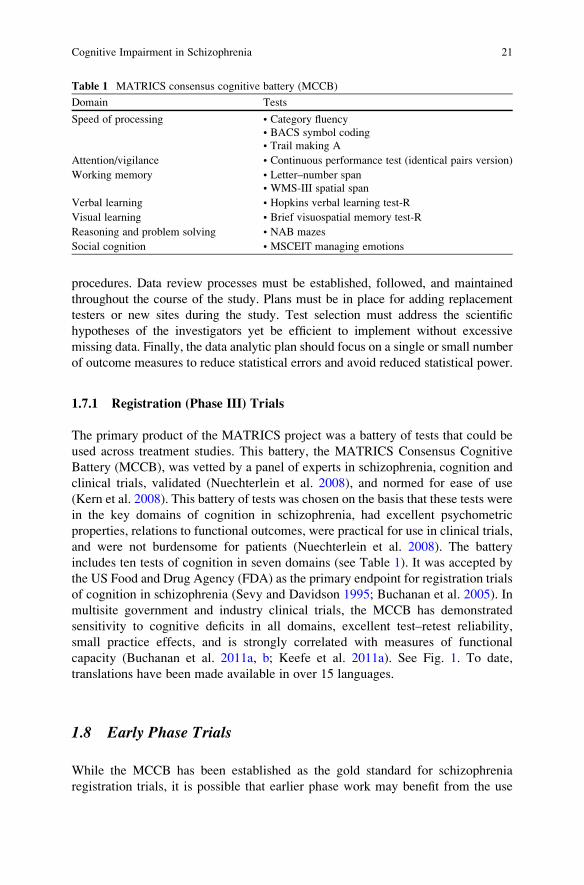
The primary product of the MATRICS project was a battery of tests that could be
used across treatment studies. This battery, the MATRICS Consensus Cognitive
Battery (MCCB), was vetted by a panel of experts in schizophrenia, cognition and
clinical trials, validated (Nuechterlein et al. 2008), and normed for ease of use
(Kern et al. 2008). This battery of tests was chosen on the basis that these tests were
in the key domains of cognition in schizophrenia, had excellent psychometric
properties, relations to functional outcomes, were practical for use in clinical trials,
and were not burdensome for patients (Nuechterlein et al. 2008). The battery
includes ten tests of cognition in seven domains (see Table 1). It was accepted by
the US Food and Drug Agency (FDA) as the primary endpoint for registration trials
of cognition in schizophrenia (Sevy and Davidson 1995; Buchanan et al. 2005). In
multisite government and industry clinical trials, the MCCB has demonstrated
sensitivity to cognitive deficits in all domains, excellent test–retest reliability,
small practice effects, and is strongly correlated with measures of functional
capacity (Buchanan et al. 2011a, b; Keefe et al. 2011a). See Fig. 1. To date,
translations have been made available in over 15 languages.
1.8 Early Phase Trials
While the MCCB has been established as the gold standard for schizophrenia
registration trials, it is possible that earlier phase work may benefit from the use
Table 1 MATRICS consensus cognitive battery (MCCB)
Domain Tests
Speed of processing • Category fluency
• BACS symbol coding
• Trail making A
Attention/vigilance • Continuous performance test (identical pairs version)
Working memory • Letter–number span
• WMS-III spatial span
Verbal learning • Hopkins verbal learning test-R
Visual learning • Brief visuospatial memory test-R
Reasoning and problem solving • NAB mazes
Social cognition • MSCEIT managing emotions
Cognitive Impairment in Schizophrenia 21
of measures that assess cognition in a manner that is closer to the actual neurobio-
logical circuits that mediate cognitive function. To meet the need for more precise
assessment instruments for measuring changes in specific cognitive functions in
treatment studies, cognitive neuroscience methods with known linkages to specific
brain systems, and to some extent their biochemistry, provide a logical alternative
assessment strategy for identifying specific cognitive impairments to be targeted in
schizophrenia treatment trials. These methods can potentially distinguish specific
cognitive deficits from generalized deficits that are well assessed by neuropsycho-
logical testing. For instance, while list-learning tests may assess memory in a
manner that is clinically relevant and correlated with important functional skills,
the development of a treatment for memory impairment may need a more sensitive
task that better reflects the biological processes involved in the acquisition and
storage of representations (Table 2).
A large variety of such tests are available in the cognitive neuroscience litera-
ture, many of which have been utilized in schizophrenia research (Carter and Barch
2007; Carter et al. 2008). In order to expedite the use of these tests for early phase
drug development, the National Institute of Mental Health sponsored a series of
meetings and funding sources called the Cognitive Neuroscience Treatment
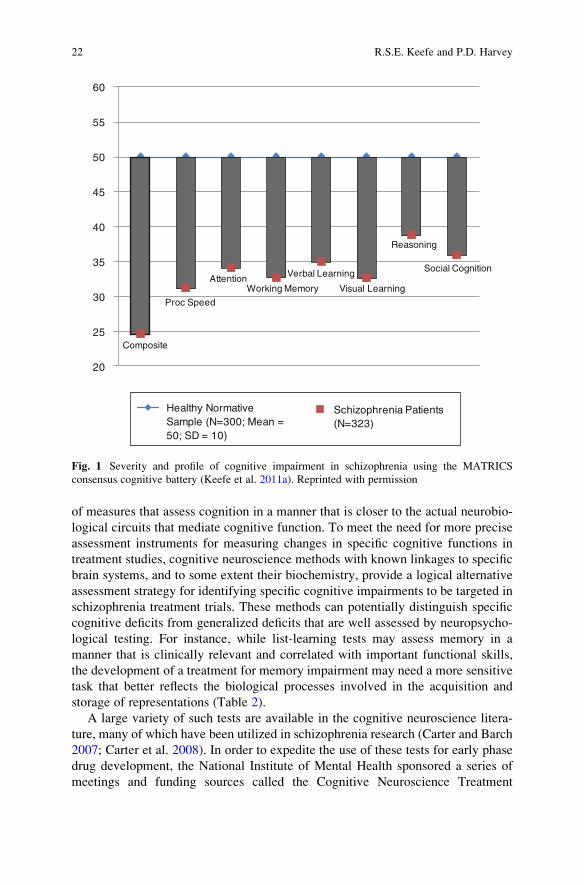
Composite
Proc Speed
AttentionWorking Memory
Verbal Learning
Visual Learning
Reasoning
Social Cognition
20
25
30
35
40
45
50
55
60
Healthy Normative Sample (N=300; Mean = 50; SD = 10)
Schizophrenia Patients (N=323)
Fig. 1 Severity and profile of cognitive impairment in schizophrenia using the MATRICS
consensus cognitive battery (Keefe et al. 2011a). Reprinted with permission
22 R.S.E. Keefe and P.D. Harvey
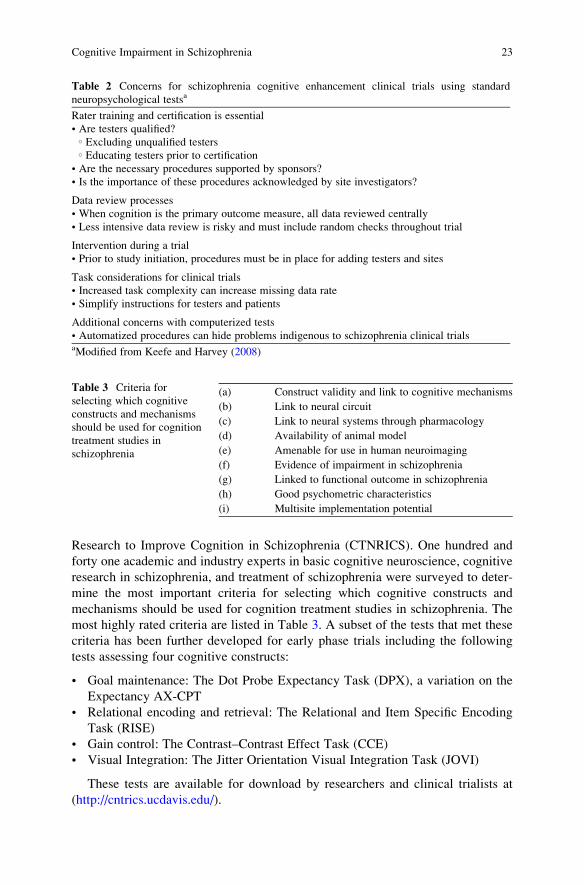
Research to Improve Cognition in Schizophrenia (CTNRICS). One hundred and
forty one academic and industry experts in basic cognitive neuroscience, cognitive
research in schizophrenia, and treatment of schizophrenia were surveyed to deter-
mine the most important criteria for selecting which cognitive constructs and
mechanisms should be used for cognition treatment studies in schizophrenia. The
most highly rated criteria are listed in Table 3. A subset of the tests that met these
criteria has been further developed for early phase trials including the following
tests assessing four cognitive constructs:
• Goal maintenance: The Dot Probe Expectancy Task (DPX), a variation on the
Expectancy AX-CPT
• Relational encoding and retrieval: The Relational and Item Specific Encoding
Task (RISE)
• Gain control: The Contrast–Contrast Effect Task (CCE)
• Visual Integration: The Jitter Orientation Visual Integration Task (JOVI)
These tests are available for download by researchers and clinical trialists at
(http://cntrics.ucdavis.edu/).
Table 2 Concerns for schizophrenia cognitive enhancement clinical trials using standard
neuropsychological testsa
Rater training and certification is essential
• Are testers qualified?○ Excluding unqualified testers○ Educating testers prior to certification
• Are the necessary procedures supported by sponsors?
• Is the importance of these procedures acknowledged by site investigators?
Data review processes
• When cognition is the primary outcome measure, all data reviewed centrally
• Less intensive data review is risky and must include random checks throughout trial
Intervention during a trial
• Prior to study initiation, procedures must be in place for adding testers and sites
Task considerations for clinical trials
• Increased task complexity can increase missing data rate
• Simplify instructions for testers and patients
Additional concerns with computerized tests
• Automatized procedures can hide problems indigenous to schizophrenia clinical trialsaModified from Keefe and Harvey (2008)
Table 3 Criteria for
selecting which cognitive
constructs and mechanisms
should be used for cognition
treatment studies in
schizophrenia
(a) Construct validity and link to cognitive mechanisms
(b) Link to neural circuit
(c) Link to neural systems through pharmacology
(d) Availability of animal model
(e) Amenable for use in human neuroimaging
(f) Evidence of impairment in schizophrenia
(g) Linked to functional outcome in schizophrenia
(h) Good psychometric characteristics
(i) Multisite implementation potential
Cognitive Impairment in Schizophrenia 23
One of the critical issues associated with sophisticated cognitive neuroscience
tests is whether these tests will manifest the substantial and consistent correlations
seen between standard neuropsychological tests and indices of everyday function-
ing. One of the reasons that these standard tests may be so strongly correlated with
everyday functioning is because that they are so global and nonspecific. It should be
noted that individuals with highly localized lesions in focal brain regions often
manifest levels of everyday disability that are less than those seen in schizophrenia.
It is entirely possible that these sophisticated tests will be highly sensitive to focal
brain functioning and only modestly sensitive to disability. If this is found,
then their use for early stage research would have to be carefully considered.
As described later, the goal of treatment of cognition, as currently conceptualized,
is to reduce disability. If task performance is uncorrelated with disability, then
it seems implausible to think that improving performance would reduce disability.
1.9 Functional Capacity
A new development in the last decade of study of cognition and functioning in
schizophrenia is that of direct measurement of the abilities that are required to
succeed in critical functional domains. Based on the idea that what one can do (i.e.,
competence or capacity) constrains what one will do (everyday functional perfor-
mance), these assessments have been developed to measure the skills that underlie
functioning. This area of research has led to findings suggesting that functional
capacity measures are highly correlated with cognitive test performance and may be
more proximal than cognitive abilities to everyday outcomes. This relationship
seems logical. If one is interested in whether someone can pay their bills, should the
predictive assessment require the patient to manage money, write checks, and make
bank deposits, or should they be asked to connect 25 dots as fast as they can?
1.9.1 Domains of Functional Capacity Assessment
Functional capacity assessments have been developed to measure everyday living
skills, social skills, vocational skills, and medication management. While a review
of these instruments could fill this entire chapter, some highlights are presented and
more details are available in Harvey et al. (2007). These measures are inherently
performance based. As a result, their psychometric characteristics can be measured
(e.g., test–retest reliability, floor and ceiling effects). At the same time, as a
performance-based assessment, practice effects can occur and other factors that
affect the validity of performance-based assessment, such as motivation and envi-
ronmental settings, can also require consideration.
The original focus of functional capacitymeasures in schizophrenia was on social
skills; these assessments are still routinely performed. Recently, everyday living
skills have been a particular focus of research and several of these assessments have
been developed and validated. The UCSD Performance-based Skills Assessment
24 R.S.E. Keefe and P.D. Harvey

(UPSA) (Patterson et al. 2001) is the most widely used. This assessment has 5 or 6
subtests depending on the version and measures finances, comprehension and
planning, communication, transportation, and household management. In the sec-
ond edition of the UPSA, the UPSA-II, medication management was added. A short
two-subtest version has also been developed. The UPSA has been shown to be quite
consistently and substantially correlated with cognitive performance; across 11
published studies to date the correlation is consistently about r ¼ 0.63. The
test–retest reliability and practice effects of the UPSA seem similar to those seen
in standard neuropsychological tests. UPSA scores predict residential independence
quite effectively. In a comparative study of several different short and long forms of
different functional capacity measures (Green et al. 2011), the UPSA was most
highly convergent with performance on theMCCB and also the most user friendly in
terms of complexity, duration, and ease of administration.
There are some issues in the interpretation of functional capacity assessments as
compared to neuropsychological tests and these issues arise when both types of
measures are used as treatment outcomes as described later. Neuropsychological
tests are designed to measure the entire range of human cognitive functioning and
are not designed to be specifically targeted at the prediction of any particularly
functional skills. As a result, there is a wide range of scores on these tests and,
because of the way that they are designed, only about 0.1% or less of the healthy
population attain perfect scores and hence show ceiling effects. In contrast, func-
tional capacity measures are intrinsically aimed at disability. Because the success-
ful performance of everyday living skills is very common in the healthy adult
population, a valid functional capacity test would have a large proportion of healthy
people passing with 100% correct. As people with schizophrenia show an extraor-
dinary prevalence of disability in domains where the healthy population typically
achieves success without a problem, the distribution of scores across the two
populations would not be expected to be equivalently normal. The uncommon
nondisabled individual with schizophrenia would also be expected to perform
extremely well on these tests. Thus, relatively higher scores on functional capacity
measures may occur in people with schizophrenia. This issue does not arise as often
with tests from the neuropsychology tradition. Similar to the discussion earlier,
disability is not a treatment target in individuals who are not disabled. Thus,
someone who is living independently, paying his/her own expenses, and otherwise
managing their everyday functioning would be expected to get a high score on
a disability-related skills measure and not to be a candidate for a treatment aimed
at disability reduction.
2 Treatments for Cognitive Impairment in Schizophrenia
As of this writing, there are no pharmacologic or behavioral treatments that have
received regulatory approval. Other chapters in this volume address the many
important advances that hold promise for the eventual development of a treatment
Cognitive Impairment in Schizophrenia 25
for cognition in schizophrenia. In this chapter, we will review the literature on the
effects of antipsychotics on cognition and discuss methodology for cognitive
enhancement studies.
2.1 Antipsychotic Effects on Cognition
The effects of antipsychotic medications on cognition remain controversial. Several
early studies and meta-analyses (Swartz et al. 2003; Davis et al. 2003; Rosenheck
et al. 2003) suggested that second-generation antipsychotic treatment may provide
greater neurocognitive benefit to schizophrenia patients than first-generation, “typ-
ical” antipsychotics. These effects extended even to first-episode patients who had
not had previous antipsychotic treatment (Keefe et al. 2004; Harvey et al. 2005).
However, many of these studies had substantial methodological limitations
or flaws, such as small sample sizes, short duration of treatment, no comparator
or a comparator of relatively high doses of first-generation antipsychotic treatment,
and inattention to important clinical factors such as the relationship of cognitive
improvement with symptom change, anticholinergic treatment, and change in
extrapyramidal symptoms (Swartz et al. 2003; Davis et al. 2003; Rosenheck et al.
2003; Stroup et al. 2006). The CATIE study enabled an examination of these issues
in a large sample of patients (Keefe et al. 2007a). Despite unprecedented statistical
power in 817 patients randomized to a single first-generation antipsychotic,
perphenazine, and the four second-generation antipsychotics available at the time
(olanzapine, quetiapine, risperidone, and ziprasidone), there were no significant
differences in the treatments after 2 months of treatment, which was the primary
analysis endpoint. All groups showed a small benefit over time, but the magnitude
of the benefit was viewed as consistent with the small practice and/or placebo
effects found with the test battery utilized (Keefe et al. 2007b). Surprisingly, in
exploratory analyses, the first-generation antipsychotic perphenazine demonstrated
greater improvement than two of the second-generation antipsychotics in the 303
(37% of those assessed in the 2-month analyses) patients who continued on the
same treatment for 18 months.
These results were unexpected and controversial (Kraemer and Frank 2010).
In comparison to previous studies, at least 60% of patients in the CATIE trial
reported being on atypical antipsychotic treatment prior to randomization,
which was substantially higher than in many of the earlier studies completed
when treatment with second-generation antipsychotics was less common. However,
more recent studies on patients with first-episode psychosis and minimal or
no previous antipsychotic treatment confirm these results. A comparison of
olanzapine, quetiapine, and risperidone in first-episode patients using the
identical neurocognitive test battery the CATIE trial produced very similar
results, with all treatments having a very modest effect on cognition (Van Putten
et al. 1991). Perhaps the most relevant study in this area was the
European Union First Episode Schizophrenia Trial (EUFEST), a comparison of
26 R.S.E. Keefe and P.D. Harvey

open-label haloperidol (1–4 mg/day), amisulpride (200–800 mg/day), olanzapine
(5–20 mg/day), quetiapine (200–750 mg/day), or ziprasidone (40–160 mg/day).
This trial produced similar results with no differences between treatments, even in
antipsychotic-naıve patients (Sweet et al. 2000). However, all groups showed a
modest improvement. These improvements were only slightly stronger than prac-
tice effects, and demonstrated a relation to clinical symptom change, suggesting
that first-episode patients may demonstrate some overall cognitive benefit related to
overall clinical improvement. However, recent studies of completely antipsychotic-
naıve patients suggest that while standard neuropsychological measures may dem-
onstrate little change with treatment, other more specific measures of cognitive
neuroscience processes such as speeded saccadic latencies to visual targets are
normalized by risperidone but not haloperidol treatment (Reilly et al. 2006).
Follow-up studies utilizing cognitive neuroscience tasks across specific cognitive
domains may yield useful insights as was observed with the CATIE trials.
Overall, these data suggest that in current treatment settings, the impact of
antipsychotic medications on neurocognition varies little on average, with minimal
benefit for most treatments. The nature of these trials cannot exclude the possibility
that some individual patients experience benefits while others worsen, possibly
differentially across medications, but do suggest that there is no specific medication
to which a switch would ensure benefit.
2.2 Pharmacological Augmentation as a Cognitive EnhancementStrategy
Pharmacological augmentation as a treatment strategy is consistent with best
practices for the treatment of other illnesses. For instance, the treatment of hyper-
tension and heart disease typically involves multiple medications with different
targets, such as diuretics, ACE inhibitors, and calcium channel blockers. In schizo-
phrenia, the analogous treatment might include atypical antipsychotic medications,
treatments for negative symptoms, and treatments for cognitive deficits. Based on
the history of FDA evaluation of treatments for cognitive and functional deficits in
dementia, a model strategy for the development of cognitive enhancing treatments
for schizophrenia has been advanced and endorsed. As a result of the MATRICS
initiative, a unique collaboration between the FDA, the National Institute of Mental
Health (NIMH), academia, and the pharmaceutical industry and a consensus
regarding the acceptable methods for conducting a registration trial were developed
(Sevy and Davidson 1995) and modified (Buchanan et al. 2005). There are several
critical features of this design.
2.2.1 Clinical Stability
The FDA has long been concerned that new treatments that improve cognition do so
directly, rather than by reducing the severity of other features of the illness. Thus, a
Cognitive Impairment in Schizophrenia 27

treatment that improves cognition must do so in the absence of improvements in
other illness features, such as psychosis. Since FDA has thus far taken the position
that simultaneous changes in illness features (cognition and psychosis) that are not
statistically correlated may be related, only patients who are clinically stable can
participate. This screening criterion was initially defined as a moderate or less (<4)
severity rating on selected PANSS positive scale items at both screening and
baseline (Sevy and Davidson 1995), but has recently been revised to allow patients
who receive a score of 5 on the PANSS positive items (Buchanan et al. 2005). Also,
there can be no hospitalization for psychiatric illness for at least 8 weeks prior to
screening.
2.2.2 Treatment Stability
This is defined by no major change in antipsychotic medications for at least 6 weeks
prior to screening.
2.2.3 No Medications That Can Influence Cognitive Functioning
This is defined by no treatment with anticholinergics, amphetamines, or L-DOPA.
2.2.4 Treatment Duration
At least some of the pivotal trials must have a 6-month treatment duration. This
requirement is based on the idea that treatment effects must be durable and is
influenced by concerns that the benefit of certain treatments may not persist over
time. However some evidence indicates that cognitive enhancing treatments in
people with schizophrenia can have benefits that occur within minutes to hours
(Carter and Barch 2007).
2.2.5 Co-primary Measure
The FDA required a “co-primary” in cognitive enhancement studies in dementia.
This requirement was designed to ensure that changes in cognition on a
performance-based test led to a clinically meaningful change in everyday function-
ing. In the context of, for instance, cholinesterase inhibitor treatment of dementia,
this requirement makes sense because none of the treatments approved by the FDA
actually led to immediate improvements in functioning, but rather treatments were
deemed successful for suspending the otherwise inexorable decline seen in
Alzheimer’s disease.
Similarly, a co-primary measure has been required for schizophrenia cognitive
enhancement trials. However, there is little evidence that any of the currently
28 R.S.E. Keefe and P.D. Harvey
available co-primary measures have the potential to be sensitive to treatment-
related changes in performance. The existence of this FDA requirement led to a
comprehensive collaborative study, funded by grants from the pharmaceutical
industry to the Foundation for the National Institute of Mental Health (F-NIMH),
which was recently completed, presented to the public, and is now published. The
results of that study (Green et al. 2011) indicated that performance-based measures
of functional capacity were clearly superior to interview-based assessments of
cognitive functioning in terms of their convergence with the MCCB. It needs to
be stressed that this was a cross-sectional validation study and not a treatment
outcomes study.
2.3 Results of Cognitive Enhancement Efforts to Date
Several cognitive enhancement treatment research programs with a wide variety of
treatment mechanisms are under way. Very recent data from Phase II trials suggest
that some compounds may have promise for improving cognition in schizophrenia,
but none of these compounds have been approved for actual use in patients. Some
of these studies have been completed with negative results (Keefe et al. 2011c).
While a full discussion of the reasons for the negative results would be speculative
and premature, one of the major issues that may be important is that of possible
interfering effects of antipsychotic medications. A single abnormal neurotransmit-
ter system is unlikely to lead to the widespread impairments seen, but it is quite
likely that single-transmitter interventions could be interfered with by the block-
ading effects of antipsychotic medications. Most importantly, however, many of the
studies completed to date have been seriously underpowered to detect true treat-
ment effects. A recent review of all studies completed as of June 1, 2011 (Keefe
et al. 2011c) suggested that none of the studies above had sufficient power to detect
a medium (d ¼ 0.5) effect size, which would require 71 subjects per group assum-
ing the primary outcome measure has excellent test–retest reliability (ICC ¼�0.90) as with the MCCB composite score (Keefe et al. 2011a). Several studies
had sufficient power to detect a large (d ¼ 0.8) effect.
2.4 Cognitive Remediation as a Platformfor Pharmacologic Studies
While broad-ranging initiatives are ongoing to refine our understanding of the
mechanisms of cognitive improvement in schizophrenia, an additional area of
consideration is the relatively impoverished cognitive lives of patients who enroll
in pharmacologic enhancement studies. It is possible that many of these experi-
mental pharmacologic interventions will be of only minimal benefit when patients
are evaluated in the context of their habitual low level of cognitive stimulation.
Cognitive Impairment in Schizophrenia 29

Part of the explanation for why clinical trials testing the efficacy of cognitive-
enhancing medications have so far been largely unsuccessful may be that patients in
these trials are not provided with substantive opportunity to utilize the cognitive
benefit that they may have acquired during the drug treatment study. Thus, analo-
gous to the need for physical exercise in an individual who takes steroids to increase
muscle mass, schizophrenia patients in pharmacological intervention trials may
require systematic cognitive training to “exercise” any newfound cognitive poten-
tial that they may have acquired from drug treatment (Keefe et al. 2011d).
Cognitive remediation may provide an excellent platform for enriching the cogni-
tive environment of patients engaged in pharmacologic trials to improve cognition.
Several studies and meta-analysis suggest that cognitive remediation produces
medium effect size improvements in cognitive performance and, when combined
with psychiatric rehabilitation, also improves functional outcomes (McGurk et al.
2007a, b). Additionally, patients find these programs to be enjoyable and engaging,
and they have been linked with increases in participant self-esteem (Wykes et al.
1999). Ongoing treatment with cognitive remediationmay thus provide schizophrenia
patients with the necessary cognitive enrichment and motivation to demonstrate the
true potential of effective cognitive enhancement with pharmacologic intervention.
Recent work suggests that these methods are feasible in clinical trials even at sites
without cognitive remediation experience (Keefe et al. 2012).
3 Conclusions
Cognitive functioning is moderately to severely impaired in patients with schizo-
phrenia. This impairment is the prime driver of the significant disabilities in
occupational, social, and economic functioning in patients with schizophrenia.
The profile of deficits in schizophrenia includes many of the most important aspects
of human cognition: attention, memory, reasoning, and processing speed. While
various efforts are under way to identify specific aspects of neurocognition that may
lie closest to the neurobiological etiology and pathophysiology of the illness, and
may provide relevant convergence with animal models of cognition, standard
neuropsychological measures continue to demonstrate the greatest sensitivity to
functionally relevant cognitive impairment. These measures have been the primary
outcome measures in treatment studies, as exemplified by the MCCB.
There have been several prominent negative treatment trials, including large-
scale studies examining the effects of antipsychotic medications on cognition in
schizophrenia and first-episode psychosis. There have also been a number of
prominent negative studies of add-on treatments, although very few of these studies
have had sufficient statistical power to generate firm conclusions. In addition, a few
recent studies examining novel add-on treatments have produced some encouraging
findings. Ongoing work aims to produce more specific cognitive neuroscience
measures that may be more sensitive targets for pharmacologic intervention.
30 R.S.E. Keefe and P.D. Harvey

Cognitive remediation programs have generated considerable interest as these
methods are far less costly than pharmacologic treatment and are likely to be safer.
A growing consensus suggests that these interventions produce modest gains
for patients with schizophrenia, but the efficacy of the various methods used
has not been empirically investigated. An additional consideration for cognitive
remediation methods is that they may serve as an excellent platform of cognitive
enrichment in trials of pharmacologic treatment to generate the cognitive activity
that may be necessary to register pharmacologic benefit.
References
Addington J, Addington D (1998) Facial affect recognition and information processing in schizo-
phrenia and bipolar disorder. Schizophr Res 32:171–181
Addington J, Addington D (2000) Neurocognitive and social functioning in schizophrenia:
a 2.5 year follow-up study. Schizophr Res 44:47–56
Addington J, Addington D, Maticka-Tyndale E (1991) Cognitive functioning and positive and
negative symptoms in schizophrenia. Schizophr Res 5:123–134
Aleman A, Hijman R, de Haan EH, Kahn RS (1999) Memory impairment in schizophrenia:
a meta-analysis. Am J Psychiatry 156:1358–1366
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders
DSM-IV-TR, Text Revision 4th edn. American Psychiatric Association, Washington, DC,
ISBN 0-89042-024-6
Baddeley A (1992) Working memory. Science 255:556–559, Review
Barch DM, Keefe RSE (2010) Anticipating DSM-V: Opportunities and challenges for cognition
and psychosis. Schizophr Bull 36:43–47
Bell MD, Bryson G (2001) Work rehabilitation in schizophrenia: does cognitive impairment limit
improvement? Schizophr Bull 27:269–279
Bell MD, Greig TC, Kaplan E, Bryson G (1997) Wisconsin Card Sorting Test dimensions in
schizophrenia: factorial, predictive, and divergent validity. J Clin Exp Neuropsychol
19:933–941
Bilder RM, Mukherjee S, Rieder RO, Pandurangi AK (1985) Symptomatic and neuropsychological
components of defect states. Schizophr Bull 11:409–419
Brekke JS, Long JD, Nesbitt N, Sobel E (1997) The impact of service characteristics on functional
outcomes from community support programs for persons with schizophrenia: a growth curve
analysis. J Consult Clin Psychol 65:464–475
Brekke JS, Kohrt B, Green MF (2001) Neuropsychological functioning as a moderator of the
relationship between psychosocial functioning and the subjective experience of self and life in
schizophrenia. Schizophr Bull 27:697–708
Brekke JS, Hoe M, Long J, Green MF (2007) How neurocognition and social cognition influence
functional change during community-based psychosocial rehabilitation for individuals with
schizophrenia. Schizophr Bull 33:1247–1256
Bressi S, Miele L, Bressi C et al (1996) Deficit of central executive component of working memory
in schizophrenia. New Trends Exp Clin Psychiatry 12:243–252
Brewer WJ, Wood SJ, McGorry PD, Francey SM, Phillips LJ, Yung AR, Anderson V, Copolov
DL, Singh B, Velakoulis D, Pantelis C (2003) Impairment of olfactory identification ability in
individuals at ultra-high risk for psychosis who later develop schizophrenia. Am J Psychiatry
160:1790–1794
Cognitive Impairment in Schizophrenia 31
Brewer WJ, Francey SM, Wood SJ, Jackson HJ, Pantelis C, Phillips LJ, Yung AR, Anderson VA,
McGorry PD (2005) Memory impairments identified in people at ultra-high risk for psychosis
who later develop first episode psychosis. Am J Psychiatry 162:71–78
Buchanan RW, Holstein C, Breier A (1994) The comparative efficacy and long-term effect of
clozapine treatment on neuropsychological test performance. Biol Psychiatry 36:717–725
Buchanan RW, Davis M, Goff D, Green MF, Keefe RS, Leon AC, Nuechterlein KH, Laughren T,
Levine R, Stover E, Fenton W, Marder SR (2005) A summary of the FDA-NIMH-MATRICS
workshop on clinical trial design for neurocognitive drugs for schizophrenia. Schizophr Bull
31:5–19
Buchanan RW, Keefe RS, Umbricht D, Green MF, Laughren T, Marder SR (2011a) The FDA-
NIMH-MATRICS guidelines for clinical trial design of cognitive-enhancing drugs: What do
we know 5 years later? Schizophr Bull 37:1209–1017
Buchanan RW, Keefe RS, Lieberman JA, Barch DM, Csernansky JG, Goff DC, Gold JM, GreenMF,
Jarskog LF, Javitt DC, Kimhy D, KrausMS,McEvoy JP, Mesholam-Gately RI, Seidman LJ, Ball
MP, McMahon RP, Kern RS, Robinson J, Marder SR (2011b) A randomized clinical trial of
MK-0777 for the treatment of cognitive impairments in people with schizophrenia. Biol Psychia-
try 69:442–449
Burdick KE, Goldberg TE, Cornblatt BA, Keefe RS, Gopin CB, Derosse P, Braga RJ, Malhotra AK
(2011) The MATRICS consensus cognitive battery in patients with bipolar I disorder.
Neuropsychopharmacology 36:1587–1592
Callicott JH, Mattay VS, Bertolino A, Finn K, Coppola R, Frank JA, Goldberg TE,Weinberger DR
(1999) Physiological characteristics of capacity constraints in working memory as revealed by
functional MRI. Cereb Cortex 9:20–26
Cannon TD, Cadenhead K, Cornblatt B,Woods SW, Addington J,Walker E, Seidman LJ, Perkins D,
TsuangM,McGlashan T,Heinssen R (2008) Prediction of psychosis in youth at high clinical risk:
a multisite longitudinal study in North America. Arch Gen Psychiatry 65:28–37
Carter CS, Barch DM (2007) Cognitive neuroscience-based approaches to measuring and improving
treatment effects on cognition in schizophrenia: the CNTRICS initiative. Schizophr Bull
33:1131–1137
Carter C, Robertson L, Nordahl T, Chaderjian M, Kraft L, O’Shora-Celaya L (1996) Spatial
working memory deficits and their relationship to negative symptoms in unmedicated schizo-
phrenia patients. Biol Psychiatry 40:930–932
Carter CS, Barch DM, Buchanan RW, Bullmore E, Krystal JH, Cohen J, Geyer M, Green M,
Nuechterlein KH, Robbins T, Silverstein S, Smith EE, Strauss M, Wykes T, Heinssen R (2008)
Identifying cognitive mechanisms targeted for treatment development in schizophrenia: An
overview of the first meeting of the Cognitive Neuroscience Treatment Research to Improve
Cognition in Schizophrenia Initiative. Biol Psychiatry 64:4–10
Caspi A, Reichenberg A, Weiser M, Rabinowitz J, Kaplan Z, Knobler H, Davidson-Sagi N,
Davidson M (2003) Cognitive performance in schizophrenia patients assessed before and
following the first psychotic episode. Schizophr Res 65:87–94
Corcoran R, Mercer G, Frith CD (1995) Schizophrenia, symptomatology and social inference:
investigating “theory of mind” in people with schizophrenia. Schizophr Res 17:5–13
Corrigan PW, Liberman RP, Engel JD (1990) From noncompliance to collaboration in the
treatment of schizophrenia. Hosp Commun Psychiatry 41:1203–1211
David AS, Malmberg A, Brandt L, Allebeck P, Lewis G (1997) IQ and risk for schizophrenia:
A population-based cohort study. Psychol Med 27:1311–1323
Davidson M, Harvey PD, Powchik P, Parrella M, White L, Knobler HY, Losonczy MF, Keefe RS,
Frecska E (1995) Severity of symptoms in chronically institutionalized geriatric schizophrenic
patients. Am J Psychiatry 152:197–207
Davidson M, Reichenberg A, Rabinowitz J, Weiser M, Kaplan Z, Mark M (1999) Behavioral and
intellectual markers for schizophrenia in apparently healthy male adolescents. Am J Psychiatry
156:1328–1335
Davis SM, Koch GG, Davis CE, LaVange LM (2003) Statistical approaches to effectiveness
measurement and outcome-driven re-randomizations in the Clinical Antipsychotic Trials
of Intervention Effectiveness (CATIE) studies. Schizophr Bull 29:73–80
32 R.S.E. Keefe and P.D. Harvey

Dias EC, Butler PD, Hoptman MJ, Javitt DC (2011) Early sensory contributions to contextual
encoding deficits in schizophrenia. Arch Gen Psychiatry 68:654–664
Dickerson F, Boronow JJ, Ringel N, Parente F (1999) Social functioning and neurocognitive
deficits in outpatients with schizophrenia: A 2-year follow-up. Schizophr Res 37:13–20
Dickinson D, Ramsey ME, Gold JM (2007) Overlooking the obvious: A meta-analytic comparison
of digit symbol coding tasks and other cognitive measures in schizophrenia. Arch Gen
Psychiatry 64:532–542
Donohoe G, Owens N, O’Donnell C, Burke T, Moore L, Tobin A, O’Callaghan E (2001)
Predictors of compliance with neuroleptic medication among inpatients with schizophrenia:
A discriminant function analysis. Eur Psychiatry 16:293–298
Drury VM, Robinson EJ, Birchwood M (1998) Theory of mind skills during an acute episode of
psychosis and following recovery. Psychol Med 28:1101–1112
Edwards J, Pattison PE, Jackson HJ, Wales RJ (2001) Facial affect and affective prosody
recognition in first-episode schizophrenia. Schizophr Res 48:235–253
Ertugrul A, Ulug B (2002) The influence of neurocognitive deficits and symptoms on disability in
schizophrenia. Acta Psychiatr Scand 105:196–201
Evans JD, Heaton RK, Paulsen JS, Palmer BW, Patterson T, Jeste DV (2003) The relationship of
neuropsychological abilities to specific domains of functional capacity in older schizophrenic
patients. Biol Psychiatry 53:422–430
Fenton WS, Blyler CR, Heinssen RK (1997) Determinants of medication compliance in schizo-
phrenia: empirical and clinical findings. Schizophr Bull 23:637–651
Friedman L (2002) Psychoanalysis: practice and technique. J Am Psychoanal Assoc 50:727–732
Fuller R, Nopoulos P, Arndt S, O’Leary D, Ho BC, Andreasen NC (2002) Longitudinal assessment
of premorbid cognitive functioning in patients with schizophrenia through examination of
standardized scholastic test performance. Am J Psychiatry 159:1183–1189
Gaebel W, W€olwer W (1992) Facial expression and emotional face recognition in schizophrenia
and depression. Eur Arch Psychiatry Clin Neurosci 242:46–52
George TP, Ziedonis DM, Feingold A, Pepper WT, Satterburg CA, Winkel J, Rounsaville BJ,
Kosten TR (2000) Nicotine transdermal patch and atypical antipsychotic medications for
smoking cessation in schizophrenia. Am J Psychiatry 157:1835–1842
Gold JM, Goldberg RW, McNary SW, Dixon LB, Lehman AF (2002) Cognitive correlates of job
tenure among patients with severe mental illness. Am J Psychiatry 159:1395–1402
Gold JM, Wilk CM, McMahon RP, Buchanan RW, Luck SJ (2003) Working memory for visual
features and conjunctions in schizophrenia. J Abnorm Psychol 112:61–71
Goldberg TE, Weinberger DR, Berman KF, Pliskin NH, Podd MH (1987) Further evidence for
dementia of the prefrontal type in schizophrenia? A controlled study of teaching the Wisconsin
Card Sorting Test. Arch Gen Psychiatry 44:1008–1014
Goldberg TE, Ragland JD, Torrey EF, Gold JM, Bigelow LB, Weinberger DR (1990) Neuropsy-
chological assessment of monozygotic twins discordant for schizophrenia. Arch Gen Psychia-
try 47:1066–1072
Goldman-Rakic PS (1987) Circuitry of the frontal association cortex and its relevance to dementia.
Arch Gerontol Geriatr 6:299–309
Goldman-Rakic PS (1994) Working memory dysfunction in schizophrenia. J Neuropsychiatry
Clin Neurosci 6:348–357
Green MF (1996) What are the functional consequences of neurocognitive deficits in schizophre-
nia? Am J Psychiatry 153:321–330
Green MF, Kern RS, Braff DL, Mintz J (2000) Neurocognitive deficits and functional outcome in
schizophrenia: are we measuring the “right stuff”? Schizophr Bull 26:119–136, Review
Green MF, Nuechterlein KH, Gold JM, Barch DM, Cohen J, Essock S, Fenton WS, Frese F,
Goldberg TE, Heaton RK, Keefe RSE, Kern RS, Kraemer H, Stover E, Weinberger DR,
Zalcman S, Marder SR (2004) Approaching a consensus cognitive battery for clinical trials
in schizophrenia: The NIMH-MATRICS conference to select cognitive domains and test
criteria. Biol Psychiatry 56:301–307
Green MF, Schooler NR, Kern RS, Frese FJ, Granberry W, Harvey PD, Karson CN, Peters N,
Stewart M, Seidman LJ, Sonnenberg J, Stone WS, Walling D, Stover E, Marder SR (2011)
Cognitive Impairment in Schizophrenia 33
Evaluation of functionally meaningful measures for clinical trials of cognition enhancement in
schizophrenia. Am J Psychiatry 168:400–407
Harvey PD, Keefe RSE (1997) Cognitive impairment in schizophrenia and implications of atypical
neuroleptic treatment. CNS Spectrums 2:1–11
Harvey PD, Rabinowitz J, Eerdekens M, DavidsonM (2005) Treatment of cognitive impairment in
early psychosis: a comparison of risperidone and haloperidol in a large long-term trial. Am J
Psychiatry 162:1888–1895
Harvey PD, Velligan DI, Bellack AS (2007) Performance-based measures of functional skills:
usefulness in clinical treatment studies. Schizophr Bull 33:1138–1148
Hawkins KA, Addington J, Keefe RS, Christensen B, Perkins DO, Zipursky R, Woods SW,
Miller TJ, Marquez E, Breier A, McGlashan TH (2004) Neuropsychological status of subjects
at high risk for a first episode of psychosis. Schizophr Res 67:115–122
Heaton RK, Pendleton MG (1981) Use of Neuropsychological tests to predict adult patients’
everyday functioning. J Consult Clin Psychol 49:807–821
Heinrichs RW, Zakzanis KK (1998) Neurocognitive deficit in schizophrenia: a quantitative review
of the evidence. Neuropsychology 12:426–445
Hyman SE, Fenton WS (2003) Medicine. What are the right targets for psychopharmacology?
Science 299:350–351
Jarboe KS, Schwartz SK (1999) The relationship between medication noncompliance and cogni-
tive function in patients with schizophrenia. J Am Psychiatr Nurses Assoc 5:S2–S8
Jeste SD, Patterson TL, Palmer BW, Dolder CR, Goldman S, Jeste DV (2003) Cognitive predictors
of medication adherence among middle-aged and older outpatients with schizophrenia.
Schizophr Res 63:49–58
Jones P, Rodgers B, Murray R, Marmot M (1994) Child development risk factors for adult
schizophrenia in the British 1946 birth cohort. Lancet 344:1398–1402
Keefe RSE (1995) The contribution of neuropsychology to psychiatry. Am J Psychiatry 152:6–15
Keefe RSE (2000) Working memory dysfunction and its relevance in schizophrenia. In: Sharma T,
Harvey PD (eds) Cognition in schizophrenia: characteristics, correlates, and treatment. Oxford
University Press, Oxford, pp 16–49
Keefe RSE, Fenton WS (2007) How should DSM-V criteria for schizophrenia include cognitive
impairment? Schizophr Bull 33:912–920
Keefe RSE, Harvey PD (2008) Implementation considerations for multi-site clinical trials
with cognitive neuroscience tasks. Schizophr Bull 34:656–663
Keefe RSE, Kraus MS (2009) Measuring memory-prediction errors and their consequences
in youth at risk for schizophrenia. Ann Acad Med Sing 38:414–416
Keefe RSE, Arnold MC, Bayen UJ, McEvoy JP, Wilson WH (2002) Source monitoring deficits
for self-generated stimuli in schizophrenia: Multinomial modeling of data from three sources.
Schizophr Res 57:51–67
Keefe RSE, Seidman LJ, Christensen BK, Hamer RM, Sharma T, Sitskoorn MM, Lewine RR,
Yurgelun-Todd DA, Gur RC, Tohen M, Tollefson GD, Sanger TM, Lieberman JA (2004)
Comparative effect of atypical and conventional antipsychotic drugs on neurocognition in
first-episode psychosis: A randomized double-blind trial of olanzapine versus low-doses of
haloperidol. Am J Psychiatry 161:985–99
Keefe RSE, Eesley CE, Poe M (2005) Defining a cognitive function decrement in schizophrenia.
Biol Psychiatry 57:688–691
Keefe RSE, Bilder RM, Harvey PD, Sm D, Palmer BW, Gold JM, Meltzer HY, Green MF,
Miller DD, Canive JM, Adler LW, Manschreck TC, Swartz M, Rosenheck R, Perkins DO,
Walker TM, Stroup TS, McEvoy JP, Lieberman JA (2006a) Baseline neurocognitive deficits in
the CATIE schizophrenia trial. Neuropsychopharmacology 31:2033–2046
Keefe RSE, Perkins DO, Gu H, Zipursky RB, Christensen BK, Lieberman JA (2006b) A
longitudinal study of neurocognitive function in individuals at-risk for psychosis. Schizophr
Res 88:26–35
Keefe RSE, Bilder RM, Davis SM, Harvey PD, Palmer BW, Gold JM, Meltzer HY, Green MF,
Capuano G, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, Davis CE,
Hasiao JK, Lieberman JA, CATIE Investigators, Neurocognitive Working Group (2007a)
34 R.S.E. Keefe and P.D. Harvey
Neurocognitive effects of antipsychotic medications in patients with chronic schizophrenia in
the CATIE trial. Arch Gen Psychiatry 64:633–647
Keefe RSE, Malhotra AK, Meltzer H, Kane JM, Buchanan RW, Murthy A, Sovel M, Li C,
Goldman R (2007b) Efficacy and safety of donepezil in patients with schizophrenia or
schizoaffective disorder: Significant placebo/practice effects in a 12-week, randomized,
double-blind, placebo-controlled trial. Neuropsychopharmacology 33:1217–1228
Keefe RSE, Fox KH, Harvey PD, Cucchiaro J, Siu C, Loebel A (2011a) Characteristics of the
MATRICS consensus cognitive battery in a 29 site antipsychotic schizophrenia clinical trial.
Schizophr Res 125:161–168
Keefe RSE, Kraus MS, Krishnan RR (2011b) Failures in learning-dependent predictive perception
as the key cognitive vulnerability to psychosis in schizophrenia. Neuropsychopharmacology
36:367–380
Keefe R, Buchanan R, Marder S et al (2011c) Clinical trials of potential cognitive-enhancing
drugs in schizophrenia: What have we learned so far? Annual Meeting of NCDEU, Boca
Raton, FL
Keefe RSE, Vinogradov S, Medalia A, Silverstein SM, Bell MD, Dickinson D, Ventura J,
Marder SR, Stroup TS (2011d) Report from the Working Group Conference on multi-site
trial design for cognitive remediation in schizophrenia. Schizophr Bull 37:1057–1065
Keefe RSE, Vinogradov S, Medalia A, Buckley PF, Caroff SN, d’Souza DC, Harvey PD,
Graham KA, Hamer RM, Marder SM, Miller DD, Olson SJ, Patel JK, Velligan D, Walker TM,
Haim AJ, Stroup TS (2012) Feasibility and pilot efficacy results from the multi-site Cognitive
Remediation in the Schizophrenia Trials Network (CRSTN) study. J Clin Psychiatry 73:
1016–1022
Kern RS, Nuechterlein KH, Green MF, Baade LE, Fenton WS, Gold JM, Keefe RS, Mesholam-
Gately R, Mintz J, Seidman LJ, Stover E, Marder SR (2008) The MATRICS consensus
cognitive battery: Part 2. Co-norming and standardization. Am J Psychiatry 165:214–220
Kraemer HC, Frank E (2010) Evaluation of comparative treatment trials: assessing clinical
benefits and risks for patients, rather than statistical effects on measures. J Am Med Assoc
304:683–684
Kraus MS, Keefe RSE, Krishnan RK (2009) Memory-prediction errors and their consequences
in schizophrenia. Neuropsychol Rev 19:336–352
Kremen WS, Seidman LJ, Faraone SV, Toomey R, Tsuang MT (2000) The paradox of normal
neuropsychological function in schizophrenia. J Abnorm Psychol 109:743–752
Krishnan RR, Fivaz M, Kraus M, Keefe RSE (2011a) Hierarchical temporal processing deficit
model of reality distortion and psychoses. Mol Psychiatry 16:129–144
Krishnan RR, Kraus MS, Keefe RSE (2011b) Comprehensive model of how reality distortion
and symptoms occur in schizophrenia. Could impairment in learning-dependent predictive
perception account for the manifestations of schizophrenia? Psychiatry Clin Neurosci
65:305–317
Leung WW, Bowi CR, Harvey PD (2008) Functional implications of neuropsychological normality
and symptom remission in older outpatients diagnosed with schizophrenia: A cross-sectional
study. J Int Neuropsychol Soc 14:479–488
Lysaker P, Bell M (1995) Work rehabilitation and improvements in insight in schizophrenia.
J Nerv Ment Dis 183:103–106
Malla AK, Norman RM, Manchanda R, Townsend L (2002) Symptoms, cognition, treatment
adherence and functional outcome in first-episode psychosis. Psychol Med 32:1109–1119
Mausbach BT, Bowie CR, Harvey PD, Twamley EW, Goldman SR, Jeste DV, Patterson TL
(2008) Usefulness of the UCSD performance-based skills assessment (UPSA) for predicting
residential independence in patients with chronic schizophrenia. J Psychiatr Res 42:320–327
McClure MM, Bowie CR, Patterson TL, Heaton RK, Weaver C, Anderson H, Harvey PD (2007)
Correlations of functional capacity and neuropsychological performance in older patients with
schizophrenia: evidence for specificity of relationships? Schizophr Res 89:330–338
McGurk SR, Meltzer HY (2000) The role of cognition in vocational functioning in schizophrenia.
Schizophr Res 45:175–184
Cognitive Impairment in Schizophrenia 35
McGurk SR, Mueser KT, Harvey PD, LaPuglia R, Marder J (2003) Cognitive and symptom
predictors of work outcomes for clients with schizophrenia in supported employment.
Psychiatr Serv 54:1129–1135
McGurk SR, Mueser KT, Feldman K, Wolfe R, Pascaris A (2007a) Cognitive training for
supported employment: 2–3 year outcomes of a randomized controlled trial. Am J Psychiatry
164:437–441
McGurk SR, Twamley EW, Sitzer DI, McHugo GJ, Mueser KT (2007b) A meta-analysis
of cognitive remediation in schizophrenia. Am J Psychiatry 164:1791–1802
Mohamed S, Paulsen JS, O’Leary D, Arndt S, Andreasen N (1999) Generalized cognitive deficits
in schizophrenia: A study of first-episode patients. Arch Gen Psychiatry 56:749–754
Mohamed S, Rosenheck R, Swartz M, Stroup S, Lieberman JA, Keefe RS (2008) Relationship of
cognition and psychopathology to functional impairment in schizophrenia. Am J Psychiatry
165:978–987
Morrison RL, Bellack AS, Mueser KT (1988) Deficits in facial-affect recognition and schizophrenia.
Schizophr Bull 14:67–83, Review
Mueser KT, Bellack AS, Douglas MS, Wade JH (1991) Prediction of social skill acquisition in
schizophrenic and major affective disorder patients from memory and symptomatology.
Psychiatry Res 37:281–296
Nuechterlein KH, Barch DM, Gold JM, Goldberg TE, Green MF, Heaton RK (2004) Identification
of separable cognitive factors in schizophrenia. Schizophr Res 72:29–39, Review
Nuechterlein KH, Green MF, Kern RS, Baade LE, Barch DM, Cohen JD, Essock S, Fenton WS,
Frese FJ III, Gold JM, Goldberg T, Heaton RK, Keefe RS, Kraemer H, Mesholam-Gately R,
Seidman LJ, Stover E, Weinberger DR, Young AS, Zalcman S, Marder SR (2008)
The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity.
Am J Psychiatry 165:203–213
Palmer BW, Heaton RK, Paulsen JS, Kuck J, Braff D, Harris MJ, Zisook S, Jeste DV (1997) Is it
possible to be schizophrenic yet neuropsychologically normal? Neuropsychology 11:437–446
Patterson TL, Goldman S, McKibbin CL, Hughs T, Jeste DV (2001) UCSD Performance-Based
Skills Assessment: development of a new measure of everyday functioning for severely
mentally ill adults. Schizophr Bull 27:235–245
Patterson TL, Lacro J, McKibbin CL, Moscona S, Hughs T, Jeste DV (2002) Medication
management ability assessment: results from a performance-based measure in older outpatients
with schizophrenia. J Clin Psychopharmacol 22:11–19
Penn DL, Spaulding W, Reed D, Sullivan M (1996) The relationship of social cognition to ward
behavior in chronic schizophrenia. Schizophr Res 20:327–335
Penn DL, Corrigan PW, Bentall RP, Racenstein JM, Newman L (1997) Social cognition
in schizophrenia. Psychol Bull 121:114–132
Pinkham AE, Loughead J, Ruparel K, Overton E, Gur RE, Gur RC (2011) Abnormal modulation
of amygdala activity in schizophrenia in response to direct- and averted-gaze threat-related
facial expressions. Am J Psychiatry 168:293–301
Reichenberg A, Harvey PD, Bowie CR, Mojtabai R, Rabinowitz J, Heaton RK, Bromet E (2009)
Neuropsychological function and dysfunction in schizophrenia and psychotic affective
disorders. Schizophr Bull 35:1022–1029
Reichenberg A, Caspi A, Harrington H, Houts R, Keefe RS, Murray RM, Poulton R, Moffitt TE
(2010) Static and dynamic cognitive deficits in childhood preceding adult schizophrenia:
A 30-year study. Am J Psychiatry 167:160–169
Reilly JL, Harris MSH, Keshavan MS, Sweeney JA (2006) Adverse effects of risperidone on
spatial working memory in first-episode schizophrenia. Arch Gen Psychiatry 63:1189–1197
Rosenheck R, Doyle J, Leslie D, Fontana A (2003) Changing environments and alternative
perspectives in evaluating the cost-effectiveness of new antipsychotic drugs. Schizophr
Bull 29:81–93
Sarfati Y, Hardy-Bayle MC, Nadel J et al (1997) Attribution of mental states to others
by schizophrenic patients. Cogn Neuropsychiatr 2:1–17
36 R.S.E. Keefe and P.D. Harvey

Saykin AJ, Gur RC, Gur RE, Mozley PD, Mozley LH, Resnick SM, Kester DB, Stafiniak P (1991)
Neuropsychological function in schizophrenia. Selective impairment in memory and learning.
Arch Gen Psychiatry 48:618–624
Seidman LJ, Giuliano AJ, Meyer EC, Addington J, Cadenhead KS, Cannon TD, McGlashan TH,
Perkins DO, Tsuang MT, Walker EF, Woods SW, Bearden CE, Christensen BK, Hawkins K,
Heaton R, Keefe RS, Heinssen R, Cornblatt BA, North American Prodrome Longitudinal
Study (NAPLS) Group (2010) Neuropsychology of the prodrome to psychosis in the NAPLS
consortium: relationship to family history and conversion to psychosis. Arch Gen Psychiatry
67:578–588
Sevy S, Davidson M (1995) The cost of cognitive impairment in schizophrenia. Schizophr Res
17:1–3
Silver H, Feldman P, Bilker W, Gur RC (2003) Working memory deficit as a core neuropsycho-
logical dysfunction in schizophrenia. Am J Psychiatry 160:1809–1816
Strauss ME (1993) Relations of symptoms to cognitive deficits in schizophrenia. Schizophr Bull
19:215–231, Review
Stroup TS, Lieberman JA, McEvoy JP, Swartz MS, Davis SM, Rosenheck RA, Perkins DO,
Keefe RS, Davis CE, Severe J, Hsiao JK, Investigators CATIE (2006) Effectiveness of
olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia
after discontinuing a previous atypical antipsychotic. Am J Psychiatry 13:611–622
Swartz MS, Perkins DO, Stroup TS, McEvoy JP, Nieri JM, Haak DC (2003) Assessing clinical and
functional outcomes in the Clinical Antipsychotic Trials of Intervention Effectiveness
(CATIE) schizophrenia trial. Schizophr Bull 29:33–43
Sweet RA, Pollock BG, Mulsant BH, Rosen J, Sorisio D, Kirshner M, Henteleff R, DeMichele MA
(2000) Pharmacologic Profile of Perphenazine’s Metabolites. J Clin Psychopharmacol
20:181–187
Tamlyn D, McKenna PJ, Mortimer AM, Lund CE, Hammond S, Baddeley AD (1992) Memory
impairment in schizophrenia: Its extent, affiliations and neuropsychological character. Psychol
Med 22:101–115
Tan HY, Choo WC, Fones CS, Chee MW (2005) fMRI study of maintenance and manipulation
processes within working memory in first-episode schizophrenia. Am J Psychiatry
162:1849–1858
Trumbetta SL, Mueser KT (2001) Social functioning and its relationship to cognitive deficits over
the course of schizophrenia. In: Keefe RSE, McEvoy JP (eds) Negative Symptom and
Cognitive Deficit Treatment Response in Schizophrenia. American Psychiatric Association,
Washington, DC, pp 33–67
Twamley EW, Doshi RR, Nayak GV, Palmer BW, Golshan S, Heaton RK, Patterson TL, Jeste DV
(2003) Generalized cognitive impairments, ability to perform everyday tasks, and level of
independence in community living situations of older patients with psychosis. Am J Psychiatry
159:2013–2020
Van Putten T, Marder SR, Wirshing WC, Aravagiri M, Chabert N (1991) Neuroleptic plasma
levels. Schizophr Bull 17:197–216
Velligan DI, Bow-Thomas CC, Mahurin RK, Miller AL, Halgunseth LC (2000) Do specific
neurocognitive deficits predict specific domains of community function in schizophrenia?
J Nerv Ment Dis 188:518–524
Walker E, Lewine RJ (1988) The positive/negative symptom distinction in schizophrenia. Validity
and etiological relevance. Schizophr Res 1:315–328
Weinberger DR (1987) Implications of normal brain development for the pathogenesis of
schizophrenia. Arch Gen Psychiatry 44:660–669
Wykes T, Reeder C, Corner J, Williams C, Everitt B (1999) The effects of neurocognitive
remediation on executive processing in patients with schizophrenia. Schizophr Bull
25:291–307
Yung AR, McGorry PD (1996) The prodromal phase of first-episode psychosis: past and current
conceptualizations. Schizophr Bull 22:353–370
Cognitive Impairment in Schizophrenia 37
http://www.springer.com/978-3-642-25757-5
Related Documents











