Cognitive Deficits in Olivopontocerebellar Atrophy: Implications for the Cholinergic Hypothesis of Alzheimer's Dementia Stephen J. Ksh, PhD,"IS Munir El-Awar, MD," Lawrence Schut, MD,' Larry Leach, PhD," Marlene Oscar-Berrnan, PhD,**ti. and Morris Freedman, MD8 - A cerebral cortical cholinergic reduction in dominantly inherited olivopontocerebellar atrophy (OPCA) was recently described. Although the magnitude of the cholinergic reduction was similar to that observed in Alzheimer's disease (AD), none of the OPCA patients was reported to have been demented. We now describe a comprehensive neuro- psychological assessment of 11 patients from cine of the OPCA pedigrees which we examined biochemically. Detailed neuropsychological testing disclosed previously unrecognized deficits in verbal and nonverbal intelligence, memory, and frontal system function which were positively correlated with the severity of cerebellar ataxia. However, our OPCA patients appeared to be at most only mildly disabled by their cognitive impairment and scored within or close to the normal range on a simple mental statiis screening examination. This, as well as an absence of any aphasia, apraxia, or agnosia, contrasts with the profile and severity observed in advanced AD dementia, characterized by a similar cortical cholinergic deficit. This finding also suggests that cholinergic reduction may explain only part of the pathophysiology underlying the dementia of AD. Kish SJ, El-Awai. M, Schut L, Leach L, Oscar-Berman M, Freedman M. Lognitive deficits in olivopontocerebellar atrophy: implications for the cholinergic hypothesis of Alzheimer's dementia. Ann Neurol 1988;24:200--206 Much circumstantial evidence suggests that part of the cognitive dysfunction of patients with Alzheimer's dis- ease (AD) results from reduced cholinergic innerva- tion of the cerebral cortical and limbic brain. This evi- dence is derived from autopsy and biopsy brain studies demonstrating reduced activity in AD of the choliner- gic enzymes choline acetyltransferase and acetyl- cholinesterase, as well as a loss of cholinergic neurons emanating from the nucleus basalis-septum brain area and terminating in cerebral cortex and limbic struc- tures [cf 251. These findings, together with results of clinical pharmacological studies demonstrating cogni- tive impairment after anticholinergic drug administra- tion [lo, 341, and nonhuman experimental studies in- dicating impaired performance due to lesion of the cholinergic nucleus basalis of Meynert innervation to cortex [cf 41, provide the basis for the cholinergic hy- pothesis of AD dementia [Z, 3, 251. Should the brain cholinergic dysfunction of ,4D ac- tually represent one of the critical biochemical causes of AD dementia [25], a cholinergic reduction in brain of patients without AD would presumably be associ- ated with a cognitive impairment similar to that ob- served in AD. We were thus surprised to observe a group of patients afflicted with a cerebellar ataxia clis- order, dominantly inherited olivopontocerebellar at- rophy (OPCA), having a cerebral cortical cholinergic deficiency as severe as that in AD brain, but without obvious cognitive impairment 121, 221. As part of a prospective neurobehaviord-neuropatholo~ical-bio- chemical study, we examined 14 OPCA patients from the largest pedigree biochemically studied 1321 to as- sess the presence of any cognitive changes. We report significant though generally mild neuropsychological deficits in our OPCA patients, with a neurobehavioral profile and severity differing from those typically ob- served in AD. Patients and Methods We examined 14 patients with dominantly inherited OI'<,A from the Schut [32} pedigree This kindred, which now spans eight generations, was originally dex ribeci by Gray 'ind From the 'Huinan Bran LAboratory, Clarke Institute of Psvchiatry, Toronto, the Departments of tpsychiatry, $Pharrnacolosy, and 9Medicine (Neurology), Universiry of Toronto, 'Baycrest Center tor Geriatric Care, Toronto, 'Mount Sinai Hospital Research Insti- cute, T ~ ~ ~ ) ~ ~ ~ , ontarlo, VA Medical Centers, x~~~~~~~~~ s, MN, and **Bosron, MA, and the i tDepartmrnts of Psychiatry a r d Neu- rology, Boston Universiry School ot Medicine, Boston, MA Received Oct 30, 1987, and in revised form Jan 27, 1')XX Acccpttr\ for publication Feb 4, 1988 Address correspondence to Dr ffish, Human Bran I.ddhorCitory, Clarke Institute of Psychiatry, 250 College Sr, Toronro. Omrio M5T 1R8 200 Copyright 0 1988 by the American Neurological Association

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cognitive Deficits in Olivopontocerebellar Atrophy: Implications for the Cholinergic
Hypothesis of Alzheimer's Dementia Stephen J. Ksh, PhD,"IS Munir El-Awar, MD," Lawrence Schut, MD,' Larry Leach, PhD,"
Marlene Oscar-Berrnan, PhD,**ti. and Morris Freedman, MD8
- A cerebral cortical cholinergic reduction in dominantly inherited olivopontocerebellar atrophy (OPCA) was recently described. Although the magnitude of the cholinergic reduction was similar to that observed in Alzheimer's disease (AD), none of the OPCA patients was reported to have been demented. We now describe a comprehensive neuro- psychological assessment of 11 patients from cine of the OPCA pedigrees which we examined biochemically. Detailed neuropsychological testing disclosed previously unrecognized deficits in verbal and nonverbal intelligence, memory, and frontal system function which were positively correlated with the severity of cerebellar ataxia. However, our OPCA patients appeared to be at most only mildly disabled by their cognitive impairment and scored within or close to the normal range on a simple mental statiis screening examination. This, as well as an absence of any aphasia, apraxia, or agnosia, contrasts with the profile and severity observed in advanced AD dementia, characterized by a similar cortical cholinergic deficit. This finding also suggests that cholinergic reduction may explain only part of the pathophysiology underlying the dementia of AD.
Kish SJ, El-Awai. M, Schut L, Leach L, Oscar-Berman M, Freedman M. Lognitive deficits i n olivopontocerebellar atrophy: implications for the cholinergic hypothesis
of Alzheimer's dementia. Ann Neurol 1988;24:200--206
Much circumstantial evidence suggests that part of the cognitive dysfunction of patients with Alzheimer's dis- ease (AD) results from reduced cholinergic innerva- tion of the cerebral cortical and limbic brain. This evi- dence is derived from autopsy and biopsy brain studies demonstrating reduced activity in AD of the choliner- gic enzymes choline acetyltransferase and acetyl- cholinesterase, as well as a loss of cholinergic neurons emanating from the nucleus basalis-septum brain area and terminating in cerebral cortex and limbic struc- tures [cf 251. These findings, together with results of clinical pharmacological studies demonstrating cogni- tive impairment after anticholinergic drug administra- tion [lo, 341, and nonhuman experimental studies in- dicating impaired performance due to lesion of the cholinergic nucleus basalis of Meynert innervation to cortex [cf 41, provide the basis for the cholinergic hy- pothesis of AD dementia [Z, 3 , 251.
Should the brain cholinergic dysfunction of ,4D ac- tually represent one of the critical biochemical causes of AD dementia [ 2 5 ] , a cholinergic reduction in brain
of patients without A D would presumably be associ- ated with a cognitive impairment similar to that ob- served in AD. We were thus surprised to observe a group of patients afflicted with a cerebellar ataxia clis- order, dominantly inherited olivopontocerebellar at- rophy (OPCA), having a cerebral cortical cholinergic deficiency as severe as that in AD brain, but without obvious cognitive impairment 121, 221. As part of a prospective neurobehaviord-neuropatholo~ical-bio- chemical study, we examined 14 OPCA patients from the largest pedigree biochemically studied 1321 to as- sess the presence of any cognitive changes. We report significant though generally mild neuropsychological deficits in our OPCA patients, with a neurobehavioral profile and severity differing from those typically ob- served in AD.
Patients and Methods We examined 14 patients with dominantly inherited OI'<,A from the Schut [32} pedigree This kindred, which now spans eight generations, was originally dex ribeci by Gray 'ind
From the 'Huinan B r a n LAboratory, Clarke Institute of Psvchiatry, Toronto, the Departments of tpsychiatry, $Pharrnacolosy, and 9Medicine (Neurology), Universiry of Toronto, 'Baycrest Center tor Geriatric Care, Toronto, 'Mount Sinai Hospital Research Insti- cute, T ~ ~ ~ ) ~ ~ ~ , ontarlo, VA Medical Centers, x~~~~~~~~~ s, MN, and **Bosron, MA, and the i tDepartmrnts of Psychiatry a rd Neu- rology, Boston Universiry School ot Medicine, Boston, MA
Received Oct 30, 1987, and in revised form Jan 2 7 , 1')XX Acccpttr\ for publication Feb 4 , 1988 Address correspondence to Dr ffish, Human Bran I.ddhorCitory, Clarke Institute of Psychiatry, 250 College S r , Toronro. O m r i o M5T 1R8
200 Copyright 0 1988 by the American Neurological Association

Oliver { 161 and has been followed continuously. The auto- soma1 dominant locus resides on a region 15 centimorgans telomeric of HLA-A on the short arm of chromosome 6 C29l.
The diagnosis of dominantly inherited OPCA was made on the basis of clinical signs (limb and gait ataxia, dysarthria, dysphagia). Each patient received a general neurological ex- amination and a bedside mental status assessment. The neurological severity of the disorder was scored using the Ataxia Clinical Rating Scale 1271. This scale has been suc- cessfully used to assess patients with ataxia, including patients with OPCA from the Schut pedigree (32) . A battery of standardized neuropsychological tests was administered to characterize and quantify cognitive deficits in the OPCA pa- tients. To minimize any influence on test performance by impairment in articulation and motor function, all of the neuropsychological tests placed minimal or no reliance on complex motor tasks. The same neurological and neuro- psychological tests were administered to 14 control subjects, equated for age (controls: 32 2 8 years, mean -+ SD; OPCA: 34 t 8 years), educational status (controls: 12 ? 3 years; OPCA: 13 5 2 years), and sex ratio (8 male, 6 female for both groups).
The following neuropsychological tests were administered. First, tests of verbal and nonverbal intellectual ability were given, including the following:
Mini-Mental State Examination (MMSE) [8 , 13): MMSE scores were prorated for the patients who could not write, draw, or fold paper. Wechsler Adult Intelligence Scale-Revised (WAIS-R, verbal subtest) 1371: there are six verbal subtests of the WAIS-R-Information, Digit Span, Vocabulary, Arith- metic, Comprehension, and Similarities. Peabody Picture Vocabulary Test (PPVT) 1111: the PPVT measures verbal intellectual ability. After each of a maximum of 150 words is read aloud by the examiner, the subject is asked to indicate its meaning by selecting the correct one of four pictures shown on a plate. Raven’s Colored Progressive Matrices (RCPM) [28]: the RCPM measures nonverbal reasoning ability. Subjects are presented with a series of visual patterns, each with one part removed, and must select the missing part from a multiple choice array.
Second, memory was tested with the Wechsler Memory Scale (MMS) {36]. The WMS consists of sections on Infor- mation, Orientation, Mental Control, Digit Span, Logical Memory (Story Recall), Paired Associate Learning, and Vi- sual Reproductions. The visual reproductions section was not given to patients whose ataxia interfered with the mechanics of drawing. Scores of those patients were prorated.
Third, attention was tested with the following:
1. Modified Continuous Performance Test (MCPT) (231 (modified by Kaplan, personal communication). The MCPT is a test of attention in which the patient raises his hand every time he hears the letter “A” in a recording of randomly presented letters of the alphabet.
2. Digit Span Forward. 3. Digit Span Backward.
Fourth, naming was tested with the Boston Naming Test (BNT) {201. This standardized naming test contains drawings of 60 items arranged by increasing difficulty.
Fifth, visuospatial function was measured with the Hooper Visual Organization Test [ 181, which measures visuospatial organizational ability. Subjects must identify 30 drawings of fragmented objects.
Sixth, frontal system function was measured with two tests:
1. Wisconsin Card Sorting (WCS) Test [7, 151 tests concept formation and provides a sensitive measure of persevera- tion due to frontal system dysfunction. Subjects sort 128 cards according to a predetermined principle (form. n u n - ber, or color) which must be deduced from the e x a m iner’s feedback. After sorting 10 cards correctly, the prin- ciple is changed and must again be deduced by the subject. Subjects must place each card below the appro- priate stimulus card. Where ataxia prevented subjects from handling cards, the examiner placed the cards where indicated by the subject.
2. Visual-Verbal Test (VVTI (12). The VVT measures the ability to sort objects into classes according to a concept, and then to shift from this concept to another which may be evolved from the same stimulus item. Subjects are presented with plates containing four items. One subset of three is alike in some way and a second subset of three is alike in a different way. Subjects must identify each group. There are 42 plates.
Finally, depression is tested with ( 1 ) the Hamilton Rating Scale for Depression 1171, and (2) the Beck Depression In- ventory [ S ] .
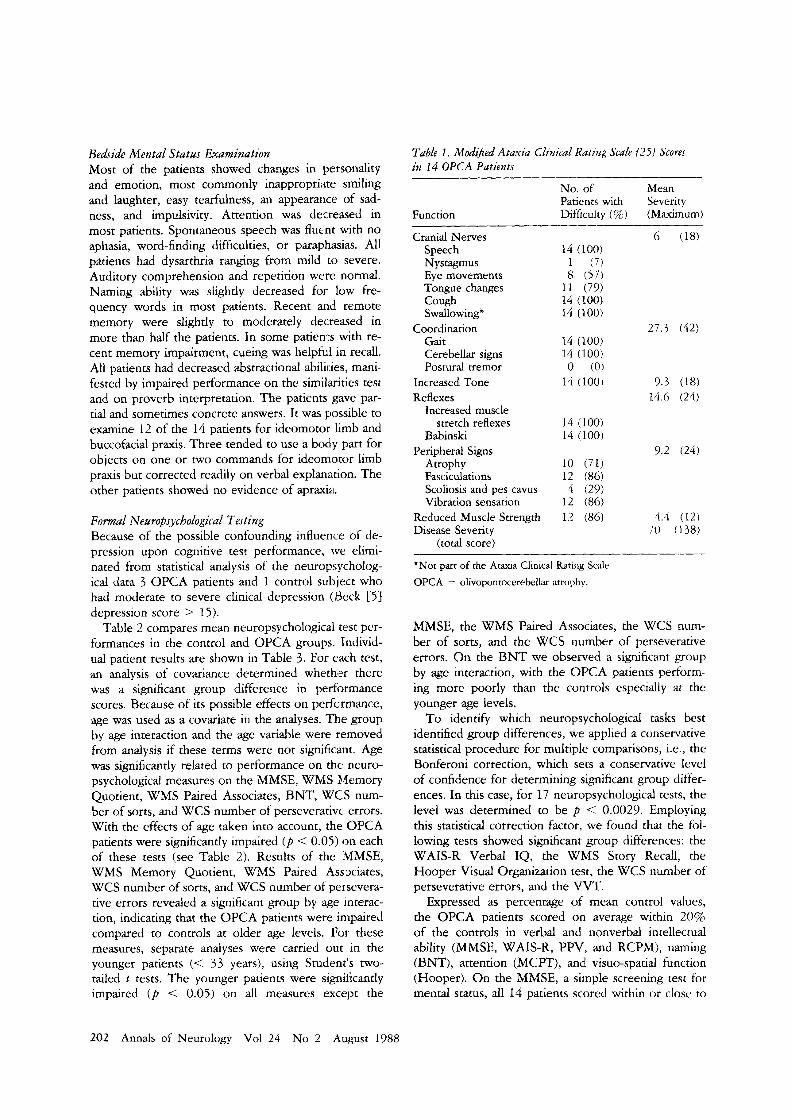
Results Neurological Findings All 14 OPCA patients had clinical features of cerebel- lar ataxia, cranial nerve involvement, hyperreflexia, and extensor plantar responses (Table 1). In addition, most had signs of motor neuron involvement with at- rophy and fasciculations. The severity of the disease, as measured by the Ataxia Clinical Rating Scale 1271 (maximum score = 135), varied considerably among the patients. Those with scores equal to or greater than 70 (n = 8) were wheelchair-bound or bedridden. Pa- tients scoring 60 or below (n = 6 ) could walk indepen- dently or with a cane or quad-cane. The severity of the disease correlated significantly with the estimated du- ration (Pearson Y = 0.63, p < 0.02).
Despite moderate to severe ataxia, most of the OPCA patients were able to take care of their personal hygiene and keep their living places in order. Some patients, despite severe ataxia, lived alone, required only parttime help for preparation of meals, and were able to care for a pet. With the exception of patient S8 (see Table 3 ) who was severely dysarthric, all others were able to engage in normal conversations, as re- ported by their spouses or caregivers.
Kish et al: Cognitive Deficits in OPCA 201
Bedside Mental Statzls Examination Most of the patients showed changes in personhty and emotion, most commonly inappropri;ne smiling No. of Mean and laughter, easy tearfulness, an appearance of sad-
Table I . Mod$ed Ataxia Clinical Rating Scale {25) Scores in 14 OPCA Patients
Patients with Severity ness, and impulsivity. Attention was decreased in most patients. Spontaneous speech was fluent with no aphasia, word-finding difficulties, or paraphasias. All patients had dysarthria ranging from mild to severe. Auditory comprehension and repetition were normal. Naming ability was slightly decreased for low fre- quency words in most patients. Recent arid remote memory were slightly to moderately decreased in more than half the patients. In some patients with re- cent memory impairment, cueing was helpful in recall. All patients had decreased abstractional abilii:ies, mani- fested by impaired performance on the similxities test and on proverb interpretation. The patients gave par- tial and sometimes concrete answers. It was possible to examine 12 of the 14 patients for ideomotor limb and buccofacial praxis. Three tended to use a body part for objects on one or two commands for ideomotor limb praxis but corrected readily on verbal explanation. The other patients showed no evidence of apraxia.
F o m l Neuropsychological Testing Because of the possible confounding influence of de- pression upon cognitive test performance, we elimi- nated from statistical analysis of the neuropsycholog- ical data 3 OPCA patients and 1 control subject who had moderate to severe clinical depression (9eck [ 5 ] depression score > 15).
Table 2 compares mean neuropsychological test per- formances in the control and OPCA groups. Individ- ual patient results are shown in Table 3. For each test, an analysis of covariance determined whether there was a significant group difference in performance scores. Because of its possible effects on perfcrmance, age was used as a covariate in the analyses. The group by age interaction and the age variable were removed from analysis if these terms were not significant. Age was significantly related to performance on the neuro- psychological measures on the MMSE, WMS Memory Quotient, WMS Paired Associates, BNT, WCS num- ber of sorts, and WCS number of perseverative errors. With the effects of age taken into account, the OPCA patients were significantly impaired ( p < 0.05) on each of these tests (see Table 2). Results of the IMMSE, WMS Memory Quotient, WMS Paired Associates, WCS number of sorts, and WCS number of persevera- tive errors revealed a significant group by age interac- tion, indicating that the OPCA patients were impaired compared to controls at older age levels. For these measures, separate analyses were carried out in the younger patients (< 33 years), using Student's two- tailed t tests. The younger patients were significantly impaired ( p < 0.05) on all measures except the
Function
Cranial Nerves Speech Nystagmus Eye movements Tongue changes Cough Swallowing'
Gait Cerebellar signs Postural tremor
Coordination
Increased Tone Reflexes
Increased muscle stretch reflexes
Babinski Peripheral Signs
Atrophy Fasciculations
Difficulty (s) (Maximum)
6 (18) 14 (100) 1 (7) 8 ( 5 7 )
1 3 (79) 14 (100) 14 (100)
27.3 (42) 14 (100) 14 (100) 0 (0)
14 (100) 9.3 (18) 14.6 (24)
14 (100) 14 (100)
10 (71) 12 (86)
Scoliosis and pes cavus 4 (29) Vibration sensation 1 2 (86)
Reduced Muscle Strength 1.2 (86) 4.4 (12) Disease Severity 70 (138)
(total score)
*Not part of the Ataxia Clinical Rating Scale OPCA = olivopontocerebellar atrophy.
MMSE, the WMS Paired Associates, the WCS num- ber of sorts, and the WCS number of perseverative errors. On the BNT we observed a significant group by age interaction, with the OPCA patients perform- ing more poorly than the controls especially at the younger age levels.
To identify which neuropsychological tasks best identified group differences, we applied a conservative statistical procedure for multiple comparisons, i.e., the Bonferoni correction, which sets a conservative level of confidence for determining significant group differ- ences. In this case, for 17 neuropsychological tests, the level was determined to be p < 0.0029. Employing this statistical correction factor, we found that the fol- lowing tests showed significant group differences: the WAIS-R Verbal IQ, the WMS Story Recall, the Hooper Visual Organization test, the WCS number of perseverative errors, and the VVT.
Expressed as percentage of mean control values, the OPCA patients scored on average within 20% of the controls in verbal and nonverbal intellectual ability (MMSE, WAIS-R, PPV, and RCPM), naming (BNT), attention (MCPT), and visuo-spatial function (Hooper). On the MMSE, a simple screening test for mental status, all 14 patients scored within o r close to
202 Annals of Neurology Vol 24 N o 2 August 1988
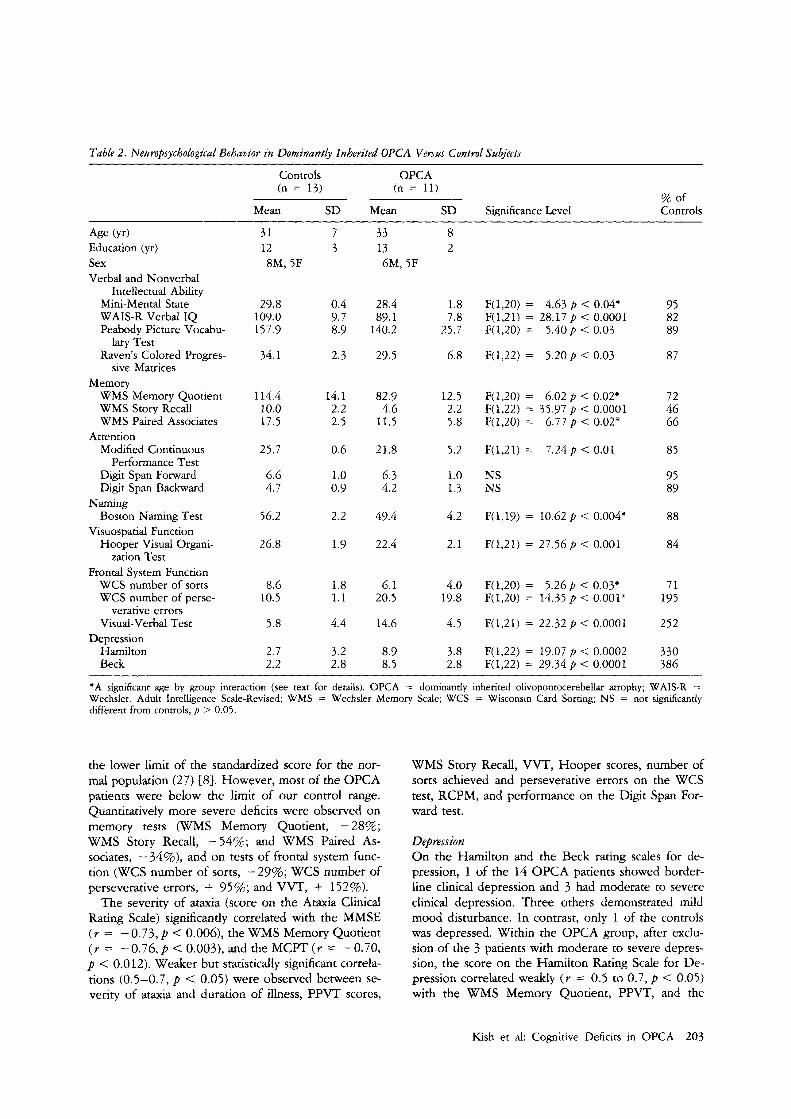
Table 2. Neuropsychological Behavior in Dominantly Inherited OPCA Versus Control Subjects
Controls OPCA (n = 13) (n = 11)
Mean SD Mean SD Significance Level
Age (yr) Education (yr) Sex Verbal and Nonverbal
Mini-Mental State WAIS-R Verbal IQ Peabody Picture Vocabu-
Raven's Colored Progres-
Intellectual Ability
lary Test
sive Matrices Memory
WMS Memory Quotient WMS Story Recall WMS Paired Associates
Modified Continuous Performance Test
Digit Span Forward Digit Span Backward
Boston Naming Test
Hooper Visual Organi-
Attention
Naming
Visuospatial Function
zation Test Frontal System Function
WCS number of sorts WCS number of perse-
verative errors Visual-Verbal Test
Depression Hamilton Beck
31 12 8M, 5F
29.8 109.0 157.9
34.1
114.4 10.0 17.5
25.7
6.6 4.7
56.2
26.8
8.6 10.5
5.8
2.7 2.2
7 3
0.4 9.7 8.9
2.3
14.1 2.2 2.5
0.6
1.0 0.9
2.2
1.9
1.8 1.1
4.4
3.2 2.8
33 13 6M, 5F
28.4 89.1
140.2
29.5
82.9 4.6
11.5
21.8
6.3 4.2
49.4
22.4
6.1 20.5
14.6
8.9 8.5
8 2
1.8 7.8
25.7
6.8
12.5 2.2 5.8
5.2
1.0 1.3
4.2
2.1
4.0 19.8
4.5
3.8 2.8
F(1,20) = F(1,21) = 28.17p < 0.0001 F(1,20) = 5.40p < 0.03
F(1,22) = 5.20p < 0.03
4.63 p < 0.04"
F(1,20) = F(1,22) = 35.77 p < 0.0001 F(1,20) =
6.02 p < 0.02*
6.77 p < 0.02"
F(1,21) = 7.24p < 0.01
NS NS
F(1,19) = 10.62 p < 0.004*
F(1,21) = 27.56p < 0.001
F( 1,20) = F(1,20) = 14.35 p < 0.001"
5.26 p < 0.03"
F(1,21) = 22.32 p < 0.0001
F(1,22) = 19.07 p < 0.0002 F(1,22) = 29.34 p < 0.0001
95 82 89
87
72 46 66
85
95 89
88
84
71 195
252
330 386
"A significant age by group interaction (see text for details). OPCA = dominantly inherited olivopontocerebellar atrophy; WAIS-R = Wechsler. Adult Intelligence Scale-Revised: WMS = Wechsler Memory Scale; WCS = Wisconsin Card Sorting; NS = not significantly different from controls, p > 0.05.
the lower limit of the standardized score for the nor- mal population ( 2 7 ) 181. However, most of the OPCA patients were below the limit of our control range. Quantitatively more severe deficits were observed on memory tests (WMS Memory Quotient, -28%; WMS Story Recall, -54%; and WMS Paired As- sociates, -34%), and on tests of frontal system func- tion (WCS number of sorts, -29%; WCS number of perseverative errors, + 95%; and VVT, + 152%).
The severity of ataxia (score on the Ataxia Clinical Rating Scale) significantly correlated with the MMSE ( Y = -0 .73 ,p < 0.006), the WMS Memory Quotient ( Y = -0.76,p < 0.003), and the MCPT ( r = -0.70, p < 0.0 12). Weaker but statistically significant correla- tions (0.5-0.7, p < 0.05) were observed between se- verity of ataxia and duration of illness, PPVT scores,
WMS Story Recall, VVT, Hooper scores, number of sorts achieved and perseverative errors on the WCS test, RCPM, and performance on the Digit Span For- ward test.
Depression On the Hamilton and the Beck rating scales for de- pression, 1 of the 14 OPCA patients showed border- line clinical depression and 3 had moderate to severe clinical depression. Three others demonstrated mild mood disturbance. In contrast, only 1 of the controls was depressed. Within the OPCA group, after exclu- sion of the 3 patients with moderate to severe depres- sion, the score on the Hamilton Rating Scale for De- pression correlated weakly ( r = 0.5 to 0.7, p < 0.05) with the WMS Memory Quotient, PPVT, and the
Kish et al: Cognitive Deficits in OPCA 203
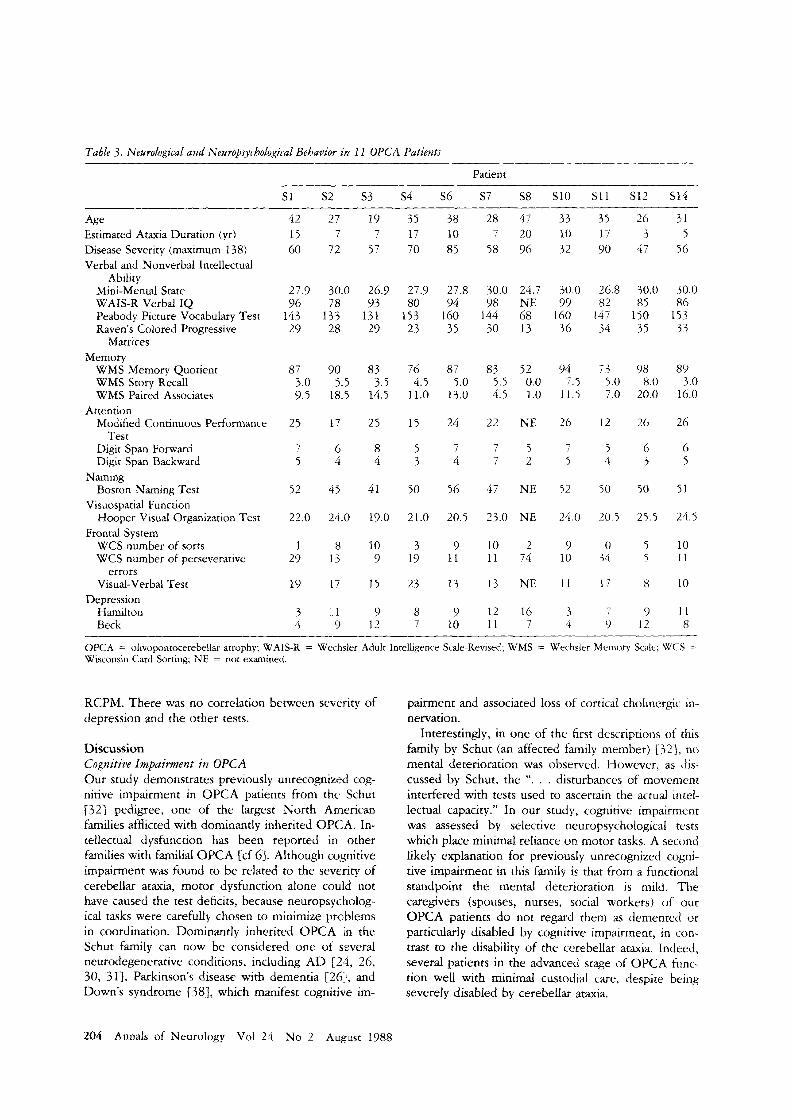
Table 3. Neurological and Neuropsychological Behavior in 1 1 OPCA PatientJ
Patient
S1 S2 S3 S4 S6 S7 S8 S10 S11 S12 S14
Age Estimated Ataxia Duration (yr) Disease Severity (maximum 138) Verbal and Nonverbal Intellectual
Ability Mini-Mental State WAIS-R Verbal IQ Peabody Picture Vocabulary Test Raven’s Colored Progressive
Matrices Memory
WMS Memory Quotient WMS Story Recall WMS Paired Associates
Modified Continuous Performance
Digit Span Forward Digit Span Backward
Boston Naming Test
Hooper Visual Organization Test
WCS number of sorts WCS number of perseverative
errors Visual-Verbal Test
Depression Hamilton Beck
Attention
Test
Naming
Visuospatial Function
Frontal System
42 27 19 35 38 28 47 33 35 26 31 15 7 7 17 10 7 20 10 17 3 5 60 72 57 70 85 58 96 32 90 47 56
27.9 30.0 26.9 27.9 27 8 30.0 24.7 30.0 26.8 30.0 30.0 96 78 93 80 94 98 NE 99 82 85 86
143 133 131 153 160 144 68 I60 147 150 153 29 28 29 23 35 30 13 36 34 15 3 %
87 90 83 76 8 7 83 52 94 73 98 89 3.0 5.5 3.5 4.5 5.0 5.5 0.0 7.5 5.0 8.0 3.0 9.5 18.5 14.5 11.0 13.0 4.5 1.0 11.5 7.0 20.0 16.0
25 17 25 15 24 22 NE 26 12 26 26
7 6 8 5 7 7 5 7 5 6 6 5 4 4 3 4 7 2 5 4 3 5
52 45 41 50 56 47 NE 52 50 50 51
22.0 24.0 19.0 21.0 20.5 23.0 NE 24.0 20.5 25.5 24.5
1 8 10 3 9 10 2 9 0 5 10 5 11 9 19 11 11 74 10 34 29 13
19 17 I5 23 13 13 NE 11 17 8 10
3 1 9 8 9 12 16 3 7 9 I1 4 9 12 7 10 11 7 4 9 12 8
OPCA = ohopontocerebellar atrophy; WAIS-R = Wechsler Adult Intelligence Scale-Revised; WMS = Wechsler Memory Scale; W<:S = Wisconsin Card Sorting; NE = not examined.
RCPM. There was no correlation between seterity of depression and the other tests.
Discussion Cognitive Impairment in OPCA Our study demonstrates previously unrecognized cog- nitive impairment in OPCA patients from the Schut [32] pedigree, one of the largest North American families afflicted with dominantly inherited OPCA. In- tellectual dysfunction has been reported in other families with familial OPCA Ecf 61. Although cognitive impairment was found to be related to the severity of cerebellar ataxia, motor dysfunction alone could not have caused the test deficits, because neuropsycholog- ical tasks were carefully chosen to minimize prcblems in coordination. Dominantly inherited OPCA in the Schut family can now be considered one of several neurodegenerative conditions, including AD [ 2 4 , 26, 30, 311, Parkinson’s disease with dementia 12611, and Down’s syndrome {38], which manifest cognitive im-
pairment and associated loss of cortical cholinergic in- nervation.
Interestingly, in one of the first descriptions of this family by Schut (an affected family member) r321, no mental deterioration was observed. However, as dis- cussed by Schut, the I ‘ . . . disturbances of movement interfered with tests used to ascertain the actual intel- lectual capacity.” In our study, cognitive impairment was assessed by selective neuropsychological tests which place minimal reliance on motor tasks. A second likely explanation for previously unrecognized cogni- tive impairment in this family is that from a functional standpoint the mental deterioration is mild. The caregivers (spouses, nurses, social workers) of our OPCA patients do not regard them as demented or particularly disabled by cognitive impairment, in con- trast to the disability of the cerebellar ataxia. Indeed, several patients in the advanced stage of OPCA func- tion well with minimal custodial care, despite being severely disabled by cerebellar ataxia.
204 Annals of Neurology Vol 24 No 2 August 1988

Although in a restricted environment such as a nurs- ing home, dementia might not be recognized in these patients, disability due to the cognitive impairment might be observed in more demanding environments (e.g., workplace).
Dementia in OPCA and the Cholinergic Hypothesis We have recently demonstrated in OPCA brain a marked cortical cholinergic deficiency, evidenced by reduced activity of the cholinergic marker enzymes choline acetyltransferase C2 11 and acetylcholinesterase [223 (7 cases examined), together with a severe loss of nucleus basalis cholinergic neurones (Kish and Robitaille, unpublished observations; 5 cases exam- ined). These findings were observed in all affected family members autopsied who died with ataxia sever- ity and age similar to those of the patients in our pres- ent neuropsychological study. Since the magnitude of the cerebral cortical cholinergic deficit in OPCA (mean cerebral choline acetyltransferase reduction of 65 to 72%) in the 7 cases biochemically studied was as severe as that observed in clinically disabling AD de- mentia 124, 26, 30, 311, we reasoned that, should the cholinergic dysfunction actually represent a fundamen- tal biochemical cause of the cognitive impairment in AD, an Alzheimer’s-like dementia in this OPCA fam- ily should be uncovered upon comprehensive neuro- psychological testing. Our finding of subnormal per- formance on cognitive testing in this OPCA family adds circumstantial support for the cholinergic hy- pothesis of dementia; however, the neuropsychological profile also suggests that the cognitive impairments in OPCA differ from those in AD dementia both in se- verity and behavioral pattern of deficits. Cortical cho- linergic deficits in AD of the magnitude previously observed in the Schut family are associated with a moderate to severe dementia. These AD individuals were clearly disabled by their dementia in most aspects of daily living [31}. In contrast, our patients appeared to be only mildly demented, with scores on a mental screening test (MMSE) close to or within control lim- its, and they did not appear disabled by their cognitive impairment in daily living skills. Employing DSM-III- R 171 criteria, the majority of patients would most likely be considered only mildly demented.
Our neuropsychological data also suggest that the OPCA patients do not have the behavioral profile of cognitive changes observed in AD dementia. In this regard, and as also observed by Tagliavini and Pilleri {35} in a single case with dominantly inherited OPCA (and accompanying nucleus basalis cholinergic neurone loss), none of our patients experienced aphasia, apraxia, or agnosia, all commonly present in AD. Also, the OPCA patients scored poorly on the WCS perse- verative errors and the VVT, pointing to a prominent cognitive impairment in the frontal system. In contrast,
most A D patients with MMSE scores similar to those of our OPCA patients (2 27) perform within the nor- mal range on the Weigl Test, a test similar to the WCS {cf 17; Huff, personal communication]. Our patients have relatively prominent frontal deficits without aphasia, which more closely resembles “subcortical” or “frontal-subcortical” dementia [l, cf 141 than AD de- mentia.
In conclusion, we report previously unrecognized cognitive impairment in 11 OPCA members of a fam- ily previously shown to have a cerebral cortical cholin- ergic deficiency as severe as that in AD brain. While our data provide circumstantial support for the cholin- ergic hypothesis of AD dementia, our observations also support our working hypothesis, namely, that the cholinergic reduction explains some but not all of the AD dementia. From this revised hypothesis we predict that cholinergic pharmacotherapy in AD will prove to be of limited use 1331. Prospective comparison of the neurobehavioral, neurochemical, and neuropatholog- ical changes in our OPCA versus AD patients may help to resolve this clinically important question.
The authors gratefully acknowledge the financial assistance of the Medical Research Council of Canada (S. K. and M. F.), the National Ataxia Foundation (U.S.A.) (S. K.), the Ontario Mental Health Foundation (M. F.), and a scholarship to Dr Freedman from the Gerontology Research Council of Canada. Dr Oscar-Berman was supported by the U.S. Veterans Administration and U.S. DHHS- NIAAA grant AA07112 to Boston University. Dr Kish is a Career Scientist of the Ontario Ministry of Health.
We also wish to thank Celia Greenwood, Stephanie Bernstein, and Reesa Hotz-Sud for assistance with data analysis.
Presented in part at the 112th annual meeting of the American Neurological Association, San Francisco, CA, October 1787.
References 1.
2.
3.
4.
5 .
6.
7.
8.
Albert ML, Feldman RG, Willis AL The “subcortical dementia” of progressive supranuclear palsy. J Neurol Neurosurg Psychia- try 37:121-130, 1974 Allain H, Reymann JM, Cognez P, et al: Alzheimer’s disease and the cholinergic hypothesis: an overview. In Bes A, Cahn J, Cahn R, et al (eds): Senile Dementias: Early Detection. London: Libbey, 1986, pp 331-336 Bartus RT, Dean RC, Beer B, et al: Cholinergic hypothesis of geriatric memory dysfunction. Science 2 17:408-4 17, 1982 Bartus RT, Flicker C, Dean RL, et al: Selective memory loss following nucleus basalis lesions: long-term behavioral recovery despite persistent cholinergic deficiencies. Pharmacol Biochem Behav 23:125-135, 1985 Beck AT, Ward CH, Mendelson M, et al: An inventory for measuring depression. Arch Gen Psychiatry 4:561-571, 1961 Berciano J: Olivopontocerebeltar atrophy. A review of 117 cases. J Neurol Sci 53:253-272, 1982 Berg EA: A simple objective test for measuring flexibility in thinking. J Gen Psycho1 39: 15-22, 1948 Bleecker ML, Bolla-Wilson K New age-specific norms for the Mini-Mental State Exam. Neurology (Suppl) 1:279, 1987
Kish et al: Cognitive Deficits in OPCA 205

9. Diagnostic and Statistical Manual of Mental Disorders, 3rd edi- tion-revised. Washington, DC: American Psychiatric Associa- tion, 1987, p 107
10. Drachman DA, Leavitt J: Human memory and thc cholinergic system. Arch Neurol 30:113-121, 1974
11. Dunn LM: Expanded manual for the Peabody Piciure Vocabu- lary Test. Circle Pines, MN: American Guidance Itervice, 1965
12. Feldman MJ, Drasgow J: The Visual-Verbal Test Manual. Los Angeles: Western Psychological Services, I959
13. Folstein MF, Folstein SE, McHugh PR: “Mini Mental State”: a practical method for grading cognitive state of patients for the clinician. J Psychiarr Res 12:189-198, 1975
14. Freedman M, Albert M L Subcortical dementia. In Fredericks JAM (ed): Handbook of Clinical Neurology. Neurobehavioural Disorders, Vol 2(46) . Amsterdam: Elsevier Scie’ice, 1985, pp
15. Grant DA, Berg EA. A behdviourd analysis of c,egree of rein- forcement and ease of shifting to new responses i n a Weigl-type card-sorting problem. J Exp Psycho1 38:401-441, 1948
16. Gray RC, Oliver CP: Marie’s hereditary cerebellar ataxia (oljvop~~ntocerebellar atrophy). Minn Med 24:3’!7-335, 1941
17. Hamilton M: A rating scale for depression. J Neiirol Neurosurg Psychiatry 12:56-62, 1960
18. Hooper HE: The Hooper Visual Organization T’:st Manual. Los Angeles: Western Psychological Services, 1958
10. Huff FJ, Becker JT, Belle SH, er al: Cognitive deficits and clinical diagnosis of Alzheimer’s disease. Neurology 37: 1 119- 1124, 1987
20. Kaplan E: Boston Naming Test. Philadelphia: I r a and Febiger, 1982
2 I . Kish SJ, Currier RD, Schut L, et al: Brain choline acetyltransfer- ase reduction in dominantly inherited olivopoiitocerebellar at- rophy. Ann Neurol 22:272-275, 1987
2 2 . G s h SJ, Schut L, Simmons J, et al: Brain acetylcholinesterase is markedly reduced in dominantly inherited olivopontocerebellar atrophy. J Neurol Neurosurg Psychiatry 5 1:544-548, 1988
21. hlirsky A: Behavioral and psychophysiological .markers of disor- dered attention. Environmental Health Perspectives 74: 191- 199, 1987
311-316
24. Perry EK, Perry RH: The cholinergic rystem in Alzheimer’s disease. In Roberts PJ (ed): Biochemistry of Dementia. New York: John Wiley, 1980, pp 135-183
25. Perry EK. The cholinergic hypothesis-ten years o n . Hr Med
26. Perry EK, Curtis M, Dick DJ, et al: Cholinergic correlates of cognitive impairment in Parkinson’s &ease: compartscins with Alzheimer’s disease. J Neurol Neurosurg Psychiatry 48:4 13- 421, 1985
27. Pourcher E, Barbeau A: Field testing o f ataxia scoring and stag- ing system. Can J Neurol Sci 7:339-344, 1980
28. Raven JC: Guide to using the coloured progressive. matrices. London: H K Lewis, 1965
29. Rich SS, Wilkie PJ, Schut L, set al: Spinocerebellar ataxia: locali- zation of an autosomal dominant locus between two markers on human chromosome 6. Am J Human Genet 4 1.524--5 5 I, I987
30. Rossor MN, Garrett NJ, Johnson AI., et al: A post-mortem study of the cholinergic and GABA systems in scnilc Jemctntia. Brain 105:313-330, 1982
31. Rossor MN, Iversen LL, Reynolds GP, et al Neurochemical characteristics of early and late onset types of Alzheimer’s dis- ease. Br Med J 288:961-96)4, 1984
32. Schut JW: Hereditary ataxia: clinical study through 5ix gcnera- tions. Arch Neurol Psychiatry 168:-5--95, 1950
33. Stern Y , Sano M, Mayeux R. Effects of oral physosripminc iri Alzheimer’s disease. Ann Neurol 22.30h-310. 1?H!
34. Sunderland T, Tarior PN, Cohen RM, er d: Anti<holinergic sensitivity in patients with dementia of the A1zheimc.r type and age-marched controls. Arch Gen Psychiatry 44.4 IX--426, 1087
35. Tagliavini F , Pilleri G: Neuronal loss in the hasdl nucleus of Meynert in a patient with olivopcinn~cerebell:rr atrophy. Actlr Neuropathol 66127-133. I985
36. Wechsler D: Wechsler Memory Stale. New York Psycholop cal Corporation, 1973
37. Wechsler D: WAIS-R Manual. Niw York: Psychoiogicdl Cor- poration, 1981
38. Yates CM, Simpson J, G d o n A. Regional brain 5-hydroxy- tryptamine levels are reduced in smile Down’s syrirlr~imc as i n
Alzheimer’s disease. Neurosci Le t t 0 5 : 189- 102. 1<)86
Bull 42:63-69, 1986
206 Annals of Neurology Vol 24 No 2 August 1988
Related Documents











